
Abstract
Background:
Bankart repair is commonly performed for traumatic anterior shoulder instability. Modern arthroscopic techniques have advanced considerably, raising the question of whether their clinical performance now matches that of traditional open repair.
Purpose:
To compare contemporary arthroscopic and open Bankart repair across instability-related, functional, perioperative, and complication outcomes.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic search of the PubMed, Scopus, Cochrane Library, and Google Scholar databases was conducted through December 2025. A total of 32 comparative studies met inclusion criteria. Extracted outcomes included postoperative dislocation, subluxation, overall instability, apprehension, patient-reported outcome measures (Rowe, American Shoulder and Elbow Surgeons [ASES], University of California Los Angeles [UCLA], Western Ontario Shoulder Instability Index [WOSI], and visual analog scale [VAS] scores), postoperative range of motion (ROM), loss of motion relative to baseline, operative time, infection, and reoperation rates. A subgroup analysis stratified studies by publication period (before 2010 vs 2010 onward) to explore the influence of evolving surgical techniques over time.
Results:
No differences were found between arthroscopic and open Bankart repair in postoperative dislocation (P = .05), subluxation (P = .40), overall instability (P = .06), or apprehension (P = .40). Patient-reported outcomes, including Rowe (P = .19), ASES (P = .28), UCLA (P = .41), WOSI (P = .40), and VAS pain (P = .05) scores, were comparable between groups. Postoperative ROM showed no differences across most parameters; however, loss of external rotation in abduction relative to baseline favored arthroscopic repair (mean difference, −1.67; P = .04). Operative time did not differ between groups (P = .11). Arthroscopic repair was associated with a shorter hospital stay (P = .0001). Reoperation rates were higher after arthroscopic repair (RR, 2.15; P = .0004). Infection rates were similar (P = .13). In subgroup analysis, studies published before 2010 showed higher postoperative dislocation (RR, 2.13; P = .01) and overall instability (RR, 1.67; P = .02) after arthroscopic repair, as well as greater external rotation in abduction with arthroscopy. In contrast, studies published from 2010 onward demonstrated no differences between arthroscopic and open repair across instability, functional, or ROM outcomes.
Conclusion:
Arthroscopic and open Bankart repair provide largely comparable postoperative stability, functional recovery, and ROM, with modest differences reflecting the intrinsic nature of each technique. Publication period subgroup analysis suggests that historical instability differences were driven primarily by earlier studies, whereas contemporary studies show comparable instability and functional outcomes between approaches. Given its minimally invasive profile, arthroscopy offers practical advantages, including slightly better preservation of external rotation in abduction, while maintaining stability outcomes comparable to open repair.
Keywords
Anterior shoulder instability is a common and often debilitating condition that significantly affects function, activity levels, and quality of life in young, active individuals. It accounts for the vast majority of glenohumeral instability cases, with peak incidence in adolescents and adults <30 years, and higher prevalence among males and overhead or contact athletes. Traumatic detachment of the anteroinferior labrum (Bankart lesion) is a primary contributor to recurrent instability, compounded by capsular laxity, glenoid bone loss, and Hill-Sachs defects that alter joint biomechanics and reduce stability during shoulder motion.24,58 Because of the substantial risk of recurrence, surgical stabilization is commonly recommended, sometimes even after the first dislocation, when there are additional risk factors for failure (eg, young age, contact or overhead sport, bone loss, and large labral/Hill-Sachs lesions), rather than waiting for multiple instability events. 41
In the surgical management of traumatic anterior shoulder instability, several stabilization techniques are available, ranging from soft tissue repairs to bony augmentation procedures. The most used operations include Bankart repair, remplissage, Latarjet (coracoid transfer), and, less frequently, bone-grafting procedures for significant glenoid defects. 33 The choice of procedure is determined by patient-specific factors, including glenoid bone loss, Hill-Sachs lesion engagement, sports participation, and tissue quality. Current guidelines suggest that isolated Bankart repair is appropriate when glenoid bone loss is <13% to 15%, capsulolabral tissue is of good quality, and instability is not associated with an engaging Hill-Sachs lesion. 33 Remplissage may be added when a moderate Hill-Sachs lesion is present, especially if it is off-track or contributes to engagement during abduction–external rotation. 56 In contrast, coracoid transfer procedures such as Latarjet are recommended for patients with substantial glenoid bone loss (>15%-20%), bipolar bone loss, recurrent instability despite soft tissue repair, or collision/contact athletes at high risk of failure. 12 Among available surgical options, arthroscopic and open Bankart repair remain among the most widely used soft tissue stabilization techniques for managing recurrent anterior shoulder instability. Both procedures seek to restore labral integrity, retension the capsuloligamentous complex, and prevent further instability, yet they differ fundamentally in surgical exposure, technical execution, and postoperative expectations.
Arthroscopic Bankart repair is a minimally invasive approach that provides broad visualization of intra-articular structures and enables simultaneous management of associated pathology while preserving surrounding soft tissues. The technique has become widely adopted with advancements in arthroscopic instrumentation and suture anchor technology. 25 Open Bankart repair, in contrast, involves direct exposure of the capsulolabral complex and the inferior glenohumeral ligament, allowing a traditionally well-established method of capsular and labral reconstruction. 44 Although both techniques share the goal of restoring stability through labral reattachment and capsular tensioning, they differ in surgical exposure, tissue handling, and the mechanics of repair, reflecting 2 distinct operative philosophies within shoulder stabilization surgery.
Given these distinct risk profiles of each technique, a comprehensive quantitative synthesis is necessary to determine which technique offers more favorable clinical and functional outcomes in patients with traumatic anterior shoulder instability. The present systematic review and meta-analysis compares instability recurrence, functional scores, range of motion (ROM) recovery, perioperative outcomes, complications, and reoperation rates between patients undergoing arthroscopic Bankart repair and those treated with open Bankart repair.
Methods
Search Strategy
A comprehensive literature search was conducted in the PubMed, Scopus, Cochrane Library, and Google Scholar databases, covering all available studies from database inception through December 4, 2025. The search strategy combined predefined keywords and Medical Subject Headings (MeSH) using Boolean operators (“AND” and “OR”). The following terms and their variations were used: “Bankart repair,”“arthroscopic Bankart,”“open Bankart,”“shoulder instability,” and “recurrent shoulder dislocation.” To ensure a comprehensive capture of contemporary surgical techniques, both MeSH and non-MeSH terminology related to arthroscopic and open stabilization were included. Reference lists of all included studies and relevant systematic reviews were manually screened to identify any additional eligible articles not retrieved during the electronic search. This systematic review protocol was registered in the PROSPERO international prospective register of systematic reviews (CRD420261338579).
Eligibility Criteria and Study Selection
Eligible studies included adult patients diagnosed with traumatic anterior shoulder instability based on clinical and radiographic criteria. The intervention of interest was arthroscopic Bankart repair performed for soft tissue stabilization of anterior shoulder instability (whether primary or recurrent) using any technique, including single- or double-row suture anchors, capsular plication, and management of associated pathologies when reported. The comparator was open Bankart repair performed for anterior shoulder instability (whether primary or recurrent), encompassing classic open capsulolabral repair, bony Bankart fixation, or open capsular shift techniques. Only peer-reviewed, full-text comparative clinical studies, including randomized controlled trials (level 1 or 2 evidence), prospective or retrospective cohort studies, and registry-based analyses (level 2 or 3 evidence), directly comparing outcomes between arthroscopic and open Bankart repair, were included.
Exclusion criteria included noncomparative designs (eg, single-arm cohorts, case series, and case reports); cadaveric or animal studies; reviews, systematic reviews, meta-analyses, editorials, or conference abstracts; non–English-language publications; studies evaluating multidirectional, posterior, or atraumatic instability patterns; studies involving other surgical treatments (eg, Latarjet, Bristow, remplissage-only procedures, or Bankart repair combined with concomitant procedures such as remplissage); patients with concomitant major shoulder injuries such as full-thickness rotator cuff tears, proximal humerus or glenoid fractures, large bony defects requiring bone-block procedures, or neurological injuries affecting shoulder stability; studies including revision surgery or mixed primary and revision cohorts without separable primary-case data; and studies in which separate data for arthroscopic and open Bankart repair could not be extracted.
Data Extraction
Two independent reviewers (G.A. and J.P.S.) extracted data from each included study using a standardized spreadsheet developed for this meta-analysis. Extracted variables covered study-level characteristics such as author, publication year, study design, sample size of each group, surgical approach (arthroscopic vs open Bankart repair), stabilization technique details (eg, use of capsular shift, remplissage, or additional labral procedures), and maximum follow-up duration. Patient characteristics collected included mean age, sex distribution, and body mass index, as well as side and dominance of the operated shoulder when reported. Details of the fixation constructs and implants used for arthroscopic repair (eg, transglenoid sutures, bioabsorbable tacks, metallic or bioabsorbable suture anchors, and polyether-ether-ketone (PEEK) anchors) were also extracted when reported to characterize the evolution of arthroscopic techniques across study eras.
