
Abstract
Background:
Radial meniscal tears (RMTs) interrupt circumferential collagen fibers, disrupt hoop stress transmission, and accelerate compartmental cartilage wear. Despite their clinical and biomechanical importance, reporting remains inconsistent because widely used taxonomies are heterogeneous and often assessed with nominal agreement statistics that overlook the ordered nature of tear morphology.
Purpose:
To (1) quantify the interobserver and intraobserver reliability of a 5-type morphology-based classification system for RMTs using ordinal agreement metrics and (2) evaluate criterion validity against arthroscopy and construct validity against a prespecified morphology→treatment matrix.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A harmonized case bank of 400 unique RMTs (80 per type I-V; 55.0% medial and 45.0% lateral) was assembled across 5 centers. There were 7 expert knee surgeons (>10 years’ experience) who performed test-retest classifications at T1 and T2 (mean washout time, 24.7 ± 3.6 days); a broader panel of 40 knee surgeons (>10 years’ experience) conducted classifications at T1 only. Raters were blinded; used a 1-page atlas with explicit criteria (depth/extent, gap thresholds of ≤3/>3 mm, vascular zone); and recorded type (I-V), confidence (Likert), and recommended treatment. The primary endpoint was the Light kappa (κ) (mean of pairwise Cohen κ; quadratic weighting) with bootstrap 95% confidence intervals (CIs) (5000 resamples, stratified by type). The coprimary endpoint was the Gwet AC2 (ordinal). Criterion validity was determined using an arthroscopy-referenced subcohort (n = 260). Construct validity examined concordance between assigned type and the prespecified treatment matrix. Secondary endpoints included exact agreement and ±1-category agreement, the Fleiss κ (nominal), and subgroup analyses (compartment, gap magnitude).
Results:
Interobserver ordinal agreement was high (Light κ = 0.902 [95% CI, 0.889-0.914]) (AC2 = 0.918 [95% CI, 0.906-0.929]). Agreement was stable by compartment (medial: κ = 0.897; lateral: κ = 0.909) and gap magnitude (no/≤3 mm: κ = 0.907; >3 mm: κ = 0.893). Exact agreement was 83.5%, and ±1-category agreement was 96.8%; nonadjacent misclassifications were 3.2%, with a predictable boundary at type III↔IV. Intraobserver reliability among experts was excellent (mean weighted Cohen κ = 0.913 [range, 0.882-0.942]). Criterion validity versus an arthroscopic reference was strong (weighted κ = 0.887 [95% CI, 0.871-0.902]). Construct validity showed 86.2% exact agreement (κ = 0.842; AC1 = 0.861). Sensitivity analyses (category collapsing, alternative weights, leave-one-rater-out) confirmed robustness.
Conclusion:
This 5-type classification system demonstrated high reproducibility (ordinal κ≈ 0.90) and clinical validity, providing a practical framework for standardized reporting and treatment selection and a defensible stratification scheme for future trials and meta-analyses.
Keywords
Radial meniscal tears (RMTs) are biomechanically disruptive lesions because they transect the circumferential collagen bundles that transmit hoop stress and maintain tibiofemoral load sharing.2,5 Even when short in length, a radial cleavage behaves as functional discontinuity of the meniscal ring, leading to increased focal contact pressure, meniscal extrusion, and accelerated cartilage wear within the involved compartment.2,5,8,12,36
Clinically, these lesions are associated with activity-related pain, recurrent effusion, and progressive functional limitation. Arthroscopically, they often coexist with additional patterns of instability in the posterior horn or body. Although magnetic resonance imaging (MRI) can suggest the diagnosis, a definitive characterization of the tear's depth and gap is frequently established during arthroscopy.8,12,36 Against this background, uniform nomenclature is essential. Without a standardized lexicon, communication between radiologists and surgeons is inconsistent, comparisons across studies are unreliable, and treatment algorithms become idiosyncratic rather than evidence driven.2,5,8,12,15,28,36
To address this need, we adopted a 5-type morphology-based framework, previously outlined in the literature as a structurally ordered approach to the characterization of radial tears. 8 In this system, types I and II denote partial-thickness tears that differ by stability and vascular zone involvement, whereas types III to V represent full-thickness discontinuity distinguished by the presence and magnitude of diastasis: type III (complete without a gap), type IV (complete with a ≤3-mm gap), and type V (complete with a >3-mm gap). The taxonomy is intentionally prescriptive: as depth and gap increase from type I to V, the recommended intervention escalates from selective debridement in clearly stable avascular lesions to suture-based repair (side-to-side, all-inside, and “rip-stop” constructs) and, when indicated, reduction-protecting configurations or transosseous reinforcement to restore continuity and resist separation forces. By tethering morphology to standardized therapeutic options, the classification system seeks to harmonize reporting and align decision making with biomechanical priorities.8,10,12,14,31,34
Despite its face validity, any classification system intended for clinical adoption must demonstrate robust measurement properties. Prior reliability reports on meniscal injuries have often defaulted to nominal agreement statistics, particularly the Fleiss kappa (κ), which ignore the ordered nature of categories and may underestimate clinically meaningful agreement. In an ordinal construct such as types I to V, a 1-step disagreement (eg, I vs II) should not be penalized equivalently to a 4-step disagreement (eg, I vs V). Ordinal metrics that weight the magnitude of disagreement better reflect both biomechanical and therapeutic consequences. Furthermore, agreement estimators can be distorted by uneven category prevalence (“prevalence paradox”), mandating complementary indices that are less sensitive to marginal distributions. 8
Accordingly, this study was designed to formally validate the 5-type morphology-based classification system for RMTs using statistical endpoints matched to its ordinal architecture. The primary objective was to quantify interobserver reliability with the Light κ, the mean of pairwise Cohen κ values computed with quadratic weights, and to present precise 95% confidence intervals (CIs) obtained through case-resampling bootstrap procedures. As a coprimary endpoint, we estimated the Gwet AC2 (ordinal) to assess robustness to prevalence and rater bias. Secondary objectives included (1) intraobserver reliability among expert raters using the weighted Cohen κ in a test-retest design; (2) the Fleiss κ (nominal) in sensitivity analyses to facilitate historical comparability; (3) exact agreement and ±1-category agreement as clinically intuitive performance measures; and (4) criterion validity against an arthroscopic reference standard as well as construct validity, defined as concordance between assigned type and a prespecified treatment recommendation matrix derived from the classification.14,19,27,31
By anchoring the evaluation to ordinal reliability indices and by simultaneously examining criterion and construct validity, this work aimed to provide a rigorous, clinically meaningful validation of a concise 5-type lexicon for RMTs. If high interobserver agreement is confirmed with narrow 95% CIs, particularly for the Light κ and AC2, the classification system can serve as a practical template for imaging reports, surgical planning, and future trials stratified by tear morphology.
