
Abstract
Background:
Previous studies have demonstrated that as posterior tibial slope (PTS) increases, increased force is transmitted through anterior cruciate ligament (ACL) grafts, but limited literature assesses PTS effects on anterior tibial translation (ATT) with concomitant medial meniscus (MM) pathology.
Purpose:
To investigate the effects of varying PTS angles on ATT in the presence of MM ramp tear and MM subtotal meniscectomy in the setting of ACL-sectioned and ACL-reconstructed knees.
Study Design:
Controlled laboratory study.
Methods:
Ten male matched-paired cadaveric knees underwent a posterior tibial osteotomy. Specimens were robotically assessed for ATT changes to an 88-N anterior tibial load at 30° and 90° of flexion. Slopes of 0°, 4°, 7°, 9°, 12°, 15°, 18°, and 21° were tested: ACL-intact, ACL-sectioned, ACL-sectioned and MM ramp tear, ACL reconstruction (ACLR) and MM ramp tear, and ACLR and MM ramp repair for group 1; and ACL-intact, ACL-sectioned, ACL-sectioned and subtotal medial meniscectomy, and ACLR and subtotal medial meniscectomy for group 2.
Results:
The baseline tibial position (BTP) and PTS in ACL-intact knees demonstrated a significant positive linear relationship (P < .001) at 30° of flexion. There was no significant ATT difference between ACL-sectioned states across all tested PTS angles at 30° of flexion (P > .63). The ACL-sectioned and MM ramp tear state had significantly increased ATT compared to the ACL-intact state at all tested PTS angles at 30° of flexion (P < .001). An ACLR and residual ramp tear had significantly increased ATT compared to the ACL-intact state at PTS angles of 4°, 7°, 9°, and 18° at 30° of flexion (P < .04). The ATT of the ACLR and ramp repair was not significantly different from that of the ACL-intact state at all PTS angles at 30° of flexion (P > .34). The ACLR and subtotal medial meniscectomy state had a significantly increased ATT compared to the ACL-intact state at PTS angles of 15° and 21° at 30° (all P < .04) and 18° and 21° at 90° of flexion (all P < .04).
Conclusion:
This biomechanical cadaveric study demonstrated that as PTS increases, the BTP in intact knees shifts anterior and the absolute amount of ATT with ACL sectioning does not increase as PTS increases. Also, increases in ATT were found for an ACLR with a nonrepaired MM ramp tear, while a concomitant ramp repair restored ATT to intact. Also, an ACLR with a subtotal medial meniscectomy resulted in increases in ATT with a PTS >12°.
Clinical Relevance:
A slope-reducing tibial osteotomy may be considered in knees with >12° PTS undergoing ACLR with a subtotal medial meniscectomy to optimally protect an ACLR graft. An MM ramp repair is needed with ACLR to restore ATT.
Keywords
Increased posterior tibial slope (PTS) is a significant risk factor for anterior cruciate ligament reconstruction (ACLR) graft failure due to the increased force transmitted to the graft as tibial slope increases.3,25 Thus, when increased PTS (commonly defined as ≥12°) is identified during a primary anterior cruciate ligament (ACL) tear or revision ACLR workup, anterior closing-wedge proximal tibial osteotomies (ACWPTOs) are being increasingly used with a goal to reduce the PTS between 5° and 7°. 26 Currently, the indications for ACWPTO are evolving, including identifying other concurrent pathologies that can lead to further increases in anterior tibial translation (ATT) and on ACLR graft loads with an increased PTS.
The posterior horn of the medial meniscus (MM) effectively acts as a secondary restraint to increased ATT, and when it is torn or absent, there is increased stress on an ACLR graft and an increased risk of failure.7,18,21,30 MM ramp tears 28 have been reported to occur in up to 40% of ACL tears 9 and should be suspected with the presence of a high-grade Lachman examination.9,24 Untreated ramp tears have also been recognized to place increased loads on an ACLR. 7 Thus, investigations into ways to protect an ACLR graft in the setting of MM tears or deficiency are important to a successful long-term outcome. Currently, there is a paucity of information in the literature investigating what effects varying degrees of PTS have on increases in ATT for knees with a meniscal ramp tear or a subtotal medial meniscectomy in an ACL-sectioned knee and after an ACLR.
Therefore, the purpose of this study was to investigate the effects of varying PTS angles on ATT in the presence of posterior MM pathology in the setting of ACL-sectioned and ACLR knees. The null hypothesis for the study's primary outcome was that there would be no significant difference in ATT between varying degrees of PTS for the ACL-sectioned and either ramp tear or repair or subtotal medial meniscectomy ACLR groups.
Methods
Specimen Preparation
This study was a biomechanical robotic study using 10 matched-paired fresh-frozen cadaveric knees (n = 20; mean ± SD age, 65.3 ± 9.3 years [range, 44-79 years]; 10 male, 0 female) obtained from an anatomy bequest program (Anatomy Bequest Program, University of Minnesota Medical School, Minneapolis, Minnesota, USA). Only male specimens were selected to ensure adequate bone quality that would withstand the long and rigorous testing protocol. Institutional review board approval was not necessary because de-identified cadaveric specimens were exempt from review at our institution. Specimens without evidence of prior injury (including significant meniscal tears, Outerbridge grade 3 or 4 chondromalacia), 17 surgical history, or gross anatomic abnormality were included in the study. Specimens were stored at −20°C and thawed at room temperature 24 hours before preparation.
Specimens were prepared first by performing a diagnostic arthroscopy to confirm there was minimal chondromalacia and the ACL and menisci were intact. All diagnostic arthroscopy was performed by a single investigator (MTR) in a standardized manner to evaluate the suprapatellar pouch, medial gutter, lateral gutter, medial compartment, lateral compartment, intercondylar notch, and posterior medial and posterior lateral compartments. A probe was utilized during arthroscopy to evaluate the integrity of the ACL, menisci, and cartilage surfaces within the knee. Specimens with advanced chondromalacia, defined as Outerbridge grades 3 and 4, were excluded from the study. This was followed by excising all skin and dissecting posterior subcutaneous tissues from the specimen >2 cm proximal and distal to the joint line. The popliteus muscle belly was elevated off the posterior cortex to provide direct visualization of the planned osteotomy site. The popliteus was then anchored to the posterior cortex of the tibia with a staple to maintain rotational stability. 3 The femoral and tibial diaphyses were potted in a cylindrical mold with poly (methyl methacrylate) (Newstetic) that permits fixation within the robotic testing system.
