
Abstract
Background:
Smoking increases retear rates after rotator cuff repair. However, the cessation duration required to achieve outcomes comparable to those of nonsmokers remains unclear.
Purpose:
To determine the cessation duration required for former smokers to achieve retear rates comparable to those of nonsmokers after arthroscopic rotator cuff repair.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
The study included 1902 patients who underwent arthroscopic rotator cuff repair for full-thickness tears between March 2012 and October 2023. Patients were categorized as nonsmokers (1172 patients); former smokers stratified by cessation duration of <1 year, 1 to <3 years, 3 to <5 years, and ≥5 years (454 patients); or current smokers (276 patients). After 1:1:1 propensity score matching based on age, employment status, tear size, and fatty infiltration, the records of 276 patients per group were analyzed. The visual analog scale, Subjective Shoulder Value, American Shoulder and Elbow Surgeons score, University of California at Los Angeles score, and range of motion were used to compare functional outcomes. Six-month postoperative magnetic resonance imaging assessed structural integrity using the Sugaya classification.
Results:
At the 2-year (range, 23-27 months; mean, 24.5 ± 1.0 months) follow-up evaluation, clinical scores and range of motion had significantly improved (P < .001 for all) in all groups without significant intergroup differences. However, retear rates differed significantly: 17.8% in nonsmokers, 25.4% in former smokers, and 29.3% in current smokers (P = .005). Former smokers demonstrated progressively decreasing retear rates with longer cessation: 28.6% at <1 year, 27.0% at 1 to <3 years, 20.1% at 3 to <5 years, and 19.4% at ≥5 years. Patients with ≥3 years’ cessation achieved rates comparable to those of nonsmokers. Multivariable analysis identified smoking status, pack-years (cutoff, 14), and cessation duration (cutoff, 44 months) as independent predictors. The combined cessation duration/pack-year model demonstrated superior predictive performance (AUC, 0.716).
Conclusion:
Sustained smoking cessation significantly lowers retear rates after rotator cuff repair, with at least 3 years of abstinence required to achieve rates comparable to those of nonsmokers. Pack-years and duration of cessation serve as independent predictors of tendon healing.
Among various patient-related comorbidities, smoking has emerged as one of the most detrimental factors affecting tendon healing and clinical outcomes after rotator cuff repair.4,10,14,28,29,36,44 Nicotine and other toxic components in tobacco compromise the biological environment for healing by impairing microvascular perfusion, inhibiting fibroblast proliferation, and reducing collagen synthesis.38,40,47 These mechanisms collectively hinder tendon-to-bone integration and increase the risk of repair failure. 46 Consequently, numerous clinical studies have shown that current smokers experience significantly higher retear rates, inferior functional outcomes, and delayed healing compared with nonsmokers.6,24,33
As public awareness of the health risks associated with smoking has grown, the global smoking prevalence has steadily declined over recent decades. 43 Global smoking rates have steadily declined from 22.7% to 17.5% between 2007 and 2021. 19 In orthopaedic practice, preoperative counseling often highlights the negative effect of smoking on tendon healing, and the decision to proceed with rotator cuff repair frequently serves as a compelling impetus for patients to initiate smoking cessation.18,45
The detrimental effects of smoking have been well established in fields such as pulmonary and cardiovascular medicine, where former smokers have been shown to experience gradual reductions in risk over time, with outcomes approaching those of nonsmokers after certain periods of abstinence.7,11,16,21,23,39 However, the evidence remains limited regarding the outcomes of patients who have quit smoking before undergoing rotator cuff repair. Moreover, it is still unclear whether the risk of tendon retear is primarily influenced by cumulative lifetime exposure versus ongoing active smoking, or the extent to which these risks can be reversed after smoking cessation.
The purpose of this study was to compare the retear rates after arthroscopic rotator cuff repair between nonsmokers, former smokers, and current smokers, and to determine the time interval after smoking cessation at which the risk of retear approximates that of nonsmokers. We hypothesized that retear rates among former smokers would decrease with increasing duration of cessation and that beyond a certain threshold, the outcomes would not significantly differ from those of nonsmokers. In addition, we sought to explore whether cumulative lifetime smoking exposure, expressed in pack-years, might independently affect tendon integrity after repair.
Methods
This study was approved by the institutional review board of our hospital, which waived the need for informed consent from patients owing to the retrospective nature of this study. All procedures were performed in accordance with the guidelines of the Declaration of Helsinki.
Data Sources and Study Population
This retrospective analysis included 2418 patients who underwent arthroscopic rotator cuff repair between March 2012 and October 2023. The surgical indications included refractory pain or functional disability despite nonoperative management for at least 3 months. The inclusion criterion was a full-thickness, degenerative posterosuperior rotator cuff tear, regardless of subscapularis involvement. Patients were excluded from the study if they (1) had follow-up periods of <2 years, (2) refused to undergo postoperative magnetic resonance imaging (MRI), (3) had undergone partial repair, (4) had a history of previous surgery on the ipsilateral shoulder, or (5) had workers’ compensation claims. After applying these criteria, 1902 patients were included for analysis (Supplemental Figure 1).
