
Abstract
Background:
Labral reconstruction has become an essential technique for treating irreparable acetabular labral pathology. While both segmental and circumferential reconstruction techniques are utilized, it remains unclear whether one provides superior clinical outcomes.
Purpose:
To compare patient-reported outcomes, complications, and reoperation rates between segmental and circumferential labral reconstruction.
Study Design:
Meta-analysis.
Methods:
A systematic review of the PubMed, Embase, and Scopus databases was performed in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines on February 2, 2025. Studies were included if they reported clinical outcomes after arthroscopic hip labral reconstruction using either segmental or circumferential techniques. Data were extracted on patient characteristics, surgical details, patient-reported outcome measures, complications, revision arthroscopy, and conversion to total hip arthroplasty (THA). Meta-analyses were performed using random-effects models, and heterogeneity was assessed using the I2 statistic.
Results:
A total of 28 studies consisting of 1817 hips were included, with 1086 undergoing segmental and 731 undergoing circumferential reconstruction. Patient characteristics were similar between groups, except for a lower proportion of women in the segmental cohort than circumferential cohort (44.6% vs 73.2%; P < .001). Both techniques resulted in significant improvements in all patient-reported outcomes, including the Harris Hip Score, Hip Outcome Score–Activities of Daily Living, Hip Outcome Score–Sports, International Hip Outcome Tool–12 score, Short Form–12 score, and visual analog scale pain score, with no significant differences between groups (all P > .05). Complication rates and revision rates were comparable (P = .05 and P = .06, respectively). However, circumferential reconstruction was associated with a significantly lower conversion to THA compared with segmental reconstruction (P = .01).
Conclusion:
Both segmental and circumferential labral reconstruction techniques provide significant and comparable improvements in functional outcomes and pain. Circumferential reconstruction was associated with a lower pooled rate of conversion to THA; however, causality cannot be inferred given the heterogeneity, nonrandomized design, and differences in follow-up duration between studies.
The acetabular labrum is a fibrocartilaginous structure that lines the acetabular rim and contributes to hip joint stability. The labrum decreases stress by increasing contact area between the femoral head and acetabulum.5,14 Biomechanical analyses have shown that when placed under distraction and translation forces, the labrum resists femoral head displacement, further contributing to stability.5,23 Additionally, the labrum preserves negative intra-articular pressure by maintaining a suction seal. This aids in lubrication, load distribution, and stability against distraction of the hip joint.5,66 Once considered an uncommon injury, improvements in magnetic resonance imaging and arthroscopic procedures have resulted in a dramatic increase in the diagnoses of labral tears over the last 20 years.43,55
Recent literature has demonstrated that surgical reattachment of native labral tissue, or labral repair, significantly improves clinical outcomes compared to simple debridement and resection.13,19,20,39,50 However, labral repair requires adequate quality of the native tissue, and it may not be a viable technique when treating an irreparable labrum. When damage is severe, a native labrum may be considered irreparable and not suitable for repair. Although imprecisely defined, factors including high complexity of labral tear, degeneration, calcification, bruising, and hypoplasia often result in tissue that cannot be anchored back to the acetabular rim. In these instances, an alternative treatment is labral reconstruction. First described by Sierra and Trousdale in 2009, 53 a labral reconstruction involves removing damaged native labrum and replacing it with graft tissue. There has been a marked increase in the use of labral reconstruction to treat patients with severely damaged or deficient labra over the last decade. 7 Labral reconstruction appears to be a promising procedure, as recent studies have reported comparable short- to midterm outcomes of labral repair.3,4,11,16,47,57,64 Of note, a 2023 systematic review of 4 studies with a minimum 5-year follow-up demonstrated improved patient-reported outcomes, suggesting long-term durable results of labral reconstruction. 9
Although current literature continues to support the efficacy of labral reconstruction, uncertainty remains regarding which surgical technique yields the most favorable outcomes, as selection is influenced by both the integrity of the native labrum and the extent of labral pathology. The 2 broad variations of labral reconstruction are described as segmental and circumferential. 49 In a segmental reconstruction, only a severely damaged portion of the native labrum is resected and reconstructed with a graft. In a circumferential reconstruction, the entire native labrum is decorticated and debrided from the most anterior to the most posterior aspect of the transverse acetabular ligament and is fully reconstructed with graft tissue. 30
Conventional wisdom has dictated that in the presence of an irreparably damaged labrum and compromised chondrolabral junction, segmental reconstruction is the preferred technique if any healthy native labrum remains, while circumferential reconstruction should be reserved for patients with a complete defect of the labrum.30,45 Other factors such as biomechanical considerations, operative time, and implant cost also play a role in determining the appropriate technique.25,51 However, there is no clear evidence demonstrating the superiority of either technique. Previous systematic reviews have reported no significant differences in short- and midterm outcomes between segmental and circumferential reconstruction techniques.28,33 However, since those publications, additional comparative cohorts have been reported, including studies with longer follow-up and expanded circumferential reconstruction series. Furthermore, pooled survivorship data and conversion to total hip arthroplasty (THA) have not been comprehensively reanalyzed with inclusion of these newer cohorts. Therefore, the purpose of this study was to provide an updated systematic review and meta-analysis comparing segmental and circumferential labral reconstruction techniques with respect to patient-reported outcomes, complication rates, revision arthroscopy, and conversion to THA.
Methods
Search Strategy
A systematic literature search was performed across the PubMed, Embase, and Scopus databases in accordance with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. The search was conducted on February 2, 2025, using the Boolean string “hip AND (labral[title] OR labrum[title]) AND reconstruction[title].” No filters were applied to maximize sensitivity, and references of included studies were reviewed to ensure no relevant studies were missed. The aim was to identify original studies reporting outcomes of arthroscopic labral reconstruction of the hip. Articles were screened independently by 3 reviewers (M.R., S.S., M.K.), and conflicts were resolved by consensus. Inclusion criteria required studies to report clinical outcomes after arthroscopic labral reconstruction and to specify the reconstruction technique as either segmental or circumferential. Studies were excluded if they were not primary outcome studies; were review articles, meta-analyses, or case reports; or had <5 patients. Additional exclusions included mean follow-up <1 year, nonarthroscopic techniques, or unclear documentation of segmental or circumferential reconstruction technique. The selection process is depicted in Figure 1.
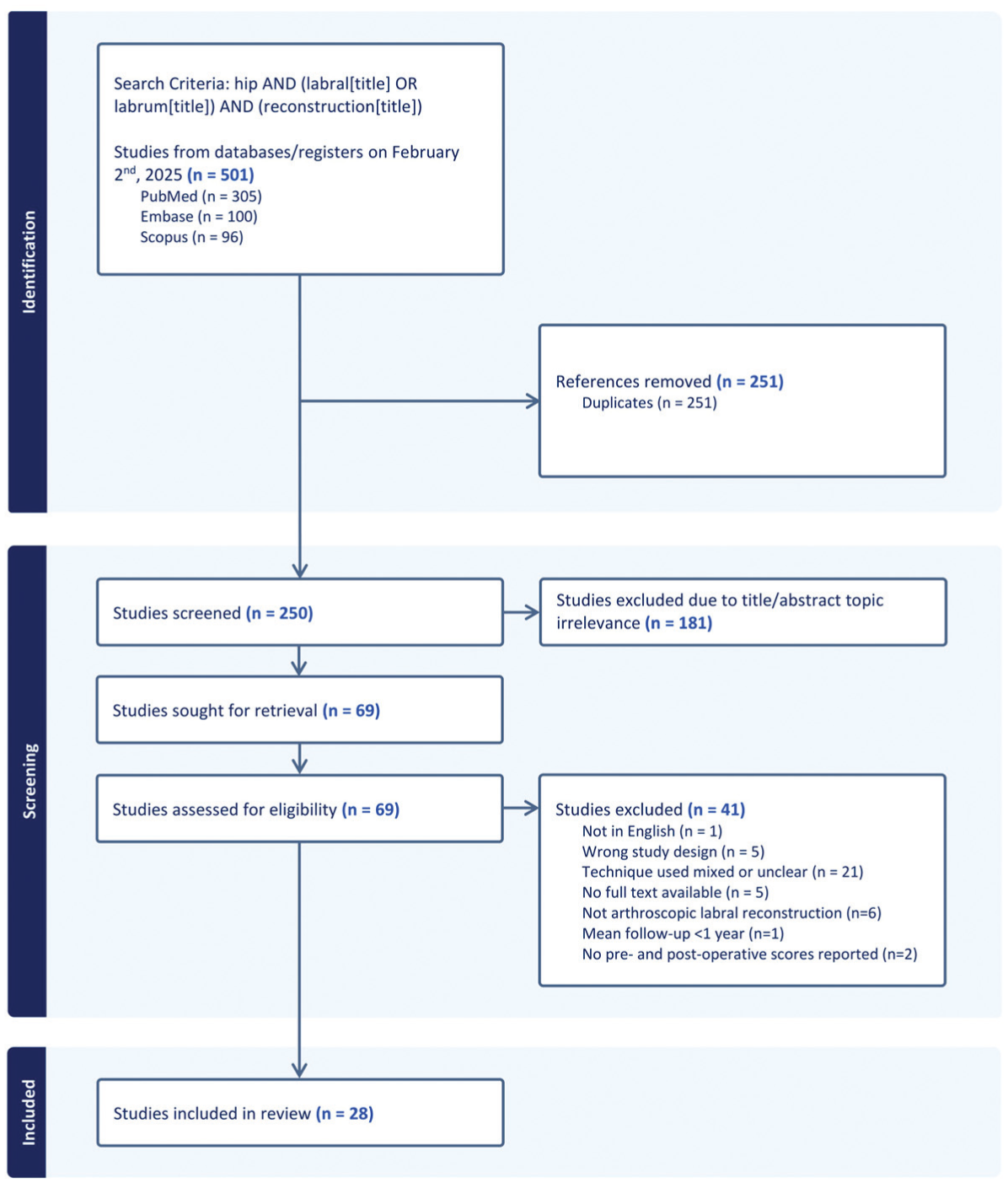
Study selection process.
