
Abstract
Background:
Trochlear dysplasia is a critical risk factor for patellar instability, and existing animal models focus on indirect mechanical intervention and fail to replicate its pathological process.
Purpose:
To describe a novel trochlear dysplasia model in rats and investigate changes in external morphology and internal architecture of the trochlea in this model.
Study Design:
Controlled laboratory study.
Methods:
Twenty immature 4-week-old Sprague-Dawley rats were subjected to targeted injury of the anterior distal femoral epiphysis in the left knee, with the right knee used as the control group. All rats were evaluated by gross observation and micro–computed tomography. Macroscopic measurements included sulcus angle (SA), trochlear groove depth (TGD), trochlear width, medial condylar height, lateral condylar height, medial trochlear inclination (MTI), lateral trochlear inclination (LTI), and trochlear bump height. Trabecular microarchitectural parameters of the distal femoral epiphysis included bone mineral density (BMD), bone volume fraction (BV/TV), trabecular number (Tb.N), trabecular thickness (Tb.Th), and trabecular spacing (Tb.Sp).
Results:
The surgical group exhibited growth arrest at the anterior distal femoral epiphysis and 4 distinct types of trochlear dysplastic manifestations with a flat, shallow trochlea and bump deformity at the entrance of the trochlea, whereas the control group showed normally deepened trochlear grooves. Compared with the control group, the surgical group had significantly larger SA (136.13°± 7.32° vs 122.45°± 8.28°; P = .020) and smaller TGD (0.49 ± 0.15 mm vs 0.67 ± 0.10 mm; P = .033), MTI (17.15°± 7.96° vs 24.32°± 4.27°; P = .018), and LTI (26.72°± 4.72° vs 34.65°± 6.04°; P = .012). No significant differences were observed in BMD, BV/TV, Tb.N, Tb.Th, and Tb.Sp between the 2 groups.
Conclusion:
A novel trochlear dysplasia animal model similar to humans was established in immature rats via targeted injury of the anterior distal femoral epiphysis, which exhibited growth arrest at the anterior distal femoral epiphysis and key pathological features of human trochlear dysplasia.
Clinical Relevance:
The model is a potential platform for investigating the basic mechanisms of trochlear dysplasia and developing therapeutic treatments.
Trochlear dysplasia is a critical and common risk factor for patellar instability, significantly raising the incidence of patellofemoral osteoarthritis.3,4,11,19 However, the biological mechanism of trochlear dysplasia remains unclear. Animal models serve as valuable tools for exploring the pathogenesis of diseases. Existing models for trochlear dysplasia were based on the mechanism that mechanical factors play crucial regulatory roles in trochlear development and induced trochlear dysplasia by reducing patellofemoral stress, including patellar dislocation, patellectomy, patella alta, femoral torsion, breech position, and straight-leg swaddling position models.8,9,12,22,24 However, these models mainly focused on altering patellofemoral mechanical stress to indirectly affect trochlear development, which only simulated the secondary adaptive changes of the trochlea rather than targeting its primary developmental origin, and failed to replicate its pathological process, leading to limited clinical relevance and applicability.8,9,12,22,24 Thus, there is a need for a novel model that could reflect the potential pathogenesis of trochlear dysplasia.
Recently, studies regarding the relationship between the trochlea and distal femoral epiphysis have provided novel insights into exploring the mechanism of trochlear dysplasia. A close spatial association exists between the proximal-most part of the trochlea and the anterior distal femoral epiphysis. 16 In patients with skeletal immaturity with trochlear dysplasia, the medial distal femoral epiphyseal plate has been found to be dysplastic through clinical studies.5,10 Notably, a separate longitudinal follow-up study by the same research team showed that surgical correction of patellar dislocation caused significant improvements in the morphology of both the previously dysplastic epiphyseal plate and the trochlea.5,10 Additionally, the epiphysis serves as the primary site for chondrocyte proliferation and differentiation, which is a critical process for trochlear development. 18 Injury of the distal femoral epiphysis has been shown to cause permanent growth disturbance and femoral shortening. 14 Collectively, these findings indicate that the distal femoral epiphysis is necessary for normal trochlear formation and suggest that injury of the distal femoral epiphysis may induce trochlear dysplasia.
Additionally, the correlation between femoral head epiphyseal injury and subsequent femoral head deformity provides a critical mechanistic reference for exploring trochlear dysplasia, as both the femoral head epiphysis and distal femoral epiphysis belong to articular epiphyses of long bones, sharing the core developmental mechanism of chondrocyte proliferation-driven morphological development.7,20 For instance, partial medial epiphysiodesis of the femoral head epiphyseal plate arrested medial physeal growth while preserving normal lateral longitudinal growth, ultimately resulting in femoral head varus. 20 Similarly, medial femoral head epiphyseal injury in immature rabbits caused proximal femoral physeal growth arrest, leading to femoral head deformities similar to human femoroacetabular impingement. 7 By extension, a logically sound approach to induce trochlear dysplasia would be to intentionally target and injure the anterior distal femoral epiphysis in the immature knee.
The purposes of this study were to (1) describe a novel minimally invasive surgical technique for establishing a trochlear dysplasia model in skeletally immature rats via targeted injury of the anterior distal femoral epiphysis and (2) investigate the changes in external morphology and internal architecture of the trochlea in this model. It was hypothesized that a trochlear dysplasia model could be successfully established, and the subsequent pathological morphological and architectural changes in the trochlea could be observed.
Methods
Study Design
The experimental protocol was approved by the Animal Care and Use Committee of our institution and was conducted in accordance with the Guide for the Care and Use of Laboratory Animals. Twenty immature 4-week-old female Sprague-Dawley rats with normal birth and life history were included. Preoperative screening confirmed no patellar dislocation during knee extension and flexion activities and no limp in daily walking. All rats were raised under uniform conditions. Each animal was housed individually in a stainless steel cage with free access to cage activity. The left knees of all rats received the surgery targeting injury of the anterior distal femoral epiphysis and were classified into the surgical group. The contralateral right knees were used as the control group. All rats were euthanized at 4 weeks postoperatively.