A detailed smoking history was initially obtained at the time of hospitalization and confirmed postoperatively during the follow-up. Patients were categorized as nonsmokers (group 1), former smokers (group 2A-2D), or current smokers (group 3). The nonsmoker group included individuals with no previous exposure to any form of tobacco products. Former smokers were defined as those who had ceased smoking before surgery and remained abstinent throughout the follow-up period. Based on established cardiopulmonary recovery trajectories reported in previous literature, the former smoker group was further stratified according to the duration of smoking cessation as follows: <1 year (group 2A), 1 to <3 years (group 2B), 3 to <5 years (group 2C), and ≥5 years (group 2D). 8 This classification was based on previous literature suggesting that physiological recovery from the effects of smoking, including improvements in vascular function, oxygenation, tissue healing, and systemic inflammation, progresses gradually over time, with meaningful improvements beginning after 1 to 3 years and near normalization occurring after >5 years of cessation.2,34 Pack-years of smoking were calculated by dividing the number of cigarettes smoked per day by 20 and multiplying by the total number of years of smoking, following established definitions.9,20
Clinical and Radiological Assessments
Functional outcomes were collected preoperatively and at each scheduled outpatient follow-up using the visual analog scale score for pain, the Subjective Shoulder Value, the American Shoulder and Elbow Surgeons shoulder score, and the University of California at Los Angeles shoulder score. Active range of motion (ROM) measurements included forward flexion in the scapular plane, external rotation with the elbow at the side, and internal rotation. Internal rotation was quantified by assigning a numeric score to the highest spinal vertebra level reached by the patient’s thumb. Vertebral levels T1 to T12 were scored from 1 to 12, L1 to L5 from 13 to 17, and the sacrum as 18. All ROM and functional assessments were performed by an independent examiner (H.H.C.) blinded to group assignments and patient identifiers.
Preoperative MRI scans were reviewed to evaluate tear size and fatty infiltration, which was measured at the most lateral T1-weighted sagittal oblique image at the junction of the scapular spine and body based on the Goutallier classification. 13 Structural integrity of the repaired postero-superior rotator cuff tendon was assessed on 6-month postoperative MRI (3.0-T MAGNETOM Trio, Tim System; Siemens) using the Sugaya classification, with types 4 and 5 considered indicative of retear. 37 Two shoulder subspecialty orthopaedic fellows, blinded to group assignments, assessed the grade of fatty infiltration and the cuff healing status twice at 4-week intervals. The interobserver correlation coefficients were 0.822 for the fatty infiltration of the supraspinatus muscle, 0.792 for the infraspinatus muscle, 0.737 for the subscapularis muscle, and 0.854 for rotator cuff integrity, representing acceptable results.
Surgical Procedure and Postoperative Rehabilitation
Arthroscopic repair was performed under general anesthesia with patients in the standard beach-chair position. A standard posterior portal was used to evaluate the rotator cuff tears and other intra-articular pathologies. Posterosuperior rotator cuff tears were mobilized using techniques such as coracoacromial ligament release to ensure anatomic footprint restoration. A double-row suture bridge repair was performed when complete footprint coverage was possible; otherwise, a single-row repair using 2 or 3 triple-loaded anchors was performed. Rehabilitation commenced with self-assisted circumduction exercises beginning the day after surgery, as tolerated. After 6 weeks of immobilization with an abduction brace, patients initiated passive ROM exercises, followed by active ROM at 8 weeks. Isotonic strengthening with elastic bands began at 3 months postoperatively, and a gradual return to premorbid-level sports activities was allowed after 6 months.
Statistical Analysis
A 1:1:1 propensity score matching was performed to select 276 patients in each of the nonsmoker, former smoker, and current smoker groups. Matching was based on age, employment status, tear size, and degree of fatty infiltration, which are established prognostic factors for rotator cuff healing. One-way analysis of variance was used to compare continuous variables among the groups, and categorical variables were analyzed using the chi-square test. Variables that showed statistically significant differences were further examined using post hoc subgroup analysis with Bonferroni correction.
Multivariable logistic regression was performed on the entire cohort to identify independent predictors of tendon retear as the dependent variable. Independent variables included smoking cessation duration as well as smoking pack-years, age, sex, employment status, past medical history such as diabetes mellitus and hypercholesterolemia, type and size of tear, repair technique, and fatty infiltration grade. Receiver operating characteristic (ROC) curve analysis was performed to determine optimal cutoff values for smoking cessation duration and smoking amount in relation to tendon retear. The optimal cutoff points were identified using the Youden index, which maximizes the sum of sensitivity and specificity. Based on coefficients estimated from logistic regression analysis and under the assumption that a longer cessation period and lower smoking exposure are associated with a reduced risk of retear, the cutoff points for these variables were derived using the following formula:
Statistical analyses were conducted using SAS (Version 9.4; SAS Institute) and R (Version 4.2.2; R Foundation for Statistical Computing). A P value <.05 was considered statistically significant.
