
Abstract
Background:
Significant variation has been reported within published postoperative rehabilitation protocols after proximal hamstring tendon repair undertaken for acute tendon avulsion injuries, particularly with respect to bracing and the restriction and progression of weightbearing.
Purpose:
To investigate clinical outcomes, the recovery of strength and functional symmetry, and complications and reinjuries in patients undergoing proximal hamstring repair for acute tendon avulsions involving at least 2 tendons, following a conservative (CR) or accelerated (AR) rehabilitation pathway.
Study Design:
Randomized controlled trial; Level of evidence, 1.
Methods:
This prospective RCT allocated patients undergoing proximal hamstring tendon repair to the CR pathway (n = 30), which included 6 weeks of knee bracing and restricted weightbearing, or the AR pathway (n = 27), which did not require knee bracing and allowed full weightbearing as tolerated. All patients underwent repair due to an acute avulsion injury involving at least 2 tendons and due to a specific traumatic incident. Patients were assessed presurgery and at 3-, 6-, 12-, and 24-month postoperatively using patient-reported outcome measures (PROMs), peak isokinetic knee flexor (PKFT) and extensor (PKET) torque, and the single-leg horizontal hop test for distance (SLHD). Normalized outcomes and limb symmetry indices (LSIs) were presented for objective measures. Complications and reinjuries were reported. The primary study outcome was the 6-month postoperative LSI for PKFT.
Results:
While the AR group reported a significantly better 12-item Short-Form Health Survey physical score at 3 months (P = .039) and lower severity of hamstring pain at 3 months (P = .034) and 12 months (P = .010), no other group-based differences were observed. The normalized PKFT (P < .001), PKET (P < .001), and SLHD (P < .001) improved over time, as did the PKFT (P < .001) and SLHD (P < .001) LSIs. No group differences (P > .05) were observed for hop or strength outcomes. Four patients were reinjured over the 24 months, including 2 CR patients (at 6 weeks and 3 months) and 2 AR patients (at 10 and 12 months), with an overall rerupture rate of 7%.
Conclusion:
After proximal hamstring repair undertaken due to an acute avulsion injury involving at least 2 tendons, patients demonstrated improved PROMs, a sound recovery of strength and function, and a low reinjury rate over a 2-year postoperative period. The AR pathway that did not employ bracing and permitted full weightbearing as tolerated demonstrated subjective, functional, and reinjury outcomes that were largely comparable over the 2 years. However, the study was not powered to investigate differences in reinjury risk.
Registration:
Australian New Zealand Clinical Trials Registry (ACTRN12621000913875).
Hamstring injuries are common among recreational and professional athletes, 1 and 12% of these result in rupture of the proximal tendon attachment. 11 While surgical repair may be indicated, systematic reviews have highlighted the improvement in clinical scores and strength, high patient satisfaction, and ability to return to sport (RTS) as a result of surgery.3,5,7,9,10,17 It has been reported that surgical (versus nonoperative) management of proximal hamstring tears results in superior satisfaction, perceived functional outcome, and hamstring strength symmetry, and single-limb hop capacity. 4 However, Bodendorfer et al 4 reported a 23% complication rate with surgical repair, including wound complications and peri-incisional numbness, neurological complications, deep vein thrombosis, and rerupture.
Rehabilitation protocols after proximal hamstring repair are varied. There is a lack of consensus on various components of rehabilitation, including bracing, weightbearing (WB) progression, timing to full WB, and the prescription of range of motion (ROM) and strengthening exercises, with a strong tendency toward limited weightbearing and early bracing. 14 Lightsey et al 14 assessed variability across proximal hamstring tendon repair rehabilitation protocols published in United States orthopaedic teaching programs, reporting that 40% of protocols advised immediate non-WB with crutches, 46% permitted toe-touch WB, and the mean time to full WB was >7 weeks. Furthermore, of the 71% of protocols that advocated immediate bracing, 34% braced the knee, 23% braced the hip, and 14% did not specify. Of interest, despite the cumbersome and restrictive nature of bracing, a recent systematic review demonstrated lower complication and reoperation rates, higher clinical scores and satisfaction, and a higher rate of RTS in patients who are braced (vs unbraced) after proximal hamstring repair. 21
No study has been undertaken to directly compare outcomes specifically in patients undergoing proximal hamstring repair who are then managed with accelerated versus conservative rehabilitation. The PHARRLAP (Proximal Hamstring Avulsion Rehabilitation Regimes: Longitudinal versus Accelerated Protocol) study represents the first prospective, randomized controlled trial (RCT) dedicated to investigating the outcomes of proximal hamstring repair followed by a conservative (CR, braced and restricted WB) versus accelerated (AR, unbraced and WB as tolerated) rehabilitation pathway. Recently published outcomes demonstrated early safety and efficacy of this AR protocol, with clinical outcomes similar to those at 6 months after surgery. 2 The present study presents a robust 2-year subjective and objective review of patients undergoing proximal hamstring repair, randomized to the AR or CR intervention. It was hypothesized that after proximal hamstring repair (1) improved knee flexion strength symmetry would be observed in favor of the AR (vs CR) pathway, and no differences would be observed between the 2 rehabilitation pathways in (2) single-limb functional hop or quadriceps strength symmetry, (3) patient-reported outcome measures (PROMs), or (4) complications and/or reinjury over the 2-year postoperative period.
Methods
Participants
Patients who were scheduled to undergo proximal hamstring repair within 6 weeks (42 days) of an acute avulsion injury were identified and referred for recruitment by 1 of 3 sports fellowship-trained orthopaedic surgeons (P.D., P.A., and B.R.). Using a “random number sequence generator” that was maintained by a member of the research team, patients were subsequently randomized to either an AR (no bracing and full WB as tolerated) or more traditional CR (knee bracing with a 30° of knee flexion deficit and 6 weeks of restricted WB) postoperative rehabilitation pathway. Patients were included if they were 18 to 65 years old and sustained an acute proximal hamstring tendon avulsion injury involving at least 2 tendons after an acute injury, with the injury confirmed on magnetic resonance imaging (MRI) and retraction of up to 10 cm from the ischium. The exclusion criteria included a body mass index (BMI) ≥40, unwillingness to provide written consent to participate or verbally comply with their assigned rehabilitation pathway, previous repair (revision surgery), identification of an isolated semimembranosus rupture, or if surgery could not be performed within 6 weeks of the injury. Ethics approval for this prospective RCT was granted by the University of Western Australia Human Research Ethics Committee (2021/ET000117), and the trial was conducted in accordance with the Declaration of Helsinki. The study was registered with the Australian New Zealand Clinical Trials Registry (ACTRN12621000913875).
