
Abstract
Background:
Graft failure after anterior cruciate ligament (ACL) reconstruction (ACLR) may be influenced by both extrinsic exposure and intrinsic patient susceptibility. A contralateral ACL rupture could reflect an inherent predisposition to ligament injury.
Purpose:
To determine whether a history of bilateral native ACL ruptures increases the risk of graft failure after primary ACLR.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
A total of 7718 consecutive patients who underwent primary ACLR by a single surgeon (2003-2022) were included. Graft failure, defined as a clinically and magnetic resonance imaging–confirmed rupture, was compared between patients with bilateral versus unilateral native ACL ruptures. Multivariable logistic regression identified independent predictors, including age, sex, Tegner score, sport type, and a history of bilateral rupture.
Results:
The cohort included 6327 patients with isolated native ACL rupture and 1391 patients with bilateral native ACL rupture. The overall graft failure rate was 6% (461-7718), with a mean follow-up of 135.9 months. Patients with bilateral ACL ruptures had a higher failure rate (9.3%) than those with unilateral injuries (5.2%) (P < .0001). Independent predictors included younger age (odds ratio [OR], 0.92 [95% CI, 0.90-0.93]; P < .0001), male sex (OR, 1.46 [95% CI, 1.10-1.96]; P = .0089), higher Tegner score (OR, 1.09 [95% CI, 1-1.19]; P = .043), and bilateral rupture (OR, 1.34 [95% CI, 1.03-1.73]; P = .028).
Conclusion:
Bilateral native ACL rupture independently increases the risk of graft failure after ACLR. This finding supports its use as a marker of intrinsic vulnerability that may warrant targeted preventive or surgical strategies.
Keywords
Anterior cruciate ligament (ACL) rupture is a common and severe injury among young athletes, with substantial risk of reinjury and graft failure after reconstruction. 33 While extrinsic factors such as sport exposure and contact mechanisms are widely recognized, there is growing evidence that certain individuals may possess intrinsic characteristics predisposing them to ligamentous injury. One potential marker of such predisposition is bilateral ACL rupture, which may reflect underlying patient-specific risk factors such as neuromuscular control deficits, anatomical variations, or hormonal influences.1,18,20
Bilateral ACL injuries are reported in approximately 2% to 4% of patients undergoing ACL reconstruction (ACLR). 24 However, this rate can vary substantially depending on the population studied and specific exposure risk factors, including the level and type of sport.3,4,7
These cases provide a unique model for assessing whether graft failure risk is increased by intrinsic susceptibility rather than by surgical or rehabilitation-related factors. Previous studies have shown that patients who experience ACL ruptures in both knees often display higher rates of subsequent graft failure or new contralateral ACL injuries, indicating a potential underlying susceptibility rather than isolated traumatic events.25,26,34 Identifying such a population could influence surgical decision-making, graft choice, and postoperative strategies tailored to higher-risk patients.
This study aimed to compare graft failure rates after ACLR between patients with bilateral ACL rupture and those with unilateral injuries. We hypothesized that patients with bilateral ACL ruptures would exhibit a significantly higher rate of graft failure, consistent with an intrinsic risk profile.
