
Abstract
Background:
Patients with femoroacetabular impingement syndrome (FAIS) experiencing >2 years of pain before hip arthroscopy have been linked with worse short-term and midterm outcomes.
Purpose:
To examine the effect of preoperative pain duration on patient-reported outcomes (PROs), clinically significant outcomes, and reoperation rates in patients undergoing primary hip arthroscopy for FAIS.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A prospectively maintained surgical repository was reviewed to select patients who underwent primary hip arthroscopy for FAIS between January 2012 and October 2014 with 10-year follow-up. Patients who reported pain ≥2 years before surgery were propensity score matched 1:1 to patients reporting preoperative pain <2 years by age, sex, and body mass index (BMI). PRO scores collected included those for the Hip Outcome Score–Activities of Daily Living (HOS-ADL), Hip Outcome Score–Sports Subscale (HOS-SS), modified Harris Hip Score (mHHS), and visual analog scale (VAS) for pain and satisfaction. Achievement rates of the minimal clinically important difference and patient acceptable symptom state were compared. Reoperation-free survivorship was compared with Kaplan-Meier analysis.
Results:
A total of 164 patients who had a symptom duration ≥2 years (mean age, 35.9 ± 11.7 years; 64.0% female; mean BMI, 25.3 ± 5.2 kg/m2) were successfully matched to 164 patients who had a symptom duration <2 years (mean age, 35.8 ± 11.9 years; 64.6% female; mean BMI, 25.3 ± 4.7 kg/m2). Patient characteristics were similar between groups. Preoperative and 2-year PRO scores were similar between groups. At 10 years, the prolonged pain group had worse mHHS (P = .027), higher VAS pain (P = .002), and lower VAS satisfaction (P = .002) scores than the short pain group. The prolonged pain group also had significantly lower achievement rates of the minimal clinically important difference for the HOS-ADL (P = .024) and HOS-SS (P = .039) and lower achievement rates of the patient acceptable symptom state for the VAS pain (P = .006) and at least 1 PRO measure (P = .041). Reoperation-free survivorship did not differ between groups (P = .11).
Conclusion:
Patients with pain ≥2 years before undergoing primary hip arthroscopy for FAIS significantly improved at 10 years but experienced worse function, pain, satisfaction, and achievement of clinically significant outcomes, with similar survivorship, compared to a matched group of patients with preoperative pain <2 years.
Femoroacetabular impingement syndrome (FAIS) has been shown to be a cause of hip pain in young and active adults, with an increasing incidence over the past 2 decades.16,38 Hip arthroscopy has been utilized as an effective minimally invasive treatment option to correct bony morphology and repair soft tissue while preserving the capsule.10,14 Long-term studies examining the effects of various preoperative characteristics and predictors continuously refine the indications for the procedure and have shown consistent improvements in patient outcomes.6,7,25
Traditionally, in the orthopaedic literature, a longer duration of preoperative symptoms has been negatively correlated with patient outcomes after surgery.9,29,37 In hip arthroscopy, short-term and midterm studies have found worse patient-reported outcomes (PROs) and delayed achievement of clinically significant outcomes (CSOs) in patients with prolonged preoperative pain ≥2 years.3,23,24,39 Kim et al 23 performed a systematic review of 6 primary hip arthroscopy studies (3298 hips) and determined that patients with a prolonged pain duration experienced worse 2-year outcomes and higher rates of revision hip arthroscopy and conversion to total hip arthroplasty (THA). It has been suggested that delays in a surgical intervention can lead to pathological compensatory mechanisms or dysfunctional pain pathways, which may play a role in more limited recovery postoperatively compared to more acutely presenting patients.17,19,26 In addition, untreated symptomatic impingement within the joint can lead to the development of additional cartilage wear and secondary osteoarthritis.20,36
To date, long-term studies within the hip arthroscopy literature examining preoperative pain duration and patient outcomes have not been described. Thus, the purpose of the current study was to determine the effects of a prolonged preoperative pain duration on 10-year PROs, CSOs, and reoperation rates after hip arthroscopy for FAIS. We hypothesized that patients with a preoperative pain duration ≥2 years would have worse short-term and long-term PROs and CSOs with a higher rate of reoperations.