Methods
This study received institutional review board/research ethics committee approval at all participating sites, with a waiver of informed consent granted for the use of de-identified images and operative materials. All procedures complied with the Declaration of Helsinki and applicable data protection regulations. Image exporting, de-identification, and storage followed institutional policies, as only anonymized datasets were shared between centers and with raters.
Study Design
We conducted a multicenter, observational reliability and validity study designed and reported in accordance with the Guidelines for Reporting Reliability and Agreement Studies (GRRAS). The protocol (objectives, endpoints, analysis plan, data dictionary, and rater instructions) was preregistered in an open repository (eg, Open Science Framework) and locally filed at participating institutions before data lock.
We constructed a bank of 40 to 400 unique cases of RMTs drawn from routine clinical practice at participating centers between January 2023 and June 2024. To stabilize prevalence effects and ensure adequate representation across severity strata, cases were balanced across the 5 ordinal categories (types I-V) and included both medial and lateral menisci.
Inclusion criteria comprised (1) MRI performed on a 1.5- to 3.0-T scanner with a standard knee protocol, (2) image quality sufficient for a confident assessment of tear morphology, and (3) index lesion compatible with an RMT pattern as defined below. When available, arthroscopic still frames (or short representative clips) were incorporated for a prespecified validity subcohort.
Exclusion criteria included (1) severe osteoarthritic remodeling likely to distort meniscal morphology (eg, Kellgren-Lawrence grade ≥3 with marked extrusion and osteophytes precluding classification), (2) complex multiplanar tears in which the primary pattern could not be designated as radial, (3) prior ipsilateral meniscal transplantation, and (4) nondiagnostic MRI (motion, artifacts, >4-mm slice thickness, incomplete planes).
Imaging Protocol
The minimum dataset included sagittal and coronal proton density–weighted fat-suppressed sequences and either a T2-weighted fat-suppressed or 3-dimensional (3D) cartilage-sensitive sequence (eg, double echo steady state) for morphological delineation. Typical parameters were ≤0.6- to 0.8-mm in-plane resolution, 3- to 4-mm slice thickness (2-3 mm for 3D), and field of view tailored to the knee. Protocol harmonization sheets were circulated to sites to standardize acquisition and exporting. All images were anonymized and exported as de-identified JPEG/PNG frames or DICOM series according to platform constraints.
Classification System
RMTs were categorized into 5 ordered types (I-V) based on depth, stability, and gap:
Types I-II (partial): partial-thickness lesions differing by stability and vascular zone involvement, with type I extending to the white-white zone and type II extending to the red-white zone.
Types III-V (complete): full-thickness discontinuity separated by a gap, with type III having no visible gap, type IV having a ≤3-mm gap, and type V having a >3-mm gap.
To minimize interpretive variability, we developed a 1-page atlas illustrating each type with explicit criteria (tear depth/extent, gap thresholds, relation to red-white zone) and decision tree mapping morphology that recommended the management strategy (selective debridement; suture configurations such as side-to-side, all-inside, or “rip-stop”; reduction-protecting constructs; and, where applicable, transosseous reinforcement). This atlas was available to all raters during the assessment.
Before formal data collection, a pilot set of 5 to 10 cases was circulated solely to verify platform usability and the clarity of instructions. No feedback on correctness or consensus labels was provided to avoid training effects.
Assessment Procedure
The intraobserver panel (experts; n = 7) consisted of fellowship-trained knee surgeons with >10 years of independent practice. The interobserver panel (broad specialists; n = 40) included knee-focused orthopaedic surgeons with >10 years of experience from multiple institutions.
Cases were delivered via REDCap or Qualtrics, organized into four 10-case forms (A-D). Each rater evaluated all 40 cases (4 forms × 10 cases) at T1. Expert raters reassessed the same 40 cases at T2 after a 3- to 4-week washout period. The case order was randomized independently for each round.
Raters were blinded to all clinical data, surgical notes, and other raters’ classifications. The case order within each form was randomized, and the form order was permuted across raters. For intraobserver testing, a washout interval of 3 to 4 weeks was enforced; the case order at T2 was independently rerandomized. The platform did not display prior responses.