Clinical and radiographic baseline information was also extracted, including instability pattern (primary vs recurrent and anterior involvement with or without posterior extension), associated lesions such as soft tissue or bony Bankart lesions, superior labrum anterior-posterior (SLAP) tears, anterior labral periosteal sleeve avulsion (ALPSA) lesions, humeral avulsion of the glenohumeral ligament (HAGL) lesions, glenolabral articular disruption (GLAD) lesions, glenoid fractures or subcritical bone loss, presence and quantitative description of Hill-Sachs lesions (eg, lesion width and depth in millimeters), dominant-hand involvement, and preoperative shoulder-specific functional scores when available (eg, Rowe, Constant, American Shoulder and Elbow Surgeons [ASES], University of California Los Angeles [UCLA], Western Ontario Shoulder Instability Index [WOSI], and Quick Disabilities of the Arm, Shoulder and Hand scores). When reported, information on glenoid bone loss and bipolar bone loss characteristics was also collected to assess baseline anatomic comparability between arthroscopic and open cohorts.
This review examined postoperative outcomes across instability-related, patient-reported, ROM, perioperative, and complication domains. Instability-related outcomes included recurrent dislocation, subluxation, overall postoperative instability, and apprehension. Patient-reported outcome measures (PROMs) encompassed the Rowe, ASES, UCLA, WOSI, and visual analog scale (VAS) pain scores. Shoulder motion outcomes evaluated both absolute postoperative ROM, including external rotation at the side, external rotation in abduction, forward flexion, and internal rotation at 90° of abduction, and loss of ROM relative to baseline for the same movement planes. Perioperative outcomes included operative time and hospital length of stay. Complication-related endpoints assessed all-cause reoperation rates and postoperative infection. All extracted data were independently cross-verified for accuracy. Disagreements between reviewers were resolved through discussion or, when necessary, adjudication by a third reviewer (M.B.).
Risk of Bias Assessment
Study quality was assessed using the Risk of Bias Version 2 (ROB 2) tool 54 for randomized controlled trials and the Risk of Bias in Nonrandomized Studies of Interventions (ROBINS-I) tool for nonrandomized studies. 53 ROB 2 evaluates 5 domains: randomization, deviations from intended interventions, missing data, outcome measurement, and selective reporting. ROBINS-I addresses similar domains adapted for nonrandomized designs (bias in selection of participants, classification of interventions, measurement of outcomes, selection of the reported results, and missing data). Each domain was rated as low risk, some concerns, or high risk, with the overall judgment based on the highest rating. Assessments were performed independently by 2 reviewers (G.A. and J.P.S.), with disagreements solved by a third reviewer (M.B.).
Statistical Analysis
All statistical analyses were performed using Review Manager 5.4 (Cochrane Collaboration). Continuous outcomes were analyzed using either mean differences (MDs) or standardized mean differences, both reported with 95% confidence intervals, depending on the consistency of the measurements. Dichotomous outcomes were evaluated using risk ratios (RRs) with 95% confidence intervals. Heterogeneity was assessed with the Q test and I2 statistic; a P value ≤.10 or an I2 value >50% was considered indicative of significant heterogeneity.
Statistical pooling was performed using either fixed-effects or random-effects models depending on the degree of statistical heterogeneity. When heterogeneity was low to moderate (I2≤ 50%), a fixed-effects model was applied. When substantial heterogeneity was present (I2 > 50%), a random-effects model was used to account for potential variability in true effect sizes across studies. Statistical significance was defined as a P value <.05. To explore the potential effect of temporal changes in surgical technique, an additional subgroup analysis was performed according to publication period (before 2010 vs 2010 onward).
Results
Study Selection
The systematic literature search resulted in 967 relevant preliminary records across electronic databases. After deduplication, 432 records were assessed for title and abstract screening, leaving 141 studies for full-text evaluation. Of these, 32 studies met all inclusion criteria and were included in the quantitative synthesis. The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart (Figure 1) provides a detailed overview of record exclusion at each stage.
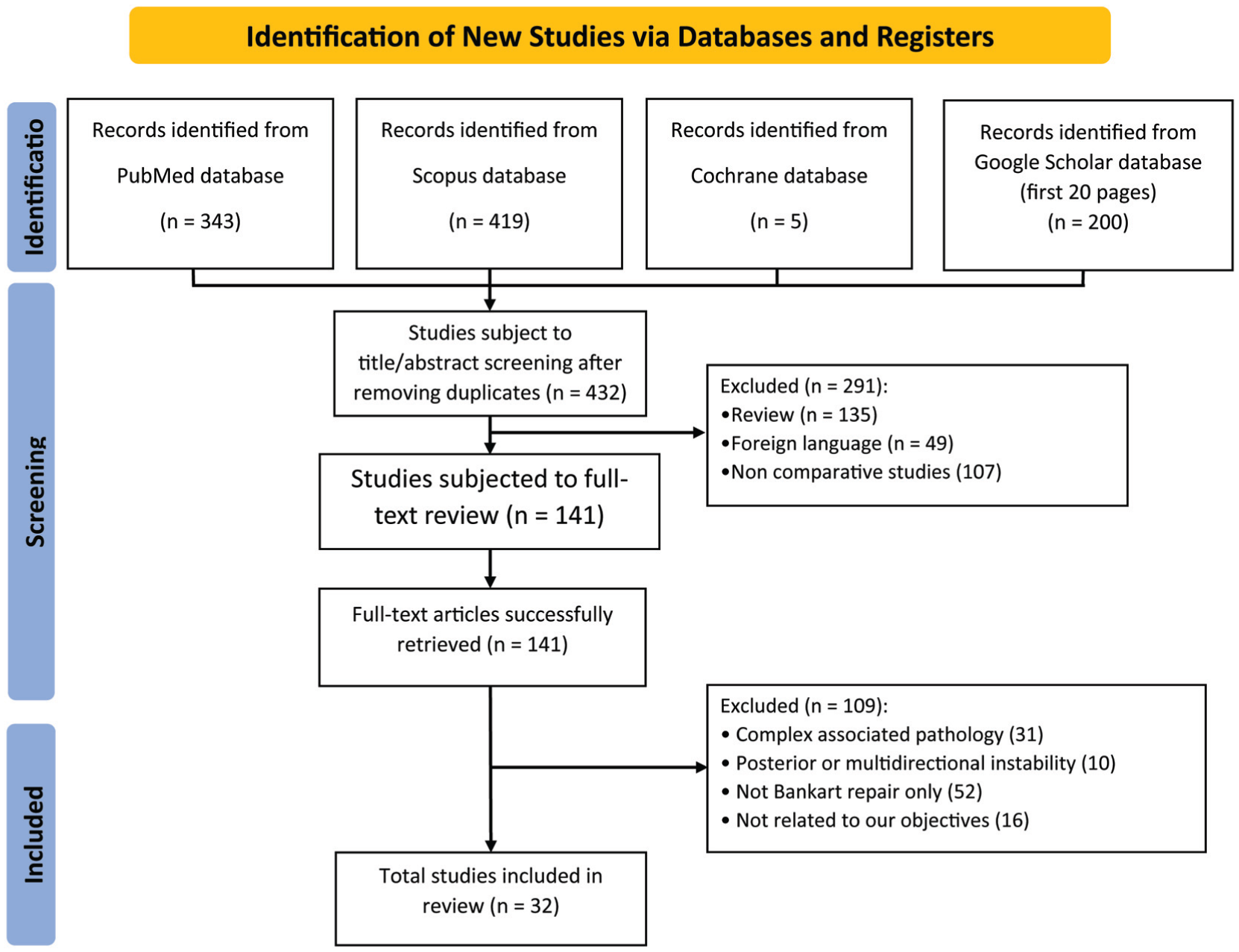
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram for study identification and selection.
Characteristics of Included Studies
A total of 32 comparative studies published between 1993 and 2025 were included, encompassing approximately 3000 shoulders that underwent either arthroscopic or open Bankart repair for traumatic anterior shoulder instability. The included studies consisted of 4 randomized controlled trials, 19 prospective cohort studies, and 9 retrospective cohort studies.
Sample sizes varied substantially, from small institutional cohorts with <20 patients per group to larger multicenter or registry-type series including up to 364 patients in total across arthroscopic and open groups. Follow-up durations ranged from short-term evaluations of 12 to 24 months to long-term analyses extending 10 to 15 years, with several studies reporting survivorship and recurrence-free outcomes beyond a decade.
Across included studies, patients undergoing Bankart repair were predominantly young adults, most commonly between 17 and 35 years of age. Male patients represented most of both cohorts, frequently exceeding 70% to 80% of the study populations, reflecting the typical demographic pattern of traumatic anterior instability in contact and overhead athletes. When reported, dominant shoulder involvement was common, and a substantial proportion of patients participated in sport at recreational or competitive levels.
Across the included studies, anterior shoulder instability presentations ranged from recurrent dislocation to recurrent subluxation after a traumatic event. The structural lesions documented were predominantly soft tissue Bankart tears and bony Bankart lesions, with several studies also reporting ALPSA lesions, HAGL lesions, SLAP type 2 to 5 tears, Perthes lesions, GLAD lesions, and capsulolabral disruptions of varying extent. Hill-Sachs defects were frequently identified, with studies reporting both the presence and quantitative measurements of lesion width and depth when available. Some cohorts explicitly included only patients without critical glenoid bone loss or engaging Hill-Sachs lesions, whereas others included patients with subcritical glenoid bone loss detected on imaging or arthroscopy. Overall, both arthroscopic and open Bankart repair groups consisted of patients with well-characterized anterior instability pathology, with lesion types and associated findings consistently reported across studies. None of the included studies reported the use of concomitant remplissage procedures.
With respect to surgical technique, earlier arthroscopic studies commonly used transglenoid sutures, suture punch techniques, and bioabsorbable tacks or fixators, whereas later studies more frequently used contemporary suture anchor constructs, including metallic, bioabsorbable, titanium, and PEEK anchors. Open Bankart repair was most commonly performed through a deltopectoral approach, with several studies incorporating capsular shift or capsulolabral reconstruction techniques.
