
Abstract
Background:
A prospective, randomized, placebo-controlled trial showed reduced retears after arthroscopic rotator cuff (RC) repair in patients without osteoporosis by a systemic single-dose of zoledronic acid. Distinct micro-ribonucleic acids (miRNAs) related to inflammation, fibrosis, and tendon-to-bone healing are associated with RC injuries.
Purpose:
To investigate the longitudinal effects of a single-dose of zoledronic acid in patients without osteoporosis undergoing arthroscopic RC repair on circulating miRNAs in order to explore the molecular mechanism of this treatment.
Study Design:
Controlled laboratory study.
Methods:
Data were collected in the course of a single-center, prospective, randomized, placebo-controlled, triple-blinded (investigator, surgeon, patient) phase II trial. A total of 80 patients underwent arthroscopic RC repair and were intraoperatively randomized to the zoledronic acid group (n = 40) or the control group (n = 40). Circulating plasma miRNAs were assessed preoperatively, 2 days postoperatively, and 3 months postoperatively using small RNA sequencing and reverse transcription quantitative polymerase chain reaction (RT-qPCR).
Results:
Six miRNAs were selected for validation by RT-qPCR based on small RNA-sequencing analysis. No statistical differences in miRNA plasma levels were observed preoperatively between the 2 study groups. Two days after surgery, plasma levels were significantly lower for miR-140-3p (P = .047) in the zoledronic acid group. In the control group, plasma levels were significantly lower for miR-29a-3p (P < .001), miR-21-5p (P = .036), miR-192-5p (P = .034), and miR-146a-5p (P < .001) 2 days after surgery. Three months after surgery, miRNA plasma levels of the 2 study groups equalized without any significant differences. Gene target analysis identified collagen type I alpha 1 chain, collagen type III alpha 1 chain, vascular endothelial growth factor, insulin-like growth factor 1, and transforming growth factor-β1 as targets of miRNAs impacted by zoledronic acid.
Conclusion:
Longitudinal plasma miRNA expressions suggest a molecular response to zoledronic acid, potentially indicating a reduction of inflammation and fibrosis at the enthesis as well as increased collagen synthesis and vascularization, possibly explaining improved tendon-to-bone healing.
Clinical Relevance:
Zoledronic acid is a safe and easy-to-apply augmentation technique for patients undergoing arthroscopic RC repair.
Registration:
NCT05677152 (ClinicalTrials.gov identifier).
Full-thickness rotator cuff (RC) tears are reported in up to 68% of patients between 50 and 69 years of age.38,50 Such chronic RC tears are associated with degenerative changes like tendon retraction, tendon delamination, fatty muscle infiltration, and muscle atrophy. 44 Furthermore, patients with chronic RC tears commonly have osteoporotic changes in the whole humeral head. 39 If part because of an increased osteoclast density at the footprint of RC repairs, 58 osteoporosis is an independent risk factor that negatively affects RC healing after surgical repair. 4
In order to improve outcomes after RC repair, investigations inhibiting bone resorption were increasingly conducted in recent years.20,27,28,45,46,58 Preclinical studies using a systemic postoperative body weight–dependent bisphosphonate treatment after RC repair showed improved bone microarchitecture in the humeral head as well as increased mechanical tendon strength.20,46,58 Furthermore, administration of a single-dose of zoledronic acid was associated with improved muscle regeneration after RC repair in a rat model mediated by increased myogenic proliferation and differentiation. 45 First clinical trials investigated the effects of bisphosphonates after arthroscopic RC repair in patients with osteoporosis.27,28 In a prospective, randomized, placebo-controlled trial, an intraoperative single-dose of zoledronic acid led to significantly reduced retears after arthroscopic RC repair in patients without osteoporosis at short-term follow-up. 47
Micro-ribonucleic acids (miRNAs) are short, noncoding RNA sequences that play an essential role in gene regulation by sequence-specific posttranscriptional gene silencing, and their circulating levels in serum or plasma are considered informative biomarkers in various settings of musculoskeletal pathologies and regeneration.11,15,16,56 Differential miRNA expressions are associated with bone formation, bone resorption, and bone remodeling, commonly observed after antiosteoporotic treatments.15,23,55 Furthermore, distinct miRNA expressions related to inflammation, fibrosis, and tendon-to-bone healing are associated with RC injuries.17,40
The aim of this study was to longitudinally evaluate circulating plasma miRNAs in patients without osteoporosis undergoing arthroscopic RC repair with a single-dose of zoledronic acid. We hypothesized that a systemic treatment with zoledronic acid would affect circulating plasma miRNAs, possibly influencing tendon-to-bone healing.
Methods
Study Design and Patients
Data from this controlled laboratory study were collected in the course of a single-center, prospective, randomized, placebo-controlled, triple-blinded (investigator, surgeon, patient) phase II trial, registered at ClinicalTrials.gov (NCT05677152). 47 All patients were recruited between September 2022 and January 2025 at the Department for Orthopedics and Trauma Surgery at the Austrian Workers’ Compensation Board (AUVA) Trauma Center Vienna–Meidling, Austria. The study was conducted in accordance with the Helsinki Declaration and was approved and supervised by the local ethics committee of the AUVA (EK-No. 06/22) as well as the Austrian Agency for Health and Food Safety. Written informed consent was given by all patients before any investigational procedures were performed.