Methods
Patient Selection
This study was approved by the local institutional review board (No. 23092101-IRB01). A prospectively maintained surgical repository was retrospectively reviewed to identify patients who underwent primary hip arthroscopy between January 2012 and October 2014. The following inclusion criteria were utilized: (1) primary hip arthroscopy, (2) clinical and radiographic diagnoses of FAIS, 34 and (3) mean 10-year follow-up. The following exclusion criteria were utilized: (1) prior ipsilateral hip surgery, (2) hip abnormalities other than FAIS, (3) concomitant hip procedures at the time of surgery (eg, gluteus medius/minimus repair, psoas lengthening, core decompression, iliotibial band lengthening), (4) Tönnis grade >1, (5) history of hip disorders (eg, slipped capital femoral epiphysis, Legg-Calve-Perthes disease), (6) hip dysplasia (defined as a lateral center edge angle [LCEA] <18°), 28 and (7) no 10-year follow-up. A follow-up compliance rate of 70% was used, meaning that at least 70% of eligible patients within the time frame had 10-year scores for at least 1 PRO measure. This threshold was similar to that in prior long-term studies to maintain the reliability and validity of the findings.7,13 Before surgery, patients were required to have failed a course of nonoperative management, which included activity modification, anti-inflammatory medications, and physical therapy.21,32 In cases of an atypical clinical presentation of FAIS, intra-articular injections were sometimes utilized as both a diagnostic and therapeutic tool. 22
Surgical Technique and Rehabilitation
All hip arthroscopic procedures were performed at a high-volume academic center by a single fellowship-trained hip surgeon (S.J.N.) using techniques that have been well described in the literature.4,30 To summarize, anterolateral and midanterior portals were established under traction with fluoroscopic guidance. Interportal capsulotomy was created between portals, and intra-articular abnormalities, such as labral tears, were addressed in the central compartment. If the labrum's tissue quality was too poor for repair, labral debridement versus reconstruction was performed. After traction release, the interportal capsulotomy site was extended distally at the midpoint to create T-capsulotomy for access to the peripheral compartment. The leaflets of the iliofemoral ligament were tagged with sutures for retraction and visualization. Cam morphology was resected under fluoroscopic guidance until an adequate femoral head-neck offset was achieved. On completion, a dynamic examination of the operative leg was performed under direct arthroscopic visualization and under fluoroscopy to confirm an appropriate resolution of impingement. The capsule was then closed using a suture-shuttling system, and plication was performed depending on the degree of capsular laxity. All procedures were performed on an outpatient basis, and all patients were discharged home from the postanesthesia care unit on the day of surgery. A 4-phase rehabilitation program was started on postoperative day 1 for all patients as previously described. 21
Patient, Radiographic, and Intraoperative Variables
Patient characteristics, including sex, BMI, follow-up time, weekly physical activity participation, and other preoperative data, were obtained via a chart review. Preoperative hip pain duration is part of every patient history taking as standard practice during new patient visits and was documented for each patient. Patients were considered to have prolonged preoperative pain if their onset of pain occurred ≥2 years before their primary hip arthroscopy date. Standard preoperative and postoperative radiographs were obtained for all patients. The anterior-posterior view was used to measure the LCEA, Tönnis angle, and Tönnis grade, while the 90° lateral Dunn view was used to measure the alpha angle. Intraoperative findings were collected, including the Beck classification of acetabular cartilage damage and the ICRS (International Cartilage Regeneration and Joint Preservation Society) classification of femoral head cartilage damage.5,8 Procedures performed, including labral repair, acetabular rim trimming, osteochondral femoroplasty, and capsular plication, were recorded during surgery.
PROs and CSOs
PROs were collected preoperatively and at 2 and 10 years after surgery through a secure, semiautomated PRO collection software platform (PatientIQ). When eligible for follow-up at the time points above, patients were emailed, texted, and called each week for the first month and monthly thereafter if there was no response. The PROs collected included scores for the Hip Outcome Score–Activities of Daily Living (HOS-ADL), Hip Outcome Score–Sports Subscale (HOS-SS), modified Harris Hip Score (mHHS), and visual analog scale (VAS) for pain and satisfaction. Endpoints were defined as reoperations (revision arthroscopy or total hip replacement). Further PROs past these endpoints were not collected.
Cohort-specific thresholds for the minimal clinically important difference (MCID) and patient acceptable symptom state (PASS) were determined by the distribution method and an anchor question, respectively.27,31 MCID thresholds were determined by taking half the standard deviation of the difference between preoperative and final PRO scores. For the PASS, binary responses to an anchor question (“Taking into account all the activities you have during your daily life, your level of pain, and also your functional impairment, do you consider that your current state is satisfactory?”) were used to generate a receiver operating characteristic curve for each PRO measure. 15 An area under the curve ≥0.70 was regarded as clinically useful. 33 MCID and PASS thresholds were established for each PRO measure, respectively: HOS-ADL (9.7 and 87.4), HOS-SS (15.1 and 64.6), mHHS (9.4 and 74.7), and VAS pain (–15.0 and 29.1). Final PRO scores beyond determined thresholds were deemed to have achieved the MCID/PASS for a given PRO measure. CSO achievement rates for each PRO measure were compared between patients with prolonged preoperative pain and those with short preoperative pain. Outcomes on these patients may have been reported by prior studies,7,18 but this study offers a unique analysis on new groups and outcomes at long-term follow-up.
Statistical Analysis
Propensity score matching was performed 1:1 using nearest neighbor matching to minimize baseline differences between patients with ≥2 years of preoperative pain and those with <2 years. Propensity scores were estimated via logistic regression using age, sex, body mass index (BMI), and Tönnis grade as covariates. A cutoff of 2 years was used as previously described by literature examining preoperative pain duration and outcomes in hip arthroscopy.23,24,39 The caliper was set to 0.2, as previous literature has demonstrated that this caliper width eliminates >98% of bias. 2 After matching, covariate balance was evaluated using standardized mean differences (SMDs) and variance ratios (VRs), with adequate balance defined as an absolute SMD <0.10 and a VR between 0.5 and 2.0. The independent-samples t test was used to compare differences in PROs between groups. All statistical tests were 2-tailed, and a statistically significant difference was established at a level of .05 (P < .05). Continuous variables are reported as mean ± standard deviation unless stated otherwise. Categorical variables are reported as frequencies and percentages and were compared with the Fisher exact test. An a priori power analysis demonstrated that to achieve 80% power with an alpha of 0.05 and an expected mean difference of 8 on the mHHS between groups, 53 patients were required in each group. 12 Statistical analyses were conducted using R statistical software (Version 4.2.3; R Core Team).
Results
Patient, Radiographic, and Intraoperative Data
A total of 852 patients underwent hip arthroscopy for FAIS between January 2012 and October 2014. After applying exclusion criteria, 215 patients were lost to follow-up, and 503 patients remained eligible for matching (Figure 1). Overall, 164 patients who had a preoperative pain duration ≥2 years (mean age, 35.9 ± 11.7 years; 64.0% female; mean BMI, 25.3 ± 5.2 kg/m2) were successfully matched to 164 patients who had a preoperative pain duration <2 years (mean age, 35.8 ± 11.9 years; 64.6% female; mean BMI, 25.3 ± 4.7 kg/m2). Before matching, clinically meaningful imbalance was observed in age and BMI, with absolute SMDs >0.10. After matching, all matched covariates demonstrated excellent balance, with absolute SMDs ≤0.03 and VRs between 0.96 and 1.20, consistent with successful matching.