Baseline anatomic parameters were commonly reported, including presence and quantitative description of Hill-Sachs lesions (width and depth in millimeters), associated glenoid bone loss or fractures, concomitant SLAP or capsulolabral lesions, and dominant-hand involvement. Several studies also documented preoperative functional and instability-related scores, such as the Rowe score, as well as baseline shoulder ROM, including external rotation at the side, external rotation in abduction, internal rotation at 90° of abduction, and forward flexion. It is worth noting that across the included studies, both arthroscopic and open Bankart groups generally demonstrated comparable baseline instability severity and functional limitation, although some open cohorts included a slightly higher proportion of patients with bony Bankart lesions or subcritical bone loss. However, only a minority of studies reported quantitative glenoid bone loss, and reporting was inconsistent, without sufficiently detailed and separable data to permit a meaningful between-group comparison or pooled analysis of bone loss differences between arthroscopic and open repair cohorts.
Detailed baseline characteristics and study-level parameters are provided in Supplementary Tables 1 and 2.
Methodological Quality Assessment
Non-Randomized Studies (ROBINS-I)
All nonrandomized studies were evaluated using the ROBINS-I tool. As shown in Figure 2A, most studies demonstrated an overall moderate risk of bias, with only a few achieving consistently low scores across domains. The domain most frequently affected was confounding (D1), reflecting the limitations of retrospective designs and the lack of adjustment for key prognostic factors such as instability severity, associated lesions, or bone loss.
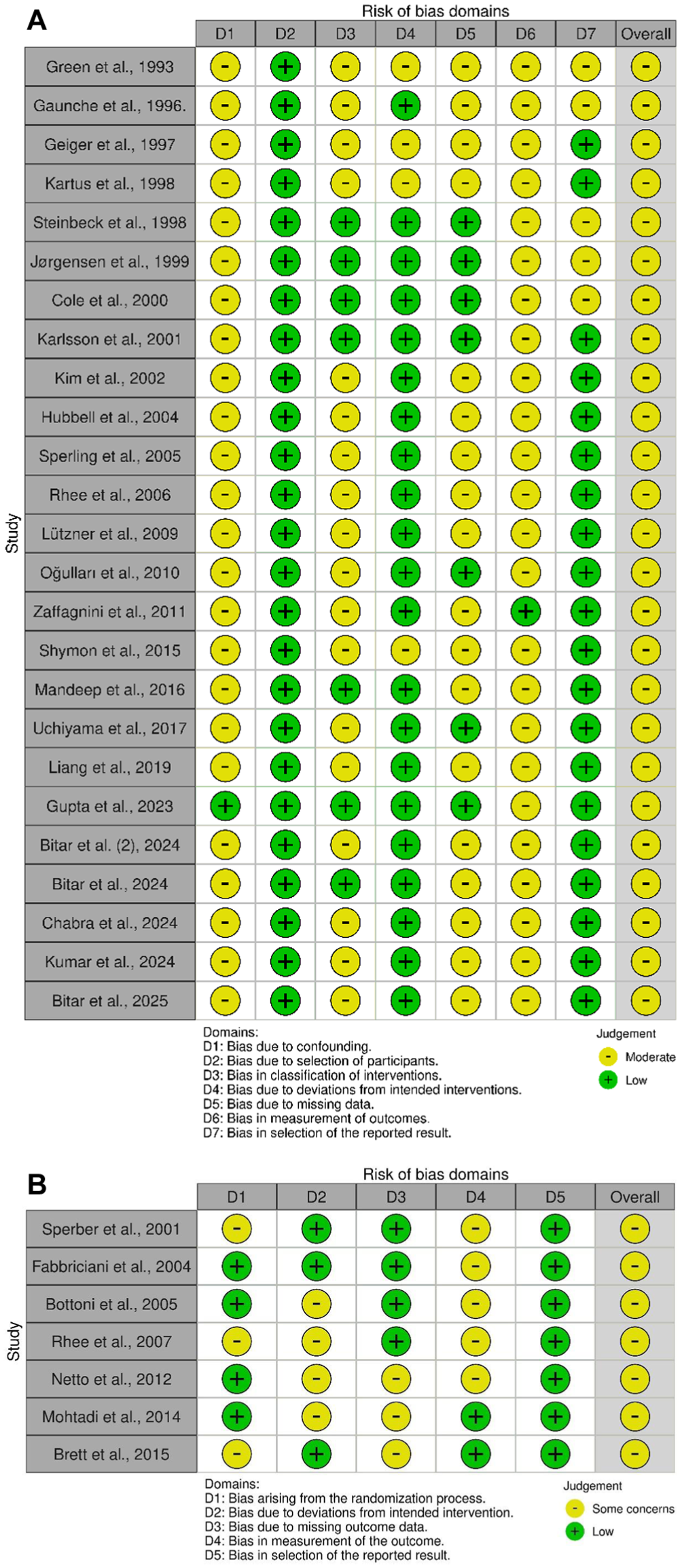
Risk of bias assessment across included studies. (A) Risk of Bias in Nonrandomized Studies of Interventions. (B) Risk of Bias Version 2.
Bias in selection of participants (D2) and classification of interventions (D3) was generally low due to clear descriptions of surgical techniques and inclusion criteria. Deviations from intended interventions (D4) and missing data (D5) were also mostly rated as low risk, indicating minimal protocol departures and acceptable follow-up completeness. Outcome measurement (D6) showed uniformly low risk, supported by the use of validated functional scores and standardized definitions of recurrence. Selective reporting (D7) showed some variability, primarily in older studies lacking prespecified protocols.
Overall, the visual summary (Figure 2A) indicates that while residual confounding remains the main methodological limitation, the overall quality of evidence is sufficient to support reliable comparative synthesis.
Randomized Studies (ROB 2)
The randomized controlled trials were assessed using the ROB 2 tool. As shown in Figure 2B, the overall risk of bias across randomized controlled trials was low to moderate, with most studies displaying some concerns rather than serious methodological flaws. The domain most affected was bias arising from the randomization process (D1), in which incomplete reporting of sequence generation or allocation concealment introduced uncertainty regarding true randomization integrity.
In contrast, other domains, including deviations from intended interventions (D2), missing outcome data (D3), and outcome measurement (D4), were consistently rated as low risk, supported by standardized operative protocols, adequate follow-up, and validated outcome measures. Selective reporting (D5) contributed to additional concerns in a few studies due to the absence of preregistered protocols or incomplete reporting of secondary outcomes.
Overall, the randomized controlled trials demonstrated sound methodological quality with only minor limitations, supporting their inclusion in the comparative synthesis (Figure 2B).
Instability-Related Outcomes
Dislocation
Eight studies (294 arthroscopic Bankart; 355 open Bankart) reported postoperative dislocation. The pooled fixed-effects analysis demonstrated a borderline difference between procedures (P = .05). Heterogeneity was low (I2 = 16%) (Figure 3A).
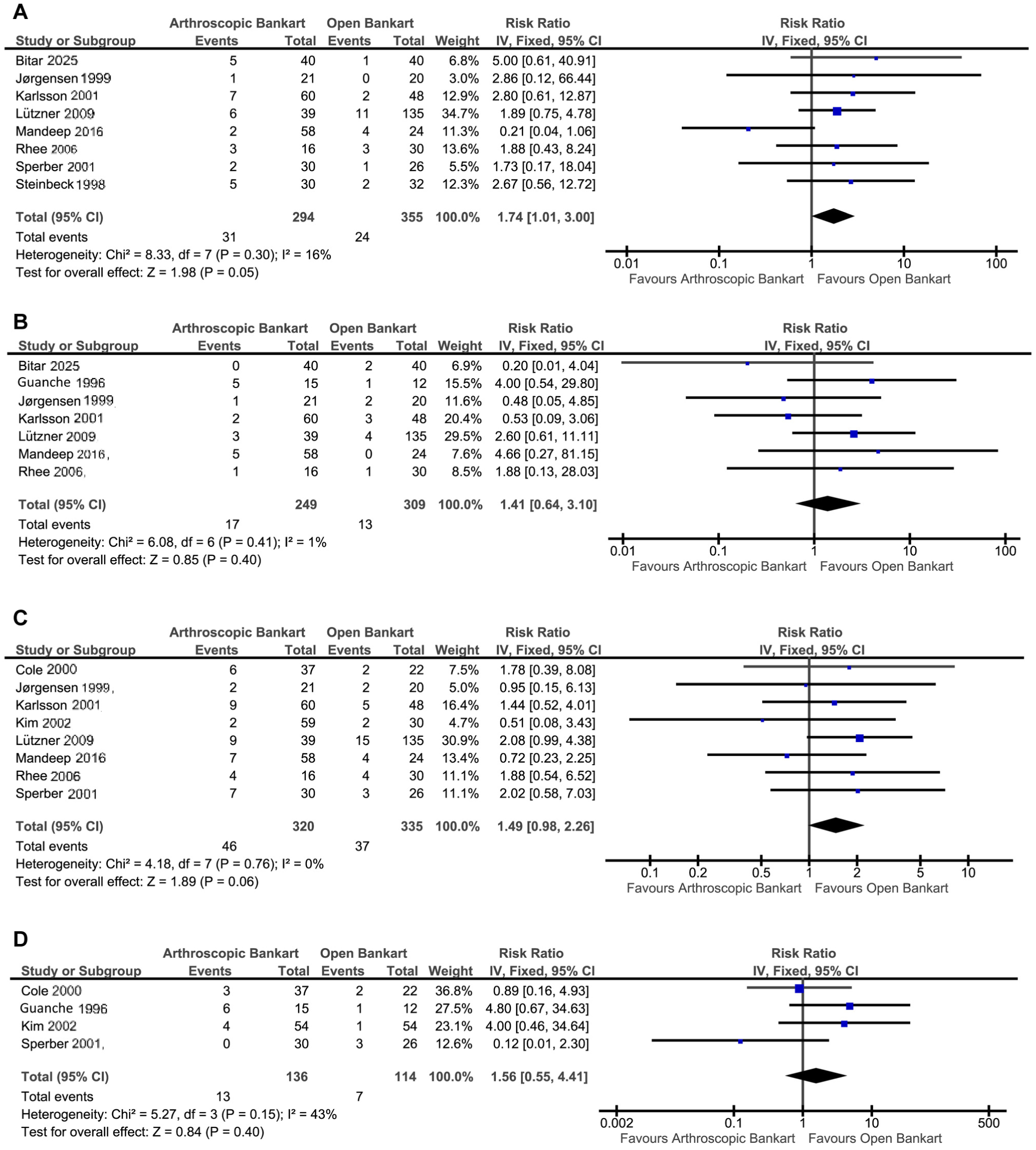
Instability-related outcome forest plots. (A) Dislocation. (B) Subluxation. (C) Instability. (D) Apprehension. IV, inverse variance.
