
Abstract
Background:
Central acetabular osteophytes (CAOs) have been implicated in abnormal hip biomechanics. However, their relationship with microinstability in borderline developmental dysplasia of the hip (BDDH) is unclear.
Purpose/Hypothesis:
The purpose of this study is to compare radiographic parameters between BDDH hips with and without CAOs and to determine whether CAOs are associated with microinstability. It was hypothesized that CAOs would correlate with increased version abnormalities and microinstability.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
We retrospectively reviewed patients with BDDH, defined as a lateral center-edge angle of 18° to 25°, who underwent hip arthroscopy from 2020 to 2024. Patients were grouped as BDDH with CAO (cBDDH) or without CAO (nBDDH). Radiographic parameters, including anterior/posterior acetabular coverage, femoral neck version, acetabular version, and combined anteversion, were compared. Intraoperative findings of microinstability and ligamentum teres (LT) pathology were analyzed. Binary logistic regression identified predictors of CAO.
Results:
A total of 157 patients were included (cBDDH, 76; nBDDH, 81). The cBDDH group demonstrated higher rates of microinstability and LT tears, as well as increased femoral neck, acetabular, and combined anteversion. Logistic regression showed that microinstability (β = .027; P < .001), LT tear (β = .010; P = .001), and combined anteversion (β = 1.343; P = .029; R2 = 0.542) were associated with CAO.
Conclusion:
In BDDH, CAOs were strongly associated with microinstability, LT tears, and increased combined anteversion. CAO may serve as a radiographic marker of instability and early osteoarthritis in BDDHs.
Hip microinstability, defined as abnormal femoral head translation without frank dislocation, reflects a subtle imbalance between osseous containment and soft tissue restraints.10,28 It is frequently encountered in patients with borderline developmental dysplasia of the hip (BDDH), in whom acetabular coverage lies within a transitional range.21,36 In patients with BDDH, the subtle reduction in anterior and lateral coverage may render the joint vulnerable to abnormal motion under physiologic loading, placing repetitive stress on soft-tissue stabilizers and predisposing to labral tearing, ligamentum teres (LT) pathology, and progressive cartilage damage.8,9,21 Increasing evidence indicates that unrecognized microinstability may contribute to suboptimal outcomes after hip arthroscopy, particularly in BDDH.7,11,18,19 Collectively, these observations suggest that BDDH might contribute to microinstability and highlight the importance of reliable markers to better characterize this complex patient population.
The term “central acetabular osteophyte” (CAO) refers to osteophytes arising from the acetabular fossa. 32 Unlike marginal osteophytes of the acetabular rim, CAO can be difficult to identify radiographically and are often overlooked. With advances in hip arthroscopy, however, the medial cotyloid fossa can be directly visualized, and osteophytosis in this region has been reported. CAO has been detected in early osteoarthritis and has been shown to correlate with femoral foveal osteophytes, cartilage damage, and labral tears.17,32 One study suggested that CAO formation may contribute to lateral or anterosuperior migration of the femoral head, accelerating cartilage degeneration. 32 Arthroscopic acetabular notch-plasty and decompression have been performed to address CAO, with favorable short-term outcomes. 6 Nevertheless, reported favorable outcomes after CAO decompression are confounded by labral repair and femoral osteoplasty, both of which independently improve clinical outcomes. Furthermore, there are no randomized controlled trials isolating the effect of CAO decompression. Recent studies demonstrated inferior outcomes when femoroacetabular impingement coexisted with CAO.12,38 However, these inferior outcomes may reflect early osteoarthritis rather than a direct detrimental effect of CAO itself.
A recent study has shown that CAO was more prevalent in patients with BDDH. 37 Although CAO might be associated with mechanical instability, there has been no study in which researchers assessed the relationship between CAO and microinstability in symptomatic patients with BDDH. The purpose of the present study was to investigate (1) the difference in radiographic parameters between BDDH with CAO and BDDH without CAO, and (2) whether CAO was associated with microinstability in BDDH. Since CAO has also been reported in normal lateral coverage hips, it was hypothesized that CAO was associated with anterior microinstability in symptomatic patients with BDDH. In the present study, hip microinstability was diagnosed intraoperatively according to recently published international consensus criteria and was defined by either excessive hip distraction under general anesthesia or arthroscopic evidence of instability. 11
Methods
The focus of this retrospective study was the potential relationship between CAO and radiographic measurements in patients with BDDH. After approval from the institutional review board of our hospital (XHBC-2025-510), 2 senior fellows (Y.H. and Y.-z.C.) reviewed the medical records of patients with hip disorders undergoing hip arthroscopic surgeries in our hospital from January 2020 to December 2024. The inclusion criteria were patients with a lateral center-edge angle (LCEA), measured from the lateral edge of the sourcil, between 18° and 25° on anteroposterior pelvic plain radiographs, as measured using Hip2Norm software, who underwent arthroscopic surgery. 39 The exclusion criteria were advanced osteoarthritis (Tönnis grade ≥2), Legg-Calve-Perthes disease, previous hip or spine surgeries, leg length discrepancy (>5 mm on standing EOS imaging), general joint laxity (Beighton scores ≥4), and cerebral palsy. Consecutive patients who met the inclusion criteria were enrolled in the study. The presence of CAO was first assessed preoperatively and subsequently confirmed intraoperatively (Figure 1). The patients included were divided into a BDDH with CAO group (cBDDH) and a BDDH without CAO group (nBDDH). The radiographic data were collected and reviewed.