Results
Of the 1902 patients who met the inclusion criteria, 1172 were in the nonsmoker group, 454 were in the former smoker group, and 276 were in the current smoker group. The mean age of patients in the nonsmoker group was significantly older than that of the former and current smoker groups, with differences also noted in sex distribution, employment status, tear size, repair technique, and degree of fatty infiltration (Table 1). The mean pack-years were similar between former and current smokers, at 19.5 ± 8.7 and 18.6 ± 8.8, respectively (P = .124). Similar baseline characteristics were achieved after 1:1:1 propensity score matching, with no significant differences among the 3 groups except for sex (Table 2).
Comparison of Nonsmoker, Former Smoker, and Current Smoker Groups a
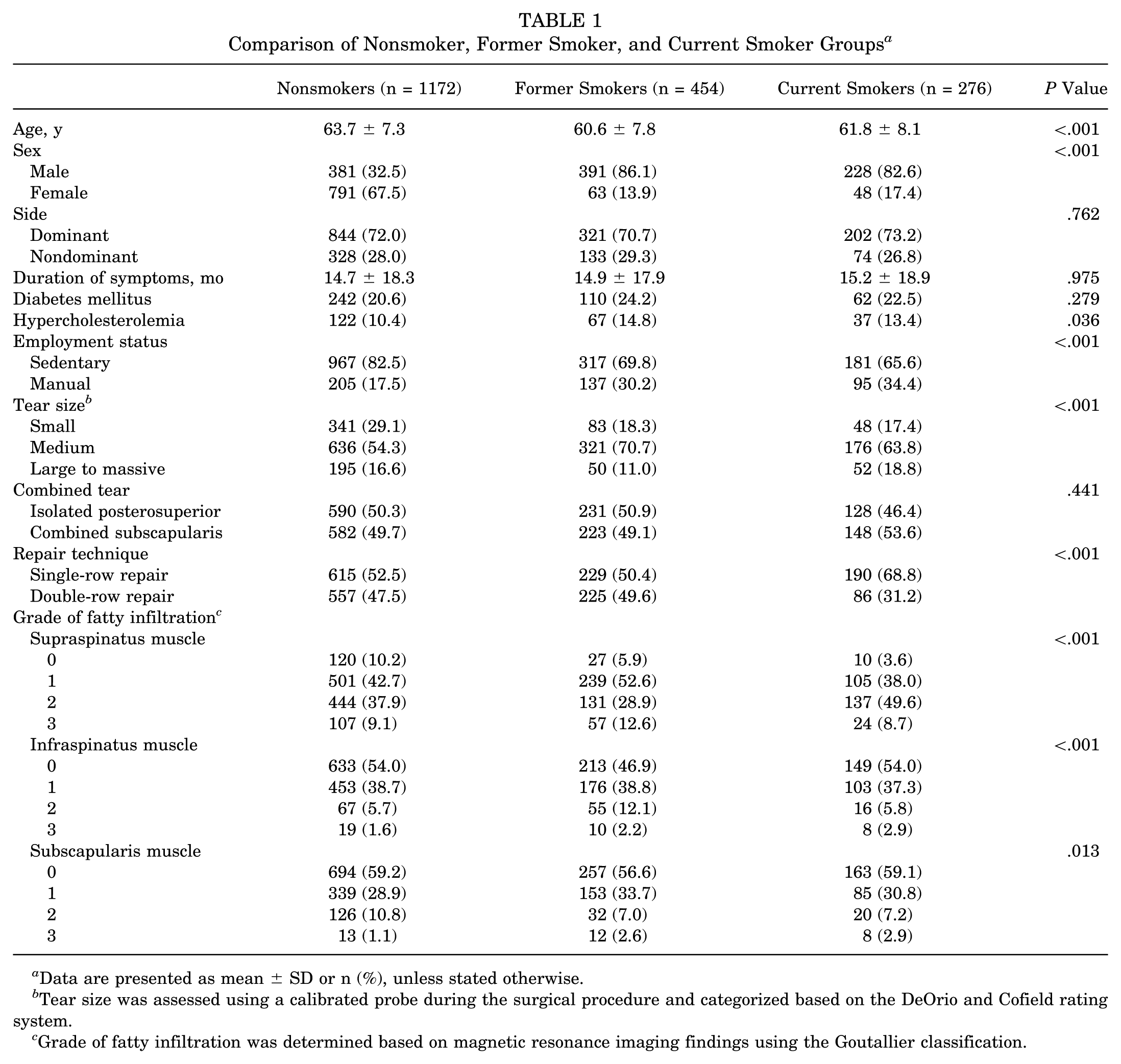
Data are presented as mean ± SD or n (%), unless stated otherwise.