Surgical Technique
Fluoroscopic imaging was used to obtain a true lateral radiograph of the knee. A standard validated technique was used to measure the native anatomic PTS, which was defined as the angle between the lateral tibial plateau and the mid-diaphysis of the tibia (mean ± SD angle, 9.1°± 3.3° [range, 4°-15°]). 5 Two circles were drawn within the proximal and distal tibia, 5 cm and 15 cm distal to the joint line, respectively. The mid-diaphysis line was then connected between the 2 respective circles (Figure 1).3,5,19
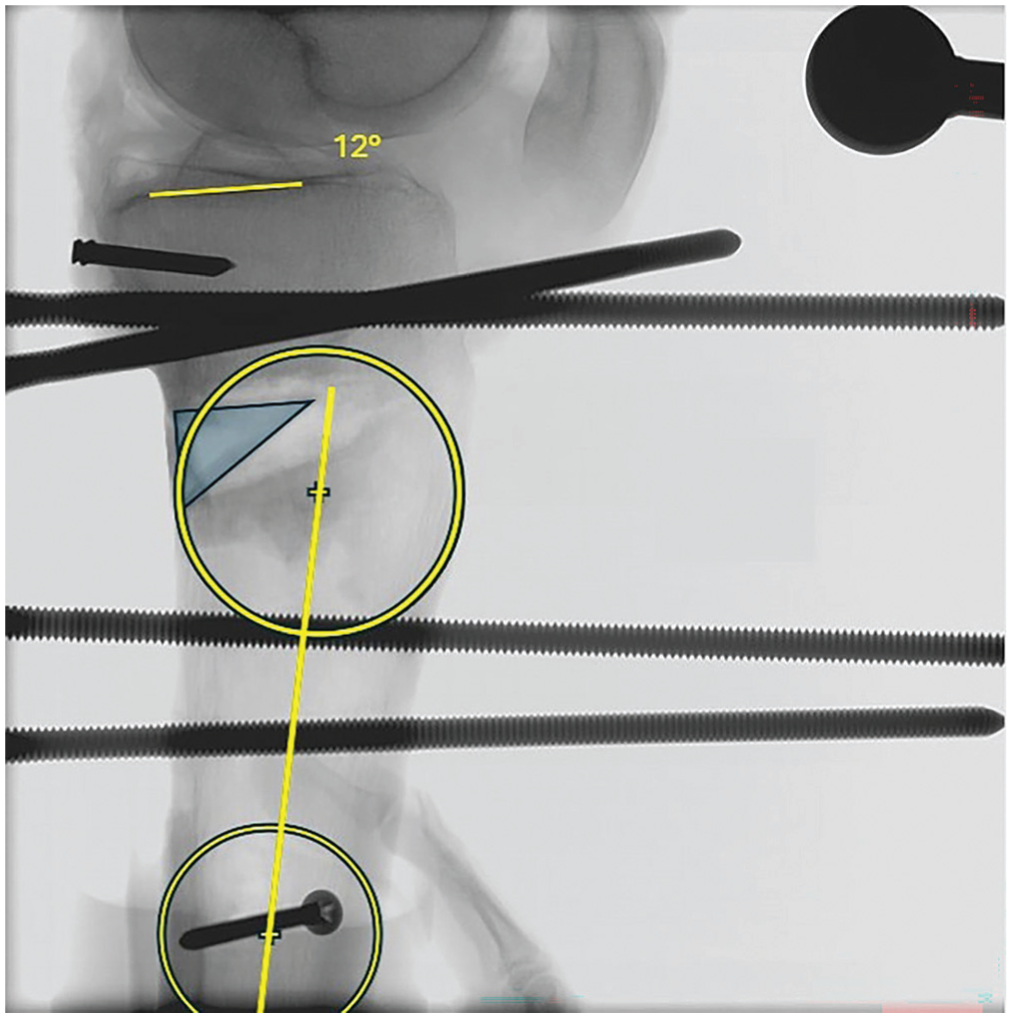
True lateral knee radiograph demonstrating the anatomic posterior tibial slope (PTS) measurement with a wedge (triangle) placed within the posterior tibial osteotomy. The anatomic PTS measurement was obtained by determining the angle between the lateral tibial plateau and the mid-diaphysis of the tibia. First, a line was drawn parallel to the lateral tibial plateau. Two circles were then placed within the tibia to obtain the mid-diaphysis line, one 5 cm and the other 15 cm distal to the joint line. The mid-diaphysis line was then drawn from the center points of the 2 circles. The angle between the lateral tibial plateau and the mid-diaphysis line of the tibia was then subtracted from 90° to calculate the resultant native PTS.
A posterior tibial osteotomy, which allowed the ACLR tibial tunnels to not cross the osteotomy site, was performed under fluoroscopic guidance 3.5 cm distal and parallel to the joint line with a saw blade while leaving a 1-cm anterior cortical hinge. The size of the osteotomy was based on the native PTS and calculated to achieve a maximum PTS of 21° when fully closed, while also permitting wedge placement to achieve a 0° PTS. The PTS was fixed with an anterior and posterior external fixator that allowed the slope to vary depending on the respective wedge size. Corresponding 3-dimensional printed wedges of varying sizes (1-24 mm) were then placed within the osteotomy site, and radiographs were acquired to determine the necessary wedge size to obtain PTS angles of 0°, 4°, 7°, 9°, 12°, 15°, 18°, and 21°. This allowed for adjustments to be made to the PTS with improved ease and reliability while keeping the specimen mounted within the robotic testing setup.
The ACLR was performed in accordance with previous techniques for an anatomic single-bundle ACLR.12,16 Femoral and tibial tunnels were reamed after creation of the osteotomy to avoid placing the tibial tunnel aperture near the osteotomy site and leaving adequate cortical bone for placement of the tibial fixation button. Graft preparation was performed using semitendinosus allografts, which were obtained from a tissue supplier and selected to be of similar length and diameter. The grafts were quadrupled to achieve a diameter of 9 mm and length of 60 to 65 mm. Both ends were then whipstitched 25 mm from each end with nonabsorbable suture (No. 2 FiberWire; Arthrex). Grafts were pretensioned on a graft board for 10 minutes to minimize creep during testing. Femoral fixation was performed with a cortical button (EndoButton; Smith & Nephew), and the tibial end was fixed using a custom adjustable loop button that allowed for adjustments after PTS changes to permit ACLR graft retensioning. After ACLR, arthroscopy was performed in a manner similar to that done intraoperatively to ensure appropriate graft tension and that there was no impingement in full extension. Before testing at each variable PTS, the knee was again placed in full extension with a posterior drawer applied as the adjustable loop button was retensioned. The adjustable loop button and graft were tensioned until the button laid flat on the tibial cortex with the graft held in maximal tension to ensure consistent graft tension across PTS levels. The ACL graft was tensioned by a single investigator (MTR) for consistent graft tensioning. The knee was then cycled 20 times and checked for maintained tension before being mounted on the robot.