Surgical Technique
The proximal hamstring tendon repair procedure was standardized among 3 fellowship-trained orthopaedic surgeons and has been previously described. 2 Briefly, surgery was undertaken with the patient in a prone position under a general anesthetic. Preoperative antibiotics were provided, while aseptic protocols included hair removal, prewash, and placement of a betadine-soaked gauze into the perineal area. After skin preparation and draping, the surgical field was sealed with an Ioban. A transverse skin incision was used within the gluteal fold, with subgluteal dissection down to the ischium performed with careful visualization, formal identification, neurolysis, and protection of the sciatic nerve. Tendon mobilization was undertaken to ensure adequate reduction under minimal tension. The lateral wall of the ischium was prepared, and repair was undertaken using ≥3 anchors in a double-row configuration. After repair, the surgical field was irrigated with saline, and the sciatic nerve was reinspected. The wounds were closed in layers, the skin closed with absorbable subcuticular sutures, and a waterproof dressing was applied.
Rehabilitation
The rehabilitation pathways have been previously described. 2 The AR pathway was permitted full WB as tolerated and did not wear a brace of any kind. The CR pathway was braced at the knee and restricted from the last 30° of terminal knee extension for 6 weeks, while WB was also restricted over the first 6 weeks. Some variation in the progression of exercises was permitted between groups, given the differences in WB and bracing restrictions. The rehabilitation pathways were otherwise developed based on a combination of existing published protocols and recommendations at the time of study development, along with the research team’s clinical experience, in consultation with local university and private therapy groups actively engaged in treating patients undergoing proximal hamstring repair. The relevant detailed rehabilitation overview was provided to the patient’s treating therapist, with periodic communication sought to ensure the guide was being followed.
Clinical Assessment
Several PROMs were employed preoperatively and at 3-, 6-, 12-, and 24-month after surgery. These validated tools included the Perth Hamstring Assessment Tool (PHAT), the Lower Extremity Functional Scale (LEFS), the 12-item Short-Form Health Survey (SF-12) with both physical (PCS) and mental (MCS) component subscales, the Tegner Activity Scale (TAS), and a visual analog scale (VAS) for hamstring pain frequency (VAS-F) and severity (VAS-S).
At 6, 12, and 24 months, patients completed the single-leg horizontal hop test for distance (SLHD). A verbal description and practical demonstration were provided, and, following 2 to 3 warm-up hops on each limb, 3 valid trials on each limb (alternating between the nonoperated and operated side) were collected. The best hop (m) was used for analysis. Peak isokinetic knee extensor (PKET) and flexor (PKFT) torque were measured at 90 deg/s, using an isokinetic dynamometer (Isosport International). Patients were informed that each trial would consist of 4 repetitions on the same leg: 3 low-intensity repetitions of knee extension and flexion, immediately followed by 1 maximal test effort. Each test was initiated on the nonoperated limb, then alternated between the nonoperated and operated limbs, and 3 valid sets were completed on each limb. For the hop and strength measures, patients were given as much time as required between trials to minimize fatigue. However, this was not standardized and dictated by the individual patient’s readiness to proceed. Normalized outcomes (N·m/kg) and limb symmetry indices (LSIs) were presented for strength measures, with absolute distance (m) and LSIs presented for the SLHD. All clinical reviews were conducted at a single outpatient rehabilitation facility by an experienced therapist (J.R.E.), who was blinded to group allocation.
Statistical Analysis
As previously reported, an a priori power calculation was performed for this prospective RCT using G*Power. 2 The primary outcome variable was the 6-month postoperative LSI for PKFT. For an anticipated large effect size based on a 10% improvement in the PKFT LSI due to the AR (vs CR) pathway, an estimated sample of 48 patients (24 per group) was required to detect differences at an alpha level of .05 and 80% power.
The primary method for data analysis was the intention-to-treat approach. Continuous data with baseline measures were analyzed using linear mixed models to analyze between- and within-group treatment effects at each follow-up time point (3-, 6-, 12-, and 24-month after surgery). Missing continuous data in both groups were accounted for using restricted maximum likelihood estimation in the linear mixed models. Group, time, and their interaction (group × time) variable were included as fixed effects, along with age and sex. Participants were included as a random effect to account for within-person correlation. For all other variables without baseline measures, including the PKFT, PKET, and SLHD, linear mixed models were performed. Estimated marginal means for all models were reported, and pairwise comparisons were performed to evaluate specific between-group differences and within-group changes at each time point. Analysis was performed with JASP (Version 0.18.3). All tests were 2-tailed with an alpha level set at .05.
Results
Between 2021 and 2023, a total of 65 patients were screened for participation; 57 were recruited, randomized, and underwent surgery (Figure 1). There were no differences in patient characteristics or time to surgery between the groups. In the early postoperative period, 2 patients randomized to the CR pathway developed postoperative infections that required further surgery, and 2 further patients randomized to the CR group suffered early reinjury due to a traumatic fall at 6 weeks and 3 months, respectively. A further 2 patients in the AR group suffered late reinjury at 10 and 12 months, respectively (Figure 1). Table 1 shows the patient characteristics, injury, and surgical information for the full cohort that was recruited and randomized and underwent surgery.