Surgical Technique
Preoperatively, surgical anesthesia was induced with an intraperitoneal injection of pentobarbital sodium (50 mg/kg). Then the knee surgical site was shaved and disinfected with povidone iodine (10% solution) to ensure an aseptic environment, followed by 2% lidocaine subcutaneous infiltration anesthesia. The knee was draped in a standard sterile fashion to expose the distal femur in the operative field. In the surgical group, the rat was placed in the right lateral position, and a 1-cm straight incision was made along the lateral border of the left knee, parallel to the femoral shaft. The subcutaneous tissue and superficial fascia were bluntly dissected with hemostatic forceps to expose the lateral femoral condyle. After localizing the distal femoral epiphysis, 8 the center point of the anterior distal femoral epiphysis was used as the landmark site to determine the location of epiphyseal injury and guide the drilling direction (Figure 1).
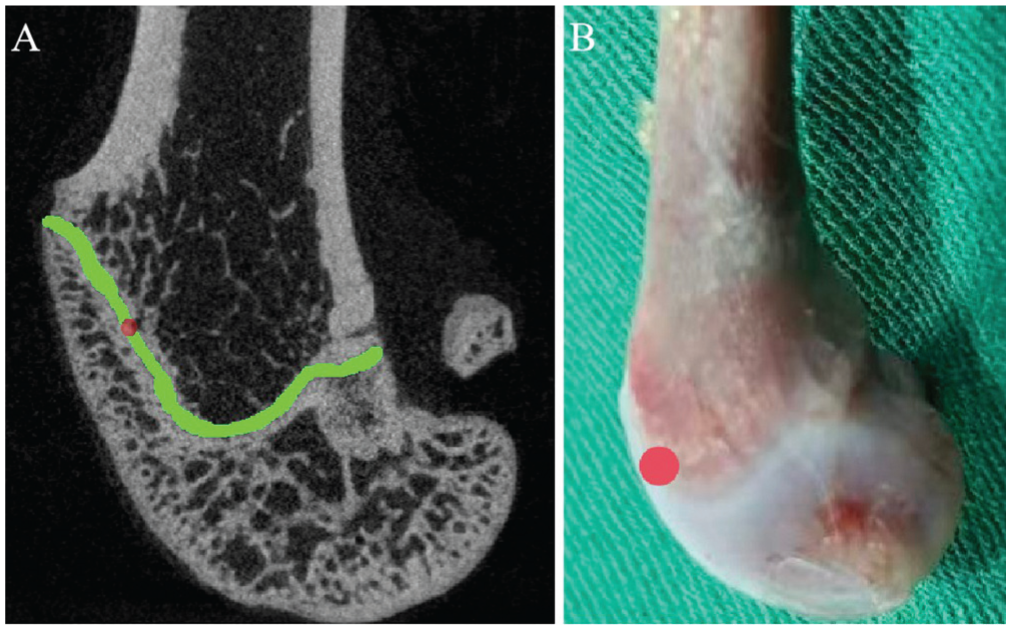
Schematic diagram of drilling location. (A) The center point of the anterior distal femoral epiphysis was used as the landmark site to determine the location of epiphyseal injury. (B) The drilling position in the distal femur.
A sterile stainless steel drill bit (orthopaedic microdrill, 1.3 mm in diameter, 1500 rpm) was held perpendicular to the anterior distal femoral epiphyseal surface, aligned with the prelocalized landmark. The epiphyseal plate was drilled through, and the drilling was stopped when slight resistance was felt, indicating that the epiphysis had been penetrated. Continuous irrigation with sterile normal saline was applied to the drill bit during drilling to reduce thermal necrosis of epiphyseal chondrocytes caused by friction. Therefore, a parallel penetrating defect was created on the targeted anterior distal femoral epiphysis according to the landmark site. The defect was gently irrigated with sterile normal saline to remove bone debris. Passive knee extension or flexion was then performed to assess patellar kinematics, confirming no patellar dislocation and smooth patellar tracking within the full range of motion. The fascia, subcutaneous tissue, and skin were closed using sutures in separate layers. The dressing was applied to protect the wound. The contralateral right knees did not undergo any surgery and served as the control group. Postoperatively, acetaminophen (200 mg/kg) was administered via intraperitoneal injection for 5 days for postoperative analgesia.
Gross Observation
All rats were euthanized 4 weeks postoperatively. The distal femurs were harvested, and adherent soft tissues including muscle and fascia were carefully removed. One independent researcher (K.H.), blinded to the group assignments and study hypothesis, performed a visual assessment of trochlear gross morphology. Additionally, the presence of cartilage degeneration on the trochlear surface was assessed in all knees.
Micro–Computed Tomography
After gross observation, all distal femoral samples were scanned using a micro–computed tomography (CT) scanner (PerkinElmer) to analyze trochlear deformity and trabecular microarchitectural features. The scanning parameters were set as follows: tube current, 88 μA; tube voltage, 90 kVp; and resolution, 45 μm.