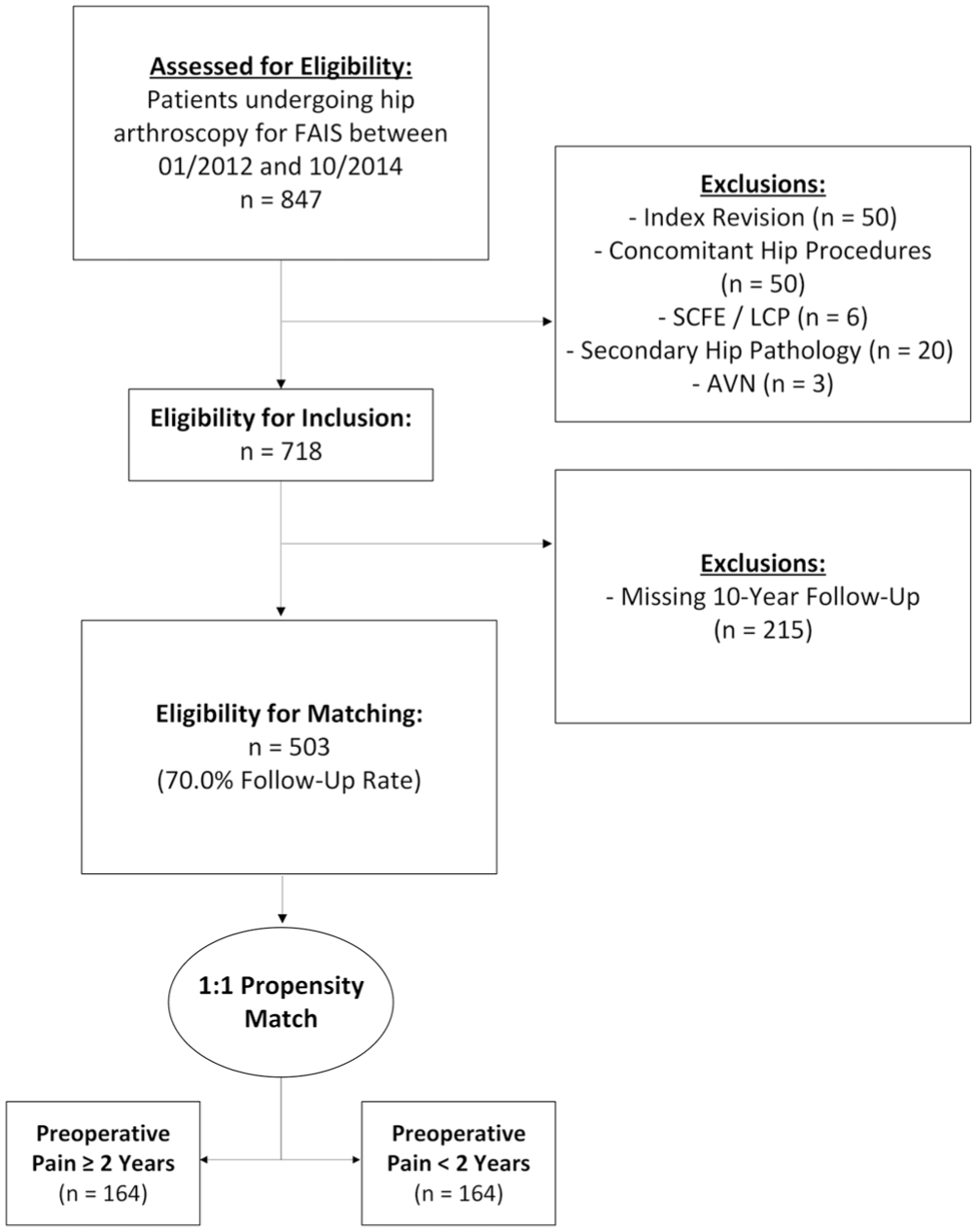
CONSORT (Consolidated Standards of Reporting Trials) diagram of patient selection and matching processes for those undergoing primary hip arthroscopy (HA) for femoroacetabular impingement syndrome (FAIS) between January 2012 and October 2014. AVN, avascular necrosis; LCP, Legg-Calve-Perthes disease; SCFE, slipped capital femoral epiphysis.
The follow-up duration did not differ significantly between the prolonged and short pain groups (10.4 ± 0.5 vs 10.4 ± 0.5 years, respectively; P = .64). There were no significant differences between groups regarding age, sex, BMI, percentage of patients with a psychiatric history (P > .99), percentage reporting concomitant back pain (P = .78), percentage reporting exercise ≥1 time a week (P = .32), those who refilled their opioid prescription postoperatively (P = .75), and those who had a previous narcotic prescription (P = .08). Preoperative radiographic findings, such as LCEA, Tönnis angle, or alpha angle, did not differ between groups. In addition, because of matching, the prolonged pain group had a similar incidence of Tönnis grade 1 (17.1% vs 16.5%, respectively; P > .99) compared to the short pain group (Table 1).
