
Abstract
Background:
Hip arthroscopy has demonstrated favorable short- and mid-term outcomes for femoroacetabular impingement syndrome (FAIS) in patients with borderline hip dysplasia (BHD). However, long-term outcomes in patients with FAIS and BHD treated with hip arthroscopy remain understudied.
Purpose:
To evaluate hip survivorship and patient-reported outcomes (PROs) in patients with FAIS and BHD compared with those without BHD at a minimum 10-year follow-up.
Study Design:
Cohort Study; Level of evidence, 4.
Methods:
A retrospective matched-cohort study was conducted on patients undergoing primary hip arthroscopy for FAIS by a single surgeon (2012-2024). BHD was defined as a lateral center-edge angle (LCEA) of 20° to 25°. Patients with BHD were matched 1 to 2 to controls without BHD based on age, sex, body mass index, and preoperative modified Harris Hip Score (mHHS). Radiographic parameters (eg, alpha angle, LCEA) were assessed pre- and postoperatively. PROs—including mHHS, Non-Arthritic Hip Score (NAHS), and hip survivorship (revision arthroscopy, conversion to total hip arthroplasty [THA])—were compared.
Results:
The study included 23 patients with BHD (mean age, 33.6 years; 69.6% women) and 46 controls (mean age, 32.7 years; 65.2% women). Both groups showed significant improvements in mHHS and NAHS at 10 years (all P < .001), with no differences in postoperative scores or minimal clinically important difference achievement (BHD group, 91.3% vs control group, 97.5%; P = .55). There were no conversions to THA in the BHD group and 2 in the control group (4.3%; P = .189). Revision arthroscopy rates were 0% in the BHD group and 8.7% in the control group (P = .549). Patients with BHD exhibited significantly greater reductions in alpha angles on 45° Dunn views (−13° vs −1.9°; P = .01).
Conclusion:
At a minimum 10-year follow-up, patients with BHD who underwent hip arthroscopy for FAIS achieved comparable PROs and hip survivorship to those without BHD. These findings support the use of hip arthroscopy as a durable and effective treatment for FAIS in this population.
Keywords
In recent years, hip arthroscopy has gained popularity, becoming the primary treatment tool for the majority of nonarthritic intra-articular hip pathologies—including femoroacetabular impingement syndrome (FAIS).6,10 However, for patients with concomitant borderline hip dysplasia (BHD), there is still ongoing debate regarding the preferred treatment for FAIS.2,25 Patients with BHD, defined by decreased acetabular coverage, present unique biomechanical challenges related to shallow coverage and resulting hip instability.7,32 There is disagreement in the literature about what exactly constitutes BHD, although it is commonly considered to include patients with a lateral center edge angle (LCEA) of between 20° and 25°. Historically,19,21,29 periacetabular osteotomy has been the treatment of choice for hip dysplasia, particularly when the LCEA is >18°. However, as periacetabular osteotomy is a more invasive and involved procedure, hip arthroscopy has gained favor as a less invasive alternative for treating concomitant FAIS and labral tears in patients with BHD. 24
Several studies have demonstrated that patients with BHD undergoing hip arthroscopy for FAIS achieve good short- and mid-term outcomes, with results comparable to those of patients without BHD.16,17,23 While short-term studies generally indicate favorable outcomes, longer follow-up studies, such as the work by Chapman et al, 8 suggest that patients with BHD may experience lower rates of clinically meaningful improvements, as reflected by lower rates of achieving the patient acceptable symptom state at 10 years. Understanding long-term outcomes of hip arthroscopy in patients with BHD is especially important, as these patients are predisposed to hip instability and abnormal stress distribution patterns, which may only become apparent at longer follow-up periods.13,14
This study, therefore, aimed to examine the clinical outcomes of hip arthroscopy in patients with FAIS and BHD compared with those without BHD at 10-year follow-up. We hypothesized that patients with FAIS and BHD would demonstrate no significant difference in hip survivorship or patient-reported outcomes (PROs) compared with patients with FAIS without hip dysplasia.
Methods
Study Design and Ethical Approval
A retrospective matched-cohort study was conducted using data from a prospectively collected database of patients who underwent hip arthroscopy for FAIS by a single sports medicine fellowship-trained orthopedic surgeon (T.Y.) at a single urban academic medical center between January 2010 and December 2013. All patients provided consent for study participation as outlined by the approved institutional review board (IRB) protocol (IRB Protocol i15-00058).
Cohort Selection and Matching
For this study, BHD was defined as LCEA between 20° and 25° based on Wiberg’s original classification. 31 For patients with BHD, the inclusion criteria were ≥18 years at the time of surgery, (2) diagnosis of FAIS based on clinical and radiographic findings, (3) primary surgery, (4) radiographic evidence of BHD as indicated by LCEA between 20° and 25°, and (5) minimum 10-year follow-up. The inclusion criteria for controls without BHD were identical, except that they required a normal LCEA, defined as 25° to 40°. Both groups had exclusion criteria of (1) Tönnis grade >1 or hip joint space <2 mm, (2) radiographic evidence of hip dysplasia (LCEA <20°) or acetabular overcoverage (LCEA >40°), (3) history of rheumatological disease, (4) history of slipped capital femoral epiphysis, and (5) previous ipsilateral hip surgery. Figure 1 displays radiographs of hips with and without BHD. To assess potential bias due to loss to follow-up, baseline characteristics and clinical outcomes were compared between patients with BHD who completed at least 10 years of follow-up and those who did not.
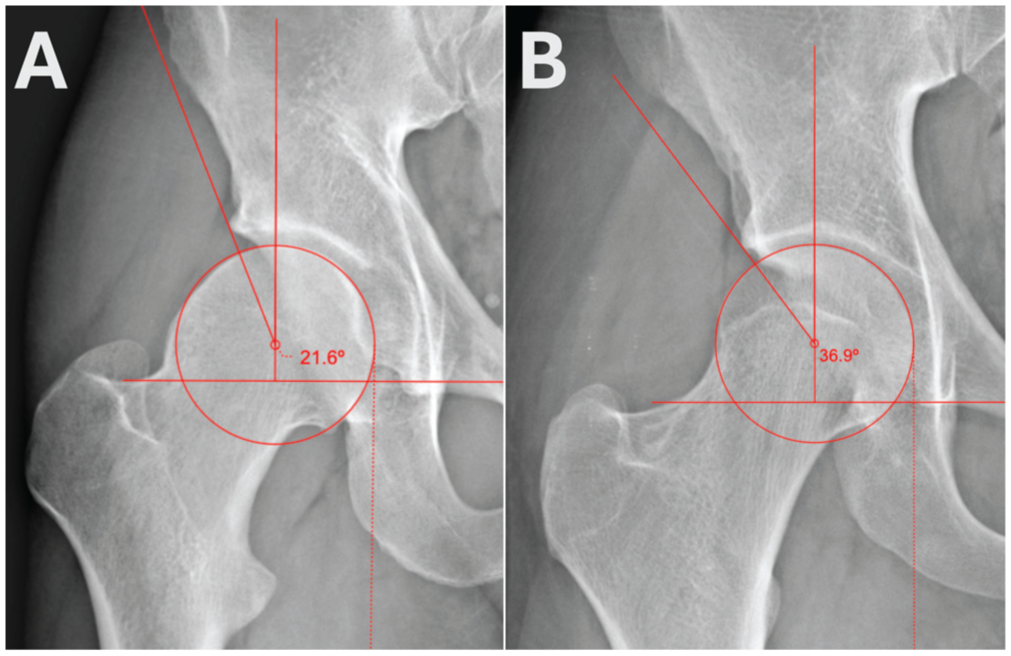
Radiographs of hips with and without borderline hip dysplasia. (A) Hip with BHD, demonstrating an LCEA of 21.6°. (B) Hip with BHD, demonstrating an LCEA of 36.9°. BHD, borderline hip dysplasia; LCEA, lateral center edge angle.