For the MM ramp tear creation and repair, a 2-portal posteromedial approach as described by Siboni et al 23 was utilized. With the arthroscope in the anterolateral portal, a transnotch view was performed between the medial femoral condyle and medial aspect of the posterior cruciate ligament to allow for direct visualization of the posteromedial compartment. The posteromedial viewing portal was identified with an 18-gauge spinal needle placed proximal to the medial femoral condyle and posterior to the posterior femoral cortex, entering just proximal to the synovial fold. Next, a No. 11 blade was then used for portal creation, and the distal working portal was created in line with the joint line in a similar fashion. The arthroscope was then moved to the posteromedial viewing portal and a complete type 4 meniscocapsular and meniscotibial MM ramp lesion, approximately 2 cm in length, was made with a beaver blade.8,28 After testing of the ramp tear state, a ramp repair was performed with a No. 0 nonabsorbable braided suture passed using a combination of suture passers and/or suture hooks. The repair was performed in a medial to lateral direction, placing suture knots every 3 to 4 mm for a total of 3 knots to complete the repair. After tying all knots, repair stability and adequate tissue tension were confirmed by palpation with a probe while flexing and extending the knee.
The subtotal medial meniscectomy was performed using a combination of meniscal punches and a shaver to remove the posterior half of the MM to a <2-mm rim. In specimens with a tight medial compartment, a valgus force was applied to ensure adequate posterior meniscus resection. Of note, pie-crusting of the medial collateral ligament (MCL) was not required since a portion of the distal tibial attachment of the MCL was elevated using a Cobb elevator to allow safe placement of a z-retractor for soft tissue protection during osteotomy creation. Subsequently, this resulted in approximately 1 mm of gapping within the medial compartment, which was sufficient to visualize the posterior horn of the MM for resection.
Biomechanical Testing
Specimens were then mounted within custom fixtures of a universal force-torque sensor (Delta F/T Transducer; ATI Industrial Automation) affixed to the robotic end effector of a 6 degrees of freedom robotic testing system (KUKA KR 300-3; Kuka Robotics) (Figure 2).12,21 Once the knee was mounted, a digitizing probe (Optitrack; NaturalPoint) was used to determine the spatial relationships among the robot, load cell, and specimen based on all 3 Cartesian axes as previously described by Badida et al. 2 Before each mechanical test, the equilibrium position of the native intact knee relative to the femur was determined at 30° and 90° of knee flexion under 30 N of compression while applying zero forces and torques in every other direction. This served as the zero value for calculating ATT for additional mechanical test states. A coordinate system was then developed for each specimen based on the equilibrium position of the knee at its native PTS, which was then utilized as a reference during PTS alteration. The ATT was calculated as the maximum amount of anterior translation of the tibia in relation to the femur during a loaded anterior drawer test compared to the unloaded ACL-intact state with the native PTS equilibrium position. A larger value indicates a greater amount of ATT. Negative values indicate that, after varying the PTS, the tibia did not reach the equilibrium position of the native PTS during the anterior drawer test. The ATT was measured by the robot as it analyzed the changes that occurred in the robot joint angles. This method of measurement is calculated automatically by the robotic software and has been verified to be accurate within 0.05 mm.
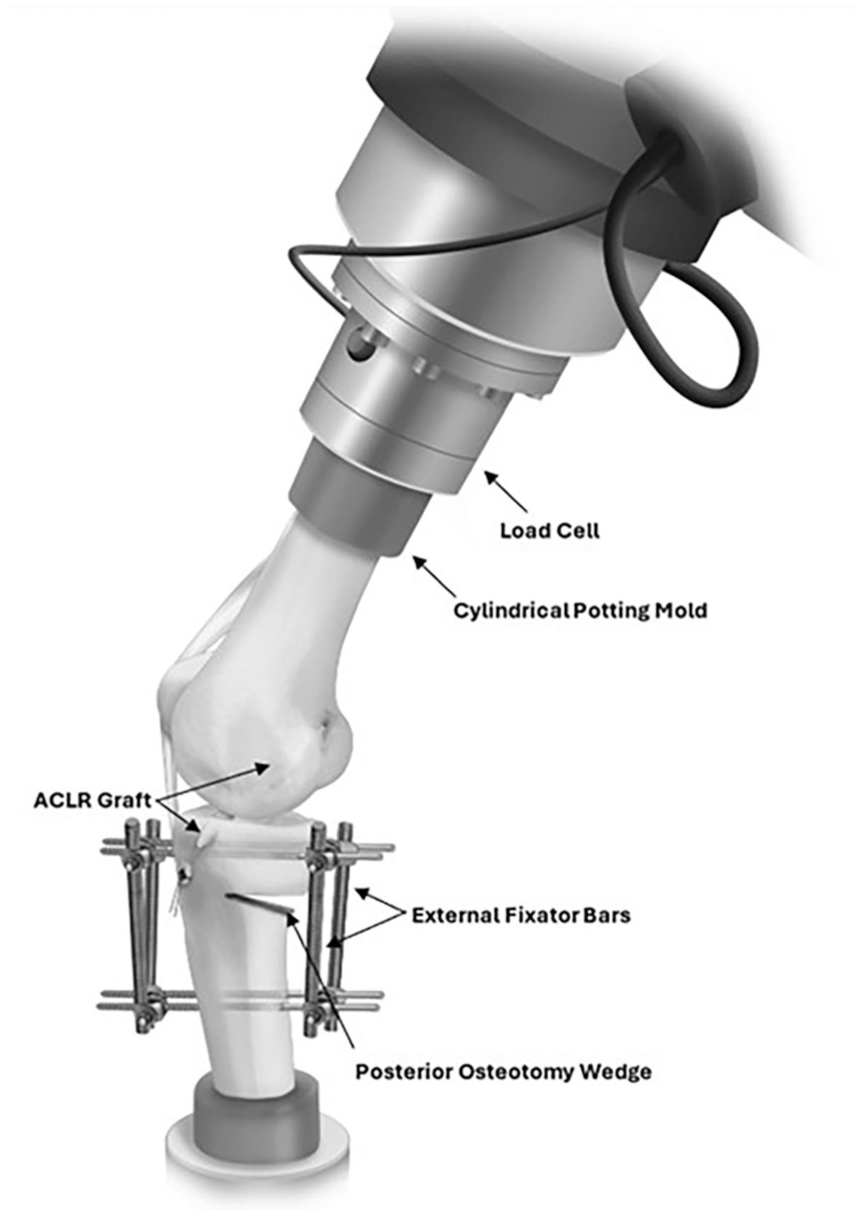
Illustration of the robotic testing setup. The knee was mounted in the robotic frame with external fixators applied to the anterior and posterior aspects of the knee to hold the desired slope angle. The hamstring anterior cruciate ligament reconstruction (ACLR) allograft is seen coursing through respective tibial and femoral tunnels using a suspensory fixation technique.