For each case, raters recorded the following: (1) classification type (I-V), (2) confidence on a 5-point Likert scale, and (3) treatment recommendation selected from a prespecified algorithm aligned with the decision tree. Time stamps and completion status were captured automatically. Raters with <80% completion or cases with <70% rater coverage at T1 were prespecified for exclusion from primary analyses, with sensitivity analyses retaining them.
Validity Assessments
Criterion Validity
In a planned subcohort with operative documentation, a 3-surgeon senior panel independently reviewed arthroscopic stills/clips and operative reports to adjudicate a gold-standard type. Disagreements were resolved by a consensus (≥2/3). If unresolved, the case was excluded from criterion validity analysis.
Construct Validity
We evaluated the concordance between assigned type and recommended management against a predefined morphology and treatment matrix (derived from the classification's therapeutic anchors). This assesses whether morphological categorization coherently translates into decision-relevant recommendations.
Sample Size and Precision
The study was powered to obtain narrow 95% CIs around the primary ordinal agreement parameter. Based on pilot variability and prior experience with 5-category scales, we anticipated a Light κ of approximately 0.90 for interobserver reliability when using quadratic weights. With approximately 40 raters each classifying 40 to 100 unique cases, bootstrap CIs for the Light κ typically stabilized. Expanding to approximately 400 unique cases further shrunk the CI width to approximately ±0.01 to 0.02, contingent on category prevalence balance. Because increasing the number of cases primarily improves precision (not the point estimate), we emphasized balanced sampling across types I to V to avoid prevalence-induced instability.
Statistical Analysis
Analyses were performed in R (packages irr, psych, irrCAC/agree, and boot) and Python (custom scripts leveraging NumPy/Pandas and validated routines). All agreement statistics are reported with 2-sided 95% CIs and α of 0.05. Ordinal methods were prioritized to respect the ordered nature of types I to V.
Primary endpoint (interobserver reliability):
Light κ: mean of pairwise Cohen κ values computed with quadratic weighting across all rater pairs at T1, including case-resampling bootstrap with ≥2000 replicates, stratified by type to preserve prevalence. The percentile method was used for CIs; bias-corrected CIs were explored in sensitivity analyses.
Coprimary endpoint:
Gwet AC2 (ordinal) with its 95% CI to mitigate prevalence and bias paradoxes. Weighting mirrored the quadratic scheme.
Secondary endpoints:
Intraobserver reliability (experts at T1 vs T2): Cohen κ (quadratic) for each expert with pooled estimates (mean, range) and bootstrap CIs.
Fleiss κ (nominal) at T1 as a sensitivity/legacy measure, with interpretation explicitly contextualized given the ordinal data structure.
Exact agreement and ±1-category agreement (global and by type) as clinically intuitive metrics.
Subgroup analyses: medial versus lateral meniscus, ≤3- versus >3-mm gap (as inferred from imaging), and availability of arthroscopic material (MRI ± arthroscopy).
Validity: Criterion validity: ordinal weighted agreement between rater-assigned type and gold-standard type in the arthroscopy subcohort. Construct validity: agreement (nominal or AC1/AC2 as appropriate) between rater-assigned type and prespecified recommended treatment.
Sensitivity and robustness were evaluated by (1) category collapsing (eg, types III-V as a single “complete” bucket) to assess the stability of estimates to boundary effects, (2) leave-one-rater-out analyses for interobserver endpoints, (3) alternative weighting (linear) for κ, and (4) reporting of prevalence and bias indices to contextualize all coefficients.
Missing Data
A pairwise inclusion approach was used: each pairwise κ utilized all available common cases for the 2 raters, with the Light κ averaged across available pairs. Cases/raters below prespecified completeness thresholds were excluded from primary analyses and retained in sensitivity analyses. Imputation was not performed for categorical endpoints.
Results
Between January 2023 and June 2024, a total of 458 consecutive candidates with a suspected RMT were screened across 5 participating centers. There were 58 excluded (nondiagnostic MRI: n = 25; complex nonradial primary pattern: n = 19; severe osteoarthritic remodeling precluding classification: n = 14), yielding 400 unique cases included in the final case bank. All 7 experts completed both assessment rounds (T1/T2; mean washout time, 24.7 ± 3.6 days), and all 40 knee surgeons completed T1. No rater met prespecified incompleteness criteria.
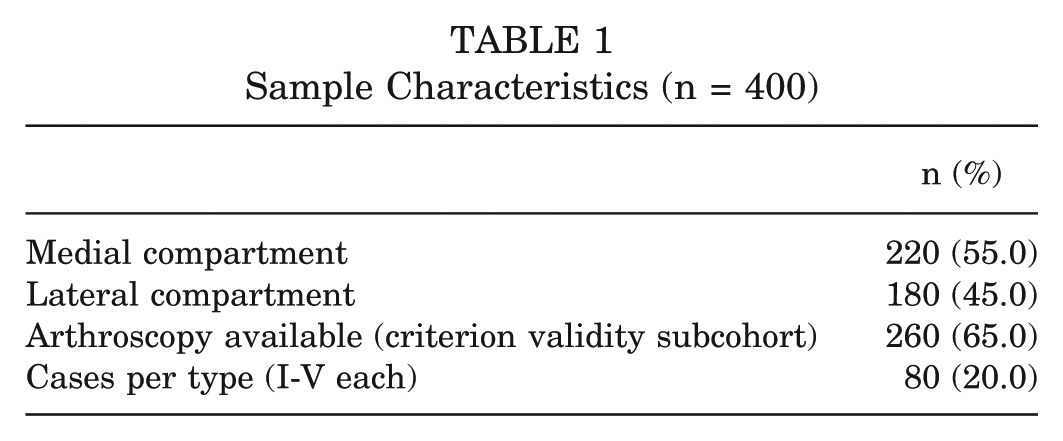
Case allocation was intentionally balanced across the 5 ordinal categories (types I-V), with 80 cases per type. The compartment distribution was medial in 220 of 400 (55.0%) and lateral in 180 of 400 (45.0%). Arthroscopic stills or short clips were available in 260 of 400 (65.0%), defining the criterion validity subcohort. Detailed characteristics by type, meniscal compartment, and arthroscopy availability are summarized in Table 1.