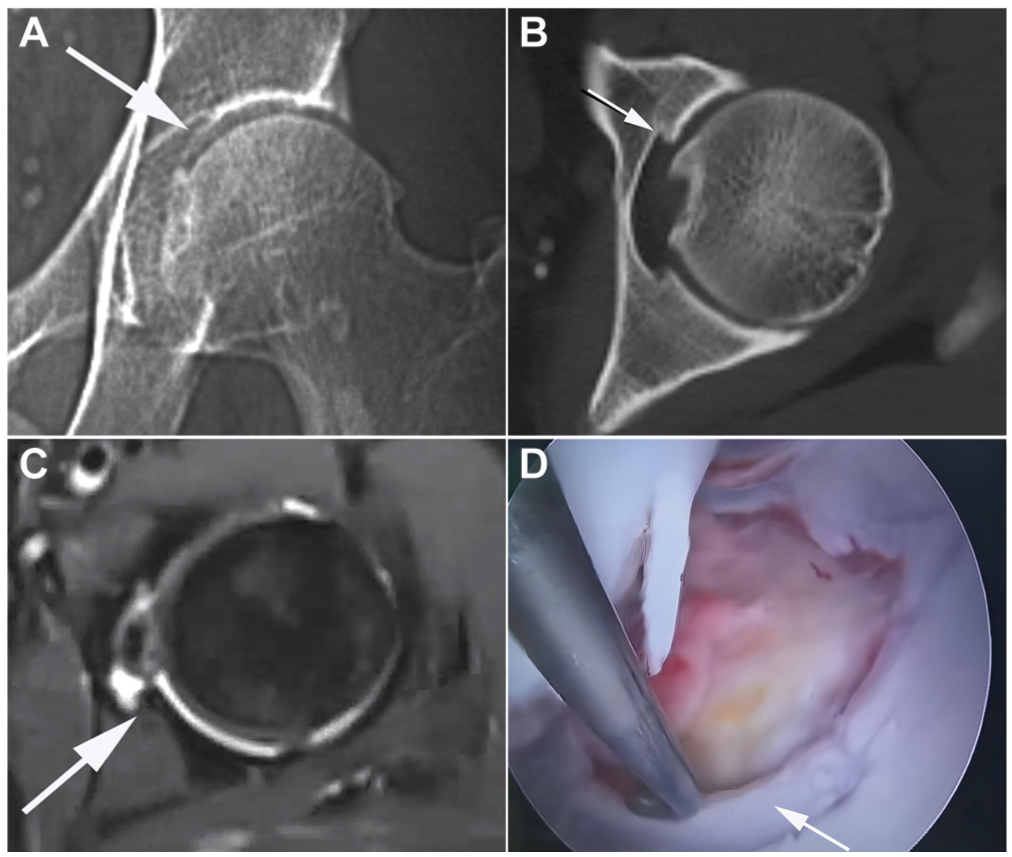
Imaging of CAO. (A and B) Detection of CAO on CT images. (C) Evaluation of CAO on MRI. (D) Arthroscopic visualization of CAO. White arrowheads indicate CAO. CAO, central acetabular osteophytes; CT, computed tomography; MRI, magnetic resonance imaging.
Surgical Procedures
The patient undergoing hip arthroscopy was placed on the operative table in the supine position and hip traction. Traction was gradually applied to the operative limb to create an 8 to 10 mm operative joint space. The anterolateral (AL) and mid-anterior portals (MAP) were used for the procedures. After these 2 portals were created, an interportal capsulotomy was performed between them. During operation of the central compartment, the presence of CAO, the chondral lesions of the acetabulum and femoral head, and the state of LT were assessed and recorded. The labrum repair and chondroplasty were also performed in the central compartment. The peripheral compartment was also addressed via the AL and MAP portals to treat cam lesions. After finishing osteochondroplasty of the femoral head-neck junction, the capsule closure was routinely performed in all the patients.
Radiographic Measurements
Radiographic measurements related to anterior acetabular instability were analyzed using a supine AP view of pelvic plain radiograph and computed tomography (CT) imaging (Figure 2). On the acetabular side, the anterior/posterior coverage, extrusion index, and Tönnis angle were assessed using Hip 2 Norm software (Bernese).30,31,39 The acetabular versions were investigated at the 1, 2, and 3 o’clock positions using the clockface orientation of the acetabulum on axial CT images. 24 On the femoral side, the femoral neck version was also investigated using the Reikeras method in axial CT imaging. 25 The neck shaft angle was also measured on sagittal CT imaging to minimize the effect of femoral neck version. 2 Pelvic tilt may affect the degree of acetabular version. Therefore, the pelvic incidence was assessed using sagittal CT imaging. 33 During CT examination, patients were scanned in a standardized supine position, with the pelvis in a natural resting orientation, the legs in native abduction-adduction alignment, and the patellae oriented anteriorly. 27 The radiographic parameters were reviewed independently by 2 senior fellows (J.-b.Z. and R.D.) in a blinded manner. Interobserver reliability was assessed using the intraclass correlation coefficient. Patients were stratified into 2 groups according to the presence or absence of CAO. Cross-sectional demographic and radiographic parameters were compared between groups to account for potential confounding. Parameters demonstrating significant between-group differences were subsequently entered into a binary logistic regression analysis.