Data Extraction
Three authors (M.R., S.S. and M.K.) extracted data from all eligible studies. Extracted information included study author, year of publication, level of evidence, study design, country, number of patients and hips, mean age, mean follow-up duration, reconstruction technique (segmental or circumferential), graft material, and the presence of any concomitant arthroscopic procedures. Clinical outcome data included pre- and postoperative values for the modified Harris Hip Score (mHHS), Hip Outcome Score–Activities of Daily Living (HOS-ADL), Hip Outcome Score–Sports subscale (HOS-Sports), International Hip Outcome Tool–12 (iHOT-12), visual analog scale (VAS) for pain, and Short Form–12 (SF-12) Physical and Mental component scores. Additionally, complication rates, revision arthroscopy rates, and conversion to THA were recorded. All outcome measures were collected and analyzed using the preoperative time point and latest follow-up time point. Data for studies that reported outcomes by technique were stratified accordingly.
Risk of Bias
Methodological quality of included studies was assessed using the Methodological Index for Non-Randomized Studies (MINORS) criteria 54 by 2 authors (M.Y. and M.K.), with disagreements resolved by consensus. Noncomparative studies were evaluated using items 1 to 8 (maximum score: 16), while comparative studies were assessed using all 12 items (maximum score: 24). Each domain was scored from 0 to 2, with higher scores indicating better methodological quality. This risk of bias quality assessment was performed to provide a descriptive evaluation of relevant hip labral reconstruction study rigor in the existing literature rather than to exclude studies from analysis.
Statistical Analysis
Statistical analysis was performed using RStudio (Version 2023.09.0+473; Posit) with the metafor and tidyverse packages. Continuous variables such as age and follow-up are summarized using weighted means to account for differences in sample size. Pooled estimates for complication, revision, and conversion rates were calculated using random-effects meta-analysis, allowing for clinical and methodological heterogeneity across studies. Heterogeneity was assessed using the I 2 statistic and interpreted using standard thresholds: low (0%-40%), moderate (30%-60%), and high (75%-100%). Where outcome data were insufficient or inconsistently reported, those measures were excluded from meta-analysis. Subgroup analysis was conducted to compare outcomes between segmental and circumferential reconstruction techniques.
Results
Included Study Characteristics and Risk of Bias
The literature search and screening process are outlined in Figure 1. A total of 28 studies met all inclusion criteria. # Of these, 18 studies reported on segmental labral reconstruction and 11 studies on circumferential reconstruction. Most studies were conducted in the United States, with a range of study designs including retrospective cohorts, case series, and case studies (level of evidence, 3 and 4). Full details on study design, sample sizes, follow-up duration, graft type, and reconstruction technique are provided in Table 1.
Included Studies on Labral Reconstruction a
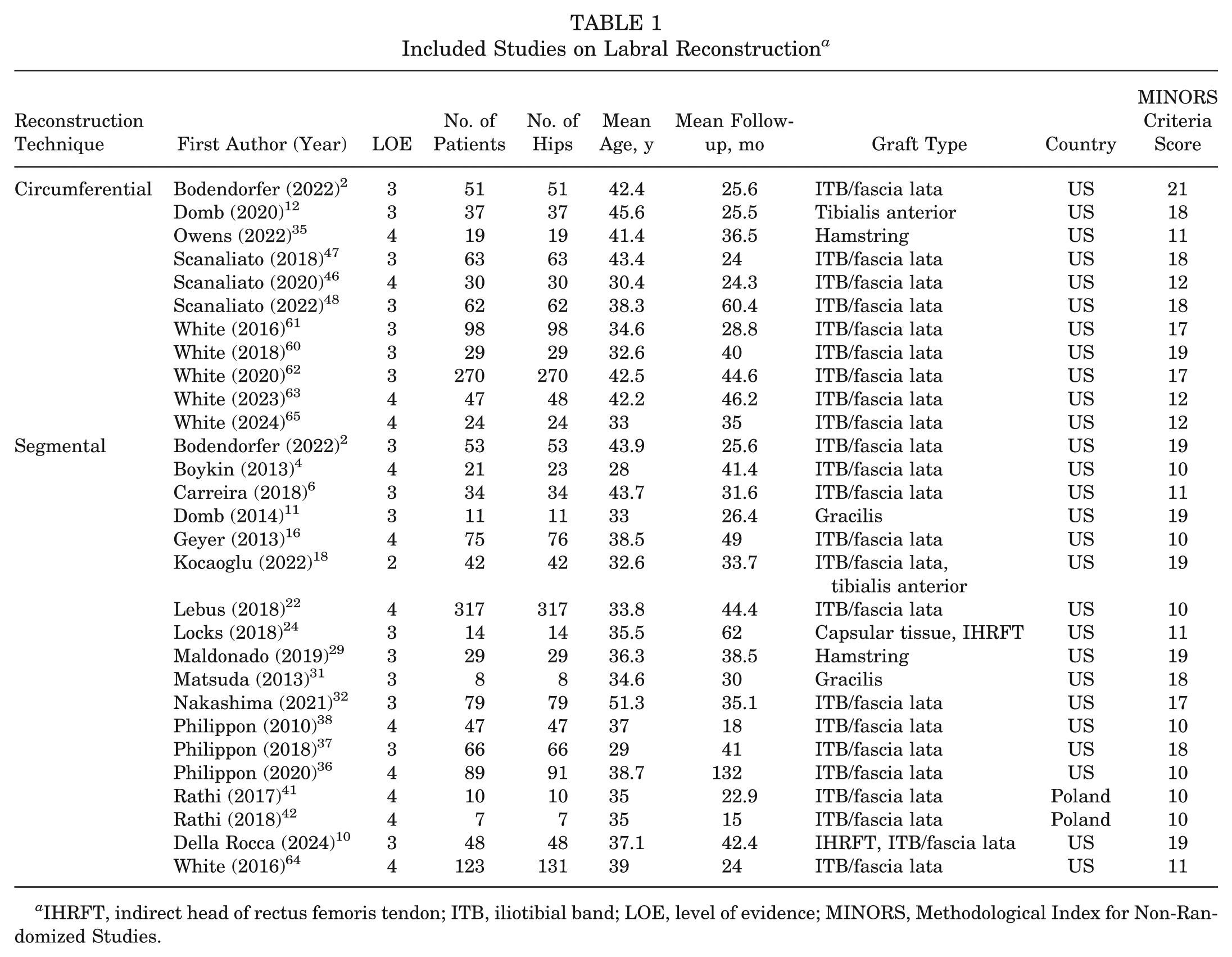
IHRFT, indirect head of rectus femoris tendon; ITB, iliotibial band; LOE, level of evidence; MINORS, Methodological Index for Non-Randomized Studies.
Regarding nonrandomized study risk of bias, MINORS assessment demonstrated overall moderate methodological quality (mean MINORS score, 14.5 of 24 across included studies), as summarized in Table 1. Noncomparative studies generally achieved lower scores, primarily due to the absence of control groups and lack of prospective study design, while comparative studies demonstrated higher scores reflecting more robust methodology. Common limitations across studies included lack of blinded outcome assessment, absence of prospective sample size calculation, and incomplete reporting of follow-up. Detailed MINORS scoring for each study is provided in the Appendix (available in the online version of this article).
Patient Characteristics
In total, 1817 hips were included, with 1086 hips (59.8%) undergoing segmental reconstruction and 731 hips (40.2%) undergoing circumferential reconstruction. Patient characteristics for each cohort are summarized in Table 2. The mean age was slightly lower in the segmental group (37.2 ± 5.2 years) compared to the circumferential group (40.1 ± 5.2 years), although the difference was not statistically significant (P = .27). There was a significant difference in sex distribution: 44.6% of the segmental cohort were female compared to 73.2% in the circumferential cohort (P < .001). The mean body mass index (BMI) was similar between groups (24.6 ± 1.8 kg/m2 for the circumferential group and 24.2 ± 1.7 kg/m2 for the segmental group; P = .79). The mean follow-up duration was longer in the segmental cohort (45.1 ± 24.0 months) than in the circumferential cohort (38.3 ± 11.6 months), although this difference was not statistically significant (P = .42).
Overall Patient Characteristics in Segmental and Circumferential Technique Cohorts a
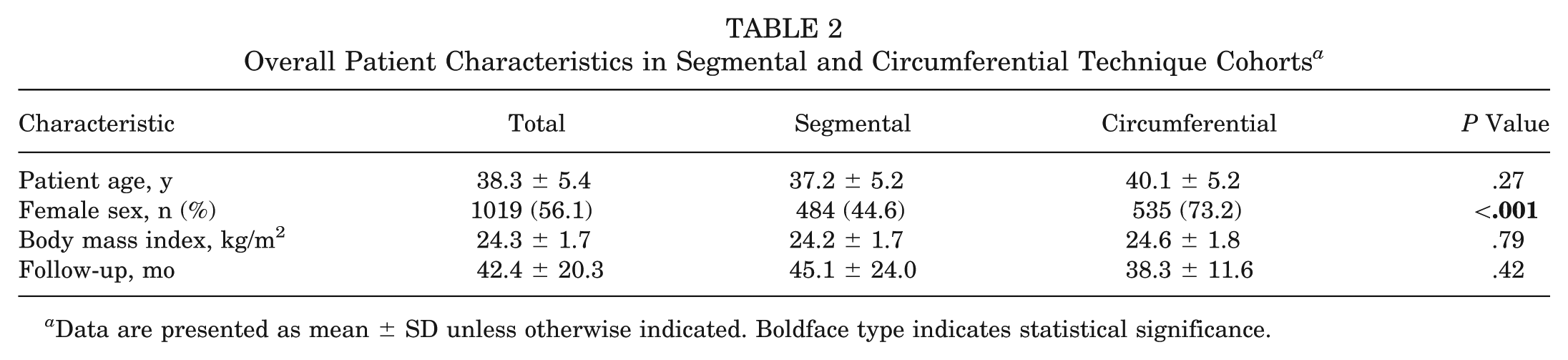
Data are presented as mean ± SD unless otherwise indicated. Boldface type indicates statistical significance.
Concomitant Procedures
A range of concomitant arthroscopic procedures was reported across studies (Table 3). These included femoral osteoplasty, acetabular rim trimming, capsular plication, anterior inferior iliac spine (AIIS) decompression, and periacetabular osteotomy, among others. The frequency and distribution of these additional procedures varied by study and reconstruction technique.
