
Abstract
Background:
Multiple grafts have been described for glenoid resurfacing in the setting of anterior shoulder instability with glenoid bone loss. The medial tibial plateau has been shown to have a similar radius of curvature to the glenoid and may be an appropriate anatomic match for glenoid resurfacing.
Purpose:
To evaluate restoration of glenoid concavity and anterior glenohumeral stability among the distal tibial allograft (DTA), distal clavicle autograft (DCA), and medial tibial plateau allograft (MTPA).
Study Design:
Controlled laboratory study.
Methods:
Nine sets of fresh-frozen unpaired shoulder, knee, and ankle cadaveric specimens were obtained (mean specimen age, 58.7 years; range, 51-63). Specimens underwent preoperative computed tomography to assess glenoid depth and radius to define the bony shoulder stability ratio (BSSR; glenoid depth over radius). A Kuka robot was used to assess shoulder stability with forces loaded through the rotator cuff and the shoulder in 90° of abduction and neutral rotation. Glenoid bone loss was created via a 10-mm cut, with each graft restoring 100% of the native glenoid width. The following conditions were tested: intact state followed by reconstructions with the DTA, MTPA, and DCA. Posttest computed tomography scans were obtained to calculate the reconstructed BSSR, and motion detectors were used to calculate maximum anterior humeral translation.
Results:
The BSSR was similar between the intact state (mean ± SD, 0.39 ± 0.11) and 3 reconstructed glenoid grafts (DCA, 0.46 ± 0.11 [P = .10]; MTPA, 0.43 ± 0.07 [P = .45]; DTA, 0.39 ± 0.11 [P = .21]). Maximum anterior translation did not differ between the 3 grafts (DCA, 6.4 ± 3.0 mm [P = .29]; MTPA, 8.4 ± 5.3 mm [P = .11]; DTA, 6.7 ± 3.6 mm [P = .21]) and the intact state (6.0 ± 2.8).
Conclusion:
By way of a cadaveric analysis, the DCA, MTPA, and DTA restored glenoid concavity to a point similar to the intact state. Future investigations with larger sample sizes are warranted to confirm these biomechanical trends and determine clinical significance.
Clinical Relevance:
Restoration of glenoid concavity is essential for achieving stability in patients with anterior shoulder instability and critical glenoid bone loss. This biomechanical study demonstrates that distal clavicle autograft, distal tibia allograft, and medial tibial plateau allograft each restore native glenoid concavity comparable to the intact state, supporting their use as reliable free bone block options for anatomic glenoid reconstruction. Future clinical studies are warranted to determine whether these biomechanical findings translate to improved clinical outcomes.
Keywords
Glenoid bone loss (GBL) is present in >80% of patients with recurrent anterior shoulder instability and can be a difficult clinical problem to treat. 3 Biomechanical studies have suggested that soft tissue repair alone in the setting of >15% bone loss can lead to suboptimal anterior shoulder stability and can restrict glenohumeral rotational motion. 22 Furthermore, clinical studies suggest that even 13.5% GBL may affect outcomes for soft tissue–only stabilization procedures. 21 This understanding of the biomechanical problem has stimulated interest in bone block procedures to treat patients with anterior shoulder instability with associated GBL. Traditionally, the Latarjet has been the gold standard for bone block procedures worldwide. However, despite the overall clinical success of the Latarjet procedure, the complication rates remain high, in the range of 15% to 30%, and recent concerns have been raised about the limitations of the procedure regarding its ability to reliably restore glenoid width and concavity in larger defects.2,7 Free bone blocks lend themselves to a greater ability for the surgeon to customize graft size to match patient anatomy, rather than be constrained by the size of the coracoid. Additionally, free bone blocks may allow for a less demanding arthroscopic approach than Latarjet. As a result, bone block procedures such as the distal clavicle autograft (DCA) and distal tibial allograft (DTA) have been proposed and performed as alternatives to the traditional Latarjet.13,24 More recently, the medial tibial plateau allograft (MTPA) has been proposed as a suitable anatomic match to the glenoid articular surface in topographic 8 and computed tomography (CT) joint contact pressure analyses. 14 Despite the recent interest in these newer bone block procedures, there has been little investigation into their ability to restore glenoid concavity and reduce anterior humeral translation.
The current study sought to evaluate glenoid concavity restoration and anterior humeral stability among the DTA, DCA, and MTPA in a reproducible and validated GBL model. We hypothesized that all 3 bone block procedures would restore glenoid concavity and anterior glenohumeral translation back to the native state.
Methods
Specimen Preparation
This investigation used 9 fresh-frozen unpaired human cadaveric forequarter specimens (mean specimen age, 58.7 years; range, 51-63). Each specimen underwent preoperative CT scanning to confirm the absence of glenohumeral osteoarthritis, glenoid fractures, or any other bony irregularities. Each specimen was thawed at ambient temperature the night before dissection. Skin and soft tissues were removed while preserving essential anatomic structures: the musculotendinous units of the supraspinatus, infraspinatus, subscapularis, and teres minor; the pectoralis major and conjoint tendons; and the ligaments and capsule of the glenohumeral joint. A No. 0 Vicryl suture (Ethicon) was utilized to perform a locking running stitch across the subscapularis, supraspinatus, infraspinatus, pectoralis major, and conjoint tendons to facilitate load application along physiologic lines of force. A supracondylar humeral osteotomy was performed approximately 15 cm above the elbow, and the distal humerus was potted into a 12.7 × 3.8–cm aluminum cylinder with polymethylmethacrylate cement to secure it for testing. The medial 5 cm of the scapula was denuded of soft tissues to optimize its fixation to the mounting plate. A previously validated shoulder table 5 was utilized, allowing 6° of motion on the glenohumeral joint. The scapula was positioned in 0° of anterior tilt and 30° of upward rotation and the humerus in 60° of glenohumeral abduction simulating 90° of humerothoracic elevation.20,23,27
Measurement of Glenohumeral Translation
Clusters of reflective markers were attached to the scapula and humerus via bone pins to monitor 3-dimensional positions of the segments with a high-resolution motion capture system (0.2 mm, Cortex; Motion Analysis Corp). A coordinate system was established with markers, which were localized on posttest CT scans to allow for precise calculations of the various movements of the humeral head related to the center of the glenoid.