Cohort matching was performed using SPSS Statistics, Version 29.0.2.0 (IBM Corp). Patients with BHD were matched 1 to 2 to controls without BHD based on age, sex, body mass index (BMI), and preoperative modified Harris Hip Score (mHHS) using propensity score matching. Balance diagnostics—including the percent reduction in the standardized mean difference of the logit propensity score and the variance ratio—were calculated after matching.
Diagnostic Inclusion and Surgical Indications
Patients were diagnosed with FAIS based on a clinical history of pain localized to the hip, physical examination, and radiographic findings. Provocative testing for anterior impingement and Patrick tests were performed in the clinic. FAIS morphology was identified on plain hip radiographs with standing anteroposterior (AP), 45° Dunn, and 90° Dunn views. Magnetic resonance imaging and/or magnetic resonance arthrography were used to identify concomitant soft tissue pathology of the cartilage, labrum, and chondrolabral junction. Radiographic evidence of FAI morphology included alpha (α) angle ≥55° (cam morphology) and/or crossover sign (pincer morphology due to acetabular retroversion). While LCEA >40° was considered indicative of pincer morphology due to acetabular overcoverage, these patients were excluded from the cohort as per the eligibility criteria.
All patients underwent a trial of nonsteroidal anti-inflammatory medications and physical therapy for at least 6 weeks before undergoing surgery. In patients with atypical hip pain, a diagnostic injection into the symptomatic hip joint was performed to localize the cause of the symptoms and provide symptomatic relief. If these nonoperative measures failed to provide lasting relief, surgical treatment was offered.
Surgical Technique and Rehabilitation Protocol
All patients received general anesthesia with local anesthetic intraoperative injection or regional anesthesia and were positioned supinely on a hip distraction system. Standard portal placement, comprising mid-anterior and anterolateral portals, was used for all cases. Access to the joint was obtained through interporal capsulotomy using a beaver blade. Any chondral delamination or synovitis was debrided. Shaving chondroplasty was used to stabilize chondral borders for Outerbridge grade 1 to 3 lesions. All labral tears were repaired, preserving the chondrolabral junction whenever possible. In cases of nonviable tissue, selective debridement was performed. Cam and Pincer-type impingement were then identified by dynamic fluoroscopic examination of the hip joint. Femoral osteochondroplasty was performed to correct cam deformity, and acetabuloplasty was performed to correct pincer deformity. Resection in both cases was guided by fluoroscopy, with the intent of restoring concavity or head-neck offset without violating subchondral bone or compromising acetabular coverage. This conservative approach focused on avoiding overcorrection to maintain native joint stability and biomechanics.5,9,15 In patients with BHD, acetabuloplasty was minimal. Bleeding bone was achieved, but no significant acetabular resection was performed. Subspine impingement was resected. Routine capsular closure was not implemented by the senior author until 2016; therefore, none of the patients in this study underwent capsular closure.
After surgery, all patients were given a hip brace to restrict hip extension and external rotation for 2 weeks. Activity was restricted to flatfoot weightbearing on the operative side with assistive crutches for 4 weeks. All patients were discharged with 3 days of cephalexin (500 mg, 4 times daily) for infection prophylaxis, celecoxib (200 mg per day) for 14 days for heterotopic ossification prevention, and aspirin (81 mg per day) for 7 days for deep venous thrombosis prophylaxis.
Radiographic Measurements and Classifications
Pre- and postoperative hip radiographs were obtained as standard of care for all patients, with postoperative radiographs obtained within 1 to 2 weeks after surgery. The alpha angle was measured on AP, 45° Dunn, and 90° Dunn views. The LCEA, Tönnis angle and grade, the Femoro-Epiphyseal Acetabular Roof (FEAR) index, and the anterior wall index (AWI) were measured on AP view.
The severity of the cam lesions was classified based on alpha-angle cutoff values as defined by Agricola et al. 1 A lower cutoff of 60° and a higher cutoff of 78° were used to categorize participants. Those with an alpha angle <60° were classified as not having cam morphology, while those with angles between 60° and 78° were considered to have mild/moderate cam lesions. An alpha angle >78° indicated the presence of large cam lesions.
On AP view, acetabular retroversion was assessed through the presence of the ischial spine sign (ischial spine projecting medial to the pelvic brim), posterior wall sign (posterior wall line medial to the femoral head center), and crossover sign (anterior acetabular wall crosses over posterior acetabular wall). 18 Participants were divided into 3 groups based on the presence or absence of retroversion signs: global retroversion (both the posterior wall sign and crossover sign were positive), focal retroversion (at least 1 sign was positive, but either the posterior wall sign or the crossover sign was negative), and no retroversion (all signs were negative). Figure 2 displays radiographs of hips with BHD and the levels of retroversion.
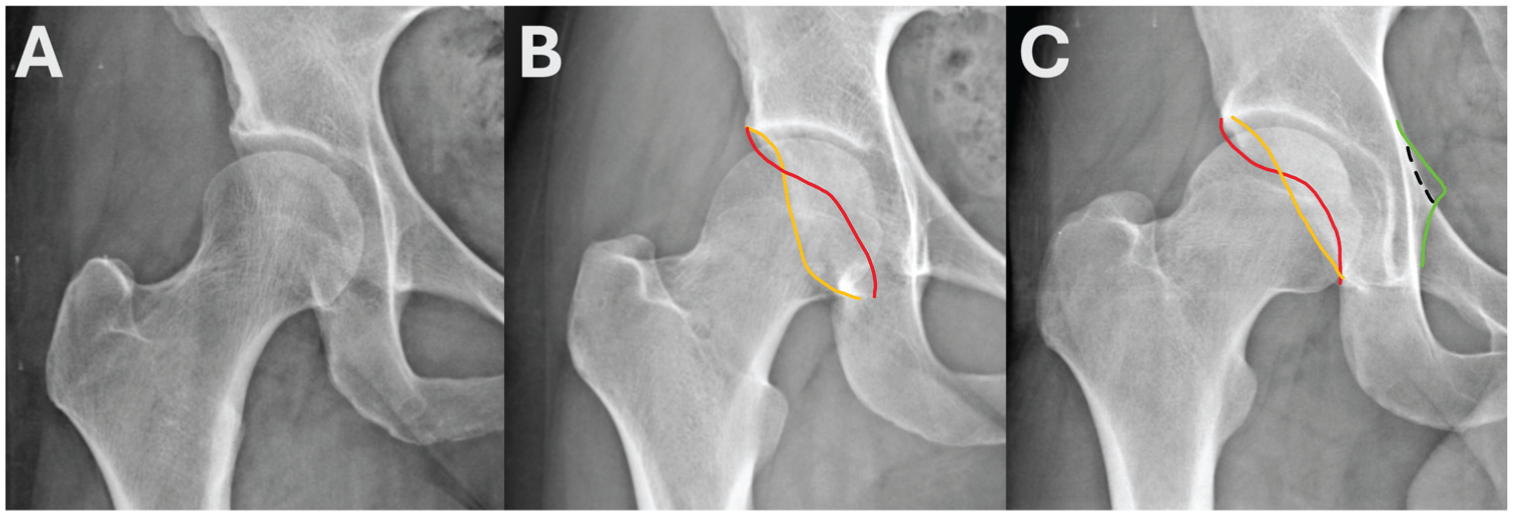
Radiographs of hips with varying retroversion. (A) Hip with BHD, no retroversion. (B) Hip with BHD, focal retroversion (crossover sign only). (C) Hip with BHD, global retroversion. BHD, borderline hip dysplasia.
