
Abstract
Background:
Current frozen shoulder (FS) therapies present a clinical dilemma: although intra-articular corticosteroids with home exercise provide proven medium-term (3-month) benefits, they lack short-term (<4-week) efficacy for rapid recovery; conversely, manipulative treatments achieve faster outcomes but carry invasiveness risks. These limitations highlight the urgent need for developing and validating novel noninvasive approaches with prompt therapeutic effects.
Purpose:
To compare the efficacy and safety of ultrasound-guided tendon surface (UGTS) injection versus manipulation under local anesthesia (MULA) and blind tender point (BTP) injection, all combined with intra-articular injection and home exercise.
Study Design:
Randomized controlled trial; Level of evidence, 1.
Methods:
The authors first developed a novel ultrasound-based strategy, which they named “ultrasound-guided tendon surface.” Then they conducted a multicenter randomized controlled trial (2019-2022). The primary outcome was 4-week shoulder function assessed by the Beijing Friendship Hospital Scale (BFHS), a modified version of the Constant-Murley Score adapted for Chinese populations with demonstrated validity. Secondary outcomes included (1) short-term (1-month) pain (visual analog scale [VAS]) score, active range of motion (ROM), Evaluation Scale of the Shoulder under Ultrasound (ESSU) score, pain relief, treatment sessions, and cartilage thickness; and (2) long-term (2-year) complete remission rates (tele-follow-up).
Results:
Among 365 screened patients, 139 were enrolled and randomized to receive UGTS (n = 49), MULA (n = 43), and BTP (n = 47). At the 1-week follow-up visit, the UGTS group showed rapid improvement in BFHS scores compared to both the MULA and BTP groups. These early functional advantages were also indicated by the VAS score, ROM, ESSU score, and pain relief. UGTS achieved faster complete remission (1 month: 59.2% vs 31.0% and 34.9% for BTP and MULA, respectively; 3-month: 79.6% vs 53.2% and 69.8% for BTP and MULA, respectively; P < .05), with remission rates converging by 24 months (P = .216), yet retained early rapid response as its key clinical advantage. UGTS showed no significant impact on articular cartilage thickness. Serial ultrasound monitoring demonstrated no rotator cuff injuries attributable to either the UGTS procedure or prescribed exercises.
Conclusion:
UGTS combined with intra-articular injection and exercise promotes faster recovery without safety concerns, representing an effective noninvasive first-line option for rapid relief in FS.
Registration:
ChiCTR1900025874 (Chinese Clinical Trial Registry number).
Keywords
Adhesive capsulitis, commonly referred to as frozen shoulder (FS), which occurs in about 2% to 5% of the general population, is characterized by pain and reduced active and passive range of motion (ROM).4,24 Without treatment, symptoms may persist for 2 to 3 years or extend beyond 10 years in some cases.3,12,26 Current clinical guidelines and systematic reviews recommend nonoperative management (including physical therapy and intra-articular corticosteroid injections) as first-line treatment for FS, resulting in medium-term pain relief and ROM improvement. However, this approach shows limited efficacy in achieving short-term remission, resulting in substantial suffering and significant impairment in quality of life of patients with FS.1,4,9 Consequently, there is a pressing need to develop rapid interventions to address this unmet clinical need in FS management.
In recent years, the most representative conventional therapies widely used in clinical practice have included blind tender point (BTP) injection and manipulation under anesthesia (MUA). BTP involves identifying periarticular tender points through physical examination and administering corticosteroid injections into the corresponding soft tissue areas.8,11 However, this approach remains limited in early improvement of shoulder ROM and pain relief. 8 Although MUA can rapidly restore joint mobility through manual MUA, it is associated with a high risk of postoperative pain recurrence and potential rotator cuff injuries, limiting its widespread clinical adoption.21,23,25 These limitations highlight the urgent need to develop faster, safer, and more effective treatment paradigms.
Driven by technological progress, arthroscopy identifies the articular capsule and rotator interval as primary pathological structures. 20 Unfortunately, clinical evidence shows no added benefit of combined rotator interval and articular injections versus articular injections alone. 22 Importantly, emerging data implicate periarticular tendons and ligaments in pain and adhesion pathogenesis in the early and middle stages of the FS. 7 These findings suggest that intervention strategies targeting tendon surface injections may represent a promising direction for addressing the slow onset of therapeutic effects in FS. However, the current lack of standardized protocols for such treatments, coupled with the absence of clinical trials validating the short-term efficacy of tendon surface injections, significantly hinders the development and application of novel therapeutic approaches.
Here, we developed the ultrasound-guided tendon surface (UGTS) technique, combining intra-articular corticosteroid injections and home exercise. Besides, we conducted a multicenter randomized controlled trial to compare the effects of UGTS injection, MUA, and BTP injection on early symptom improvement in patients with FS. Long-term outcomes were assessed via telephone follow-up, through which we compared remission rates across the 3 treatment groups at multiple time points.
Methods
Trial Design
This multicenter randomized clinical trial was approved by the institutional review board of the participating academic medical center (Approval Nos. KY2020172 and KY2025100). Conducted between September 2019 and September 2022 (screening: September 2019–September 2020; follow-up: until September 2022), the study obtained written informed consent from all participants before enrollment. No changes to the eligibility criteria were made after the commencement of the trial. Randomization of patients was carried out via a Microsoft Excel-generated randomization sequence (2clinllll019 MSO) by an independent researcher (D.Z., Y.O., Y.L., W.G.). Participants were randomly assigned with stratification by study center, using a block randomization approach with sequential numbering. The sequence was concealed from investigators until after eligibility confirmation. A detailed study flowchart is depicted in Figure 1. To minimize intercenter variability, (1) all centers followed standardized protocols for treatment, patient selection, and outcome assessment; and (2) site investigators received centralized training before study initiation.