Presence of Additional Techniques Among Included Studies a
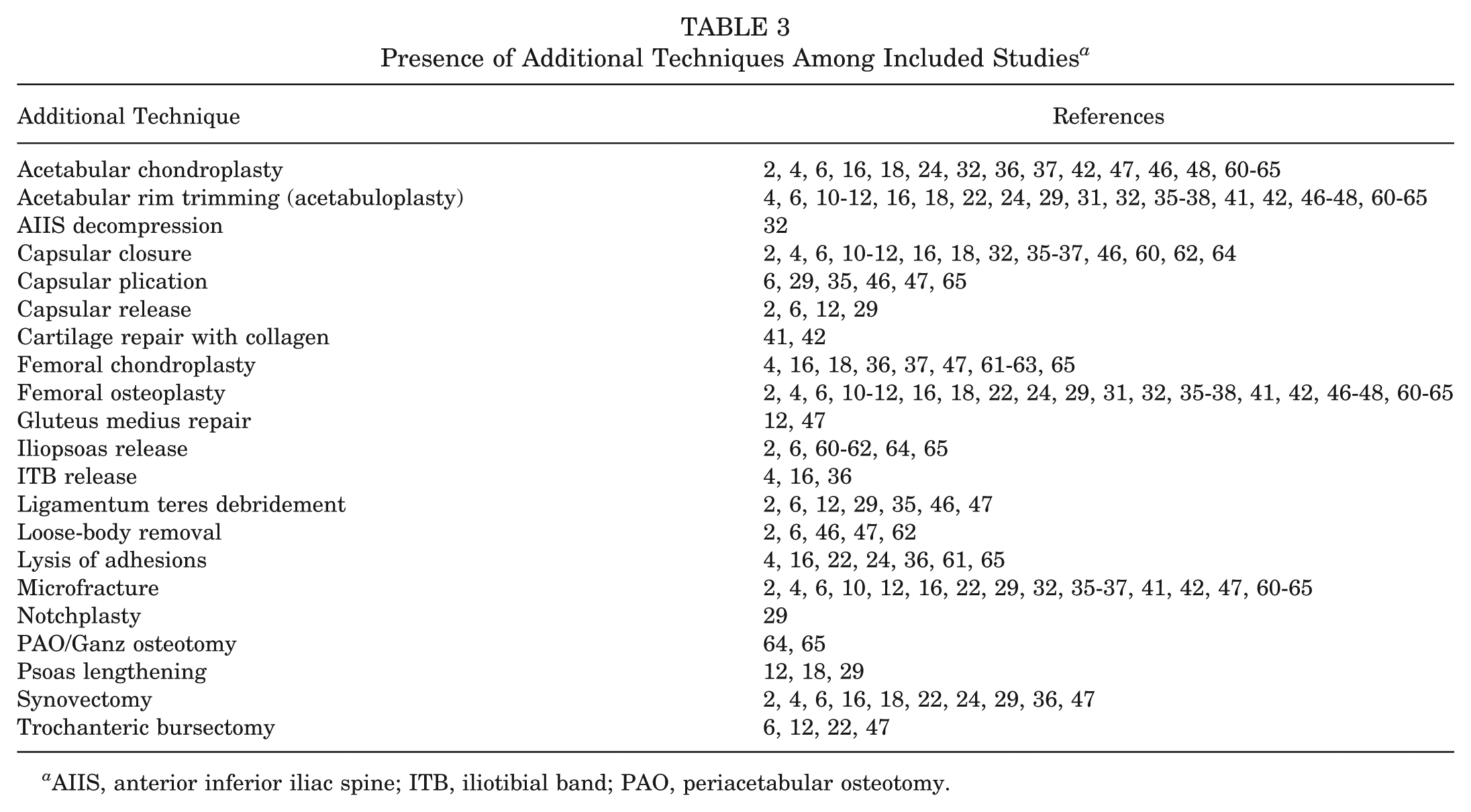
AIIS, anterior inferior iliac spine; ITB, iliotibial band; PAO, periacetabular osteotomy.
Patient-Reported Outcomes
Both segmental and circumferential labral reconstructions were associated with significant postoperative improvements across all patient-reported outcome measures (PROMs). Meta-analysis demonstrated substantial gains in mHHS, HOS-ADL, HOS-Sports, iHOT-12 score, SF-12 Physical and Mental component scores, and VAS pain score (Figures 2 -8). For example, there was a pooled improvement of 26.2 points (95% CI, 23.3 to 29.0; I2 = 84%) in mHHS (Figure 2), 21.3 points (95% CI, 17.6 to 24.9; I2 = 29%) in HOS-ADL (Figure 3), 32.9 points (95% CI, 30.7 to 35.1; I2 = 0%) in HOS-Sports (Figure 4), and 39.6 points (95% CI, 32.2 to 47.1; I2 = 94%) in iHOT-12 score (Figure 5). Similarly, SF-12 Mental scores improved by 3.1 points (95% CI, −0.7 to 6.9; I2 = 62%) (Figure 6), and SF-12 Physical scores increased by 9.2 points (95% CI, 7.1 to 11.2; I2 = 0%) (Figure 7). The VAS pain score decreased significantly, with a pooled reduction of −3.6 points (95% CI, −4.2 to −3.1; I2 = 91%) (Figure 8). Subgroup analyses revealed no statistically significant differences between segmental and circumferential reconstruction for any PROM (all P > .05).
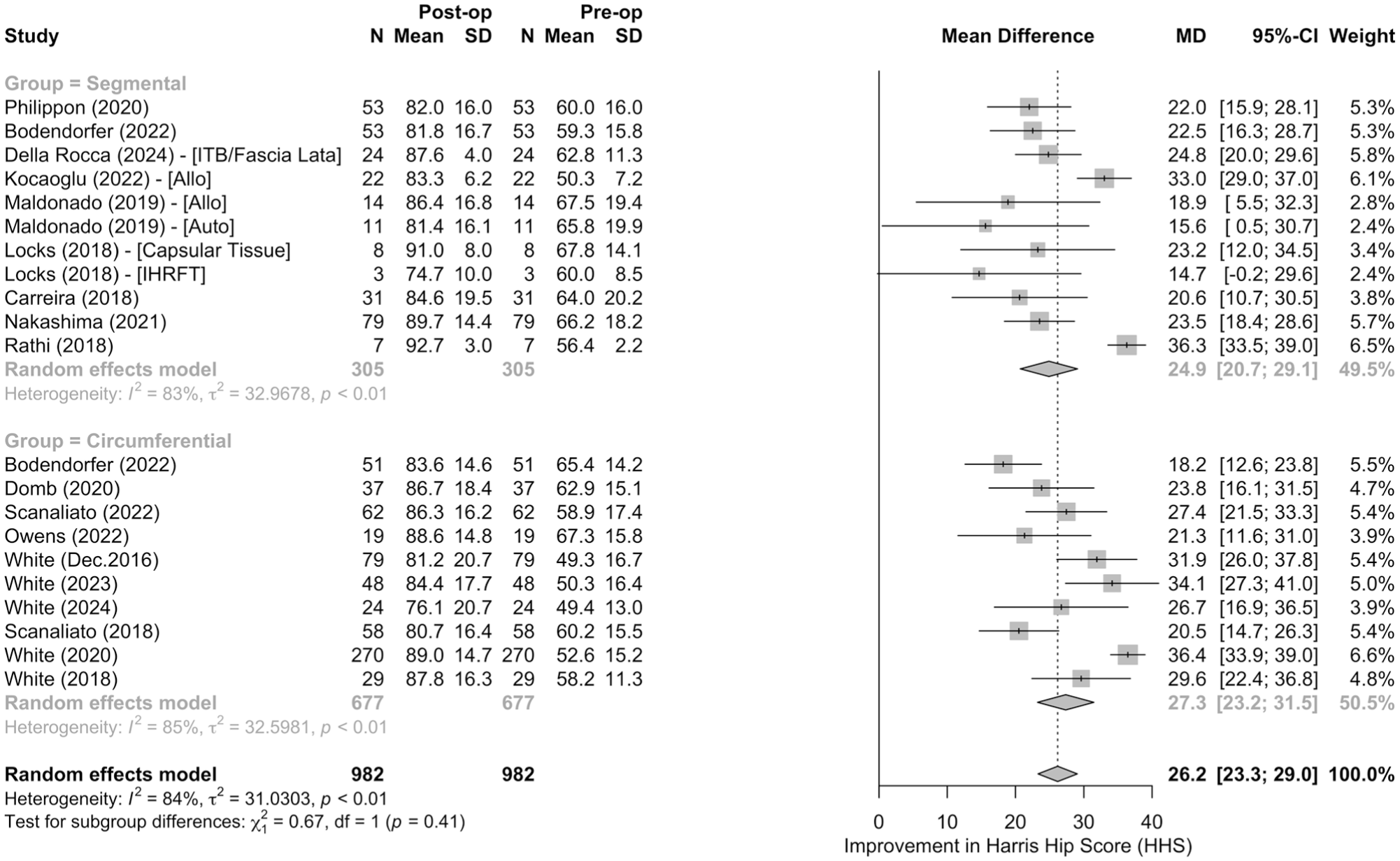
Meta-analysis of improvements in modified Harris Hip Score (mHHS) by reconstruction technique. Allo, allograft; Auto, autograft; ITB, iliotibial band; IHRFT, indirect head of rectus femoris tendon.