Loading Conditions
The shoulder simulator applied forces to the rotator cuff muscles, simulating physiologic conditions consistent with studies that have evaluated anterior shoulder stability after a Latarjet procedure. 17 This included 8.8 N applied across the supraspinatus, 13.2 N across the infraspinatus, 4.4 N across the teres minor, and 17.6 N across 3 evenly spaced sutures in the subscapularis. The intention of this loading configuration was to create a balanced force couple across the glenohumeral joint. The pectoralis major tendon was utilized to apply an anterior translation force in the anteroinferior vector parallel to the glenoid face. This force was normalized according to specimen-specific tissue laxity of the intact state. A robotic arm (Kuka KRC4 series; simVITRO) was used to translate the humeral head through the action of the pectoralis major tendon at a velocity of 1 mm/s. For the native shoulder and before any GBL or reconstruction, the humeral head was moved until its center reached beyond the anterior glenoid margin. The force required to perform this maneuver was recorded and used as the “specimen’s maximum anterior force” for the remaining testing conditions/glenoid reconstructions for that specimen.
Surgical Procedure and Biomechanical Testing Sequence
For all testing conditions, the humerus was placed in neutral rotation with the scapula positioned at 30° of upward rotation, glenohumeral joint abduction at 60°, and neutral rotation. This allowed a combined 90° of humerothoracic abduction in the scapular plane. The intact condition was tested first and followed by a lesser tuberosity osteotomy with a sagittal saw to access the glenohumeral joint. An inferior capsulotomy was then created off the humerus, and the rotator interval was opened to allow for better glenoid visualization. Kirschner wires and a reduction clamp were used to secure the lesser tuberosity osteotomy, and after each procedure the inferior capsule and rotator interval were repaired with No. 0 Vicryl sutures.
First, a Bankart tear was created with a fresh No. 10 scalpel to create an interval at the anteroinferior chondrolabral junction. This extended from anterior to the biceps anchor to the 6-o’clock position inferiorly on the glenoid. In preparation for creation of the bony defect, the vertical axis of the glenoid was identified and drawn from the biceps anchor to the triceps tendon insertion. A line representing the transverse axis was drawn perpendicular to the vertical axis through the bare area of the glenoid, typically at the junction of the upper two-thirds and lower one-third of the glenoid. The level of bony resection was measured at 10 mm from the anterior glenoid rim along the transverse axis with a caliper (Figure 1). The osteotomy was created by a sagittal saw and made parallel to the vertical axis preserving anterior capsulolabral tissues.
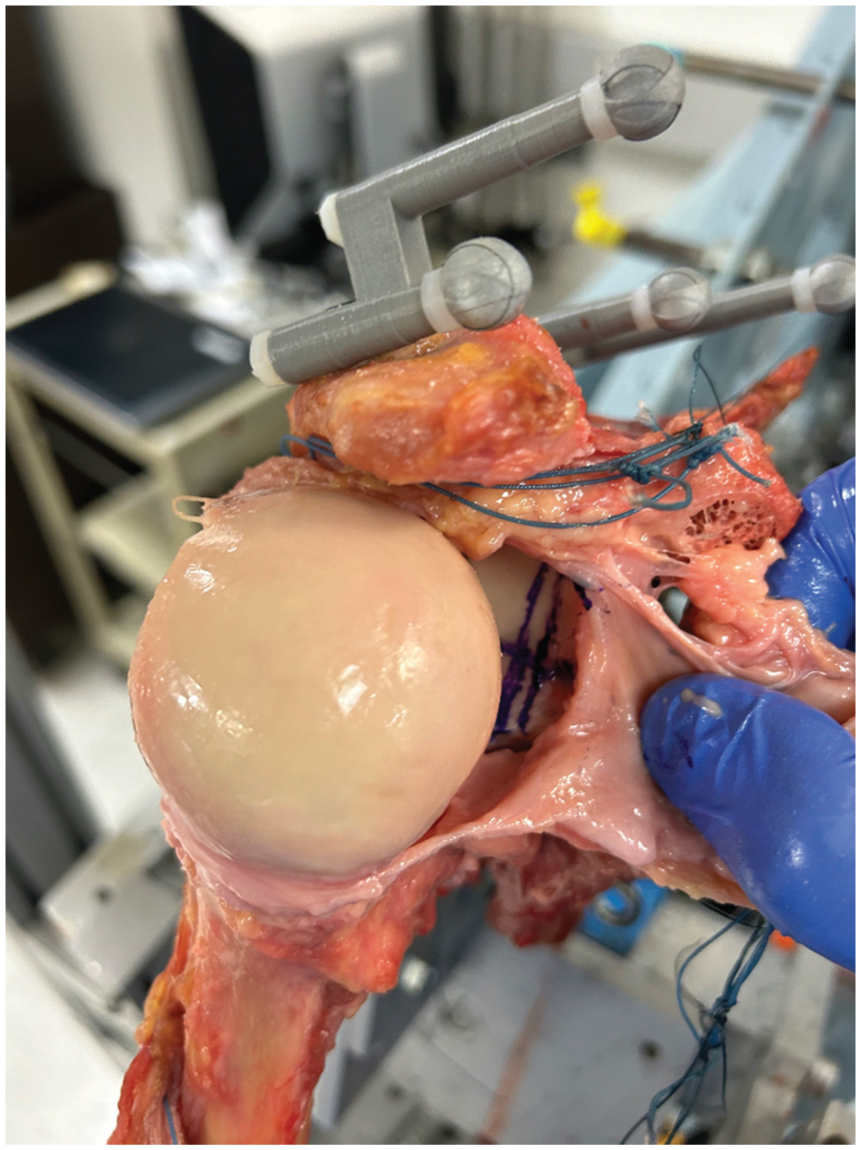
A lesser tuberosity osteotomy and capsular release allowed for increased glenoid exposure. The vertical axis of the glenoid was marked by a longitudinal line extending from the biceps anchor to the triceps insertion. A transverse line was then created perpendicular to the vertical axis at the inferior one-third of the glenoid and traversing through the bare area. The vertical osteotomy was planned by measuring the distance from the anterior glenoid rim along the transverse axis.
