
Abstract
Background:
Knotted suture bridge repair (KSB) has been widely demonstrated as an effective method for rotator cuff tears. However, it is associated with high retear rates, primarily attributed to medial row failure resulting from knot-induced stress concentration and compromised tendon perfusion. Knotless suture bridge repair (KLSB) has recently gained considerable attention as a promising alternative technique. Currently, no consensus exists regarding the necessity of medial row knot tying in suture bridge repair for rotator cuff tears. This study aimed to compare the histological and biomechanical outcomes between KLSB and KSB for rotator cuff repair.
Hypothesis/Purpose:
KLSB will yield superior histological tendon-to-bone healing as compared with KSB. The purpose was to compare the biomechanical and histological outcomes of KLSB and KSB for rotator cuff tears in a rabbit model.
Study Design:
Controlled laboratory study.
Methods:
Acute bilateral supraspinatus tears were created in the shoulders of 56 New Zealand White rabbits. KLSB and KSB procedures were randomly assigned to the left or right shoulder. Sixteen animals were euthanized at 2, 4, and 8 weeks postoperatively, with 8 rabbits allocated to histological evaluation and the remaining 8 to biomechanical testing. An additional 8 animals were utilized exclusively for initial biomechanical evaluation at week 0.
Results:
Macroscopic examination revealed secure reattachment of all repaired tendons to the footprint on the greater tuberosity, with no evident postoperative complications observed at 8 weeks. The KLSB group exhibited significantly enhanced histological tendon-to-bone integration as compared with the KSB group, particularly in fibrocartilage regeneration, collagen composition, and fiber organization at 4 and 8 weeks. Biomechanically, the KSB group demonstrated superior performance in ultimate load to failure and stiffness at 0, 2, and 4 weeks. By 8 weeks, however, no significant differences were detected between the groups.
Conclusion:
Both repair techniques are effective. KSB provides superior early biomechanical performance, whereas KLSB demonstrates distinct advantages in histological healing. Over time, the enhanced healing achieved with KLSB compensates for initial biomechanical deficits, ultimately matching the biomechanical performance of KSB.
Clinical Relevance:
This animal study suggested that KLSB could serve as an alternative option for treating rotator cuff tears in humans, with the possibility of enhancing tendon-to-bone healing. Further research is needed to confirm its applicability.
With the continuous advancement of arthroscopic instrumentation and repair concepts, arthroscopic rotator cuff repair techniques have evolved from single- to double-row repair and more recently to the suture bridge technique.28,31 Suture bridge repair has gained increasing popularity owing to its optimized biomechanical properties, including enhanced initial fixation strength, reduced gap formation, and improved footprint coverage.43,51,56 The traditional suture bridge repair construct combines medial horizontal mattress knotted sutures with a “bowtie”-like structure compressed against the footprint by lateral row anchors using the free sutures. 42
Previous investigations have proposed the promising hypothesis that restoring a larger anatomic surface area and stronger biomechanical properties through knotted suture bridge repair (KSB) would facilitate optimal biological tendon-to-bone healing.37,46 Nevertheless, recent studies have reported retear rates ranging from 10.9% to 23.4% for small to midlarge rotator cuff tears after KSB.3,19,29,30,49 Notably, medial row failures account for up to 80% of these retears. 10 It is widely acknowledged that rotator cuff retear represents a multifactorial outcome, influenced by factors including tendon quality, tear size, acromial morphology, and various patient-related or postoperative variables. Among these, excessive tension and strangulation at the medial tendon junction caused by knot tying are identified as key technical contributors to failure in the KSB approach. 9 Furthermore, knot tying in the medial row may compromise tendon perfusion and contribute to subacromial impingement, thereby impeding biological healing of the rotator cuff.53,58
Knotless suture bridge repair (KLSB) has recently attracted increased attention as an alternative to KSB.4,14,47 This technique reduces the risk of stress concentration and preserves tendon vascularization by eliminating medial row knot tying, while simultaneously mitigating knot-related impingement at the repair site, potentially promoting tendon-to-bone healing.24,60 However, several biomechanical investigators argued that KLSB may demonstrate inferior biomechanical properties as compared with KSB, which could affect tendon-to-bone healing and consequently yield significant clinical differences.32,39 Rhee et al 48 reported that the modified Mason-Allen KLSB enhanced with rip-stop significantly reduced the retear rate as compared with KSB, likely because of the rip-stop modification's ability to mitigate suture cut-through and tendon retraction. In contrast, Şahin et al 49 conducted a prospective study using conventional KLSB as in our study without rip-stop reinforcement, finding no significant differences in retear rates or clinical outcomes between KLSB and KSB.
To our knowledge, controversy persists regarding the clinical benefits of KLSB over KSB. Moreover, the interactive effects of reduced mechanical strength and enhanced biological healing factors on tendon-to-bone healing after KLSB remain incompletely understood. Currently, no animal studies have been conducted to compare biomechanical and histological outcomes between KLSB and KSB. This study aims to evaluate and compare the histological and biomechanical outcomes associated with KLSB versus KSB in a rabbit model of rotator cuff tears.
Methods
All animal care and experimental procedures were conducted in accordance with the guidelines of the National Animal Experiment Center and received approval from the Hospital Ethics Committee (2022-1124). Based on previous studies, a minimum of 6 rabbits per group was required for biomechanical testing to achieve statistical significance at the .05 level (α error = .05, β error = .2). 34 To further justify and validate this choice, we performed an independent a priori power analysis using the “paired t tests” module in PASS 2023 software. The power calculation was based on the primary and clinically most relevant outcome: load to failure at 12 weeks. The analysis indicated that 5 animals per group were required to detect a clinically meaningful difference. To ensure adequate power and account for potential variability or attrition in the study, 8 New Zealand White rabbits were assigned to each experimental group for the biomechanical testing component. Shoulder joint samples were collected at 0, 2, 4, and 8 weeks postsurgery. For the histological analysis, a separate cohort of 8 New Zealand White rabbits was designated for each group, with shoulder joint samples collected at 2, 4, and 8 weeks postoperation. In total, 56 New Zealand White rabbits were utilized throughout the experiment.
Animal Model Setup
Before surgery, a 1-week observation period was conducted to ensure that all rabbits were healthy and disease-free. We utilized 56 male New Zealand White rabbits, approximately 25 weeks old with a mean weight between 3.5 and 4 kg. Bilateral shoulder joints were employed for the study. All rabbits received prophylactic intramuscular administration of 400,000 U of penicillin G to prevent infection. All surgical procedures were performed by the same experienced surgeon (J.G.) under sterile conditions. The experiment employed a simple randomization method to allocate the bilateral procedures for each rabbit. Each rabbit served as a unit, with a random number between 0 and 1 generated via Excel's =RAND() function. If the random number was ≤0.5, the left shoulder underwent KLSB and the right shoulder KSB (group result recorded as “1”); if the random number was >0.5, the right shoulder underwent KLSB and the left shoulder KSB (group result recorded as “2”). The entire randomization process was completed automatically in Excel to ensure that the allocation was unbiased.