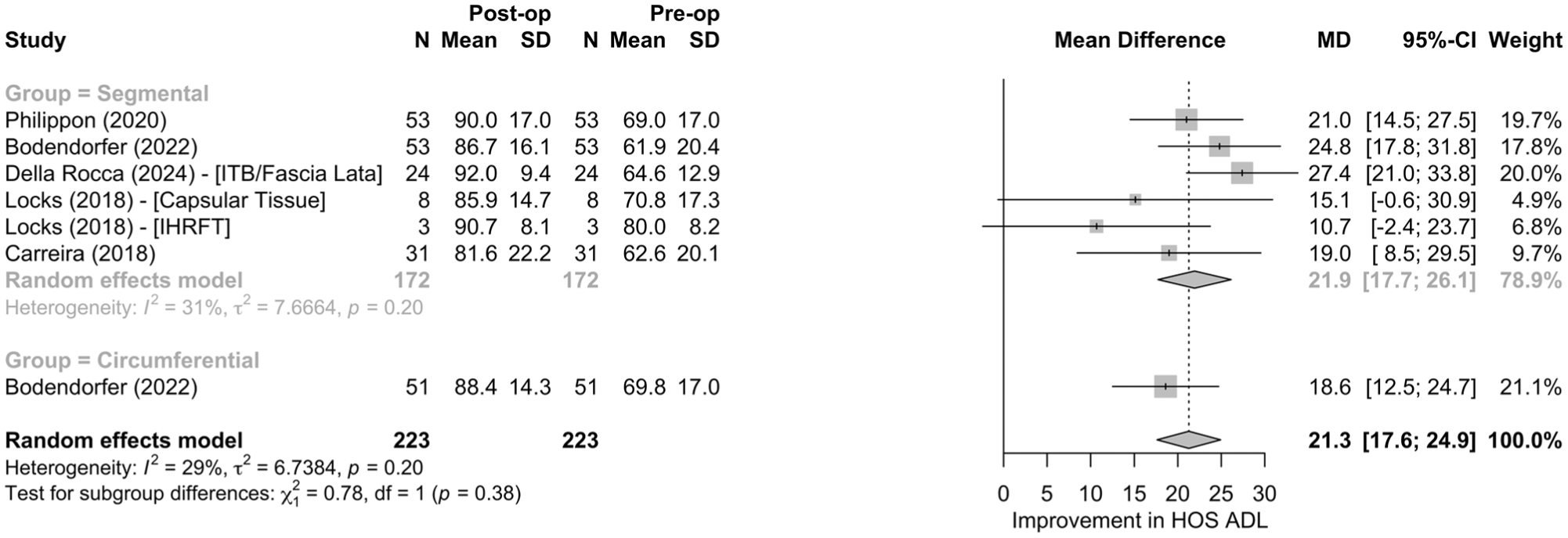
Meta-analysis of improvements in Hip Outcome Score–Activities of Daily Living (HOS ADL) subscale by reconstruction technique. ITB, iliotibial band; IHRFT, indirect head of rectus femoris tendon.
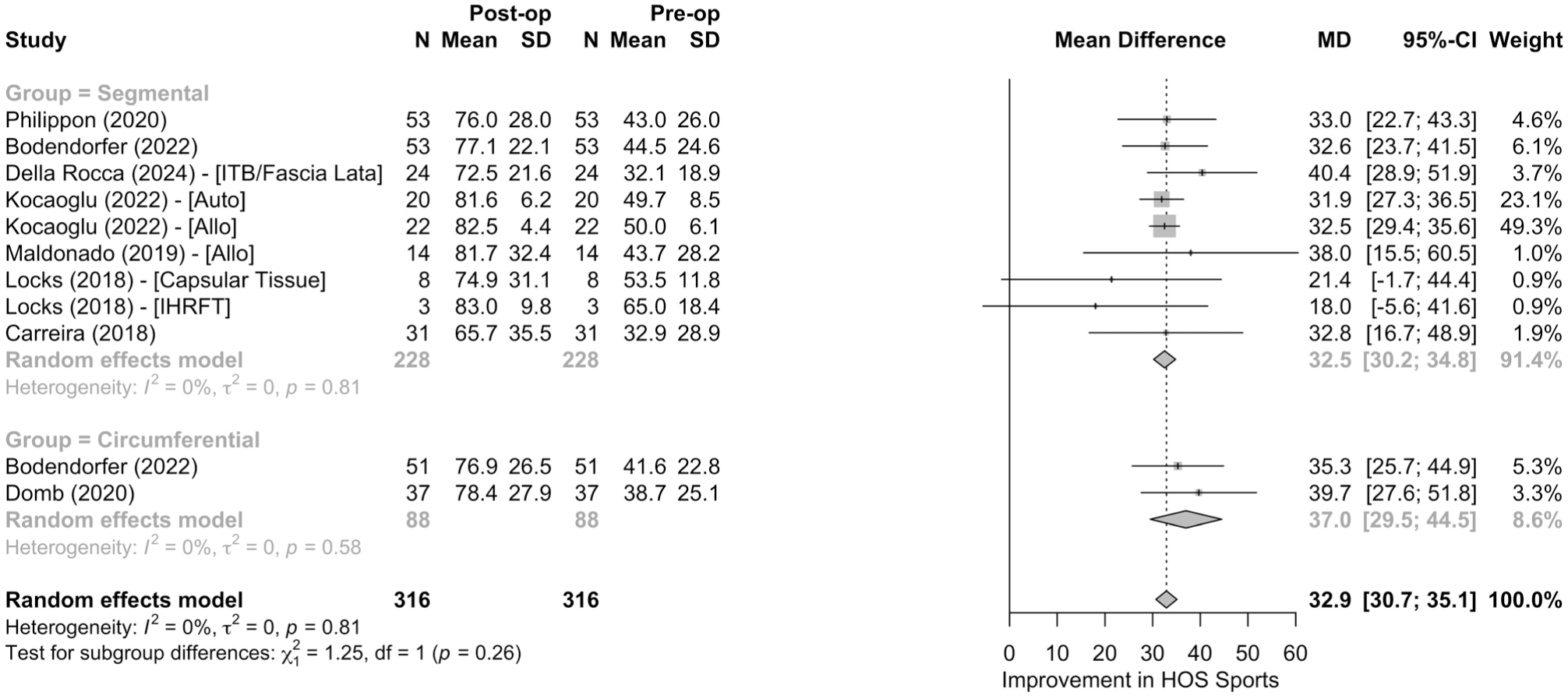
Meta-analysis of improvements in the Hip Outcome Score (HOS)–Sports subscale by reconstruction technique. Allo, allograft; Auto, autograft; ITB, iliotibial band; IHRFT, indirect head of rectus femoris tendon.
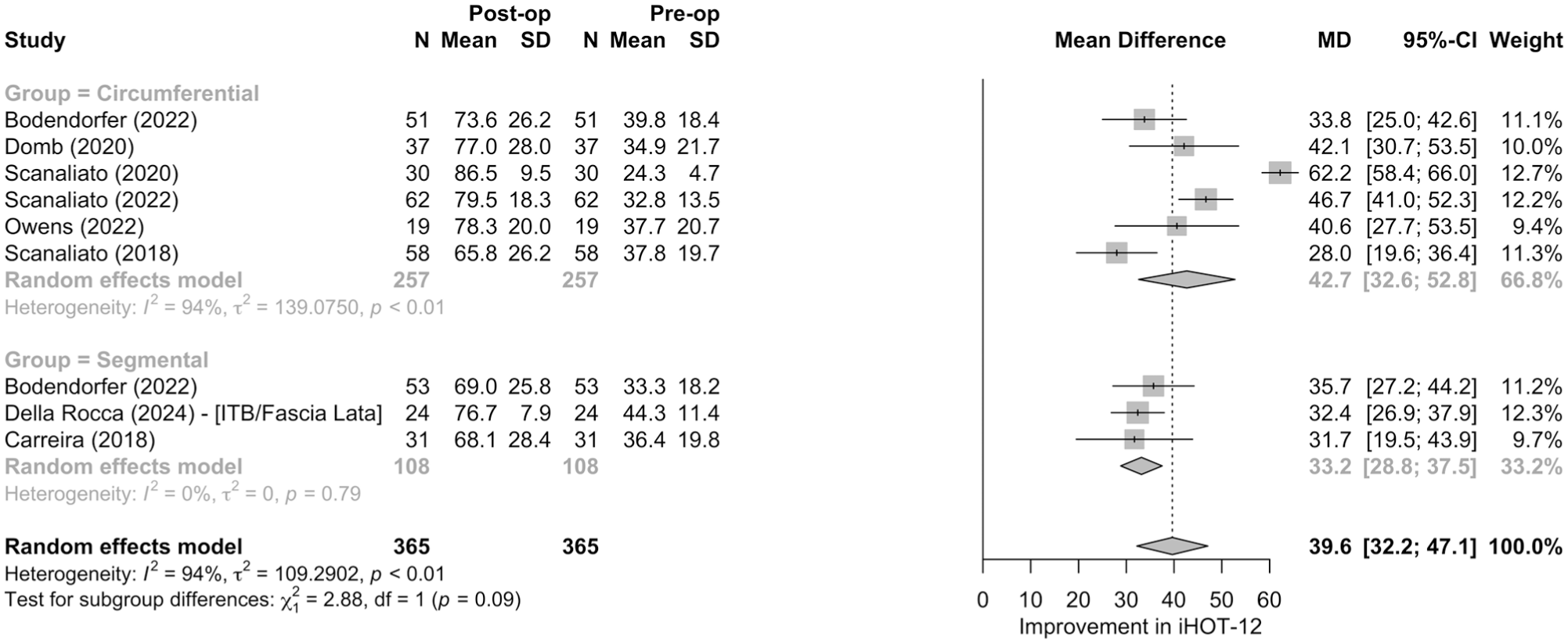
Meta-analysis of improvements in International Hip Outcome Tool (iHOT)–12 score by reconstruction technique. ITB, iliotibial band.