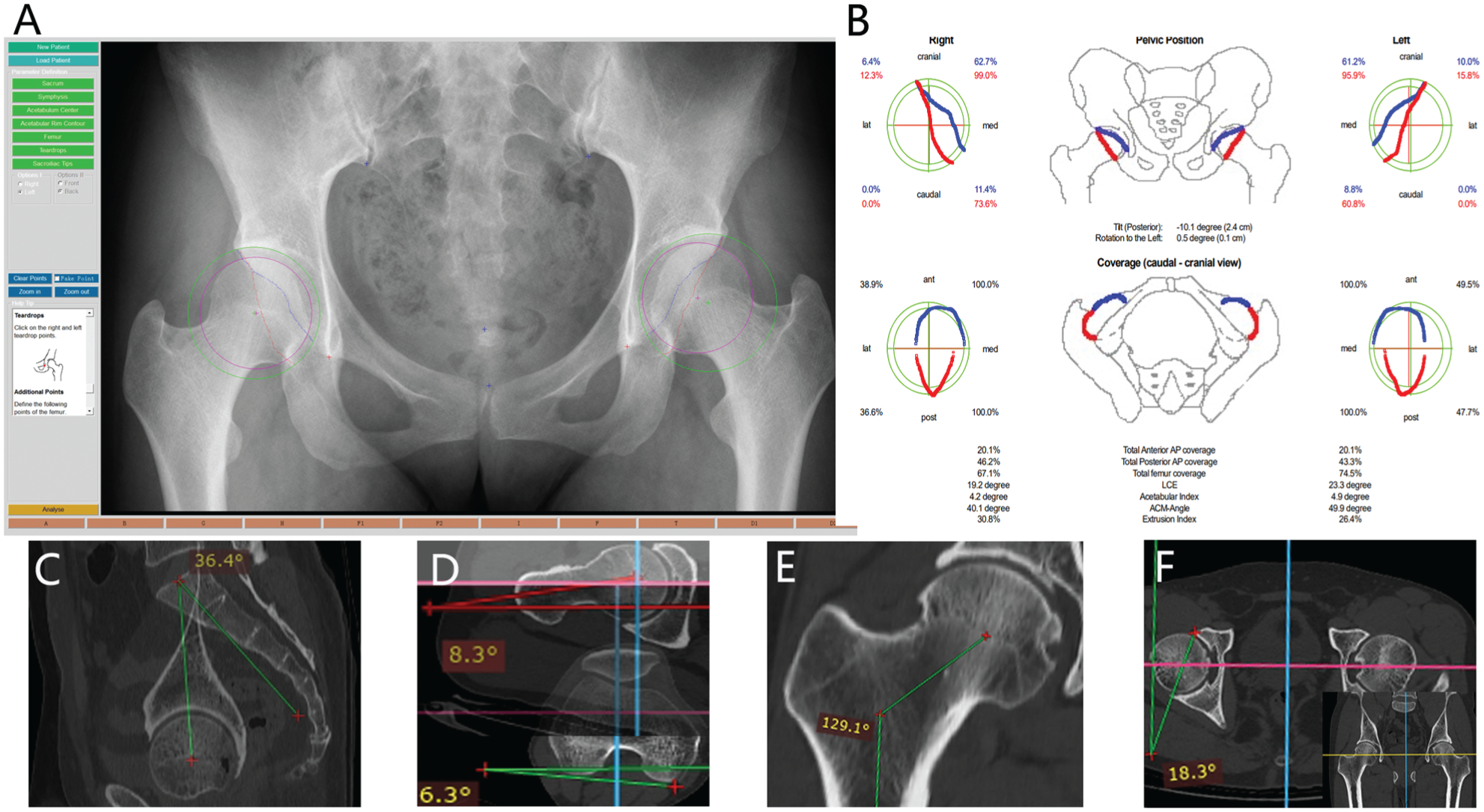
Radiographic measurements of the hip joint. (A and B) Measurement of the LCEA, anterior and posterior acetabular coverage, extrusion index, and Tönnis angle on supine anteroposterior pelvic radiographs using Hip 2 Norm software. (C-F) Assessment of pelvic incidence, femoral neck version, neck-shaft angle, and acetabular version, respectively, on CT images. AP, anteroposterior; CT, computed tomography; LCEA, lateral center-edge angle.
Assessment of Microinstability in the Hip Joint
The final diagnosis of hip microinstability was established intraoperatively according to the criteria outlined in a recently published international consensus. 11 The diagnosis was confirmed if one of the following conditions was present: (1) excessive distraction of the hip under general anesthesia, defined as separation of the joint with body weight alone or within 11 turns of fine traction. Moreover, after release of intra-articular negative pressure and withdrawal of traction, the joint could not be fully reduced. (2) Arthroscopic evidence of instability, characterized by an “inside-out” pattern of acetabular chondral injury or by linear chondrolabral damage involving the anterior or lateral acetabulum (3- to 12-o’clock positions on the acetabular clockface).
Statistical Analysis
A priori power analysis was used to evaluate the necessary numbers of patients based on a previously published study of CAO in the BDDH population, 37 and the results suggested that at least 68 hips in the CAO group and 60 hips in the non-CAO group were needed to realize a minimum of 80% power at the .05 level of significance (2-sided). Continuous parameters are presented as the mean ± standard deviation. The differences in these parameters between the cBDDH group and the nBDDH group were evaluated using independent Student t tests. The category variances were compared using the Fisher exact test. Binary logistic regression was used to investigate the associations of these osseous stability parameters, microinstability, and the presence of CAO with borderline dysplasia. SSPS 20.0 software (IBM) was used to perform statistical analyses. The level of statistical significance was set at .05.
Results
A total of 497 symptomatic hips received arthroscopic treatment in our hospital from January 2020 to December 2024. Among these hips, 169 met the LCEA inclusion criteria. However, 11 hips were excluded from the study because of an abnormal Beighton index (3 hips; Beighton score, ≥4), Legg-Calve-Perthes disease (1 hip), or previous hip or spinal surgery (3 hips). Another 5 hips were excluded from the present study because of incomplete imaging. Finally, 157 hips were included in the present study (Figure 3). In the presence of CAO, there were 76 patients (67 women/9 men) in the cBDDH group and 81 patients (69 women/12 men) in the nBDDH group. In the cBDDH group, there were 29 patients (23 women/6 men) with type 2 LT tears, 13 patients (12 women/1 men) with type 3 LT tears, and 3 patients (1 woman, 2 men) with type 1 LT tears. In the nBDDH group, there were 17 patients (13 women/4 men) with type 2 LT tears, 5 patients (2 women/3 men) with type 1 LT tears, and 1 patient (1 woman) with type 3LT tears. The cBDDH group had a higher rate of acetabular and femoral head chondral lesions as well as LT tears than the nBDDH group (63/76 vs 31/81; P < .001; 39/76 vs 19/81; P < .001; 45/76 vs 23/81; P < .001). The intraoperative findings are listed in Table 1. There was no difference in sex, age (28.22 ± 8.07 [95% CI, 25.11-31.54] vs 27.99 ± 7.28 [95% CI, 26.55-29.36]; P > .05) or body mass index (24.75 ± 3.33 [95% CI, 22.79-26.57] vs 24.15 ± 3.16 [95% CI, 24.15 ± 3.16]; P > .05) between the 2 groups (Table 2).