Anesthesia was induced via intramuscular injection of pentobarbital at a dose of 30 mg/kg. The surgical area was shaved and prepared after standard aseptic protocols. After disinfection, animals were positioned laterally and draped with sterile covers. A 2% lidocaine hydrochloride solution was infiltrated into the planned skin incision to augment anesthesia and reduce postoperative pain. Shoulders were randomly assigned to receive either KLSB or KSB. A 3.0-cm longitudinal anterolateral incision was made, exposing the deltoid muscle, which was split along its fiber direction to reveal the supraspinatus muscle and its insertion area (Figure 1A). A crescent-shaped tear (8 × 5 mm) was created at the supraspinatus insertion on the greater tuberosity with a scalpel (Figure 1B). The greater tuberosity was then prepared with a grinding drill to promote healing, exposing a bleeding cancellous bone surface.
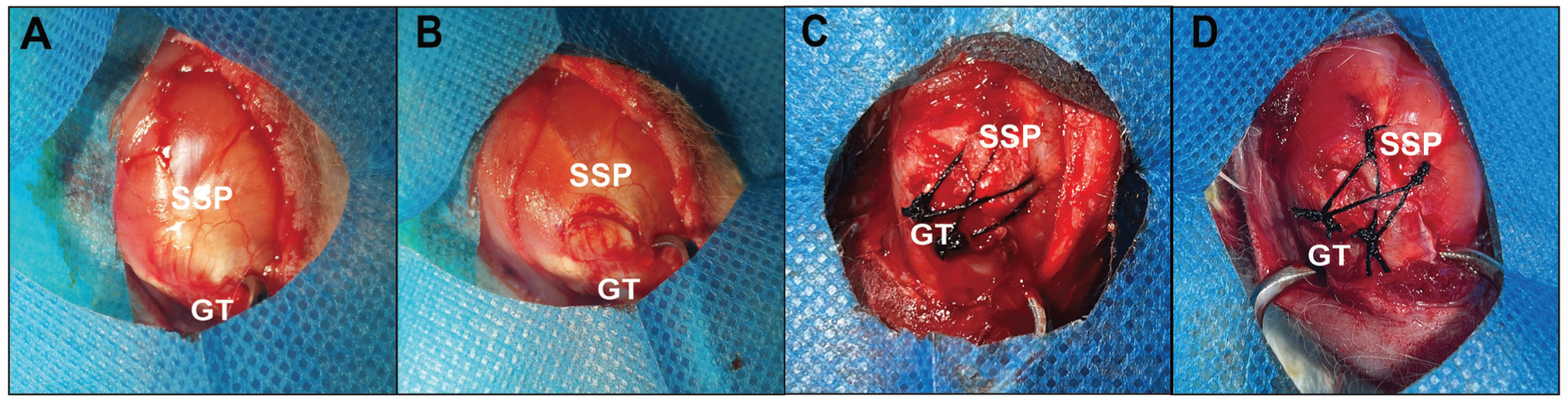
Surgical repair photographs for the torn supraspinatus tendon (SSP) to the greater tuberosity (GT) using the knotless suture bridge repair and knotted suture bridge repair in rabbits. (A) Observation of the intact tendon-to-bone insertion. (B) The crescent-shaped torn supraspinatus model. (C) The knotless suture bridge repair performed at the rabbit shoulder. (D) The knotted suture bridge repair performed at the rabbit shoulder.
Repair Groups: KLSB and KSB
For shoulders undergoing KLSB, 2 parallel bone tunnels were created 8 mm from the anterior and posterior aspects of the lateral greater tuberosity. Four 3-0 nylon sutures were passed through the torn tendon via these tunnels. Unlike KSB, the 2 sutures traversing the tendon were not tied as horizontal mattress knots at the medial row; instead, their free ends were retained and all suture limbs were tied near the bone tunnel openings to form a crossed suture bridge over the tendon (Figures 1C and 2A).
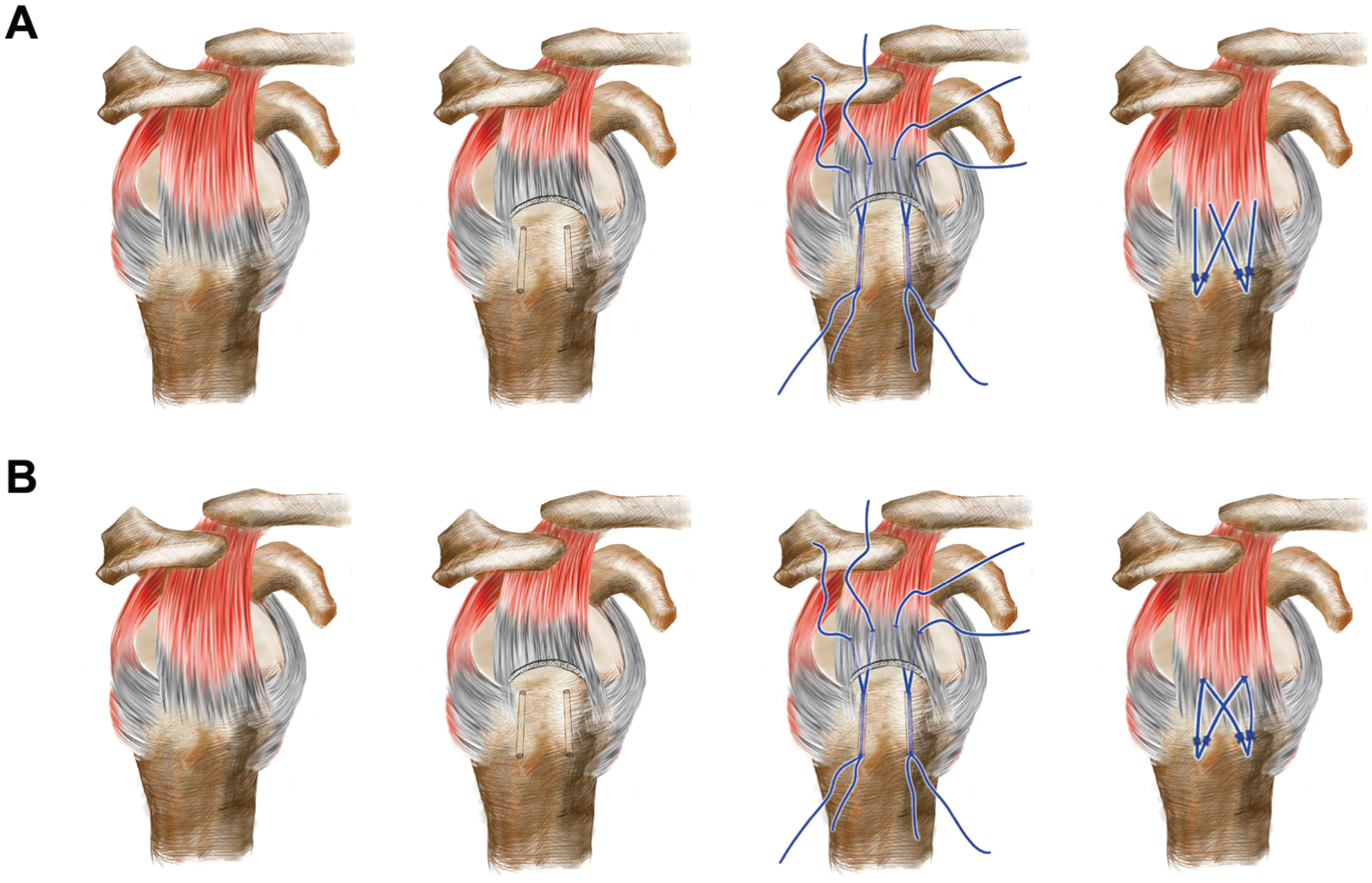
Surgical visualization of rotator cuff repairs: knotless vs knotted suture bridge. (A) Illustration of the knotless suture bridge repair. (B) Illustration of the knotted suture bridge repair.