Bone Defect Sizing
For each specimen, GBL was standardized via a 10-mm defect, which was created with a sagittal saw. Based on previous biomechanics literature, 17 the goal of each procedure in the present study was to reconstruct 100% of the native glenoid width with the MTPA, DTA, and DCA. Therefore, each graft was measured 10 mm in the anterior-posterior dimension. The cranial-caudal graft dimensions for the MTPA and DTA were adjusted to match the specimen-specific anatomy of the harvested DCA.
DCA Preparation
A 10-mm DCA was measured and harvested from the same specimen with a sagittal saw. The cranial-caudal dimension of the graft, when flipped to the appropriate orientation for graft fixation, was measured and recorded. The DCA was then placed at the inferior aspect of the glenoid defect oriented such that the undersurface (concave side) of the graft was rotated flush with the glenoid chondral surface. The graft was then secured with two 3.5-mm screws. Care was taken to orient that graft so that it was congruent to the chondral surface of the glenoid while avoiding lateral overhang (Figure 2).
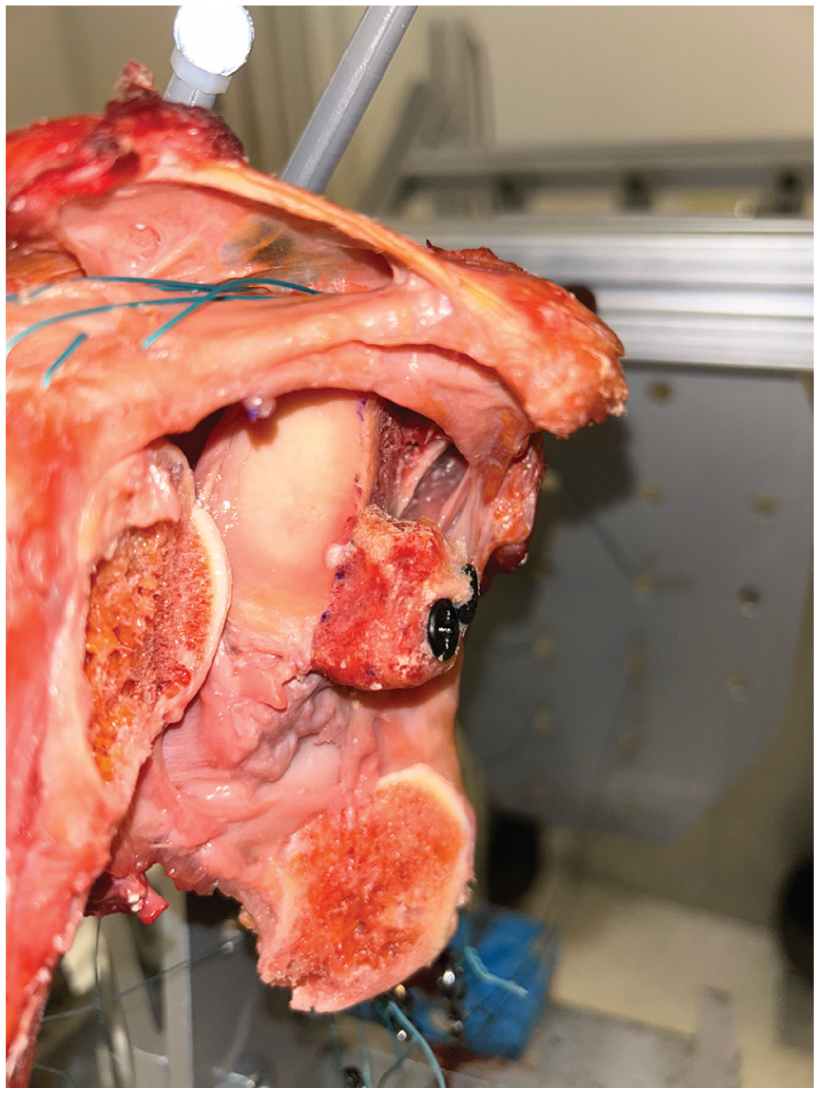
The distal clavicle autograft was positioned at the inferior aspect of the glenoid margin and oriented congruent with the native glenoid surface with the cut surface positioned flush to the anterior surface of the glenoid and the superior surface of the clavicle aligned with the glenoid articular surface.
DTA Preparation
A DTA was created as described by Provencher et al. 16 Nine cadaveric ankle specimens were obtained to create a DTA for each shoulder specimen. Using a caliper, the width of the DTA, as measured on the articular surface, was measured 10 mm. The cranial-caudal height of the DTA was then reduced to equal the height of the DCA. The DTA was then placed at the inferior aspect of the glenoid defect and secured with two 3.5-mm screws. Care was taken to orient that graft so that it was congruent to the chondral surface of the glenoid while avoiding lateral overhang (Figure 3).