Methods
Study Design and Participants
Institutional review board approval (IRB) (Conseil d’Orientation Scientifique Ramsay Santé Comité d’Ethique–IRB COS-RGDS-2025-10-009-SONNERY-COTTET-B) was granted for this study, and all patients provided informed consent to participate. This retrospective cohort study included consecutive patients who underwent arthroscopic primary ACLR by a single surgeon (B.S.-C.) between January 2003 and March 2022, identified from the Scientific Anterior Cruciate Ligament Network International (SANTI) database. Patients were excluded if they underwent ACL revision or major concomitant procedures (eg, multiligament reconstruction, high tibial osteotomy, or slope osteotomy), were skeletally immature, or underwent ACL repair. All eligible consecutive patients were included to minimize selection bias. The surgical technique involved anatomic ACLR using autografts: bone-patellar tendon-bone, quadriceps tendon, or hamstring tendon, with or without lateral extra-articular procedures (LEAP) selected based on patient age, activity level, and surgeon preference, with standardized femoral and tibial fixation. Because these procedures were performed at the surgeon's discretion based on evolving clinical practice patterns, but not according to a predefined risk-based algorithm, and were not related to the intrinsic exposure of interest (bilateral rupture history), LEAP status was not included as a covariate in the statistical model. Postoperative rehabilitation adhered to a structured protocol emphasizing early mobilization within the first week, progressive strengthening over 3 to 6 months, and return-to-sport clearance at 6 to 9 months, contingent on achieving symmetrical quadriceps strength, hop test performance, and dynamic knee stability. The epidemiology of ACL graft failure was assessed using incidence data stratified by the presence of bilateral native ACL ruptures, as depicted in the patient flowchart (Figure 1). Bilateral ACL rupture was defined as a history of native ACL rupture in the contralateral knee occurring either before or after the index ACLR. Although the timing of the contralateral injury relative to the index procedure was available in the database, it was not incorporated into the present analysis, as the primary objective was to evaluate bilateral rupture history as a marker of intrinsic patient susceptibility rather than as a time-dependent exposure. Potential risk factors—including age, sex, Tegner activity level (preinjury or patient-reported), and type of sport (pivot-contact sports, eg, soccer and basketball vs nonpivot sports, eg, running and cycling)—were analyzed for their association with graft failure. These factors were examined within the cohorts of 6327 patients with unilateral ACLR and 1391 patients with bilateral ACLR to identify independent predictors of rupture during follow-up (minimum 2 years).
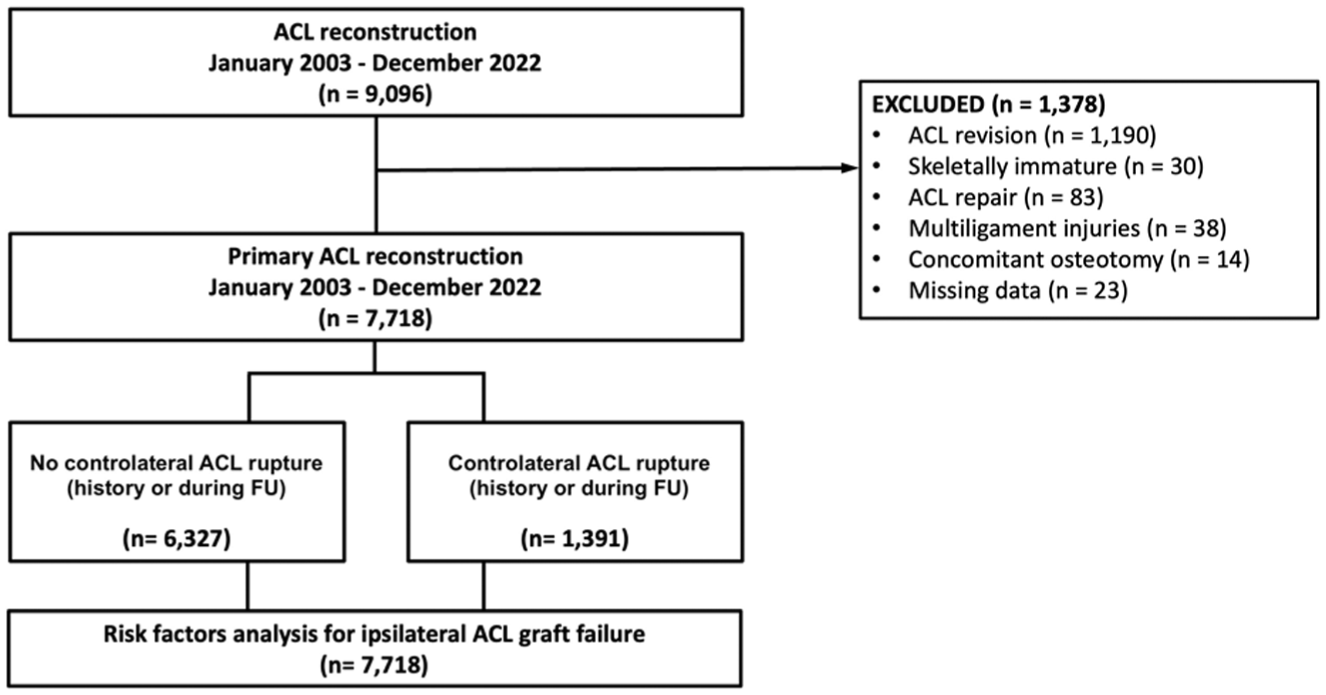
Study flowchart. ACL, anterior cruciate ligament; FU, follow-up.