For shoulders treated with KSB, 2 parallel bone tunnels were created 8 mm from the anterior and posterior aspects of the lateral greater tuberosity. Four 3-0 nylon sutures were passed through the torn tendon via these tunnels. Two sutures were passed through the tendon and tied as a horizontal mattress knot within the same tunnel. The suture limbs were then tied near the bone tunnel openings, creating a crossed suture bridge over the tendon (Figures 1D and 2B).
Animals were monitored until full recovery from anesthesia and resumption of feeding. Each rabbit was housed individually in separate cages. Closure of skin, deltoid muscle, fascia, and subcutaneous tissue was performed with interrupted nylon sutures. Postoperatively, 400,000 U of penicillin G was administered intramuscularly once daily for 3 days, and animals were permitted free shoulder movement.
Examination and Processing of Specimens After Harvest
Euthanasia was performed using an overdose of pentobarbital. Surgical sites were sampled, and all collected humeral heads, supraspinatus muscles, and scapulae underwent gross examination to assess healing status. Specimens for biomechanical evaluation were stored at −40°C, while those for histological evaluation were fixed in 4% paraformaldehyde.
Biomechanical Evaluation
Before being sent to the biomechanical laboratory, all specimens were labeled anonymously with codes containing only group identifiers and time points, without any information related to the repair techniques. The 2 technicians responsible for biomechanical testing (failure load and stiffness measurements) remained unaware of the allocation of the left and right shoulders throughout the testing process. The anonymization of specimens was decoded only after all biomechanical data collection and recording were completed, ensuring that the evaluators’ judgments were not influenced by information regarding the repair techniques.
All samples were thawed to room temperature on the day of biomechanical testing. 18 The supraspinatus was carefully dissected from the scapula while preserving the muscle-tendon junction. 44 The tendon was sutured with No. 2-0 Ethibond (Ethicon) from the myotendinous junction to the insertion point, following established techniques. The sutured supraspinatus was secured to the mechanical loading arm via a custom jig. 52 The humeral component was embedded in cylindrical polyvinyl chloride molds using bone cement. To simulate neutral shoulder abduction, the humeral specimen was mounted on the biomechanical testing machine (Bose 3510-AT) at the anatomic angle. A preload of 20 N was applied for 2 minutes according to the testing protocol. Subsequently, 60 loading cycles were performed at forces ranging from 5 to 50 N with a frequency of 0.25 Hz. 59 After these cycles, an ultimate load-to-failure test was conducted at a rate of 1 mm/s to determine maximum pullout force. Stiffness was defined as the resistance of the tendon-bone repair construct to linear deformation under tensile loading, calculated as the slope of the linear portion (after the toe region) of the load-displacement curve according to linear least squares regression analysis.
Histological Evaluation
After 48-hour fixation in 4% paraformaldehyde, specimens underwent decalcification in 10% EDTA solution for 25 to 30 days. Decalcified specimens were embedded in paraffin blocks. Serial coronal sections (5-μm thickness) parallel to the tendon's long axis were prepared and stained with hematoxylin and eosin, safranin O/fast green, Masson trichrome, and sirius red. For immunohistochemical analysis, CD31 antibody staining was employed to evaluate vascular distribution. Assessments were conducted by 2 independent pathologists blinded to experimental group assignments.
Immunohistochemical Analysis
CD31, serving as an endothelial cell marker, was utilized to evaluate angiogenesis at the repair site. Paraffin-embedded tendon-to-bone sections underwent dewaxing and rehydration. Antigen retrieval was performed using citrate buffer with a 2-stage microwave heating procedure: 10 minutes at high temperature followed by 8 minutes at low temperature. Sections were rinsed with phosphate-buffered saline containing 0.05% Tween 20, then treated with 3% hydrogen peroxide–methanol at room temperature to inhibit endogenous peroxidase activity. Sections were incubated overnight at 4°C with rabbit anti-CD31 primary antibody, followed by incubation with secondary anti-rabbit antibody at room temperature for 1 hour. Finally, sections were counterstained with hematoxylin. Within the sutured region, 3 random microvascular areas were selected under low magnification (3×40). Five nonoverlapping fields were randomly designated, and CD31-positive cells were quantified at 200× magnification for each specimen.
Data Analysis
Statistical analyses were performed in GraphPad Prism 8.0 software. Based on the paired experimental design of this study, paired t tests were employed to compare the biomechanical parameters and histological outcomes between the groups.
For the modified Watkins Tendon Maturity Scoring System (ordinal variables), the paired Wilcoxon signed rank test was used instead of parametric t tests to compare histological outcomes between the groups at the same time point.
Results
General Observation
Macroscopic examination at 8 weeks postoperatively revealed complete healing of all repaired tendons in the KLSB and KSB groups. The supraspinatus tendon exhibited firm attachment to the greater tuberosity with optimal anatomic positioning. The tendon-to-bone interface demonstrated continuous healing characteristics without discernible demarcation from surrounding normal tissues. No intraoperative or postoperative complications were observed.