Patient and Radiographic Characteristics a
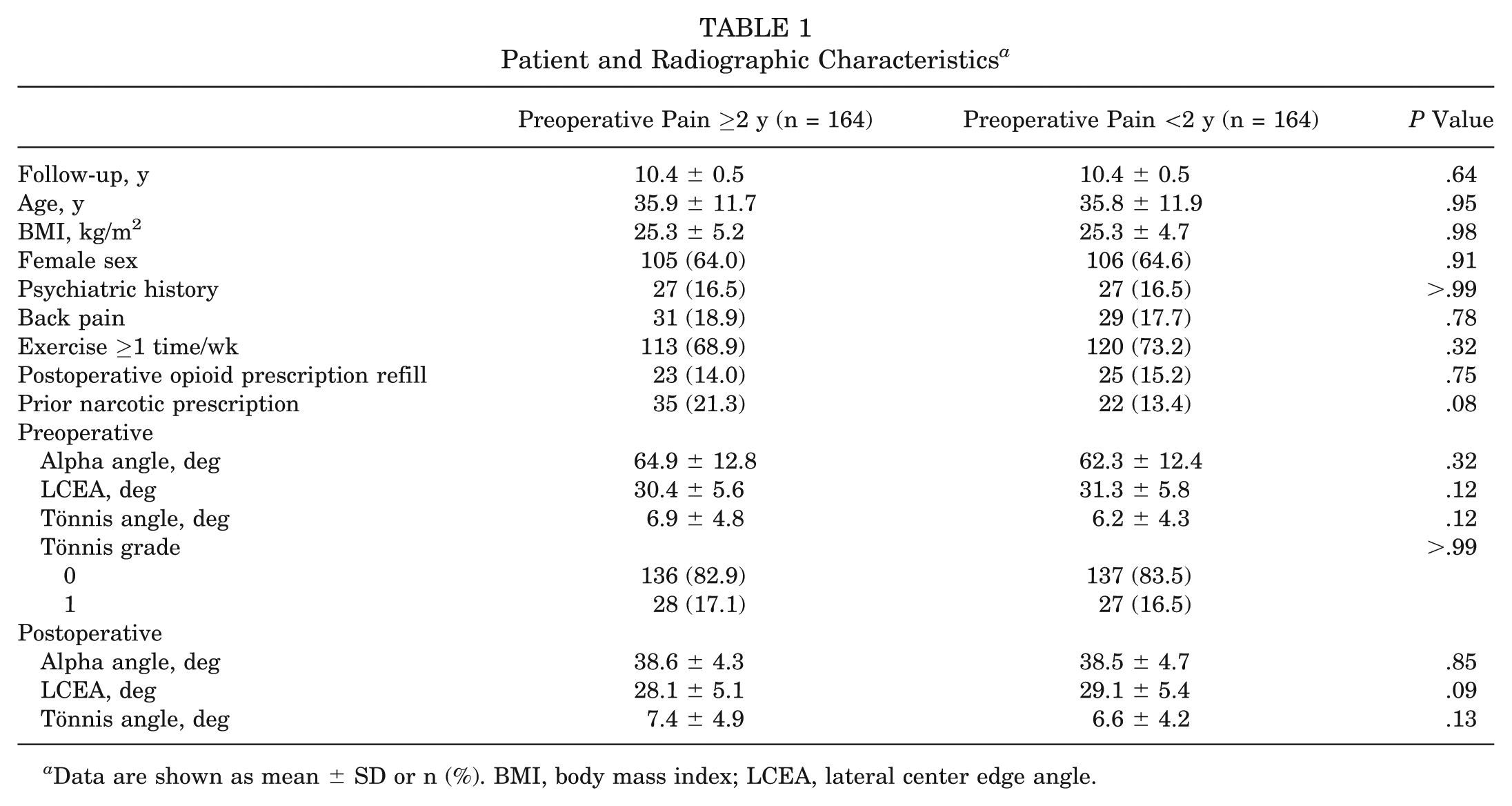
Data are shown as mean ± SD or n (%). BMI, body mass index; LCEA, lateral center edge angle.
The prolonged pain group and short pain group had similar high incidences of acetabular (86.6% vs 84.1%, respectively; P = .64) and femoral head (96.3% vs 95.7%, respectively; P > .99) cartilage grades 0 to 2. Almost all patients underwent femoroplasty (P > .99), labral repair (P = .57), capsular plication (P > .99), and acetabular rim trimming (P = .72), with no differences seen between groups (Table 2).
Intraoperative Findings and Procedures Performed a
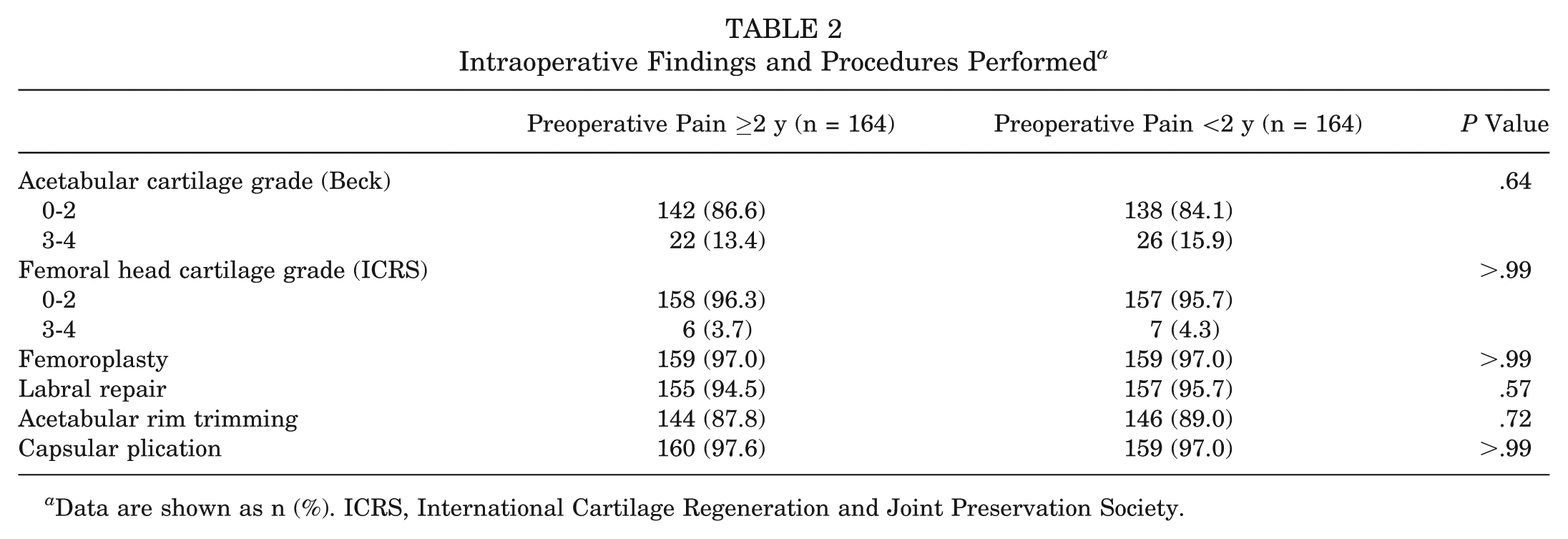
Data are shown as n (%). ICRS, International Cartilage Regeneration and Joint Preservation Society.