Outcome Measures
The primary endpoint was ACL graft failure, defined as a confirmed ipsilateral graft rupture diagnosed by clinical evaluation (positive Lachman and pivot-shift tests) and confirmed on magnetic resonance imaging. Covariates included age, sex, Tegner activity level, type of sport (pivot-contact vs nonpivot), and whether the ACL rupture was bilateral or not during the follow-up study.
Statistical Analysis
Descriptive statistics were reported for both continuous and categorical variables. For quantitative data, this included the number of filled and missing values, the arithmetic mean, standard deviation, median, first and third quartiles, and minimum and maximum. Group comparisons were performed using chi-square tests for categorical variables and t tests for continuous variables, with normality assumptions verified. Logistic regression modeling was used to determine independent risk factors for graft failure. Variables with P < .05 in univariate analysis were included in the multivariate model. Multicollinearity was assessed using variance inflation factors, and model fit was evaluated with the Hosmer-Lemeshow test. Results are presented as odds ratios (OR) with 95% CIs. Analyses were performed using SAS software (Version 9.4, SAS Institute Inc).
Results
Patient Characteristics
Among the 7718 patients, 6327 had unilateral ACLR, and 1391 (18%) had bilateral native ACL ruptures (Figure 1). The mean follow-up was 135.9 ± 60.02 months. Patients with bilateral ruptures were younger on average (mean age, 27.3 ± 9.7 years) compared with those with unilateral injuries (mean age, 28.8 ± 10.1 years; P = .012). Men comprised 72.1% of the cohort, and the frequency of bilateral ACL rupture was slightly higher among men than women (18.8% vs 16%; P = .004). A higher proportion of patients with bilateral ACL rupture participated in pivot-contact sports (70% vs 57%; P < .001). Also, 4133 (53.5%) patients underwent combined ACL and LEAP reconstruction, whereas 3585 (46.5%) underwent isolated ACLR. Baseline demographic and clinical characteristics are shown in Table 1. Graft failure rates and between-group comparisons are summarized in Table 2.
Patient Characteristics a
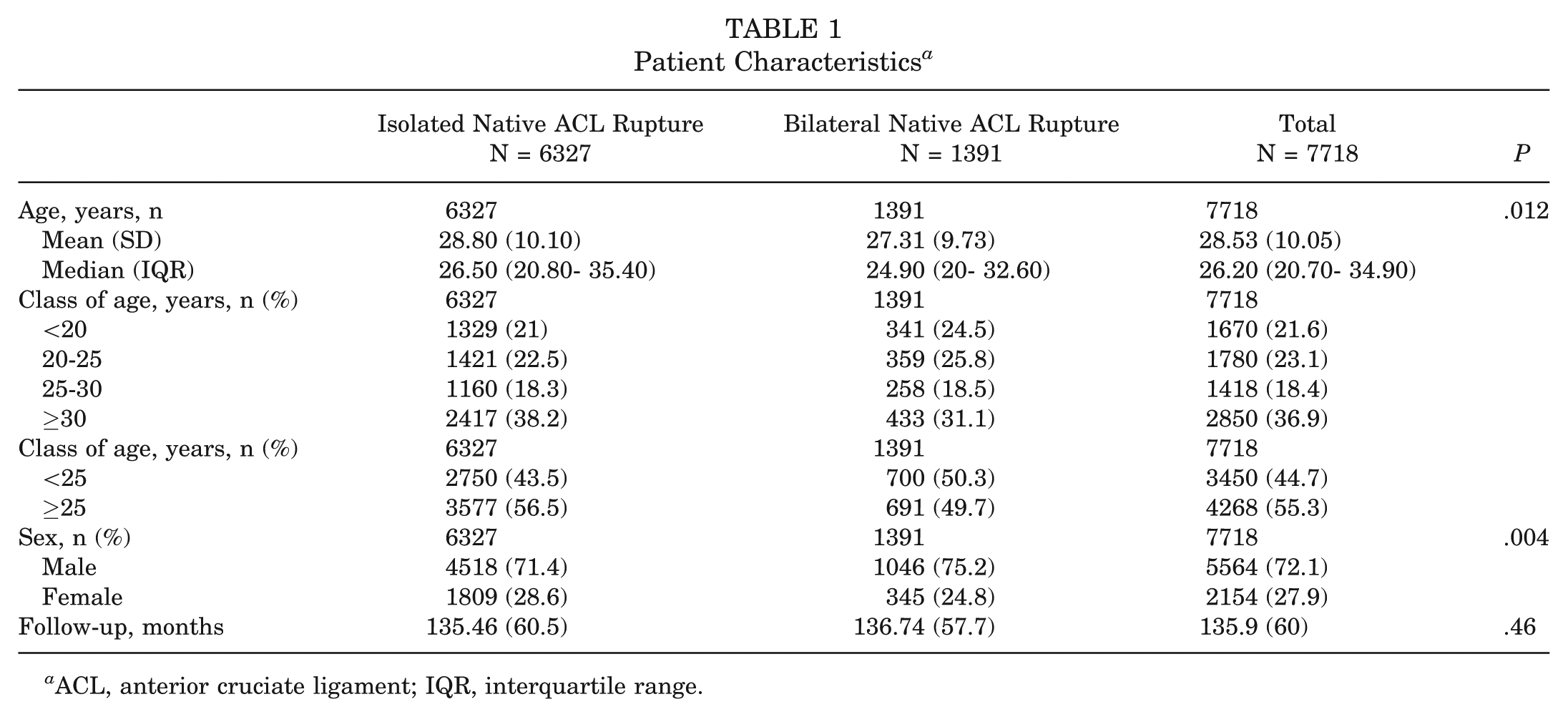
ACL, anterior cruciate ligament; IQR, interquartile range.
Sports Analysis a
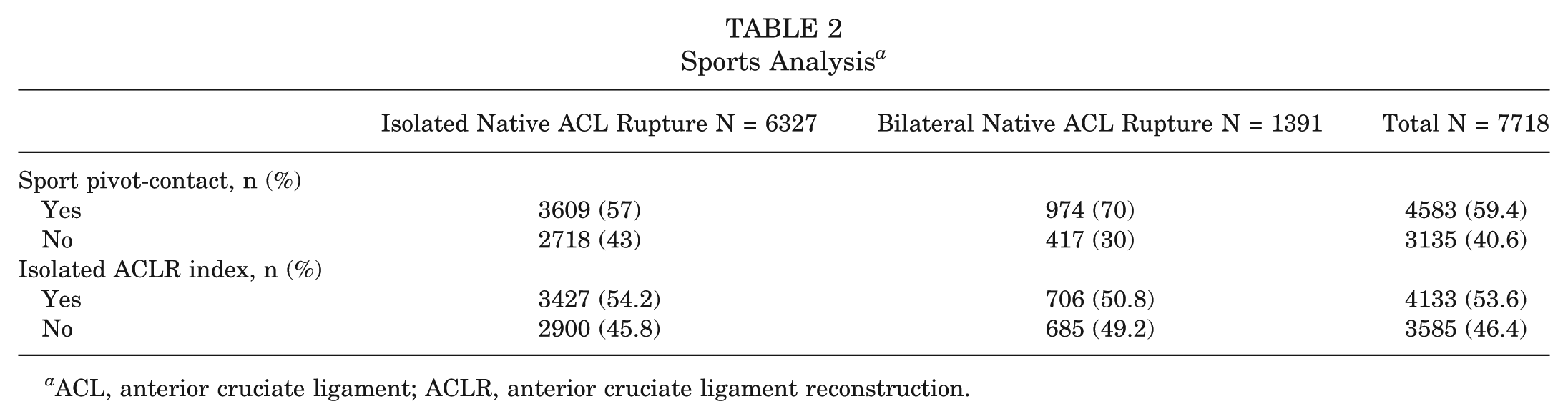
ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction.