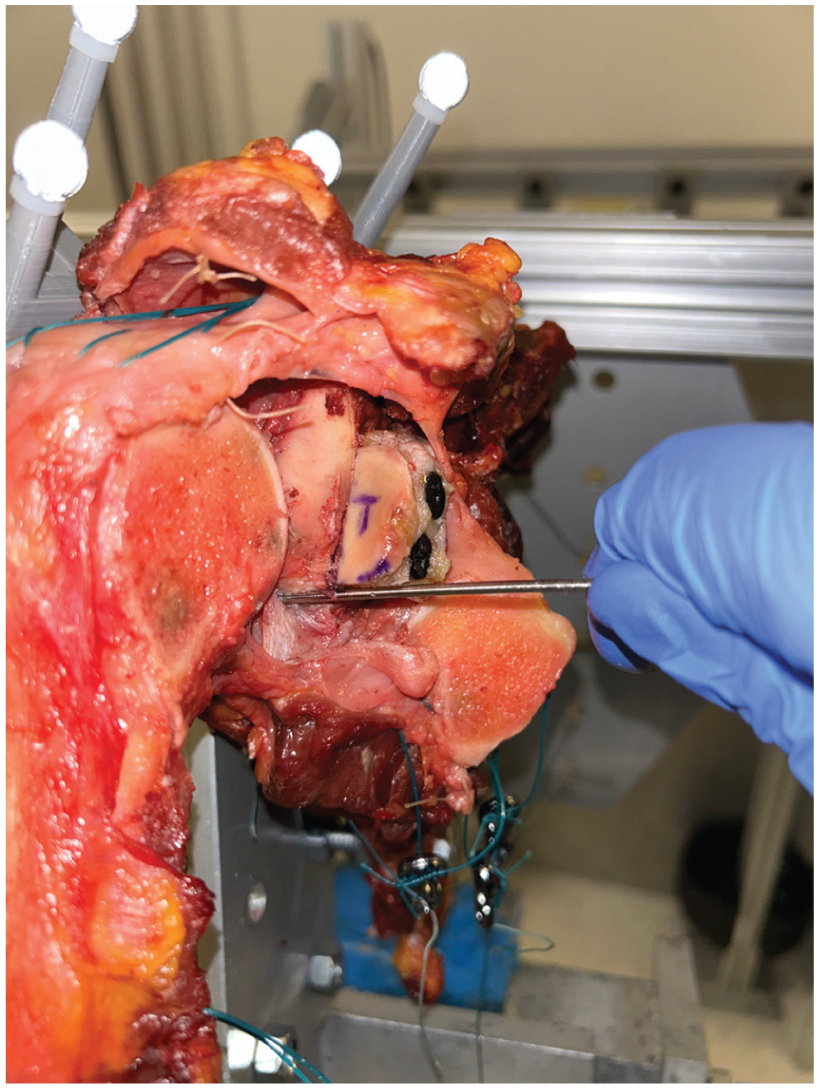
The distal tibial allograft was positioned at the inferior aspect of the glenoid margin and oriented congruent with the native glenoid surface.
MTPA Preparation
The MTPA was created in a similar fashion to the DTA. Nine cadaveric tibial plateau specimens were obtained to create a new MTPA for each shoulder specimen. Using a caliper, the width of the allograft, as measured on the articular surface, was 10 mm. The cranial-caudal height of the MTPA was then reduced to equal the length of the DCA. The MTPA was placed at the inferior aspect of the glenoid defect and secured with two 3.5-mm screws. Care was taken to orient that graft so that it was congruent to the chondral surface of the glenoid while avoiding lateral overhang (Figure 4).
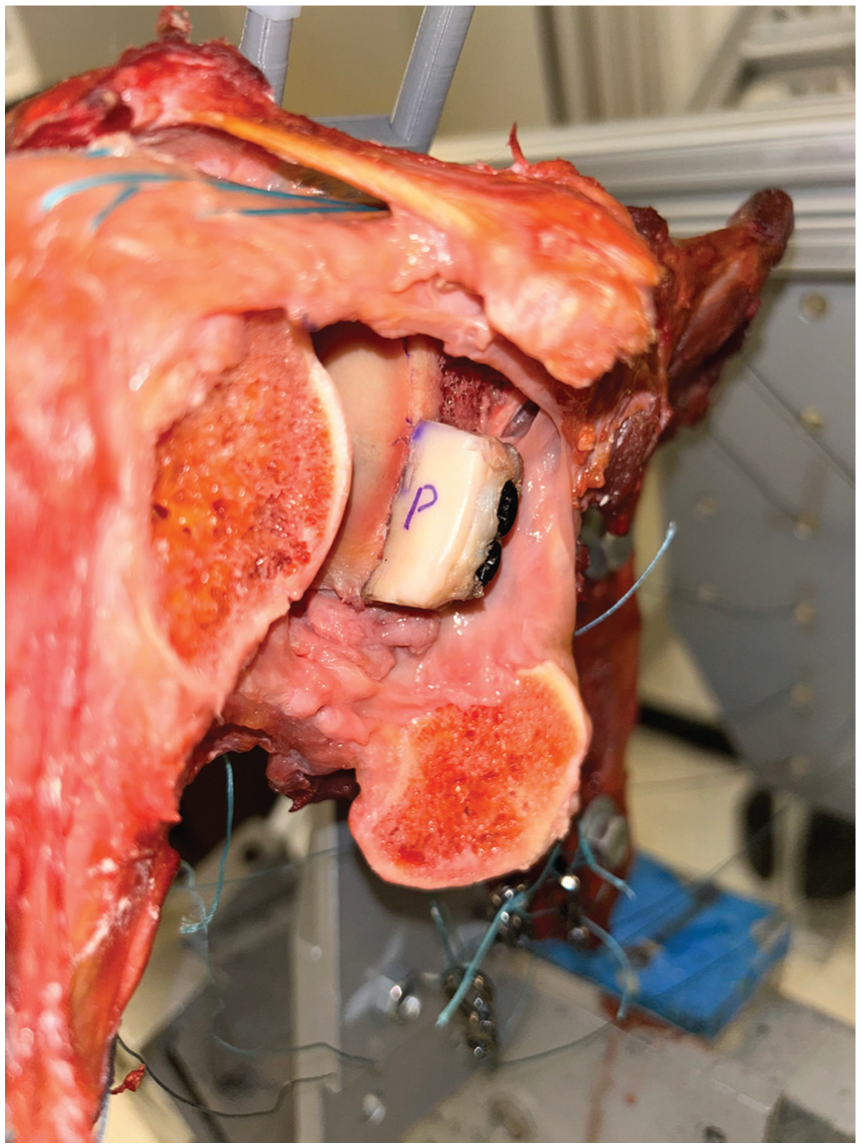
The medial tibial plateau allograft was positioned at the inferior aspect of the glenoid margin and oriented congruent with the native glenoid surface.