Subluxation
Seven studies (249 arthroscopic Bankart; 309 open Bankart) reported postoperative subluxation. The pooled fixed-effects analysis showed no statistically significant difference between procedures (P = .40). Heterogeneity was low (I2 = 1%) (Figure 3B).
Instability
Eight studies (320 arthroscopic Bankart; 335 open Bankart) reported postoperative instability. The pooled fixed-effects analysis demonstrated no statistically significant difference between procedures (P = .06). Heterogeneity was low (I2 = 0%) (Figure 3C).
Apprehension
Four studies (136 arthroscopic Bankart; 114 open Bankart) reported postoperative apprehension, defined as patient-perceived fear or instability during provocative positions. The pooled fixed-effects analysis demonstrated no statistically significant difference between both procedures (P = .40). Heterogeneity was moderate (I2 = 43%) (Figure 3D).
Patient-Reported Outcome Measures
Rowe Score
Eleven studies (464 arthroscopic Bankart; 423 open Bankart) reported postoperative Rowe scores, a composite measure of instability, motion, and function in which higher scores indicate better shoulder stability and overall clinical outcomes. The pooled random-effects analysis demonstrated no statistically significant difference between procedures (P = .19). Heterogeneity was high (I2 = 96%) (Figure 4A).
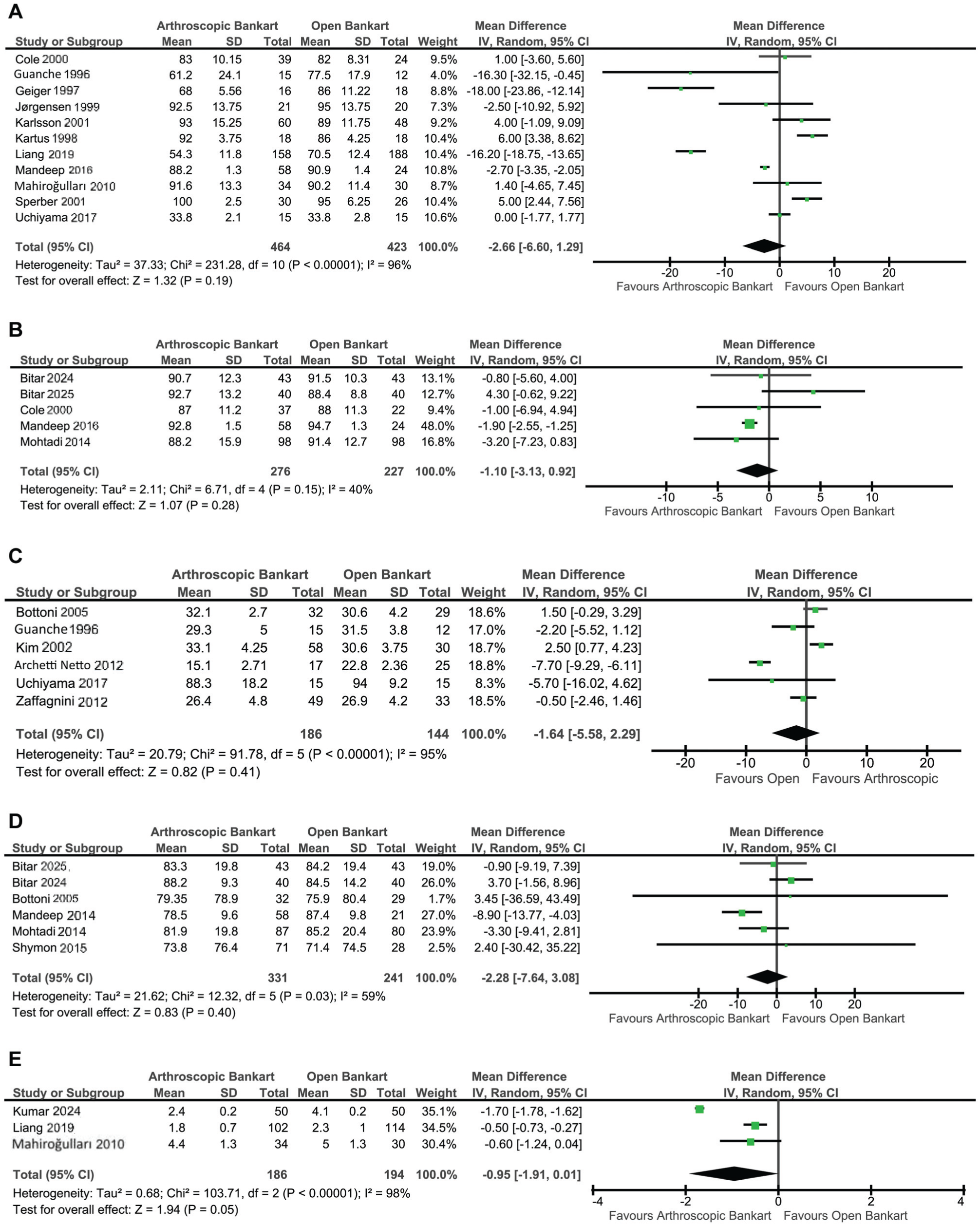
Patient-reported outcome measure forest plots. (A) Rowe score. (B) American Shoulder and Elbow Surgeons score. (C) University of California Los Angeles score. (D) Western Ontario Shoulder Instability Index score. (E) Visual analog scale for pain score. IV, inverse variance.
ASES Score
Five studies (276 arthroscopic Bankart; 227 open Bankart) reported postoperative ASES scores, a shoulder-specific functional measure in which higher scores reflect better pain relief and functional performance. The pooled random-effects analysis demonstrated no statistically significant difference between procedures (P = .28). Heterogeneity was moderate (I2 = 40%) (Figure 4B).
UCLA Score
Six studies (186 arthroscopic Bankart; 144 open Bankart) reported postoperative UCLA scores, a composite measure of pain, function, and patient satisfaction in which higher scores indicate superior shoulder performance. The pooled random-effects analysis showed no statistically significant difference between arthroscopic and open Bankart repair (P = .41). Heterogeneity was high (I2 = 95%) (Figure 4C).
WOSI Score
Six studies (331 arthroscopic Bankart; 241 open Bankart) reported postoperative WOSI scores, a validated PROM in which lower scores indicate better shoulder-related quality of life. The pooled random-effects analysis demonstrated no statistically significant difference between arthroscopic and open Bankart repair (P = .40). Heterogeneity was substantial (I2 = 59%) (Figure 4D).
VAS for Pain Score
Three studies (186 arthroscopic Bankart; 194 open Bankart) reported postoperative VAS pain scores, in which lower scores reflect less pain. The pooled random-effects analysis demonstrated a borderline difference between procedures (P = .05). Heterogeneity was high (I2 = 98%) (Figure 4E).
Shoulder Postoperative ROM
External Rotation at the Side
Five studies (322 arthroscopic Bankart; 330 open Bankart) reported postoperative external rotation at the side. The pooled random-effects analysis demonstrated no statistically significant difference between procedures (P = .13). Heterogeneity was substantial (I2 = 70%) (Figure 5A).