Patient-Reported Outcomes
No differences were seen between groups preoperatively for any PRO measure (P≥ .15) (Figure 2). This was also true for patients at 2-year follow-up (P≥ .05). At 10 years, the prolonged pain group had worse mHHS (75.4 ± 17.1 vs 79.9 ± 14.7, respectively; P = .027), VAS pain (26.3 ± 26.4 vs 16.7 ± 21.8, respectively; P = .002), and VAS satisfaction (81.4 ± 26.8 vs 91.3 ± 18.6, respectively; P = .002) scores than the short pain group. The prolonged pain group also had a worse magnitude of improvement from preoperatively to 10-year follow-up on the HOS-SS (27.9 ± 30.1 vs 37.6 ± 29.5, respectively; P = .024) and VAS pain (−43.5 ± 30.9 vs −52.2 ± 28.7, respectively; P = .032) (Table 3).
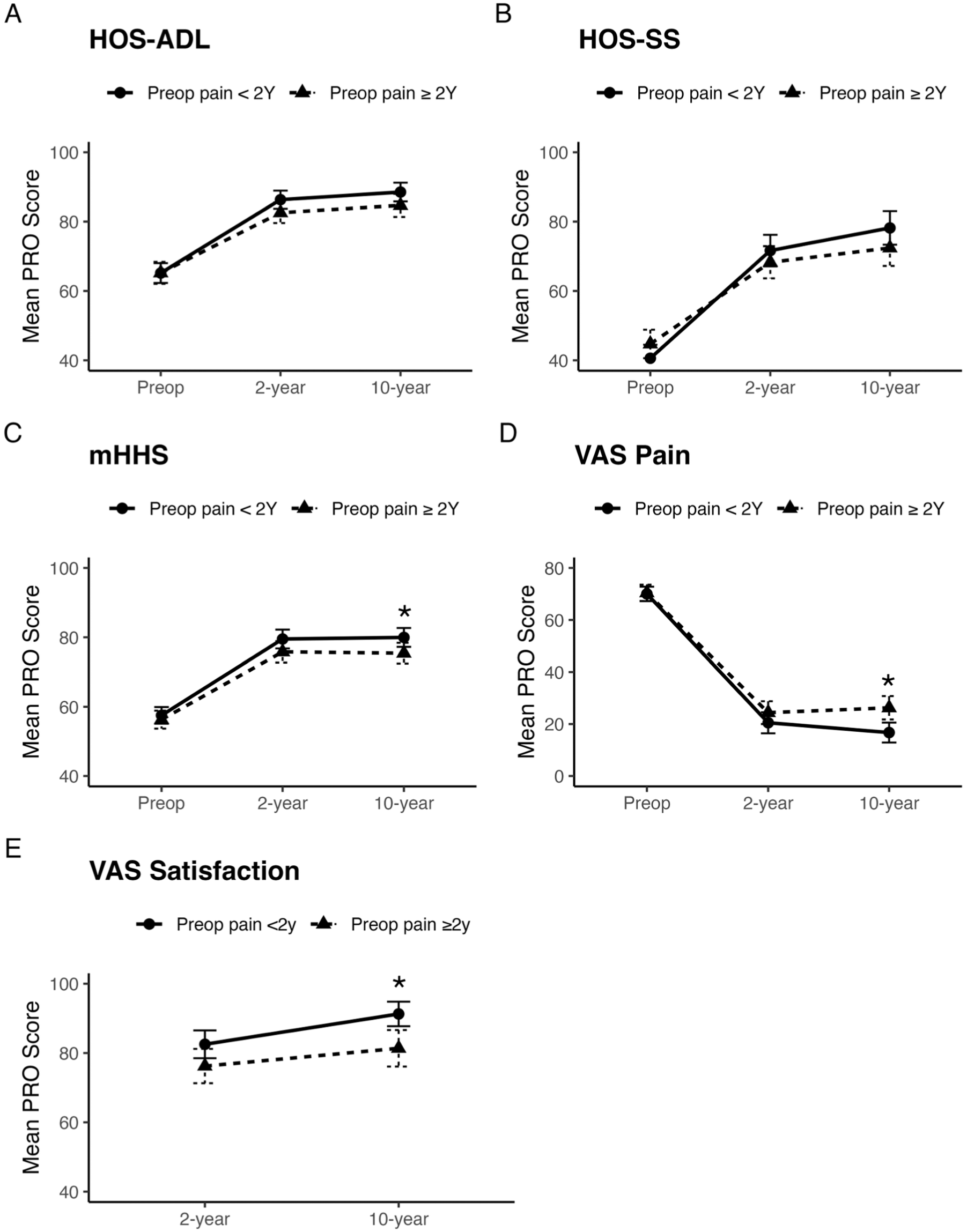
Patient-reported outcome scores preoperatively and at 2- and 10-year follow-up. Asterisk (*) denotes statistical significance at P < .05 at that time point. (A) Hip Outcome Score–Activities of Daily Living (HOS-ADL). (B) Hip Outcome Score–Sports Subscale (HOS-SS). (C) Modified Harris Hip Score (mHHS). (D) Visual analog scale for pain (VAS Pain). (E) Visual analog scale for satisfaction (VAS Satisfaction).