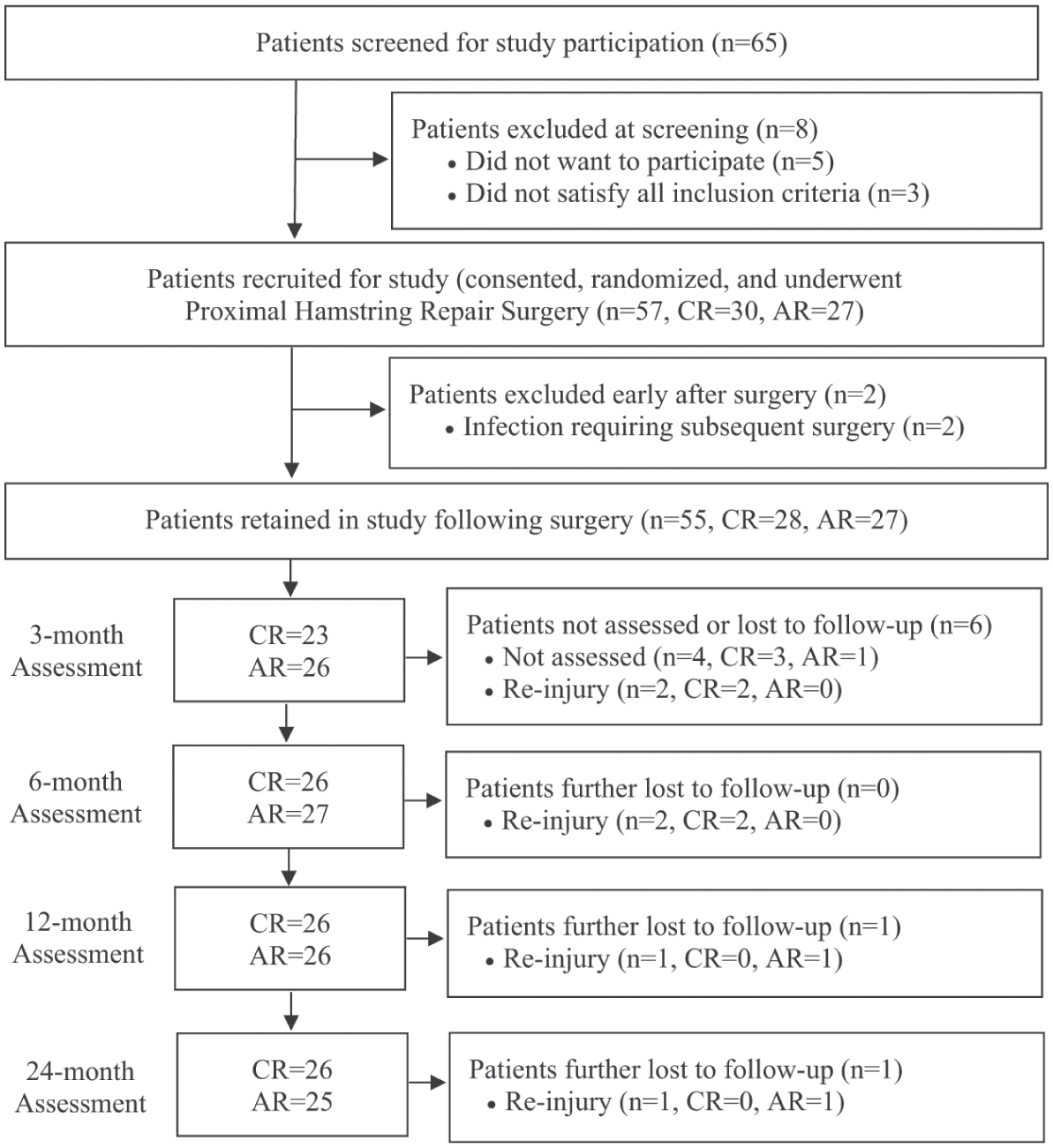
Flowchart demonstrating patient screening, recruitment, evaluation, and loss to follow-up over the 24-month postoperative period, in patients randomized to the accelerated (AR) or conservative (CR) rehabilitation pathways.
Patient, Injury, and Surgery Characteristics of Patients Randomized to the Accelerated or Conservative Rehabilitation Pathways a
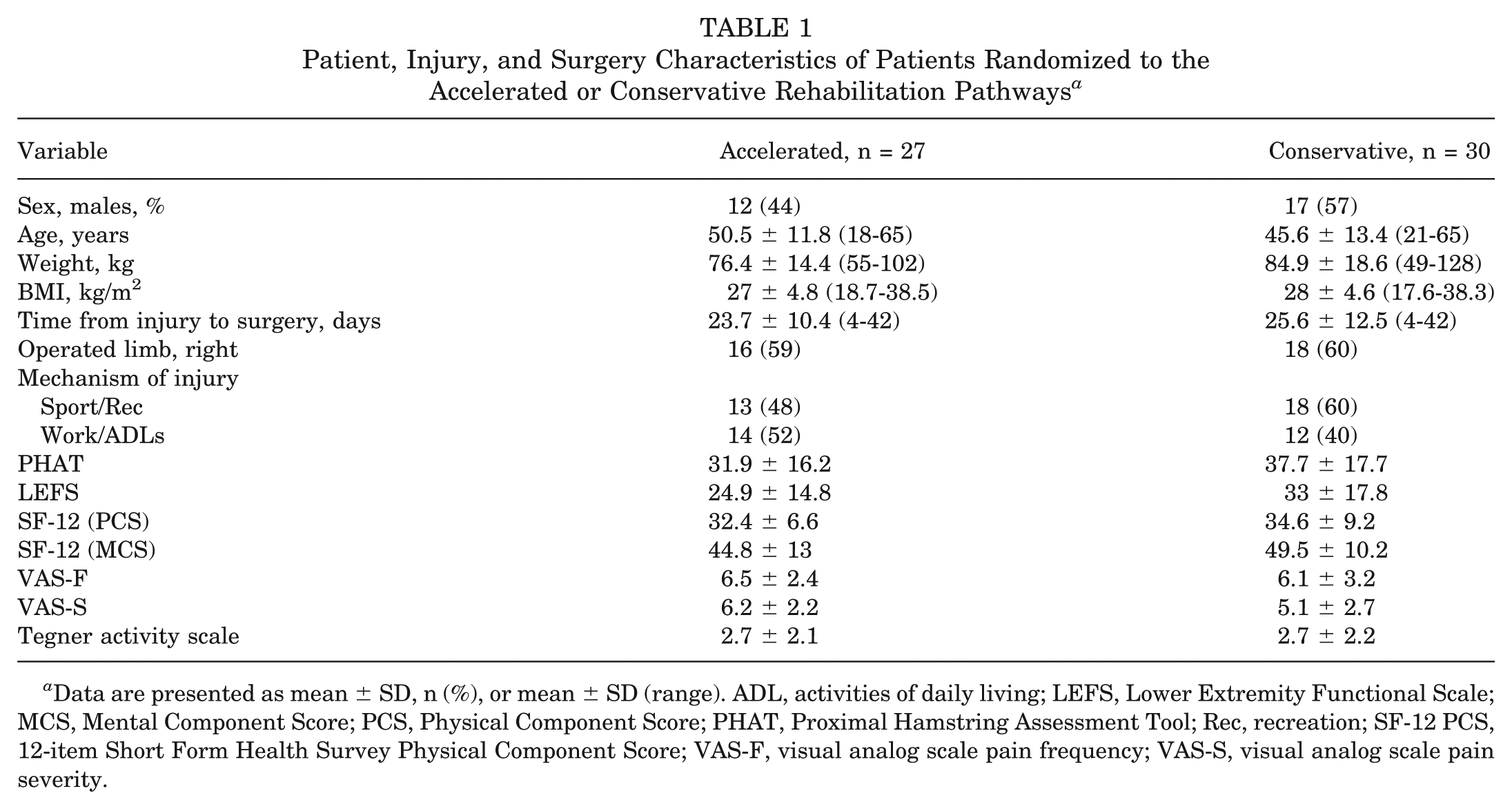
Data are presented as mean ± SD, n (%), or mean ± SD (range). ADL, activities of daily living; LEFS, Lower Extremity Functional Scale; MCS, Mental Component Score; PCS, Physical Component Score; PHAT, Proximal Hamstring Assessment Tool; Rec, recreation; SF-12 PCS, 12-item Short Form Health Survey Physical Component Score; VAS-F, visual analog scale pain frequency; VAS-S, visual analog scale pain severity.