Biomechanical Evaluation
The typical failure mode of the KSB technique primarily involved tearing of the suture loops in the medial row, while the KLSB technique primarily exhibited tearing of the sutures in the lateral row. The KLSB and KSB groups demonstrated time-dependent increases in ultimate load to failure and stiffness at the tendon-to-bone interface. The KSB group exhibited significantly higher ultimate failure load and stiffness at 0, 2, and 4 weeks postoperatively as compared with the KLSB group (P < .05). However, by 8 weeks postoperatively, no significant differences were observed between the groups in either ultimate failure load or stiffness (P > .05) (Tables 1 and 2).
Ultimate Load to Failure a
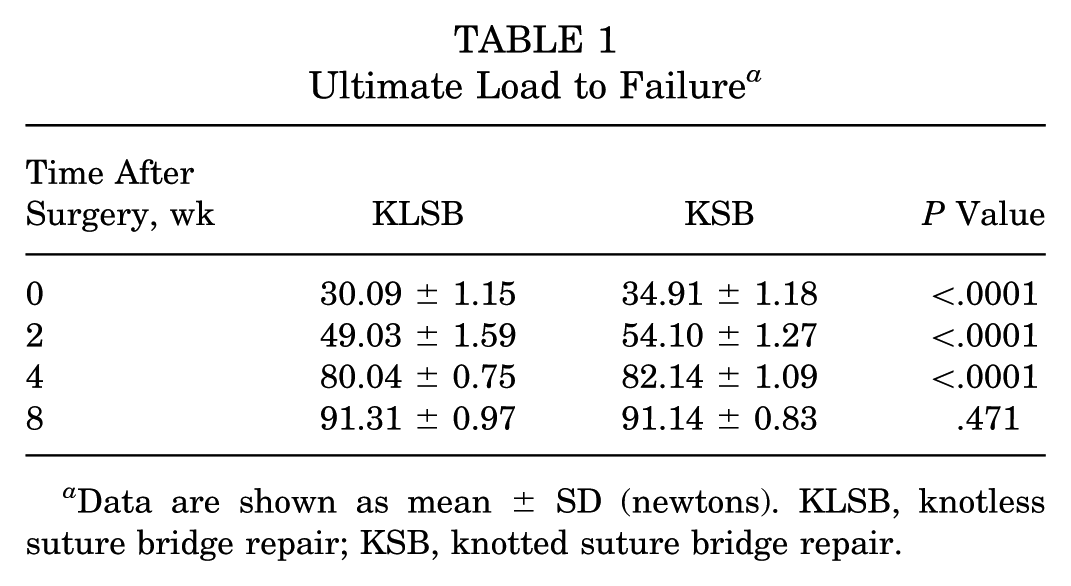
Data are shown as mean ± SD (newtons). KLSB, knotless suture bridge repair; KSB, knotted suture bridge repair.
Stiffness a
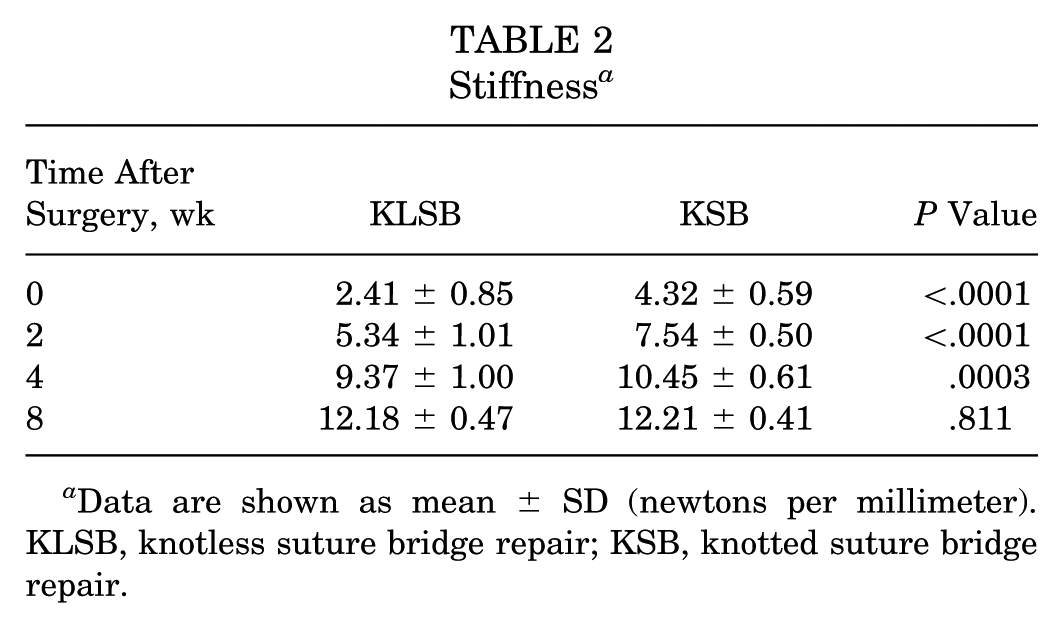
Data are shown as mean ± SD (newtons per millimeter). KLSB, knotless suture bridge repair; KSB, knotted suture bridge repair.
Histological and Immunohistochemical Evaluations
Hematoxylin and Eosin Staining and Modified Tendon Maturity Score
At 2 weeks postoperatively, both groups demonstrated tendon-to-bone connections with inflammatory cell infiltration and granulation tissue formation. Osteoblast and chondrocyte proliferation was observed to be limited. By 4 weeks, inflammatory cell numbers had decreased in both groups, with a notable presence of osteoblasts and immature chondrocyte-like cells. Typical tendon-to-bone interface structures were evident at the repair site, characterized by irregular collagen fiber arrangement and chondrocyte distribution. At 8 weeks, neither group exhibited inflammatory cells, and the repaired site showed continuous, regularly arranged collagen fibers, indicating maturation of the tendon-to-bone interface. The KLSB group demonstrated significantly higher tendon maturity scores at 4 and 8 weeks as compared with KSB (P < .05), with no significant differences observed at 2 weeks (P > .05) (Figure 3).