Patient-Reported Outcome Scores a
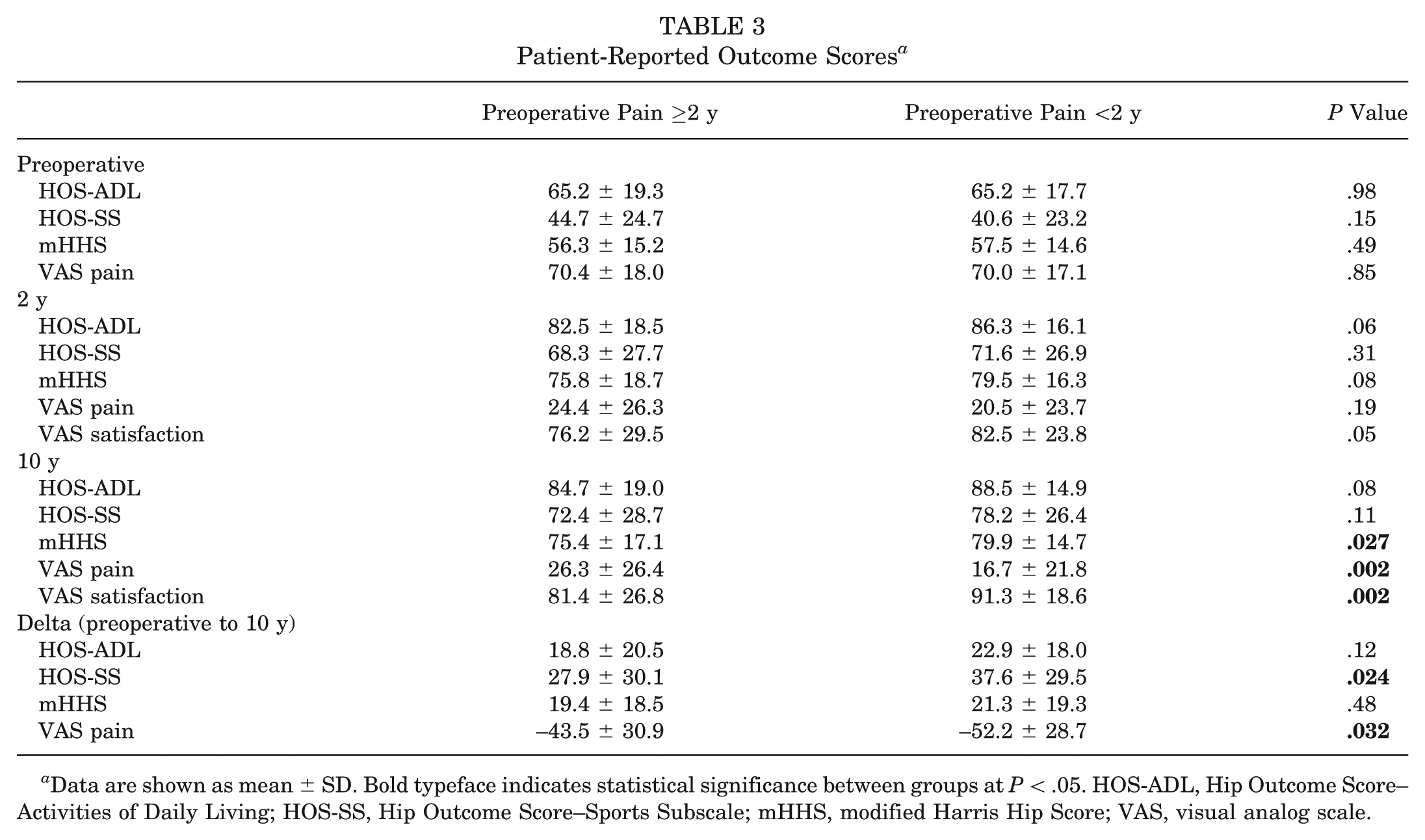
Data are shown as mean ± SD. Bold typeface indicates statistical significance between groups at P < .05. HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sports Subscale; mHHS, modified Harris Hip Score; VAS, visual analog scale.
Clinically Significant Outcomes
In terms of achieving CSOs, patients in both groups had similar MCID achievement rates for the mHHS, VAS pain, and ≥1 PRO measure at 10-year follow-up (Table 4). The prolonged pain group had lower achievement rates for the HOS-ADL (66.1% vs 79.8%, respectively; P = .024) and HOS-SS (66.7% vs 79.8%, respectively; P = .039) than the short pain group. For PASS achievement, the 2 groups had similar rates for the HOS-ADL, HOS-SS, and mHHS. The prolonged pain group had lower achievement rates of the PASS for the VAS pain (59.0% vs 75.6%, respectively; P = .006) and at least 1 PRO measure (79.2% vs 89.0%, respectively; P = .041).