Patient-Reported Outcome Measures
The AR group reported a significantly better SF-12 PCS at 3 months (P = .041) and a lower VAS-S at 3 months (P = .034) and 12 months (P = .011). No other differences (P > .05) were observed between groups over the 24 months (Table 2).
PROMs and Rehabilitation Group Comparisons for Estimated Marginal Means and Between-Group Differences for the Intention to Treat Analysis a
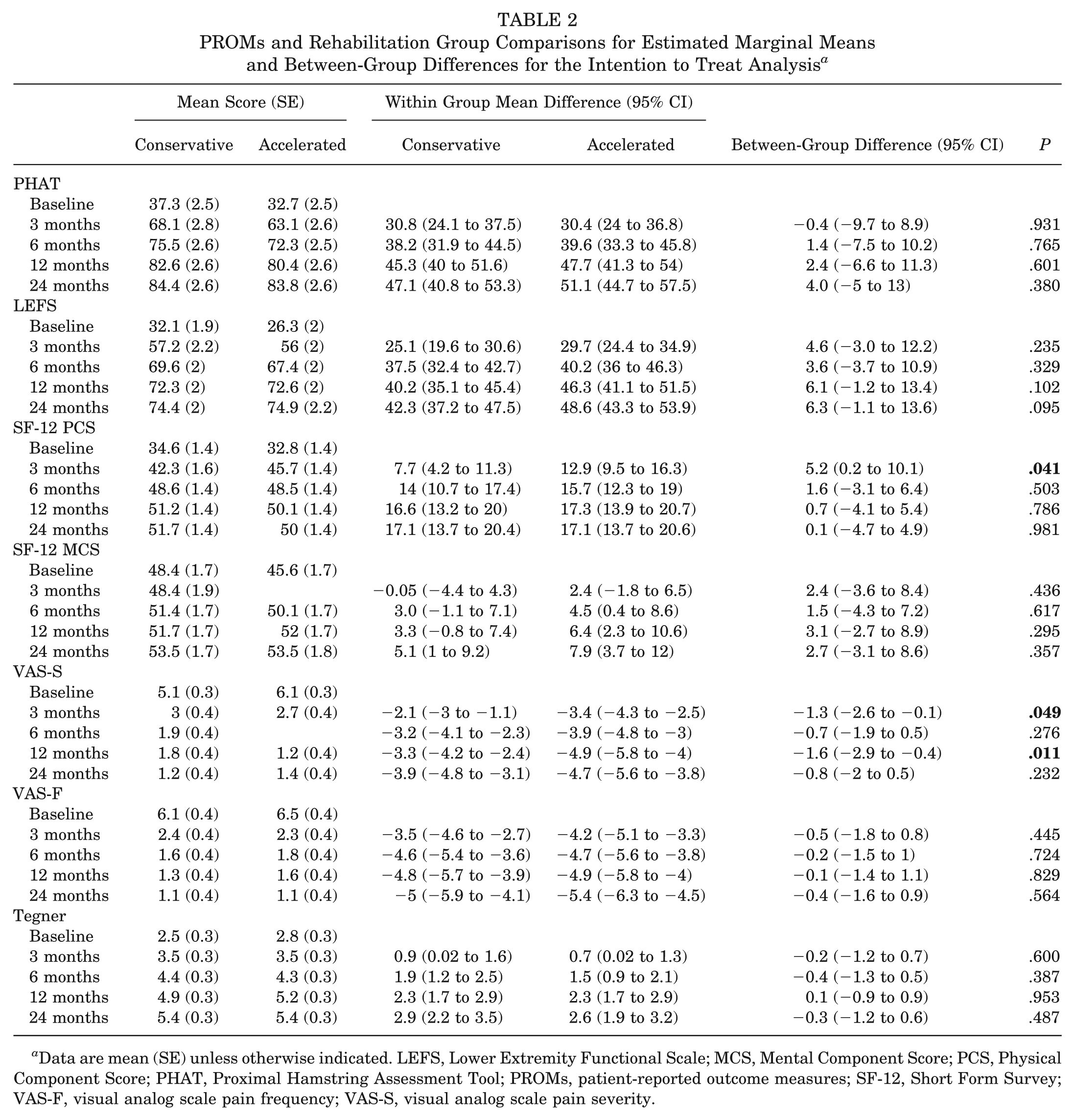
Data are mean (SE) unless otherwise indicated. LEFS, Lower Extremity Functional Scale; MCS, Mental Component Score; PCS, Physical Component Score; PHAT, Proximal Hamstring Assessment Tool; PROMs, patient-reported outcome measures; SF-12, Short Form Survey; VAS-F, visual analog scale pain frequency; VAS-S, visual analog scale pain severity.
