
Abstract
Background:
Rotator cuff tears lead to bone loss because of reduced mechanical loading at the tendon-bone interface, which results in poor healing after rotator cuff repair (RCR). Whether Yoda1, the specific Piezo1 agonist, can counteract bone loss and promote rotator cuff healing has not yet been explored.
Hypothesis:
Yoda1 promotes tendon-to-bone healing in a rat model of RCR and regulates M1/M2 macrophage polarization at the tendon-bone interface.
Study Design:
Controlled laboratory study.
Methods:
A total of 120 male rats aged 12 weeks, which were randomly divided into 4 groups, were used to establish the RCR model: vehicle-only (control [CON]), low-concentration Yoda1 (LC), moderate-concentration Yoda1 (MC), and high-concentration Yoda1 (HC) intraperitoneal injection. The rats were sacrificed at 4 and 8 weeks. Tendon-to-bone healing at the repair site was evaluated using histological, bone microstructure, and biomechanical analyses. Macrophage polarization was observed through immunofluorescence staining.
Results:
The LC group showed higher histological scores compared with the CON group at each time point (P < .001). More organized collagen fibers and greater cartilage regeneration were observed in the intervention groups compared with the CON group, as confirmed by immunohistochemistry for collagen type II. Additionally, the LC group exhibited more new bone formation compared to the CON group at 4 weeks (P < .001). Biomechanically, all intervention groups exhibited significantly higher failure loads and stiffness than the CON group at 4 and 8 weeks. In immune regulation, the expression of CD86 was significantly decreased, and CD206 expression was significantly increased, in the intervention groups compared to the CON group at 4 weeks. However, there were no significant differences in the expression of CD86 and CD206 among the groups at 8 weeks.
Conclusion:
Yoda1 improved tendon-to-bone healing in a rat model of RCR. In addition, Yoda1 promoted the infiltration of M2 macrophages at the repair site, which may have facilitated healing at the tendon-bone interface.
Clinical Relevance:
The present study is an exploratory investigation. Postoperative treatment using Yoda1 could be a potential therapeutic strategy to improve tendon-to-bone healing in patients with rotator cuff tears.
A rotator cuff tear (RCT) is one of the most common shoulder disorders, which leads to shoulder pain and functional impairment. 32 The incidence of RCTs in the general population is approximately 20%, and it significantly increases with age, reaching up to 50% in patients aged >65 years. 2 Currently, arthroscopic rotator cuff repair (RCR) has become a mainstay treatment option for RCTs. However, postoperative retear rates remain high, ranging from 21% to 90%. 10 Studies have shown that the greater tuberosity of the humerus would lose the mechanical load generated by muscle contractions after RCTs, resulting in bone loss at the enthesis. 3 Bone deterioration at the tendon-bone interface has been identified as an independent risk factor for postoperative retears. 54 Bone loss at the humeral tendon attachment compromises the stability of repair anchors, increasing the risk of retears. 48 Additionally, bone loss may alter the local microenvironment, further impeding tendon-to-bone healing. 29 Addressing this issue, strategies aimed at promoting bone formation at the tendon-bone interface have increasingly become a focus in the treatment of RCTs.44-46,51,55
Some treatment strategies that promote bone formation or inhibit bone loss, such as bisphosphonates, have been shown to improve tendon-to-bone healing after RCTs by enhanced bone quality at the enthesis.36,45,46 Xu et al 45 reported that the postoperative administration of risedronate significantly improved proximal humeral bone quality and enhanced biomechanical properties at the tendon-bone interface. Clinical studies 25 have also shown that bisphosphonate therapy after RCR reduced retear rates. Therefore, inhibiting bone loss and increasing bone formation at the repair site may reduce the retear rate.45,46 However, the long-term use of bisphosphonates may increase the risk of osteonecrosis of the jaw and atypical femoral fractures,22,37 which limit the application of bisphosphonates in postoperative management. Therefore, novel approaches to promote bone formation should be explored to improve tendon-to-bone healing after RCR.
Piezo1 is a critical mechanosensitive ion channel protein for the musculoskeletal system, playing an important role in regulating bone homeostasis.9,26 When mechanical stress is applied to osteocytes, the conformation of Piezo1 would be changed on the cell membrane, leading to calcium ion influx and promoting the deposition of mineralized substances in bone.43,49 Yoda1 is a specific agonist of Piezo1 that selectively enhances Piezo1’s sensitivity and range of perception to mechanical loads on the cell membrane.49,53 A previous study 17 showed that Yoda1 promotes the osteogenic differentiation of bone marrow–derived mesenchymal stem cells (BMSCs) in vitro and that Yoda1 enhances cranial defect healing in mice. Furthermore, Gan et al 15 demonstrated that Yoda1 significantly promoted bone formation and accelerated fracture healing in a mouse model. However, whether Yoda1 improves bone quality and promotes tendon-to-bone healing in the rotator cuff remains unclear.
In recent years, macrophage polarization has been recognized as a critical regulator of tendon-to-bone healing. 14 During the early phase of an injury, macrophages predominantly exhibit the M1 phenotype with proinflammatory responses, whereas in the later phase, macrophages polarize to the M2 phenotype, exerting anti-inflammatory effects and promoting tissue repair. 30 Cai et al 5 demonstrated that a local injection of M2 macrophage–derived exosomes into the rotator cuff promoted fibrocartilage regeneration at the tendon-bone interface and improved biomechanical properties. Notably, Piezo1 plays a crucial regulatory role in macrophage-mediated immune responses.30,56 A previous study 4 reported that Piezo1-mediated M2 macrophages promote bone formation through the secretion of transforming growth factor–β1, which suggests that activating Piezo1 may regulate macrophage polarization and improve injury healing. However, whether Yoda1 regulates macrophage polarization at the tendon-bone interface and contributes to rotator cuff healing remains to be investigated.
In the present study, Yoda1 was administered intraperitoneally in rats to investigate whether Yoda1 promotes rotator cuff healing after RCR. We hypothesized that Yoda1 would enhance tendon-to-bone healing in the rotator cuff by promoting osteogenesis and regulating M1/M2 macrophage polarization at the tendon-bone interface.
Methods
Study Design
Animal experiments were approved by the Animal Care and Use Committee of Lanzhou University Second Hospital (No. D2024-816). All relevant institutional and national guidelines for the care and use of animals were strictly adhered to during the study. The overall research process is shown in Figure 1.