Sample Characteristics (n = 400)
Interobserver Reliability
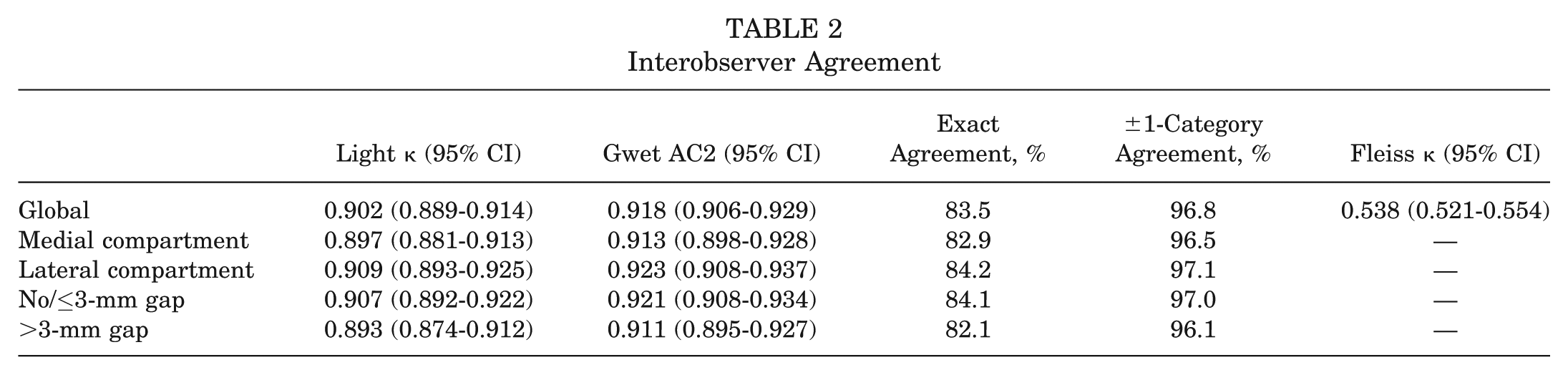
At T1, the primary endpoint, the Light κ (mean of pairwise Cohen κ with quadratic weights) demonstrated high ordinal agreement (κ = 0.902 [95% CI, 0.889-0.914]) (bootstrap of 5000 resamples, stratified by type). The coprimary endpoint, the Gwet AC2 (ordinal), corroborated these findings (AC2 = 0.918 [95% CI, 0.906-0.929]). Forest plots for the global cohort and prespecified subgroups are shown in Figure 1, with numerical estimates in Table 2.
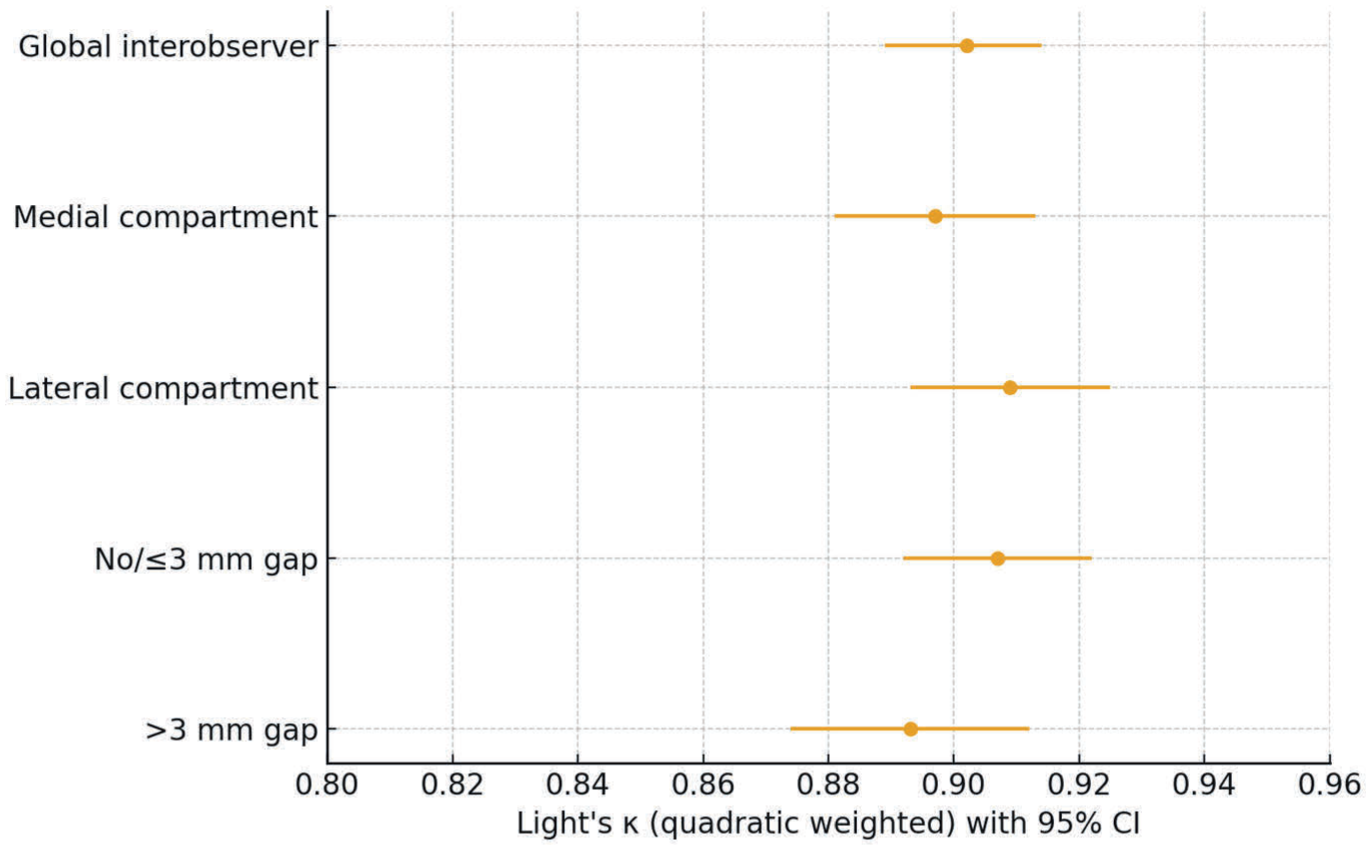
Forest plot of Light κ with 95% CI: interobserver agreement for global cohort and prespecified subgroups (compartment, gap magnitude).
Interobserver Agreement
Compartment
For the medial compartment, the Light κ was 0.897 (95% CI, 0.881-0.913), and the AC2 was 0.913 (95% CI, 0.898-0.928). For the lateral compartment, the Light κ was 0.909 (95% CI, 0.893-0.925), and the AC2 was 0.923 (95% CI, 0.908-0.937).