Objective Measures
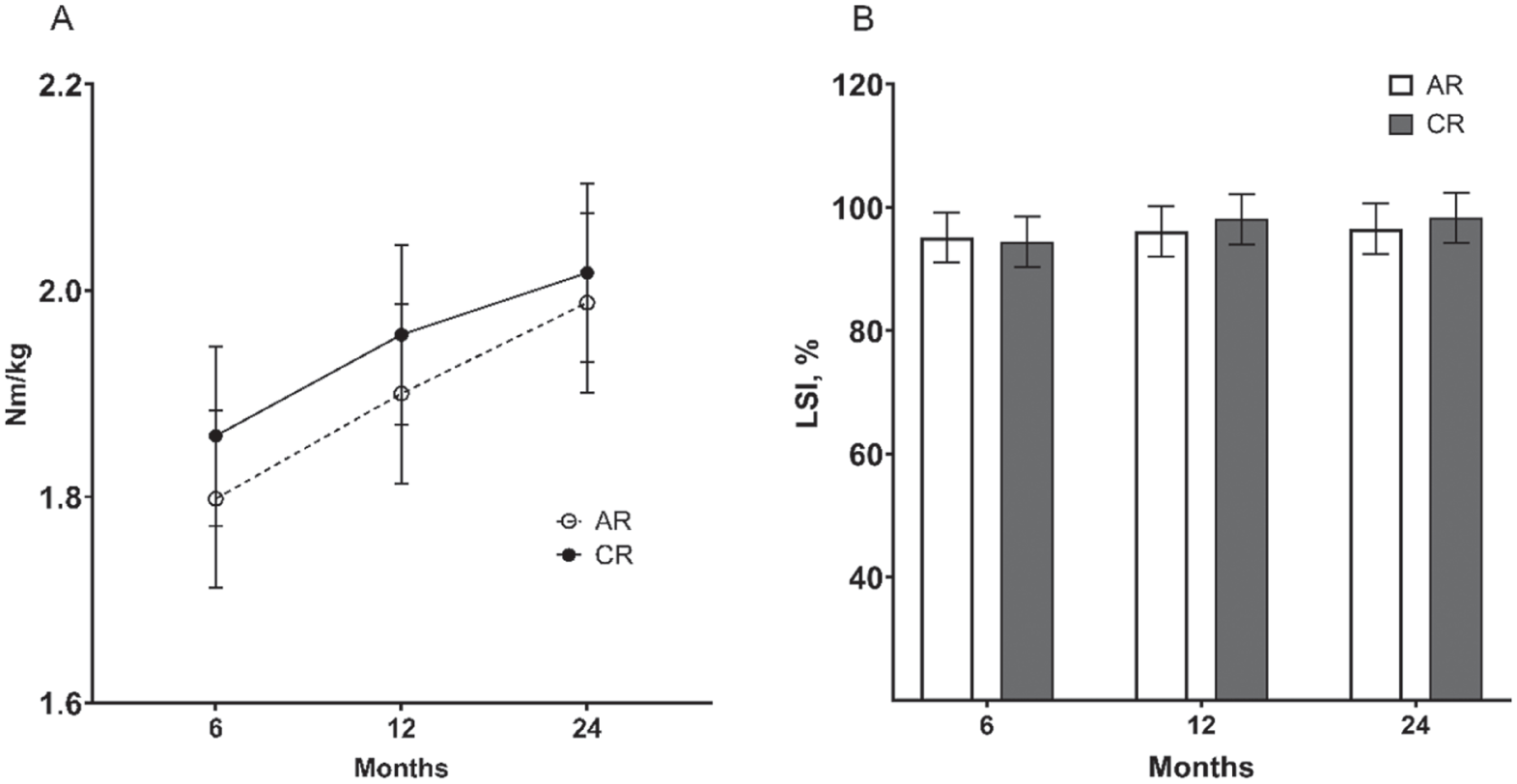
An improvement over the postoperative period was observed for the normalized (N·m/kg) PKFT (P < .001) and PKFT LSI (P < .001), although no group differences (P > .05) were observed (Figure 2). Estimated marginal means (95% CIs) for the PKFT LSI at 6 (AR, 0.82 [95% CI, 0.78-0.86], CR 0.82 [95% CI, 0.78-0.86]; P = .993), 12 (AR, 0.86 [95% CI, 0.83-0.90], CR, 0.90 [95% CI, 0.86-0.94]; P = .267) and 24 (AR, 0.93 [95% CI, 0.89-0.97], CR, 0.92 [95% CI, 0.88-0.96]; P = .620) months are shown in Figure 2. The normalized (N·m/kg) PKET improved over time (P < .001), although no change was observed over time in the PKET LSI (P = .094), with no group differences (P > .05) observed for either (Figure 3). The mean PKET LSIs at 6 (AR, 0.95 [95% CI, 0.91-0.99], CR, 0.94 [95% CI, 0.90- 0.99]; P = .808), 12 (AR, 0.96 [95% CI, 0.92-1], CR, 0.98 [95% CI, 0.94-1.02]; P = .508) and 24 (AR, 0.97 [95% CI, 0.93-1], CR, 0.98 [95% CI, 0.94-1.02]; P = .554) months are shown in Figure 3. The SLHD (P < .001) and SLHD LSI (P < .001) both improved over time, although no group differences (P > .05) were observed (Figure 4). The mean SLHD LSIs at 6 (AR, 0.94 [95% CI, 0.90- 0.97], CR, 0.94 [95% CI, 0.91-0.97]; P = .902), 12 (AR, 0.98 [95% CI, 0.95-1.01], CR, 1 [95% CI, 0.97-1.03]; P = .691) and 24 (AR, 1 [95% CI, 0.97-1.03], CR, 0.99 [95% CI, 0.96-1.02]; P = .541) months are shown in Figure 4.