Tear size was assessed using a calibrated probe during the surgical procedure and categorized based on the DeOrio and Cofield rating system.
Grade of fatty infiltration was determined based on magnetic resonance imaging findings using the Goutallier classification.
Characteristics of Matched Comparison of Nonsmoker, Former Smoker, and Current Smoker Groups a
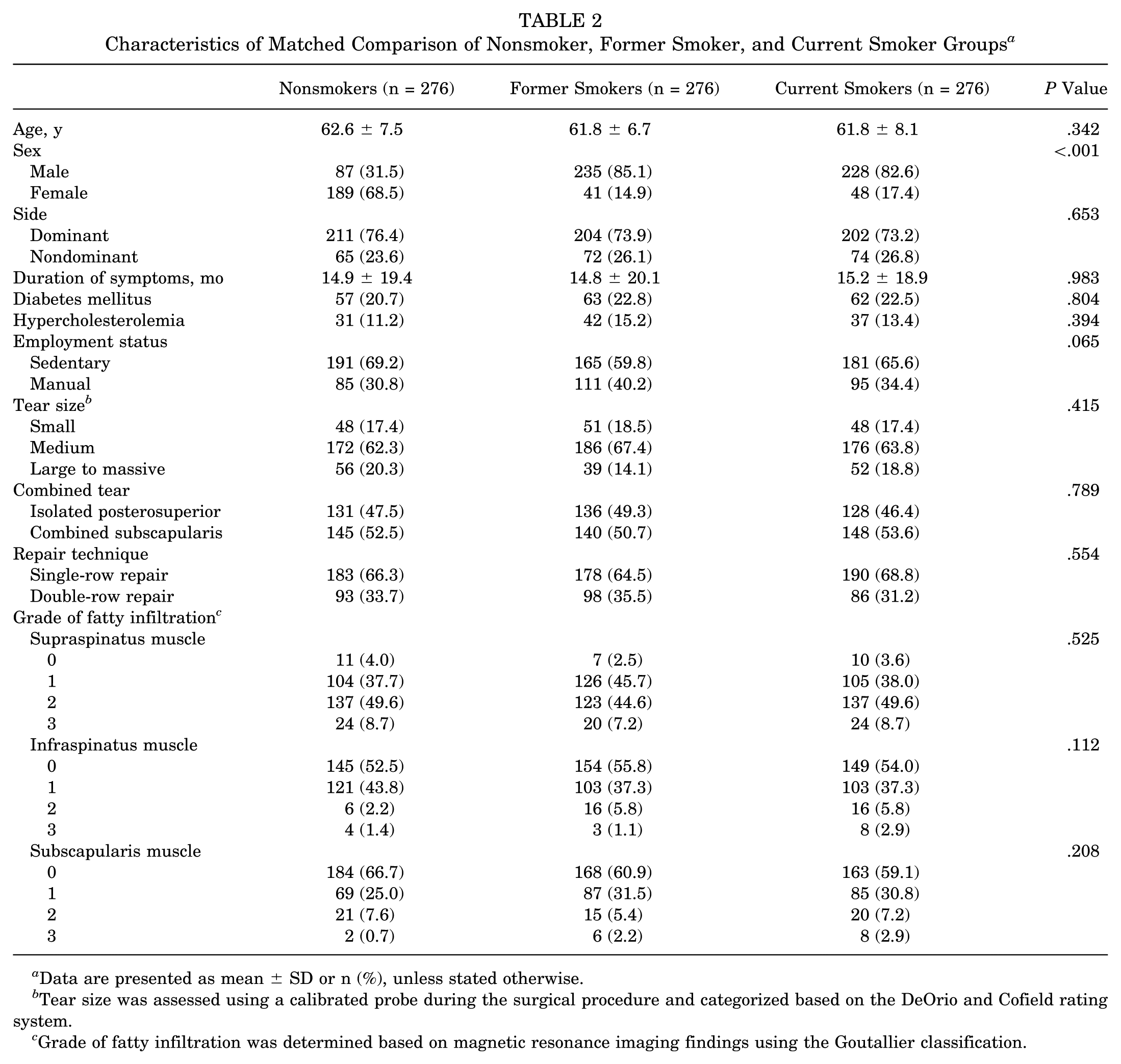
Data are presented as mean ± SD or n (%), unless stated otherwise.
Tear size was assessed using a calibrated probe during the surgical procedure and categorized based on the DeOrio and Cofield rating system.
Grade of fatty infiltration was determined based on magnetic resonance imaging findings using the Goutallier classification.