Knee kinematics were then analyzed at 30° and 90° of knee flexion during a simulated anterior drawer test with 30 N of compression and an 88-N anterior tibial load. The baseline tibial position (BTP) was established as the location of the ACL-intact state tibia relative to the femur during the loaded anterior drawer test at all PTS angles. 25
Paired knees underwent testing conditions for 2 testing protocols (Figure 3): ACL-intact, ACL-sectioned, ACL-sectioned and MM ramp tear, ACLR and MM ramp tear, and ACLR with MM ramp repair for group 1; and ACL-intact, ACL-sectioned, ACL-sectioned and subtotal medial meniscectomy, and ACLR with a subtotal medial meniscectomy with PTS values of 0°, 4°, 7°, 9°, 12°, 15°, 18°, and 21° for all testing states for group 2. The paired knees were randomly tested under 2 different protocols, and the randomization was completed using an online website (www.randomizer.com). Matched-paired cadaveric knees were placed in both protocols to ensure that specimen demographics and native PTS were similar among both testing protocols. Additionally, this permitted further analysis to be performed if there were notable discrepancies identified between intact testing states at different PTS angles that may arise due to osteotomy creation or tissue degradation during extended testing protocols. The order of PTS angles was randomized for each surgical state in each specimen to account for the risk of soft tissue creep and progressive laxity that occurs with repeated wedge changes and the manipulation of PTS. To prevent soft tissue desiccation during testing, all specimens were sprayed regularly with normal saline.

Randomization and testing sequence for groups 1 and 2. ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; SMM, subtotal medial meniscectomy.
Statistical Analysis
The primary outcome data included changes in ATT (knee stability) during the various testing states in the setting of varying degrees of PTS. Statistical software R (Version 4.3.2; R Foundation for Statistical Computing) and MATLAB (MathWorks) were used for all analyses. A linear mixed-effects regression model with a random intercept for specimen was used to model the relationship between PTS and BTP, with Pearson correlation coefficients calculated to assess association strength. ATT differences across surgical testing states at each PTS level and flexion angle were evaluated using repeated-measures analysis of variance (RM-ANOVA) with Greenhouse-Geisser correction and Tukey-adjusted post hoc comparisons. Groups 1 and 2 were analyzed independently. Analyses at 30° of knee flexion served as the primary analysis, with 90° of knee flexion as secondary. To evaluate whether the change in ATT (Δ mm) with ACL sectioning varied across PTS, delta values were computed (ACL-sectioned minus ACL-intact) and analyzed with an RM-ANOVA pooling both groups (n = 20), stratified by flexion angle. P values <.05 were considered statistically significant. This study used a predefined experimental sample; therefore, the analysis was performed post hoc using the observed variability in ATT from the cadaveric knee testing data set. A minimal detectable difference analysis indicated that with 10 knees per cohort and an α of .05 (2-sided), the study had 80% power to detect differences ≥2.38 mm in ATT for between-state differences based on the variance estimate. A post hoc analysis was performed to identify additional relevant trends in the data.
Results
The most clinically important testing results are presented in the following sections. Additional testing data obtained in this study are presented in the Appendix (available in the online version of this article).
Baseline Tibial Position
As the PTS was increased from 0° to 21° at 30° of knee flexion, the linear mixed-effects regression model demonstrated that for every 1° increase in PTS, the BTP in the ACL-intact state translated anteriorly by 0.9 mm (P < .001; 95% CI, 0.79-0.95) with a Pearson correlation coefficient of 0.85 (Figure 4). At 90° of knee flexion, for every 1° increase in PTS, the BTP translated anteriorly by 0.8 mm (P < .001; 95% CI, 0.70-0.86) with a Pearson correlation coefficient of 0.84 (Appendix Figure A1, available online).

Linear regression model demonstrating the relationship between posterior tibial slope and the baseline tibial position (BTP) with Pearson correlation coefficients at 30° of knee flexion. BTP was recorded in the anterior cruciate ligament–intact state when a simulated anterior drawer with 30 N of compression and an 88-N anterior tibial load were applied.
ACL-Intact Versus ACL-Sectioned States for Varying PTS
The change in ATT (Δ mm) from the ACL-intact to ACL-sectioned states was compared across all PTS values, and there were no significant differences in the amount of change at both 30° (all P > .63) (Figure 5; Appendix Table A1, available online) and 90° (all P > .06) (Appendix Figure A2, Appendix Table A1, available online) of knee flexion across all tested PTS angles.