The FEAR index was assessed on the AP pelvis view as an additional marker of hip stability. 33 Positive values represented a laterally directed angle, consistent with decreased femoral head containment and increased instability. Negative values indicated a medially directed angle, reflecting stable acetabular coverage. 33
Outcomes Measured
Reoperations—including revision arthroscopies and conversions to total hip arthroplasty (THA)—were documented. For this study, reoperations were defined as any additional procedures involving the same hip joint, such as revision arthroscopy or conversion THA. Intraoperative data collection included assessment of acetabular cartilage damage using the Outerbridge classification, documentation of whether cam and/or pincer resections were performed, labral treatment strategy, and the number of suture anchors deployed for labral repair.
The Nonarthritic Hip Score (NAHS) and the mHHS were measured both before surgery and at 10-year follow-up. Achievement of minimal clinically important difference (MCID) for both outcome measures was determined using cohort-specific cutoff values. Cutoff values for the MCID were calculated using a distribution-based method previously described by Watt et al, 30 where the MCID threshold is defined as one-half of the pooled standard deviation of preoperative scores across all study arms. MCID cutoff values for mHHS and NAHS were calculated separately. Patients who required subsequent revision surgery or conversion to THA were excluded from PRO analysis.
Statistical Analysis
Previous power analysis was conducted with G*Power (Version 3.1.9.7; Heinrich-Heine-Universität Düsseldorf) to determine the required sample size to detect a clinically meaningful difference in mHHS scores at 10-year follow-up. The MCID for the mHHS was set at 8.2 as determined by Nwachukwu et al. 26 A pooled standard deviation of 9.84, derived from Selley et al, 27 was used to represent the variability in mHHS scores at a mean 9.6-year follow-up for BHD and control patients. Utilizing an alpha level of .05 and assuming 2-tailed testing of independent means, 62 patients (21 cases and 41 controls) were deemed sufficient for attainment of ≥85% statistical power.
All statistical analyses were performed using SPSS Statistics, Version 29.0 (IBM Corp). Descriptive statistics were calculated for all variables, with means and standard deviations reported for continuous variables, and counts and percentages for categorical variables. The Shapiro-Wilk test was used to assess normality in continuous variables. Paired samples t tests were used to assess normally distributed continuous variables, while the Mann-Whitney U test was used for non-normally distributed variables. The Wilcoxon signed-rank test was used to evaluate differences in pre- and postoperative quantities (ie, radiographic measurements and outcome scores). Categorical variables between groups were compared using the Fisher exact test. P < .05 was considered significant.
Results
Patient Flow and Matching Results
Patient selection and flow sequence are outlined in Figure 3. From an initial cohort of 282 patients with FAIS, 52 declined participation, and 17 underwent index revision surgery, leaving 213 eligible patients. A total of 162 patients (76.1%) had complete preoperative and 10-year follow-up data. Of these 162 patients, 137 met the inclusion criteria for the study. Also, 23 were identified as having BHD, while 114 had normal LCEA. All 23 patients with BHD were successfully matched to 2 controls each (46 controls in total). Post-match diagnostic assessments showed an 80% reduction in the standardized mean difference of the propensity score and a variance ratio of 1.08, confirming adequate matching on the selected covariates.
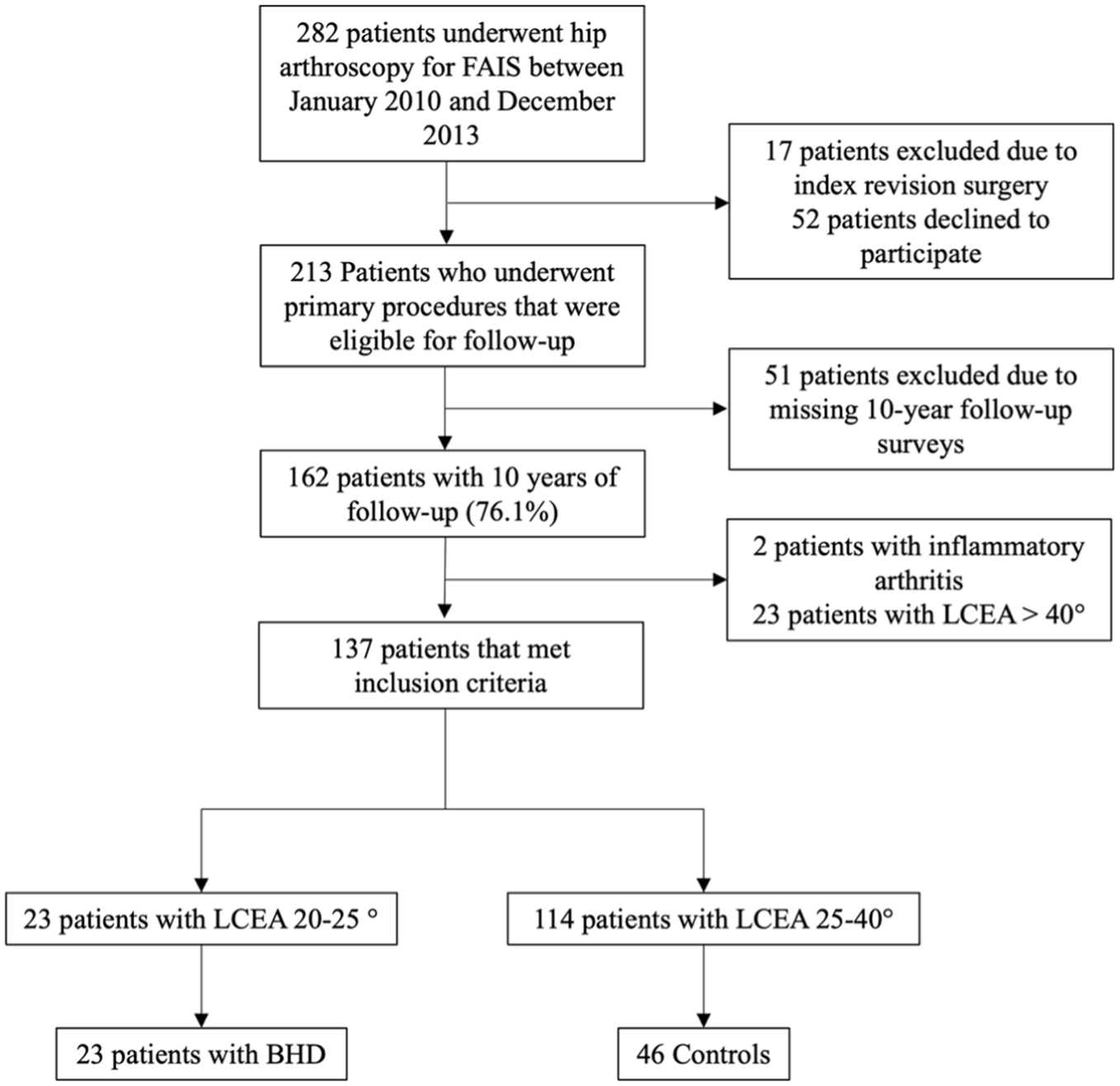
Patient flow. BHD, borderline hip dysplasia; LCEA, lateral center edge angle.