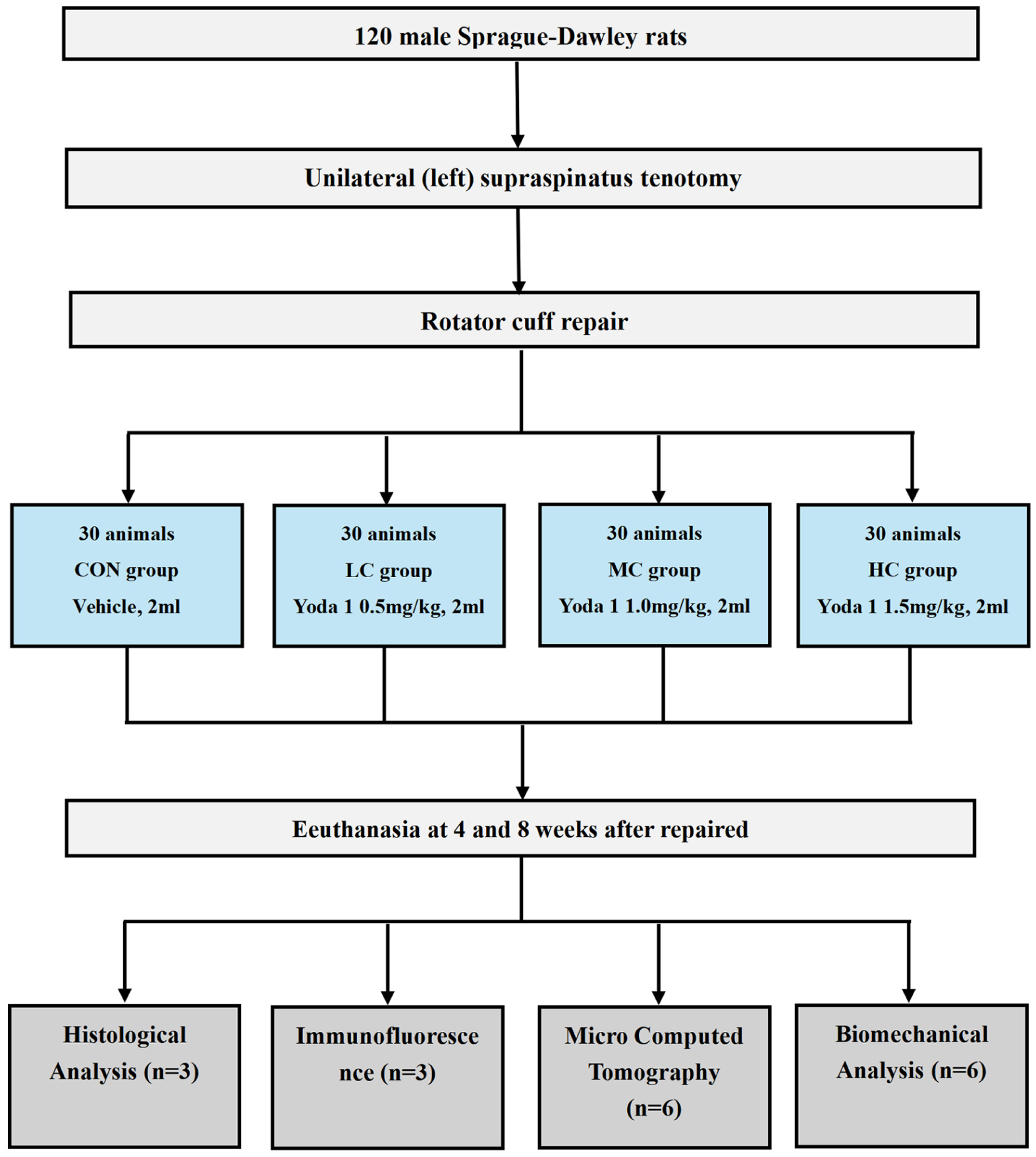
Schematic diagram showing the entire experimental process, group allocation, and methods. CON, control group; HC, high-concentration Yoda1 group; LC, low-concentration Yoda1 group; MC, moderate-concentration Yoda1 group.
All animals were sourced from the Animal Experiment Center of Lanzhou University. A total of 120 twelve-week-old male Sprague Dawley rats weighing 428 ± 48 g were used in this study. All animals were housed in temperature- and humidity-controlled rooms with a 12-hour light-dark cycle. Food and water were allowed to be freely accessed.
Surgical Procedure
After a 1-week acclimatization period, all animals underwent left-sided supraspinatus tendon transection under general anesthesia. A skin incision was made along the anterolateral aspect of the shoulder, and blunt dissection of the deltoid muscle was performed to fully expose the rotator cuff. The supraspinatus muscle was separated from the supraspinous fossa, and the tendon was detached from the bone insertion, creating an RCT. Residual tissue around the greater tuberosity was immediately cleared, and the tendon ends were trimmed. The supraspinatus tendon was repaired using Prolene 4-0 sutures (8557H; Ethicon) with a modified Mason-Allen technique. 51 A 0.8-mm drill was used to create 2 crossed-bone tunnels at the upper and lower ends of the greater tuberosity. Sutures were passed through the bone tunnels and tightened to reattach the supraspinatus tendon to the greater tuberosity. Subsequently, the deltoid muscle was reattached, and the skin was closed. All experimental procedures were carried out in the laboratory. The surgical procedure is illustrated in Figure 2.
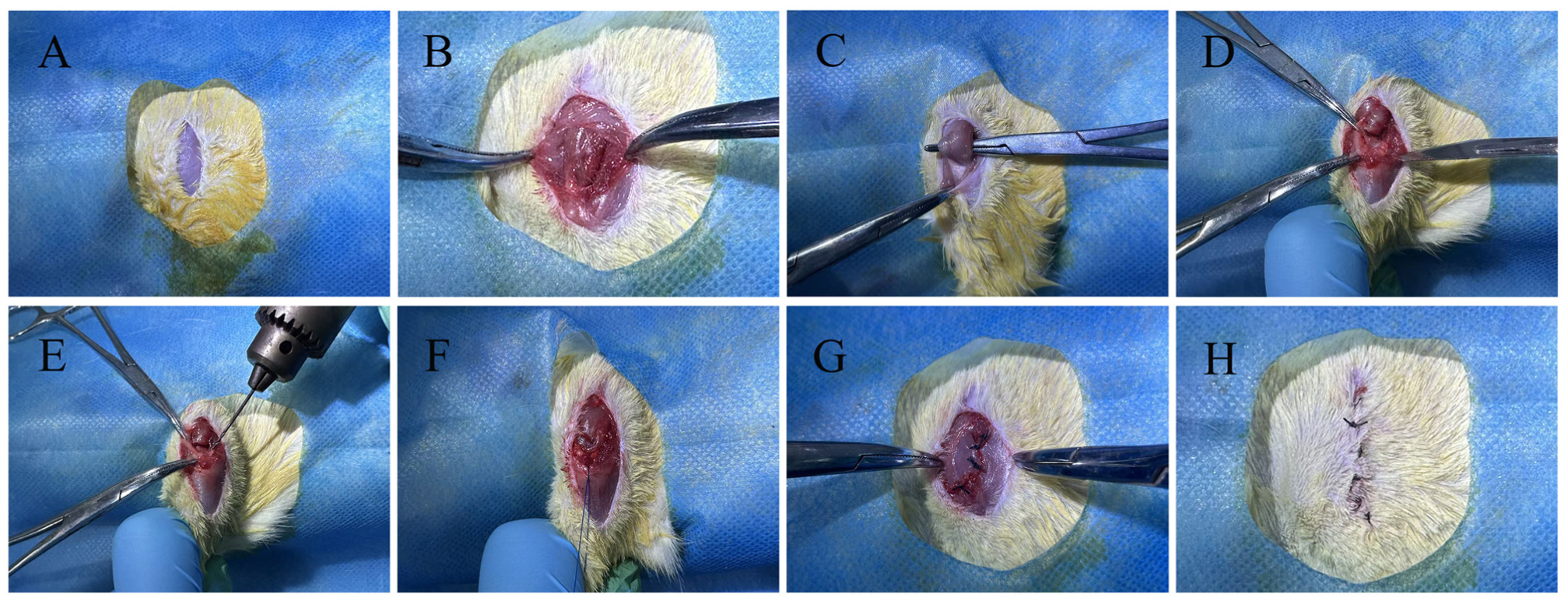
Schematic of the surgical procedure. (A) An incision was made approximately 2 cm along the lateral aspect of the shoulder joint. (B) Blunt dissection of the deltoid muscle was performed. (C) The enthesis was exposed. (D) The supraspinatus tendon was transected from the greater tuberosity of the humerus. (E) A bone tunnel was drilled. (F) The supraspinatus tendon was repaired using a modified Mason-Allen technique. (G) The deltoid muscle was sutured. (H) The skin was sutured.