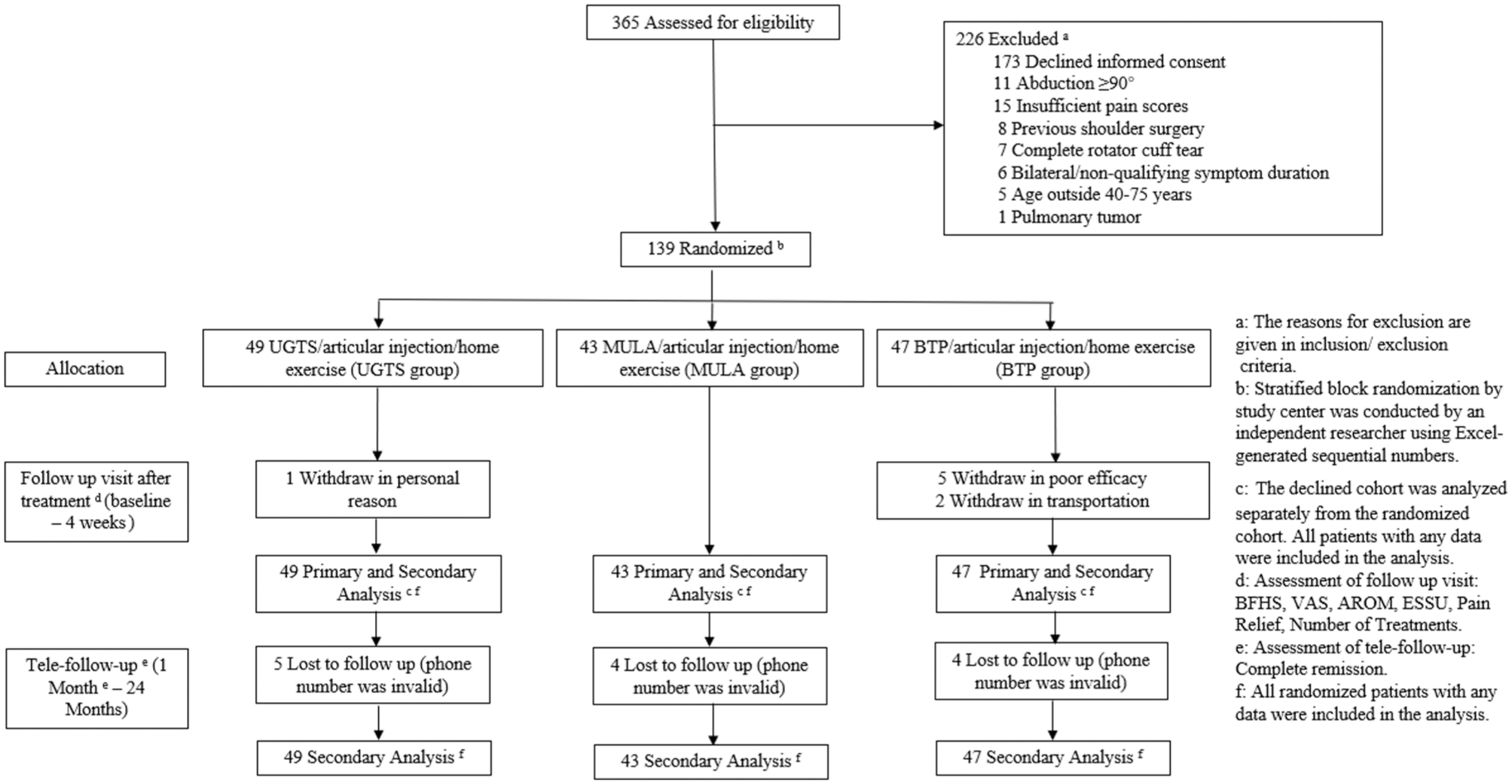
Flowchart of study population. AROM, active range of motion; BFHS, Beijing Friendship Hospital Scale; BTP, blind tender point; ESSU, Evaluation Scale of the Shoulder under Ultrasound; MULA, manipulation under local anesthesia; UGTS, ultrasound-guided tendon surface; VAS, visual analog scale.
Patient Selection
This multicenter study was conducted across 3 academic medical centers. Voluntary participants were enrolled with the right to withdraw at any time. According to the clinical diagnosis and assessment of FS,4,17,19,27 eligible patients were those who met the following key inclusion criteria: (1) abduction <90° (goniometer measured), (2) resting VAS score >3 or movement-induced VAS score >6, (3) unilateral symptom duration of 1 to 12 months, and (4) age 40 to 75 years. Patients were excluded if they met any of the following criteria: (1) any pathologies such as complete rotator cuff tear, fracture/dislocation history, and previous shoulder surgery (as determined by diagnostic ultrasonography and plain shoulder radiographic imaging); (2) coagulation disorders; (3) active infection/malignancy; (4) pregnancy; (5) corticosteroid allergy or use within 3 months; (6) local anesthetic hypersensitivity; or (7) declined informed consent.
Interventions
Manipulation Under Local Anesthesia Protocol
Ultrasound-guided brachial plexus block (C5-7) was performed using 10 mL of 2% lidocaine (He Bei Tian Cheng) + 1 mL of 1% ropivacaine (AstraZeneca) + 9 mL of normal saline, followed by intra-articular injection (2 mL of 2% lidocaine + 0.5 mL of betamethasone [MSD] + 2.5 mL of hyaluronic acid [SEIKAGAKU Corporation]) under ultrasound confirmation. Shoulder manipulation was repeated twice at 5-minute intervals (Appendix Figure A1, available in the online version of this article). Postprocedure care included 6 hours of immobilization with ice application and optional tramadol (100 mg intramuscularly) for VAS pain score >6.