Macroscopic Measurement
Micro-CT scan data were reconstructed into 3-dimensional (3D) models using Mimics software (Version 19.0; Materialise) to enable the trochlea-related parameters to be directly measured at an independent workstation. Subsequent measurements were performed on the axial slices showing the “Roman arch,” including the following parameters: sulcus angle (SA), trochlear groove depth (TGD), trochlear width (TW), medial condylar height (MCH), lateral condylar height (LCH), medial trochlear inclination (MTI), and lateral trochlear inclination (LTI) (Figure 2).5,8,13 All macroscopic measurements were performed based on bony landmarks using 3D reconstructed micro-CT models. SA was defined as the angle formed between the medial and lateral trochlear facets. TGD was defined as the perpendicular distance from the deepest point of the trochlear groove to the line connecting the most anterior points of the medial and lateral femoral condyles. TW was defined as the distance between the most anterior points of the medial and lateral femoral condyles. MCH or LCH was defined as the perpendicular distance from the most anterior point of the medial or lateral femoral condyle to the line connecting the posterior edges of the femoral condyles. MTI or LTI was defined as the angle between the medial or lateral trochlear facet and the line connecting the posterior edges of the femoral condyles. For sagittal plane measurement, a sagittal slice passing through the center of the trochlear groove was selected to measure trochlear bump height (TBH) (Figure 2). TBH was defined as the perpendicular distance from the highest point of the trochlear bump to the extension line of the femoral anterior cortical bone. 8
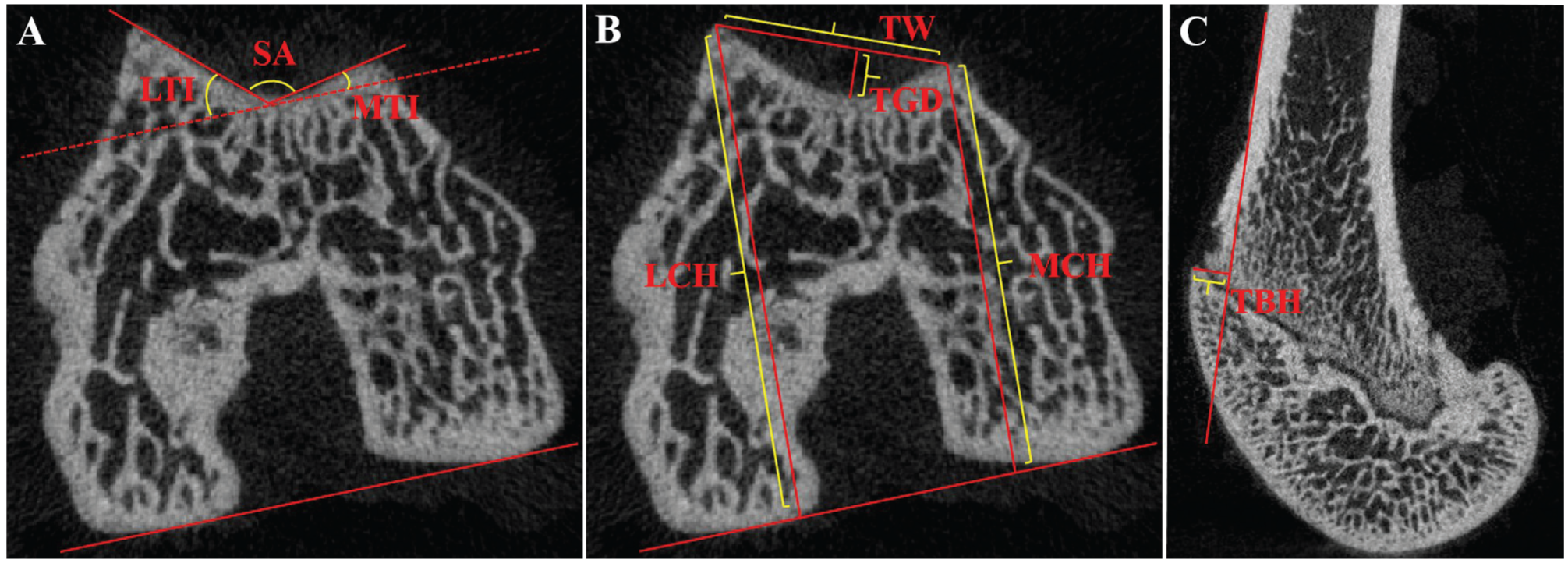
Schematic diagram of macroscopic measurements. (A) Sulcus angle (SA), medial trochlear inclination (MTI), and lateral trochlear inclination (LTI). (B) Trochlear groove depth (TGD), trochlear width (TW), medial condylar height (MCH), and lateral condylar height (LCH). (C) Trochlear bump height (TBH).
Microscopic Measurement
For microarchitectural analyses, 2 cylindrical bone regions of interest with a diameter of 1 mm were defined within the medial and lateral distal femoral epiphyses, respectively (Figure 3).
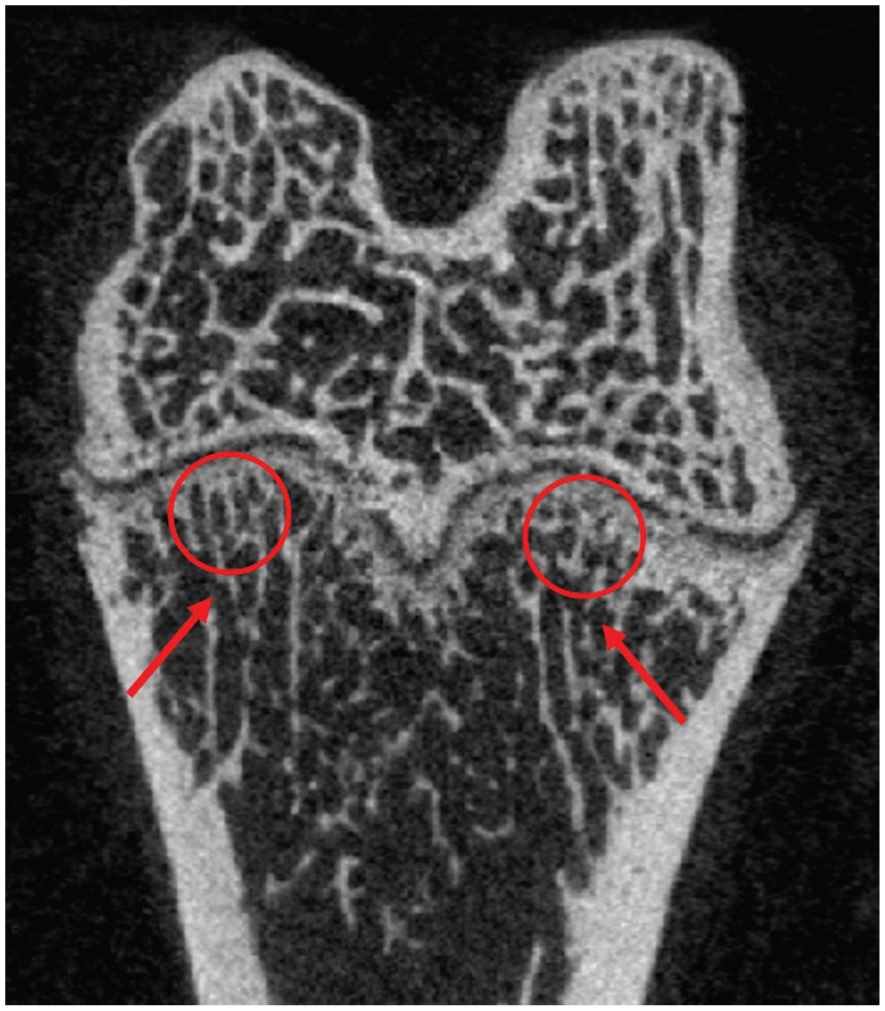
Schematic diagram showing the regions of interest within the medial and lateral distal femoral epiphyses for trabecular microarchitectural analyses. Arrows indicate the regions of interest in the medial and lateral distal femoral epiphyses.