After RCR, rats were randomly allocated into 4 groups using the random number table method: control group (CON; n = 30; vehicle [2% DMSO, 4% ethanol, 94% saline]), low-concentration Yoda1 group (LC; n = 30; 0.5 mg/kg), moderate-concentration Yoda1 group (MC; n = 30; 1 mg/kg), and high-concentration Yoda1 group (HC; n = 30; 1.5 mg/kg).19,20,33 Yoda1 was dissolved in the vehicle and intraperitoneally injected into rats every 2 days, starting on the second day postoperatively until sacrifice. A single investigator (D.X.), who was not involved in the confirmation of RCTs, administered all the injections.
At 4 and 8 weeks postoperatively, 15 rats from each group were euthanized for subsequent experiments. The left shoulder was excised en bloc. The supraspinatus tendon–humeral complex was separated, and the sutures were removed. Overall, 3 samples from each group were immersed in formalin for histological analysis, while the remaining samples were wrapped in saline-soaked gauze and stored at −20°C for biomechanical testing and micro–computed tomography (micro-CT) (Figure 1).
Histological Analysis
There were 3 samples per group used for histological staining. All samples were fixed in 10% neutral buffered formalin at 4°C for 48 hours and then decalcified using 10% EDTA. The samples were embedded in paraffin after dehydration with 70% ethanol and prepared into 5-μm sections. The sections were stained using hematoxylin and eosin, safranin O/Fast Green, and Masson trichrome. An optical microscope was used to examine the tendon-bone interface. As Xu et al 46 have described, a semiquantitative scoring system was applied to assess tissue quality (Table 1). The metachromasia ratio of the cartilage area and collagen fiber organization were determined using safranin O/Fast Green and Masson trichrome staining, respectively. Semiquantitative analysis of the metachromasia ratio using ImageJ software (National Institutes of Health) was conducted by 2 independent researchers (Y.S. and Z.L.), who were blinded to the intervention groups.
Histological Scoring System a
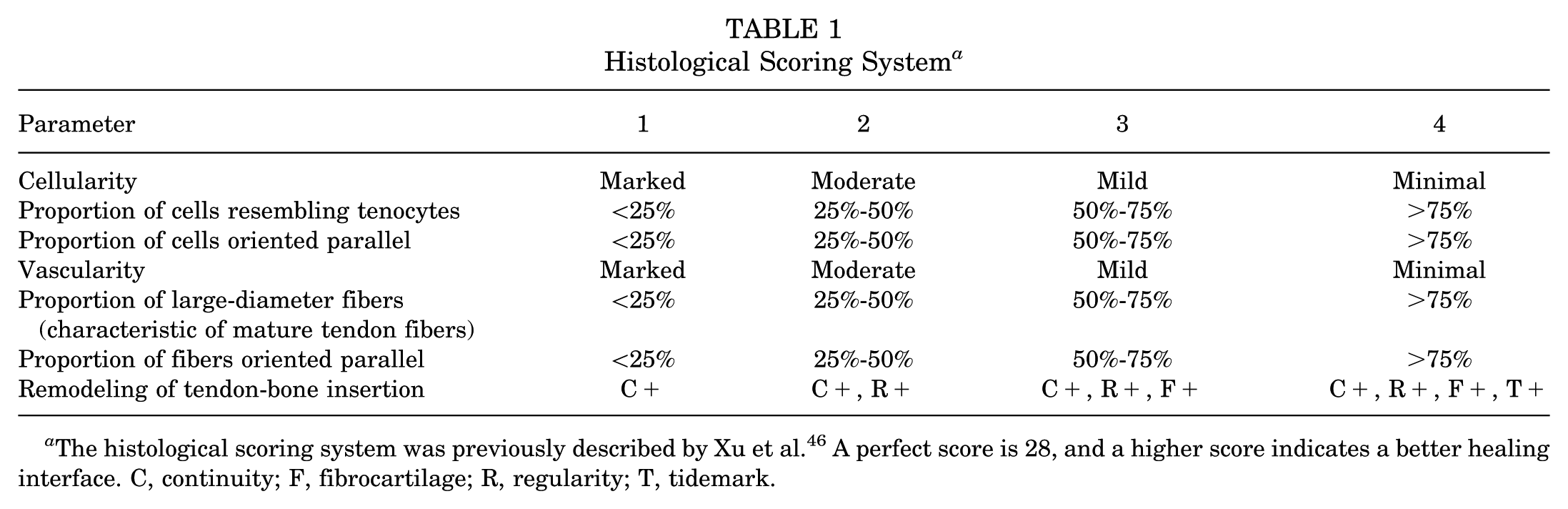
The histological scoring system was previously described by Xu et al. 46 A perfect score is 28, and a higher score indicates a better healing interface. C, continuity; F, fibrocartilage; R, regularity; T, tidemark.
Immunohistochemistry
Collagen type II expression was evaluated at 4 and 8 weeks postoperatively. Immunohistochemical analysis was carried out with the Immunohistochemical Staining Kit (KIT-9720; MXB Biotechnologies). In brief, tissue sections were prepared by cutting 5-μm slices from paraffin-embedded blocks, followed by deparaffinization and rehydration through a graded ethanol series. To block endogenous peroxidase activity, 3% hydrogen peroxide was applied. The sections were then incubated with primary antibodies specific to collagen type II (1:200; Ab185430 [Abcam]) at 4°C for 12 hours. Subsequently, the samples underwent incubation with a secondary antibody and a Novolink polymer (RE7150CE; Leica Biosystems) for 30 minutes each. Peroxidase activity was visualized by developing with a DAB working solution for 5 minutes, and the sections were counterstained with hematoxylin. Semiquantitative analysis of collagen type II using ImageJ software was conducted by 2 independent researchers (Y.S. and Z.L.), who were blinded to the intervention groups.
Bone Morphometric Evaluation
A total of 6 rats from each group were sacrificed at 4 and 8 weeks, and the humerus was carefully dissected to observe any changes in the bone microstructure. All samples were assessed using micro-CT (MNC-200; Pingsheng Medical Technology) for bone microarchitecture analysis under the following conditions: 80 kV, 0.06 mA, 7.5-μm resolution, and 0.051-mm pixel size. 41 The 3-dimensional reconstruction software Recon (Scanco Medical) was used to reconstruct the original images. Data analysis software Avatary (Facegood) was used for analysis of the region of interest, with all samples selected from the same region for analysis. The region of interest included trabecular bone within the humeral head near the tendon insertion and proximal to the growth plate. Again, 2 evaluators (Y.S. and Z.L.), who were blinded to the intervention groups, analyzed the bone morphometric parameters, including bone mineral density (BMD), ratio of bone volume to total volume (BV/TV), trabecular number (Tb.N), and trabecular separation (Tb.Sp). 35
Biomechanical Testing
Biomechanical testing was conducted on 6 supraspinatus tendon–humeral complexes per group at 4 and 8 weeks after RCR. The proximal humerus was secured in the apparatus, and the supraspinatus tendon was wrapped with gauze and sutured using a whipstitch technique. 39 All samples were tested according to the methods described earlier. 50 After preconditioning at 0.1 N, they were subjected to uniaxial tension until failure at a constant speed of 10 mm/min. Testing concluded upon the rupture or failure of the reattached tendon at the repair site. 8 Load-deformation curves were used to determine the failure load and stiffness.