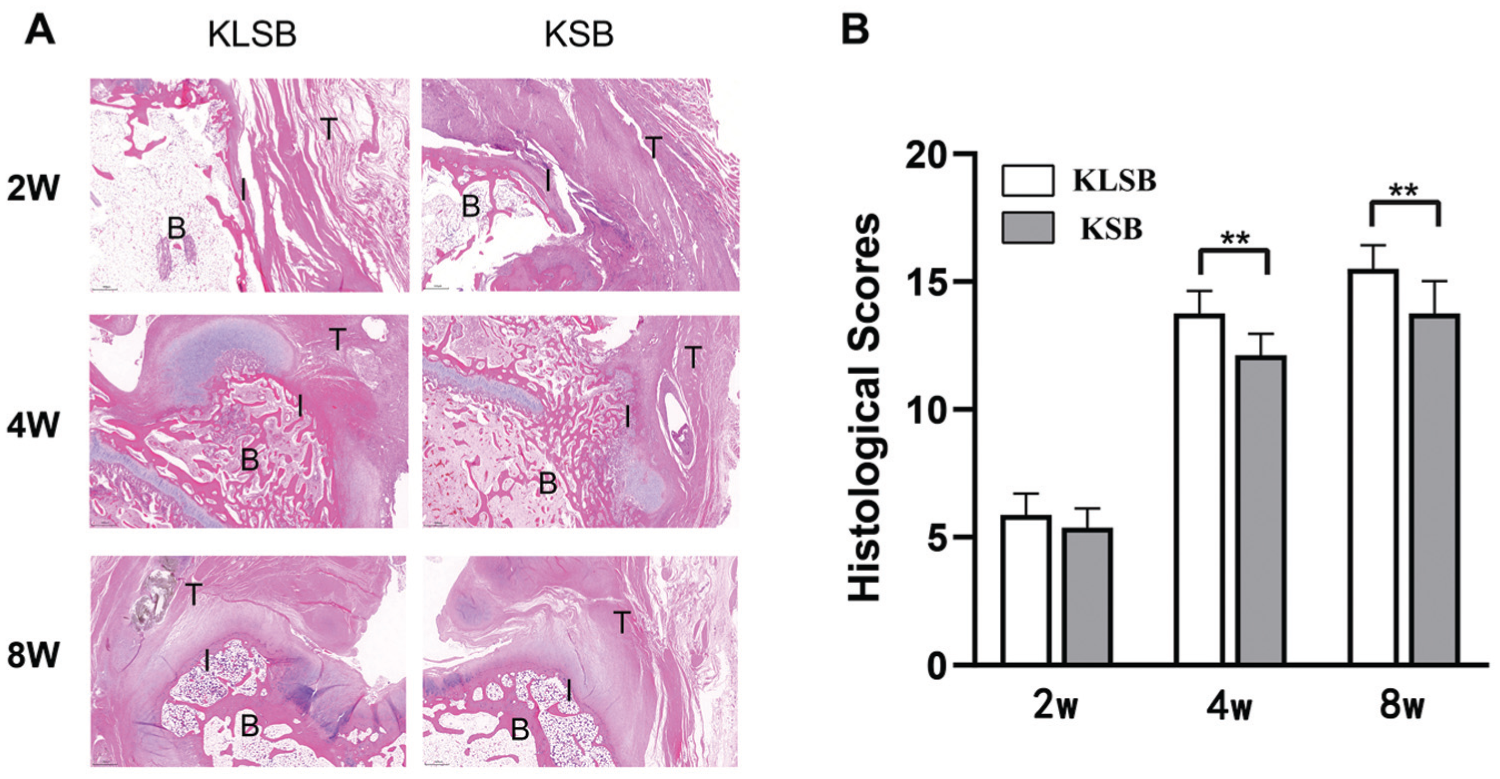
(A) Representative hematoxylin and eosin staining (×40 magnification) of the tendon-to-bone interface formation in the knotless suture bridge repair (KLSB) and knotted suture bridge repair (KSB) groups at 2, 4, and 8 weeks postoperatively. (B) The healing of the repaired tendon-to-bone insertion was quantified by the modified Watkins Tendon Maturity Scoring System. Data are shown as mean ± SD. **P < .01. B, bone; I, tendon-to-bone interface; T, tendon; W, weeks.
Safranin O/Fast Green Staining
No significant differences were observed between groups at 2 weeks postoperatively (P > .05). However, at 4 and 8 weeks, the KLSB group exhibited significantly larger metachromatic staining areas, indicating newly formed fibrocartilage at the tendon-to-bone interface, as compared with the KSB group (P < .05). Additionally, fibrocartilage organization was more structured in the KLSB group (Figure 4).
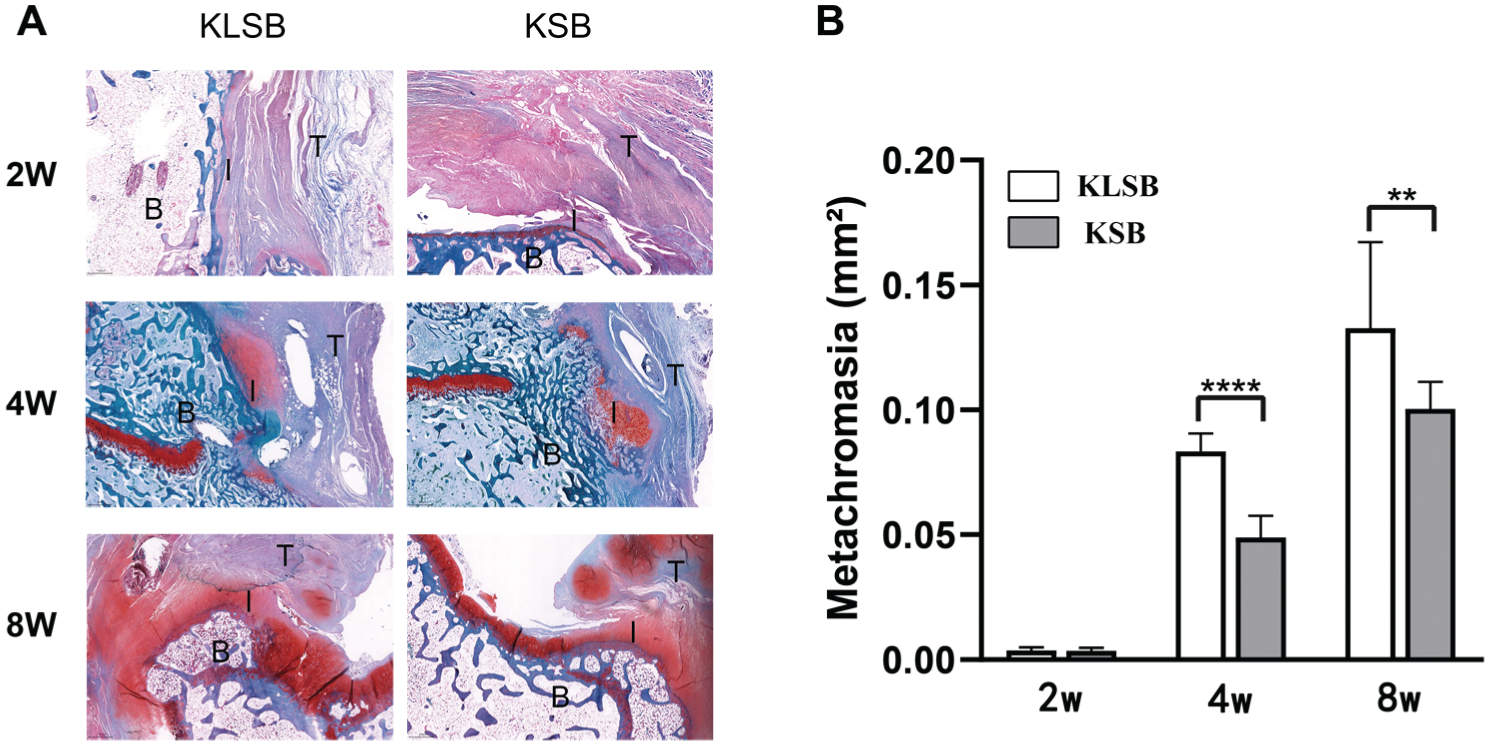
(A) Representative safranin O/fast green staining (×40 magnification) of the tendon-to-bone healing in the knotless suture bridge repair (KLSB) and knotted suture bridge repair (KSB) groups at 2, 4, and 8 weeks postoperatively. (B) The metachromasia was stained red and represented the newly formed fibrocartilage. Data are shown as mean ± SD. **P < .01. ****P < .0001. B, bone; I, tendon-to-bone interface; T, tendon; W, weeks.