After integrating micro-CT scan data into 3D voxel images and completing 3D reconstruction, the following parameters were measured to analyze the trabecular microarchitecture of the distal femoral epiphysis: bone mineral density (BMD; g/cm3), bone volume fraction (BV/TV; %), trabecular number (Tb.N; 1/mm), trabecular thickness (Tb.Th; mm), and trabecular spacing (Tb.Sp; mm).
Measurement Reliability
To minimize measurement bias, 2 independent, experienced orthopaedic researchers (L.K. and Y.Q.), blinded to the group assignments and study hypothesis, evaluated all images and measured the aforementioned parameters. For any measurement discrepancies, a third independent researcher (H.K.) was consulted to resolve the issue through discussion until a consensus was reached. Additionally, 1 researcher (L.K.) repeated all measurements after a 4-week interval. Intraclass correlation coefficient (ICC) values were calculated to assess intraobserver and interobserver reliabilities. An ICC value of 0.75 to 0.9 indicated good reliability, and an ICC value > 0.9 indicated excellent reliability.
Statistical Analysis
Continuous variables are described as means and standard deviations. Before statistical comparisons, data were tested for normality using the Shapiro-Wilk test and for homogeneity of variance using the Levene test. Normally distributed data with homogeneous variances were analyzed using the paired-samples t test, and nonnormal data or data with heterogeneous variances were analyzed using the Wilcoxon signed-rank test. All statistical analyses were performed using IBM SPSS Statistics (Version 26.0; IBM Corp). A 2-tailed P value <.05 was considered statistically significant. Sample size calculation using an a priori power analysis for paired samples was performed using G*Power (Version 3.1.9.4; Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany). To detect an effect size of 0.8 with a 2-tailed α of .05 and statistical power of 0.9, the minimum estimated sample size was 15 rats (30 knees).
Results
Gross Observation
No patellar dislocation was observed in any knees of the surgical group and the control group preoperatively. The surgical group exhibited 4 distinct types of trochlear dysplastic manifestations (Figure 4): (A) mild trochlear dysplasia with a shallow, flat trochlear groove; (B) trochlear dysplasia with dysplasia of the lateral femoral condyle; (C) trochlear dysplasia with a bump deformity at the entrance of the trochlea; and (D) severe trochlear dysplasia with the presence of osteoarthritis. Types A, B, and C trochlea showed no patellar instability, while type D trochlea exhibited patellar instability, defined as patellar laxity, abnormal patellar tracking, or transient patellar subluxation during passive knee movement. In contrast, all knees in the control group developed normally deepened trochlear grooves and showed no signs of patellar instability.
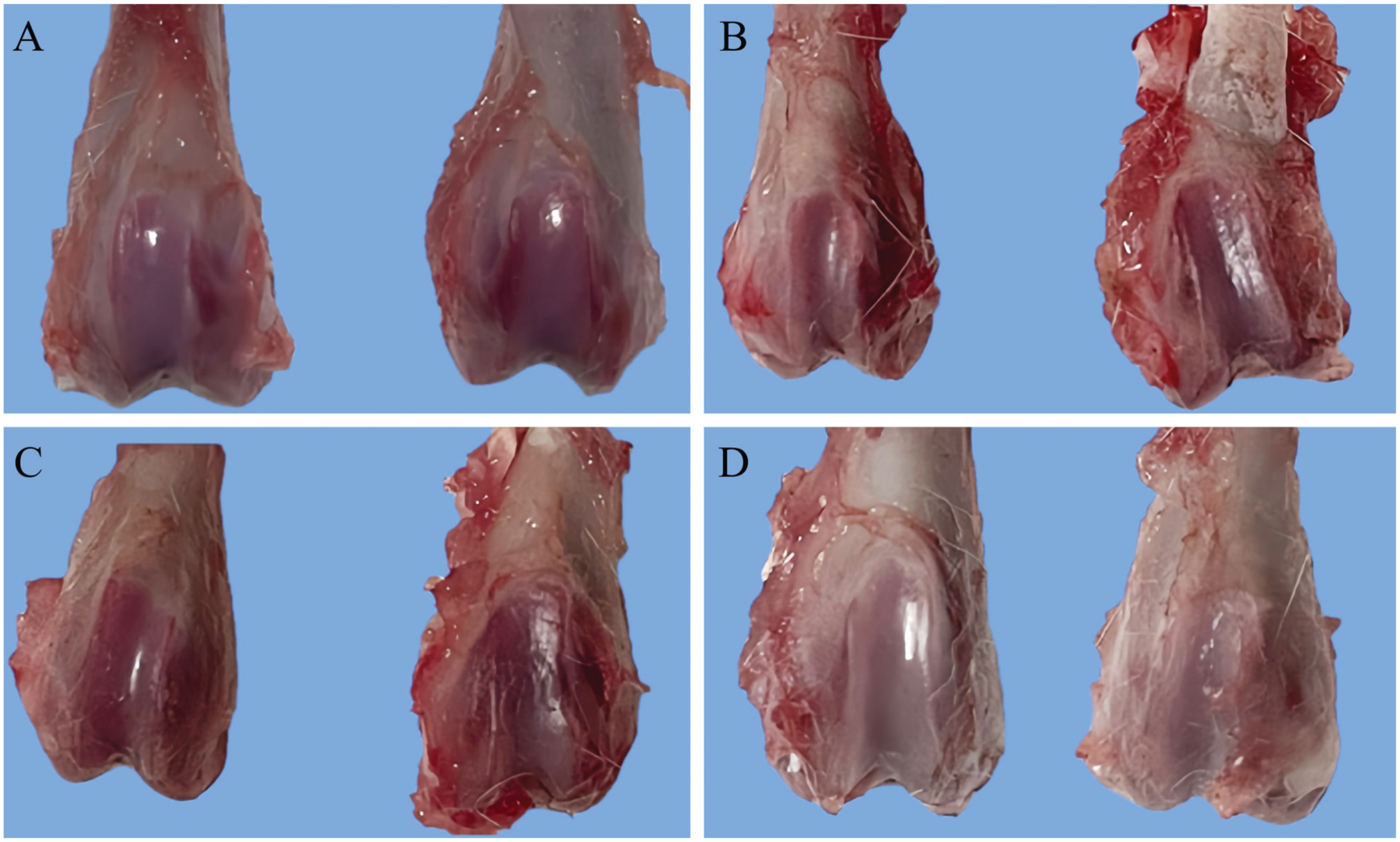
Gross observation of the trochlea. The right side of each image was obtained from the surgical group. (A) Mild trochlear dysplasia with a shallow, flat trochlear groove. (B) Trochlear dysplasia with dysplasia of the femoral lateral condyle. (C) Trochlear dysplasia with a bump deformity at the entrance of the trochlea. (D) Severe trochlear dysplasia with the presence of osteoarthritis. The left side of each image was obtained from the control group, showing normally deepened trochlear grooves.