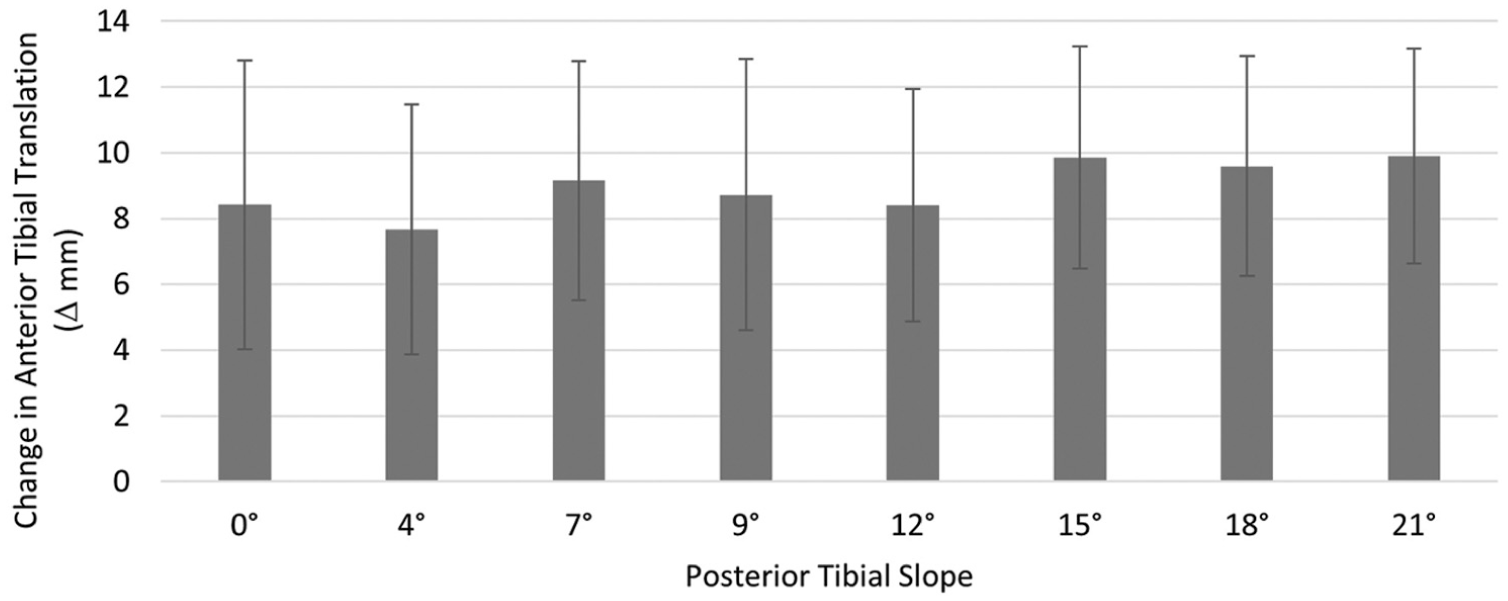
Change in anterior tibial translation (ATT) (mean ± SD) from the anterior cruciate ligament (ACL)–intact to the ACL-sectioned states at 30° of knee flexion compared across the tested posterior tibial slope (PTS) angles (degrees). The change in ATT (Δ mm) was calculated by subtracting the ACL-intact state ATT from the respective ACL-sectioned state ATT. The changes in ATT comparison across all PTS angles were not significant (all P > .63).
Group 1: ACLR With MM Ramp Tear and Repair
ACL-Sectioned State
Compared to the ACL-intact state, ACL-sectioned knees at 30° of flexion resulted in significantly increased ATT (Figure 6; Appendix Table A2, available online) at each corresponding PTS angle (all P < .002) (Appendix Table A3, available online). Compared to the ACL-intact state, ACL-sectioned knees at 90° of flexion resulted in significantly increased ATT (Appendix Figure A3, Appendix Table A4, available online) at PTS angles of 7°, 12°, 15°, 18°, and 21° (all P < .004) (Appendix Table A5, available online).
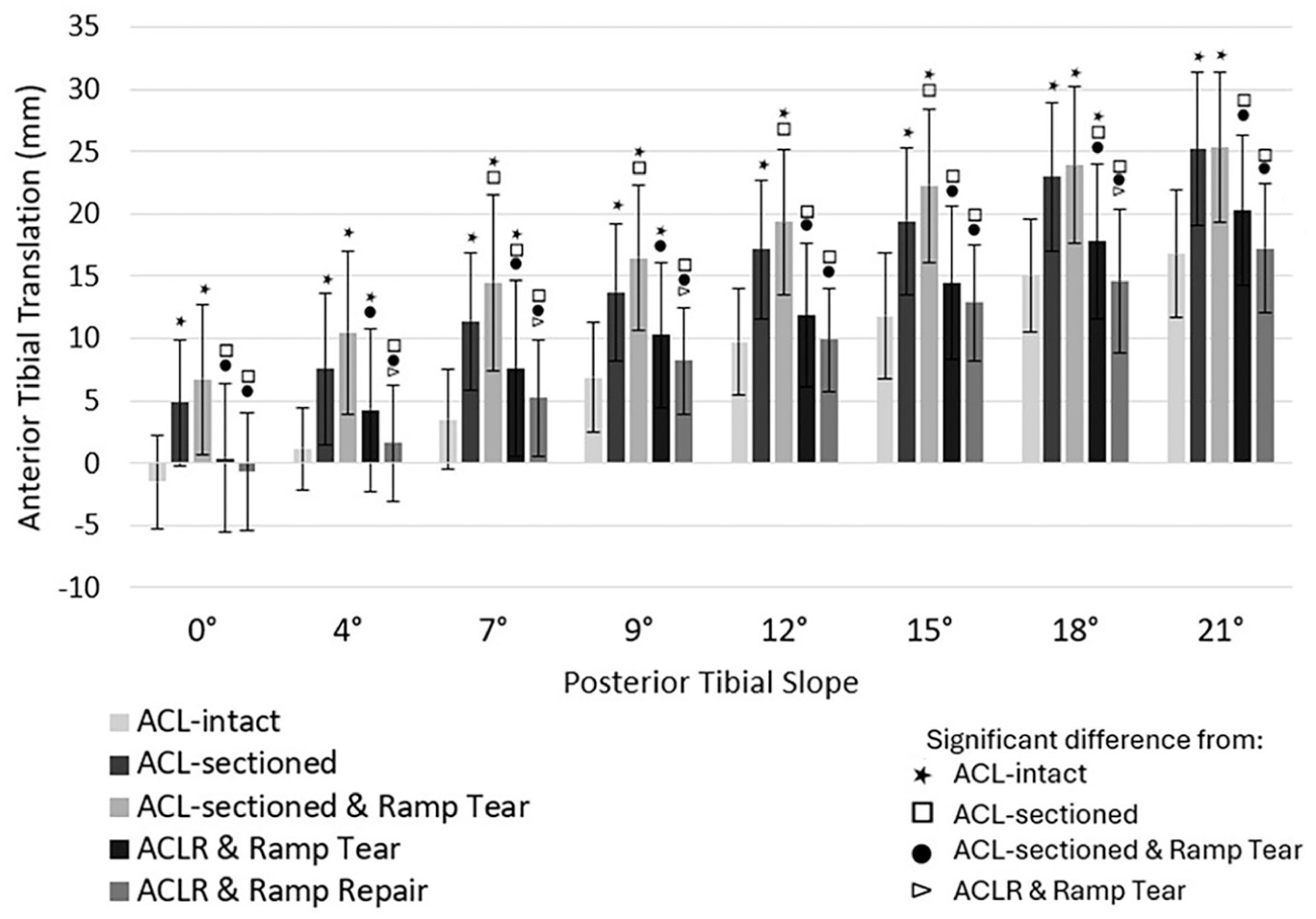
Graphic representation of anterior tibial translation (ATT) at the tested posterior tibial slope angles across 5 separate testing states in group 1 at 30° of knee flexion. Bars represent the amount of ATT in millimeters, and lines represent the standard deviation. ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction.