Testing Conditions
The sequence of testing proceeded as follows: intact state → Bankart lesion. The following experimental states were tested in random order, each without capsular repair: DCA, DTA, MTPA. The order of graft testing was randomized across cadavers to minimize potential confounding effects related to soft tissue stretch during biomechanical evaluation. Each condition was tested twice.
Radiographic Assessment for Glenoid Concavity Restoration
Native glenoid and postreconstruction concavity were determined by pre- and posttesting CT scans. Posttesting CT scans were obtained after completion of all experimental states, rather than between testing conditions. The bony shoulder stability ratio (BSSR) was used to measure glenoid concavity, where r is the radius of curvature per a best-fit circle on the glenoid face and d is the depth of the glenoid measured by the perpendicular distance from a line connecting the anterior and posterior rim of the glenoid to the deepest part of the glenoid (Figure 5). 25
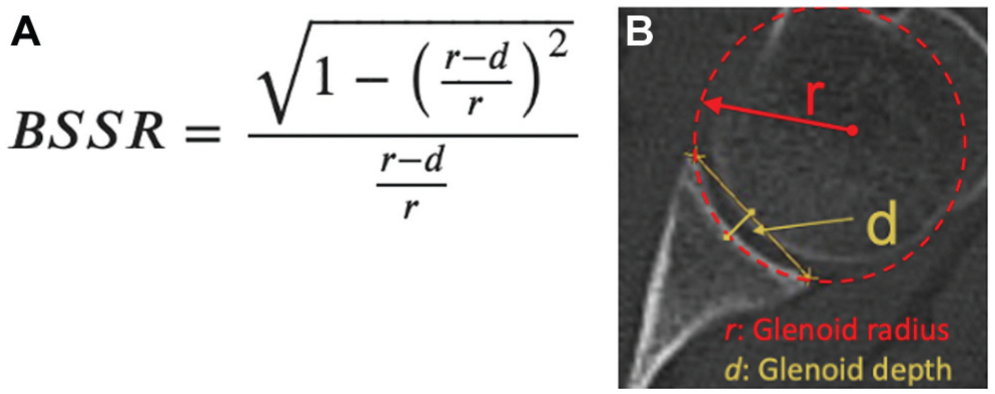
(A) The formula used to calculate the bony shoulder stability ratio (BSSR). (B) Measurement of the glenoid depth, d, and the placement of a best-fit circle to obtain the radius of curvature, r, used in the calculation.
Statistical Analysis
As no prior biomechanical data exist for the DCA or MTPA, the study's sample size was determined by the findings of Fury et al, 5 which compared DTA, classic Latarjet, and intact glenoids based on a similar robotic testing model. Assuming a similar BSSR difference of 1.1 between the grafts for this study and using a desired power of 0.90 and alpha of .05, the a priori power analysis indicated that 8 specimens (n = 7.8) would be sufficient to detect a significant difference in the BSSR. To ensure adequate power and account for potential variability, 9 specimens were ultimately tested for each graft and testing condition. A repeated measures analysis of variance test was also performed to determine if there was a difference in maximum anterior translation or BSSR among the 3 bone blocks. Statistical significance was determined by a P value <.05.
Results
Glenoid Concavity Restoration
The mean ± SD preoperative glenoid depth measured 2.2 ± 0.6 mm with a BSSR of 0.37 ± 0.1 mm. None of the BSSRs for the 3 reconstructed states were significantly different from the intact state: DCA produced a mean BSSR of 0.38 ± 0.09 (P = .2); MTPA, a mean BSSR of 0.35 ± 0.10 (P = .137); and DTA, a mean BSSR of 0.37 ± 0.11 (P = .416) (Figure 6). While there were subtle differences in mean BSSR between the DCA and MTPA as compared with the intact state, none of these pairwise comparisons met statistical significance (P = .220 for intact vs DCA; P = .137 for intact vs MTPA; P = .416 for intact vs DTA).