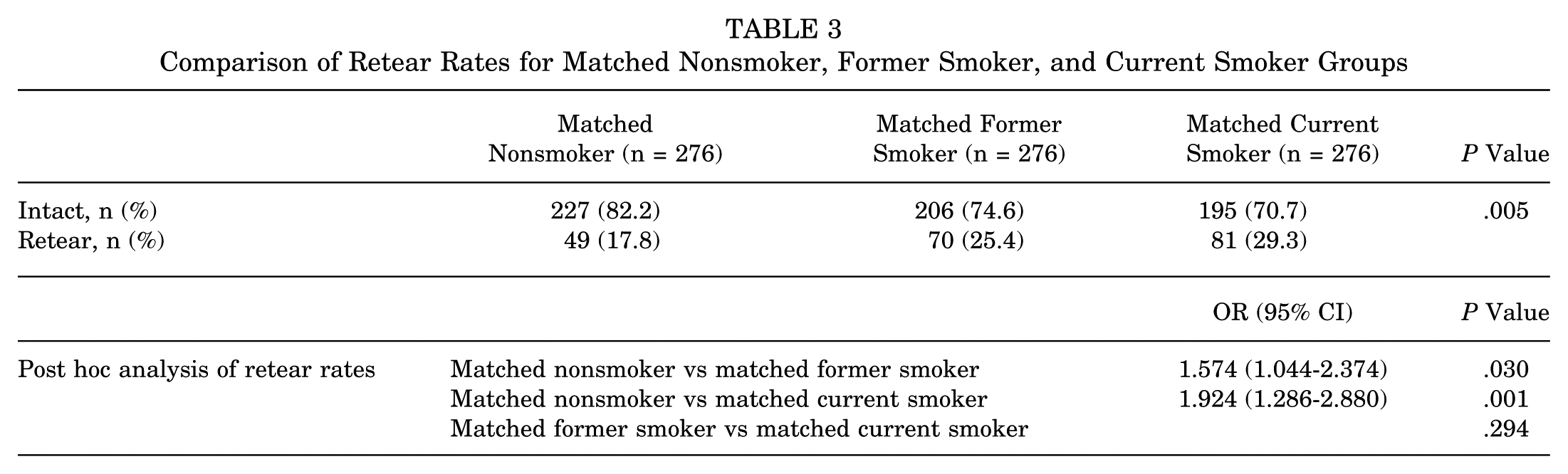
No significant differences in clinical scores or ROM were observed between the matched groups at either the preoperative baseline or 2 years postoperatively (Supplemental Table 1). In contrast, retear rates differed significantly among the 3 matched groups (P = .005). Post hoc analysis revealed significant differences between current smokers and nonsmokers and between former smokers and nonsmokers. The odds ratios for retear were 1.574 (CI, 1.044-2.374; P = .030) for former smokers compared with nonsmokers and 1.924 (CI, 1.286-2.880; P = .001) for current smokers compared with nonsmokers (Table 3). A subgroup analysis was performed to investigate the association between the duration of smoking cessation and the incidence of retears among former smokers. Patients were stratified into 4 subgroups based on cessation duration, revealing a decreasing trend in retear rates with longer cessation periods: 28.6% in subgroup 2A, 27.0% in subgroup 2B, 20.1% in subgroup 2C, and 19.4% in subgroup 2D. Using the former smoker subgroup as the reference, comparisons with the nonsmoker group revealed no significant differences in retear rates beginning from subgroups 2C and 2D, indicating that patients with smoking cessation intervals of ≥3 years had comparable outcomes to nonsmokers. In contrast, when compared with the current smoker group, only subgroup 2C demonstrated a significantly reduced retear rate (Supplemental Table 2).
Comparison of Retear Rates for Matched Nonsmoker, Former Smoker, and Current Smoker Groups
Univariate logistic regression analysis was performed on the entire cohort and identified age, smoking status, smoking pack-years, tear size, and fatty infiltration as significant predictors of retear. In the subsequent multivariable logistic regression analysis, which included all covariates, age, smoking status, pack-years, tear size, and fatty infiltration of the supraspinatus and infraspinatus muscles remained as independent prognostic factors (Table 4). ROC curve analysis of cessation duration demonstrated limited discriminatory power, with an area under the curve (AUC) of 0.577. The cutoff point for cessation duration associated with retear risk was 44 months (sensitivity, 71.2%; specificity, 46.4%; accuracy, 52.1%). Pack-year history demonstrated slightly better performance, with an AUC of 0.586. The cutoff point for pack-year history associated with retear risk was 14 pack-years (sensitivity, 41.1%; specificity, 75.8%; accuracy, 69.1%). Moreover, when cessation duration and pack-year history were combined in a composite model, the predictive performance substantially improved, with an AUC of 0.716 (sensitivity, 56.7%; specificity, 79.1%; accuracy, 74.0%), indicating that the combination of smoking duration and cessation period provided better discrimination for retear risk assessment (Figure 1).