Graft Failure
The overall graft failure rate was 6% (461-7718). The rate was significantly higher in patients with bilateral ACL ruptures (9.3%) compared with those with unilateral ruptures (5.2%) (P < .0001) (Table 3). Multivariate logistic regression analysis identified younger age, male sex, higher Tegner score, and bilateral ACL rupture as independent predictors of graft failure (Table 4; Figure 2, forest plot of odds ratios). Each additional year of age reduced the odds of failure by 8% (OR, 0.92 [95% CI, 0.90-0.93]; P < .0001). Male sex was associated with a higher risk than female sex (OR, 1.46 [95% CI, 1.10-1.96]; P = .0089). Patients with higher Tegner scores were more likely to experience graft failure (OR, 1.09 [95% CI, 1-1.19]; P = .0428).
Graft Failure a
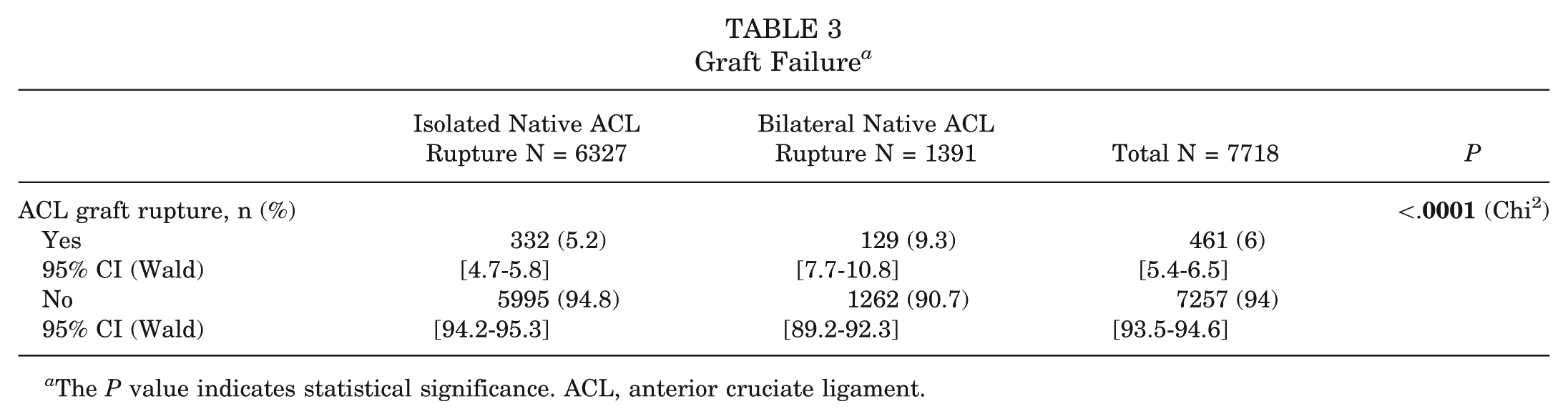
The P value indicates statistical significance. ACL, anterior cruciate ligament.
Multivariate Logistic Regression for Graft Failure a
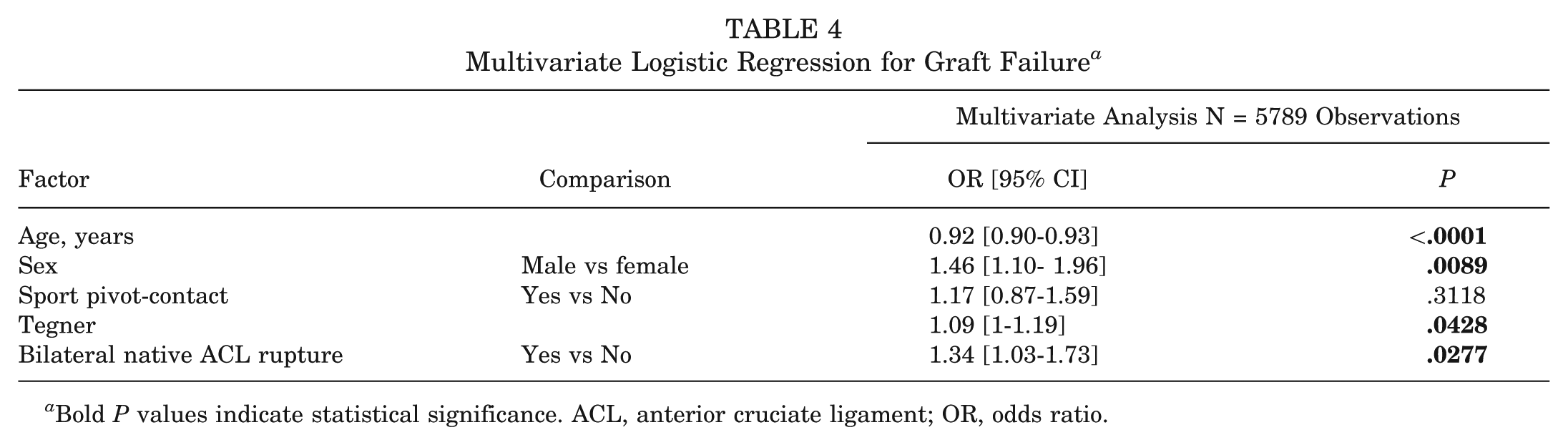
Bold P values indicate statistical significance. ACL, anterior cruciate ligament; OR, odds ratio.