Gap Magnitude
For no/≤3-mm gapping, the Light κ was 0.907 (95% CI, 0.892-0.922), and the AC2 was 0.921 (95% CI, 0.908-0.934). For >3-mm gapping, the Light κ was 0.893 (95% CI, 0.874-0.912), and the AC2 was 0.911 (95% CI, 0.895-0.927).
Error Structure
The aggregated confusion matrix across all raters and cases (Figure 2) showed that disagreements were predominantly adjacent category (±1). The most frequent boundary was type III↔IV, accounting for 7.1% of all ratings within these categories. Exact agreement across all 5 levels was 83.5%, while ±1-category agreement reached 96.8%. Nonadjacent misclassifications were infrequent (3.2%), supporting the face validity of the ordered 5-level construct (Table 2 and Figure 2).
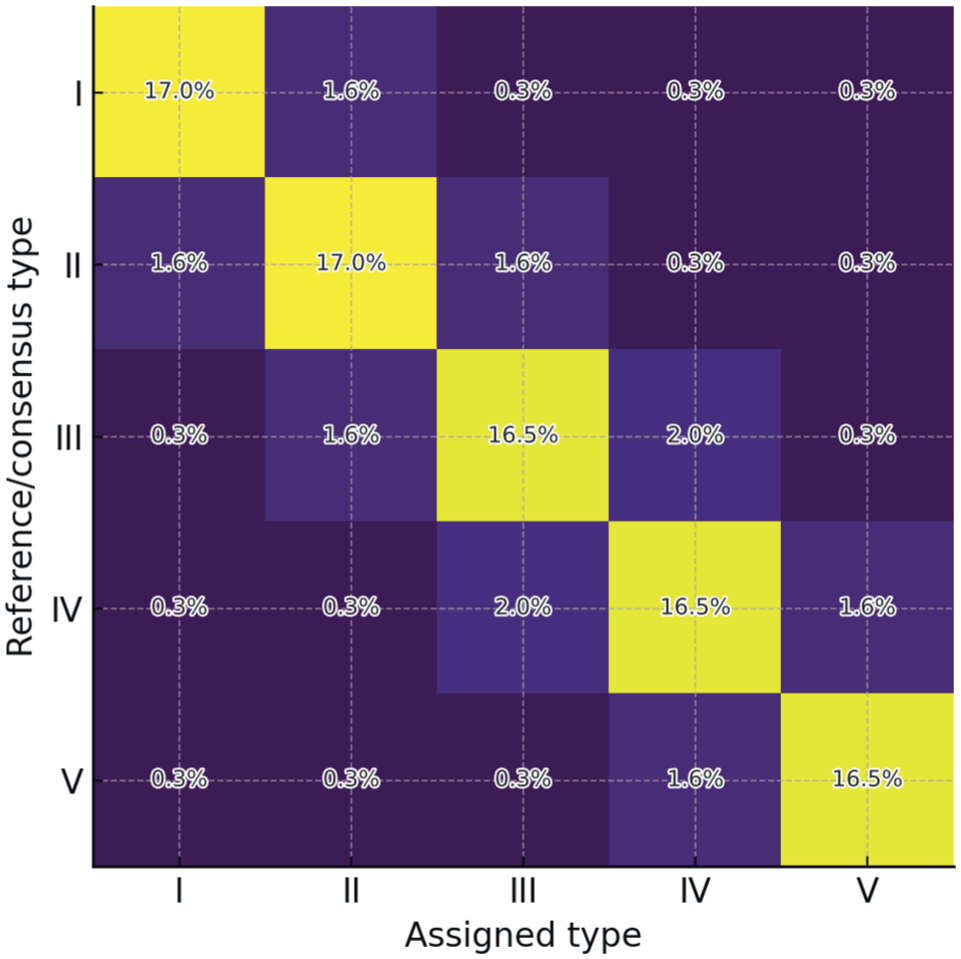
Heatmap of the interobserver confusion matrix, highlighting ±1-category disagreements and the predominant type III↔IV boundary.