Patients without osteoporosis aged between 50 and 70 years with a full-thickness posterosuperior RC tear and a maximum tear size of 3 cm were included in this study. Exclusion criteria were (1) irreparable RC tear, (2) tear of the subscapularis tendon (Lafosse II-V), (3) increased fatty muscle infiltration of the supraspinatus or infraspinatus muscle (Goutallier 3 and 4), (4) glenohumeral osteoarthritis (Hamada 3-5), (5) previous fracture of the affected shoulder, (6) previous surgery of the affected shoulder, (7) previous or persisting septic arthritis of the affected shoulder, (8) known allergy to zoledronic acid or other components of the medicinal product, (9) previous therapy with antiosteoporotic drugs (bisphosphonates, denosumab, teriparatide, romosozumab), (10) underlying disease interfering with bone metabolism, (11) underlying malignant tumor disease, (12) diabetes mellitus (HbA1c ≥6.5%), (13) concomitant diseases that do not permit general anesthesia, (14) pathological dental status, (15) epilepsy, (16) claustrophobia, (17) chronic alcohol abuse, (18) drug abuse, (19) patients receiving workers’ compensation, and (20) pregnancy. All patients underwent preoperative evaluation of the Fracture Risk Assessment Tool (FRAX), a 12-point questionnaire to estimate the 10-year probability of experiencing a major osteoporotic fracture and hip fracture. 48
Intraoperatively, group randomization was performed by a single anesthesiologist (R.U.) using sealed envelopes to one of the 2 study groups (zoledronic acid: n = 40; control: n = 40). The intervention group was treated with an intraoperative single-dose of 5 mg zoledronic acid as a 100-mL infusion (Aclasta; Novartis) and the control group obtained a single 100-mL infusion of 0.9% saline solution. As only patients without osteoporosis were included in this study, drug application was performed as off-label therapy in this phase II trial (Figure 1).
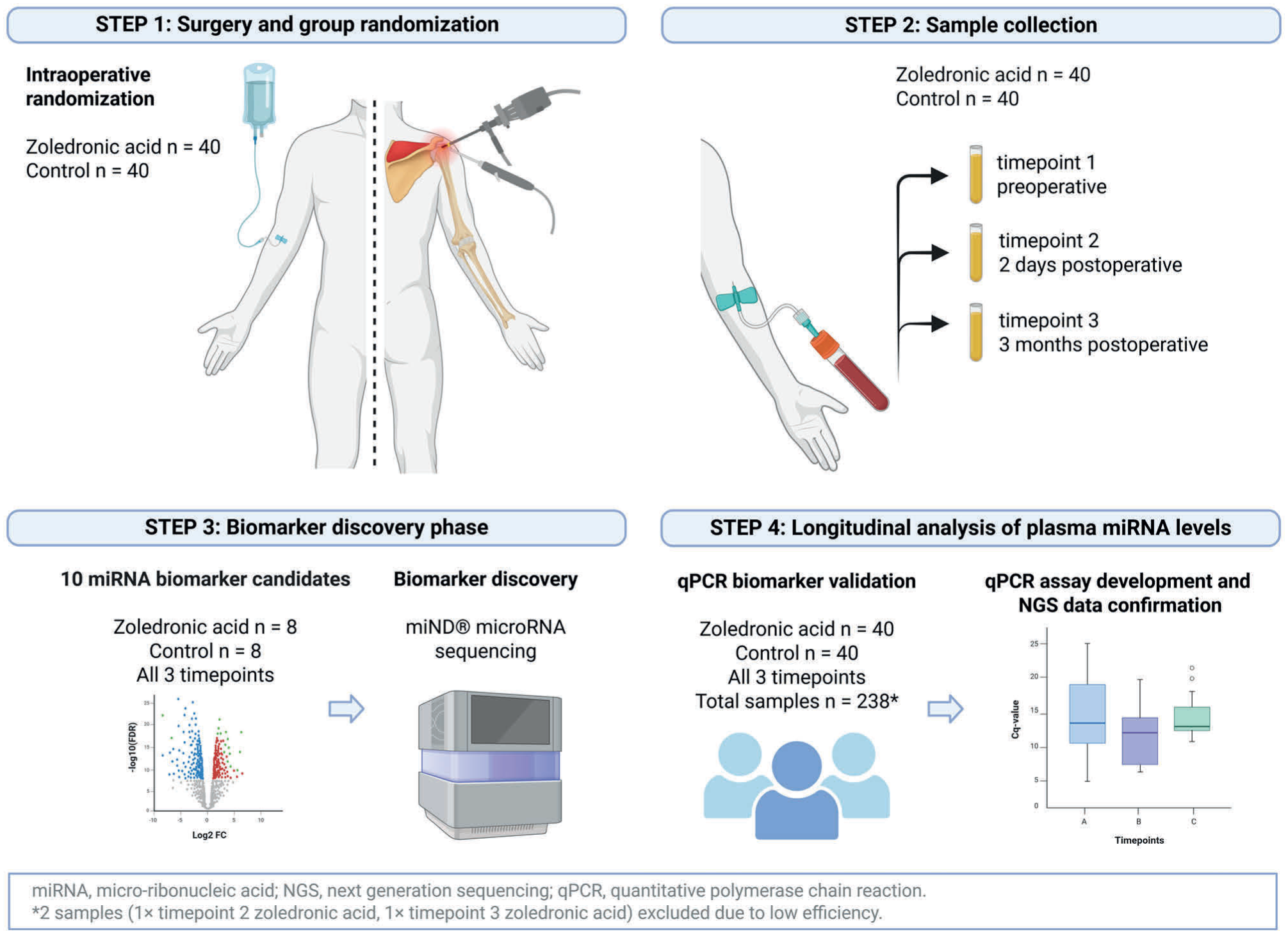
Illustration of the study protocol.