UGTS Protocol
The injection sites were personalized based on a 2-step diagnostic reasoning process focused on identifying painful tendon restrictions. First, a clinical shoulder ROM assessment was performed to identify tendons that were likely adherent or contracted. This was inferred from the pattern of pain provoked by passive stretching during specific movements. For example, pain during passive external rotation suggested possible involvement of the subscapularis tendon (which is stretched in this motion). Pain during passive abduction raised the possibility of supraspinatus tendon involvement. Pain during passive posterior elevation or horizontal adduction suggested potential involvement of the infraspinatus and teres minor tendons. Subsequently, a targeted musculoskeletal ultrasound examination was conducted to objectively evaluate the integrity of the rotator cuff tendons and the long head of the biceps tendon. Pretreatment physical examination and ultrasonography identified ≤4 target sites for ultrasound-guided injections (5 mL/site, 20 mL total of the same formulation used in the manipulation under local anesthesia [MULA] and BTP groups), followed by standard anterior intra-articular injection under ultrasound guidance (Appendix Figure A2, available online).
BTP Protocol
Standardized palpation of predefined tender points (levator scapulae, supraspinatus muscle, infraspinatus muscle, quadrangular space, subacromial bursa, deltoid muscle, bicipital groove, and coracoid process) was performed in a systematic clockwise direction. In terms of pain severity, ≤4 sites received blinded injections, followed by ultrasound-guided anterior intra-articular injection via medication protocols identical to those used in the UGTS group.
Postprocedural Care and Home Exercise Protocol
The standardized postprocedural care for all patients consisted of 2 components: (1) a prescribed home exercise regimen and (2) scheduled clinical follow-ups. The home exercise consisted of therapeutic wall climbing (Appendix Figure A3, available online), to be performed for 15 minutes per session, 3 times daily, with instruction to avoid strenuous activity. This exercise was initiated after each treatment session. Once the functional recovery endpoint was attained (active abduction >120° and resting VAS score <3),4,6 patients were instructed to continue the daily wall climbing exercise for an additional 1 month to maintain gains and prevent readhesion. Adherence was reviewed during the comprehensive follow-up visits at 1 week and 4 weeks, which included evaluation of shoulder function (BFHS score), active ROM (AROM), pain (VAS score), and ultrasonography.
Patients underwent mandatory 15-minute in-hospital monitoring for acute complications (eg, bleeding, vasovagal reactions), with late adverse events (rotator cuff swelling and tears) assessed via ultrasound at short-term follow-up visits. All participants received tele-follow-ups at 1, 3, 6, 12, and 24 months.
Sample Size and Statistical Power
Sample Size Estimation
The initial sample size was calculated to detect a 20% absolute difference in efficacy rates (80% for UGTS vs 60% for control groups) with 80% power at an α of .05 (2-tailed), using a chi-square test for 3 proportions in OpenEpi. Accounting for a 10% dropout rate, this yielded a requirement of 92 patients per group (276 total). The 1:1:1 randomization scheme was implemented after approval by the ethics committee.
Interim Analysis and Early Termination
The interim analysis of the first 139 enrolled patients (50.4% of target) demonstrated markedly higher efficacy in the UGTS group (93.9%; 46/49) compared to the MULA (62.7%; 32/51; P < .001) and BTP (53.2%; 25/47; P < .001) groups, with absolute differences of 30.3% and 39.8%, respectively (Appendix Table A2, available online). Post hoc power analysis (G*Power) confirmed >99.99% power for these comparisons at an α of .05 (effect size w = 0.41). After review by the ethics committee and confirmation of statistical sufficiency, the study was completed early with follow-up of enrolled participants.
Outcome Evaluation
The primary outcome measure was the Beijing Friendship Hospital Scale (BFHS) score, 13 a validated assessment tool adapted from the Constant-Murley Score with 2 distinct modifications: (1) incorporation of shoulder morphological evaluation and (2) culturally adapted functional items specific to Chinese daily activities. The validation study 13 reported high reliability coefficients across all BFHS subscales: interrater reliability (λ1) (mean, 0.83; 95% CI, 0.76-0.90) and test-retest reliability (λ2) (mean, 0.84; 95% CI, 0.76-0.92). Both λ1 and λ2 coefficients range from 0 to 1, with higher values indicating better reliability. Compared with the American Shoulder and Elbow Surgeons Standardized Shoulder Assessment Form score, the BFHS score demonstrates superior cultural adaptation for Chinese patients, incorporating both subjective (pain, daily activities) and objective (muscle strength, ROM, morphology) assessments across 5 domains (see Appendix for detailed scale criteria). Trained evaluators (D.Z., W.G., Y.O.) administered the BFHS at baseline and 1-week and 4-week posttreatment intervals.
The secondary outcome measures included the following: (1) visual analog scale (VAS) score, (2) AROM, (3) Evaluation Scale of the Shoulder under Ultrasound (ESSU) score, and (4) pain relief. (5) Additionally, telephone follow-ups were conducted at 1, 3, 6, 12, and 24 months posttreatment to assess whether the affected shoulder had achieved complete remission. The detailed assessment criteria are provided in the Appendix (available online).
Adverse effects including palpitation, VAS score >6 points within 24 hours after treatment, tramadol injection within 24 hours after treatment, dizziness, nausea, and swelling and tearing of the rotator cuff were evaluated. To evaluate the impact of UGTS and BTP on articular cartilage, we conducted measurements of articular cartilage thickness at pretreatment (baseline) and posttreatment (1 week). Ultrasound assessments were performed using clinical ultrasound systems (SonoScape S9, TUORen 100, and Huasheng Navii) equipped with a standardized high-frequency linear array transducer (9.5-15 MHz). B-mode (grayscale) imaging was used for primary anatomic measurement of cartilage thickness and tendon morphology. Color Doppler imaging was applied adjunctively to assess synovial and peritendinous vascularity.