ACL-Sectioned and MM Ramp Tear State
Compared to the ACL-intact state, the ACL-sectioned and MM ramp tear states had significantly increased ATT at all tested PTS angles at 30° of flexion (all P < .001) (Figure 6; Appendix Tables A2 and A3, available online) and for all PTS angles at 90° of flexion except 0° (P > .07) (Appendix Figure A3, Appendix Tables A4 and A5, available online). Compared to the ACL-sectioned knee state, the addition of a ramp tear resulted in significantly increased ATT at 30° of flexion for PTS angles of 7°, 9°, 12°, and 15° (all P < .04) and at 90° of flexion for PTS angles of 9°, 12°, 15°, and 18° (all P < .04).
ACLR and MM Ramp Tear State
Compared to the ACL-intact state, the ACLR and MM ramp tear state had significantly increased ATT at 30° of flexion for PTS angles of 4°, 7°, 9°, and 18° (all P < .04) (Figure 6; Appendix Tables A2 and A3, available online) and at 90° of flexion for PTS angles of 7° and 21° (all P < .03) (Appendix Figure A3, Appendix Tables A4 and A5, available online). Compared to the ACL-sectioned state, the ACLR with an MM ramp tear state had significantly decreased ATT at 30° of flexion for PTS angles of 0°, 7°, 12°, 15°, 18°, and 21° (all P < .02), but at 90° of flexion there were no significant differences in ATT (all P > .64). Compared to the ACL-sectioned and MM ramp tear state, the ACLR with an MM ramp tear state resulted in significantly decreased ATT for all PTS angles at 30° of flexion (all P < .02) and at 90° of flexion for PTS angles of 7° and 12° (all P < .006).
ACLR and MM Ramp Repair State
Compared to the ACL-intact state, the ACLR with a ramp repair state had no significant differences in ATT at all PTS angles at 30° of flexion (all P > .34) (Figure 6; Appendix Tables A2 and A3, available online) and 90° of flexion (all P > .51) (Appendix Figure A3; Appendix Tables A4 and A5, available online). When compared to the ACL-sectioned state, the ACLR and MM ramp repair state had significantly decreased ATT at all PTS angles at 30° of flexion (all P < .008) and at 90° of flexion for PTS angles of 4° and 21° (all P < .03). When compared to the ACL-sectioned and MM ramp tear state, the ACLR and MM ramp repair state had significantly decreased ATT at all PTS angles at 30° of flexion (all P < .001) and at PTS angles of 4°, 7°, 9°, 12°, 15°, 18°, and 21° at 90° of flexion (all P < .02). Compared to the ACLR and MM ramp tear state, the ACLR and MM ramp repair state resulted in significantly decreased ATT at PTS angles of 4°, 7°, 9°, and 18° at 30° of flexion (all P < .02) and PTS angles of 7°, 9°, and 18° at 90° of flexion (all P < .02).
Group 2: ACLR With a Subtotal Posterior Medial Meniscectomy
ACL-Sectioned State
Compared to the ACL-intact state, ACL-sectioned knees resulted in significantly increased ATT at all PTS angles at 30° of flexion (all P < .001) (Figure 7; Appendix Tables A6 and A7, available online) and 90° of flexion (all P < .04) (Appendix Figure A4, Appendix Tables A8 and A9, available online).
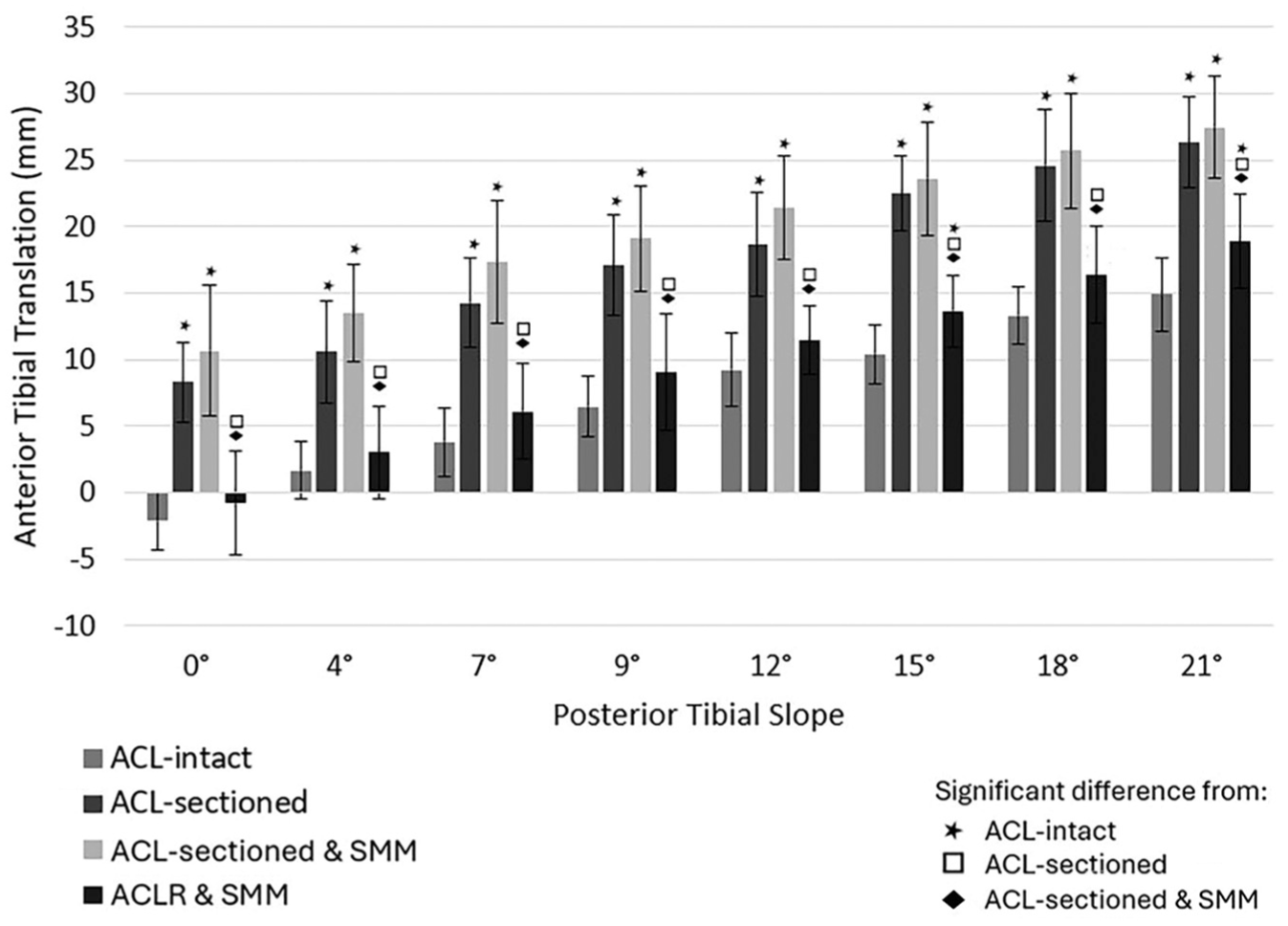
Graphic representation of anterior tibial translation (ATT) at the tested posterior tibial slope angles across 4 separate testing states in group 2 at 30° of knee flexion. Bars represent the amount of ATT in millimeters, and lines represent the standard deviation. ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; SMM, subtotal medial meniscectomy.