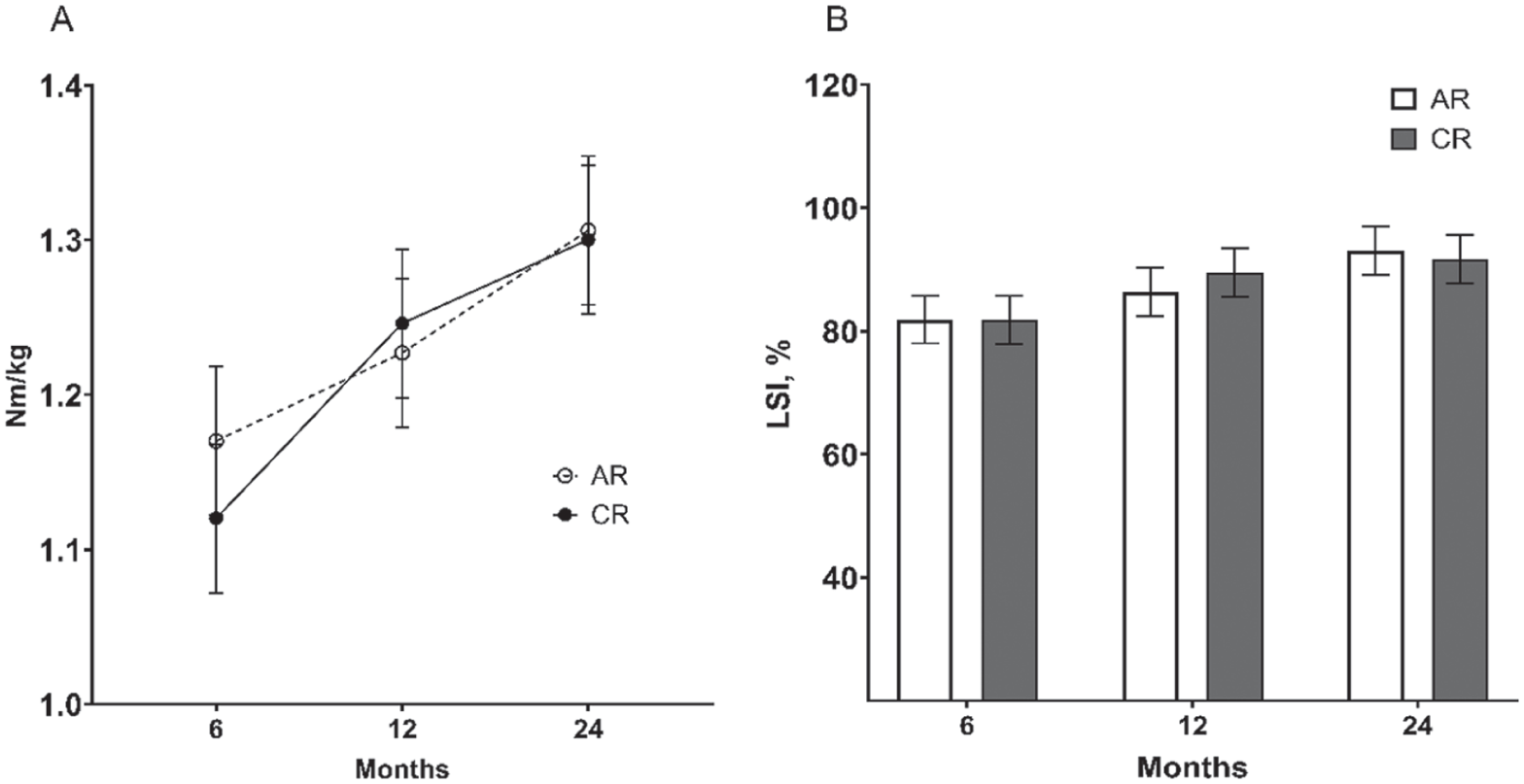
The postoperative progression of (A) PKFT normalized to body weight (N·m/kg), and (B) PKFT LSI (%) for patients undergoing the AR and CR rehabilitation pathways, with no differences observed between groups. Shown are means (SD). AR, accelerated; CR, conservative; LSI, limb symmetry index; PKFT, peak knee flexor torque.
The postoperative progression of (A) PKET (normalized to body weight, N·m/kg) and (B) PKET LSI (%) in patients undergoing the AR and CR rehabilitation pathways, with no differences observed between groups. Shown are means (SD). AR, accelerated; CR, conservative; LSI, limb symmetry index; PKET, peak knee extensor torque.