Statistical Analysis
Statistical analysis was performed using IBM SPSS Version 23.0, with a significance threshold set at a P value <.05. Continuous variables (age, symptom duration, weight, height, and BMI) are expressed as mean ± SD. Parametric tests (analysis of variance [ANOVA]) were applied as they are robust to mild nonnormality with adequate sample sizes; nonparametric alternatives were used for severely skewed distributions (Shapiro-Wilk P < .01). When the Levene test indicated heteroscedasticity (P < .05), Welch ANOVA with Games-Howell post hoc tests was used. Intergroup comparisons were performed via 1-way ANOVA (or the Kruskal-Wallis rank-sum test for nonparametric data) with Bonferroni post hoc correction. Categorical variables such as gender, affected side, degree of pain relief (>50%), and probability of complete remission were summarized using frequencies and percentages. The Pearson chi-square test was applied for categorical variables with all expected frequencies ≥5; otherwise, the Fisher exact test was used. In cases in which sample sizes were small, such as degree of pain relief (>50%), probability of complete remission, diabetes, a history of trauma, and adverse effects, the Fisher exact test was applied to ensure a more robust analysis. Longitudinal comparisons used repeated-measures ANOVA with Greenhouse-Geisser correction where sphericity (Mauchly test) was violated. All post hoc tests applied Bonferroni correction, with sensitivity analyses including analysis of covariance and bootstrap resampling. Missing data were primarily addressed via multiple imputation (missing at random), with worst-case imputation (missing not at random) used to evaluate robustness. Effect size (φ) with 95% CI is reported for significant findings.
Results
Participant Characteristics
A total of 139 patients with FS were randomized into 3 treatment groups: UGTS (n = 49), MULA (n = 43), and BTP (n = 47). No significant differences were observed among the groups at baseline regarding gender, age, symptom duration, diabetes history, history of trauma, affected side, body mass index (BMI), weight, or height (all P > .05) (Table 1).
Characteristics of Participants in the UGTS, MULA, and BTP Groups a
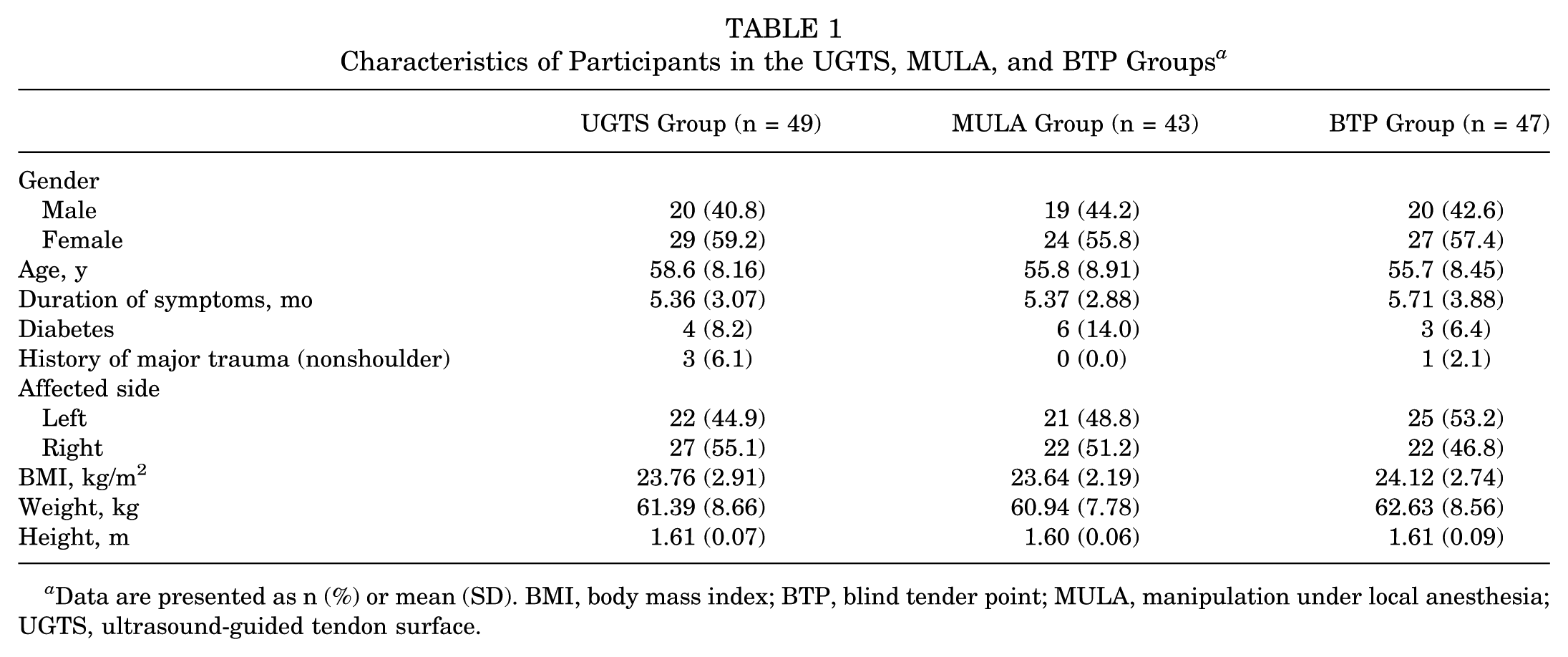
Data are presented as n (%) or mean (SD). BMI, body mass index; BTP, blind tender point; MULA, manipulation under local anesthesia; UGTS, ultrasound-guided tendon surface.