Regression Analysis of Factors Associated With Retear After Rotator Cuff Repair
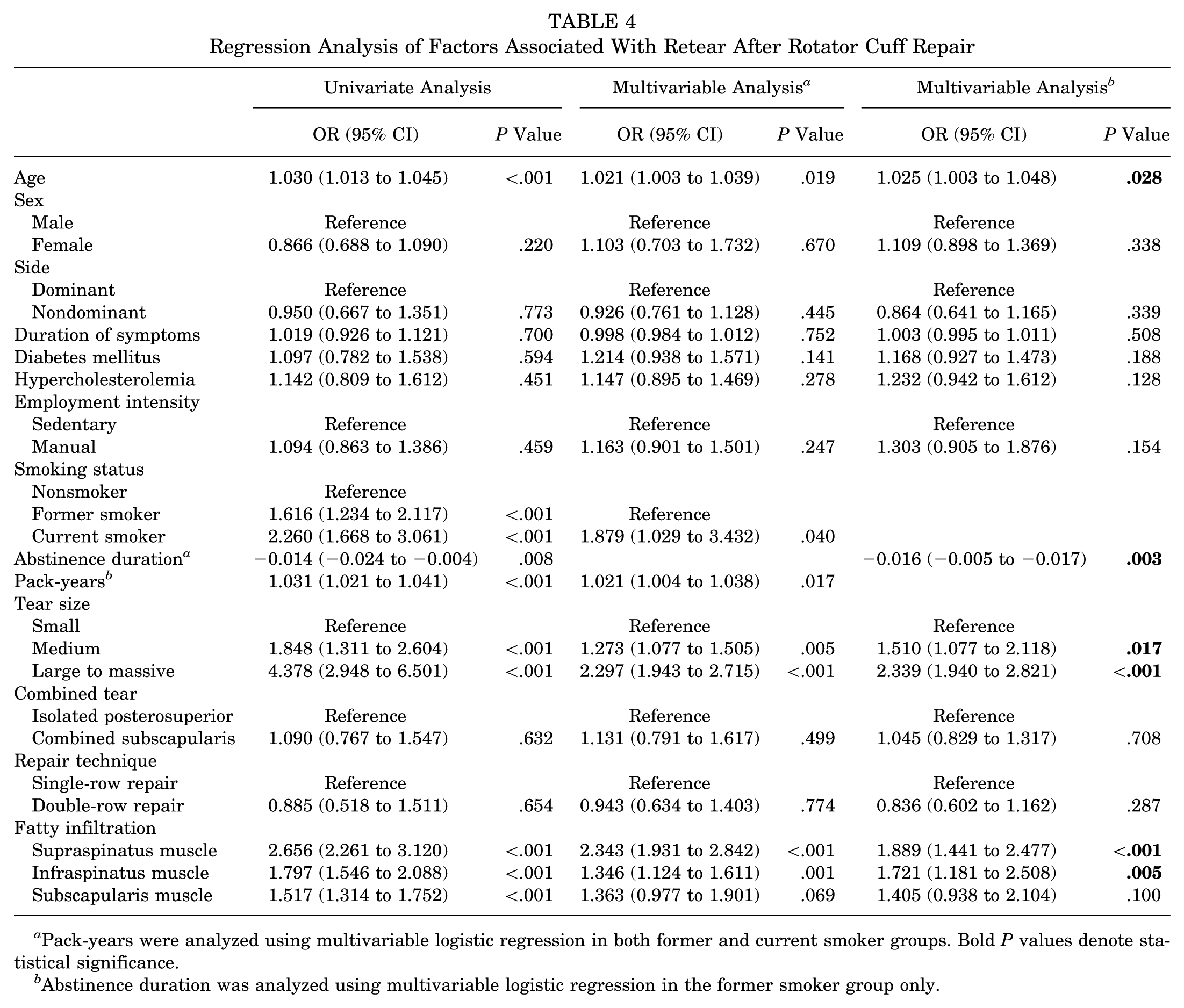
Pack-years were analyzed using multivariable logistic regression in both former and current smoker groups. Bold P values denote statistical significance.
Abstinence duration was analyzed using multivariable logistic regression in the former smoker group only.