Immunofluorescence
The expression of CD86 and CD206 were assessed at 4 and 8 weeks after surgery. In brief, slides were prepared by cutting 5-μm sections from paraffin blocks, followed by deparaffinization and rehydration through an ethanol gradient. To inhibit endogenous peroxide activity, 3% hydrogen peroxide was applied. The sections were next incubated overnight at 4°C with primary antibodies targeting CD86 at a dilution of 1 µg/mL (942-RBM4-P1; Thermo Fisher Scientific). The samples were then incubated with Alexa Fluor 594–labeled alpaca anti-rabbit secondary antibody (1:200; SA00013-4 [Proteintech]) in the dark for 60 minutes. Similarly, other sections were incubated overnight at 4°C with primary antibodies targeting CD206 (1:200; 60143-1-Ig [Proteintech]). Alexa Fluor 488–labeled alpaca anti-rabbit secondary antibody (1:200; SA00013-2 [Proteintech]) was used to identify the CD206 primary antibodies. Finally, DAPI (G1012-100ML; Servicebio) was added to stain nuclei for 10 minutes. Overall, 3 random 100-μm2 areas were selected, and the average number of positive cells was calculated. The expression levels of CD86 and CD206 were expressed as the number of positive cells per 100 μm2.
Statistical Analysis
Sample size calculation was performed based on preliminary experimental data and prior studies on tendon-to-bone healing in the rotator cuff of Sprague Dawley rats with a power of 0.80 and an alpha of 0.05.46,52 The results suggested that a minimum of 6 shoulder joint samples per group was required to ensure statistical power in biomechanical testing and micro-CT. Data are presented as mean ± standard deviation, with normality assessed via the Shapiro-Wilk test and variance equality evaluated using the Levene test. One-way analysis of variance was utilized to analyze differences among groups, followed by the Bonferroni post hoc test (Prism 10; GraphPad Software). Significance was set at P < .05.
Results
Gross Observation
Throughout the study, all animals exhibited good wound healing, and no deaths occurred because of infections or adverse events. Additionally, continuity between the repaired supraspinatus tendon and bone was observed in all animals. However, no significant differences were seen at any of the time points on gross observation.
Histological Analysis
General Morphological Characteristics
The CON group exhibited more inflammatory cells at 4 weeks after surgery, while the LC group showed relatively fewer cells. Additionally, tissue in the CON group was more disorganized, with poorer collagen fibers. At 8 weeks, inflammatory cells had dissipated in all groups, and collagen fibers began to align more regularly. Compared to the intervention groups, the CON group still showed the poorest collagen fiber alignment. In the LC group, tissue at the tendon-bone interface was more mature than in the other groups (Figure 3A).
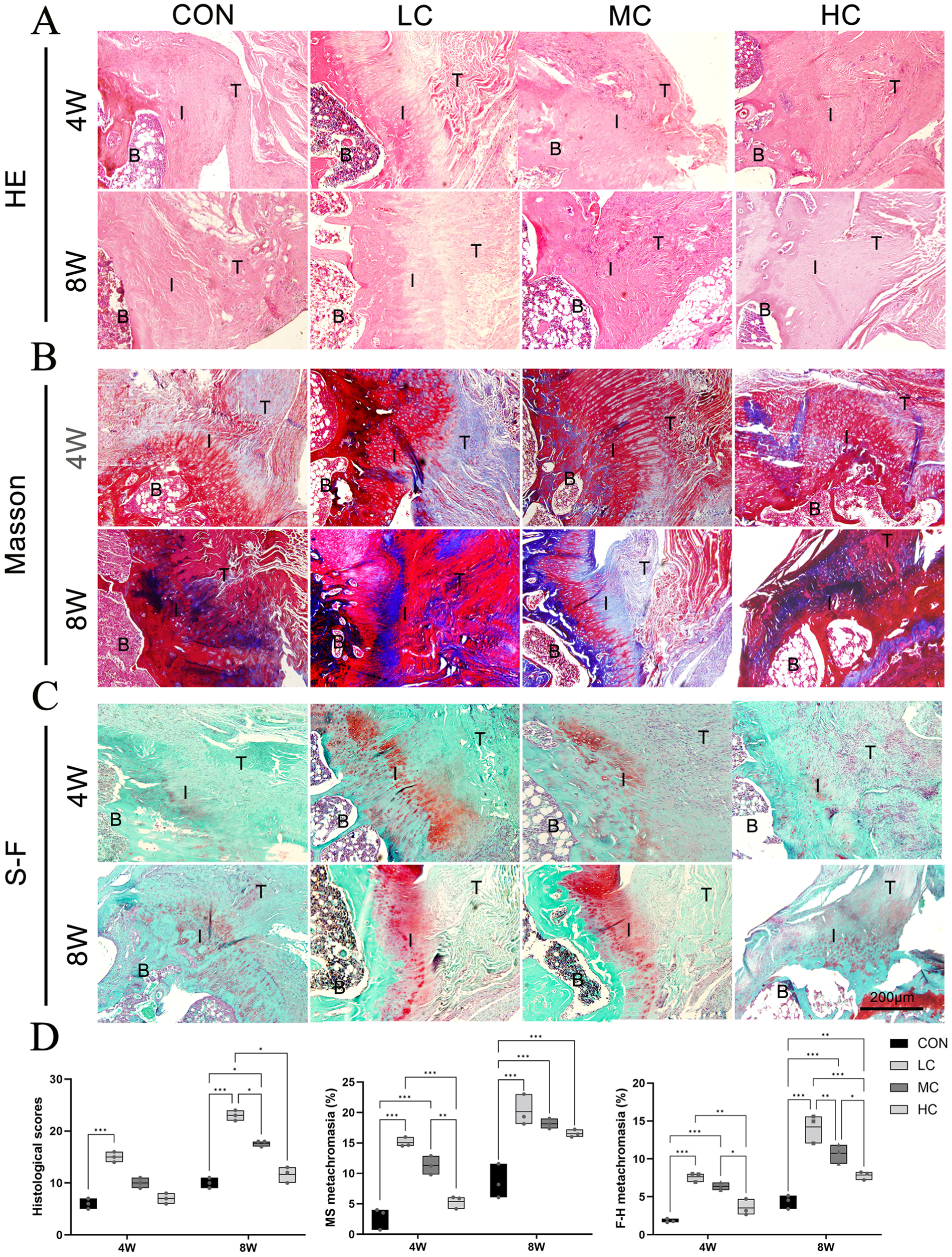
(A) Representative hematoxylin and eosin–stained images at the healing interface. (B) Representative Masson trichrome–stained images at the healing interface. (C) Representative safranin O– and Fast Green–stained images at the healing interface. (D) Histological statistical results. Significant difference: *P < .05, **P < .01, ***P < .001. B, bone; CON, control group; HC, high-concentration Yoda1 group; I, interface; LC, low-concentration Yoda1 group; MC, moderate-concentration Yoda1 group; T, tendon; W, weeks.
Collagen Composition and Organization
The collagen fibers in the intervention groups were more regular and organized compared to the CON group at 4 weeks after RCR. No significant collagen composition was observed in the CON group. Semiquantitative analysis showed that the LC and MC groups had a significantly higher metachromasia ratio than the CON group (15.06 ± 0.80 and 11.31 ± 1.50 vs 2.76 ± 1.76, respectively; all P < .001). At 8 weeks, the collagen fibers in the intervention groups exhibited greater regularity and organization compared to the CON group. Semiquantitative analysis revealed a significantly higher metachromasia ratio in the LC, MC, and HC groups compared with the CON group (20.16 ± 2.55, 18.16 ± 0.82, and 16.54 ± 0.62 vs 8.62 ± 2.78, respectively; all P < .001) (Figure 3B).
Cartilage Area
At 4 weeks, the cartilage area was observed in the LC and MC groups, while cartilage in the CON group was not significant. At 8 weeks, cartilage was observed in all groups, with a significantly larger area in the LC group than the CON, MC, and HC groups (14.21 ± 1.89 vs 10.72 ± 1.26, 7.85 ± 0.54, and 4.37 ± 0.88, respectively; P < .001, P = .007, and P < .001, respectively). Additionally, the MC and HC groups demonstrated greater improvement than the CON group (P < .001 and P = .007, respectively). Generally, the CON group showed a minimal cartilage area, whereas the LC group exhibited the most cartilage compared to the other 3 groups (Figure 3C).