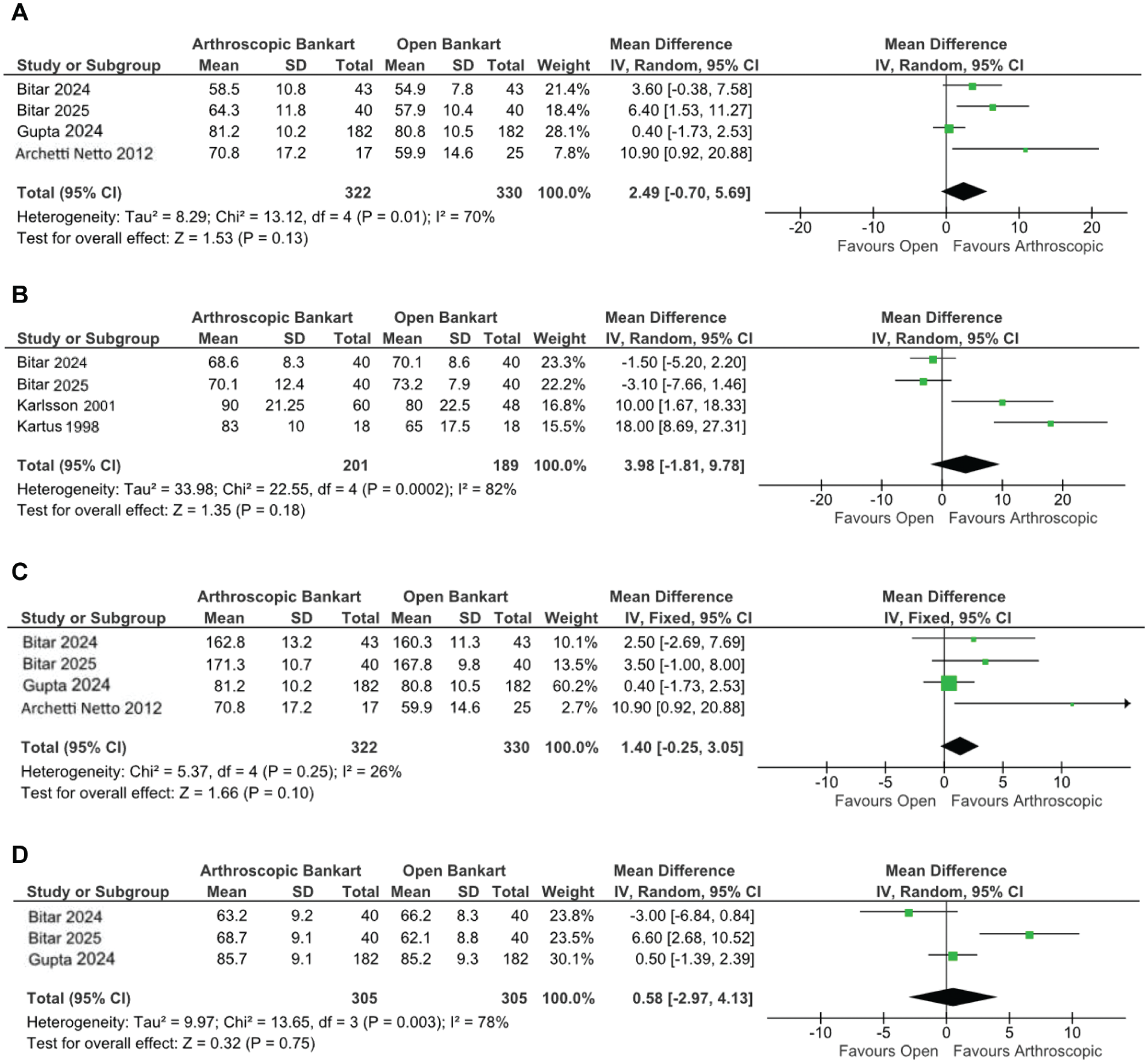
Shoulder postoperative range of motion forest plots. (A) External rotation at the side. (B) External rotation in abduction. (C) Forward flexion. (D) Internal rotation in 90° of abduction. IV, inverse variance.
External Rotation in Abduction
Five studies (201 arthroscopic Bankart; 189 open Bankart) reported postoperative external rotation in abduction. The pooled random-effects analysis demonstrated no statistically significant difference between arthroscopic and open Bankart repair (P = .18). Heterogeneity was high (I2 = 82%) (Figure 5B).
Forward Flexion
Five studies (322 arthroscopic Bankart; 330 open Bankart) reported postoperative forward flexion. The pooled fixed-effects analysis demonstrated no statistically significant differences between both groups (P = .10). Heterogeneity was moderate (I2 = 26%) (Figure 5C).
Internal Rotation in 90° of Abduction
Four studies (305 arthroscopic Bankart; 305 open Bankart) reported postoperative internal rotation. The pooled random-effects analysis demonstrated no statistically significant difference between arthroscopic and open Bankart repair (P = .75). Heterogeneity was high (I2 = 78%) (Figure 5D).
Shoulder Loss of ROM
Loss of External Rotation at the Side
Four studies (167 arthroscopic Bankart; 121 open Bankart) reported loss of external rotation at the side, defined as the postoperative reduction in external rotation compared to preoperative baseline. The pooled random-effects analysis demonstrated no statistically significant difference between arthroscopic and open Bankart repair (P = .11). Heterogeneity was substantial (I2 = 66%) (Figure 6A).
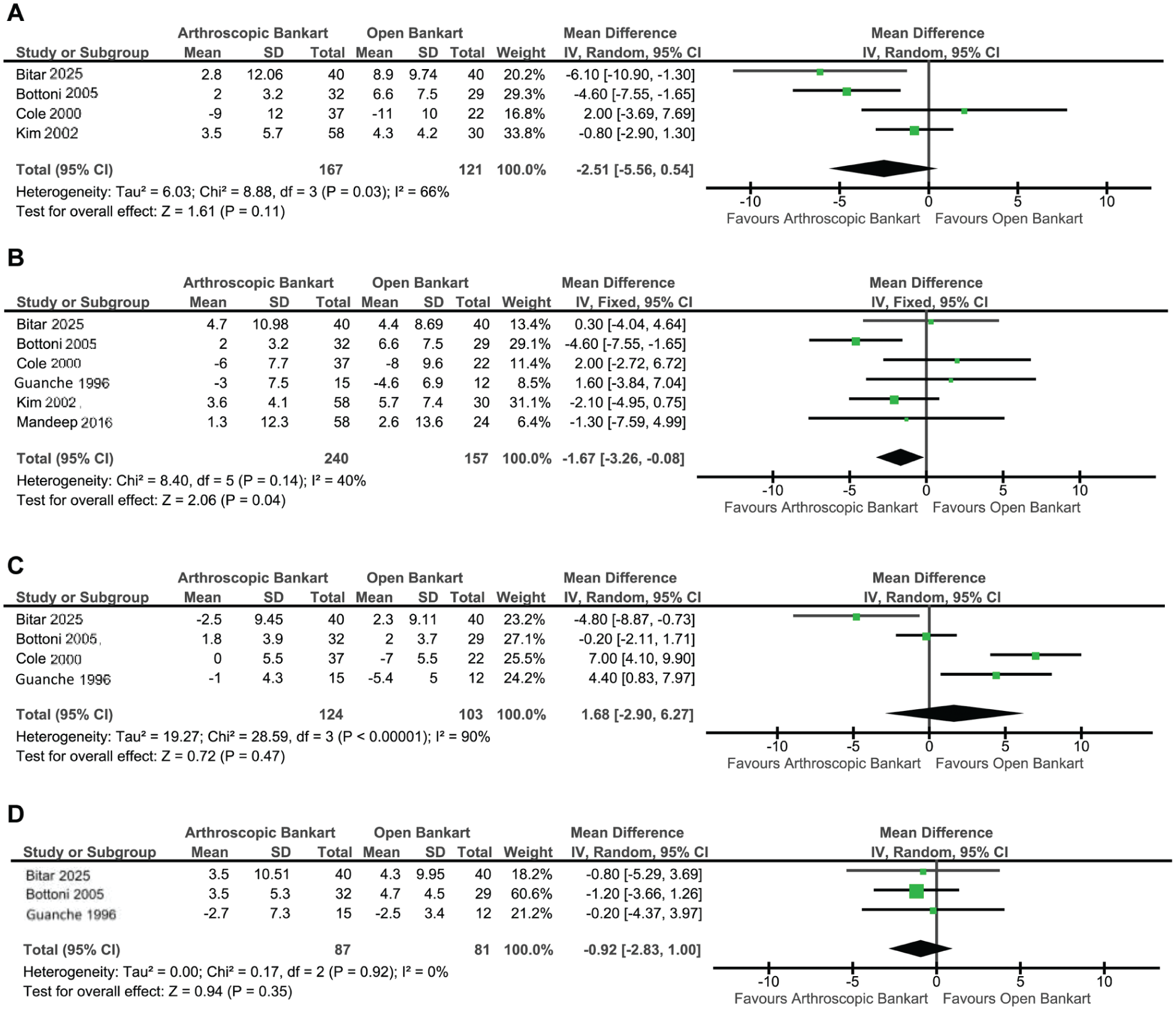
Shoulder loss of range of motion forest plots. (A) Loss of external rotation at the side. (B) Loss of external rotation in abduction. (C) Loss of forward flexion. (D) Loss of internal rotation at 90° of abduction. IV, inverse variance.
Loss of External Rotation in Abduction
Six studies (240 arthroscopic Bankart; 157 open Bankart) reported loss of external rotation in abduction, defined as the postoperative reduction relative to baseline. The pooled random-effects analysis demonstrated more loss of this movement in open Bankart repair compared to arthroscopic repair (MD, −1.67; 95% CI, −3.26 to −0.08; P = .04). Heterogeneity was moderate (I2 = 40%) (Figure 6B).
Loss of Forward Flexion
Four studies (124 arthroscopic Bankart; 103 open Bankart) reported loss of forward flexion, defined as postoperative reduction in forward flexion relative to baseline. The pooled random-effects analysis demonstrated no statistically significant difference between arthroscopic and open Bankart repair (P = .47). Heterogeneity was high (I2 = 90%) (Figure 6C).