ACL-Sectioned and Subtotal Medial Meniscectomy State
Compared to the ACL-intact state, ACL-sectioned knees with a subtotal medial meniscectomy resulted in significantly increased ATT at all tested PTS angles at 30° of flexion (P < .001) (Figure 7; Appendix Tables A6 and A7, available online) and 90° of flexion (all P < .003) (Appendix Figure A4, Appendix Tables A8 and A9, available online). Compared to the ACL-sectioned state, the addition of a subtotal medial meniscectomy resulted in no significant differences in ATT at all PTS angles at both 30° of flexion (P > .13) and 90° of flexion (P > .07).
ACLR and Subtotal Medial Meniscectomy State
An ACLR with a subtotal medial meniscectomy compared to the ACL-intact state had significantly increased ATT at PTS angles of 15° and 21° at 30° of flexion (all P < .04) (Figure 7; Appendix Tables A6 and A7, available online) and at 90° of flexion for PTS angles of 18° and 21° (P < .04) (Appendix Figure A4, Appendix Tables A8 and A9, available online). Compared to the ACL-sectioned knee state, the ACLR and subtotal medial meniscectomy state had significantly decreased ATT at all PTS angles at 30° of flexion (all P < .005) and at PTS angles of 0°, 15°, 18°, and 21° at 90° of flexion (all P < .02). Compared to the ACL-sectioned and subtotal medial meniscectomy knee state, the addition of an ACLR resulted in significantly decreased ATT at all PTS angles at 30° of flexion (all P < .003) and 90° of flexion (all P < .01).
Discussion
The most important findings of this study were that increasing PTS led to an increased BTP, PTS did not impact the absolute change in ATT with ACL sectioning, an ACLR with a concomitant ramp repair restored ATT to an ACL-intact state across all PTS values, and an ACLR with a subtotal posterior medial meniscectomy was unable to restore ATT compared to the ACL-intact state at PTS >12°.
Our study found that for every 1° increase in PTS, the BTP in the ACL-intact knee translated anteriorly by 0.9 mm at 30° of knee flexion and 0.8 mm at 90° of knee flexion. This corroborated a recent clinical study by Tollefson et al 25 reporting a 0.67-mm increase in ATT for every 1° increase in slope in ACL-intact knees on ACL stress radiographs obtained at 20° to 30° of knee flexion. The small differences in ATT with increasing PTS between our study and theirs is likely due to the difference between the static testing conditions in the robot and the dynamic conditions seen clinically, which could result in less ATT. Relying solely on the position of the tibia relative to the femur of the ACL-deficient knee to objectively determine increases in ATT with an ACL tear may over- or underestimate values depending on the PTS. In addition, the increased ATT found with increases in PTS would further support biomechanical studies that have reported that increased PTS increases the load experienced by both an ACL and an ACLR graft.3,29 Our findings help to provide further evidence to explain why increases in PTS lead to increased ACL forces and ultimately increased rates of ACL and ACLR graft failures.
In our testing conditions, we found no significant difference in the change in ATT between the ACL-intact and ACL-sectioned states when compared across all PTS values at 30° and 90° of knee flexion. In a clinical study, Dejour and Bonnin 6 reported that for every 10° of increased PTS, there was a 6-mm increase in ATT when comparing the ACL-intact and ACL-torn knees on standing lateral knee radiographs. Tollefson et al 25 also reported a 0.52-mm increase in ATT per 1° of increased PTS on bilateral ACL stress radiographs. Differences between our study and these other studies could be due to various reasons, including a smaller sample size (compared to a clinical study) and the difficulties in comparing in vitro cadaveric investigations to clinical studies due to the lack of other factors such as the dynamic stabilizers present in vivo. Furthermore, direct comparison between our controlled biomechanical testing conditions and clinical studies is challenging, as ACL injuries are commonly seen with associated pathologies, such as MM ramp tears 7 and lateral meniscus root tears,10,11 both of which have been reported to increase ATT in ACL-torn knees. In any event, further studies are recommended to assess the pathologies that contribute to increases in ATT in addition to the effects of an ACL-deficient state.