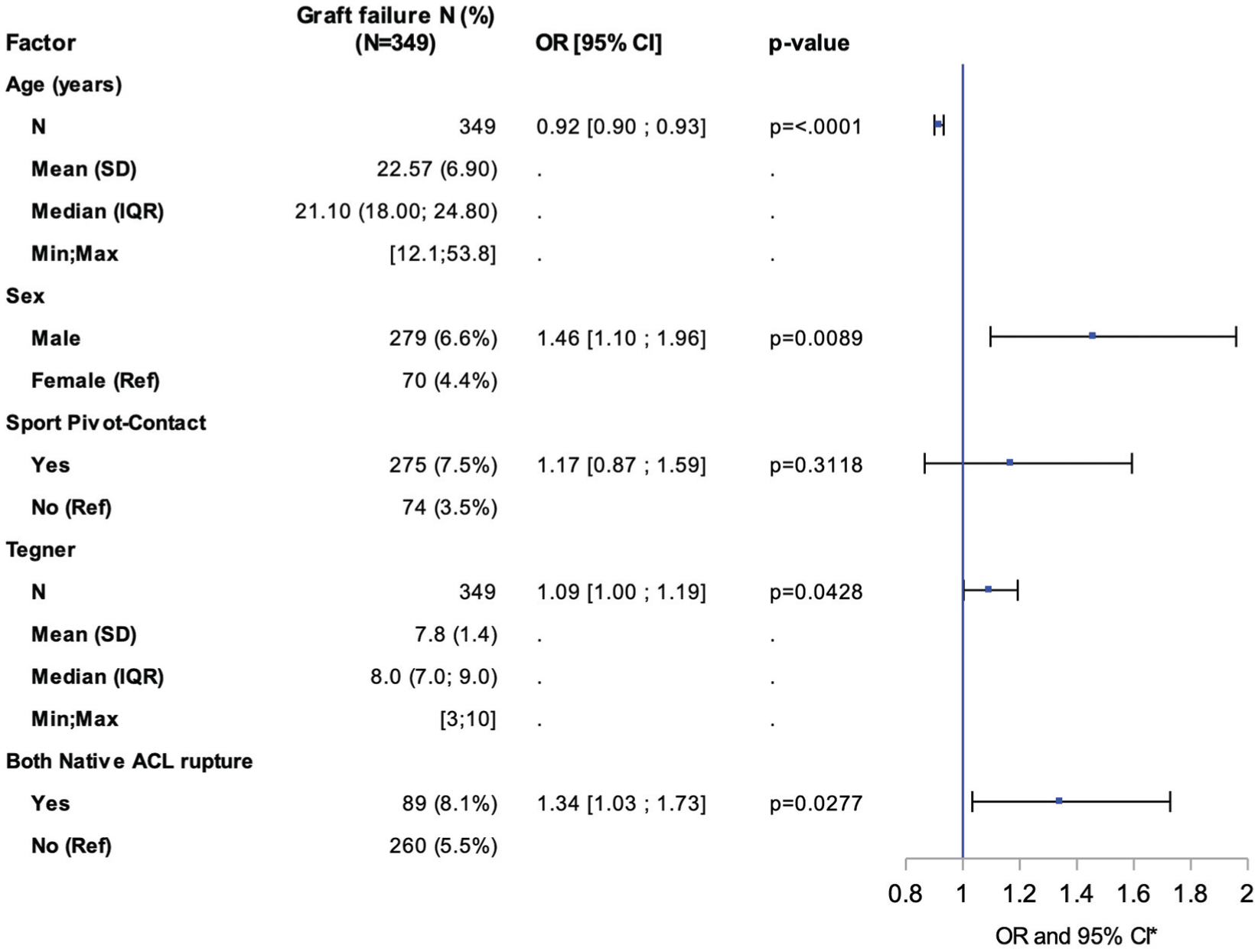
Forest plot of ORs of graft failure. ACL, anterior cruciate ligament; IQR, interquartile range; OR, odds ratio; Ref, reference.