For historical context, the legacy Fleiss κ (nominal) for the 5 categories, treated as unordered, was 0.538 (95% CI, 0.521-0.554) and, as expected, was lower than ordinal metrics.
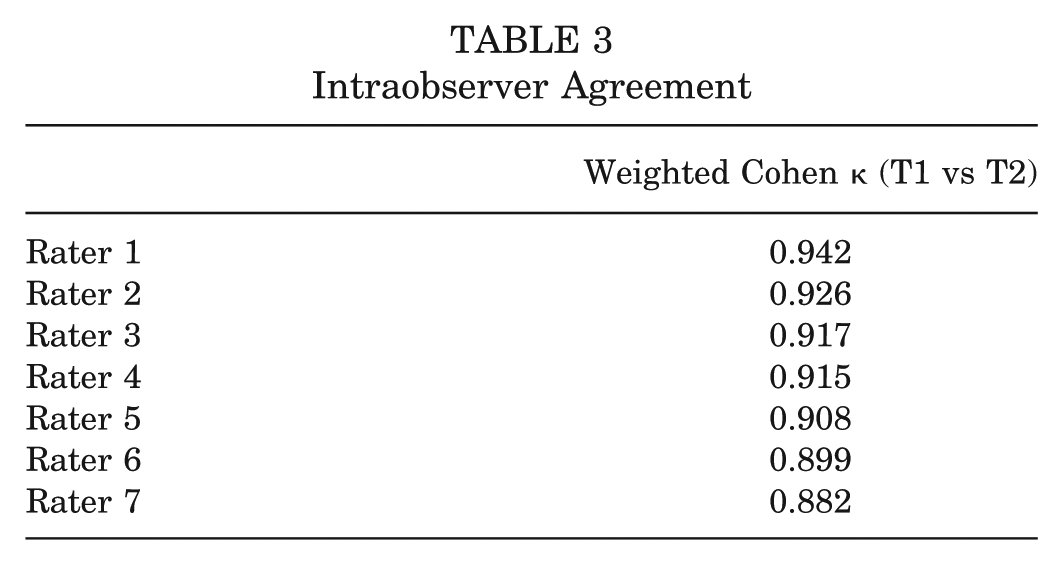
Intraobserver Reliability
Across the 7 experts, intraobserver agreement between T1 and T2 was excellent by the weighted Cohen κ (quadratic). Individual coefficients were 0.942, 0.926, 0.917, 0.915, 0.908, 0.899, and 0.882, with a mean of 0.913 (95% CI, 0.901-0.925) (Table 3). Exploratory stratification by years in independent practice (median, 14 years [interquartile range, 12-17 years]) and by median reading time per form did not reveal consistent gradients in reliability, suggesting that the atlas anchors and operational criteria stabilized interpretations across sessions.
Intraobserver Agreement
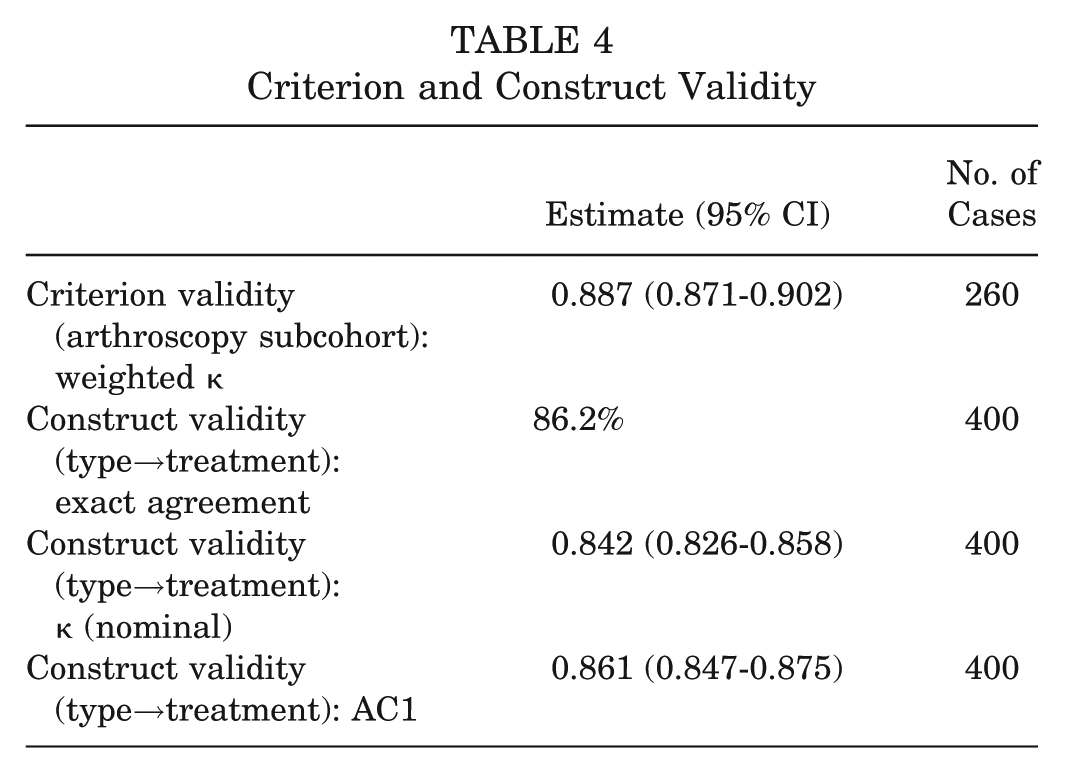
Criterion Validity
In the arthroscopy-referenced subcohort (n = 260), the ordinal weighted agreement between rater-assigned type and the gold-standard type adjudicated by the senior panel was high (weighted κ = 0.887 [95% CI, 0.871-0.902]). Panelists reached independent concordance in 96.2% of cases, with the remaining 3.8% resolved by a consensus. The most common discrepancies mirrored the interobserver error structure at the type III↔IV boundary.