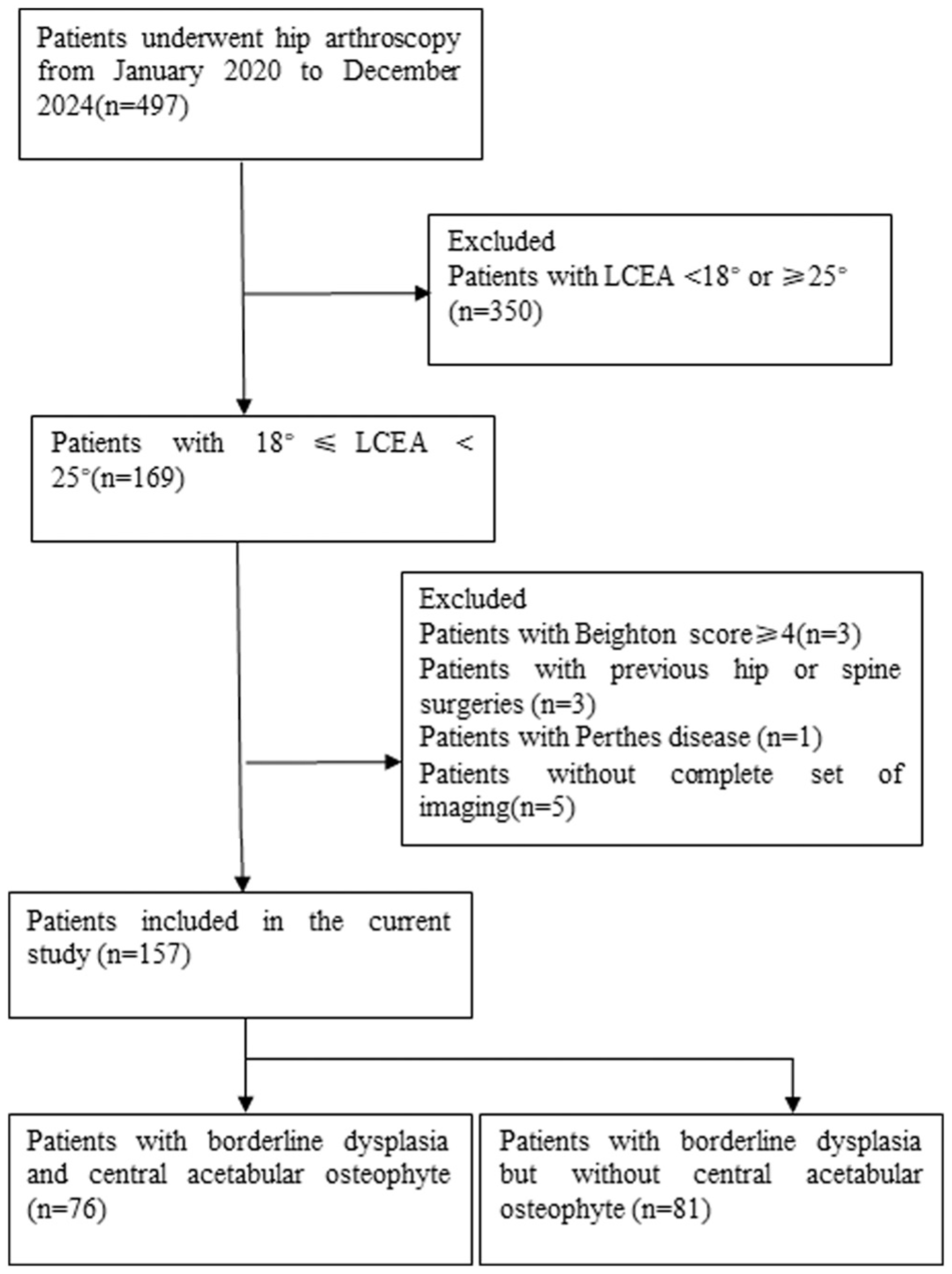
Flowchart of patient inclusion in the present study. LCEA, lateral center-edge angle
Intraoperative Findings a
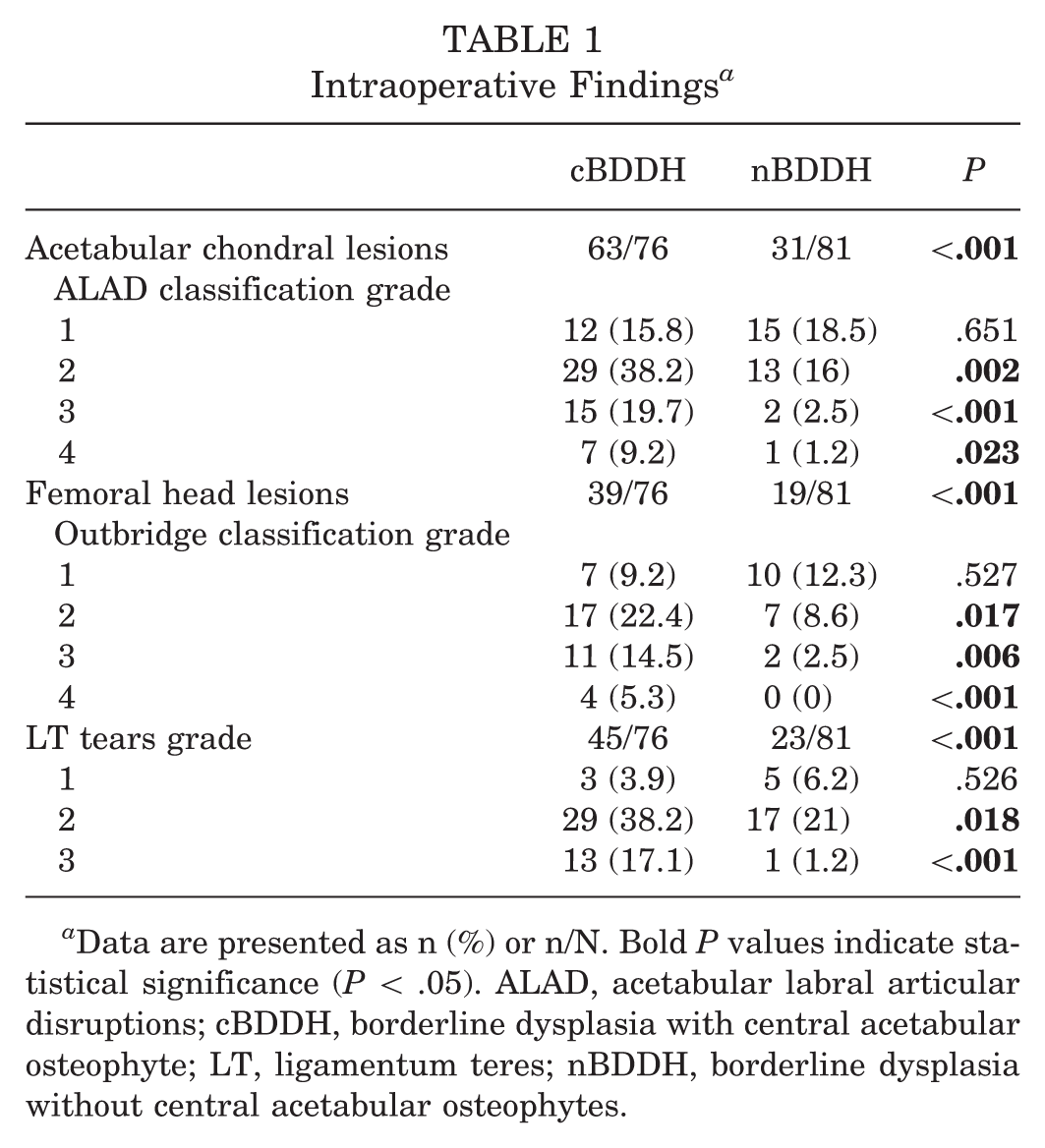
Data are presented as n (%) or n/N. Bold P values indicate statistical significance (P < .05). ALAD, acetabular labral articular disruptions; cBDDH, borderline dysplasia with central acetabular osteophyte; LT, ligamentum