Demographic Comparison
Table 1 contains descriptive data for the BHD group and the matched cohorts. No significant differences were observed in the matched demographic characteristics of age, sex, and BMI between the 2 groups (all P > .05).
Descriptive Data a
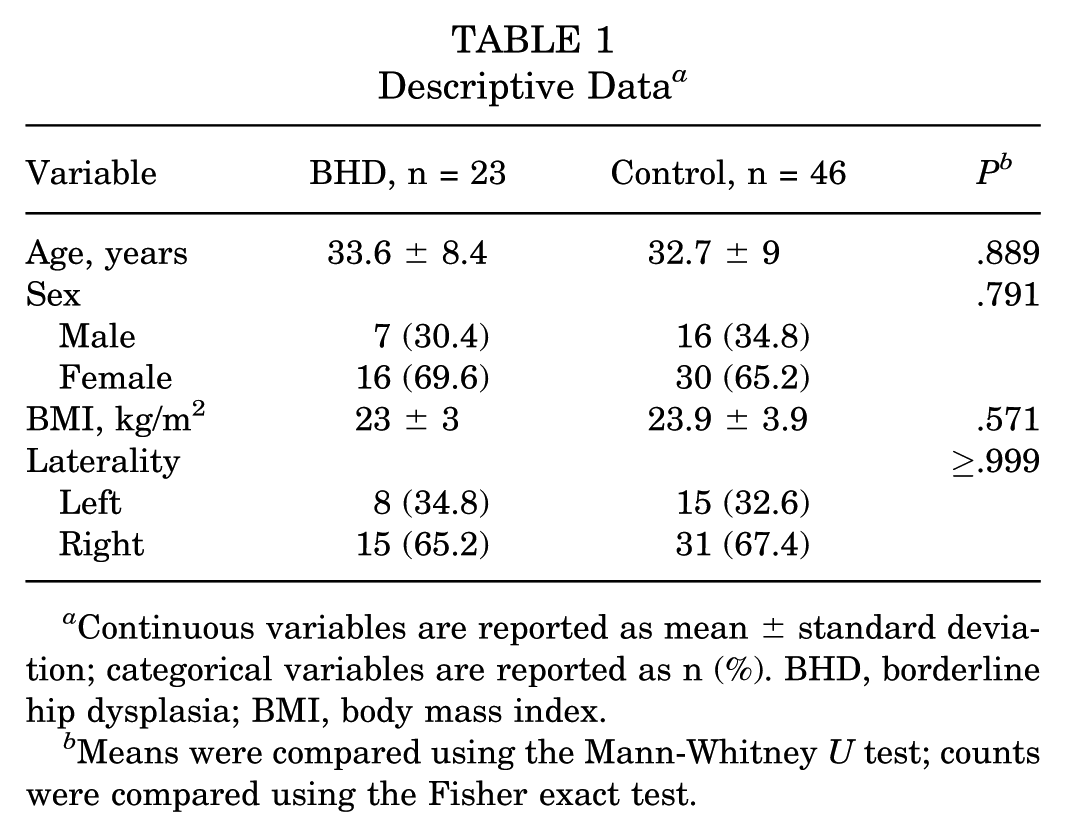
Continuous variables are reported as mean ± standard deviation; categorical variables are reported as n (%). BHD, borderline hip dysplasia; BMI, body mass index.
Means were compared using the Mann-Whitney U test; counts were compared using the Fisher exact test.
Comparison of Included Versus Excluded BHD Patients
Table 2 contains baseline and clinical outcome information for included and excluded patients with BHD. Eleven patients with BHD were excluded from the study (7 declined to participate, 4 were lost to follow-up). No significant differences were observed between the included and excluded patients with BHD with respect to age, sex, BMI, laterality, LCEA, and baseline mHHS and NAHS scores (all P > .05). No patients with BHD, included or excluded, underwent revision arthroscopy or conversion to THA.
Descriptive Data of Included and Excluded Patients With BHD a
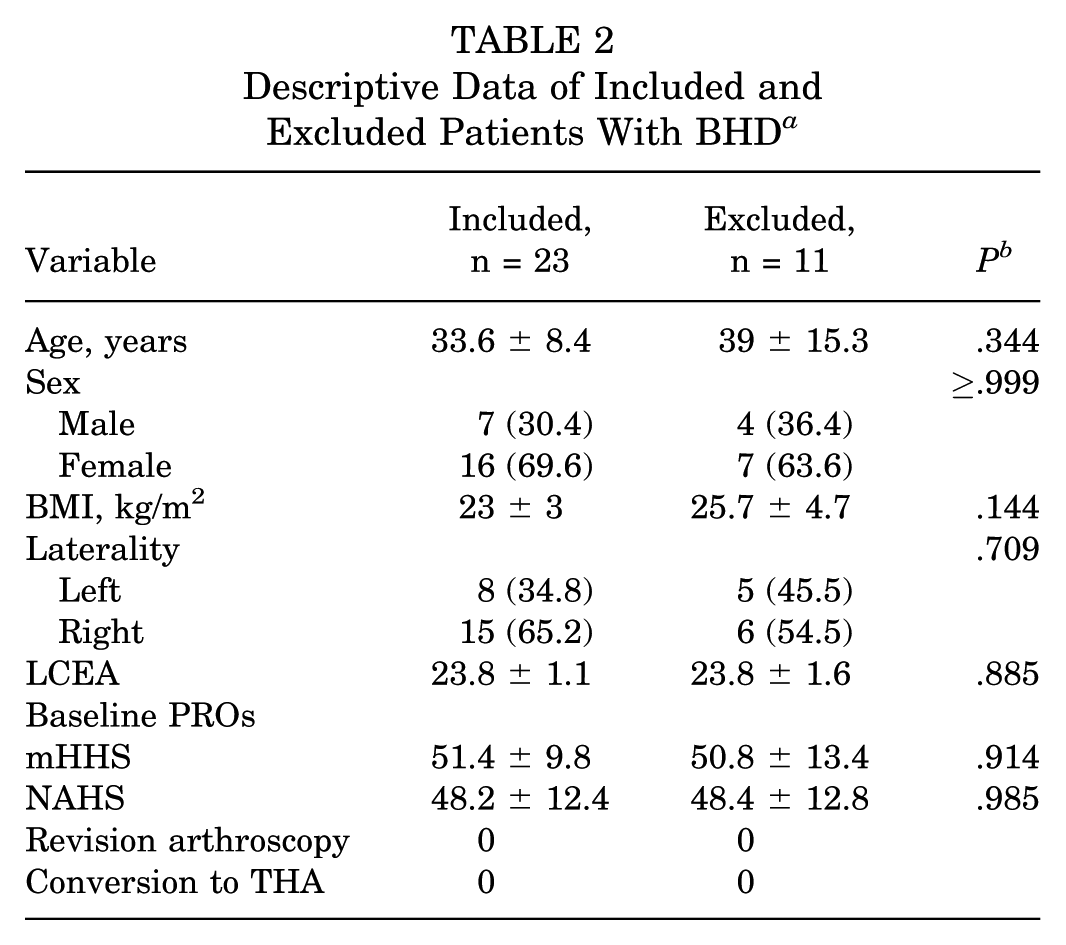
Continuous variables are reported as mean ± standard deviation; categorical variables are reported as n (%). BHD, borderline hip dysplasia; BMI, body mass index; LCEA, lateral center edge angle; mHHS, modified Harris Hip Score; NAHS, Non-Arthritic Hip Score; PRO, patient-reported outcome; THA, total hip arthroplasty.