Loss of Internal Rotation at 90° of Abduction
Three studies (87 arthroscopic Bankart; 81 open Bankart) reported loss of internal rotation at 90° of abduction compared to baseline. The pooled random-effects analysis demonstrated no statistically significant difference between arthroscopic and open Bankart repair (P = .35). Heterogeneity was low (I2 = 0%) (Figure 6D).
Perioperative Outcomes
Operative Time
Five studies (442 arthroscopic Bankart; 467 open Bankart) reported surgical duration. The pooled random-effects analysis demonstrated no statistically significant difference between techniques (P = .11). Heterogeneity was high (I2 = 100%) (Figure 7A).
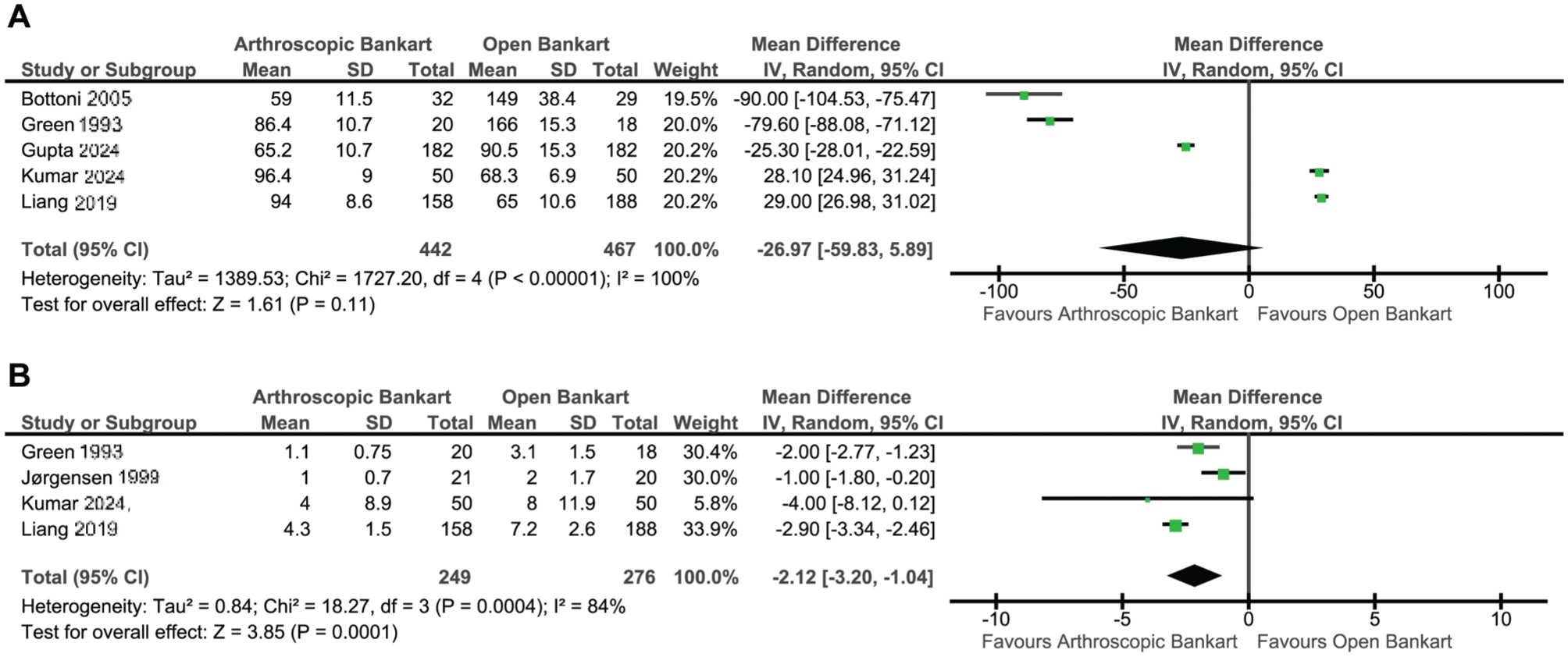
Perioperative outcome forest plots. (A) Operative time. (B) Hospital length of stay. IV, inverse variance.
Hospital Length of Stay
Four studies (249 arthroscopic Bankart; 276 open Bankart) reported hospital stay duration. The pooled random-effects analysis demonstrated a statistically significant difference, with arthroscopic Bankart repair associated with a shorter hospital stay compared to open repair (MD, −2.12; 95% CI, −3.20 to −1.04; P = .0001). Heterogeneity was high (I2 = 84%) (Figure 7B).
Complications
Reoperation
Seventeen studies (573 arthroscopic Bankart; 539 open Bankart) reported reoperation rates, defined as any subsequent surgical procedure performed to address persistent instability, hardware issues, or postoperative complications. The pooled fixed-effects analysis demonstrated a statistically significant difference, with arthroscopic Bankart repair associated with a higher likelihood of reoperation compared to open repair (RR, 2.15; 95% CI, 1.41-3.26; P = .0004). Across the contributing studies, most reported reoperations were revision procedures for recurrent instability, although a smaller number were performed for noninstability causes such as stiffness or implant-related problems. Heterogeneity was low (I2 = 0%) (Figure 8A).
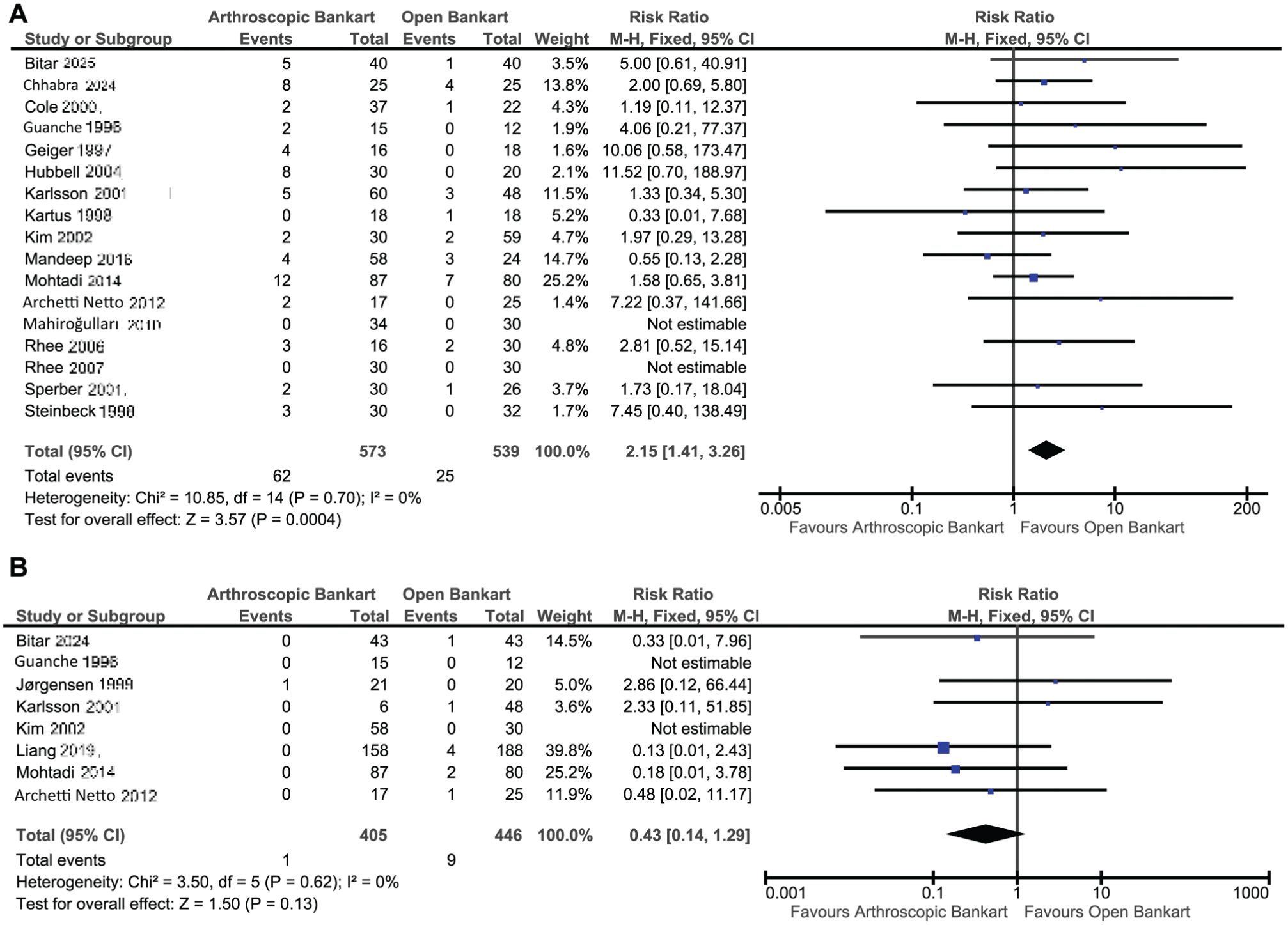
Complication Forest Plots. (A) Reoperations. (B) Infections. M-H, Mantel-Haenszel.
Infection
Eight studies (405 arthroscopic Bankart; 446 open Bankart) reported postoperative infection rates. The pooled fixed-effects analysis demonstrated no statistically significant difference between arthroscopic and open Bankart repair (P = .13). Heterogeneity was low (I2 = 0%) (Figure 8B).
Subgroup Analysis by Publication Period
To account for the evolution of surgical techniques over time, a subgroup analysis stratified studies by publication period (before 2010 vs 2010 onward) (Table 1).