teres; nBDDH, borderline dysplasia without central acetabular osteophytes.
Radiographic Parameters and Descriptive Data Between Borderline Dysplasia ± CAO a
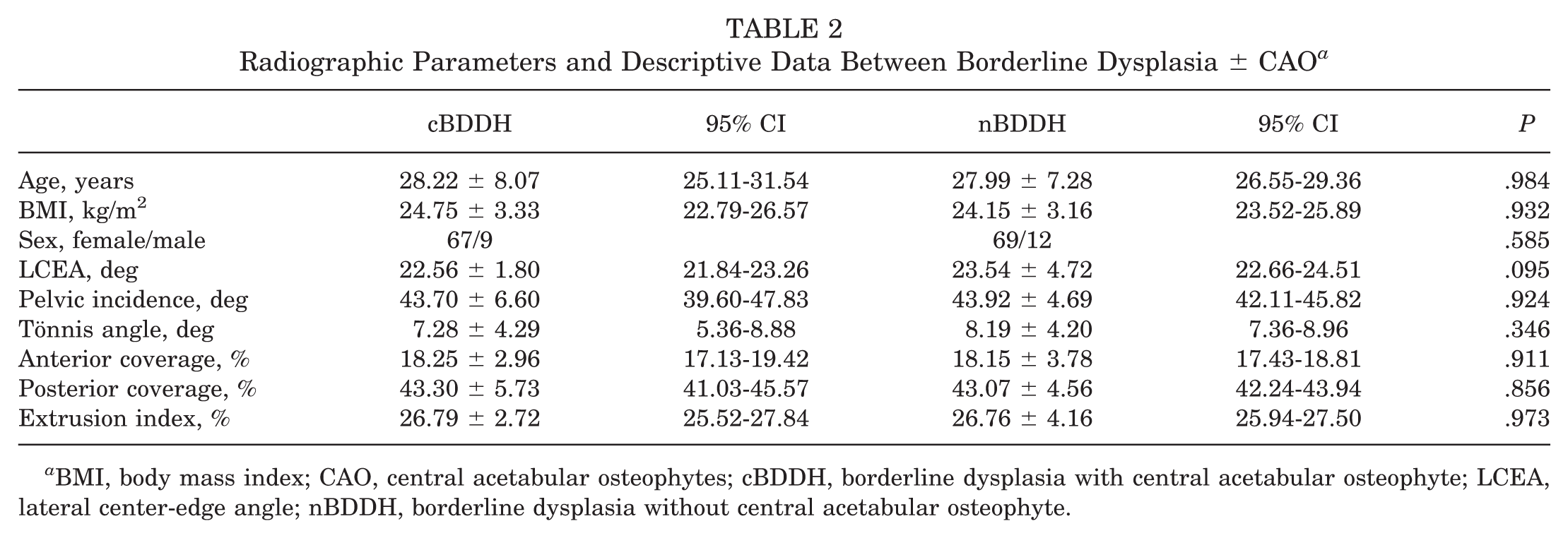
BMI, body mass index; CAO, central acetabular osteophytes; cBDDH, borderline dysplasia with central acetabular osteophyte; LCEA, lateral center-edge angle; nBDDH, borderline dysplasia without central acetabular osteophyte.