Means were compared using the Mann-Whitney U test; counts were compared using the Fisher exact test.
Radiographic Findings
Table 3 displays pre- and postoperative radiographic findings. The mean preoperative LCEA was significantly lower in the BHD group compared with the control group (23.8 ± 1.1 vs 31.3 ± 3.5; P < .001). The preoperative Tönnis angle in the BHD group was significantly higher than the control group (9.7 ± 3.29 vs 4.8 ± 4; P < .001). Patients in the BHD group also had a significantly lower AWI compared with controls (0.31 ± 0.099 vs 0.44 ± 0.056; P < .001). No significant difference in FEAR index was found between groups (−5.7 ± 2.8 vs −7.7 ± 4.6; P = .110). No significant differences between the groups (all P > .05) were found in preoperative alpha angle on all views, distribution of cam lesion size (none, mild, or large), incidence of acetabular retroversion signs, or distribution of acetabular retroversion categories (non, focal, or global). Tönnis grade distribution was similar between groups, with 82.6% of patients with BHD and 73.9% of controls demonstrating grade 0 changes, and 17.4% and 26.1%, respectively, demonstrating grade 1 changes (P = .550).
Radiographic Findings a
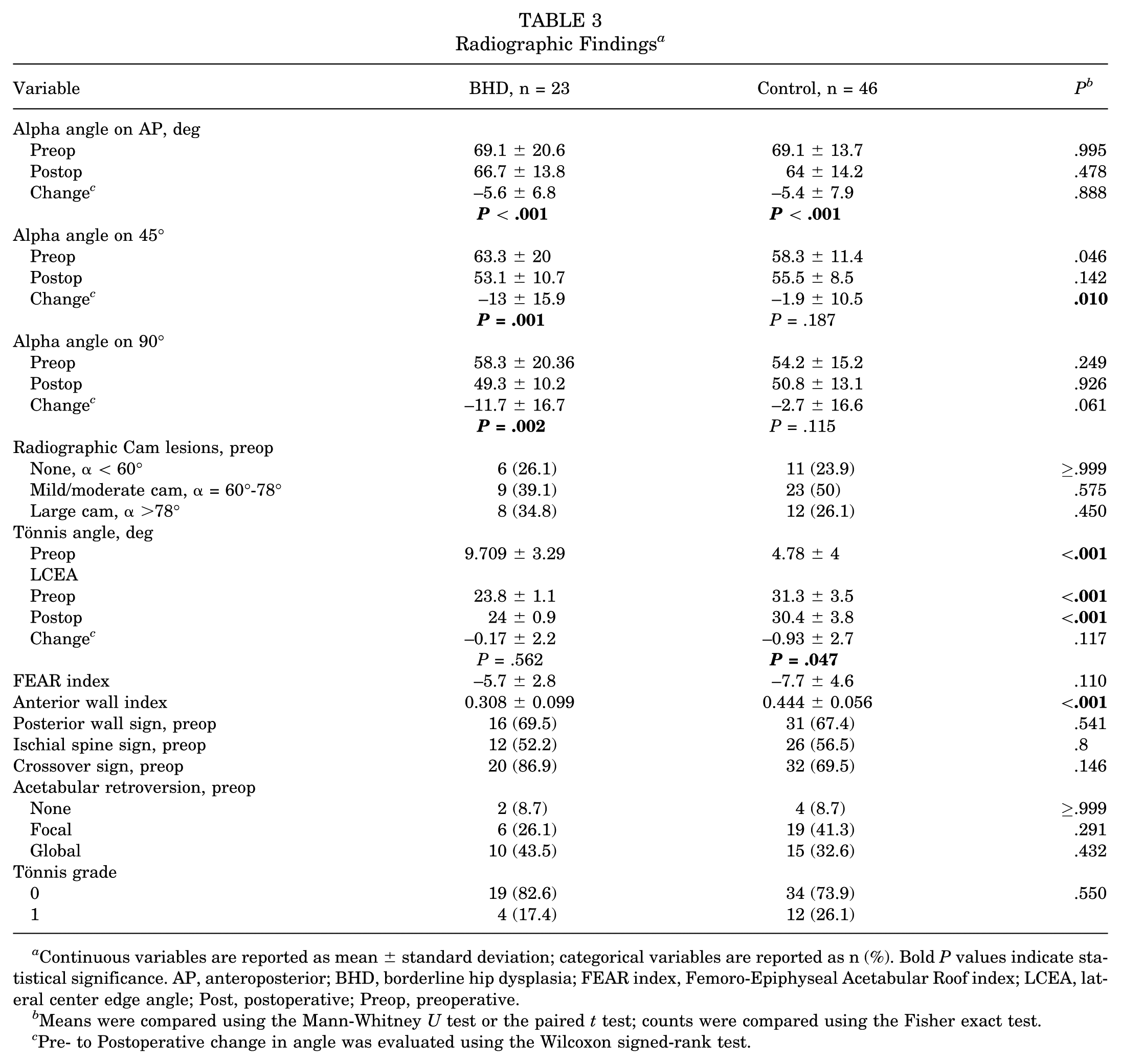
Continuous variables are reported as mean ± standard deviation; categorical variables are reported as n (%). Bold P values indicate statistical significance. AP, anteroposterior; BHD, borderline hip dysplasia; FEAR index, Femoro-Epiphyseal Acetabular Roof index; LCEA, lateral center edge angle; Post, postoperative; Preop, preoperative.
Means were compared using the Mann-Whitney U test or the paired t test; counts were compared using the Fisher exact test.