Macroscopic Evaluation
Representative micro-CT images of the distal femur are shown in Figure 5. At 4 weeks postoperatively, the distal femoral epiphyseal closure was observed in the surgical group, and some of them were accompanied by a bump deformity at the entrance of the trochlea, whereas the control group showed the intact distal femoral epiphyseal line without the secondary trochlear deformity.
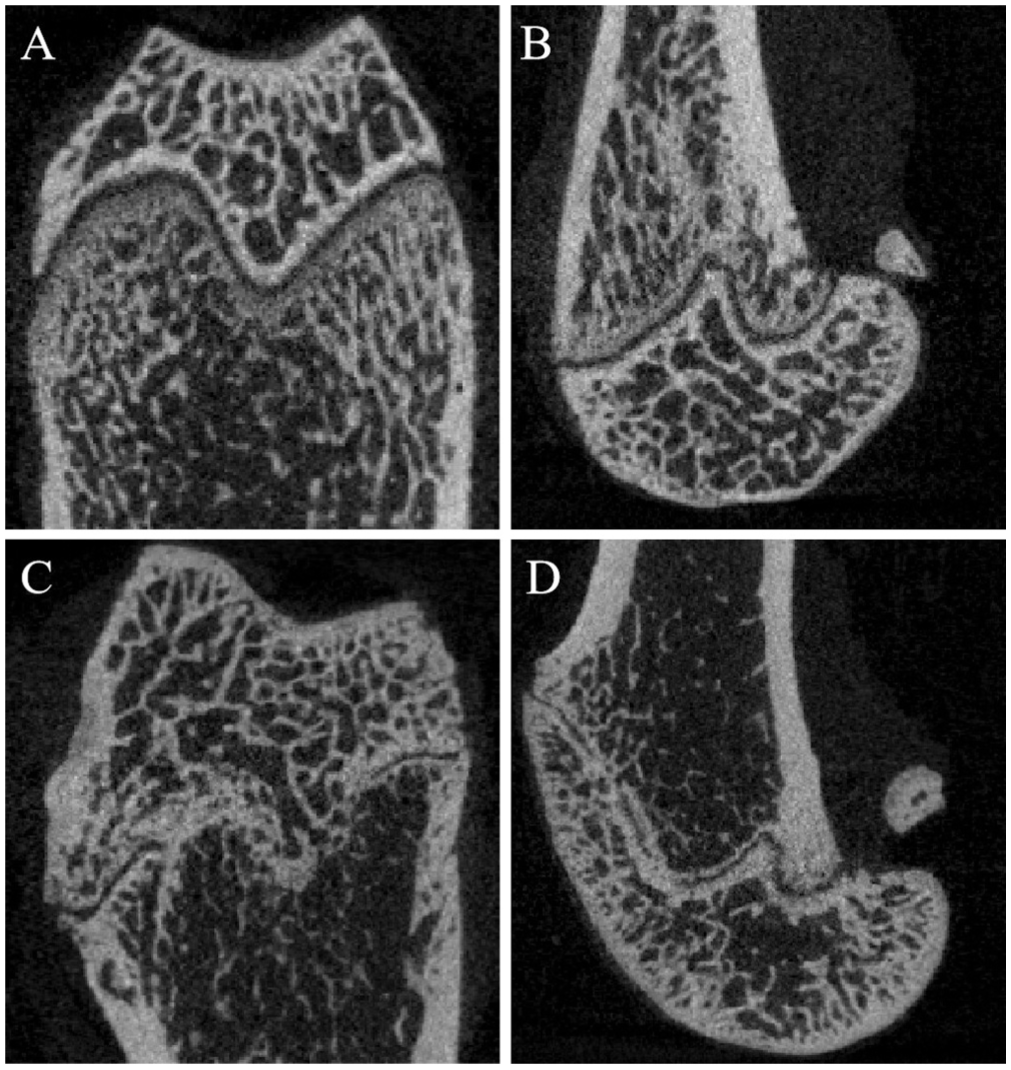
Representative micro–computed tomography (CT) images of the distal femur. The coronal (A) and sagittal (B) micro-CT images obtained in the control group showed the intact distal femoral epiphyseal line. The coronal (C) and sagittal (D) micro-CT images obtained in the surgical group showed the distal femoral epiphyseal closure accompanied by a bump deformity at the entrance of the trochlea.
Macroscopic parameters of trochlear morphology are presented in Table 1. For measurement reliability, intraobserver ICC values ranged from 0.895 to 0.964, and interobserver ICC values ranged from 0.882 to 0.956, indicating good to excellent measurement reliability for all macroscopic measurements. Compared with the control group, the surgical group exhibited significantly larger SA (136.13°± 7.32° vs 122.45°± 8.28°; P = .020) and significantly smaller TGD (0.49 ± 0.15 mm vs 0.67 ± 0.10 mm; P = .033), LTI (26.72°± 4.72° vs 34.65°± 6.04°; P = .012), and MTI (17.15°± 7.96° vs 24.32°± 4.27°; P = .018). No significant differences were observed in TW, MCH, LCH, or TBH between the 2 groups. Collectively, these macroscopic parameters confirmed that injury of the anterior distal femoral epiphysis successfully induced dysplastic trochlea.