Masson Trichrome Staining
Both groups demonstrated progressively organized and mature fibrous tissue formation at the tendon-to-bone interface over time. The KLSB group exhibited superior results, showing more organized and mature fibrous tissue as compared with the KSB group at 2, 4, and 8 weeks postoperatively (Figure 5).
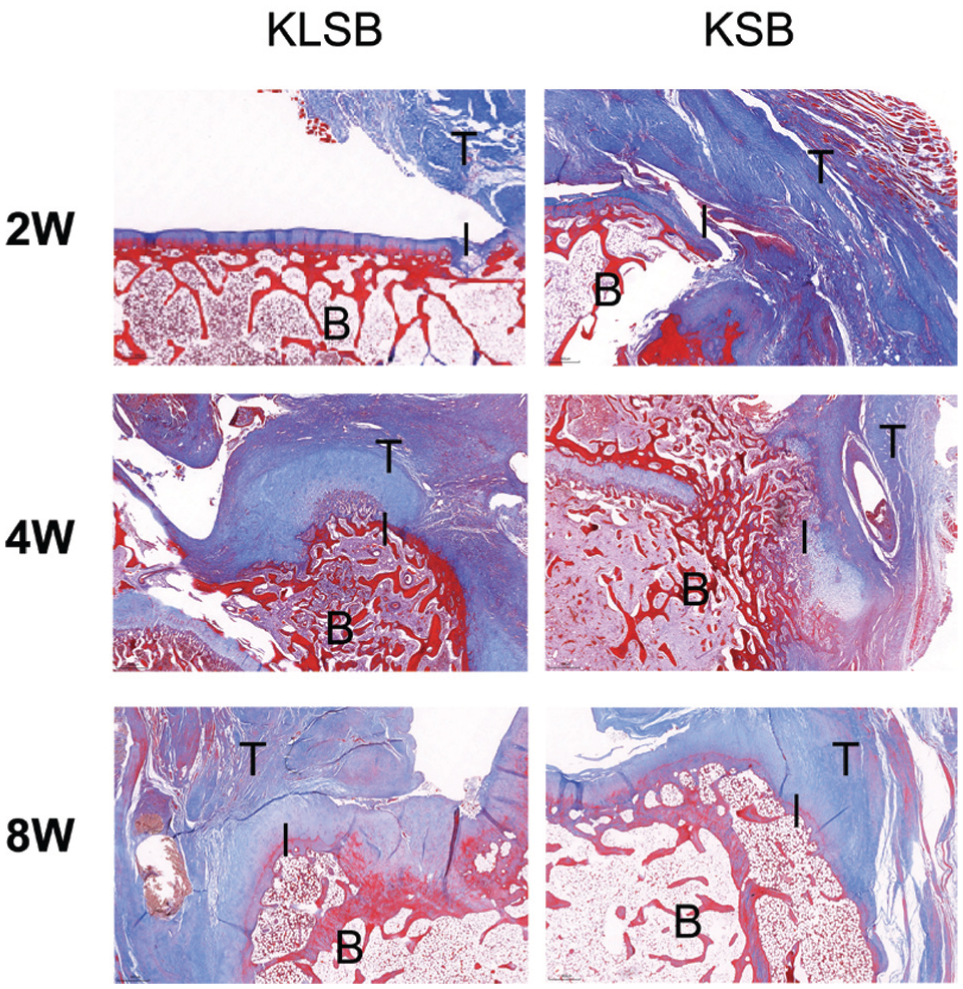
Representative Masson trichrome staining (×40 magnification) of the tendon-to-bone healing in the knotless suture bridge repair (KLSB) and knotted suture bridge repair (KSB) groups at 2, 4, and 8 weeks postoperatively. B, bone; I, tendon-to-bone interface; T, tendon; W, weeks.
Sirius Red Staining
No significant differences in type I collagen composition were observed between groups at 2 weeks postoperatively (P > .05). However, at 4 and 8 weeks, the KLSB group demonstrated significantly higher intensity in yellow-red strong birefringent regions as compared with the KSB group (P < .05) (Figure 6).