During the operation, we evaluated the microinstability of hip joints before CAO was finally confirmed by arthroscopy. The rates of microinstability and TL tear were significantly higher in the cBDDH group than in the nBDDH group (61/76 vs 19/81; P < .001; 45/76 vs 23/81; P < .001). The values of femoral neck version (34.47° ± 8.18° [95% CI, 30.93-37.88] vs 26.49° ± 12.18° [95% CI, 24.32-28.78]; P < .001), the acetabular version at the 2 o’clock (17.08° ± 4.13° [95% CI, 15.47-18.95] vs 14.58° ± 4.69° [95% CI, 13.72-15.40]; P < .05) and 3 o’clock positions (22.40° ± 4.10° [95% CI, 20.80-24.19] vs 19.60° ± 4.42° [95% CI, 18.81-20.48]; P < .001), and combined anteversion (42.92° ± 8.74° [95% CI, 39.28-46.44] vs 34.45° ± 13.10° [95 % CI, 31.88-36.77]; P < .001; 51.55° ± 9.03° [95% CI, 47.93-55.37] vs 41.07° ± 13.06° [95% CI, 38.55-43.46]; P < .001; 56.87° ± 8.25° [95% CI, 53.68-60.33] vs 46.09° ± 13.14° [95% CI, 43.62-48.55]; P < .001) were significantly higher in the cBDDH group than in the nBDDH group. There was no difference in the LCEA (22.56° ± 1.80° [95% CI, 21.84-23.26] vs 23.54° ± 4.72° [95% CI, 22.66-24.51]; P > .05), neck-shaft angle (133.06° ± 4.39° [95% CI, 131.29-134.96] vs 132.07° ± 4.10° [95% CI, 131.28-132.80]; P > .05), extrusion index (26.79% ± 2.72% [95% CI, 25.52-27.84] vs 26.76% ± 4.16% [95% CI, 25.94-27.50]; P > .05), pelvic incidence (43.70° ± 6.60° [95% CI, 39.60-47.83] vs 43.92° ± 4.69° [95% CI, 42.11-45.82]; P > .05), Tönnis angle (7.28° ± 4.29° [95% CI, 5.36-8.88] vs 8.19° ± 4.20° [95% CI, 7.36-8.96]; P > .05), or anterior coverage (18.25% ± 2.96% [95% CI, 17.13-19.42] vs 18.15% ± 3.78% [95% CI, 17.43-18.81]; P > .05)/posterior coverage (43.30% ± 5.73% [95% CI, 41.03-45.57] vs 43.07% ± 4.56% [95% CI, 42.24-43.94]; P > .05) of the acetabulum to the femoral head between 2 groups (Tables 2 and 3). The interobserver reliability of the radiographic parameters ranged from 0.812 to.921 (LCEA, .801; anterior coverage, 853; posterior coverage, 0.871; Tönnis angle, 0.903; femoral neck version, 0.867; acetabular version anteversion at the 1-, 2-, and 3-o’clock positions, 0.835/0.857/0.819; combined anteversion at the 1-, 2-, and 3-o’clock positions, 0.839/0.861/0.823; P < .01). The interobserver reliability of the intraoperative finding ranged from .0877 to 0.953 (LT tear, 0.953; diagnosis of microinstability, 0.877; CAO presence, 0.906).
Radiographic Parameters and Intraoperative Data Between Borderline Dysplasia ± CAO a
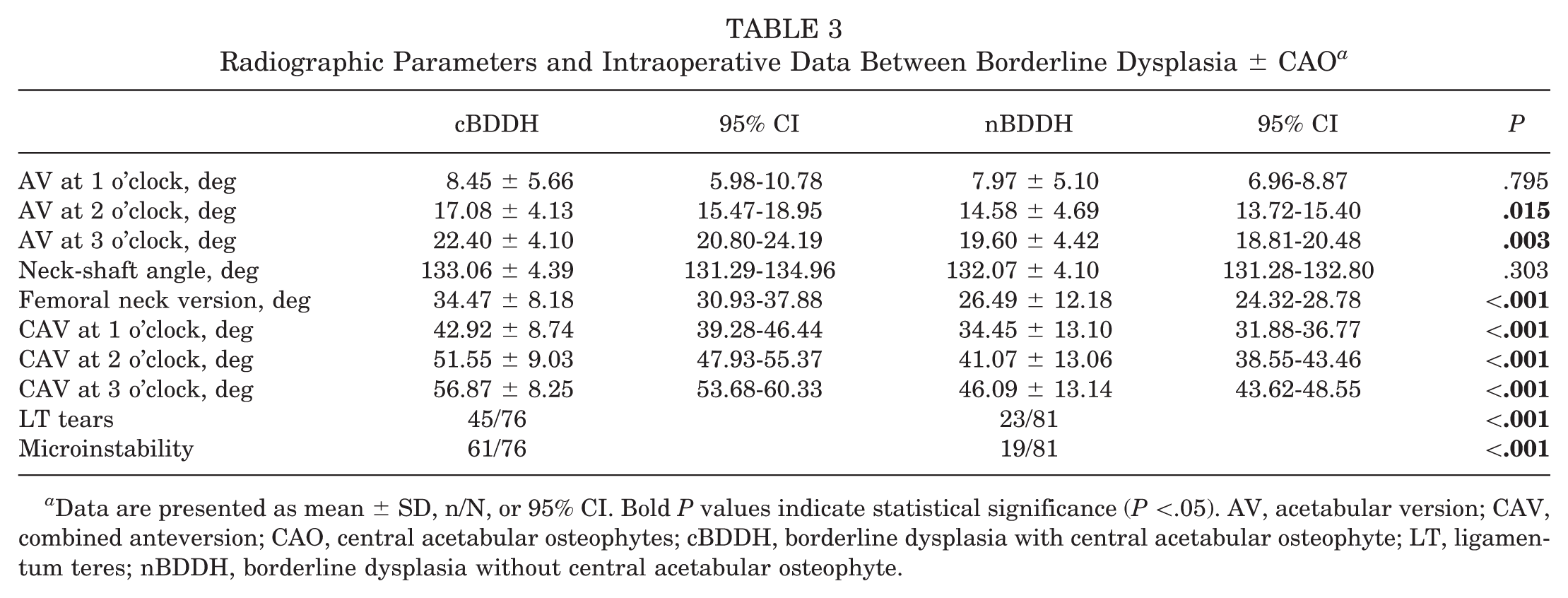
Data are presented as mean ± SD, n/N, or 95% CI. Bold P values indicate statistical significance (P <.05). AV, acetabular version; CAV, combined anteversion; CAO, central acetabular osteophytes; cBDDH, borderline dysplasia with central acetabular osteophyte; LT, ligamentum teres; nBDDH, borderline dysplasia without central acetabular osteophyte.