Construct Validity
Concordance between assigned type and prespecified treatment (morphology→treatment matrix) was also strong, with an exact agreement of 86.2% (κ [nominal] = 0.842 [95% CI, 0.826-0.858]) (AC1 = 0.861 [95% CI, 0.847-0.875]) (Table 4). These results indicated that classification not only is reproducible but also translates coherently into decision-relevant recommendations.
Criterion and Construct Validity
Sensitivity and Robustness
Preplanned sensitivity analyses confirmed the robustness of the findings. When categories were collapsed by relabeling types III to V as “complete,” the Light κ increased to 0.934 (95% CI, 0.925-0.943) and the AC2 to 0.946 (95% CI, 0.938-0.954). Applying alternate weighting with linear rather than quadratic weights yielded a Light κ of 0.887 (95% CI, 0.873-0.901), consistent with the primary results. Leave-one-rater-out analyses demonstrated stable interobserver reliability, with the Light κ ranging from 0.896 to 0.908 (median, 0.902), indicating that no single rater materially influenced the overall agreement. Finally, prevalence and bias indices were small in magnitude and did not account for the high levels of ordinal agreement observed.
Discussion
This multicenter study demonstrated that a concise 5-type morphology-based classification system for RMTs achieved high interobserver ordinal agreement on routine clinical imaging, with a Light κ of 0.902 (95% CI, 0.889-0.914) and a Gwet AC2 of 0.918 (95% CI, 0.906-0.929), thus corroborating robustness. Agreement was stable across prespecified subgroups, medial and lateral compartments, and gap magnitude, without clinically meaningful degradation. The error structure was dominated by adjacent-category (±1) discrepancies, with a predictable boundary at type III↔IV, while nonadjacent misclassifications were uncommon. Intraobserver reliability among 7 experts was excellent (mean weighted Cohen κ = 0.913 [range, 0.882-0.942]), indicating that the operational definitions and 1-page atlas stabilized interpretations on repeat reading. Beyond reliability, the classification system exhibited criterion validity against an arthroscopic reference (weighted κ = 0.887 [95% CI, 0.871-0.902]) and construct validity in the mapping from morphology to standardized management (exact agreement: 86.2%; κ = 0.842; AC1 = 0.861). Taken together, these findings support the classification system's measurement soundness and its clinical coherence.7-9,13
The clinical relevance of a morphology-based classification system lies in its ability to align tear morphology with rational treatment selection. Unlike longitudinal or oblique meniscal tears, radial tears disrupt the circumferential fibers that transmit hoop stress and therefore require a repair strategy that restores continuity along the meniscal ring. Current treatment options include capsular repair (side-to-side stitches), intrameniscal repair, and transosseous reinforcement, each addressing different mechanical deficits. However, the field lacks a consensus regarding when to apply each technique, particularly for complete radial tears with varying degrees of gapping.
The proposed classification system directly addresses this gap by stratifying radial tears according to depth and gap magnitude—parameters that determine whether the lesion behaves as a stable partial-thickness defect (types I-II), a complete but apposed tear amenable to capsular repair (type III), a tear with a gap requiring intrameniscal reinforcement or rip-stop constructs (type IV), or a structurally incompetent lesion in which hoop integrity cannot be restored without transosseous fixation (type V). 8
The importance of this distinction is magnified by the fact that radial tears have highly variable healing potential and biomechanical consequences and that no universally accepted treatment guideline currently exists. Surgeons therefore rely on heterogeneous criteria, such as arthroscopic impression, subjective stability, or surgeon preference, which leads to inconsistent outcomes. A morphology-driven framework provides a common language and a decision-relevant structure that links the severity of structural disruption with the escalating need for mechanical protection (from capsular stitches to reinforced constructs to transosseous repair).
By explicitly mapping tear morphology to the biomechanical demands of each repair strategy, the classification system helps clarify why treatment escalation is necessary in certain morphologies and unnecessary in others. This has immediate implications for standardizing care, improving communication between surgeons and radiologists, designing prospective trials, and ultimately guiding evidence-based treatment recommendations for RMTs.