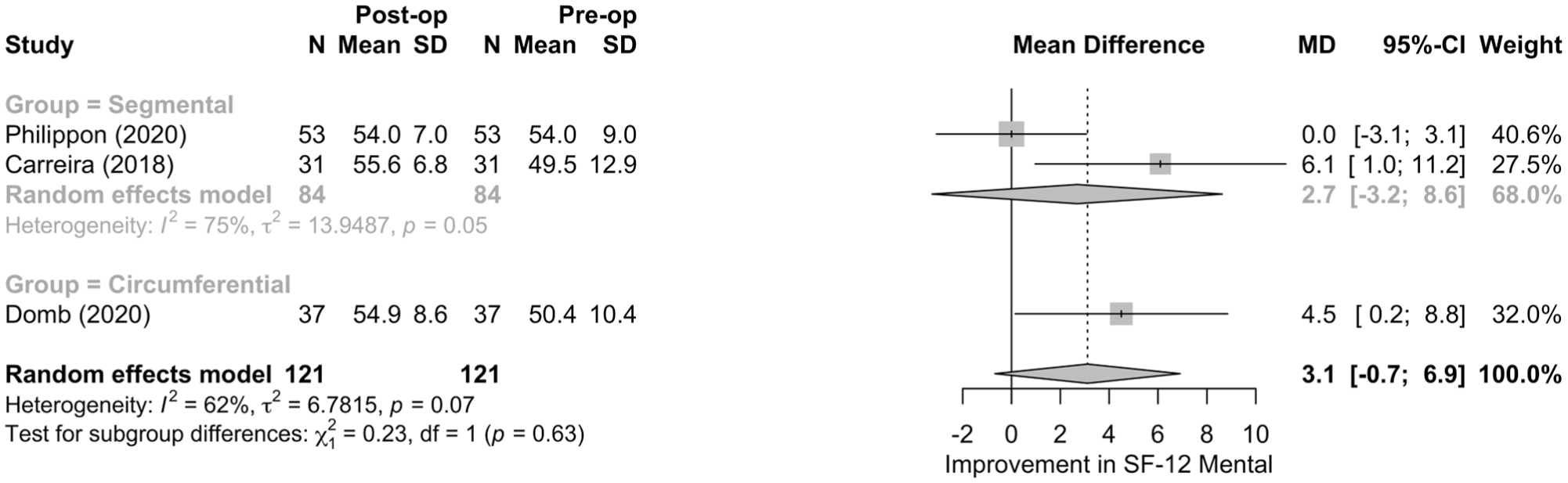
Meta-analysis of improvements in Short Form (SF)–12 Mental scores by reconstruction technique.
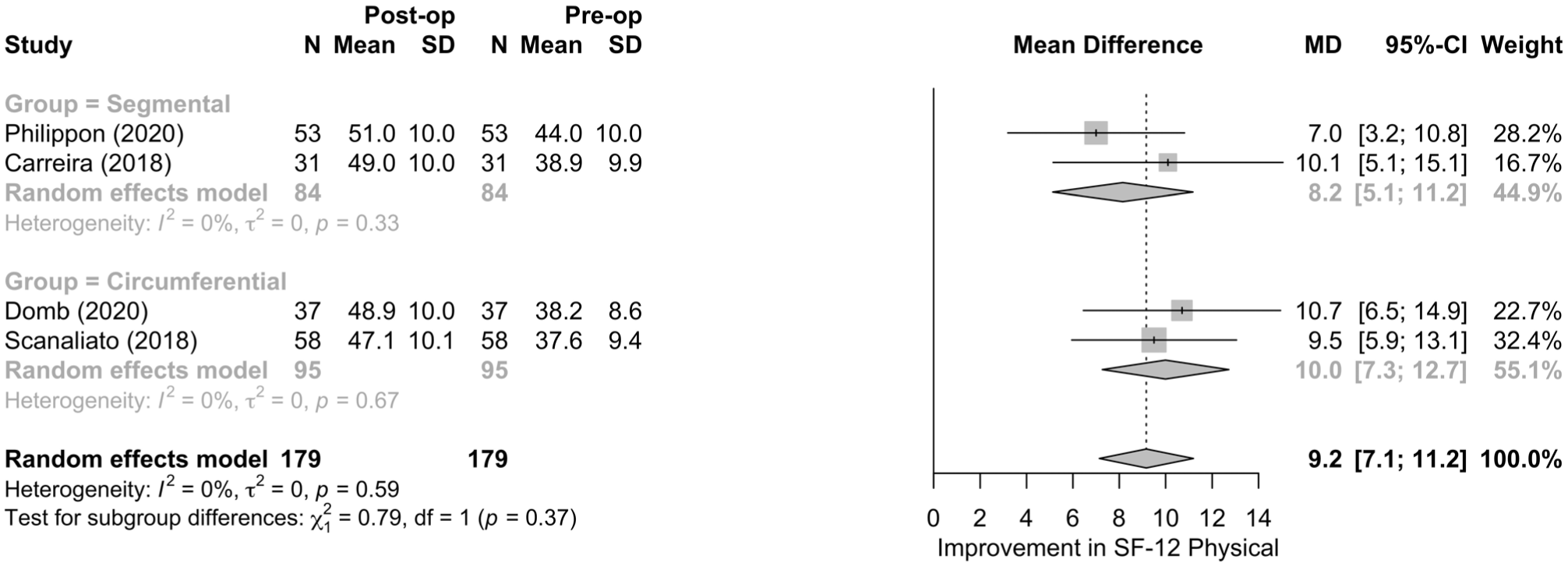
Meta-analysis of improvements the Short Form (SF)–12 Physical scores by reconstruction technique.
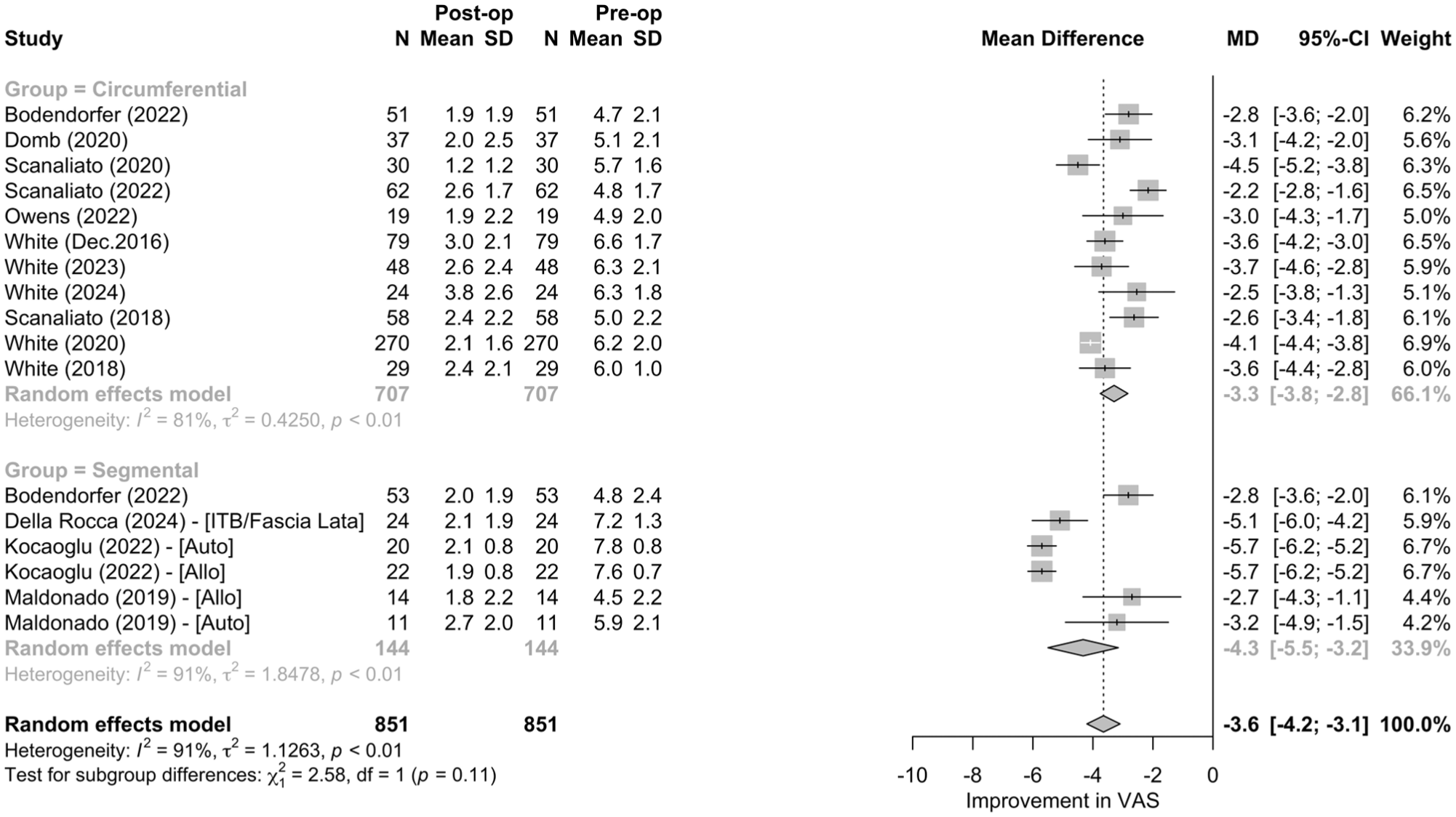
Meta-analysis of improvements in visual analog scale (VAS) pain scores by reconstruction technique. Allo, allograft; Auto, autograft; ITB, iliotibial band.
Complications, Revision Arthroscopy, and Conversion to THA
Outcomes related to survivorship, complications, and further surgical intervention are provided in Table 4. The proportion of patients undergoing revision arthroscopy ranged from 0% to 18.2%, with circumferential techniques generally associated with lower revision rates. Time to revision, when reported, ranged from 12.8 to 36 months. Conversion to THA occurred at variable rates across studies, with the highest conversion rate observed in the segmental reconstruction cohort (24.2%). Time to THA conversion ranged from 15 to 38.4 months. Overall survivorship was high (>90%) in most studies, regardless of technique.