Histological Scoring
At 4 weeks, the LC group presented significantly higher scores compared with the CON group (13.67 ± 1.53 vs 6.00 ± 1.00, respectively; P < .001). Yet, no significant difference was detected between the MC, HC, and CON groups (10.72 ± 1.26 and 6.67 ± 0.58 vs 6.00 ± 1.00, respectively; P = .89 and P > .99, respectively). At 8 weeks, significantly higher scores were found in the LC and MC groups compared to the CON group (23.00 ± 1.00 and 17.67 ± 0.58 vs 10.00 ± 1.00, respectively; P < .001 and P = .02, respectively). There was no significant difference between the HC group and the CON group (11.67 ± 1.23 vs 10.00 ± 1.00, respectively; P > .99).
Immunohistochemistry
Significant differences in collagen type II expression were identified between the CON and intervention groups. At 4 weeks, the expression of collagen type II was 2.78 ± 0.57 in the CON group, 9.22 ± 0.70 in the LC group, and 6.97 ± 0.81 in the MC group (P < .001 and P = .002, respectively). There was no significant difference between the CON group and the HC group (P = .12). Similarly, collagen type II expression in the LC and MC groups was significantly higher than in the CON group at 8 weeks, with the LC group showing the highest expression (21.81 ± 1.75 vs 11.35 ± 1.03, respectively [P < .001] and 16.82 ± 1.12 vs 11.35 ± 1.03, respectively [P < .001]). There was no significant difference between the CON group and the HC group at 8 weeks (11.35 ± 1.03 vs 13.22 ± 0.86, respectively; P = .32) (Figure 4).
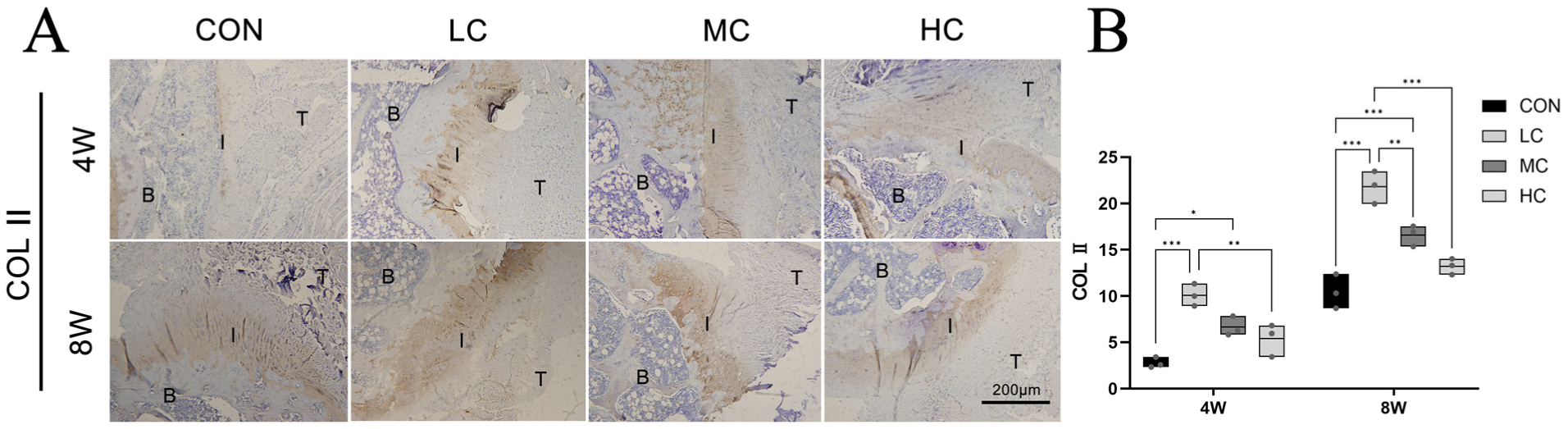
(A) Immunohistochemical staining image of collagen type II at the healing interface. (B) The expression of collagen type II was quantified at the healing interface. Significant difference: *P < .05, **P < .01, ***P < .001. B, bone; CON, control group; HC, high-concentration Yoda1 group; I, interface; LC, low-concentration Yoda1 group; MC, moderate-concentration Yoda1 group; T, tendon; W, weeks.
Micro-CT
At each time point, significant bone loss and bone microstructure damage were observed at the humeral greater tuberosity insertion site in the CON group. However, in the intervention groups, bone loss was significantly reduced, and a higher bone density was observed. Bone formation was more pronounced in the LC group compared to the MC and HC groups. At 4 weeks, the BMD in the CON group (1.35 ± 0.03) was significantly lower than that in the LC group (1.46 ± 0.03; P < .001), MC group (1.42 ± 0.01; P < .001), and HC group (1.40 ± 0.02; P < .03). Moreover, a significantly greater BV/TV was observed in the LC, MC, and HC groups compared with the CON group (55.77 ± 2.82, 50.20 ± 2.79, and 49.32 ± 3.97 vs 42.52 ± 1.29, respectively; P < .001, P = .003, and P = .01, respectively). The Tb.N was significantly greater in the LC and MC groups (1.71 ± 0.15 and 1.66 ± 0.13, respectively) than the CON group (1.35 ± 0.15) (P < .001 and P = .005, respectively). A significantly lower Tb.Sp was found in the LC, MC, and HC groups compared to the CON group (P < .001, P < .001, and P = .02, respectively). At 8 weeks, the LC and MC groups exhibited a significantly higher BMD at the humeral head tendon insertion site compared to the CON group (1.52 ± 0.04 and 1.50 ± 0.03 vs 1.44 ± 0.02, respectively; P < .001 and P = .007, respectively). Additionally, the BV/TV was significantly higher in the LC group than in the CON group. However, there was no significant difference in the Tb.N and Tb.Sp between the intervention groups and the CON group at 8 weeks (Figure 5).