Surgical Technique and Rehabilitation
All surgical procedures were performed in the beach-chair position under general anesthesia and interscalene plexus blockade by a single fellowship-trained shoulder surgeon blinded to group randomization (C.F.). First, debridement of the tear margins, comprehensive bursectomy, and subacromial decompression were performed in all patients. In case of inflammation, instability, dislocation, or tearing of the long head of the biceps tendon, additional biceps tenotomy or tenodesis was performed. After cortical preparation of the greater tuberosity, a medially knotted transosseous suture-bridge equivalent of the posterosuperior RC was performed using titanium suture anchors for the medial fixation (5.5 mm CorkScrew FT III; Arthrex) and polyether ether ketone suture anchors for the lateral fixation (5.5 mm vented PEEK SwiveLock; Arthrex). In case of tendon delamination, both layers were repaired.
Postoperatively, patients were immobilized for 4 weeks using an abduction brace. All patients underwent a standardized postoperative rehabilitation protocol. Phase 1 (postoperative weeks 1-4) allowed passive and assistive abduction and flexion until 30° as well as strengthening of the scapula fixators. Phase 2 (postoperative weeks 5 and 6) allowed passive and assistive abduction and flexion until 90° as well as active abduction and flexion until 30°. Phase 3 allowed passive and assistive abduction and flexion >90° as well as active abduction and flexion until 90° (postoperative weeks 7-8), full abduction and flexion as well as the beginning of external rotation (postoperative weeks 9-12), and active full range of motion against resistance (starting at postoperative week 13).
Micro-RNA
All patients underwent circulating miRNA analysis before surgery as well as 2 days and 3 months postoperatively. miRNA analysis was performed in the same patient cohort with recently published radiological, clinical, and functional outcomes. 47 Overnight fasting blood samples were drawn from all patients using ethylenediaminetetraacetic acid at the AUVA Trauma Center Vienna–Meidling between 7:00 and 10:00 a.m. All samples were immediately centrifuged at 1000g for 10 minutes (Rotanta 460 RC; Andreas Hettrich GmbH) and the plasma was transferred into microtubes. Then, the plasma was centrifuged at 10,000g for 10 minutes (Mikro 200; Andreas Hettrich GmbH), aliquoted into 3 microtubes with 0.5 mL, and stored at −20°C for up to 1 week, followed by transfer to −80°C. Further miRNA analyses were performed at TAmiRNA, Vienna.
In an initial discovery phase, plasma samples of 16 patients (zoledronic acid: n = 8; control: n = 8) were analyzed at all 3 timepoints (preoperatively, 2 days postoperatively, 3 months postoperatively). Based on the discovery phase, putative plasma miRNA candidates that exclusively changed between all 3 timepoints between the 2 study groups and showed the greatest significance according to P values were selected for the validation phase. In the validation phase, these putative miRNAs were measured in the plasma of all patients (zoledronic acid: n = 40; control: n = 40) at all 3 timepoints (sample size: n = 240). Data from the discovery phase and validation phase were merged to determine the effect of zoledronic acid compared with saline solution on plasma miRNA expressions as well as time-dependent changes.
Total RNA Extraction
RNA extraction from 200 µL of plasma was carried out using the Maxwell RSC miRNA tissue kit AS1460 (Promega). miRCURY spike-in controls (Qiagen) were introduced into the lysis buffer before extraction to assess the efficiency of RNA recovery. To prevent excessive spike-in amounts from compromising sequencing depth for endogenous RNAs such as miRNAs, a predilution step (1:250) was performed before use, deviating from the manufacturer’s original protocol. The total RNA was subsequently eluted in 50 µL of nuclease-free water.