Pre- to Postoperative change in angle was evaluated using the Wilcoxon signed-rank test.
The BHD group displayed significant decreases in pre- to postoperative alpha angle on AP, 45° Dunn, and 90° Dunn views (69.1° to 66.7° [P < .001]; 63.3° to 53.1° [P = .001]; 58.3° to 49.3° [P = .002], respectively). The control group also showed significant decreases in alpha angle on AP view (69.1° to 64.0°; P < .001), but not on 45° Dunn or 90° Dunn views (both P > .05). Furthermore, the BHD group showed significantly higher decrease in alpha angle on 45° Dunn view compared with the control group (−13° vs −5.4°; P = .01). In contrast, the control group displayed significant decreases in pre- to postoperative LCEA (31.3° to 30°; P = .047), whereas the BHD group did not (23.8° to 24°; P = 562). The decrease in LCEA in the control group was also similar to that of the BHD group (P = .117).
Intraoperative Findings
Table 4 summarizes intraoperative findings for both cohorts. No significant differences were found between the BHD and control groups in Outerbridge grade of chondral wear, with the majority of patients demonstrating low-grade (grade 1) changes (90.5% vs 93%; P≥.999). Rates of cam resection (78.3% vs 82.6%; P = .75), pincer resection (95.7% vs 97.8%; P≥.999), and labral repair (100% vs 95.7%; P = .549) were similar between groups. The mean number of anchors used for labral repair did not differ significantly (1.91 ± 0.45 vs 1.73 ± 0.42; P = .116).
Intraoperative Findings a
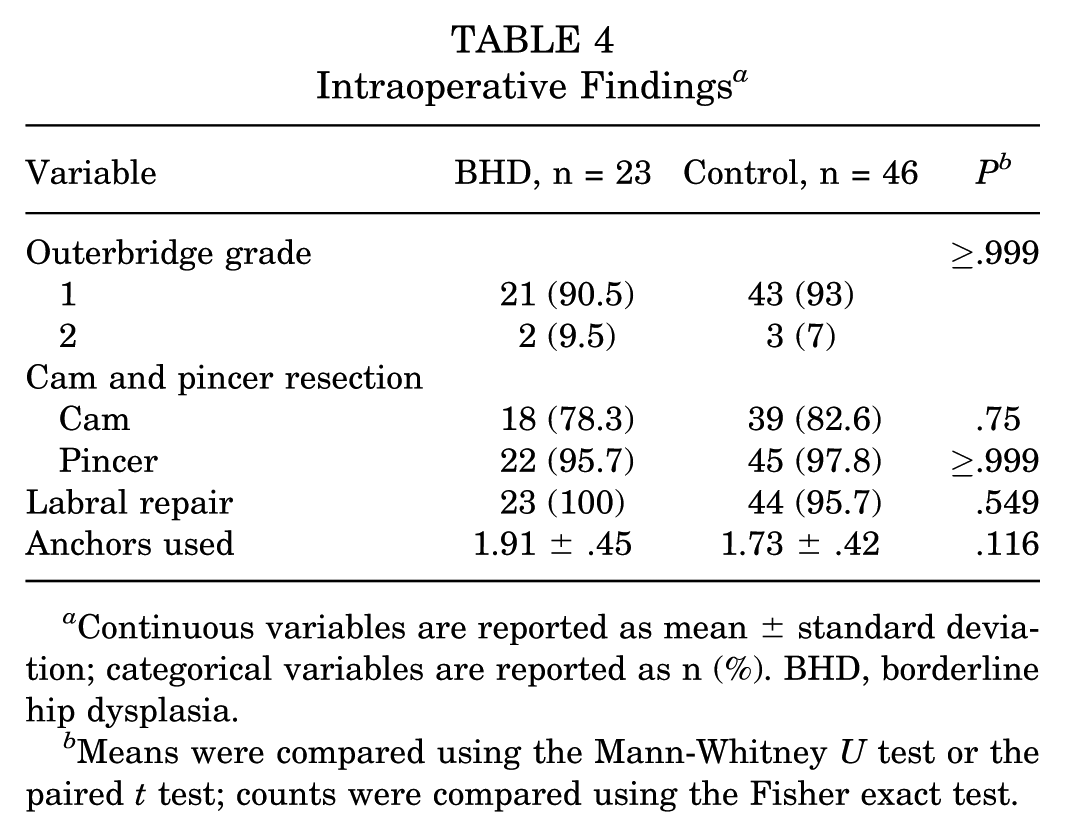
Continuous variables are reported as mean ± standard deviation; categorical variables are reported as n (%). BHD, borderline hip dysplasia.
Means were compared using the Mann-Whitney U test or the paired t test; counts were compared using the Fisher exact test.
Patient-Reported Outcomes
Table 5 contains PROs at 10-year follow-up. No significant differences in baseline or 10-year postoperative mHHS and NAHS scores were found between the BHD and control groups. Both groups showed significant improvements from the MHHS and NAHS baseline to 10 years postoperative (both P < .001). However, there were no significant differences between groups in 10-year improvement in mHHS and NAHS scores (P > .05).
PROs at 10-Year Follow-up a
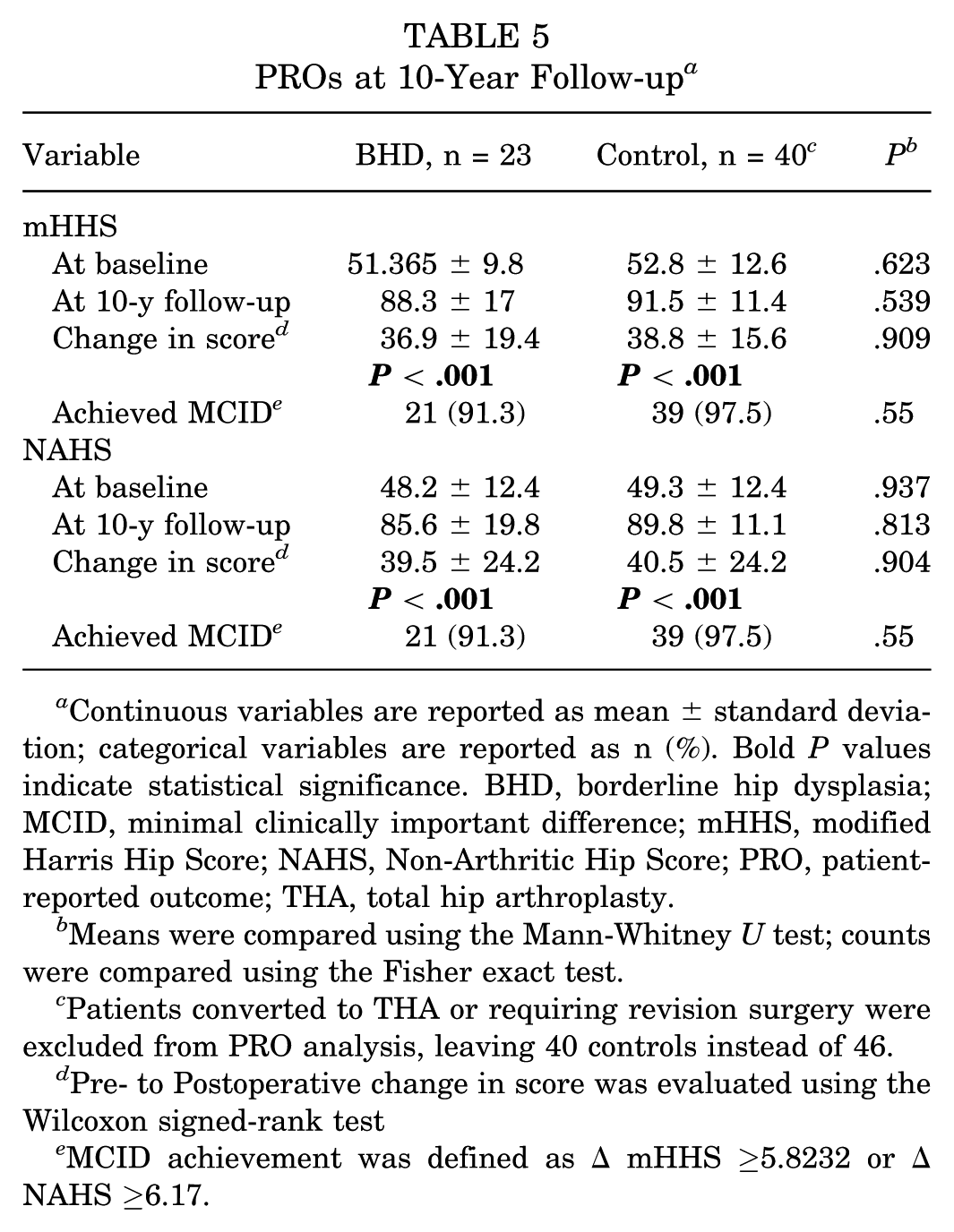
Continuous variables are reported as mean ± standard deviation; categorical variables are reported as n (%). Bold P values indicate statistical significance. BHD, borderline hip dysplasia; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; NAHS, Non-Arthritic Hip Score; PRO, patient-reported outcome; THA, total hip arthroplasty.