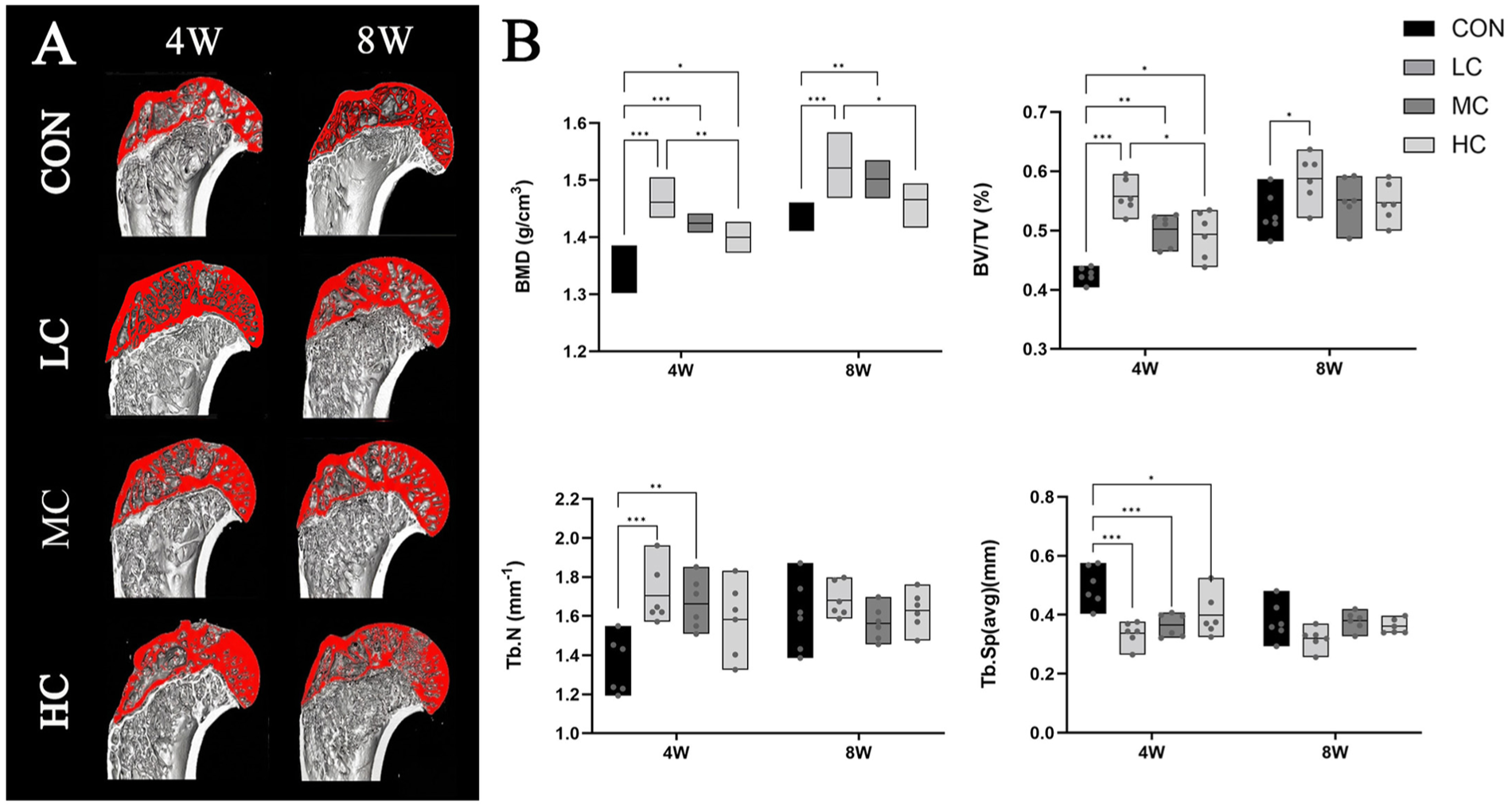
(A) Representative reconstructed micro–computed tomography images showing the bone microarchitecture in the 4 groups at both 4 and 8 weeks. The region of interest is labeled in red including trabecular bone within the humeral head near the tendon insertion and proximal to the growth plate. (B) Quantitative bone microarchitecture results at the tendon insertion site of the humeral head. Significant difference: *P < .05, **P < .01, ***P < .001. BMD, bone mineral density; BV/TV, ratio of bone volume to total volume; CON, control group; HC, high-concentration Yoda1 group; LC, low-concentration Yoda1 group; MC, moderate-concentration Yoda1 group; Tb.N, trabecular number; Tb.Sp, trabecular separation; W, weeks.
Biomechanical Testing
At 4 weeks after RCR, significantly higher failure loads were found in the LC and MC groups compared with the CON group (13.70 ± 2.86 and 10.10 ± 3.09 N vs 4.80 ± 1.33 N, respectively; P < .001 and P = .009, respectively). No significant difference was observed in failure loads between the HC and CON groups (P = .75). Notably, the LC group showed significantly higher failure loads than the HC group (P = .002). At 8 weeks, the LC, MC, and HC groups revealed significantly higher failure loads than the CON group (20.16 ± 2.50, 16.50 ± 3.50, and 14.82 ± 2.07 N vs 9.64 ± 1.83 N, respectively; P < .001, P < .001, and P = .01, respectively). Similarly, the LC group (2.53 ± 0.63 N/mm; P = .009) and MC group (2.54 ± 0.78 N/mm; P = .008) showed significantly higher stiffness at 4 weeks compared with the CON group (0.61 ± 0.11 N/mm). However, only the LC group (5.22 ± 1.87 N/mm) demonstrated significantly higher stiffness compared to the CON group at 8 weeks. No significant difference was observed among the MC, HC, and CON groups, while stiffness in the MC and HC groups (3.24 ± 0.72 and 3.26 ± 0.79 N/mm, respectively) remained higher than in the CON group (2.20 ± 0.74 N/mm) (P = .66 and P = .60, respectively) (Figure 6).
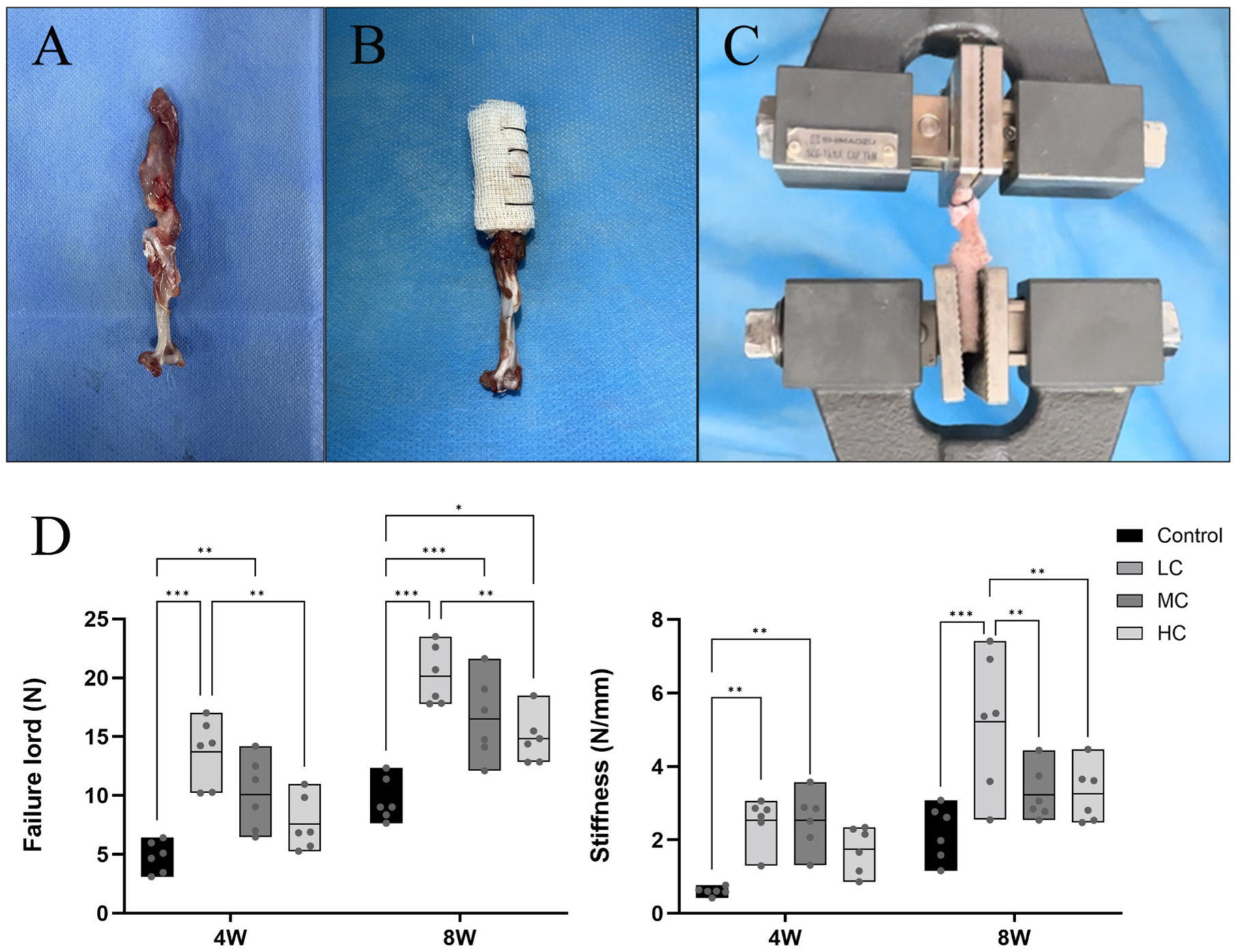
(A) Gross observation of the supraspinatus tendon–humeral complex. (B) The supraspinatus tendon was covered using gauze and woven using sutures in a whipstitch style. (C) The specimen was fixed in the machine using clamps for biomechanical testing. (D) Biomechanical results of failure load and stiffness. Significant difference: *P < .05, **P < .01, ***P < .001. CON, control group; HC, high-concentration Yoda1 group; LC, low-concentration Yoda1 group; MC, moderate-concentration Yoda1 group; W, weeks.