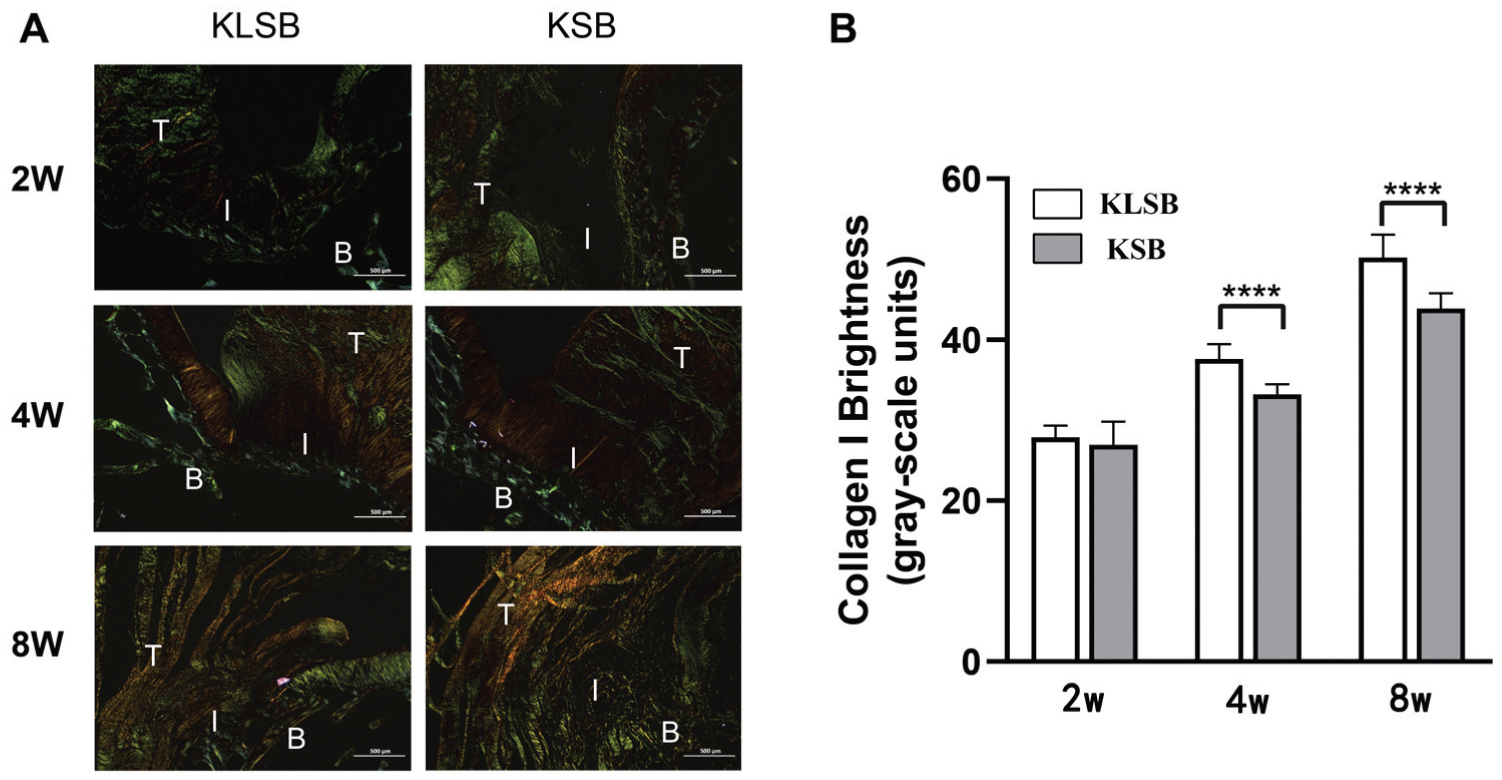
(A) Representative picrosirius red staining (×100 magnification) of the tendon-to-bone healing in the knotless suture bridge repair (KLSB) and knotted suture bridge repair (KSB) groups at 2, 4, and 8 weeks postoperatively. (B) Semiquantitative analysis of the collagen type 1 composition across the tendon-to-bone interface based on the brightness. Data are shown as mean ± SD. ****P < .0001. B, bone; I, tendon-to-bone interface; T, tendon; W, weeks.
CD31 Immunohistochemical Evaluation
Immunohistochemical analysis with CD31 staining revealed significantly higher numbers of CD31-positive vessels at the tendon-to-bone interface near the suture site in the KLSB group as compared with the KSB group at 2, 4, and 8 weeks postoperatively (P < .05) (Figure 7).
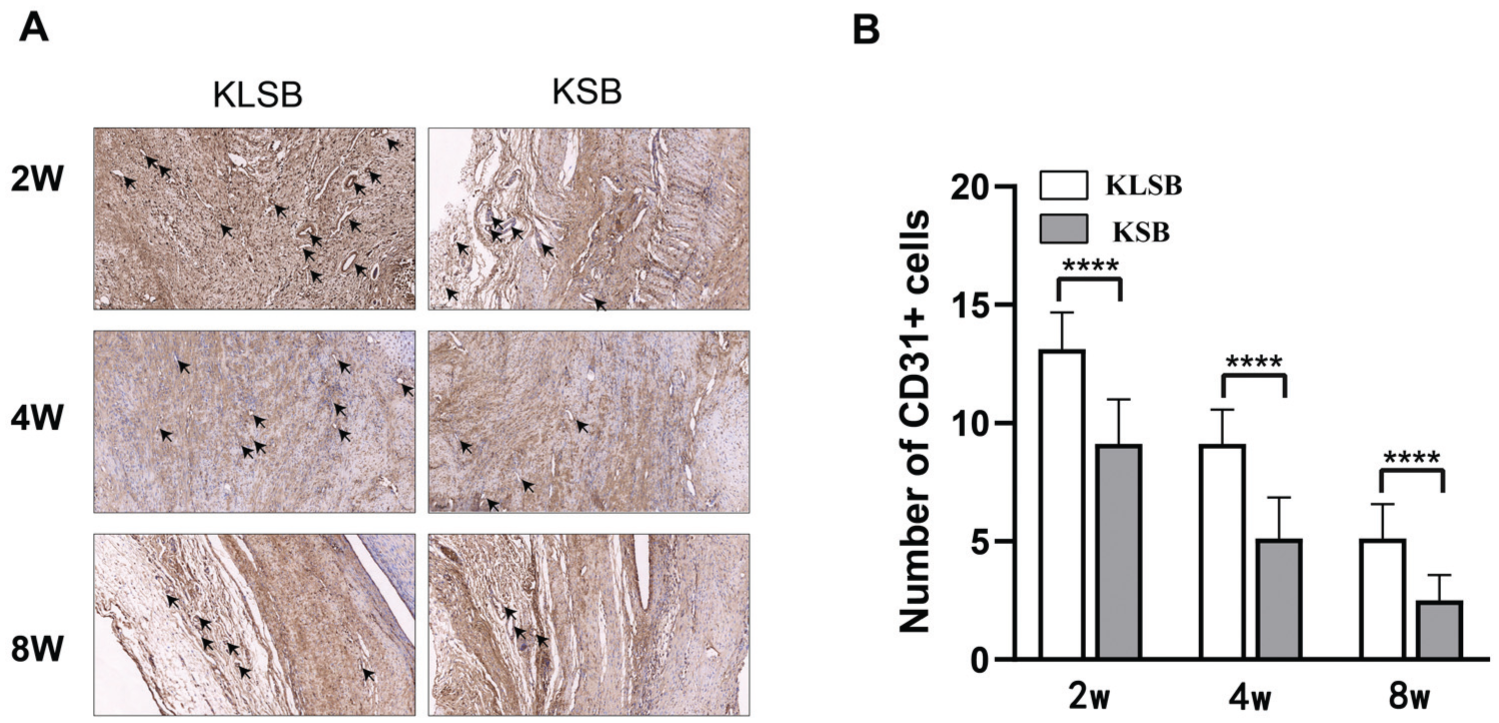
(A) Representative CD31 immunohistochemical staining (×200 magnification) of repaired site near the suture in the knotless suture bridge repair (KLSB) and knotted suture bridge repair (KSB) groups at 2, 4, and 8 weeks postoperatively. (B) Quantitative analysis of CD31 cell counts. ****P < .0001. Dark arrows identify the CD31+ vessels. W, weeks.