Primary Outcome
The primary outcome, shoulder function assessed by the BFHS, showed no significant between-group differences at baseline (P > .05). At the 1-week follow-up, the UGTS group demonstrated significantly greater improvement in BFHS scores compared to both the MULA group (mean difference [MD], 5.99; 95% CI, 2.98-9.00; P < .001) (Figure 2) and the BTP group (MD, 8.08; 95% CI, 5.14-11.02; P < .001) (Figure 2). This significant advantage persisted at the 4-week follow-up (UGTS vs MULA: MD, 7.64; 95% CI, 4.36-10.91; P < .001; UGTS vs BTP: MD, 7.85; 95% CI, 4.65; 11.05; P < .001) (Figure 2, Appendix Table A1, available online). The mean change from baseline for each group is shown in Figure 2. We also calculated the treatment effectiveness (BFHS score ≥80 was defined as treatment effectiveness) at week 4. The results indicated that the UGTS group showed significantly higher effectiveness than the MULA and BTP groups at week 4 (χ2 = 23.87; P < .001) (Appendix Table A2, available online). No significant differences were found between the MULA and BTP groups at either time point. Furthermore, a post hoc analysis stratifying patients by baseline abduction severity (median baseline/cutoff: 73°) (Appendix Table A4, available online) revealed that the treatment benefit of UGTS remained robust across severity subgroups (UGTS >73° vs UGTS ≤73°; P > .05), while the efficacy of both MULA and BTP was significantly lower in patients with more severe limitations.
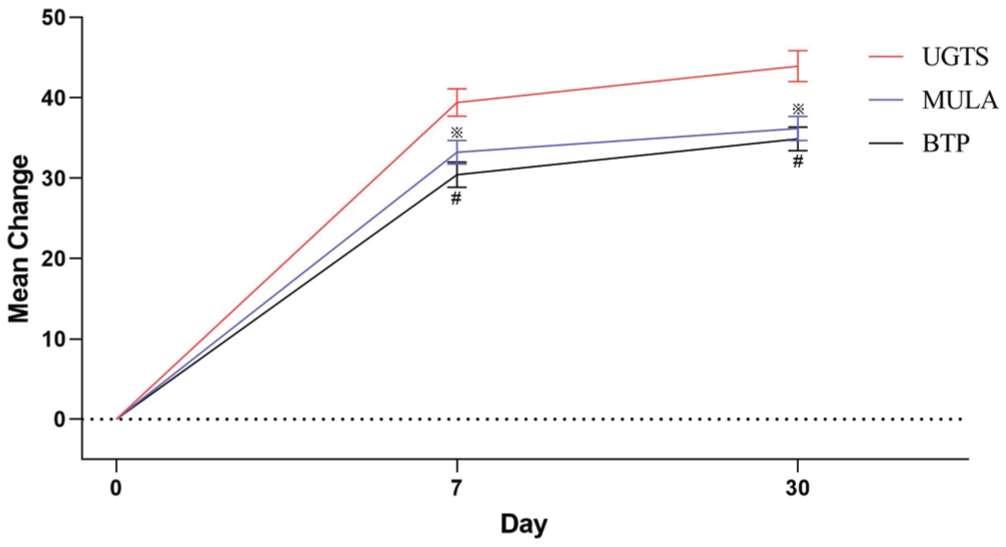
Primary outcome. Change from baseline in Beijing Friendship Hospital Scale (BFHS) scores (range, 0-100; higher scores = better function) at posttreatment intervals. The validated scale integrates subjective domains (pain, daily activities) and objective measures (strength, range of motion, morphology). Bars represent standard error. ※UGTS versus MULA: week 1 P < .001, week 4 P < .001; #UGTS versus BTP: week 4 P < .001.
Secondary Outcomes
All groups were balanced at baseline for VAS scores, AROM, and ESSU scores (P > .05). At the 1-week follow-up, the UGTS group had significantly lower VAS scores than both the MULA (MD, –0.50; 95% CI, –0.87 to −0.12; P = .01) and BTP (MD, –0.40; 95% CI, –0.77 to −0.03; P = .033) groups, with superior pain relief maintained at 4 weeks (both P < .001). The UGTS group also showed significantly greater improvements in AROM at 4 weeks, particularly in abduction, external rotation, and posterior elevation, compared to both control groups (all P < .05). Additionally, the UGTS group exhibited significantly greater reductions in ESSU scores at 4 weeks compared to both the MULA (MD, –1.78; 95% CI, –3.09 to −0.47; P = .008) and BTP (MD, –2.11; 95% CI, –3.39 to −0.83; P = .001) groups, indicating better ultrasound-evaluated shoulder recovery. The UGTS group also demonstrated significantly higher rates of >50% pain relief at both week 1 (χ2 = 12.5; P = .002) and week 4 (χ2 = 15.21; P = .005) compared to the other groups (Tables 2 and 3, Appendix Table A1, available online).