Small RNA-Sequencing Analysis
Small RNA-sequencing libraries were generated using a single-adapter ligation protocol (RealSeq Biosciences) as previously described. 21 In brief, 8.5 µL of total RNA extracted from plasma was combined with 1 µL of miND spike-in controls (TAmiRNA) and used as input for library preparation following the manufacturer’s guidelines. To enrich for miRNA-containing fragments, libraries were size-selected using an automated preparative gel electrophoresis on a 3% agarose cassette (BluePippin; Sage Biosystems). The resulting libraries were normalized to a uniform molar concentration, pooled, and sequenced on a NovaSeq 6000 SP1 flow cell (Illumina). Raw sequencing data were processed using the miND pipeline as previously reported to generate microRNA read counts. 8
Reverse Transcription Quantitative Polymerase Chain Reaction
Universal reverse transcription (RT) was carried out using 2 µL of total RNA extracted from plasma in a 10-µL reaction volume, utilizing the miRCURY RT kit (Qiagen). The reaction was incubated at 42°C for 60 minutes, followed by enzyme inactivation at 95°C for 5 minutes. To assess potential enzyme inhibition, cel-miR-39 was included in the RT mix. The resulting complementary DNA was stored at −20°C until further use in RT quantitative polymerase chain reaction (RT-qPCR) analysis. Target miRNAs were amplified using miRCURY LNA assays (Qiagen) in combination with the miRCURY SYBR Green mix (Qiagen) in a 384-well plate format on a Roche LightCycler 480 II system (Roche). Quantitative PCR was performed for 45 cycles under the cycling conditions specified by the manufacturer. To evaluate RNA extraction and RT efficiency, UniSp2 and cel-miR-39 (Qiagen) were measured. Delta cycles of quantification (ΔCq) values were determined using the Roche LightCycler 480 II system by applying the second derivative maximum method and were subsequently normalized to UniSp2 spike-in controls to minimize analytical variability.
Statistical Analysis
Micro-RNA Sequencing and Statistical Analysis
Next-generation sequencing data were analyzed using the miND analysis pipeline. 8 The overall data quality was assessed automatically and manually using FastQC Version 0.12 and MultiQC Version 1.14. 10 Adapter trimming and quality filtering were performed using Cutadapt Version 3.3, retaining reads ≥17 nucleotides in length. 34 Filtered reads were aligned to the human reference genome (GRCh38.p12), 61 using bowtie Version 1.3.0 allowing 2 mismatches, 26 followed by mapping to miRBase Version 22 restricted to hsa miRNAs with 1 mismatch tolerance. 14 Reads not annotated as miRNAs were mapped to RNAcentral Version 23.0 for general RNA composition analysis. 42
Differential expression analysis was performed in R Version 4.0 (R Foundation for Statistical Computing) using edgeR Version 3.32. 43 Count data were normalized by the trimmed mean of M-values method. Low-abundance miRNAs were removed using an independent filtering approach adapted from DESeq2 to optimize statistical power and control the false discovery rate (FDR). 32 Group comparisons were conducted using quasi-likelihood negative binomial generalized log-linear models, and dispersion estimates were obtained via empirical Bayes moderation.
Effect sizes were expressed as log2 fold changes (log2FC), with positive values indicating higher expression in the first group of each contrast. P values were adjusted for multiple testing using the Benjamini-Hochberg FDR method, 1 and miRNAs with FDR <0.1 were considered significantly differentially expressed.
Data visualization was performed in R using pheatmap, pcaMethods, and ggplot2. Volcano plots were used to depict the relationship between log2FC and statistical significance (−log10 of the FDR-adjusted P value), where points farther from zero represent larger fold changes and those higher on the y-axis represent greater significance.
Quantitative Polymerase Chain Reaction Validation and Statistical Analysis
Validation of selected miRNAs was performed by RT-qPCR. Occasional missing values occurred due to technical limitations in amplification efficiency and were automatically accounted for in the mixed-effects model.
Relative miRNA expression was quantified using ΔCq values, where a difference of 1 ΔCq corresponds to an approximately 2-fold difference in expression between samples. Data were visualized as scatter box plots, with horizontal lines indicating the median, boxes representing the interquartile range (IQR) and 25th and 75th percentiles, whiskers extending to 1.5× the IQR, and individual data points beyond this range plotted as potential outliers.
Statistical analyses were performed in GraphPad Prism Version 10.6.1 using a mixed-effects model to evaluate longitudinal differences across time points and between treatment groups. This approach accounts for repeated measures and missing data without excluding incomplete cases.
The normality of continuous data was assessed visually by histogram inspection and Q-Q plots and tested statistically using the Shapiro-Wilk test. Normally distributed continuous data are presented as mean and standard deviation. All tests were 2-sided, and P values <.05 were considered statistically significant.
Results
Plasma micro-RNA Discovery Phase
Descriptive data for the 16 patients (zoledronic acid: n = 8; control: n = 8) in the initial discovery phase are presented in Table 1. In the discovery phase, plasma miRNAs of the 16 patients were analyzed at all 3 timepoints (preoperatively, 2 days postoperatively, 3 months postoperatively), resulting in a total of 48 samples. First, cross-sectional differences were analyzed and 3 miRNAs showing significant (FDR <0.1) plasma-level elevations 2 days postoperatively after zoledronic acid treatment were identified (Figure 2A). Pair-wise longitudinal analysis identified 17 up- and 5 downregulated miRNAs 2 days postoperatively in the zoledronic acid group, and 2 differentially regulated miRNAs 2 days postoperatively in the control group (Figure 2B). Most of these changes reversed 3 months postoperatively in the zoledronic acid group, indicated by the downregulation of 16 miRNAs and upregulation of 10 miRNAs relative to timepoint 2. Based on the discovery phase, 6 miRNAs were selected for further validation, with large plasma-level differences between the zoledronic acid group and control group 2 days postoperatively (Figure 2C), and were previously reported to mediate both inflammatory and regenerative processes: miR-29a-3p, miR-425-5p, miR-21-5p, miR-192-5p, miR-146a-5p, and miR-140-3p.