Above all, bilateral ACL rupture emerged as an independent predictor of graft failure, with affected patients demonstrating an almost 1.4-fold increased risk compared with those sustaining unilateral ruptures (OR, 1.34 [95% CI, 1.03-1.73]; P = .0277).
Discussion
The principal finding of this large cohort study is that a history of bilateral native ACL ruptures is an independent predictor of graft failure after primary ACLR. Patients who sustained ACL injuries in both knees had an almost 1.4-fold higher risk of subsequent graft rupture compared with those with a unilateral injury, even after adjustment for age, sex, activity level, and sport type. This finding supports the hypothesis that repeated ligament injury may reflect an intrinsic susceptibility rather than exposure alone, and that bilateral ACL rupture can serve as a pragmatic clinical marker of such intrinsic vulnerability.
Previous work has shown that both ipsilateral graft rupture and contralateral ACL injury remain the most frequent causes of reinjury after ACLR, particularly among young, active athletes.20,25,26,34 The reinjury rate observed in the present study (6%) aligns with these reports, which typically range from 5% to 10% after primary reconstruction.21,25 Notably, the 9.3% failure rate among patients with bilateral native ACL ruptures underscores a clinically meaningful difference that cannot be fully explained by sport exposure alone.
Bilateral ACL ruptures have been reported in approximately 2% to 4% of patients after ACLR, 24 but this frequency rises markedly in high-demand cohorts such as professional skiers or football players, where contralateral injuries occur3,4,7 in up to 30%. These findings support the concept that repetitive ligament failure may identify a subgroup with intrinsic risk factors, either structural, neuromuscular, or genetic, that predispose to recurrent injury despite technically successful reconstruction and rehabilitation.
Several intrinsic factors have been proposed to explain susceptibility to repeated ACL injury. Anatomical morphology is among the most widely studied. A narrow intercondylar notch has been identified as a risk factor for both primary and secondary ACL rupture. 28 Hughes et al 15 recently demonstrated that a notch width <16 mm increases the odds of graft failure by 5-fold. Likewise, the posterior tibial slope (PTS) influences anterior tibial translation and ACL strain. 32 Webb et al 33 showed that an increased PTS, particularly ≥12°, significantly increases the risk of reinjury after ACLR, a finding confirmed by a 2022 meta-analysis.16,32 Druel et al 5 further observed that a steeper medial PTS was associated with bilateral ACL rupture, suggesting that this anatomical feature may act bilaterally and compound graft stress. However, the association between PTS and graft rupture remains debated, as Hinz et al 14 recently found no relationship between slope and failure rates after anatomic ACLR.
In addition to bony morphology, neuromuscular control deficits are thought to play a central role. Abnormal landing mechanics, reduced knee flexion, excessive valgus moments, and altered hamstring-quadriceps activation patterns have been consistently linked to ACL injury risk.13,19,35 In a notable case report, Hewett et al. 12 described twin sisters who both sustained ACL ruptures and exhibited nearly identical neuromuscular deficits, supporting a potential hereditary neuromuscular component. Persistent asymmetry in limb control and proprioception after reconstruction may therefore explain the greater reinjury risk observed in patients with bilateral ruptures.
Genetic and familial predisposition also appear relevant. Having a first-degree relative with an ACL injury more than doubles the risk of rupture. 8 Magnusson et al, 17 in a twin cohort, estimated that up to 69% of the variance in ACL rupture risk is genetically determined. Familial clustering has been confirmed among elite Australian Football League athletes, with siblings exhibiting a markedly higher incidence of ACL injury. 9 These findings reinforce the concept that ligament composition, collagen structure, or hormonal regulation may contribute to an inherited susceptibility, and that bilateral rupture history provides a simple clinical signal of such intrinsic risk.