Subgroup Meta-analysis of Outcomes Stratified by Publication Period (pre-2010 vs 2010 onward) a
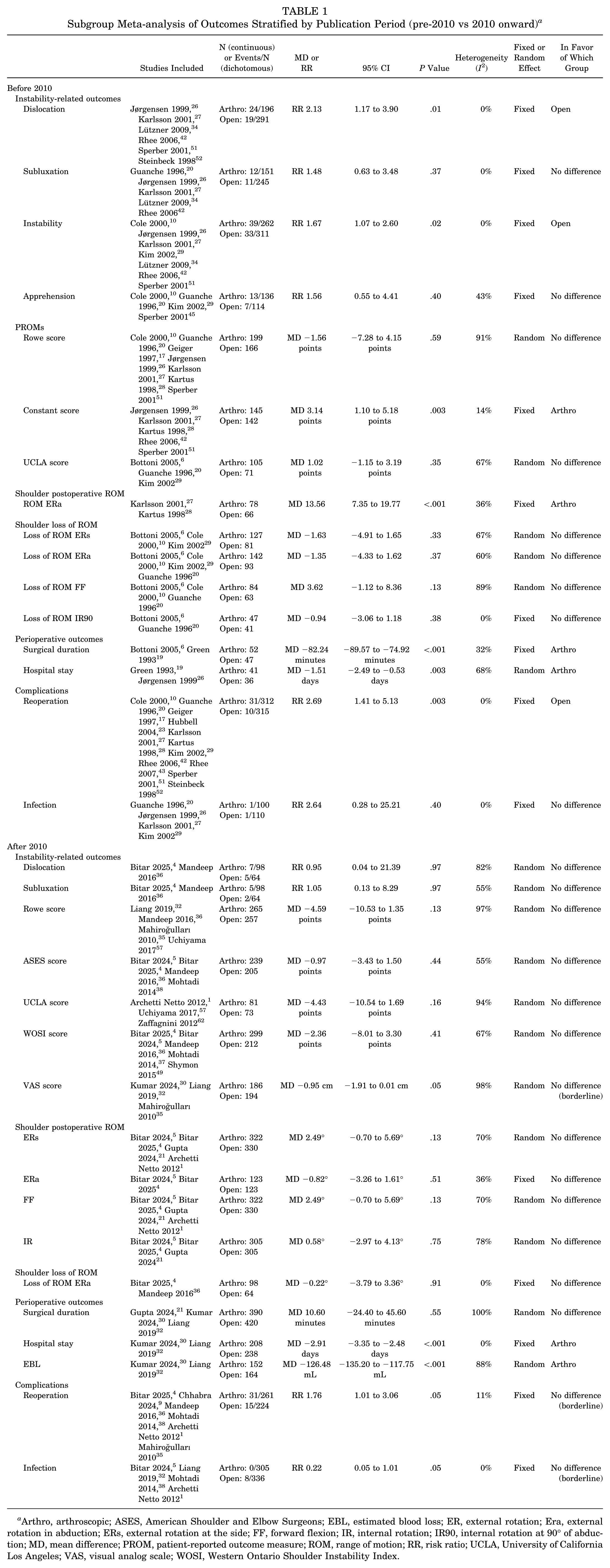
Arthro, arthroscopic; ASES, American Shoulder and Elbow Surgeons; EBL, estimated blood loss; ER, external rotation; Era, external rotation in abduction; ERs, external rotation at the side; FF, forward flexion; IR, internal rotation; IR90, internal rotation at 90° of abduction; MD, mean difference; PROM, patient-reported outcome measure; ROM, range of motion; RR, risk ratio; UCLA, University of California Los Angeles; VAS, visual analog scale; WOSI, Western Ontario Shoulder Instability Index.
Studies Published Before 2010
In the pre-2010 subgroup, instability-related outcomes showed a significantly higher risk of postoperative dislocation (RR, 2.13; 95% CI, 1.17-3.90; P = .01) and overall instability (RR, 1.67; 95% CI, 1.07-2.60; P = .02) after arthroscopic repair compared with open repair, favoring open repair. No significant differences were observed for subluxation (P = .37) and apprehension (P = .40).
Regarding patient-reported outcomes, Rowe (P = .59) and UCLA (P = .35) scores did not differ between groups, whereas the Constant score favored arthroscopic repair (MD, 3.14 points; 95% CI, 1.10-5.18 points; P = .003). In postoperative shoulder motion, arthroscopic repair demonstrated greater external rotation in abduction (MD, 13.56; 95% CI, 7.35-19.77; P < .001), while external rotation at the side, forward flexion, and internal rotation losses relative to baseline showed no significant differences (external rotation at the side loss: P = .33; external rotation in abduction loss: P = .37; forward flexion loss: P = .13; internal rotation at 90° of abduction loss: P = .38).
For perioperative outcomes, arthroscopic repair was associated with shorter surgical duration (MD, −82.24 minutes; 95% CI, −89.57 to −74.92 minutes; P < .001) and shorter hospital stay (MD, −1.51 days; 95% CI, −2.49 to −0.53 days; P = .003). In terms of complications, reoperation occurred more frequently after arthroscopic repair (RR, 2.69; 95% CI, 1.41 to 5.13; P = .003), whereas infection rates were comparable (P = .40).
Studies Published From 2010 Onward
Among studies published from 2010 onward, instability-related outcomes did not differ between arthroscopic and open repair for dislocation (P = .97) or subluxation (P = .97).
Patient-reported outcomes similarly demonstrated no significant differences across Rowe (P = .13), ASES (P = .44), UCLA (P = .16), WOSI (P = .41), or VAS pain (P = .05) scores. Postoperative shoulder ROM also showed no differences between techniques for external rotation at the side (P = .13), external rotation in abduction (P = .51), forward flexion (P = .13), or internal rotation (P = .75). Loss of external rotation in abduction relative to baseline likewise did not differ between groups (P = .91).
In perioperative outcomes, hospital length of stay favored arthroscopic repair (MD, −2.91 days; 95% CI, −3.35 to −2.48 days; P < .001), as did estimated blood loss (MD mL, −126.48; 95% CI, −135.20 to −117.75 mL; P < .001), while operative time was similar (P = .55). Complication rates did not differ significantly between techniques for reoperation (P = .05) or infection (P = .05).
Discussion
Our meta-analysis demonstrated that arthroscopic and open Bankart repair yield comparable clinical outcomes across the major domains of postoperative instability, patient-reported outcomes, shoulder ROM, perioperative parameters, and complication rates, with only isolated differences favoring one technique in specific measures. Importantly, subgroup analysis by publication period showed that the instability differences seen in older studies were no longer present in studies published from 2010 onward, supporting the view that advances in arthroscopic technique have narrowed the historical gap between approaches. Several additional differences observed in earlier studies, including Constant score, external rotation in abduction, operative time, and reoperation rates, were likewise not reproduced in more recent cohorts.
Notably, most of the individual comparative studies included in this review similarly reported no statistically significant differences between arthroscopic and open Bankart repair across instability recurrence, functional scores, and ROM outcomes, although a few studies observed modest differences favoring one technique in specific parameters such as motion preservation or recurrence patterns. Importantly, unlike several earlier systematic reviews,18,31,35,40 we found no significant differences in instability-related outcomes, suggesting that contemporary arthroscopic techniques have reached a level of performance equivalent to open repair in restoring shoulder stability. These findings indicate that, in modern practice, the choice between arthroscopic and open Bankart repair may be guided more by patient-specific and surgeon-specific factors rather than inherent superiority of one technique over the other.
Regarding perioperative outcomes, arthroscopic repair was associated with a shorter hospital stay, while operative time was comparable between approaches. Reduced length of stay likely reflects the minimally invasive nature of arthroscopy, lower postoperative pain levels, and accelerated early mobilization protocols. 14 Additionally, enhanced perioperative pathways, such as outpatient management, regional anesthesia, and improved arthroscopic instrumentation, have further streamlined postoperative recovery. The existing literature also supports these trends, with similar reports of reduced hospitalization in arthroscopic stabilization for other shoulder conditions. 48 However, it is important to recognize that hospital stay is influenced by institutional policy, surgeon preference, comorbidities, and patient expectations, in addition to the surgical technique. The high heterogeneity observed in perioperative analyses (operative time I2 = 100%; hospital stay I2 = 84%) likely reflects differences in health care systems, surgical experience, operative workflow, and discharge protocols across institutions and time periods.
In terms of postoperative ROM, we observed no significant differences for most movements, including external rotation at the side or in abduction, forward flexion, and internal rotation. 15 Only loss of external rotation in abduction favored arthroscopy, demonstrating slightly better preservation (MD, −1.67). This difference likely reflects reduced capsular dissection and less subscapularis manipulation in arthroscopic procedures compared to open techniques, in which subscapularis takedown or splitting can predispose to subtle stiffness. 55 These findings are aligned with biomechanical and clinical literature showing that open Bankart repair may lead to mild postoperative motion restriction due to capsular overtightening or scarring. 3 Nonetheless, postoperative ROM is multifactorial, with contributions from rehabilitation protocols, patient adherence, tissue quality, and preoperative ROM, which must be considered alongside surgical approach. The relatively high heterogeneity observed in several ROM analyses (eg, external rotation in abduction I2 = 82%; internal rotation in 90° of abduction: I2 = 78%) may similarly reflect differences in measurement techniques, rehabilitation strategies, and baseline mobility across study populations.