Achievement of MCID and PASS a
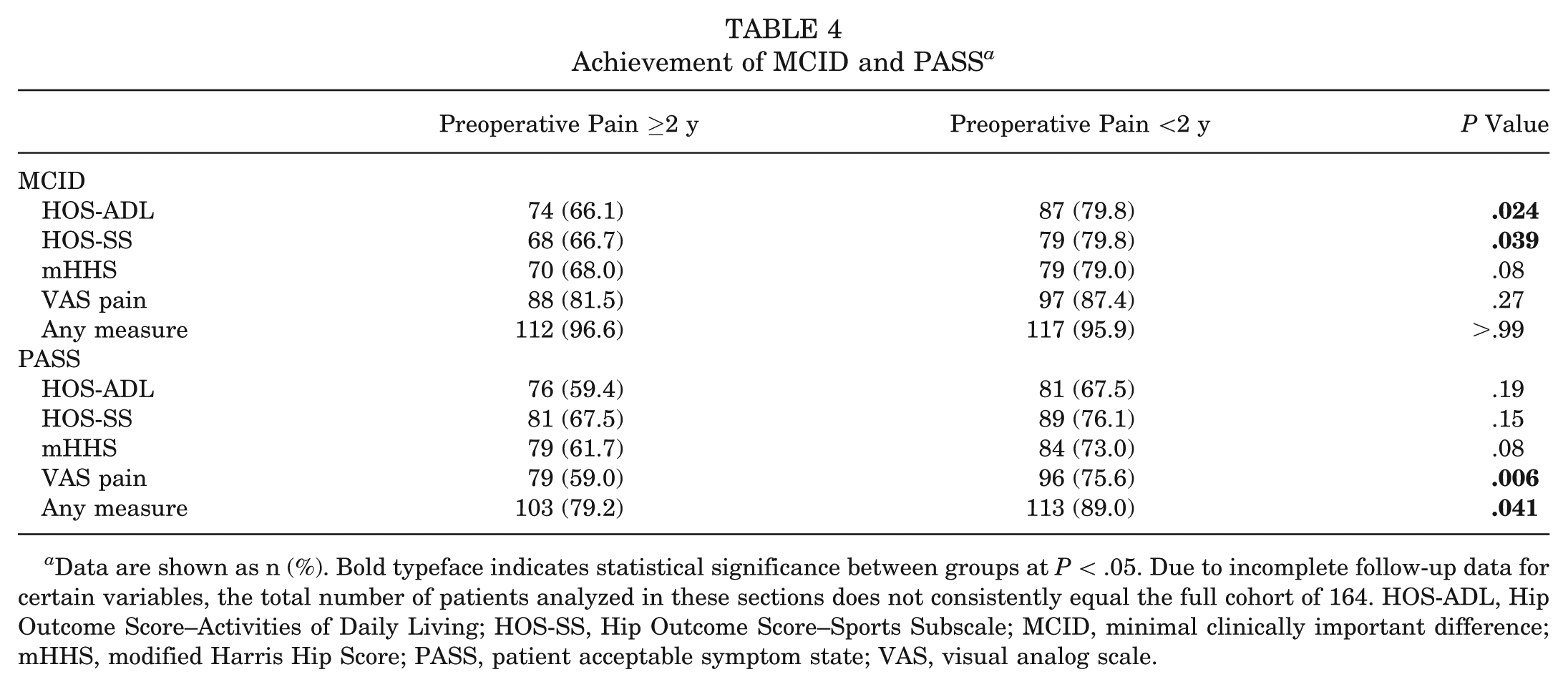
Data are shown as n (%). Bold typeface indicates statistical significance between groups at P < .05. Due to incomplete follow-up data for certain variables, the total number of patients analyzed in these sections does not consistently equal the full cohort of 164. HOS-ADL, Hip Outcome Score–Activities of Daily Living; HOS-SS, Hip Outcome Score–Sports Subscale; MCID, minimal clinically important difference; mHHS, modified Harris Hip Score; PASS, patient acceptable symptom state; VAS, visual analog scale.
Reoperations
The prolonged pain group demonstrated 89.0% reoperation-free survivorship at 10 years compared to 82.3% reoperation-free survivorship in the short pain group (Figure 3). For THA, 6.1% of the prolonged pain group converted by 10 years compared to 10.4% of the short pain group (P = .23). Additionally, 4.9% of the prolonged pain group underwent revision hip arthroscopy compared to 7.3% in the short pain group (P = .49) (Table 5).
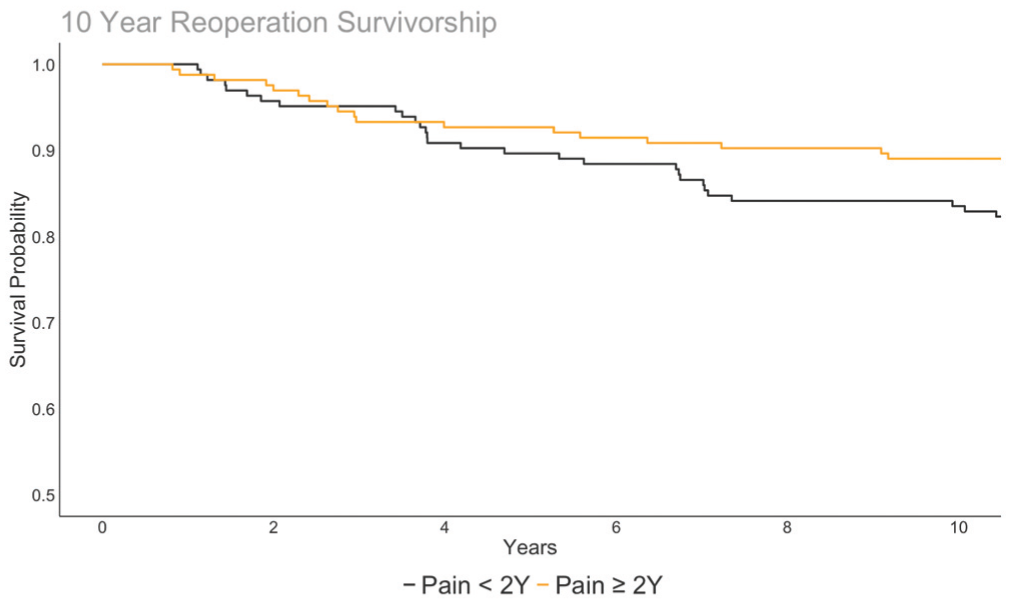
Kaplan-Meier survivorship analysis comparing prolonged and short pain groups undergoing reoperations, including revision hip arthroscopy or conversion to total hip arthroplasty. The prolonged pain group (orange line) demonstrated similar reoperation-free survivorship at long-term follow-up compared to the short pain group (black line) (P = 0.11).