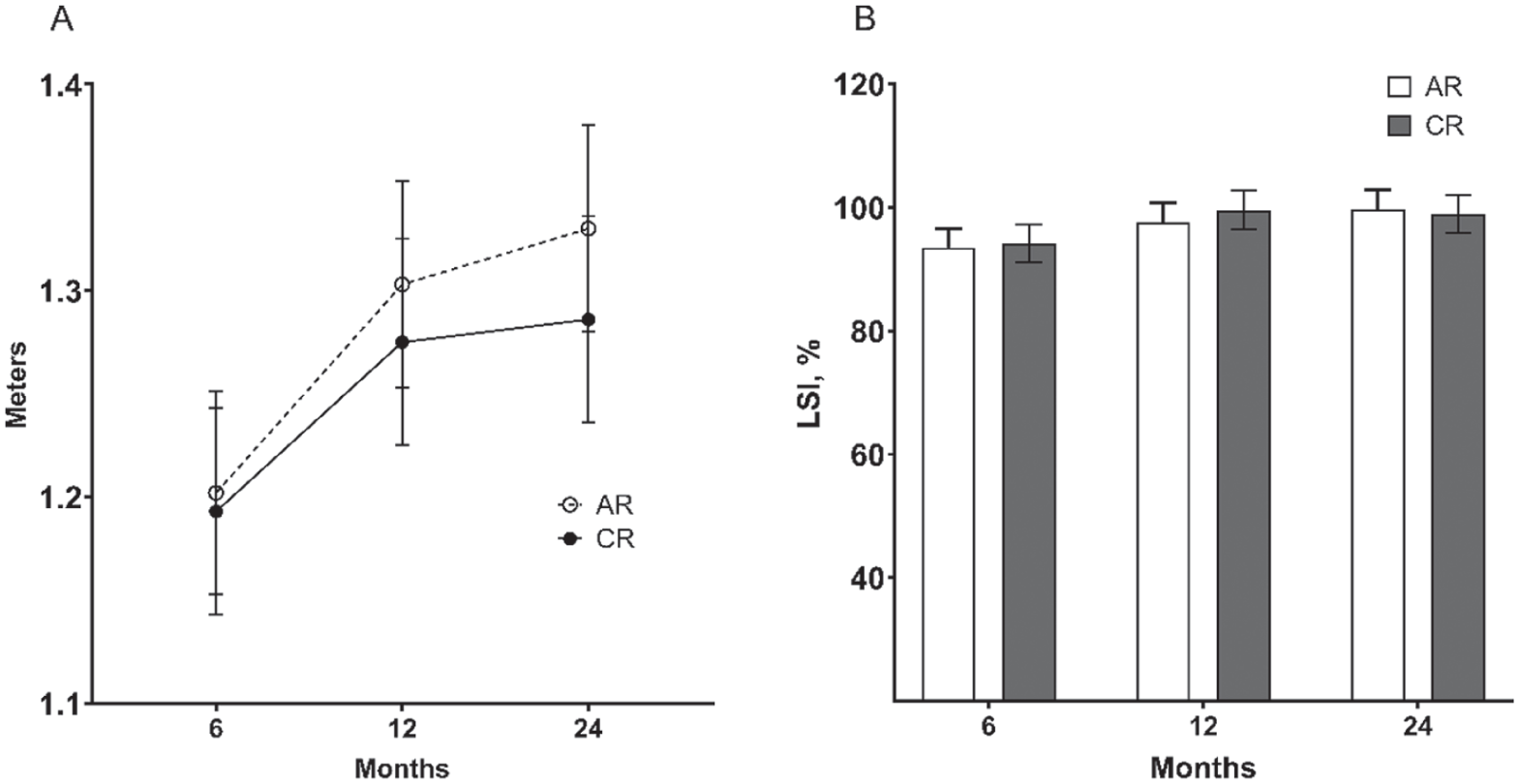
The postoperative progression of the (A) SLHD (m) and (B) the SLHD LSI (%) for patients undergoing the AR and CR rehabilitation pathways, with no differences observed between groups. Shown are means (SD). AR, accelerated; CR, conservative; LSI, limb symmetry index; SLHD, single hop for distance.
Complications, Adverse Events, and Reinjuries
Surgical or early postoperative adverse events have been previously reported. 2 Two patients, both randomized to the CR pathway, developed deep infections that required further surgery involving washout and debridement. Furthermore, a third patient randomized to the AR pathway underwent a wound washout for a superficial infection, although they were retained in the study. Two patients randomized to the CR group suffered a rerupture due to a traumatic fall at 6 weeks and 3 months, respectively. A further 2 patients randomized to the AR group suffered a rerupture at 10 and 12 months, respectively, both due to traumatic events. All reruptures subsequently underwent revision surgery. An overall rerupture rate of 7% was observed at 2 years in the present study.
Discussion
The main finding of this prospective RCT was that there were no apparent detrimental effects associated with an AR protocol after proximal hamstring repair that included full
WB as tolerated and no bracing. While the AR group showed improved early PROMS, as measured by the SF-12 at 3 months, along with improved pain scores through 12 months, subjective, functional, and reinjury outcomes were largely comparable over the 2 years. However, the study was not powered to investigate differences in reinjury risk.
The hypothesized accelerated recovery of hamstring strength symmetry in the AR group in the present study was attributable to reduced mobility restriction and earlier initiation of the WB pathway. However, no differences were observed in PKFT recovery between the AR and CR groups, which did not support the first study hypothesis. The mean hamstring strength LSIs in the present study ranged from 82% to 93% in the AR group and 82% to 92% in the CR group across the 3 postoperative assessment time points. A systematic review investigating outcomes after proximal hamstring repair in 2015 reported a mean hamstring strength symmetry ranging 17 from 78% to 101%, with a more recent systematic review and meta-analysis in 2022 reporting 10 a mean hamstring strength LSI of 87%. Fouasson-Chailloux et al 8 published a review of strength assessment methods after proximal hamstring repair, reporting 15% strength deficits observed >12 months after surgery. Although it was suggested that comparing studies was difficult because the methods used to assess strength varied (isometric, pneumatic, isotonic, and isokinetic). There were also no group differences in other objective measures, including quadriceps strength and functional hop symmetry, consistent with the second hypothesis. These outcomes reflect single-limb functional capacity, although it is less commonly assessed and/or reported, with many studies being retrospective or reporting only subjective measures of pain, function, satisfaction, and return-to-sport ability.
Early group differences were observed in some PROMs, including a better SF-12 PCS at 3 months and a lower VAS-S at both 3 and 12 months in the AR group, indicating a more satisfied cohort of AR patients. There were no other differences in PROMs, largely supporting the third hypothesis. Comparison with other studies is difficult given the array of PROMs that have been reported in patients undergoing proximal hamstring repair including the PHAT, 20 LEFS,13,19 and SF-12 19 as employed in the present study, as well as the Harris Hip Score (HHS) 18 or modified HHS, 16 Hip Outcome Score, 7 12-item International Hip Outcome Tool, 7 and Single Assessment Numerical Evaluation,13,19 as well as the TAS16,18,19 or Marx 13 to report on activity level. Of interest, relatively few studies (and certainly prospective studies) have employed the PHAT and LEFS as employed in the present study, despite a recent systematic review of outcome measures employed after proximal hamstring repair recommending an increased commitment to the use of PROMs such as the LEFS and PHAT, as well as RTS and isokinetic strength testing. 15 A sound 2-year mean TAS was reported across patients in both groups, similar to other studies, although some reported at varied postoperative time points.16,18 While RTS was not specifically assessed in the present study, due to the nature of the heterogeneous community-level cohort recruited, reviews have reported return-to-sport rates 10 of 84.5% and 5 87%. Of relevance to the present study, Wyatt et al 21 published a systematic review of bracing after proximal hamstring repair and reported a higher rate of RTS in braced (88.4%) versus nonbraced (82.7%) patients, which was not necessarily reflected in the group-based TAS comparisons in the present study.