Post–Labral Reconstruction Revision Arthroscopy and Conversion to THA a
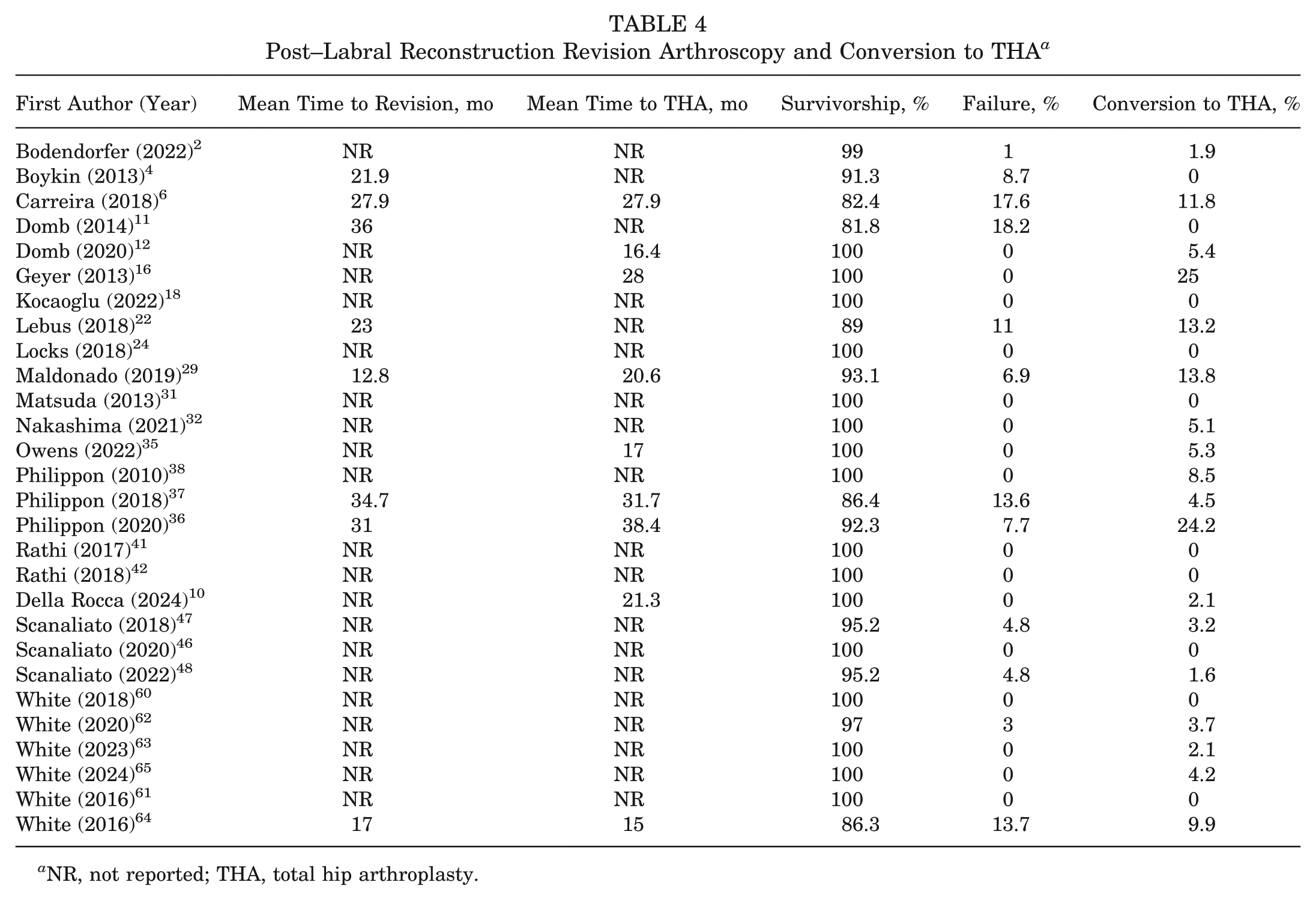
NR, not reported; THA, total hip arthroplasty.
Fifteen unique studies (17 cohorts; 646 hips) reported complication rates. The overall pooled complication rate was 1% (95% CI, 0%-3%) and 2% (95% CI, 0%-6%) for the segmental cohort and <1% (95% CI, 0%-1%) for the circumferential cohort. Heterogeneity was moderate for the segmental group (I2 = 61%, τ2 = 0.013; P < .01) but negligible for the circumferential group (I2 = 0%; τ2 = 0.0; P = .81). There was only a marginally significant subgroup difference (χ2 = 3.97; P = .05) (Figure 9). In addition, 22 unique studies (25 cohorts; 1261 hips) reported post-reconstruction revision arthroscopy rates with an overall pooled revision rate of 3% (95% CI, 1%-5%) (Figure 10). Although the circumferential cohort trended toward fewer revisions, the difference did not reach statistical significance (P = .06).
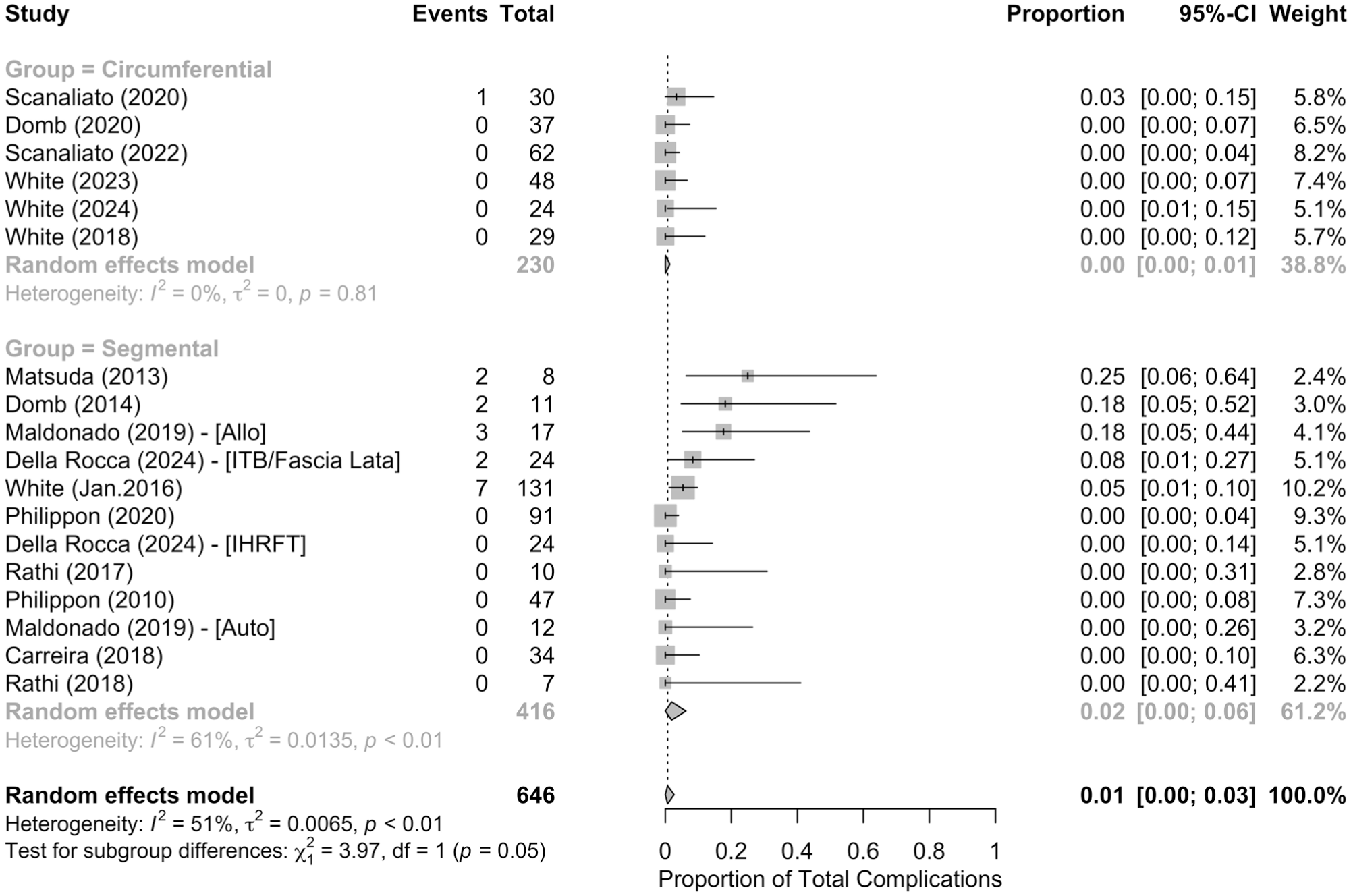
Meta-analysis of proportions for total complications by reconstruction technique. Allo, allograft; Auto, autograft; ITB, iliotibial band; IHRFT, indirect head of rectus femoris tendon.
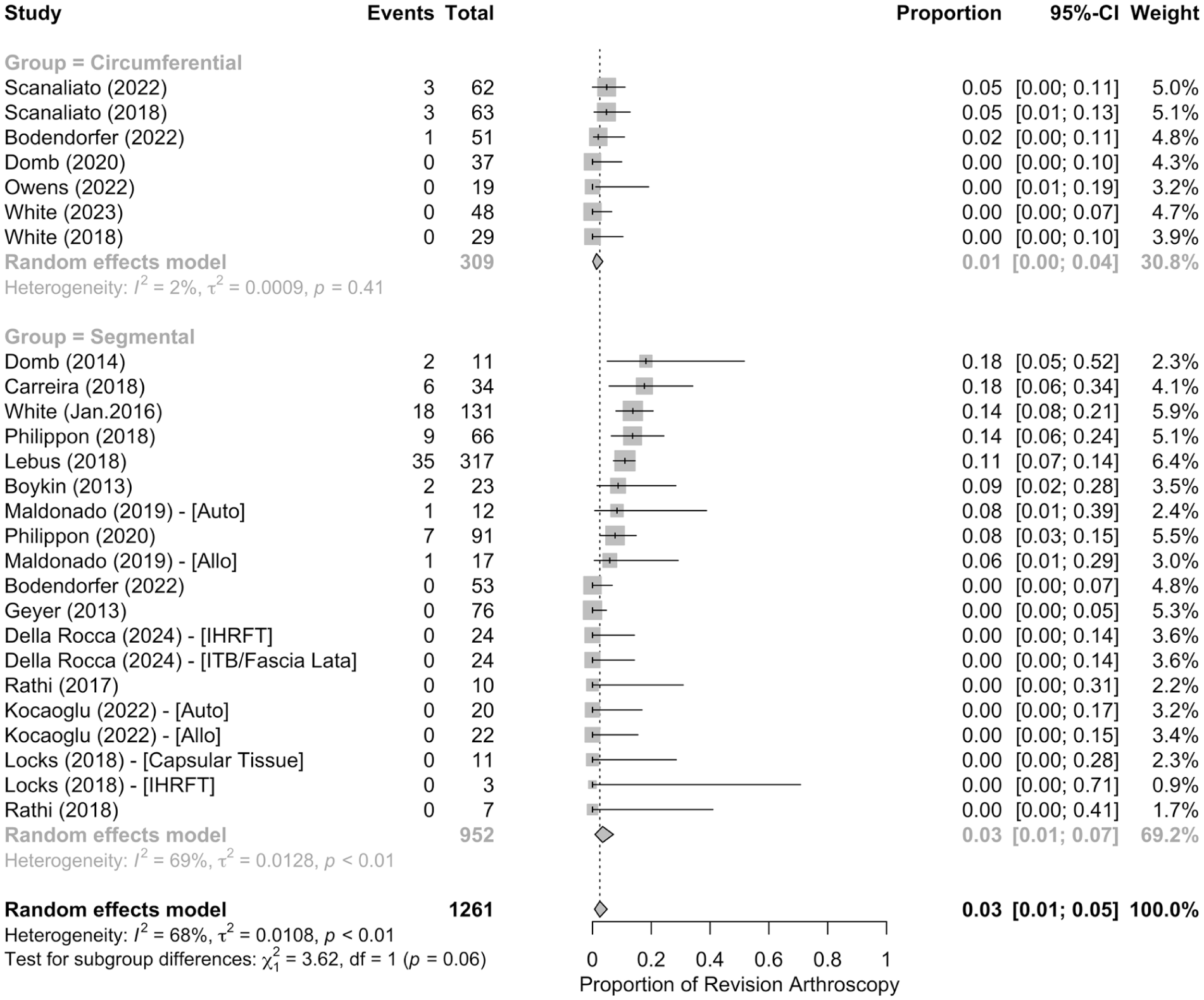
Meta-analysis of proportions for revision arthroscopy by reconstruction technique. Allo, allograft; Auto, autograft; ITB, iliotibial band; IHRFT, indirect head of rectus femoris tendon.