Despite the emphasis on intrinsic risk, extrinsic factors remain critical to graft survival. Younger age and male sex were independently associated with higher failure rates in this study, consistent with previous reports identifying young, high-demand athletes as the group at greatest risk.26,34 Participation in pivoting and contact sports further amplifies exposure to injury mechanisms.1,26,34 Although the sport type was not independently predictive in multivariate analysis, its strong univariate association with bilateral ACL rupture (70% vs 57% of unilateral cases) highlights the combined effect of exposure and predisposition.
Technical factors can also contribute to failure. Nonanatomic tunnel positioning, especially an anterior or high femoral tunnel, has been shown to significantly increase the likelihood of revision ACLR. 2 Although the study spans 19 years, the core anatomic single-bundle ACLR technique remained consistent. Minor refinements occurred over time, but none altered tunnel placement principles or fixation strategy. Thus, temporal changes are unlikely to have influenced the relationship between intrinsic factors and graft failure. The single-surgeon design ensured standardized tunnel placement and fixation, minimizing technical variability and reinforcing the observed association between bilateral injury history and graft rupture.
This study adds new evidence supporting bilateral native ACL rupture as a simple yet meaningful clinical marker of intrinsic risk. Identifying these patients preoperatively may improve counseling and risk stratification, particularly in younger, competitive athletes. While the present data do not directly assess the efficacy of adjunctive procedures, previous studies and expert consensus suggest that patients with a contralateral ACL injury may benefit from additional lateral reinforcement to reduce rotational instability and graft stress. ¶ Such findings align with the recent International Consensus Statement, in which 88.9% of surgeons favored LEAPs in patients with a previous contralateral ACL rupture. 29 The present study reinforces the rationale for considering intrinsic vulnerability, whether or not a LEAP is ultimately indicated as part of individualized surgical planning.
This study has several limitations. The retrospective design, while leveraging a large cohort, may introduce selection bias and limit the ability to capture unmeasured confounders. The single-surgeon approach, although ensuring consistency in surgical technique, may limit generalizability to broader practice settings with varying levels of expertise or protocols. Another limitation of this study is that surgical adjuncts, such as LEAP, were not analyzed, as the focus was intentionally on intrinsic patient-related risk factors rather than modifiable surgical strategies known to influence graft failure. Additionally, the absence of data on anatomical factors (eg, PTS, intercondylar notch width), neuromuscular control, or ligament laxity precludes a comprehensive assessment of their contribution to graft failure risk. Although preinjury activity level (Tegner score) was included in the multivariate analysis, this scale does not fully differentiate among competitive status (eg, recreational vs professional), training load, or cumulative sport exposure, which may independently influence graft failure risk. The study population primarily comprised young, active athletes, potentially limiting applicability to older or nonathletic individuals. Loss to follow-up, inherent in long-term cohort studies, may underestimate graft failure rates, particularly in patients with less severe outcomes who did not seek further care. Finally, only operatively treated patients were included, which may not reflect the broader ACL-injured population managed nonsurgically.
Conclusion
Bilateral native ACL rupture independently increases the risk of graft failure after ACLR. This finding supports its use as a marker of intrinsic vulnerability, helping identify patients at higher risk of reinjury and guiding individualized counseling and risk stratification.
Footnotes
Submitted October 16, 2025; accepted March 3, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.S. reports equity or stock ownership in AREAS AI; consulting or advisory roles with Convergence Medical; travel reimbursement from Newclip Technics, Arthrex, and the Arthroscopy Association of North America; support and travel reimbursement from Impact Ortho; and serves as Associate Editor for Arthroscopy and on the Editorial Board of the American Journal of Sports Medicine. A.C. and T.D.V. receive travel reimbursement from Arthrex. B.S.-C. reports equity or stock ownership in AREAS AI; and receives consulting and educational grants from Arthrex.
Ethical approval for this study was obtained from Conseil d’Orientation Scientifique Ramsay Santé Comité d’Ethique–Institutional Review Board (COS-RGDS-2025-10-009-SONNERY-COTTET).