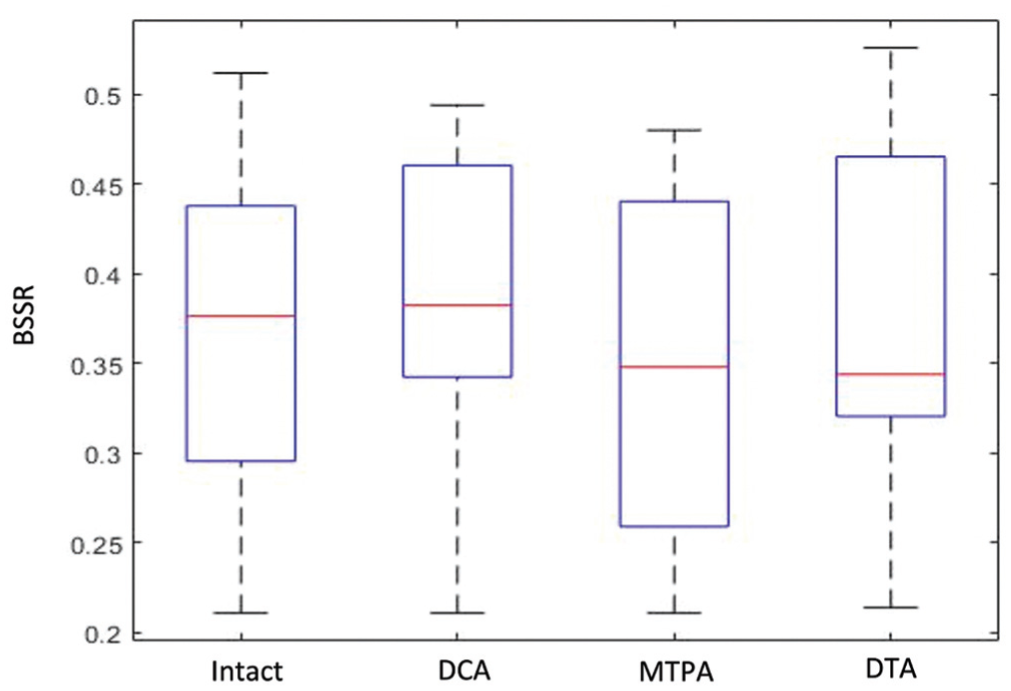
A plot of the bony shoulder stability ratio (BSSR) for all 4 conditions. Line, mean BSSR; box, range; error bars, +/−standard deviation. DCA, distal clavicle autograft; DTA, distal tibial allograft; MTPA, medial tibial plateau allograft.
Anterior Translation
There were no significant differences in the maximum anterior translation (in millimeters) after the 3 reconstructed states as compared with the intact state. The maximum anterior translation was 8.2 ± 3.1 mm for the intact state, 9.0 ± 3.6 mm for the DCA (P = .264), 10.6 ± 4.8 mm for the MTPA (P = .103), and 8.9 ± 2.4 mm for the DTA (P = .272) (Figures 7 and 8).
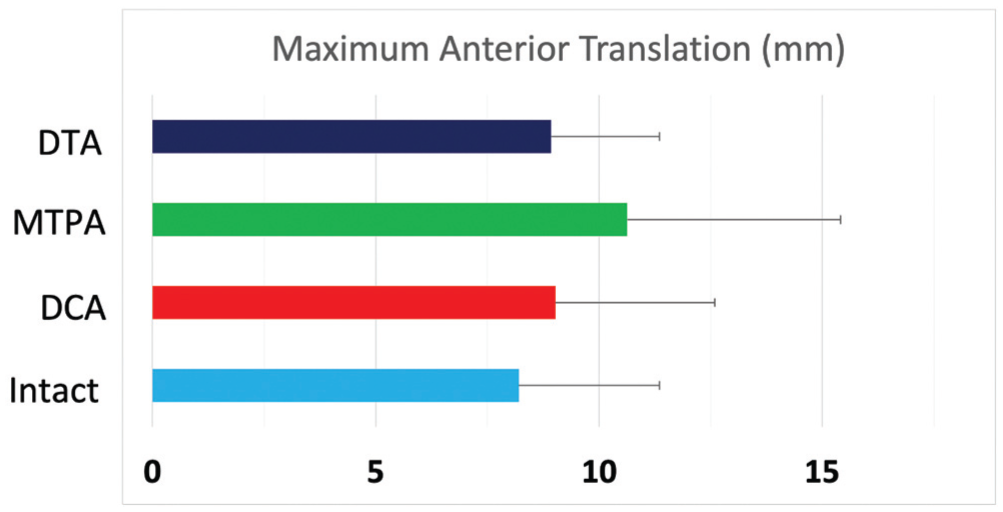
Maximum glenohumeral anterior translation of the distal clavicle autograft (DCA), distal tibial allograft (DTA), medial tibial plateau allograft (MTPA), and intact conditions. Data are presented as mean (SD).