Secondary Outcomes a
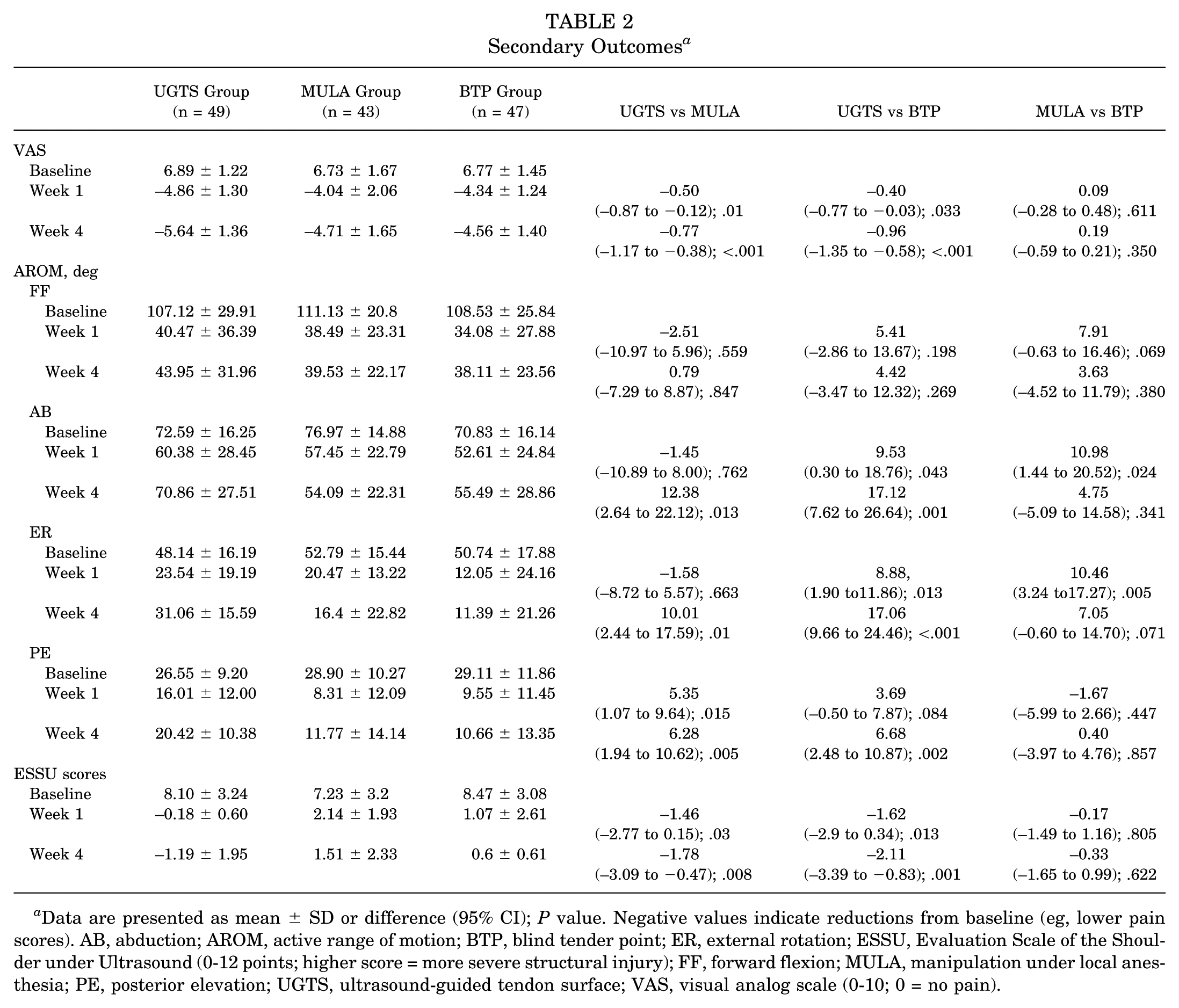
Data are presented as mean ± SD or difference (95% CI); P value. Negative values indicate reductions from baseline (eg, lower pain scores). AB, abduction; AROM, active range of motion; BTP, blind tender point; ER, external rotation; ESSU, Evaluation Scale of the Shoulder under Ultrasound (0-12 points; higher score = more severe structural injury); FF, forward flexion; MULA, manipulation under local anesthesia; PE, posterior elevation; UGTS, ultrasound-guided tendon surface; VAS, visual analog scale (0-10; 0 = no pain).
Pain Relief Rates (>50%) in Frozen Shoulder Patients: Baseline vs Posttreatment Weeks 1 and 4 a
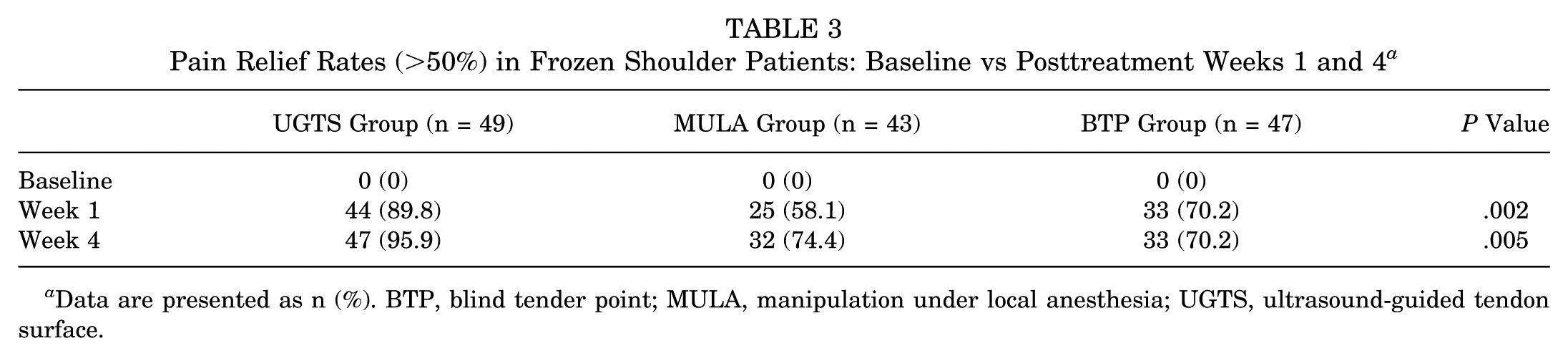
Data are presented as n (%). BTP, blind tender point; MULA, manipulation under local anesthesia; UGTS, ultrasound-guided tendon surface.