Conversion to THA was reported in 21 unique studies (26 cohorts; 1311 hips) with a pooled conversion rate of 6% (95% CI, 3%-9%) (Figure 11). Segmental reconstructions demonstrated a pooled conversion rate of 7% (95% CI, 4%-12%; I2 = 70%), significantly higher than the circumferential cohort at 3% (95% CI, 1%-5%; I2 = 0%). Subgroup analysis confirmed a statistically significant difference favoring circumferential reconstruction (P = .01), demonstrating an association with lower conversion to THA.
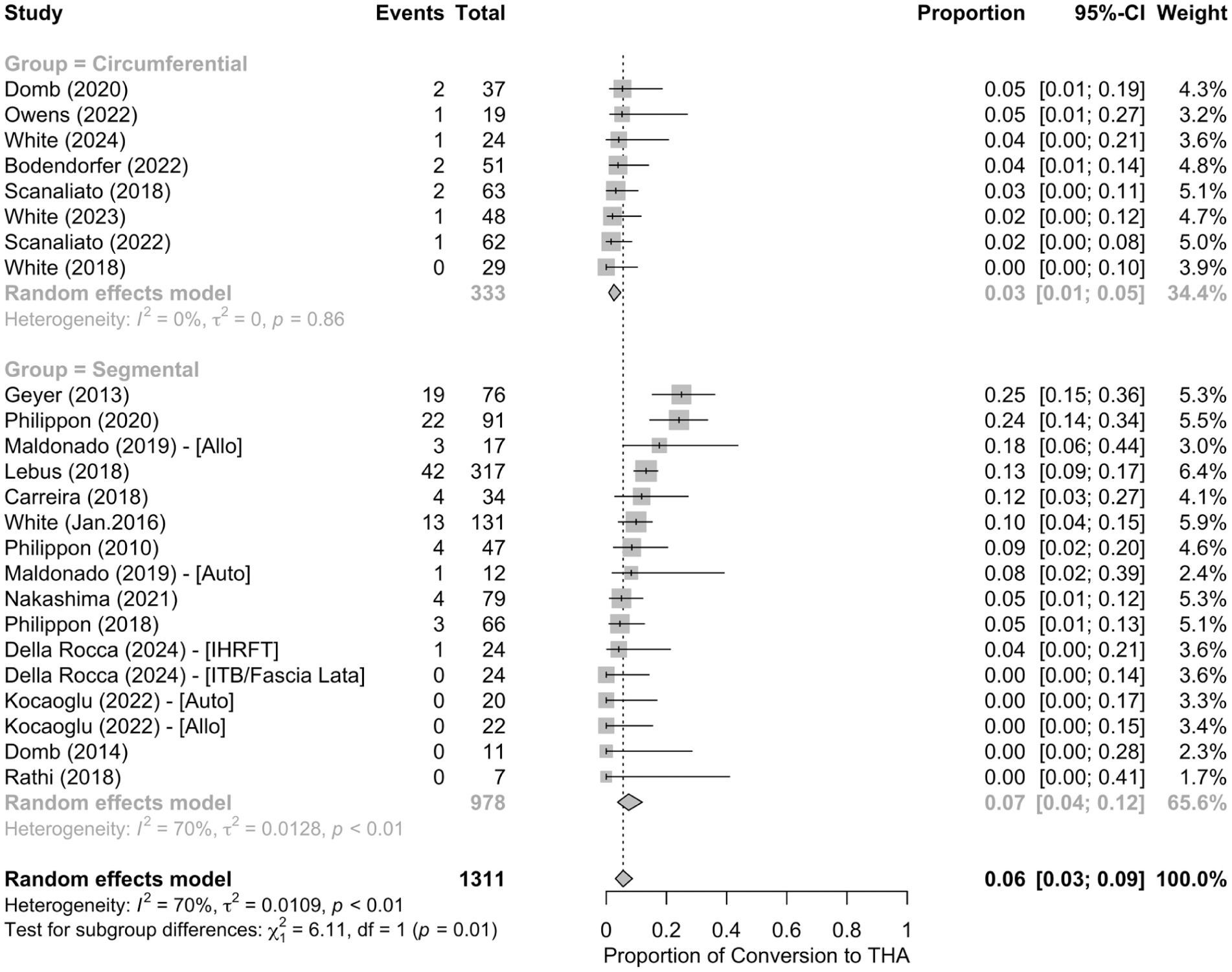
Meta-analysis of proportions for conversion to total hip arthroplasty (THA) by reconstruction technique. Allo, allograft; Auto, autograft; ITB, iliotibial band; IHRFT, indirect head of rectus femoris tendon.
Discussion
This systematic review and meta-analysis of 1817 hips across 28 studies found that both segmental and circumferential labral reconstruction techniques produce substantial improvements in patient-reported outcomes with comparable complication and revision rates. There were 1086 hips in the segmental cohort and 731 hips in the circumferential cohort, with comparable age, BMI, and follow-up time. While functional outcomes were similar between techniques, circumferential reconstruction was associated with a lower pooled rate of conversion to total hip arthroplasty. These findings suggest that both techniques are effective for treating irreparable labral pathology, although differences in survivorship outcomes should be interpreted cautiously given the heterogeneity and nonrandomized nature of the available literature.
Although descriptive characteristics between the segmental and circumferential cohorts were similar for most variables, there was heterogeneity in concomitant procedures. A total of 21 different concomitant procedures were reported across all studies. While some techniques, such as femoral osteoplasty, were performed by all included surgeons, others, such as AIIS decompression, were only explicitly reported in a single study. The variability in concomitant procedures across studies may represent an important confounding factor, as these interventions can independently influence postoperative outcomes and contribute to heterogeneity between cohorts. In addition to surgical indication and concomitant procedures, graft type also varied between studies. More than 90% of reconstructions performed with both techniques utilized iliotibial band/fascia lata for graft material, with minority alternatives including capsular tissue, gracilis tendon, hamstring tendon, indirect head of the rectus femoris tendon, and tibialis anterior muscle. With respect to graft source, a 2018 review found no increased benefit among various types of autograft (ligamentum teres capitis, iliotibial band, gracilis tendon, quadriceps tendon, capsule, IHRFT) or allograft (semitendinosus, peroneus brevis tendon, tensor fascia lata). 1 Although further research is necessary, differences in labral reconstruction outcomes in the present study may reflect factors primarily related to reconstruction technique rather than graft choice.
A notable difference between cohorts was the significantly higher proportion of female patients in the circumferential reconstruction group compared to the segmental cohort (73.2% vs 44.6%; P < .001). This imbalance may represent an important confounding variable, as sex-related anatomic differences and variations in hip pathology may influence both postoperative outcomes and long-term survivorship after hip arthroscopy. Previous literature analyzing patients undergoing arthroscopic labral repair has shown that females generally have smaller alpha angles, increased acetabular version, greater femoral anteversion, and increased prevalence of generalized ligamentous laxity compared to males.17,34 These differences are associated with higher rates of concomitant capsular plications to address underlying microinstability. 27 Additionally, male patients generally demonstrate higher rates of severe acetabular chondral damage due to larger cam-type deformities. 34 Despite these anatomic and pathological differences, previous studies in labral repair cohorts have reported broadly comparable postoperative improvement and survivorship between sexes.8,21,58 However, most of these data are derived from patients undergoing labral repair rather than reconstruction. As labral reconstruction selects for patients with failed repair or more severe primary pathology, it is unclear if the general sex-based anatomic and pathological patterns persist in reconstruction cohorts. Because patient-level data were not available, sensitivity analysis or subgroup evaluation by sex could not be performed. Accordingly, this demographic difference should be considered when interpreting comparative outcomes, particularly the observed difference in conversion to THA between reconstruction techniques.
Comparing outcomes in patients with segmental and circumferential reconstruction, the present review of 28 studies found low overall rates of complications with a marginally significant difference between groups (2% for the segmental cohort vs <1% for the circumferential cohort) that is unlikely to be clinically meaningful. Among patients with segmental reconstruction, there were 5 reported instances of neuropraxia, 2 patients with medial knee pain, 2 cases of tendonitis, 2 patients developing hematoma, 2 instances of deep vein thrombosis, 1 report of unusual edema, 1 patient with a superficial surgical site infection, and 1 case of other joint pain. Patients treated with circumferential reconstruction had only 1 reported complication, a patient with joint pain limiting recovery. This discrepancy was not statistically significant and may be related to surgeon experience and technique development, as 11 of the segmental complications occurred before 2016, compared to the circumferential complication reported in 2020. Labral reconstruction outcomes tend to improve as surgeons perform more procedures, and development of refined techniques on a novel procedure may also reduce the risk of subsequent complications. 40 Direct comparisons of segmental and circumferential reconstructions performed by the same surgeon after developing proficiency in both procedures may help clarify true complication rates.