While 2 deep infections and 1 superficial infection requiring wound washout were observed, no other significant complications were noted. Importantly, and in support of the fourth hypothesis, there were no group differences in complications or reinjury, nor were there detrimental effects or an increased risk of reinjury associated with the AR pathway. Four reinjuries were observed over the 2-year follow-up period, including 2 in the CR group within the first 3 months, and 2 in the AR group at 10 and 12 months (with no further reinjuries after the 12-month timepoint). However, despite the 2 early reinjuries in the CR group resulting from falls and the 2 late reinjuries in the AR group resulting from subsequent traumatic insults, the study was not powered to detect a difference in reinjuries. Thus, interpretation of these data should be made with caution. Varied complication and rerupture rates after proximal hamstring repair have been reported. Lawson et al 12 published a systematic review of complications after proximal hamstring repair, reporting an overall complication rate of 15.3%, with a 4.6% major complication rate (including 1.7% rate of sciatic nerve injury, 0.8% rate of venous thromboembolism, 0.8% reoperation rate, 0.8% rerupture rate, and 0.4% rate of deep infection). Other reviews have reported rerupture rates 10 of 1.2% and 17 3%, which are lower than those reported in the present study. In a systematic review of bracing after proximal hamstring repair, Wyatt et al 21 reported lower complication (10.9% braced, 12.7% nonbraced) and reoperation (0.05% braced, 3.1% nonbraced) rates in braced versus unbraced patients. It should be noted that 67% of the braced cohort underwent acute repairs, compared with 46% in the unbraced group, and that more favorable outcomes were reported in patients undergoing surgical repair for acute (vs chronic) ruptures.3,6,9,10
A study by Lightsey et al 14 reported variability across proximal hamstring tendon repair rehabilitation protocols throughout United States orthopaedic teaching programs, noting that 40% of protocols advised immediate non-WB with crutches, 46% permitted toe-touch WB, and the mean time to full WB was >7 weeks. Furthermore, among the 71% of protocols that advocated immediate bracing, 34% braced the knee, 23% braced the hip, and 14% did not specify which joint was braced. However, accelerated rehabilitation pathways have been reported after proximal hamstring repair. A retrospective study undertaken by Wong et al 19 reported outcomes at a minimum of 1 year postsurgery in 21 patients undergoing open or endoscopic proximal hamstring repair with all-suture anchors, followed by an “accelerated” rehabilitation protocol that included 6 weeks of touchdown WB in a hinged knee brace, locked in extension, for ambulation. While sound PROMs and satisfaction were reported, with 1 deep vein thrombosis and no reruptures, infections, or reoperations observed, the reported postoperative protocol appeared more conservative than the CR pathway in the present study. Leger-St-Jean et al 13 reported encouraging PROMs at a mean of 4.1 years in 34 patients who underwent proximal hamstring repair, with immediate WB as tolerated and no bracing. However, this was part of a retrospective chart review. Furthermore, of interest, formal physical therapy was not initiated until 12 weeks after surgery.
The present study presents the first prospective RCT comparing differing rehabilitation progressions after proximal hamstring repair. A robust subjective and objective review was undertaken, with no patients lost to follow-up over the 24 months (although 4 patients did not undergo functional assessments at final follow-up due to reinjury). However, some limitations are acknowledged. First, while the recruited cohort included community-level patients consistent with the treating surgeons’ standard surgical indications, the inclusion criteria (acute tears, 18-65 years, BMI <40 kg/m2) may not capture all patients presenting with symptomatic proximal hamstring tears. Second, the quality of rehabilitation can affect strength and functional recovery. The rehabilitation protocols provided to treating therapists were employed as a guide. However, further additions and variations were at the therapist’s discretion, as in standard clinical practice. Third, while the recovery of strength and function was a focus of the present study, the selected PROMs differ from those used in many other studies. However, the PROMs used in the present study, such as the PHAT and LEFS, are validated and have been recommended for use in studies investigating the outcomes of proximal hamstring repair. 15 Fourth, rerupture was largely determined by patients presenting with a recurrence (or persistence) of symptoms warranting follow-up MRI. Therefore, asymptomatic failures could not be assessed because follow-up MRI was not performed in all patients, which is consistent with the accepted standard of care. Finally, the sample was powered to detect a difference between groups in hamstring strength symmetry at 6 months postoperatively. It was not necessarily designed to detect group-based differences across the other outcome measures assessed. Importantly, despite the 2 early reinjuries in the CR group due to falls and the 2 late reinjuries in the AR group resulting from subsequent traumatic insults, the study was not powered to detect a difference in reinjury rates. While unlikely, it may be that the early mobilization pathway led to an inferior early healing response; thus, a larger study appropriately powered to investigate differences in reinjury is warranted.
Conclusion
This study presents the first prospective RCT comparing different rehabilitation progressions after proximal hamstring repair, with no loss to follow-up over the 2 years. While early PROMS outcomes favored the AR group, subjective outcomes and recovery of strength and function over the 2 years were largely comparable between the 2 groups. Finally, and most importantly, there were no detrimental or adverse effects, including reinjury risk, associated with an AR protocol after proximal hamstring repair that included full WB as tolerated and no bracing. However, the study was not powered to detect differences in the reinjury profile, and a larger study is warranted to investigate any differences in reinjury risk resulting from a rehabilitation intervention that promotes an earlier mobilization pathway. The authors recommend that a rehabilitation protocol allowing WB as tolerated without bracing be utilized for patients undergoing proximal hamstring avulsion repair, and have since incorporated this regimen as the standard of care for all patients after completion of this study.
Footnotes
Submitted March 21, 2026; accepted May 3, 2026.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Ethics approval was obtained by the University of Western Australia Human Research Ethics Committee (2021/ET000117).