Macroscopic Parameters of Trochlear Morphology a
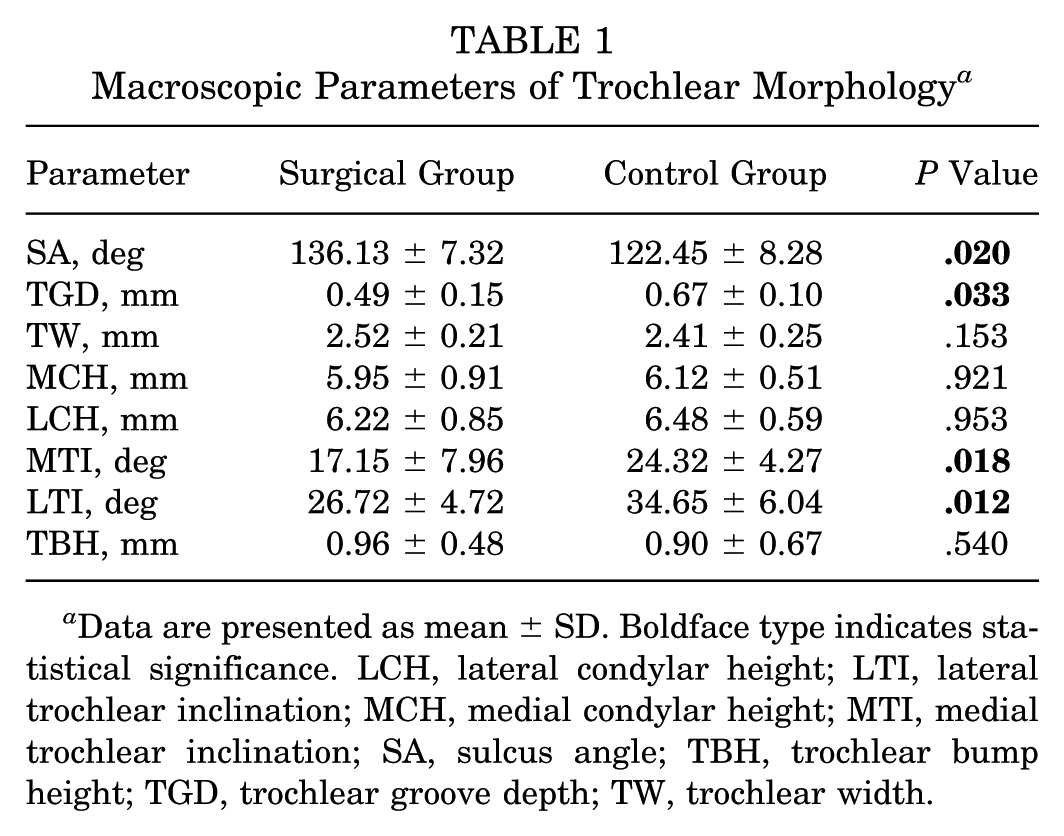
Data are presented as mean ± SD. Boldface type indicates statistical significance. LCH, lateral condylar height; LTI, lateral trochlear inclination; MCH, medial condylar height; MTI, medial trochlear inclination; SA, sulcus angle; TBH, trochlear bump height; TGD, trochlear groove depth; TW, trochlear width.
Macroscopic parameters between subtypes of trochlear dysplasia revealed distinct morphological characteristics (Table 2). Each subtype exhibited key features matching its corresponding human trochlear dysplasia phenotype. Subtype A showed a mild flat trochlear groove, subtype B showed lateral condylar dysplasia, subtype C showed a bump deformity at the entrance of the trochlea, and subtype D showed severe trochlear dysplasia with osteoarthritis. The subgroup-specific data validated the utility of this animal model to replicate the pathological heterogeneity of human trochlear dysplasia.
Macroscopic Parameters Between Subtypes of Trochlear Dysplasia a
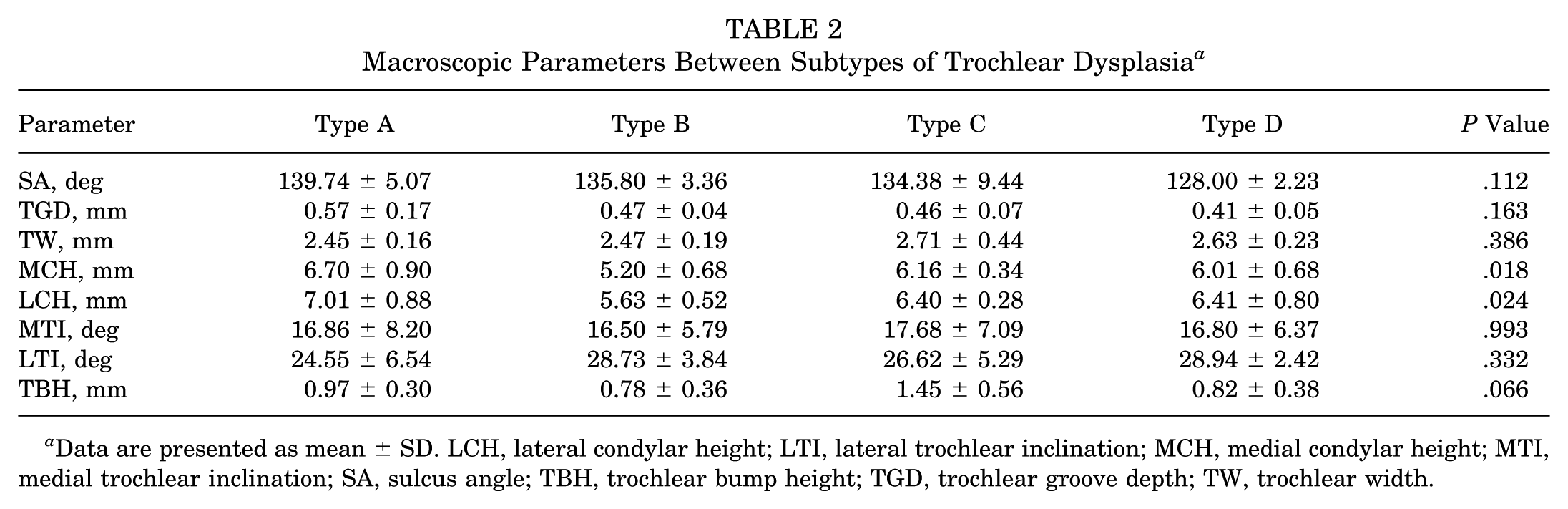
Data are presented as mean ± SD. LCH, lateral condylar height; LTI, lateral trochlear inclination; MCH, medial condylar height; MTI, medial trochlear inclination; SA, sulcus angle; TBH, trochlear bump height; TGD, trochlear groove depth; TW, trochlear width.
Microscopic Measurement
Trabecular microarchitectural parameters are presented in Table 3. No significant differences were observed in BMD, BV/TV, Tb.N, Tb.Th, or Tb.Sp between the surgical group and the control group, either in the medial distal femoral epiphysis or in the lateral distal femoral epiphysis. For measurement reliability, intraobserver ICC values ranged from 0.912 to 0.984, and interobserver ICC values ranged from 0.894 to 0.972, indicating good to excellent measurement reliability for all microscopic measurements.