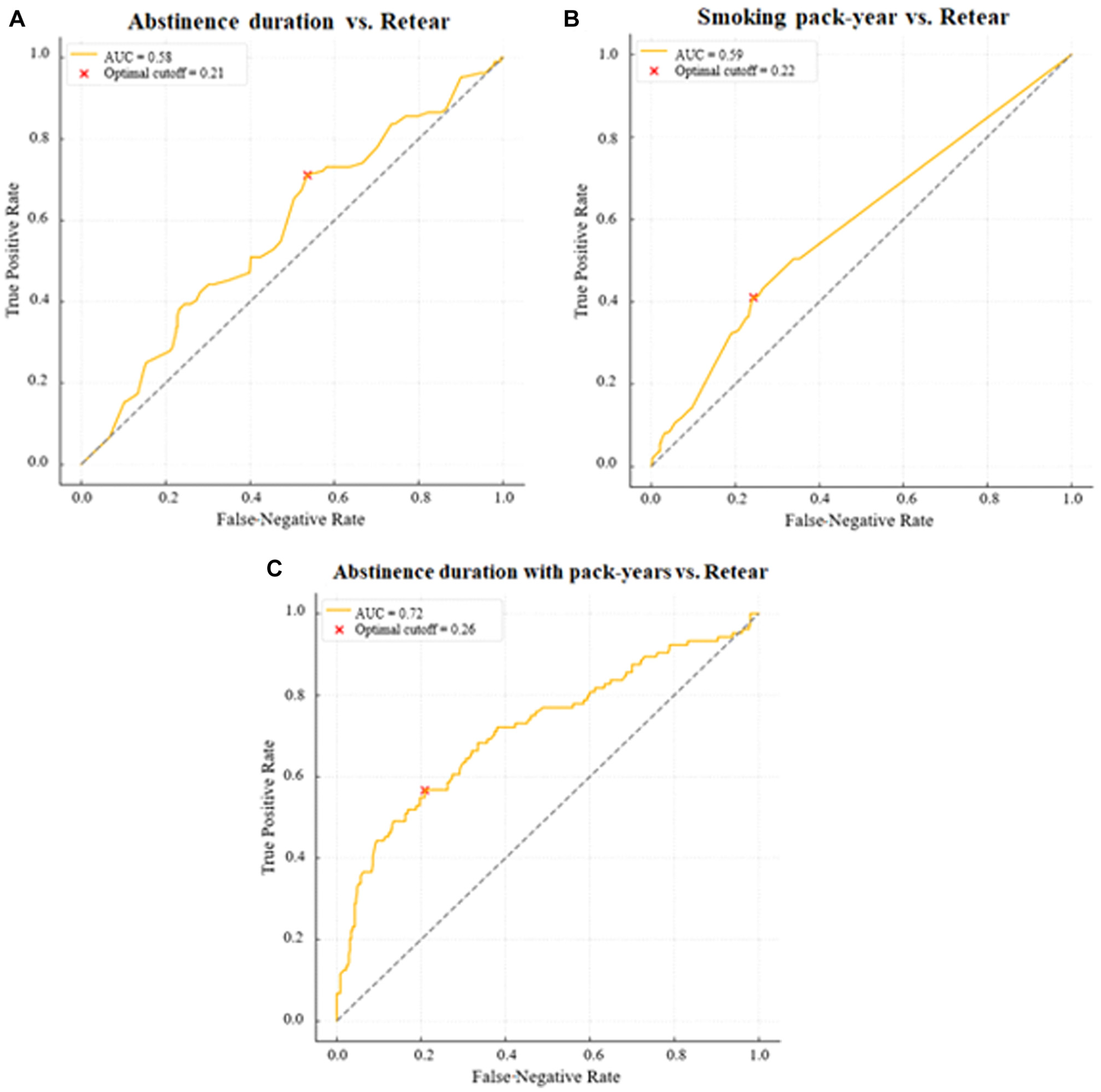
Receiver operating characteristic curves for smoking-related predictors of postoperative tendon retear: (A) smoking cessation duration alone, (B) smoking pack-years alone, and (C) combined model incorporating both cessation duration and pack-years. AUC, area under the curve.
Discussion
This study underscores the importance of sustained smoking cessation and the need to consider cumulative smoking exposure when counseling patients about expected outcomes after rotator cuff repair. Numerous previous studies have consistently demonstrated the detrimental effects of smoking on rotator cuff healing. 31 Park et al 26 reported that current smokers experienced a significantly higher healing failure rate of 29.4% compared with a failure rate of 5.9% in matched nonsmokers after arthroscopic rotator cuff repair. Importantly, evidence from other organ systems suggests that these pathophysiological changes are not permanent. Oncken et al 25 demonstrated improved bone mineral density after just 1 year of cessation, establishing that musculoskeletal tissues retain regenerative capacity after smoking cessation. This biological plausibility for recovery, combined with tissue-specific healing timelines, provides the framework for understanding why extended cessation periods may be necessary to achieve optimal tendon healing outcomes.