Prior work on the classification of meniscal tears has been hampered by heterogeneous taxonomies, limited attention to the ordered nature of morphological categories, and frequent reliance on nominal metrics that do not weight the magnitude of disagreement. As expected, when the present dataset was analyzed with the Fleiss κ (nominal), the coefficient was lower (0.538 [95% CI, 0.521-0.554]) than the ordinal estimates, despite high exact agreement. This divergence underscores a known methodological point: for constructs that are intrinsically ordinal, the nominal κ underestimates clinically meaningful agreement by penalizing minor (adjacent) disagreements as harshly as major ones. By specifying quadratic weighting for the Cohen κ and using the Light κ as the primary interobserver endpoint, complemented by the AC2 to mitigate prevalence/bias paradoxes, our study aligns analytic choices with the construct under examination and provides more faithful estimates of reproducibility. The predominance of type III↔IV disagreements also mirrors the biological continuum between complete tears with minimal versus small visible gapping, an area where subtle imaging differences and load-dependent behavior can blur categorical lines.16,17,24,26,29
Ultimately, 3 practical implications emerge. First, the atlas and ordered criteria enabled standardized reporting that is both succinct and actionable, improving communication between radiology and surgery. Second, the morphology→treatment decision pathway demonstrated high concordance, supporting its use to calibrate therapeutic selection (from observation/debridement in stable partial lesions to reduction-protected, rip-stop–reinforced repair, with or without transosseous protection, as gapping and instability increase). Third, the combination of high reliability and explicit therapeutic anchoring provides a uniform stratification scheme for meta-analyses, prospective registries, and clinical trials that compare techniques within and across RMT subtypes. The observed ±1-category agreement of 96.8% is particularly relevant for decision support in which small categorical offsets are unlikely to change the recommended management tier.2,3,20,22
This study has several strengths. It is multicenter and includes a broad panel of experienced knee surgeons (interobserver) plus a focused expert panel (intraobserver), which enhances the generalizability of the measurement properties. The design was GRRAS compliant, preregistered, and powered for narrow CIs, with bootstrap procedures that preserve category prevalence. Analytically, we prioritized ordinal reliability metrics (Light κ, Gwet AC2) that reflect the construct while transparently reporting the nominal κ as a legacy sensitivity measure. Methodologically, the 1-page atlas and decision tree functioned as shared anchors, reducing interpretive drift without providing outcome feedback that could inflate agreement spuriously. Finally, the inclusion of both criterion (arthroscopy referenced) and construct validity addresses not only “can raters agree?” but also “does the system map to what we do?”, which is central for clinical adoption.5,11,23,25,35,36
Limitations
Several limitations merit consideration. First, despite efforts to balance categories, any fixed case bank is susceptible to spectrum effects. Real-world prevalence varies across centers and indications, which can shift marginal distributions and slightly influence chance-corrected indices. Second, criterion validity was partial (arthroscopy available in 65.0%), introducing potential verification bias. However, the referenced subcohort was prespecified and large, and findings paralleled full interobserver analysis. Third, while raters were blinded and received no corrective feedback, exposure to the atlas may produce a small training effect that improves agreement relative to unaided practice; from an implementation standpoint, this is a strength (it is exactly how the system would be used), but it may overestimate reproducibility absent standardized anchors. Fourth, our operationalization of gap thresholds (≤3 vs >3 mm) is imaging based and may be modulated by knee positioning or sequence parameters. Nonetheless, the stability of subgroup estimates suggests that this did not materially bias conclusions. Finally, although nonadjacent misclassifications were rare, the principal boundary at type III↔IV indicates a gray zone that could benefit from additional imaging cues (eg, standardized 3D sequences) or intraoperative calibration.1,18,21,32,33
Future research should address external validation in distinct practice environments and with naturalistic prevalence to confirm the transportability of the coefficients. Prospective studies should link the 5 types to patient-reported outcomes, cartilage health, and reoperations to examine prognostic validity and to refine treatment thresholds, particularly around the type III↔IV boundary. From a methods perspective, expanding the atlas with case-based pitfalls, harmonized MRI acquisition (eg, routine 3D isotropic sequences), and reader calibration modules could further reduce adjacent-category drift. Finally, the classification system lends itself to machine-assisted triage: explainable artificial intelligence tools trained on the ordered criterion could prelabel candidates and highlight features (gap measurement, truncation geometry, vascular zone cues) for the clinician, improving efficiency while preserving decision authority with the surgical team.4,6,30
Conclusion
This 5-type classification system demonstrated high reproducibility (ordinal κ≈ 0.90) and clinical validity, providing a practical framework for standardized reporting and treatment selection and a defensible stratification scheme for future trials and meta-analyses.
Supplemental Material
sj-docx-1-ajs-10.1177_03635465261453085 – Supplemental material for Reliability and Clinical Validity of a Morphology-Based Classification System for Radial Meniscal Tears: A Multicenter Observer Study
Supplemental material, sj-docx-1-ajs-10.1177_03635465261453085 for Reliability and Clinical Validity of a Morphology-Based Classification System for Radial Meniscal Tears: A Multicenter Observer Study by Horacio Rivarola, Jorge Chahla, Francisco Endara Urresta, Jakob Ackermann and Bautista Rivarola in The American Journal of Sports Medicine
Footnotes
Submitted October 12, 2025; accepted April 27, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval was obtained from Department of Orthopaedics and Traumatology, Austral University Hospital, Buenos Aires, Argentina. (CIE-2024-0437).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.