Discussion
This study demonstrated that KSB exhibited significantly superior biomechanical performance in ultimate failure load and stiffness at 0, 2, and 4 weeks postoperatively as compared with KLSB. However, the histological analysis revealed that KLSB produced more organized collagen fibers and improved fibrocartilage alignment at 4 and 8 weeks, indicating enhanced tendon-to-bone healing. Notably, the KLSB group showed higher numbers of CD31-positive vessels at 2, 4, and 8 weeks as compared with the KSB group. Although KLSB initially demonstrated slightly inferior biomechanical strength, its histological advantages may provide a more favorable environment for tendon-to-bone healing.
Ideal rotator cuff repair constructs should optimize the initial biomechanical strength and biological healing environment to potentially reduce retear risk.10,17,40 The present study confirmed that KSB provides superior biomechanical strength at 0, 2, and 4 weeks postoperatively. Methods to enhance initial biomechanical strength include increasing anchor number and suture passages and improving suture techniques.1,11,13,41 When compared with KLSB, KSB generates static compression directly on the tendon through medial row horizontal mattress knots, creating rigid fixation that enhances initial biomechanical strength.27,38 Previous systematic reviews by Mall et al 39 confirmed that KSB exhibits greater strength, stiffness, and contact area than KLSB. Busfield et al 5 demonstrated that adding medial row knots to a double-row rotator cuff construct significantly improved biomechanical performance, increasing yield load by 27% and ultimate load by 39%. Consequently, it is not surprising that the KSB provides superior biomechanical strength at 0, 2, and 4 weeks postoperatively in the present study.
Interestingly, no significant biomechanical differences were observed between groups at 8 weeks. Overall biomechanical strength depends on suture construct integrity and tendon-to-bone healing quality. The healing response typically progresses through 3 overlapping stages: inflammation, proliferation/repair, and remodeling.6,21 The suture construct primarily contributes to early-stage strength. As tendon-to-bone healing advances into the remodeling phase, collagen fibers gradually reorganize along force direction, mechanical strength recovers, and the contribution of biological healing surpasses that of the suture construct.31,55 Histological observations in this study demonstrated that KLSB produced significantly better outcomes in fibrocartilage formation, type I collagen content, and collagen alignment at 4 and 8 weeks as compared with KSB. These findings suggest that enhanced tendon-to-bone healing gradually compensated for the initial mechanical deficiency in the KLSB group, ultimately resulting in comparable biomechanical strength at 8 weeks.
The superior histological outcomes in the KLSB group may be attributed to reduced inflammatory cell presence during early tendon-to-bone healing, as excessive inflammation can lead to increased fibrosis. 8 This phenomenon may result from 2 factors. First, the knotless technique eliminates knot-related mechanical irritation and scraping damage between the rotator cuff and greater tuberosity, reducing local inflammatory responses caused by physical compression and friction. 58 Second, knot tying may increase local tissue tension, impairing blood circulation and the repair microenvironment at the tendon-to-bone interface. 36 By avoiding local compression of periosteum and soft tissues by suture knots, KLSB preserves microcirculation and reduces secondary inflammation resulting from ischemia, hypoxia, and pressure-induced necrosis.
Multiple studies indicate that tendon vascularization is crucial for rotator cuff tendon-to-bone healing.22,23,35 Cho et al 9 noted that sutures may constrict peritendinous blood vessels, potentially leading to tendon necrosis. When torn rotator cuff tendons are atrophied and poorly vascularized, healing depends on cellular proliferation and vascular ingrowth from surrounding soft tissues, remaining tendon, and bone.2,15,26 However, different suture constructs can produce distinct vascular patterns postoperatively. 54 Rotator cuff tendons, particularly near the “critical zone” at the distal attachment, typically exhibit limited vascularity. Blood flow reduction caused by knots significantly impedes healing and may contribute to retear after rotator cuff repair. 20 During the first 3 postoperative months, adequate blood flow is essential to enhance biological remodeling at the tendon-to-bone interface. 33 The significantly higher CD31-positive cell counts in the KLSB group at 2, 4, and 8 weeks indicate improved blood supply, which may enhance biological remodeling and improve healing outcomes. 25
Generally, high tensile stress promotes tenogenesis while low tensile stress favors osteogenesis. 34 Safranin O/fast green staining results demonstrated significantly larger areas of newly formed fibrocartilage in the KLSB group at 4 and 8 weeks. Beyond improved blood supply, dynamic mechanical stimulation may contribute to fibrocartilage formation. Recent studies indicate that knotless repair exhibits stronger self-reinforcing properties as compared with knotted repair, potentially enhancing footprint contact pressure. 50 We hypothesize that the knotless design in the medial row allows KLSB constructs to exert dynamic compression during tendon-to-bone healing. Relative suture displacement provides nonconstant, dynamic tensile mechanical stimulation that may promote fibrocartilage formation.7,16,45,57 However, the effects of mechanical stimulation on tendon-to-bone healing are complex, requiring further investigation to confirm the specific effects of loading magnitude, duration, and frequency. 12
This study has several limitations. First, the use of New Zealand White rabbit shoulders introduces anatomic differences from human shoulders, as rabbit shoulder joints are weightbearing while human shoulders are not, potentially affecting biomechanical environments and healing mechanisms. Second, rabbits were not immobilized postoperatively. Third, an acute rotator cuff tear model was utilized, while clinical rotator cuff injuries in humans are often chronic, accompanied by tendon degeneration and tissue quality deterioration not simulated in this study. Fourth, multiple between-group comparisons were performed without statistical correction, potentially increasing type I error risk. This research represents a preliminary animal study, and large-scale clinical investigations are necessary to determine which technique yields more satisfactory functional outcomes and lower retear rates for rotator cuff tears.
Conclusion
Both repair techniques are effective. KSB provides superior early biomechanical outcomes, while KLSB demonstrates significant advantages in histological healing. Over time, the enhanced healing achieved with KLSB compensates for initial deficits, ultimately producing biomechanical results comparable to KSB.
Footnotes
Acknowledgements
The authors express their sincere gratitude to all those who have supported and contributed to the completion of this research. They thank Ying Shan from the Clinical Research Institute of Peking University Shenzhen Hospital for her valuable statistical support in this study.
Submitted September 26, 2025; accepted February 8, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by the National Natural Science Foundation of China (grants 82272568, W2421098), the Sanming Project of Medicine in Shenzhen (grant SZSM202211019), the Guangdong Medical Science and Technology Research Fund Project (grant B2024001), the Guangdong Basic and Applied Basic Research Foundation (grant 2023A1515220039), the Shenzhen Medical Research Special Fund (C2401031), and the Shenzhen Municipal Science and Technology Innovation Commission Project (grant JCYJ20230807095106013). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.