Means were compared using the Mann-Whitney U test; counts were compared using the Fisher exact test.
Patients converted to THA or requiring revision surgery were excluded from PRO analysis, leaving 40 controls instead of 46.
Pre- to Postoperative change in score was evaluated using the Wilcoxon signed-rank test
MCID achievement was defined as Δ mHHS ≥5.8232 or Δ NAHS ≥6.17.
The MCID thresholds were calculated as 5.82 for mHHS and 6.17 for NAHS. A total of 21 patients in the BHD group (91.3%) and 40 participants in the control group (97.5%) achieved the MCID for mHHS and NAHS. The difference in the proportion of participants achieving the MCID for mHHS and NAHS between groups was not significant (both P > .05).
Hip Survivorship
Table 6 displays hip survivorship at 10-year follow-up. No significant differences between the BHD and control groups were found in the rates of revision arthroscopy or conversion to THA (all P > .05).
Hip Survivorship at 10-Year Follow-up a
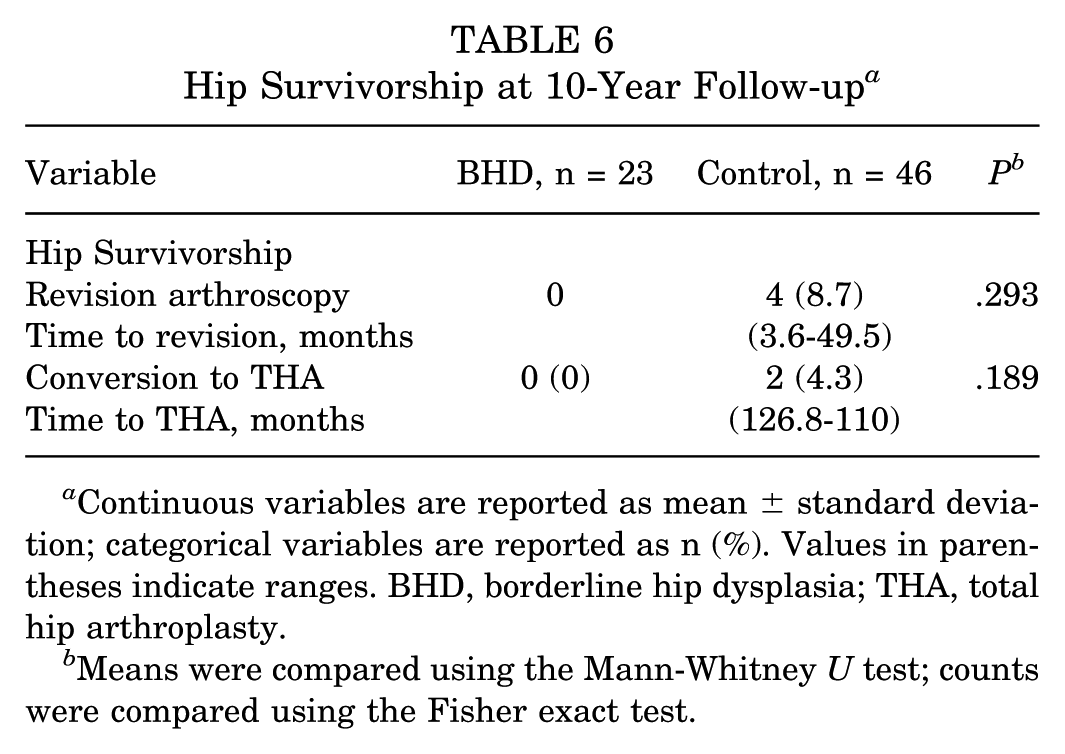
Continuous variables are reported as mean ± standard deviation; categorical variables are reported as n (%). Values in parentheses indicate ranges. BHD, borderline hip dysplasia; THA, total hip arthroplasty.
Means were compared using the Mann-Whitney U test; counts were compared using the Fisher exact test.
Discussion
The most important findings from the present study are that among patients with FAI who underwent hip arthroscopy with labral repair at a minimum 10-year follow-up, no significant differences were found between patients with and without BHD with respect to PROs, MCID achievement, rates of revision hip arthroscopy, or rates of conversion to THA. However, those with BHD demonstrated significantly greater reductions in pre- to postoperative alpha angles on both AP radiographs and 45° Dunn views compared with the control group.
PROs and MCID Achievement
The present study did not observe significant intergroup differences in 10-year improvements in the mHHS or the NAHS, nor in the MCID achievement for either measure. Results were nearly identical between groups for pre- and postoperative mHHS and NAHS. The MCID was marginally higher in the control group for both PROs; nonetheless, this did not reach significance. These results align with the authors’ previous findings at short-term follow-ups, as well as with other previous investigations. 20 In a similar 10-year analysis of BHD, Chapman et al 8 found no difference between patients with and without BHD in the setting of FAIS with regard to PROs, MCID achievement, or rates of revision hip surgery. In another 10-year analysis of 56 hips with BHD, Maldonado et al, 11 reported high rates of MCID achievement for both mHHS and NAHS, comparable to control groups. Taken together, the cadre of recent long-term outcome studies strongly suggests BHD is not a potent risk factor for poor outcomes after hip arthroscopy for labral repair. Based on current and prior work, patients with BHD can likely expect similarly strong outcomes as those without BHD at long-term follow-up.