Our study also demonstrated that for most tested PTS values, an ACLR performed alone in the presence of an MM ramp tear did not restore ATT to intact levels, but rather a concomitant ramp repair was required to restore values. In contrast, both DePhillipo et al 7 and Li et al 15 reported that with MM ramp tears, an ACLR alone with no repair of an MM ramp tear restored ATT to the ACL-intact state at both 30° and 90° of knee flexion. The difference between the results of these studies and ours could be due to the amount of the axial load applied during the simulated anterior drawer. DePhillipo et al 7 utilized a 10-N axial load with 88 N of anterior drawer, and Li et al 15 did not specify any axial load with 134 N of anterior drawer applied. With the meniscus being a pertinent weightbearing structure, the 30-N axial load applied in our study could have accounted for the increased effects and importance of the ramp repair to restore ATT with an ACLR. Additionally, our study found that changes in PTS did not significantly impact ATT once a ramp repair was performed, highlighting the critical contribution of the posterior horn of the MM at all angles of PTS in controlling ATT after an ACLR. This finding provides further clinically relevant information regarding the need to repair MM ramp tears at the time of an ACLR to reduce the risk of ACLR graft overload and subsequent stretching out or failure of the graft.7,15
Finally, we found that an ACLR with a subtotal medial meniscectomy significantly increased ATT at 30° of knee flexion compared to the ACL-intact state for most tested PTS values >12°. Previous studies have reported the important role of the posterior horn of the MM as a secondary stabilizer to ATT in the ACL-sectioned knee, with significant increases in ATT with a subtotal medial meniscectomy.1,22 Our study demonstrates that the secondary stabilizing contribution of the posterior horn of the MM in an ACL-deficient knee is particularly significant when PTS exceeds 12°. This is clinically important, as multiple clinical studies have shown that a PTS ≥12° results in increased rates of ACLR failure and revision surgery.13,20,27 A recent biomechanical study performed by Lemme et al 14 evaluated whether a lateral extra-articular tenodesis (LET) could effectively reduce the effects of varying PTS angles (0°, 10°, 20°) on knee kinematics and ACL graft forces during simulated pivot-shift loading. The authors found that at 10° and 20° PTS, the observed reductions in ACL graft loading with an ACLR+LET (22.1% and 36.6%, respectively) were comparable or superior to those of a 10° slope-reducing osteotomy (2.6% and 24.0%, respectively). Comparatively, when the authors tested ATT, they found reducing the tibial slope led to a significant difference in ATT (P < .0001), whereas performing an LET did not lead to a significant difference in ATT across all slopes (all P > .517). These findings highlight the potential benefit of an LET in reducing ACL graft loading in the “gray area slopes” between 12° and 15°, where an ACWPTO may result in morbidity; however, it is essential to consider that similar results were not seen when evaluating ATT. In this context, our findings support that further clinical studies should be considered to evaluate the functional outcomes of patients undergoing a slope-reducing high tibial osteotomy in the setting of a primary or revision ACLR with a deficient posterior horn of the MM and a PTS >12°.
We acknowledge the presence of some limitations within this study. First, cadaveric laboratory studies may not represent the same environment as an in vivo experiment, and the biological healing effects cannot be reproduced. Cadaveric tissue and desiccation along with the absence of dynamic stabilizing muscle forces on the knee are limitations that could potentially impact knee kinematics. Furthermore, the multiple testing steps required for PTS alterations through an osteotomy may lead to soft tissue tension variations, which can impact knee kinematics. However, to limit the variability of soft tissue tension, the order of PTS was randomized with each surgical state. Additionally, in order to perform a posterior osteotomy, the popliteus muscle belly was elevated and then anchored to the posterior cortex of the tibia with a staple. This was done to maintain rotational stability; however, this could potentially modify the posterolateral rotation and translation of the cadaveric knee. The age of the cadaveric specimens was higher than that typically seen within a patient population with ACL tears, although it was similar to that in other related cadaveric biomechanical studies.7,15 During testing, each specimen was assessed and removed if deemed of poor bone quality before proceeding. To further optimize bone quality, only male specimens were utilized, which reduced the risk of osteopenic bone seen in older female specimens. Female specimens were utilized throughout pilot testing; however, the osteotomy and age of the specimens demonstrated that the bone quality was not sufficient to withstand the rigors of repeated testing due to continuous bone breakdown and poor external fixation stability. A limitation of all slope-changing osteotomy biomechanical studies is the difficulty accounting for the anatomic variability of PTS and its impact on tibial position and ATT between specimens.3,4,21 The magnitude of correction (ΔPTS) may alter soft tissue tensioning, creep, and fixation micromotion, and this may be variable between specimens, making it difficult to measure ATT. Finally, this study only assessed the effects of posterior MM pathology with increases in PTS to better assess the indications for a slope-reducing high tibial osteotomy. Further studies should investigate if an anterolateral complex reconstruction (anterolateral ligament or lateral extra-articular tenodesis) can restore ATT to the ACL-intact state with these MM pathologies.
Conclusion
This biomechanical cadaveric study demonstrated that as PTS increases, the BTP in intact knees shifts significantly anterior and the absolute amount of ATT with ACL sectioning does not increase as PTS increases. Also, significant increases in ATT were found for an ACLR with a nonrepaired MM ramp tear, while a concomitant ramp repair restored ATT to intact. Also, an ACLR with a subtotal medial meniscectomy resulted in increases in ATT with a PTS >12°.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465261448522 – Supplemental material for Restoration of Anterior Tibial Translation Is Achievable With an Anterior Cruciate Ligament Reconstruction and Ramp Repair With Increasing Posterior Tibial Slope While Medial Meniscus Deficiency Requires Concomitant Slope-Correcting Osteotomy
Supplemental material, sj-pdf-1-ajs-10.1177_03635465261448522 for Restoration of Anterior Tibial Translation Is Achievable With an Anterior Cruciate Ligament Reconstruction and Ramp Repair With Increasing Posterior Tibial Slope While Medial Meniscus Deficiency Requires Concomitant Slope-Correcting Osteotomy by Matthew T. Rasmussen, Benjiman J. Wilebski, Luke V. Tollefson, Mitchell R. Carlson, Dustin R. Lee, Rylan A. Behnke, Sarah L. Larson, Nicholas K. Retzer, Romir Patel, Henri R. Brink, Christopher M. LaPrade and Robert F. LaPrade in The American Journal of Sports Medicine
Footnotes
Submitted January 23, 2026; accepted April 3, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: R.F.L. is a consultant for Ossur, Smith & Nephew, and Responsive Arthroscopy; receives royalties from Ossur, Smith & Nephew, Elsevier, and Arthrex; receives research grants from Ossur, Smith & Nephew, Arthroscopy Association of North America (AANA), and AOSSM; is on committees for the International Society of Arthroscopy, Knee Surgery and Orthopedic Sports Medicine, AANA, and AOSSM; is on the editorial board for the American Journal of Sports Medicine, Journal of Experimental Orthopedics, Knee Surgery, Sports Traumatology, Arthroscopy, Journal of Knee Surgery, Journal of Orthopedic & Sports Physical Therapy, and Operative Techniques in Sports Medicine; and receives educational support from Foundation Medical. C.M.L is a consultant for Smith & Nephew.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.