Among 81 patients with segmental reconstruction, indication for revision was only listed for 50 procedures. These included 46 adhesion lysis procedures, 1 case of arthritis, 1 report of trochanteric bursitis, 1 procedure requiring periacetabular osteotomy, and 1 patient in pain requiring further reconstruction. Of 7 patients with circumferential reconstruction requiring revision, indication for surgery was only listed for 1 patient. This was a revision due to subsequent labral tearing. While it may appear that pathological postoperative adhesions are related to segmental reconstructions, it is important to highlight that 38 of 46 revisions due to adhesions came from a single study, which may reflect individual procedural differences that are not indicative of the segmental reconstruction technique as a whole. 22 Setting aside the revisions due to adhesions, no clear patterns emerge in terms of complications. The few additional revisions in the segmental reconstruction group are varied and do not reflect pathologies that are easily explained by differences in the surgical technique. Furthermore, it is difficult to draw substantial conclusions without indications for a large proportion of revision procedures. Still, future investigation into specific revisions required after segmental and circumferential reconstructions is warranted due to the observed difference in overall revision rate associated with each labral reconstruction technique.
A significantly larger portion of the segmental reconstruction cohort required subsequent treatment with THA. In total, 116 patients with segmental reconstruction eventually converted to THA compared to 10 patients with circumferential reconstruction, representing 12% and 3% of their respective cohorts. While circumferential reconstructions were associated with lower conversion to THA, differences in follow-up time and mean time to THA among patients with segmental and circumferential reconstruction must be considered. Among segmental labral reconstruction studies, the mean follow-up time was approximately 45 months, while the mean follow-up time of circumferential labral reconstruction was approximately 38 months. Although this is a mean difference of <1 year, patients in the segmental reconstruction group were followed longer and converted to THA later than patients with circumferential reconstruction. Large-cohort long-term studies have reported mean time to THA after any type of labral reconstruction to range from 44.4 to 108 months.22,36 Therefore, further studies comparing conversion to THA after segmental and circumferential labral reconstruction at identical postoperative points are warranted to confirm our study's findings. Additionally, temporal differences between included studies may also contribute to the observed findings, as segmental reconstruction cohorts were more commonly reported in earlier literature, whereas circumferential reconstruction has been described more recently and may reflect evolving surgical techniques and indications. Other uncontrolled factors that may contribute to conversion to THA include surgeon experience and joint space narrowing.37,39 Hip joint space ≤2 mm has widely been accepted in recent literature as a contraindication to labral reconstruction, as studies demonstrated a high conversion rate to THA of 50% at 3 years in this cohort.16,44 Further randomized controlled research is necessary to delineate the impact of patient pathology, follow-up time, and fidelity of follow-up methodology on time to THA after segmental versus circumferential reconstruction.
In addition to surgical complications, the results of patient-reported outcomes were also analyzed. Various PROMs were utilized within individual studies. These included the mHHS (305 segmental, 677 circumferential), HOS-ADL (172 segmental, 51 circumferential), HOS-Sports (228 segmental, 88 circumferential), iHOT-12 score (108 segmental, 257 circumferential), SF-12 Mental score (84 segmental, 37 circumferential), SF-12 Physical score (84 segmental, 95 circumferential), and VAS pain score (144 segmental, 707 circumferential). All these surveys have been statistically validated as effective ways to interpret patient state and improvement after hip arthroscopy.15,52,56 Both groups demonstrated significant improvement in PROMs after labral reconstruction with no significant differences between techniques.
Subgroup analyses revealed no statistically significant differences between segmental and circumferential reconstruction for any PROM (all P > .05); however, substantial heterogeneity was observed for several pooled PROM outcomes, including mHHS (I2 = 84%) and iHOT-12 score (I2 = 94%). This variability likely reflects differences in patient populations, baseline pathology, surgical technique, graft selection, concomitant procedures, postoperative protocol, and duration of follow-up across the included studies. Differences in the structure and domains of PROM instruments may also contribute to variability across studies. Scores such as the mHHS and iHOT-12 score assess multiple functional domains including pain, activity level, and daily function, which may vary substantially across patient populations and follow-up durations. In contrast, outcomes reported by fewer studies or across more homogeneous cohorts may demonstrate lower statistical heterogeneity. Such heterogeneity is common in surgical meta-analyses and should be considered when interpreting pooled estimates, emphasizing that the results represent overall trends across diverse clinical settings rather than definitive comparative effectiveness.
Of technical note, the selection of appropriate surgical technique for a labral reconstruction must account for the unique advantages and disadvantages specific to each procedure. Segmental reconstruction preserves remaining native labral tissue and may require fewer anchors, potentially reducing operative time and cost, but it also creates graft-native anastomosis that may represent a technical challenge.33,51 The circumferential technique has biomechanical benefits that may contribute to improved survivorship. For example, circumferential reconstruction sacrifices all native labral tissue, eliminating mechanically insufficient tissue and possible sources of pain, while exposing the entire acetabular rim for better detection and treatment of concomitant pathologies.30,33 Reconstruction with continuous graft material of uniform width may allow for improved suction seal and pressure mechanics, without theoretical graft–native tissue weak points seen in the segmental technique. 26 Additionally, restoration of hoop fiber strength through continuous graft material may allow for more uniform load distribution around the acetabulum. 59 However, these proposed advantages remain speculative, and the present study was not designed to evaluate mechanistic differences between techniques. Surgical technique selection is strongly influenced by the extent and quality of native labral tissue, and patients undergoing circumferential reconstruction may have more severe baseline pathology, which introduces potential selection bias when comparing outcomes. Although outcomes have demonstrated comparable improvements between techniques, future randomized studies controlling for labral pathology are required to draw more definitive conclusions.
Limitations
While systematic analysis of 28 labral reconstruction studies revealed significantly lower conversion to THA among patients treated with the circumferential technique, there are several limitations with the review. First, there was significant heterogeneity among the included studies. This includes variations in surgeon experience, surgical technique, concomitant procedures, and type of graft tissue used, as well as differences in follow-up duration. Given unavailable patient-level data, many of these variables could not be controlled for. Second, there were no control groups and no patient matching between patients with segmental and circumferential reconstruction. The majority of included studies were retrospective cohort studies or case series, limiting the ability to control for confounding and precluding causal inference. Additionally, temporal differences between studies may confound comparisons, as segmental reconstruction cohorts were more commonly reported in earlier literature, whereas circumferential techniques reflect more recent surgical evolution. Third, there was an imbalance in sex distribution between cohorts, which may have influenced comparative outcomes and represents an important potential confounder that could not be adjusted for in the present analysis. Fourth, there was no standardized definition of complications, failure, revision arthroscopy, or indications for conversion to THA across studies, and PROM usage varied substantially between studies, making direct comparison of patient outcomes difficult. Fifth, although no 2 studies had identical sample sizes, mean follow-up time points, or patient characteristics, it is difficult to ascertain any extent of patient overlap between studies, especially concerning multicenter studies and studies from the same institution; possible patient overlap can influence meta-analysis findings. Additionally, follow-up duration differed between segmental and circumferential cohorts, which is particularly relevant when interpreting conversion to THA and outcomes. Sixth, it is important to note there is no precise definition of indications for hip labral reconstruction; thus, variability in indications for labral repair versus reconstruction, and severity of accompanying articular cartilage damage, joint space narrowing, and other comorbid arthritic changes, may all confound outcomes in the labral reconstruction literature. Seventh, formal assessment of publication bias was not performed, as funnel plot analysis and Egger regression may be unreliable in meta-analyses of proportions and when the number of contributing studies per outcome is limited. Similarly, formal sensitivity analyses were not performed due to inconsistent reporting of subgroup data and the limited number of studies contributing to several outcomes, which would reduce the reliability and interpretability of such analyses. Despite these limitations, the inclusion of 1817 hips provides a robust sample size that is useful for observing trends among patients with arthroscopic labral reconstruction.
Conclusion
Both segmental and circumferential techniques in arthroscopic labral reconstruction result in significant and comparable improvements in patient-reported outcomes and pain relief, with low complication and revision rates. Circumferential reconstruction was associated with a lower pooled rate of conversion to THA at short- and midterm follow-up; however, causality cannot be inferred due to the heterogeneity, nonrandomized study designs, and differences in follow-up duration and baseline characteristics between cohorts. High-quality prospective comparative studies with longer-term follow-up are necessary to determine whether true differences in survivorship exist between techniques.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465261455016 – Supplemental material for Comparative Outcomes of Circumferential Versus Segmental Labral Reconstruction in Hip Arthroscopy: A Systematic Review and Meta-analysis
Supplemental material, sj-pdf-1-ajs-10.1177_03635465261455016 for Comparative Outcomes of Circumferential Versus Segmental Labral Reconstruction in Hip Arthroscopy: A Systematic Review and Meta-analysis by Mark Kurapatti, Matthew Yuro, Brian S. Tao, Matthew D. Ramey, Srivatsan Swaminathan, Jorge Chahla and Robert L. Parisien in The American Journal of Sports Medicine
Footnotes
Submitted October 14, 2025; accepted April 24, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: R.L.P. reported grant/education and hospitality financial or material support from Arthrex; serving as the associate editor of Journal of Cartilage & Joint Preservation; serving on the editorial or governing board of Arthroscopy, Arthroscopy, Sports Medicine and Rehabilitation, and Journal of Sport Rehabilitation; serving on the Council of Delegates and Research Committee of the American Orthopaedic Society for Sports Medicine; serving on the Research Committee, Surgical Skills Committee, International Committee, and Social Media Committee of the Arthroscopy Association of North America; and serving as a committee member for the Eastern Orthopaedic Association, New England Orthopedic Society, and Society of Military Orthopaedic Surgeons.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.