Trabecular Microarchitectural Parameters a
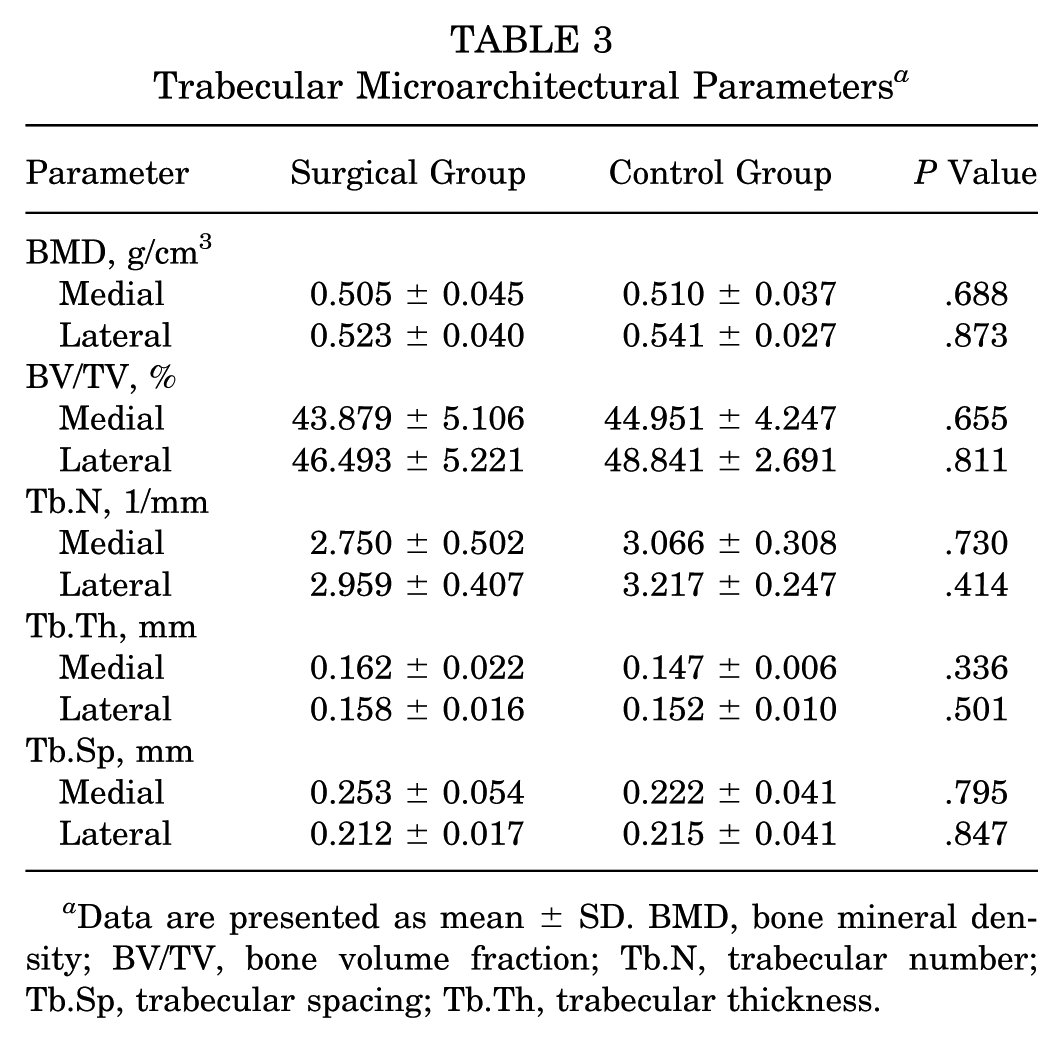
Data are presented as mean ± SD. BMD, bone mineral density; BV/TV, bone volume fraction; Tb.N, trabecular number; Tb.Sp, trabecular spacing; Tb.Th, trabecular thickness.
Discussion
The most important finding of this study was the establishment of a novel trochlear dysplasia animal model in immature rats via targeted injury of the anterior distal femoral epiphysis, which exhibited growth arrest at the anterior distal femoral epiphysis and key pathological features consistent with those seen in human trochlear dysplasia.
This model could serve as a reliable platform for investigating the dynamic temporal course of trochlear dysplasia progression, evaluating the safety and efficacy of potential therapeutic treatments, and exploring whether trochlear dysplasia could be reversed or alleviated when interventions are administered during the period of open epiphyseal plates.
The morphology of the trochlea is critical for maintaining normal patellofemoral function. However, a consensus has not yet been reached regarding the specific origin and pathogenesis of trochlear dysplasia. One hypothesis emphasizes a genetic predisposition, supported by the observation that the trochlear groove morphology is initially established during the embryonic stage, and the dysplastic phenotype does not undergo significant age-related changes in affected individuals.1,17 In contrast, another view supports a mechanically driven mechanism based on the fact that in patients with skeletal immaturity with untreated patellar dislocation, trochlear dysplasia deteriorates progressively with age, whereas the trochlea develops normally in healthy children, 15 suggesting that abnormal patellofemoral mechanical stress induced by patellar dislocation may disrupt trochlear development and contribute to dysplasia. These competing hypotheses underscore the urgent need for animal models that recapitulate the developmental origin of trochlear dysplasia, as opposed to merely simulating secondary mechanical perturbations.
It is clinically valuable to develop a small animal model to unravel the pathophysiology of trochlear dysplasia. Existing models of trochlear dysplasia primarily rely on indirect intervention of the patellofemoral mechanical environment to induce trochlear dysplasia. For example, Huri et al 6 established a patellar dislocation model via release of medial soft tissue restraints, which subsequently induced trochlear dysplasia. Wang et al 23 optimized this approach by overlapping and suturing lateral soft tissues to stabilize the surgically dislocated patella, thus achieving sustained patellar dislocation, which is essential for inducing trochlear dysplasia. Yang et al 24 also induced trochlear dysplasia via patellectomy, which eliminated physiological mechanical loading on the trochlea. Kang et al 8 increased femoral anteversion through distal femoral internal rotation in immature rabbits, resulting in trochlear dysplasia with anterior proximal trochlear bump formation. Despite their demonstrated utility, these models fail to target the core anatomic structure that drives trochlear development, which hinders their ability for investigating fundamental pathogenic mechanisms and evaluating interventions targeting developmental defects.