Descriptive Data for the Zoledronic Acid Group and the Control Group From Initial micro-RNA Discovery Phase a
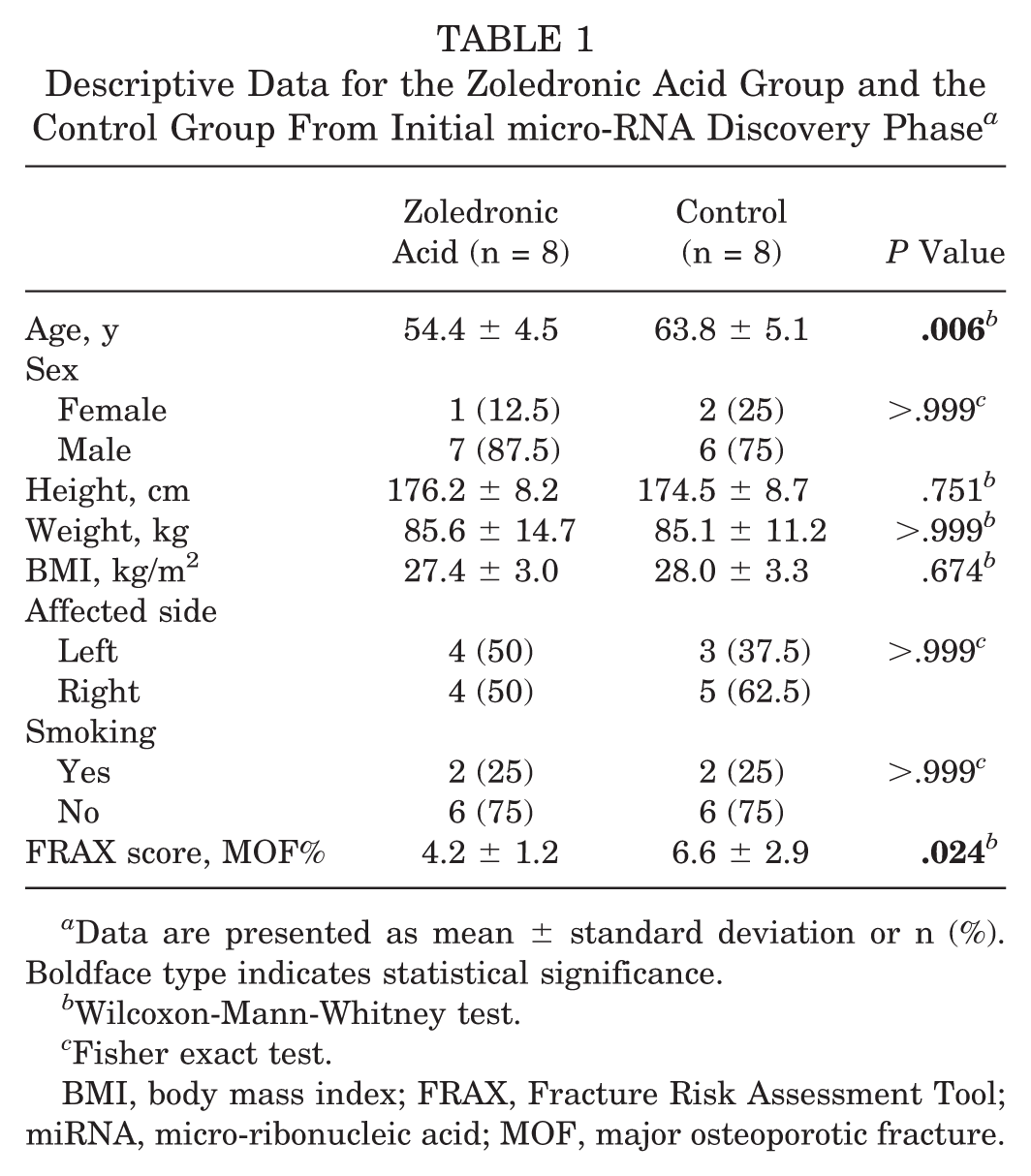
Data are presented as mean ± standard deviation or n (%). Boldface type indicates statistical significance.
Wilcoxon-Mann-Whitney test.
Fisher exact test.
BMI, body mass index; FRAX, Fracture Risk Assessment Tool; miRNA, micro-ribonucleic acid; MOF, major osteoporotic fracture.