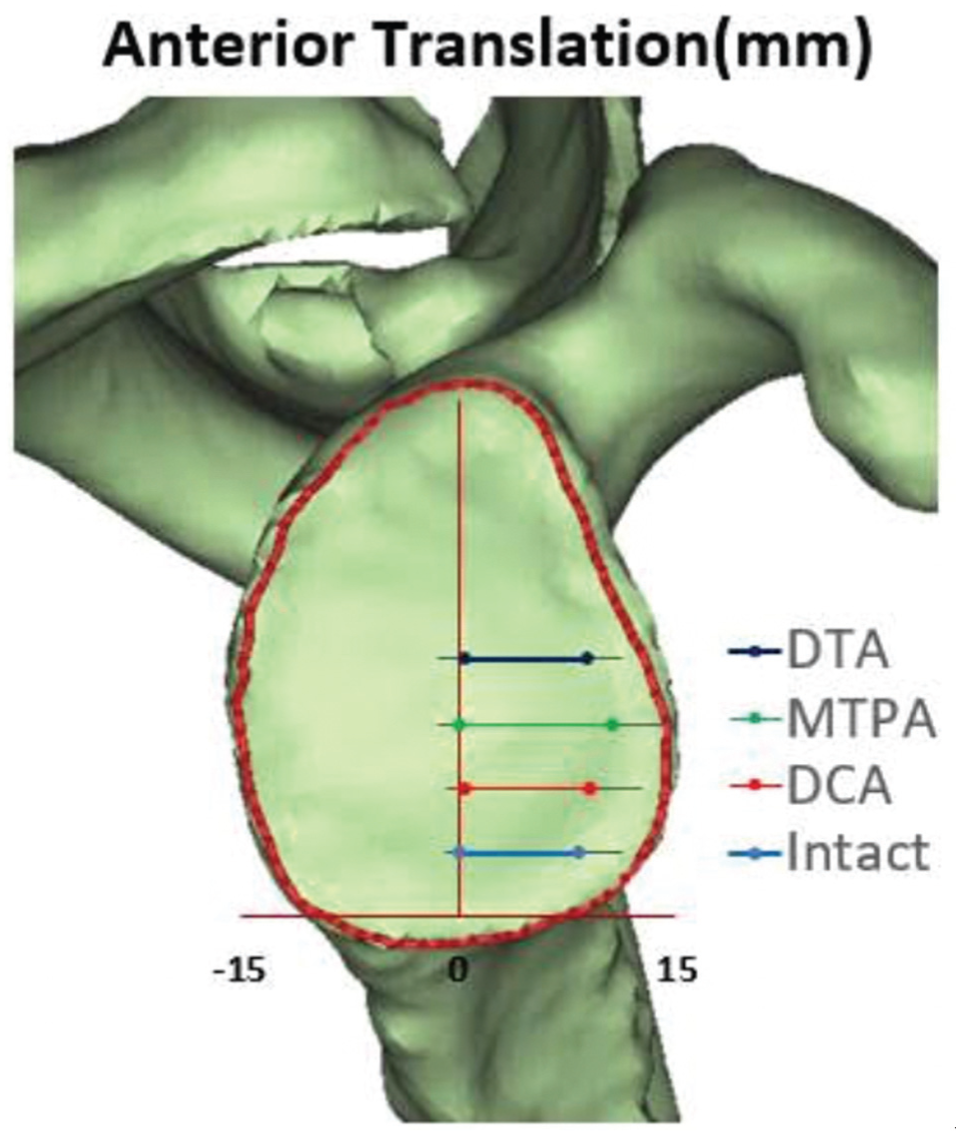
Glenoid representation of the resting position and maximum anterior humeral translation of the distal tibial allograft (DTA), medial tibial plateau allograft (MTPA), distal clavicle autograft (DCA), and intact conditions.
Discussion
The primary findings of the present study are that all 3 bone blocks (DCA, DTA, MTPA) restored glenoid concavity and anterior humeral translation that were not statistically different from the native condition. Thus, this cadaveric study demonstrates that DCA, DTA, and MTPA are all viable graft options from a biomechanical standpoint in the setting of significant GBL in anterior shoulder instability.
While the Latarjet has long been considered the gold standard bone block procedure for anterior GBL in shoulder instability, the advent of alternative bone block procedures has expanded the armamentarium for treating complex shoulder instability. In fact, a recent biomechanics study noted suboptimal coracoid graft-loading conditions and increased anterior humeral translation when 100% of the native glenoid width could not be restored by coracoid graft alone. 17 With this considered, understanding alternative bone block options is paramount. Furthermore, a recent systematic review found that the oft-touted “sling effect” of the Latarjet procedure, where the conjoint tendon passes through a split in the subscapularis, was not clinically relevant in cases where the glenoid width could adequately be restored. 9 Additionally, a recent biomechanics study demonstrated that DTA reconstruction produced greater glenoid concavity restoration as compared with the Latarjet procedure. 5 Thus, it stood to reason that a comparison among several of the common free bone block procedures was warranted. While the present study does not compare each bone block against the Latarjet procedure, it does demonstrate that the DCA, DTA, and MTPA adequately restore glenoid concavity and anterior humeral translation back to their native state.
In their study, Wermers et al 26 demonstrated that increased glenoid concavity provides inherently greater stability to the glenohumeral joint. Their introduction of the BSSR emphasizes that anterior GBL differentially affects shoulder stability depending on the native concavity of the glenoid. For instance, “20% bone loss” will have a greater effect on stability in a shoulder with a more concave glenoid versus one with less concavity. DTA was introduced as one of the first osteochondral allografts for its promise in addressing GBL and providing restoration of a chondral surface. The ability of DTA to restore glenoid concavity, however, has not been directly studied until recently—where Fury and Taylor 5 demonstrated that the DTA produced a significantly greater BSSR and decreased maximum anterior humeral translation as compared with the classic Latarjet procedure when the “sling effect” is removed. Similarly, in the present study, the DTA procedure restored glenoid concavity and decreased anterior humeral translation back to the native state.