The results from binary logistic regression analysis suggested that patients with BDDH with microinstability (β = 0.027 [95% CI, 0.006-0.133]; P < .01), LT tears (β = 0.010 [95% CI, 0.001-0.164]; P = .001), or combined anteversion at the 3 o’clock position (β = 1.343 [95% CI, 0.965-1.868]; P = .029; R2 = .542) had a higher prevalence of CAO (Table 4).
Multivariable Logistic Regression Analysis for Associated Factors of CAO a
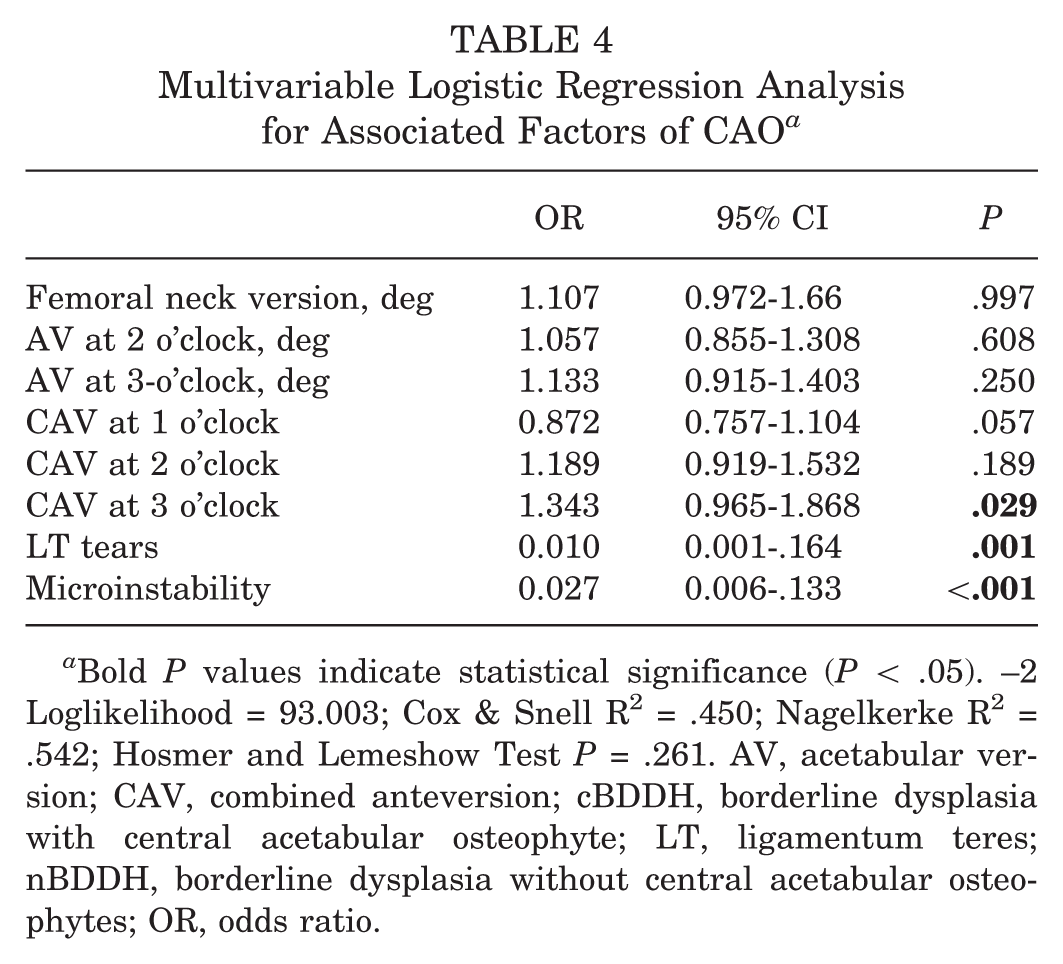
Bold P values indicate statistical significance (P < .05). –2 Loglikelihood = 93.003; Cox & Snell R 2 = .450; Nagelkerke R 2 = .542; Hosmer and Lemeshow Test P = .261. AV, acetabular version; CAV, combined anteversion; cBDDH, borderline dysplasia with central acetabular osteophyte; LT, ligamentum teres; nBDDH, borderline dysplasia without central acetabular osteophytes; OR, odds ratio.
Discussion
This study identified several important findings. Our results showed that patients with BDDH and CAO had a higher prevalence of microinstability when compared with patients with BDDH without CAO. The logistical regression analysis also suggested that CAO was associated with microinstability in patients with BDDH. In addition, the prevalence of CAO was associated with LT tears and increased combined anteversion at the 3 o’clock level of the acetabular clockface position. Given that osteophytes are widely regarded as an early marker of osteoarthritis, the observed association between CAO and microinstability in patients with BDDH may be better interpreted as reflecting overlapping biomechanical alterations and early degenerative processes rather than a single isolated mechanism.