M1/M2 Macrophage Expression
To investigate changes in the immune environment at the repair site, the expression of CD86 and CD206, the markers of M1 and M2 macrophages, was detected at 4 and 8 weeks postoperatively (Figure 7). Notably, the LC group (2.33 ± 0.67), MC group (2.44 ± 0.77), and HC group (2.22 ± 1.07) exhibited significantly lower numbers of CD86-positive cells compared with the CON group (6.22 ± 1.35) (all P < .001). A significantly higher number of CD206-positive cells was observed in the LC group (8.33 ± 1.34; P < .001), MC group (8.00 ± 1.46; P < .001), and HC group (7.33 ± 0.67; P = .002) than in the CON group (3.56 ± 1.02) at 4 weeks, which suggests that the activation of Piezo1 inhibits M1 macrophage infiltration and promotes M2 macrophage polarization at the repair site. Furthermore, the LC, MC, and HC groups (0.28 ± 0.04, 0.33 ± 0.17, and 0.31 ± 0.17, respectively; all P = .03) showed a significantly lower ratio of CD86 to CD206 compared to the CON group (1.92 ± 0.91). However, only sporadic CD86- and CD206-positive cells were observed at the repair site at 8 weeks postoperatively. Although the LC and MC groups (0.37 ± 0.07 [P = .01] and 0.58 ± 0.27 [P = .03], respectively) still showed a significantly lower ratio of CD86 to CD206 than the CON group (2.16 ± 1.14), there were no significant differences in the number of CD86- and CD206-positive cells among the LC, MC, and HC groups compared with the CON group (Figure 7).
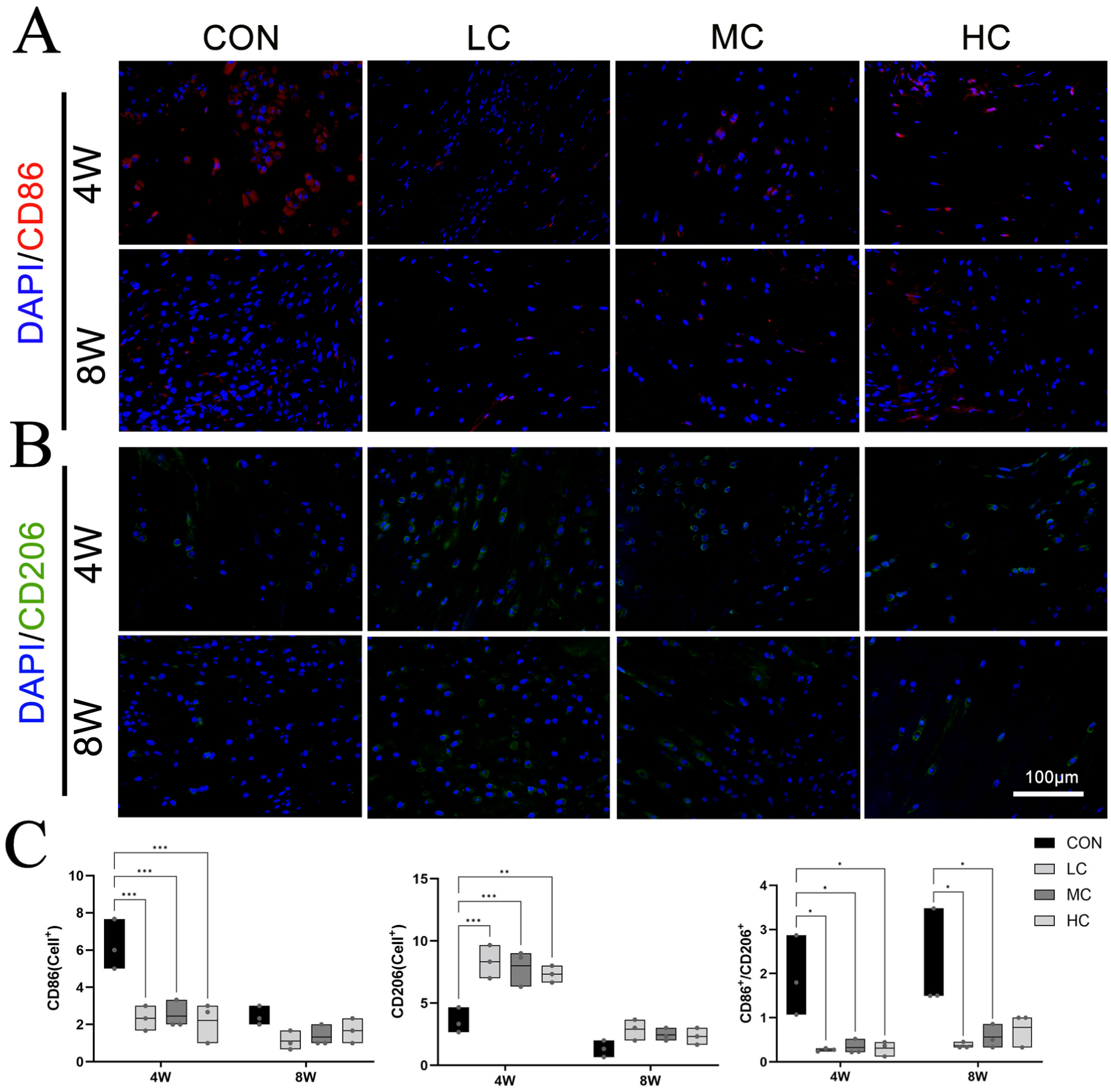
(A) Immunofluorescence staining image of CD86. (B) Immunofluorescence staining image of CD206. (C) Immunofluorescence staining results. Significant difference: *P < .05, **P < .01, ***P < .001. CON, control group; HC, high-concentration Yoda1 group; LC, low-concentration Yoda1 group; MC, moderate-concentration Yoda1 group; W, weeks.
Discussion
The present study aimed to investigate the effect of Yoda1 administration in rotator cuff healing. One of the most important findings of this study was that Yoda1 promoted bone formation at the enthesis and enhanced tendon-to-bone healing in the rotator cuff of rats after RCR. Moreover, Yoda1 suppressed M1 macrophage infiltration while enhancing M2 macrophage polarization at the tendon-bone interface, which may potentially contribute to improved rotator cuff healing.