Hip Survivorship
The present study found a surprising 0% revision arthroscopy rate and 0% conversion to THA at 10-year follow-up in the BHD group—both lower than in the control group. However, these differences did not reach significance. The literature is somewhat mixed on the reoperation rate in patients with BHD. Similar to the present study, Chapman et al 8 did not find any significant differences in the reoperation rate between those with BHD and those without at long-term follow-up. Conversely, in a study of patients with BHD (without a control), Domb et al 11 found an overall higher rate of reoperation (82.2%) at 10-year follow-up than observed here. In another single-cohort study, Beals et al 3 found that patients with BHD had a 10-year THA conversion rate of 24% and a revision hip arthroscopy rate of 7%, especially those with risk factors such as older age, higher Tönnis grades, grade 4 chondral injuries, and Tönnis angles >15°. The wide discrepancy between studies may be due to the relatively small sample sizes of existing long-term outcome investigations. However, despite the range, the overall reoperation rate is reasonably low, even at the more conservative end of the spectrum. These findings underscore the durability of hip arthroscopy outcomes in the BHD population, and it appears reasonable for patients with BHD to expect outcomes similar to those observed in patients without BHD following hip arthroscopy for FAIS.
Preoperative Cam Lesion Size and Alpha Angle Changes
This study found no significant differences in preoperative cam lesion size between the BHD and control groups, in contrast to previous findings from our group that suggested larger cam deformities in patients with BHD. 20 However, the BHD group exhibited significant reductions in pre- to postoperative alpha angles across AP, 45° Dunn, and 90° Dunn radiographic views. In comparison, the control group only demonstrated significant reductions in the AP view, with no significant changes observed in the 45° or 90° Dunn views. The limited change in alpha angle observed in the control group likely represented the underlying morphology and the senior author’s surgical philosophy. Although femoral osteochondroplasty was performed in all patients with radiographic or intraoperative evidence of cam deformity, patients in the non-BHD group more commonly presented with mild or moderate cam lesions. Cam resection was targeted to restore the head-neck offset to alleviate impingement, while avoiding excessive bone removal that could compromise femoral neck integrity. A restrained resection strategy was intentionally applied to prevent overcorrection, which can result in elevated joint loading and microinstability.5,9,12,15,22 This conservative approach likely contributed to the modest changes in the alpha angle observed. Notably, despite these more modest radiographic changes, patients in the non-BHD group demonstrated excellent long-term outcomes, with high rates of MCID achievement and low rates of revision and conversion to arthroplasty. These findings highlight the importance of tailoring surgical correction to the individual’s anatomy while maintaining joint stability and emphasize that radiographic changes alone may not fully reflect the goals or adequacy of the procedure performed.
Interestingly, Beck et al 4 reported that lower preoperative alpha angles were associated with greater odds of achieving the mHHS MCID in patients with BHD at 5 years. However, our study did not replicate these findings. Instead, we observed that high MCID achievement rates for both mHHS and NAHS were consistent across all preoperative alpha-angle measurements, suggesting that patients with BHD can achieve outcomes comparable to those without BHD. Notably, patients in our cohort had significantly higher Tönnis angles in the presence of BHD, suggesting that patients with BHD and a positive Tönnis angle can achieve favorable outcomes after hip arthroscopy. Our study, however, cannot comment on outcomes for patients with BHD who have a neutral or negative Tönnis angle, as they were not well-represented in our cohort.
Furthermore, the FEAR index trended less negatively in the BHD group compared with controls, although this difference was not statistically significant. Both groups demonstrated negative mean values, suggesting that most patients in this cohort were radiographically stable. 33 This aligns with previous literature indicating that hips with frank instability, typically characterized by a FEAR index >0°, are more often treated with periacetabular osteotomy rather than arthroscopy.32,33 In addition, the BHD group demonstrated a significantly lower AWI, indicating greater anterior undercoverage compared with controls. 28 However, the absolute AWI values were not severely low, supporting that these patients fell within the borderline dysplastic range, rather than representing frank dysplasia. 28 As such, our findings should be interpreted in the context of a borderline dysplastic population and may not be generalizable to patients with more severe dysplasia.
The management of BHD remains a crucial factor in preventing the progression to osteoarthritis and mitigating its long-term consequences. While hip arthroscopy is widely recognized as an effective intervention for FAIS, its utility in patients with BHD has been debated, given the limited long-term data. Before this study, only 3 investigations had evaluated outcomes beyond 10 years for patients with BHD undergoing hip arthroscopy.3,8,11 Findings of the present study, in conjunction with these previous studies, contribute to the growing body of evidence supporting the long-term efficacy of hip arthroscopy in patients with BHD. This study highlights comparable outcomes and survivorship rates between patients with and without BHD, further validating hip arthroscopy as a viable treatment option in this population.
Limitations
The results of this study must be understood in light of its limitations. First, the retrospective design of this study and the inclusion of 76.1% of eligible patients introduce the potential for selection bias. Of the 282 patients who underwent primary hip arthroscopy during the study period, 17 were excluded because they underwent index revision procedures, and 52 patients declined to participate in the follow-up, leaving 213 eligible patients. Among these, 162 (76.1%) completed the 10-year follow-up survey, while 51 (23.9%) were lost to follow-up. Stratifying by radiographic diagnosis, 34 patients met the criteria for BHD (LCEA, 20°-25°), of whom 23 (67.6%) completed the follow-up, 7 (20.6%) declined, and 4 (11.8%) were lost to follow-up. Among patients without BHD, 139 of 231 patients (60.2%) completed the follow-up, 45 (19.5%) declined, and 47 (20.3%) were lost to follow-up. The difference in follow-up rates between groups was not statistically significant (P = .518). Furthermore, there were no significant differences in baseline characteristics or clinical outcomes between patients with BHD included in the final analysis and those excluded. Despite this, the possibility of selection bias still remains. Second, the relatively small sample size of the BHD cohort may have resulted in insufficient power to identify significant differences in outcomes between BHD and non-BHD groups, increasing the likelihood of a type 2 error, particularly for reoperation rates. Third, radiographic analysis in this study was limited to measuring the LCEA, which restricts the ability to fully characterize the type or severity of dysplasia within the BHD cohort. We did not assess computed tomography-based parameters, such as the Ottawa classification, that could more precisely define focal dysplasia. Finally, the study did not evaluate symptoms of hip instability or ligamentous laxity at the 10-year follow-up. Although the NAHS includes a question on hip instability, responses to this item were unavailable from the single-surgeon database used for this analysis. Each of these factors must be considered when evaluating the results of this study.
Conclusion
At a minimum 10-year follow-up, patients with BHD who underwent hip arthroscopy for FAIS achieved comparable PROs and hip survivorship to those without BHD. These findings support hip arthroscopy as a durable and effective treatment for FAIS in this population.
Footnotes
Submitted February 11, 2025; accepted October 27, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: T.Y. receives intellectual property royalties, is a paid consultant, and a paid presenter or speaker for Arthrex, Inc. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.