PROMs, including Rowe, ASES, UCLA, WOSI, and VAS scores, showed no significant differences between arthroscopic and open repair. Although the VAS score approached statistical significance (P = .05), this finding should be interpreted cautiously given the very high heterogeneity (I2 = 98%) and limited number of contributing studies, and therefore was not considered evidence of a consistent difference between techniques. This suggests that, from the patient's perspective, both techniques deliver equivalent functional recovery, symptom relief, and quality of life. However, several PROM analyses demonstrated substantial statistical heterogeneity (eg, Rowe score: I2 = 96%; UCLA score: I2 = 95%; VAS score: I2 = 98%), likely reflecting differences in follow-up duration, patient activity levels, surgical techniques across decades, and variability in rehabilitation protocols among included studies. Comparable PROMs are expected in the setting of modern arthroscopy, where improved visualization, anchor design, and capsulolabral restoration mimic the biomechanical intent of open repair. 7 The convergence of outcomes also likely reflects the strong influence of rehabilitation quality, patient motivation, expectations, and concomitant pathology on functional recovery, which may outweigh subtle technical distinctions between procedures. 39
Instability-related outcomes constitute a central point of comparison, and here our analysis found no significant differences in dislocation, subluxation, overall instability, or apprehension. This finding is consistent with the majority of the included comparative studies, many of which individually reported similar recurrence rates between arthroscopic and open repair, particularly in more recent cohorts using modern suture anchor constructs. This contrasts with earlier meta-analyses, including those of Freedman et al, 14 Mohtadi et al, 37 Lenters et al, 31 Chen et al, 8 Wang et al, 60 and Gao et al, 16 which consistently reported higher recurrence rates after arthroscopic repair, particularly in the pre–suture anchor and early anchor eras. Our publication period subgroup analysis supports this temporal explanation, as the excess risk of dislocation and overall instability with arthroscopic repair was observed only in the pre-2010 subgroup and not in studies published thereafter. This interpretation is also supported by the implant and technique data summarized in Supplementary Table 1, in which earlier arthroscopic studies more often used transglenoid sutures, suture punches, and tack-based constructs, whereas more recent studies predominantly used modern suture anchor systems. Other advantages favoring arthroscopy in earlier studies, including Constant score, external rotation in abduction, and operative time, were likewise not reproduced in more recent cohorts. The discrepancy likely reflects substantial evolution in arthroscopic techniques, including the transition from transglenoid sutures and tacks to high-strength suture anchors, improved anchor placement strategies, understanding of capsular shifts, and better identification and management of engaging Hill-Sachs and glenoid bone loss. 47 Increased surgeon experience and refinement of postoperative rehabilitation also contribute to the improved stability seen today. 22 Still, instability outcomes remain influenced by patient age, participation in collision sports, hyperlaxity, glenoid bone loss, and number of preoperative dislocations, factors that require individualized consideration when selecting the optimal surgical approach. 45
In terms of complications, the only significant difference was the higher reoperation rate after arthroscopic repair, despite comparable recurrence rates. Review of the contributing studies suggests that many of these reoperations were instability-related revision procedures, but not exclusively so, as some were performed for stiffness or implant-related problems. At the same time, several studies reported recurrent instability that was managed nonoperatively or for which patients declined revision, indicating that reoperation should be interpreted as a marker of clinically significant failure requiring further surgery rather than as a direct surrogate for all postoperative instability events. These trends have been previously reported in the literature, where the ease of reoperation after arthroscopy and the lower threshold for addressing symptoms arthroscopically may contribute to higher recorded revision rates.2,50 Complication risk overall remains low with both techniques and is shaped by factors including rehabilitation adherence, tissue quality, concomitant pathology, and technical nuance.11,59
Beyond the comparison of surgical techniques, several additional considerations are crucial when selecting appropriate treatment for patients with recurrent anterior shoulder instability. Glenoid bone loss, the presence of an off-track Hill-Sachs lesion, the number and severity of prior dislocations, the level of sports participation, ligamentous laxity, and patient age all significantly affect failure risk and may shift the balance toward either arthroscopic repair, open Bankart repair, or alternative procedures such as Latarjet or remplissage. 61 Surgeon expertise and institutional resources also play nonnegligible roles, with high-volume arthroscopic surgeons achieving outcomes comparable to or better than those of traditional open procedures.13,46
In conclusion, our findings indicate that arthroscopic and open Bankart repair deliver largely equivalent outcomes across all major clinical domains, with the few observed differences aligning with the inherent characteristics of each technique. Arthroscopy, as the less invasive approach, achieved comparable stability to open repair while offering modest advantages in functional preservation and perioperative recovery. In contrast, open repair maintained a slightly lower reoperation rate. Taken together, these results suggest that in contemporary practice, where arthroscopic methods have undergone substantial refinement, arthroscopic repair may represent a favorable option for many patients, provided that anatomic features and surgeon expertise are appropriate.
Limitations
This meta-analysis has several limitations that should be acknowledged. First, although 32 comparative studies were included overall, most individual pooled outcomes were informed by only a limited number of studies (commonly 3-8, with the exception of reoperation), which reduces the statistical precision of several estimates and may limit the robustness of certain comparisons. In addition, outcome reporting varied substantially across studies, contributing to heterogeneity in several pooled analyses.
Second, although a substantial proportion of the included studies were prospective in design, a meaningful number of retrospective cohorts remain, introducing risks of selection bias and incomplete adjustment for baseline instability characteristics.
Third, surgical techniques varied across studies and over time, including differences in the number and configuration of suture anchors, capsular plication methods, management of Hill-Sachs lesions, and rehabilitation protocols. Studies involving Bankart repair combined with concomitant procedures such as remplissage were excluded. However, reporting of adjunctive procedures was not uniform across all included studies, and therefore unreported variation in associated surgical management cannot be completely excluded. Although we addressed this in part through subgroup analysis by publication period, publication year remains only an approximate surrogate for surgical era and may not fully capture the exact technical characteristics used in each study.
Fourth, several instability-related endpoints relied on subjective reporting rather than standardized examination protocols, and reoperation was not uniformly characterized across studies, with the indication for reoperation variably reported.
Fifth, follow-up durations ranged widely, from short-term evaluations of approximately 1 year to long-term analyses exceeding 10 to 15 years, limiting comparability between early and late postoperative outcomes.
Finally, patient characteristics, including age, sports participation, activity level, chronicity of instability, and limb dominance, were variably reported and not always balanced between arthroscopic and open cohorts. Because this meta-analysis was based on aggregated study-level data, control for important preoperative confounders such as baseline activity level, extent of glenoid or humeral bone loss, number of prior instability events, and prior surgical history was not feasible, especially when these factors were inconsistently reported or not stratified across studies. In particular, glenoid bone loss was not reported with sufficient consistency or granularity to determine whether open Bankart repair may confer relative benefit in patients with greater bone loss within the soft tissue stabilization spectrum, or to identify thresholds at which open Bankart repair might be preferentially selected over arthroscopic repair. In addition, revision surgery and mixed primary/revision cohorts without separable data were excluded, so the present findings should be interpreted primarily in the context of primary Bankart repair rather than revision stabilization.
These limitations underscore the need for future high-quality randomized trials with standardized outcome definitions, consistent reporting of anatomic risk factors, and clear delineation of modern surgical techniques to better characterize the comparative effectiveness of arthroscopic versus open Bankart repair.
Conclusion
This meta-analysis shows that arthroscopic and open Bankart repair achieve similarly effective stability and functional recovery in patients with traumatic anterior shoulder instability. No significant differences were found across major clinical domains, including instability outcomes, patient-reported measures, ROM, and most perioperative parameters. Arthroscopic repair offered modest advantages, such as shorter hospital stay and slightly better preservation of external rotation in abduction, while open repair showed a slightly lower reoperation rate, without corresponding differences in recurrent instability. Overall complication profiles were comparable, and neither technique demonstrated meaningful differences in pain, global shoulder function, or quality of life.
These findings indicate that modern arthroscopic stabilization has reached a performance level similar to open repair while offering the benefits of minimally invasive surgery, whereas open Bankart repair continues to represent a reliable option in selected patients, particularly when anatomic risk factors or surgical preference support its use. The subgroup findings further suggest that historical differences between techniques were driven mainly by earlier-era studies rather than contemporary practice. Taken together, these results reinforce the importance of individualized surgical decision-making, integrating patient age, sporting demands, anatomic considerations, tissue quality, and surgeon expertise.
Supplemental Material
sj-docx-1-ajs-10.1177_03635465261443999 – Supplemental material for Arthroscopic vs Open Bankart Repair for Anterior Shoulder Instability: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-1-ajs-10.1177_03635465261443999 for Arthroscopic vs Open Bankart Repair for Anterior Shoulder Instability: A Systematic Review and Meta-analysis by Marc Boutros, Guy Awad, Jean-Pierre Saad, Reina Khatib, Zina Smadi and Bassem Elhassan in The American Journal of Sports Medicine
Supplemental Material
sj-docx-2-ajs-10.1177_03635465261443999 – Supplemental material for Arthroscopic vs Open Bankart Repair for Anterior Shoulder Instability: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-2-ajs-10.1177_03635465261443999 for Arthroscopic vs Open Bankart Repair for Anterior Shoulder Instability: A Systematic Review and Meta-analysis by Marc Boutros, Guy Awad, Jean-Pierre Saad, Reina Khatib, Zina Smadi and Bassem Elhassan in The American Journal of Sports Medicine
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.