Reoperations a
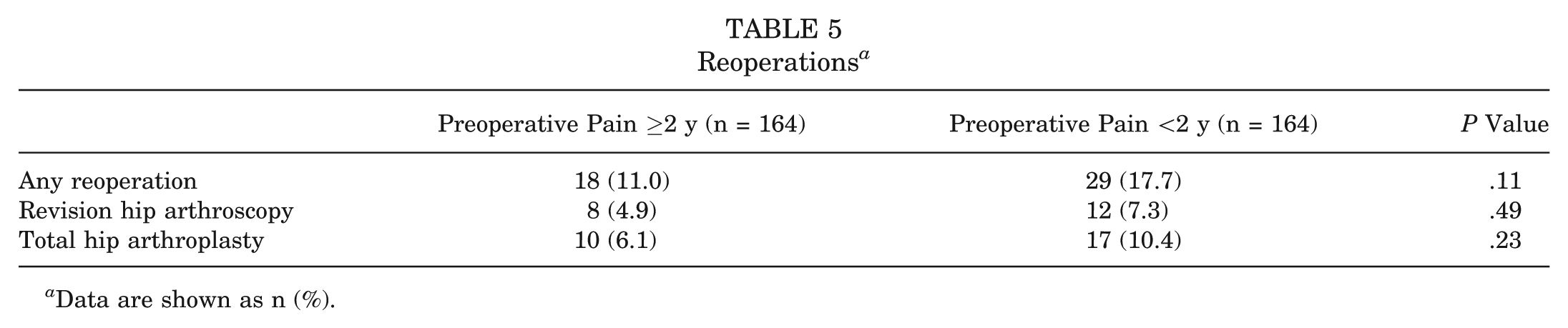
Data are shown as n (%).
Discussion
The main findings of this study were that patients with prolonged preoperative pain demonstrated similar PRO scores preoperatively and at 2 years but worse mHHS, VAS pain, and VAS satisfaction scores at 10 years after primary hip arthroscopy compared to patients with short preoperative pain. In addition, the improvements in HOS-SS and VAS pain scores were greater in patients with a short preoperative pain duration. There were significantly lower achievement rates of the MCID for the HOS-ADL and HOS-SS as well as the PASS for the VAS pain and at least 1 PRO measure in patients with prolonged preoperative pain symptoms. There were no differences in reoperation rates. These results indicate that while there are significant sustained improvements in PROs and no differences in rates of revision surgery or THA, there may be inferior outcomes at long-term follow-up in patients who experience pain symptoms ≥2 years before their primary hip arthroscopy.
There have been few prior studies in hip arthroscopy literature investigating the relationship between preoperative pain duration and postoperative outcomes. Basques et al 3 demonstrated in a retrospective cohort study of 624 patients that those with preoperative symptoms ≥2 years had significantly lower HOS-ADL scores, lower HOS-SS scores, and higher VAS pain scores at 2-year follow-up on multivariable regression analysis. In their study, at short-term follow-up, their cohort of patients with prolonged preoperative pain had higher rates of revision arthroscopy with a relative risk of 10.1, whereas when followed out to 10 years, our cohort demonstrated no differences in the reoperation rate. When examining midterm outcomes, Kunze et al 24 demonstrated in a cohort of 310 patients with a minimum 5-year follow-up that preoperative pain ≥2 years was an independent predictor of worse HOS-ADL, HOS-SS, mHHS, and VAS pain scores. Their study additionally demonstrated a lower likelihood of achieving the MCID, PASS, and substantial clinical benefit across all PRO measures, except the PASS for the HOS-ADL. When compiling recent literature, in a systematic review of 6 studies with 3298 hips with a follow-up of 2 and 5 years, Kim et al 23 demonstrated similar findings of inferior PROs in patients with a prolonged preoperative pain duration. The current study is the first to examine long-term PROs after primary hip arthroscopy in patients with a preoperative pain duration ≥2 years and <2 years. While the current study's cohort did not demonstrate differences in outcomes at short-term follow-up, there were significant differences in function, subjective pain, and satisfaction at long-term follow-up.
Preoperative pain is often associated with opioid use, which can also affect hip arthroscopy outcomes. Anciano Granadillo et al 1 and Cunningham et al 11 described preoperative opioid use in hip arthroscopy as a significant predictor of postoperative opioid use regarding chronicity and dosage, with preoperative opioid users demonstrating significantly worse outcomes. Zusmanovich et al 40 demonstrated, in a small retrospective study of 34 patients with and without preoperative opioid use, significantly greater VAS pain scores and worse mHHS scores at 1- and 2-year follow-up in the opioid group. Rocca et al 35 demonstrated similar findings in a retrospective review of 123 patients, showing that 17% of those who used opioids preoperatively had significantly worse postoperative PROMIS scores in several domains. In the present cohort, patients did not differ with regard to preoperative narcotic use or postoperative opioid refills, suggesting that a prolonged symptom duration may impact outcomes independent of narcotic/opioid use.
Many patients with FAIS have nonspecific complaints and atypical histories that may delay their diagnosis and referral to hip surgeons and, once evaluated, often undergo various courses of nonoperative management. This common preoperative course often leads to a prolonged period of symptoms before eventual primary hip arthroscopy. The importance of this study lies both in preoperative patient communication and surgeon reassurance; patients can be counseled that despite having lived with pain for ≥2 years, they can expect significant long-term improvements in multiple domains, with no difference in reoperation rates, compared to patients with a shorter pain duration, despite lower PRO scores and achievement rates of CSOs.
Limitations
There are several limitations to the current study, several of which are inherent to a retrospective review of a single-surgeon database. External validity is always in question with a single-surgeon database, as the results from a single provider's patients may not apply across various hip practices. There is also the potential for additional confounders, despite controlling for age, sex, BMI, and Tönnis grade. Surgeon indications may play a role in selection bias, as patients with a longer preoperative pain duration may have a protracted course due to concomitant abnormalities that make them less “ideal” surgical candidates for early hip arthroscopy. However, the groups in our study had no differences in psychiatric history, low back pain, narcotic use, or preoperative activity levels. There were additionally no differences in intraoperative articular chondral defects between groups. Finally, patients may be prone to recall bias related to symptom duration, as they may have difficulty accurately recalling the precise onset of symptoms, particularly when applying a fixed threshold of 2 years.
Conclusion
Patients with prolonged preoperative symptoms ≥2 years before primary hip arthroscopy for FAIS demonstrated significantly worse mHHS, VAS pain, and VAS satisfaction scores at long-term follow-up, with lower achievement rates of the MCID and PASS for several PRO measures. There were no differences in reoperation rates between patients with a preoperative pain duration ≥2 years or <2 years.