Remission Rates Through 2-Year Follow-up
Telephone follow-ups over 24 months revealed significantly higher complete remission rates in the UGTS group compared to the MULA and BTP groups at the 1-month (59.2% vs 34.9% and 31.9%, respectively; P = .013) and 3-month (79.6% vs 69.8% and 53.2%, respectively; P = .021) assessments. No significant intergroup differences were observed at the 6-, 12-, or 24-month follow-ups (Table 4).
Complete Shoulder Remission Rates Through 2-Year Telephone Follow-up a
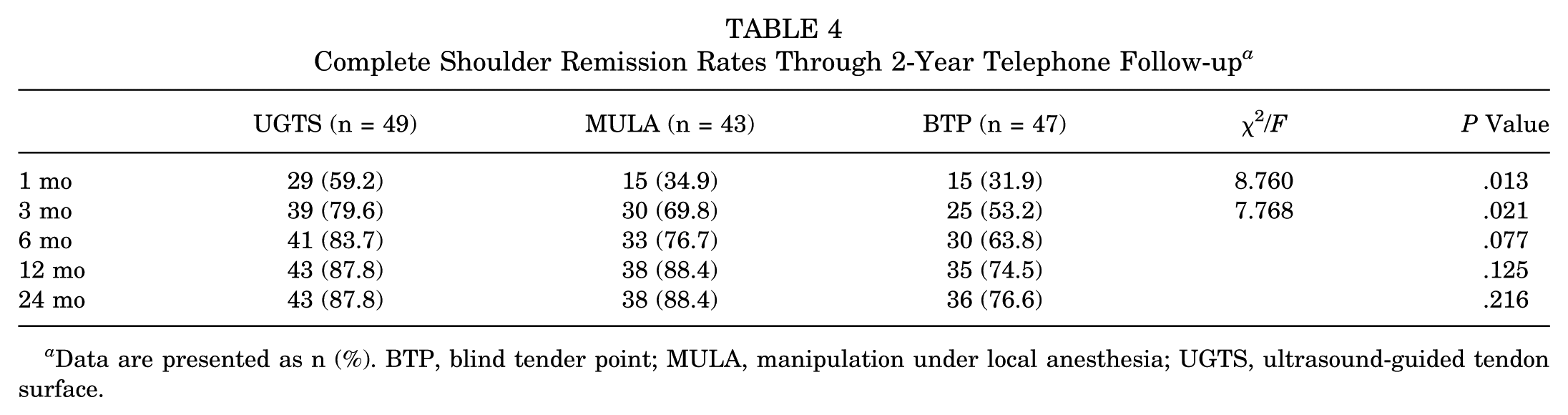
Data are presented as n (%). BTP, blind tender point; MULA, manipulation under local anesthesia; UGTS, ultrasound-guided tendon surface.
Adverse Effects
Transient palpitations or dizziness occurred in 1 (2.0%) patient in the UGTS group and 3 (6.4%) patients in the BTP group (with 1 BTP patient also reporting nausea). Within 24 hours posttreatment, 25 (58.1%) patients in the MULA group required rescue tramadol injections for severe pain (VAS score >6), whereas no patients in the UGTS or BTP groups required such intervention (P < .001). Ultrasound at 4 weeks revealed rotator cuff tears or swelling in 24 (55.8%) patients in the MULA group compared to 6 (12.8%) in the BTP group, while no UGTS-related rotator cuff injuries were observed (P < .001) (Table 5). Additionally, articular cartilage thickness remained stable at week 1 across all groups, with no significant differences detected among the 3 treatments at this early time point. This observation shows no acute detrimental effect of UGTS on cartilage thickness within 1 week (Appendix Table A3, available online).
Adverse Effects a
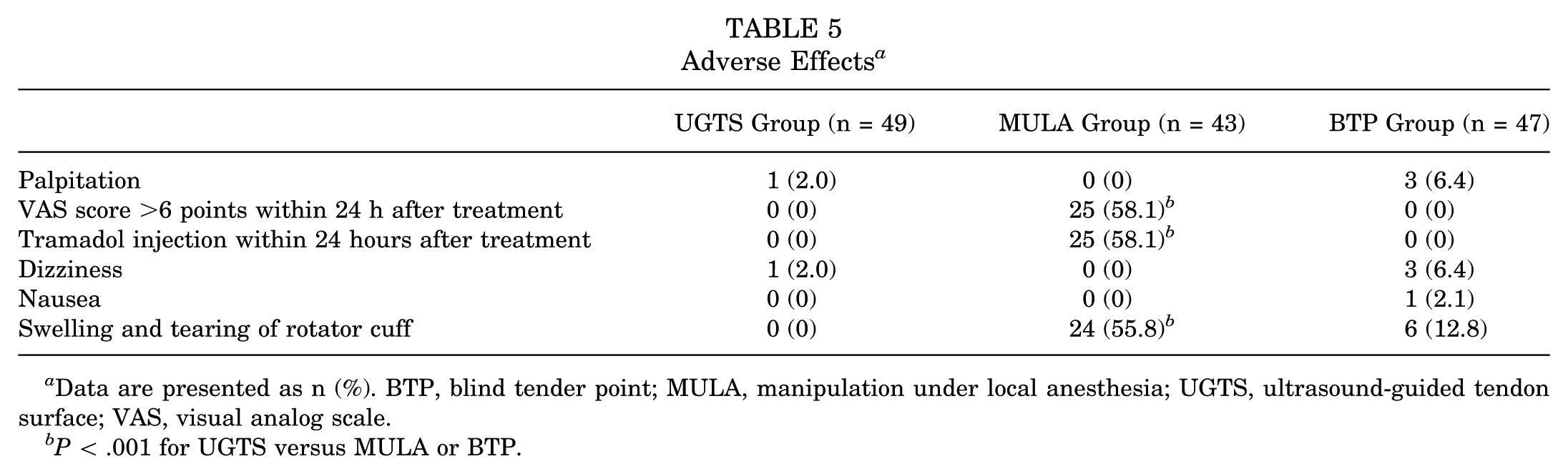
Data are presented as n (%). BTP, blind tender point; MULA, manipulation under local anesthesia; UGTS, ultrasound-guided tendon surface; VAS, visual analog scale.