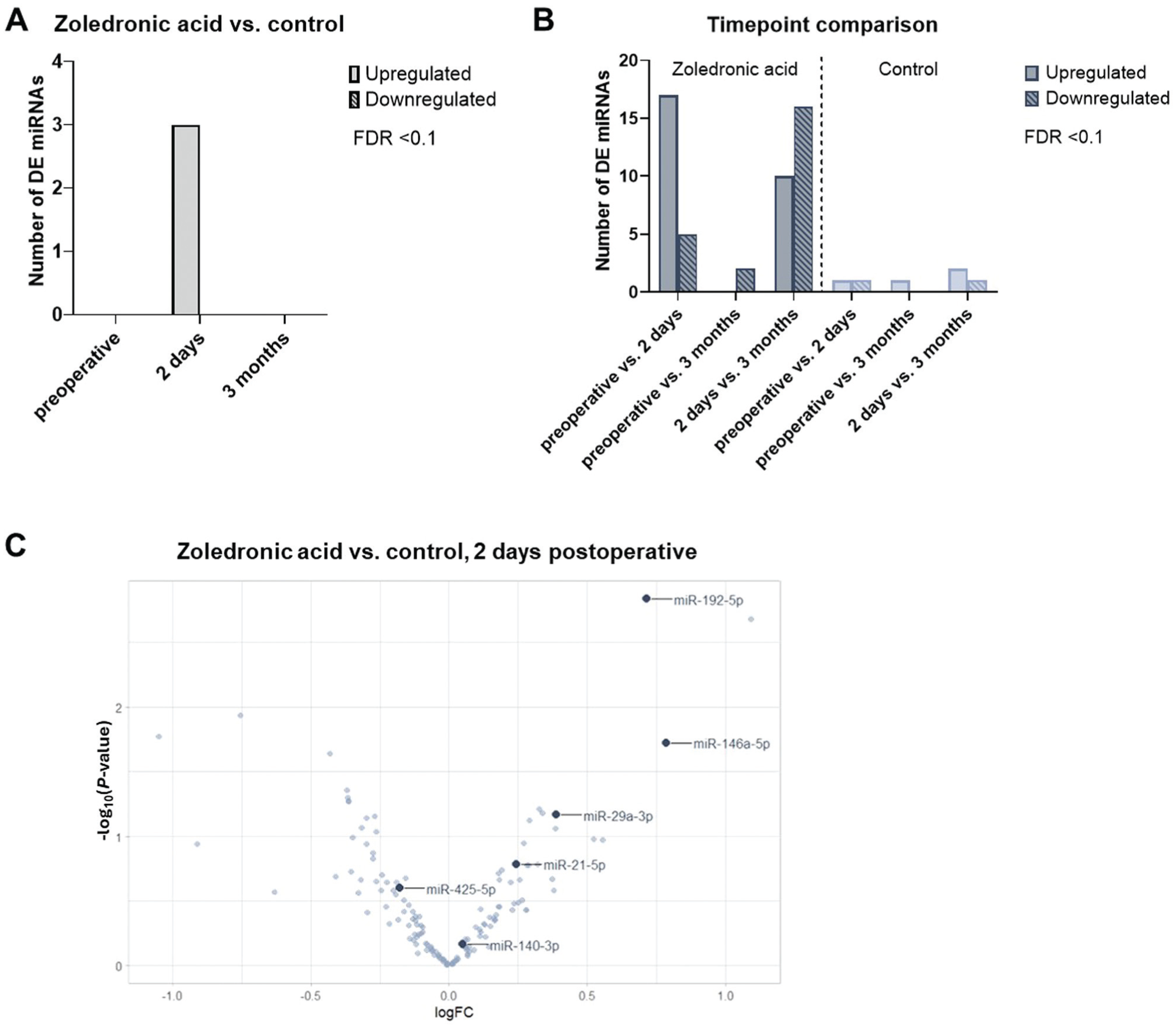
Next-generation sequencing–based analysis of micro-ribonucleic acid (miRNA) plasma levels. (A) Number of differentially expressed (DE) miRNAs observed in the zoledronic acid group and control group at each timepoint (false discovery rate [FDR] < 0.1). (B) Number of DE miRNAs observed between timepoints in the zoledronic acid group and control group (FDR < 0.1). (C) Volcano plot visualizing the effect size (log2 fold change, x-axis) and significance level (−log10 of the adjusted P value, y-axis) for miRNAs with zoledronic acid treatment 2 days after surgery.
Plasma micro-RNA Validation Phase
The descriptive data for all patients (zoledronic acid: n = 40; control: n = 40) are presented in Table 2.