Currently, although the role of Piezo1 in promoting osteogenesis has been demonstrated in many studies, research is very limited regarding the role of Piezo1 in rotator cuff healing. Anderson et al 1 found that the functional expression of Piezo1 was downregulated in glenohumeral chondrocytes during the early stages of RCTs in a mouse model, leading to a significant decrease in intracellular calcium ion influx. In our study, we established 3 experimental groups with different concentrations of Yoda1 injections to preliminarily explore the role of Piezo1 in rotator cuff healing. We found that the LC group exhibited a higher bone density and greater failure loads compared to the MC and HC groups, indicating that the appropriate activation of Piezo1 activity was the optimal solution for improving rotator cuff healing rather than overactivation. This may be related to the desensitization of Piezo1 after excessive activation with high doses of Yoda1. 40
Bone loss is an independent risk factor for tendon-bone reconstruction, which occurs at various tendon-bone interfaces, including the anterior cruciate ligament, the Achilles tendon, and the rotator cuff.11,38,46 Tanaka et al 41 found that osteoporotic rats induced with estrogen deficiency had decreased biomechanical properties and poor development of tissue at the tendon-bone reattachment site compared with rats with normal bone quality. In a clinical study, Cancienne et al 6 reported that a higher postoperative rotator cuff retear rate was observed in patients with osteoporosis compared to those with a normal bone density. Therefore, improving bone quality at the tendon-bone reconstruction site could be an effective approach to reduce the risk of retears after RCR. Xu et al 45 provided evidence that the postoperative administration of risedronate resulted in an enhanced BMD at the greater tuberosity of the humerus and improved tendon-to-bone healing after RCR. Moreover, Lee et al 25 indicated that the postoperative retear rate in patients with osteoporosis was comparable and even showed a trend of lower retear rates compared to patients with a normal bone density at 6 months when injected with zoledronic acid. In our study, we found that the injection of an appropriate dose of Yoda1 significantly increased the BMD, BV/TV, and Tb.N at the humeral tendon-bone junction. Furthermore, the LC group exhibited a lower Tb.Sp compared to the CON group. This suggests that the injection of an appropriate dose of Yoda1 inhibited bone loss and enhanced new bone formation. This may be related to the activation of Piezo1, which promotes calcium ion influx and accelerates mineral accumulation.
The enhanced biomechanical performance was considered to be related to improved bone quality. 46 Additionally, higher mechanical performance may be an important safeguard in reducing the retear rate. 34 Numerous studies have demonstrated that anti-osteoporosis treatment enhances the biomechanical properties of the tendon-bone repair site after surgery.23,34,45,46 Cadet et al 3 reported that administering zoledronic acid significantly improved the failure load of the tendon-bone complex and enhanced the BMD in the proximal humerus, although they demonstrated no significant histological differences at the tendon-bone interface. In our study, we found that as bone quality at the tendon attachment site increased, the maximum failure load of the supraspinatus tendon–humeral complex also increased. This is consistent with the results of clinical studies in which the use of anti-osteoporosis therapies to improve bone quality reduced the retear rate after RCR. 31
The native tendon-bone insertion site is composed of 4 layers: tendon, unmineralized fibrocartilage, mineralized fibrocartilage, and bone. 13 This specialized structure ensures the efficient transmission of force from the muscle to bone. 2 Therefore, restoring the native tendon-bone structure after RCR is crucial for reducing the risk of retears. However, the use of first-line anti-osteoporosis drugs, such as bisphosphonates, in improving histological healing at the tendon-bone interface remains controversial.3,18,21,34,45 Xu et al 45 found that risedronate significantly enhanced cartilage regeneration and collagen composition. In addition, the risedronate group showed higher histological scores than the control group. 45 In contrast, Hjorthaug et al 18 reported the negative effects of zoledronic acid on tendon-to-bone healing. This discrepancy may be attributed to differences at the anatomic tendon-bone repair site. The lower availability of BMSCs in the distal tibia compared with the proximal humerus may limit the healing potential. Furthermore, the inhibition of osteoclast activity by zoledronic acid could delay the transition from woven bone to lamellar bone, thereby impairing tendon-to-bone healing, which suggests that bisphosphonates may not be the optimal approach for promoting tendon-to-bone healing after RCR. 18 In the present study, we observed more cartilage regeneration and collagen formation in the Yoda1 intervention groups. The LC and MC groups showed higher semiquantitative histological scores compared to the CON group. In addition, increased levels of collagen type II were observed in the Yoda1 intervention groups. This suggests that Yoda1 improved tissue maturity at the tendon-bone interface and enhanced rotator cuff healing.
Macrophages, as one of the most important cells in regulating the body's immune system, have been shown to play a crucial role in promoting tissue repair. 30 Regulating macrophage polarization through various methods, particularly supporting M2 macrophage polarization, has been proven to be helpful in promoting tendon-to-bone healing after RCR.12,28,42 In an animal experiment, Chen et al 7 transplanted a hydrogel loaded with a BMSC-conditioned medium at the rotator cuff's tendon-bone repair site. They found that the BMSC-conditioned medium induced macrophage polarization toward the M2 type and promoted tissue maturation at the tendon-bone interface. However, in a rat model of RCR in which macrophage apoptosis was induced, the BMSC-conditioned medium lost its advantages in the absence of macrophages. It is worth mentioning that macrophages have been shown to be mechanosensitive, and their phenotype can be regulated by mechanical signals. Dong et al 12 found that mechanical stretching stimulated macrophages to polarize toward the M2 type and promoted the osteogenic differentiation of BMSCs. Consistent with Dong et al, 12 the current study found that the expression of M2 macrophages was significantly increased at the repair site after a Yoda1 injection. The tendon-bone interface with more M2 macrophages exhibited a greater bone density and higher histological scores. This may be because of activation of the Piezo1/YAP signaling pathway, which induces macrophages to polarize toward the M2 type, releasing platelet-derived growth factor and bone morphogenetic protein–2 to promote osteogenic differentiation and angiogenesis at the repair site.12,42
There are some limitations that should be noted in this study. First, an animal experiment using a rat model of RCR was conducted to investigate tendon-to-bone healing. The anatomic structure of the rat shoulder joint, weightbearing, and movement ranges of the upper limb differ from those of humans. 45 In addition, rats have superior postinjury healing ability compared to humans, which might affect the applicability of our results. 13 Moreover, there were limitations in the choice of the animal injury model. RCTs are more common in elderly patients and are often chronic injuries. In our study, we selected 12-week-old young rats as the subjects, and an acute RCT was induced in the rats. This might not represent the chronic injury status of patients with RCTs in the elderly. 55 Future studies should establish a chronic injury model in elderly rats. Second, the administration method and frequency of Yoda1 were determined based on previous studies.19,20,33 Although an intraperitoneal injection of Yoda1 exerts its function at the tendon-bone interface, the potential impact of Yoda1 on other systems of the body was not evaluated. Studies have indicated that the activation of Piezo1 may promote fibrotic processes in multiple organs, including the heart, lungs, and kidneys.27,47,53 This raises the potential of side effects regarding the systemic administration of Yoda1. Future research should explore localized drug delivery strategies to minimize such possible adverse effects. Finally, although this study presents an innovative approach to enhancing tendon-to-bone healing using Yoda1, several pharmacological and translational challenges remain to be addressed before clinical application. Yoda1 is characterized by poor aqueous solubility, 16 necessitating the use of organic solvents such as DMSO for in vivo administration, which may complicate the development of formulations. 24 In addition, the extent of Yoda1 delivery to the tendon-bone interface has not been determined, leaving uncertainty regarding the relationship between local drug concentrations and the observed therapeutic effect. Therefore, these limitations highlight the need for further formulation optimization and comprehensive safety evaluations before considering clinical translation.
Conclusion
Yoda1 promoted bone formation at the enthesis and enhanced tendon-to-bone healing in the rotator cuff of rats after RCR. Moreover, Yoda1 suppressed M1 macrophage infiltration while enhancing M2 macrophage polarization at the tendon-bone interface, which may potentially contribute to improved rotator cuff healing. Therefore, treatment with Yoda1 presents a possibility for promoting tendon-to-bone healing after RCR.
Footnotes
Submitted October 23, 2025; accepted April 3, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was funded by the National Natural Science Foundation of China (82160422 and 82460433); the Central University Basic Research Fund of China (lzujbky-2024-ey11); and the Natural Science Foundation of Gansu Province (21JR7RA393 and 22JR11RA072).