The trochlear cartilage originates from the distal femoral epiphysis, 18 and the proliferation and differentiation of epiphyseal chondrocytes directly determine trochlear morphological development. Thus, this study tested whether injury of the anterior distal femoral epiphysis could induce trochlear dysplasia and successfully established a trochlear dysplasia model. This model exhibited growth arrest at the anterior distal femoral epiphysis and 4 distinct types of trochlear dysplastic manifestations that reflect the pathological heterogeneity of human trochlear dysplasia: (A) mild trochlear dysplasia with a shallow, flat trochlear groove; (B) trochlear dysplasia with dysplasia of the lateral femoral condyle; (C) trochlear dysplasia with a bump deformity at the entrance of the trochlea; and (D) severe trochlear dysplasia with the presence of osteoarthritis. These diverse manifestations collectively reflect the pathological process of impaired chondrocyte proliferation and differentiation within the epiphysis after injury, and their consistency with human trochlear dysplasia subtypes validates the clinical relevance of this model. All 4 subtypes of trochlear dysplasia in the model exhibited core structural defects. Morphological abnormalities of each subtype (shallow trochlear groove, dysplasia of the lateral femoral condyle, and trochlear bump) directly impair the ability of the trochlea to stabilize the patella, thereby contributing to patellar instability. This aligns fully with clinical evidence indicating that trochlear structural defects are the primary risk factor for patellar instability. Additionally, this model uses rats, a widely available small animal with well-characterized skeletal development, which offered practical advantages over large animal models, including a shorter life cycle and lower costs.
This study analyzed trabecular microarchitectural parameters of the distal femoral epiphysis, but no significant differences were observed between the surgical group and the control group. Three potential explanations may account for this observation. First, early microstructural perturbations caused by epiphyseal drilling may have been offset by compensatory remodeling during growth. Second, the injury was highly localized, which may not have been severe enough to disrupt the overall trabecular network of the epiphysis. Third, immature rats exhibit inherent regenerative capacity of the epiphyseal plate, which may have partially restored trabecular integrity. However, we cannot exclude the likelihood of differences in trabecular microarchitectural parameters during short-term follow-up before skeletal maturity. Future studies using multiple earlier time points before skeletal maturity could capture transient trabecular changes caused by epiphyseal injury, which are later hidden by physiological compensatory remodeling and thus undetectable when skeletal maturity is achieved.
The potential mechanisms by which injury of the anterior distal femoral epiphysis induces trochlear dysplasia are numerous. The distal femoral epiphysis serves as the primary site for chondrocyte proliferation and differentiation, 18 which directly drives the morphological development of the trochlea. Injury of the epiphysis may disrupt the orderly proliferation of chondrocytes and the deposition of extracellular matrix, and impair the normal formation of the trochlear groove, thereby leading to a flattened or dysplastic morphology. Additionally, the epiphysis is critical for transmitting and regulating mechanical signals within the patellofemoral joint.2,21 After epiphyseal injury, the ability to sense and respond to physiological mechanical stress may be compromised, which may alter stress distribution in the trochlear region. This abnormal stress environment could further inhibit the differentiation of chondrocytes into mature chondrocytes, and even induce abnormal remodeling of the subchondral bone. However, the exact mechanism underlying epiphyseal injury–induced trochlear dysplasia remains unclear, and future studies are required to explore the dynamic changes of chondrocyte activity, extracellular matrix composition, and key signal molecules at different time points after epiphyseal injury to clarify the exact mechanism of trochlear dysplasia.
Compared with existing models, this novel model offers several advantages. It directly targets the anterior distal femoral epiphysis, which is the primary origin of trochlear cartilage differentiation and osseous development. This design thereby simulates the clinical pathological process of trochlear dysplasia caused by epiphyseal developmental abnormalities, aligning more closely with the pathological essence of human disease. This model uses a minimally invasive surgical technique that is simple to perform, is repeatable and reliable, and enables rapid and stable induction of trochlear dysplasia with typical pathological abnormalities.
The clinical relevance of this animal model lies in its ability to provide an important platform for clinical research and translational application of trochlear dysplasia. First, it provides experimental evidence for the early development of trochlear deformities in children with epiphyseal injuries. Second, it highlights the need for surgeons to prioritize epiphyseal integrity when treating distal femoral injuries in children, thereby avoiding the induction of trochlear dysplasia due to inadequate epiphyseal protection. Third, it recapitulates trochlear dysplasia caused by epiphyseal dysfunction, making it suitable for evaluating the efficacy of therapeutic strategies targeting epiphyseal repair and remodeling.
Limitations
This study has several limitations. First, the rat model is not completely matched with the biomechanics and anatomy of the human patellofemoral joint. Second, rats were euthanized at 2 months of age, precluding the assessment of the dynamic progression of trochlear dysplasia during the development process. Third, this study did not conduct mechanism analysis at the tissue, cellular, and molecular levels; thus, it was impossible to explain the exact mechanism of trochlear dysplasia caused by epiphyseal injury. Fourth, this study did not record the load changes across the patellofemoral joint, limiting the biomechanical analysis of the model. Fifth, the patellar tracking was not assessed via imaging during the follow-up period, limiting a more comprehensive and precise validation of the causal relationship between trochlear dysplasia subtypes and patellar instability. Sixth, although there is currently no evidence that physeal injury is a common cause of trochlear dysplasia in children, the purpose of this study was to verify that epiphyseal dysplasia caused by targeted injury of the anterior distal femoral epiphysis induces trochlear dysplasia, which has a potential correlation with the clinical observation that children with trochlear dysplasia present with epiphyseal plate dysplasia.5,10 Finally, this model mainly focuses on isolated trochlear structural defects induced by epiphyseal injury, without replicating other anatomic risk factors that contribute to lateral force vectors acting on the patella in human trochlear dysplasia. Future research should focus on analyzing the biological mechanism of trochlear dysplasia, especially the abnormal changes of the epiphysis, to provide novel targets for early interventions for patellar cartilage disease and instability. Additionally, more multifactorial risk factors should be incorporated to better reflect the clinical complexity of trochlear dysplasia and patellar instability.
Conclusion
A novel trochlear dysplasia animal model was established in immature rats via targeted injury of the anterior distal femoral epiphysis.
Footnotes
Submitted October 30, 2025; accepted January 24, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by the Postdoctoral Fund of Hebei Medical University, Government Training Project for Clinical Medical Talents of Hebei Province (ZF2023094), and Strong Foundation Project of Hebei Medical University Third Hospital (ydsyqjjh202510). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.