Preoperative Descriptive Data for the Zoledronic Acid Group and the Control Group a
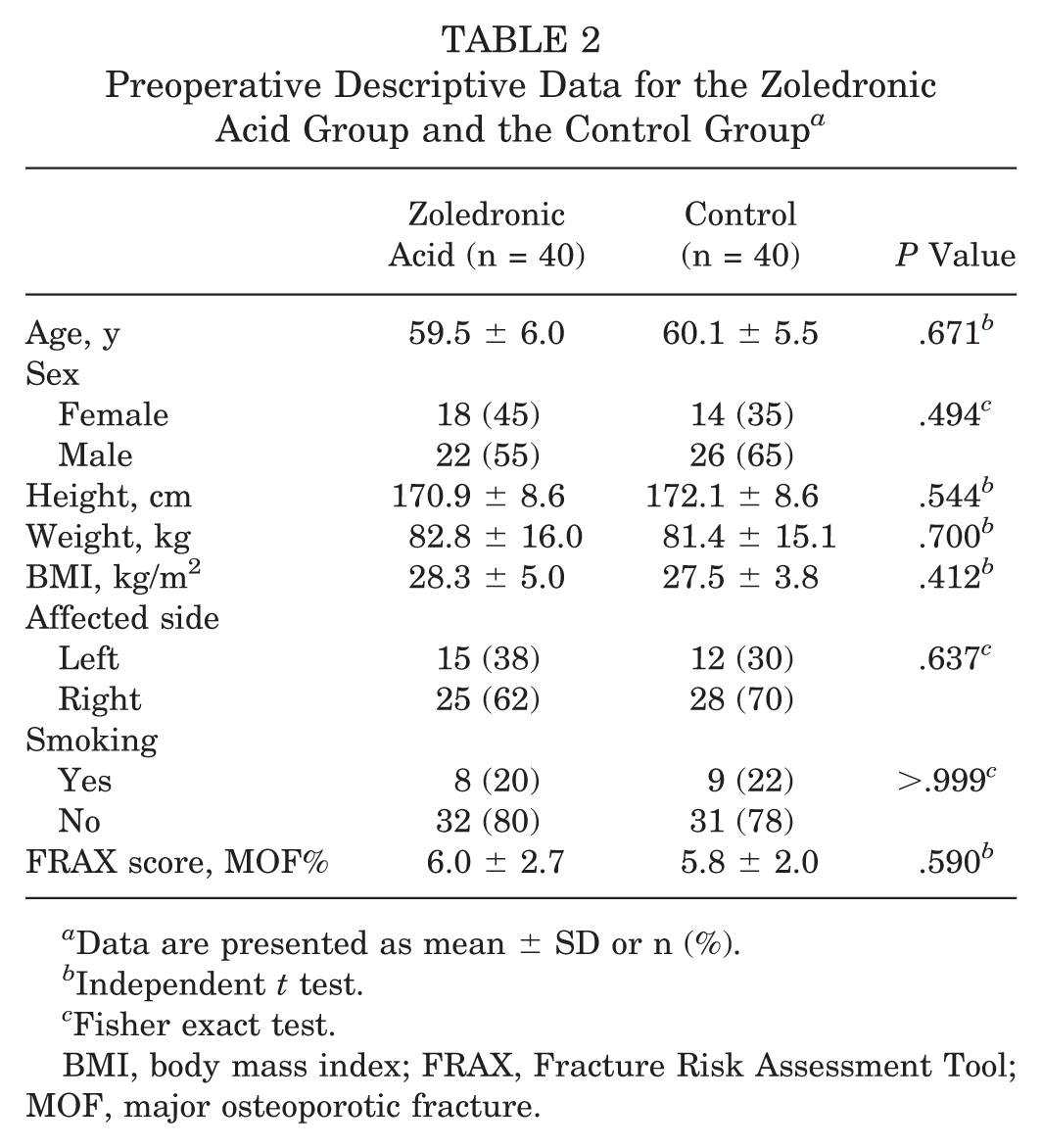
Data are presented as mean ± SD or n (%).
Independent t test.
Fisher exact test.
BMI, body mass index; FRAX, Fracture Risk Assessment Tool; MOF, major osteoporotic fracture.
Quality control was performed using spike-in controls to assess RNA extraction yield and RT-qPCR efficiency. After quality control, 238 of 240 samples were included in the analysis of the 6 preselected miRNAs. Two samples (1 × timepoint 2 zoledronic acid, 1 × timepoint 3 zoledronic acid) were excluded from analysis due to low efficiency.
miRNA outcomes are presented in Figure 3. Among all preselected miRNAs, no statistical differences in miRNA expressions were observed preoperatively between the 2 study groups. Longitudinal analysis, comparing plasma miRNA levels 2 days after surgery with preoperative plasma levels, identified a significant downregulation for miR-425-5p (P < .001) and miR-140-3p (P < .001) in the zoledronic acid group. In the control group, a significant downregulation was observed for miR-29a-3p (P < .001), miR-21-5p (P = .004), miR-192-5p (P < .001), and miR-146a-5p (P < .001) 2 days postoperatively compared to preoperative levels.