CAO was first introduced in acetabular specimens by Varich et al 32 in 1993. Recently, Yang et al 38 reported that the presence of CAO adversely affected outcomes in patients with femoroacetabular impingement (FAI) after primary arthroscopic treatment. Lerch et al 15 reviewed magnetic resonance arthrography in 27 patients with FAI who had failed arthroscopic surgery. They found that the presence of CAO was a predictor of failure of arthroscopic hip surgery. In addition, Kuhn et al 12 reviewed 155 patients with FAI and CAO who underwent hip arthroscopy and found that arthroplasty-free survival rates were lower in these patients than in the control group after 5 years of follow-up. However, the association between CAO and inferior outcomes after arthroscopic treatment remains unclear. In the present study, our results showed that the presence of CAO in patients with BDDH was associated with microinstability. Several studies have shown that unrecognized or untreated microinstability is a leading cause of suboptimal outcomes and revision surgery after hip arthroscopy.3,4,13,29 When microinstability is present, arthroscopic procedures that address only intra-articular pathology (eg, labral tears or focal chondral damage) without correcting the underlying microinstability are prone to fail. Therefore, the inferior outcomes observed in patients with FAI and CAO after arthroscopic treatment may reflect the combined influence of microinstability and early degenerative change, rather than a direct effect of CAO itself.
Varich et al 32 suggested that the formation of CAO might be due to femoral head anterosuperolateral migration during degeneration of the articular structure. Migration of the femoral head may increase tension on the LT and simultaneously promote the formation of CAO and femoral foveal osteophytes, while also generating abnormal shear forces and elevated contact stress on hyaline cartilage that are known to contribute to osteoarthritic change. The study by Lodhia et al 16 also supports this explanation. In this study, our results showed that CAO was associated with increased combined anteversion at the 3 o'clock position on the acetabular clockface position, suggesting that CAO might be closely related to anterior osseous instability of the hip joint in patients with BDDH. Increased combined anteversion alters the socket orientation, rotating the anterior acetabular rim away from the femoral head. This effectively reduces anterior hip coverage and places greater reliance on soft tissue stabilizers, such as the labrum and LT. In the presence of excessive combined anteversion, anterior undercoverage may predispose the femoral head to anterior translation, which may in turn manifest as labral injury, LT pathology, or CAO formation. Since excessive femoral head translation was closely related to hip microinstability, our results indicated that CAO formation might be induced by anterior migration of the femoral head due to increased combined anteversion in patients with BDDH.
Several studies have demonstrated a close association between LT tears and CAO. Varich et al 32 suggested that femoral head migration increases LT tension, leading to CAO formation, whereas Lodhia et al 16 reported that LT tears were more common in patients with CAO. Biomechanically, the LT functions as a secondary stabilizer, limiting femoral head translation when acetabular coverage is insufficient or femoral version is increased.1,5 Therefore, LT tear was tightly associated with hip microinstability. 35 In our study, patients with BDDH and CAO showed increased combined anteversion and a high prevalence of LT tears, indicating anterior instability. We proposed that diminished anterior coverage permits femoral head translation, thereby elevating LT tension, inducing CAO formation, and further aggravating LT pathology and joint microinstability.22,26 Thus, CAO and LT tears likely coexist as manifestations of hip microinstability in patients with BDDH, and the presence of CAO may serve as a marker of microinstability.
Osteophyte formation is widely regarded as an early marker of osteoarthritis. CAOs in borderline dysplastic hips may therefore be best understood not as isolated pathological entities, but as markers arising at the intersection of altered biomechanics and early degenerative change. While microinstability and version abnormalities may contribute to abnormal joint loading and shear stress, CAO formation may also reflect an early osteoarthritic response. Accordingly, causality cannot be inferred from our cross-sectional intraoperative observations. CAO should not be regarded as a driver of microinstability, but rather as part of an overlapping biomechanical-degenerative spectrum at the intersection of altered joint loading and early osteoarthritic response in borderline dysplastic hips, warranting longitudinal studies to clarify temporal relationships and clinical implications.
Based on our findings, symptomatic patients with BDDH may warrant more careful preoperative assessment before hip arthroscopy. A preoperative CT scan with 2-dimensional reconstruction may assist in detecting CAO and in evaluating pelvic incidence, acetabular version, and femoral version, which may help identify patients at greater risk of instability. In cases in which CAO coexists with excessive combined anteversion, correction of the underlying osseous instability with a periacetabular osteotomy may be considered in selected patients. Conversely, when combined anteversion is within a normal range, or when CAO is identified only intraoperatively, hip arthroscopy performed using a periportal rather than an intraportal capsulotomy, with meticulous capsular closure or plication to enhance anterior stability, may be appropriate.23,34 Arthroscopic iliopsoas tenotomy at the joint level should be approached with caution in this population, as it may theoretically exacerbate anterior instability.14,20
This study has several limitations. Selection bias may be present because the cohort included only patients undergoing hip arthroscopy, and intraoperative assessment of microinstability and CAO was subject to potential observer bias, with no formal interobserver reliability testing. In addition, the cross-sectional design and intraoperative identification of both findings preclude causal inference, and CAO could not be reliably detected on preoperative imaging, potentially limiting its immediate clinical utility. Because pelvic tilt may influence acetabular anteversion, pelvic incidence was used to estimate pelvic orientation. However, differences between standing and supine postures may have introduced measurement bias, although the comparable pelvic incidence between groups suggests that this likely limited its impact on our results. Finally, the absence of patient-reported outcomes and long-term follow-up prevented evaluation of prognostic implications. Future prospective longitudinal studies, including both operative and nonoperative BDDH populations, that incorporate standardized diagnostic criteria, advanced imaging assessments, and patient-reported outcomes, with extended follow-up, are warranted to clarify temporal relationships and define the clinical significance of CAO in this population.
Conclusion
CAO was associated with microinstability and LT tear in patients with BDDH. In addition, CAO is also associated with combined anteversion at the 3 o’clock level on the acetabular clockface position. Taken together, CAO might be a marker of microinstability in patients with BDDH.
Footnotes
Submitted October 6, 2025; accepted April 30, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from the Ethics Committee of Xin-Hua Hospital, affiliated with Shanghai Jiao Tong University, School of Medicine (XHBC-2025-510).