In a recent 3-dimensional imaging study, Kim et al 10 noted that the DCA for anterior GBL provides “versatile utility” with respect to its dimensions and options for orientation when placed surgically. In a cadaveric study of the distal clavicle, the authors found that the most advantageous position when utilizing the articular cartilage of the DCA includes placing the inferior surface of the clavicle flush to the glenoid's anterior surface, with the cartilage of the graft parallel to the glenoid's articular surface. 12 This positioning was found to reconstruct roughly 22% of the glenoid articular surface. 12 However, a separate cadaveric study noted that 98.1% of distal clavicle grafts could restore up to 30% of GBL with the same DCA orientation. 19 Yet, Kwapisz et al 11 found that the DCA could restore 44% of the glenoid width on average when utilized in the same fashion as previously described. Finally, one further cadaveric study noted similar articular contact pressures when comparing the DCA with the traditional Latarjet. 15 In contrast, the present study did not utilize the articular surface of the DCA and instead aimed for an ideal restoration of glenoid concavity. The ideal orientation was deemed to involve the undersurface of the clavicle aligned parallel to the glenoid cartilage with the cut surface of the DCA flush to the anterior glenoid vault. Furthermore, Larouche and colleagues 12 highlighted that the DCA had significantly lower bone density than the measured coracoid grafts in their study, thus raising concerns for bone quality and quality of graft fixation. Additionally, while a number of techniques utilizing the DCA have been described, there is a paucity of reported clinical results. To add to the growing body of literature, the present study demonstrates that the DCA can effectively restore glenoid concavity and glenohumeral stability back to the native state when utilized with the superior clavicular surface parallel to the glenoid cartilage.
The medial tibial plateau was first identified by Gupta and colleagues 8 to be an appropriate anatomic match for the glenoid articular surface when they performed a topographic CT analysis. Additionally, Rios et al 18 compared the radius of curvature and dimensional surface areas between the glenoid and MTPA and found no statistical difference between them. Millet and colleagues, 14 however, demonstrated in a cadaveric model that MTPAs resulted in increased peak contact pressures when used to restore GBL. The clinical implications of this are unclear, and unfortunately there is a scarcity of studies that have reported clinical outcomes of MTPA in the setting of anterior GBL. Despite this, the findings of the present study provide evidence that the MTPA can sufficiently restore glenoid concavity back to the native state and reduce anterior humeral translation. Future longitudinal studies should be pursued to evaluate the clinical efficacy and safety of this procedure.
Limitations
This study is not without limitations. First, while the controlled laboratory setting attempts to re-create clinical conditions, there is hardly ever perfect replication of clinical conditions and the present study is no exception. Additionally, the specimens in this study were older than the typical population affected by anterior glenohumeral instability. As a result, there may be inherent tissue differences that skew the results of this study. To perform the procedures in this study, we utilized a lesser tuberosity osteotomy to obtain access to the glenohumeral joint; however, prior studies have demonstrated no differences in anterior humeral translation, kinematics, range of motion, or stiffness when comparing a repaired lesser tuberosity osteotomy with the native intact state.1,4,6,17 Furthermore, after each procedure and testing condition, the inferior capsule and rotator interval were repaired with No. 0 Vicryl suture. Given that this repair introduces a degree of variability across testing conditions, we implemented a randomized testing sequence to mitigate the impact of this internal variability.
Inherent to controlled laboratory studies such as this one, the findings represent time-zero biomechanics, and the implications of postsurgical adaptations in a living patient are unknown. Furthermore, while the current study provides comparative biomechanical data across several bone block options, it is important to acknowledge limitations related to sample size. Further, the findings represent time-zero biomechanics, and the implications for clinical outcomes remain unknown. The sample size was determined a priori per the biomechanical data of Fury et al, 5 which demonstrated that 9 specimens would provide sufficient power to detect meaningful differences in glenoid concavity restoration among bone block reconstructions. However, the study was not adequately powered to detect small differences in anterior translation between the MTPA and the remaining grafts or the intact glenoid. The observed mean differences in anterior translation among the grafts were minimal and not felt to be clinically significant. However, future studies with larger sample sizes are warranted to specifically investigate the biomechanical influence of the MTPA on glenohumeral anterior translation. Additionally, we did not evaluate the CT scans for radiographic evidence of arthritis. Yet, all specimens were grossly inspected for any major deformity or irregularity, and the osseous structures and articular cartilage surfaces were qualitatively assessed for gross pathology. No specimens were excluded on this basis. Furthermore, the focus of our investigation was on the osseous anatomy and morphologic characteristics relevant to free bone block graft options. It is possible that concomitant soft tissue pathology could affect outcomes and be a worthwhile area for future investigation. Last, the present study does not account for the effect of humeral-sided defects; thus, further studies are needed to determine the applicability of these findings in patients with bipolar bone loss.
Conclusion
This cadaveric study showed that DCA, MTPA, and DTA effectively restored glenoid concavity to levels comparable to the intact shoulder. Future investigations with larger sample sizes are warranted to confirm these biomechanical trends and determine clinical significance.
Footnotes
Submitted October 19, 2025; accepted December 21, 2025.
One or more of the authors has declared the following potential conflict of interest or source of funding: L.V.G. has received consulting fees from Biomet, DePuy Synthes Products, Medical Device Business Services, and Responsive Arthroscopy; intellectual property royalties from Exactech and Zimmer Biomet Holdings; speaking fees from Exactech and Smith & Nephew; research support from Biomet; and support for education from Gotham Surgical Solutions & Devices. L.V.G. also holds stock or stock options in Imagen Inc and Responsive Arthroscopy. D.M.D. has received consulting fees from Zimmer, publishing royalties from Thieme, support for education from Gotham Surgical Solutions, and other financial or material support from Biomet. J.S.D. has received consulting fees and research support from Arthrex, intellectual property royalties from Arthrex and Linvatec, support for education from Gotham Surgical Solutions, and publishing royalties from Thieme and Wolters Kluwer Health–Lippincott Williams & Wilkins and holds stock or stock options in ViewFI. M.C.F. is a paid consultant for Stryker. T.A.B. has received consulting fees from Catalyst Orthoscience, LIMA, Stryker, and Zimmer and support for education from Arthrex and holds stock or stock options in Catalyst Orthoscience. S.A.T. has received consulting fees from Mediflix, Encore Medical, and Smith & Nephew and honoraria from Enovis and has ownership interest in HS2, HSS ASC Development Network, and NEST Innovations. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.