P < .001 for UGTS versus MULA or BTP.
Discussion
This randomized trial compared UGTS, MULA, and BTP interventions for patients with FS. Although all these interventions demonstrated efficacy in improving shoulder function and reducing pain compared to baseline assessments, only UGTS showed superior short-term effects. UGTS induced significantly greater improvements across all primary and secondary outcomes, including the BFHS score, VAS score, pain relief, AROM, and EUSS score. Notably, participants in the UGTS group experienced fewer unwanted side effects than participants in the BTP and MUA groups. In addition, ultrasound visualization confirmed that weekly articular cavity injections in the UGTS group had fewer effects on the cartilage.
A major challenge in FS management is the slow onset of therapeutic effects.4,9 Conventional approaches such as BTP and MULA each have inherent limitations: BTP is often imprecise and yields suboptimal short-term relief,8,25 while MULA, although faster, carries risks of invasiveness and complications such as rotator cuff injury.15,25 Our novel UGTS strategy, which combines ultrasound-guided peritendinous corticosteroid injection with standardized intra-articular administration and home-based exercise,10,16 not only facilitates more rapid symptom alleviation but also demonstrates higher efficacy and a favorable safety profile. Therefore, the UGTS approach offers a promising new intervention for achieving faster functional recovery in patients with FS.
The superior short-term efficacy of UGTS over BTP may be attributed to its precise, pathophysiology-targeted approach. While both are multisite injections, UGTS uses a systematic protocol: physical examination first localizes the “responsible tendons” based on stretch-provoked pain patterns, which is then confirmed by ultrasound-identifying objective tendinous pathology. The injectate is thus delivered precisely to the tendon surface, the site of fibroblast-mediated adhesion formation in FS. 18 In contrast, BTP injections are based on tender points and delivered into the muscular tissue, which may not optimally target the peritendinous adhesive pathology. This mechanistic distinction likely underlies the observed clinical difference.
Accumulating evidence suggests that tendon surface injections hold distinct advantages over conventional intramuscular or intra-articular injections.11,14 These advantages are likely due to the targeted delivery of anti-inflammatory agents to sites rich in activated fibroblasts and inflammatory mediators, which play a pivotal role in the fibrotic process of FS.7,18,29 Our findings indicate that UGTS injection enables more efficient and effective intervention for FS. 5 This not only provides an improved treatment strategy but also underscores the broader potential of tendon surface injections in managing periarticular and soft tissue disorders.2,28 The success of UGTS in this context may pave the way for its application in other musculoskeletal conditions involving tendon and fascial pathology.
Despite the superior performance of UGTS in the primary outcome measure and most secondary outcomes, several critical limitations must be considered. The implementation of a double-blinded design was impractical due to the fundamentally different nature of the 3 procedures. To mitigate this potential bias, all physical examinations, ultrasonic diagnoses, and treatments at each center were performed by the same physician, ensuring a standardized evaluation process. While this trial incorporated a 2-year telephone follow-up to assess long-term remission, its primary focus remained on short-term efficacy. The long-term data, based on patient-reported functional outcomes (eg, pain-free movement, ability to perform daily activities), provide valuable insights into durability. However, the absence of structured long-term physical examination and ultrasonographic assessment means that we cannot objectively confirm the persistence of functional gains or definitively rule out delayed cartilage changes. Therefore, future studies incorporating scheduled long-term clinical and imaging evaluations are warranted to corroborate our patient-reported findings and comprehensively assess safety. Furthermore, our observation that >3 consecutive corticosteroid injections may lead to dose-dependent cartilage thinning underscores the need for cautious, long-term monitoring.
Conclusion
This randomized clinical trial revealed that UGTS injection combined with intra-articular corticosteroids and home exercise represents a clinically superior therapeutic strategy for treating FSs compared with manipulative or blind injection approaches. The intervention significantly accelerated functional recovery, reduced procedural requirements, and yielded favorable safety outcomes while preserving joint integrity, positioning it as an optimal first-line treatment option for this condition.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465261427347 – Supplemental material for A Novel Ultrasound-Guided Injection Strategy for Rapid Functional Recovery in Frozen Shoulder: A Multicenter Randomized Trial
Supplemental material, sj-pdf-1-ajs-10.1177_03635465261427347 for A Novel Ultrasound-Guided Injection Strategy for Rapid Functional Recovery in Frozen Shoulder: A Multicenter Randomized Trial by Dan Zhu, Yunxia Ou, Yuping Li, Weiwei Gao, Zhenzhen Fan, Xiaona Zhu, Yaohua Chen, Li Tang, Min Wang, Jinmei Chen, Yin Cai, Guangchun Li, Wei Li, Jie Li, Xingyue Huo, Yuan Cheng and Jian Cui in The American Journal of Sports Medicine
Footnotes
Acknowledgements
The authors sincerely thank Dr. Xing Hua of the Department of Ultrasonography for his expert consultation on diagnosing our complex cases.
Submitted October 10, 2025; accepted February 6, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by the Chongqing Municipal Key Clinical Specialty Construction Project (CQZDZK001), the Chongqing Sanitation Appropriate Technology Promotion Project (2024jstg041), and the Military Medical Innovation Ability Improvement Program for Medical Personnel of the First Affiliated Hospital of Army Medical University (SWH 2019QNLC-08). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Data Accessibility Statement
The data sets supporting the results of the present study can be obtained from the corresponding author on reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.