Our finding that 3 years of cessation is required for a significant reduction in retear rates provides a crucial time frame to the limited literature on smoking cessation in orthopaedic surgery.5,27,41 Although most previous studies have examined only short-term cessation, our results align with the few investigations of longer cessation periods. Glassman et al 12 found that in lumbar fusion, former smokers who had quit for unspecified durations achieved an 82% fusion rate, intermediate between those of current smokers and never smokers (73% and 95%, respectively). This protracted recovery timeline is remarkably consistent in other organ systems. Pulmonary function follows a course, with mucociliary clearance taking up to 3 years to normalize, whereas inflammatory markers may require ≥5 years to reach nonsmoker levels. 30 Cancer epidemiology provides perhaps the most compelling parallel, with studies demonstrating that lung cancer risk decreases progressively after smoking cessation, with a 50% reduction achieved by 5 to 6 years and approaching nonsmoker levels after 10 to 15 years of abstinence. 42 Therefore, our finding that rotator cuff healing requires extended cessation periods aligns with these complex organs that undergo substantial structural remodeling. The extended recovery period likely reflects the time needed to reverse smoking-induced changes in tissue vascularity, cellular function, and extracellular matrix composition.
The influence of cumulative smoking exposure emerged as an independent predictor of repair failure in our analysis, corroborating dose-dependent relationships observed across musculoskeletal literature. 1 Park et al 26 observed a threshold effect, with patients exceeding 20 pack-years demonstrating a disproportionately high failure rate after rotator cuff repair. Similarly, Baumgarten et al 3 revealed a clear dose-dependent relationship, with odds ratios for rotator cuff tears increasing from 1.08 for patients smoking <1 pack per day to 1.66 for those smoking 1 to 2 packs per day and 3.35 for those smoking >2 packs per day. The persistent influence of pack-years even after cessation suggests that smoking induces irreversible structural changes in tendon architecture, including decreased collagen fiber organization, reduced vascularity, and altered cellular composition. 35 Our combined model incorporating both cessation duration and pack-years (AUC, 0.716) outperformed either variable alone, indicating that optimal risk stratification requires consideration of both the burden of past exposure and the duration of recovery. This has important clinical implications, as patients with heavy smoking histories may require longer cessation periods to achieve acceptable healing rates, and some patients with high smoking exposure may never fully normalize their risk profile, despite prolonged abstinence.
Although clinical scores and ROM at the 2-year follow-up did not differ significantly among the 3 groups, the higher retear rates observed in current smokers remain clinically relevant. Previous studies have consistently demonstrated a partial dissociation between structural integrity and short- to midterm clinical outcomes, with patient-reported outcomes generally improved whether or not the repair restored cuff integrity.22,32 However, accumulating evidence suggests that higher retear rates are associated with long-term functional deterioration. 15 Similarly, long-term studies with follow-up extending beyond 10 years have shown that structural integrity correlates well with clinical and functional results. 17 Therefore, our findings regarding the effect of smoking status on tendon healing provide actionable information for preoperative counseling and risk stratification, even in the absence of early differences in patient-reported outcomes.
Limitations
This study has several limitations that warrant careful consideration when interpreting our findings. The retrospective design precludes causal inference, and selection bias may exist, as patients who successfully quit smoking might represent a more health-conscious subgroup with better overall tissue healing capacity. Our reliance on self-reported smoking history without biochemical verification, such as cotinine levels, introduces potential misclassification bias, particularly regarding cessation dates and smoking intensity. The study’s geographic limitation to a single country may affect generalizability, as genetic polymorphisms affecting nicotine metabolism and tendon healing properties vary across ethnic populations. We also lacked data on several factors that could modulate the relationship between cessation and healing, including secondhand smoke exposure, nicotine replacement therapy uses, and relapse episodes during the follow-up period. Additionally, our analysis could not account for emerging tobacco products such as electronic cigarettes or heated tobacco products, which may have different effects on tissue healing. Finally, we did not incorporate specific medication uses or other systemic factors into the propensity score model, and these unmeasured or residual confounders may still have influenced tendon healing despite adjustment in the regression analysis.
Conclusion
Sustained smoking cessation significantly lowers retear rates after rotator cuff repair, with at least 3 years of abstinence required to achieve rates comparable to those of nonsmokers. Pack-years and duration of cessation serve as independent predictors of tendon healing.
Supplemental Material
sj-docx-1-ajs-10.1177_03635465261422620 – Supplemental material for Duration of Smoking Cessation Needed to Achieve Retear Rates Comparable to Those of Nonsmokers After Arthroscopic Rotator Cuff Repair
Supplemental material, sj-docx-1-ajs-10.1177_03635465261422620 for Duration of Smoking Cessation Needed to Achieve Retear Rates Comparable to Those of Nonsmokers After Arthroscopic Rotator Cuff Repair by Hsien-Hao Chang, Yong-Min Chun, Sung-Jae Kim, Won-Myung Kim and Tae-Hwan Yoon in The American Journal of Sports Medicine
Footnotes
Submitted October 24, 2025; accepted January 3, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.