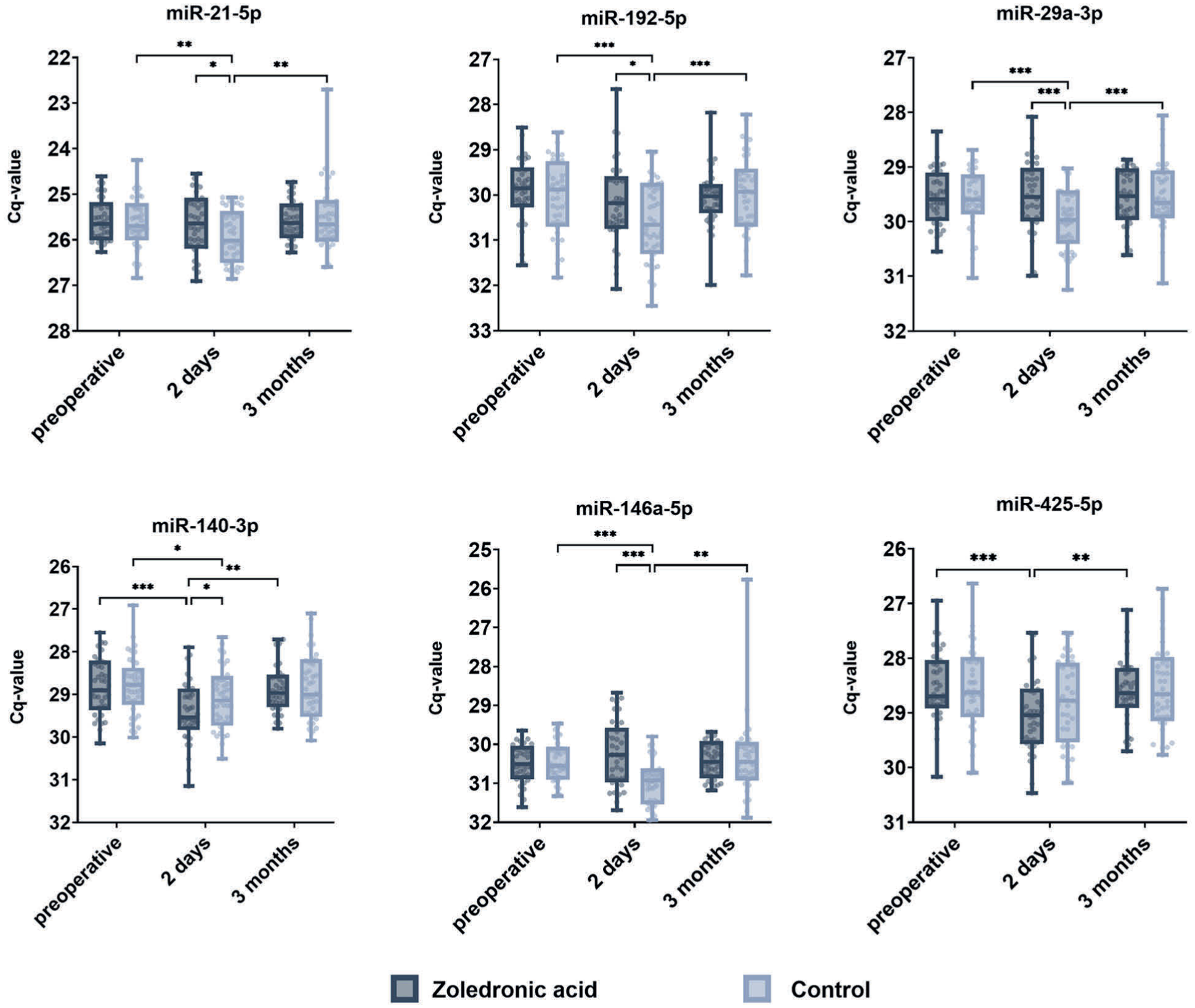
Scatter box plots illustrating the longitudinal plasma levels of micro-ribonucleic acids (miRNAs) at 3 timepoints (preoperatively, 2 days postoperatively, 3 months postoperatively) between the zoledronic acid group and control group. Data are presented as delta cycles of quantification (ΔCq) values derived from reverse transcription quantitative polymerase chain reaction analysis. Data are log2 scaled (the difference of 1 ΔCq corresponds to duplication or halving of miRNA levels). In the box plots, the horizontal lines indicate the median, the boxes represent the interquartile range (IQR) spanning the 25th (Q1) to 75th (Q3) percentiles, the whiskers extend up to 1.5 × the IQR from Q1 and Q3, and data points beyond this range are plotted individually as potential outliers. *P < .05; **P < .01; ***P < .001.
Cross section analysis 2 days postoperatively found that plasma miRNA expressions were significantly lower for miR-140-3p (P = .047) in the zoledronic acid group, and plasma miRNA expressions were significantly lower for miR-29a-3p (P < .001), miR-21-5p (P = .036), miR-192-5p (P = .034), and miR-146a-5p (P < .001) in the control group.
Three months after surgery, the miRNA expression levels of the 2 study groups equalized without any significant differences.
Discussion
Despite technical innovations and surgical improvements like arthroscopic double-row and transosseous equivalent repair techniques, retear rates up to 28% are reported in the first year after arthroscopic RC repair. 18 Therefore, multiple biological and mechanical augmentation techniques aim to improve healing after RC repair. 9 A single-dose of zoledronic acid resulted in distinct changes in circulating miRNAs after arthroscopic RC repair, possibly indicating improved tendon-to-bone healing, as these findings reflect the recently published reduction of short-term retears after arthroscopic RC repair in the same patient cohort from a prospective, randomized, placebo-controlled, triple-blinded phase II trial. 47
Preclinical studies reported increased bone mineral density and bone microarchitecture in the humeral head after RC repair with an additional systemic treatment using bisphosphonates.46,58 Furthermore, biomechanical properties of the enthesis significantly improved after RC repair and augmentation with bisphosphonates.20,46,58 In a sheep model, Johnson et al 20 reported similar biomechanical properties of the RC enthesis after repair and augmentation using alendronate, comparable to a native tendon without osteoporosis. This was also reflected in histological analyses, as the authors found marked changes at the insertional organization of the enthesis with increased interdigitation at the junction of bone and mineralized fibrocartilage, resulting in improved healing of the enthesis. 20 Moreover, zoledronic acid was associated with improvements of muscle-specific miRNAs, which was reflected by histologically verified muscle regeneration of the supraspinatus after RC repair in a rat model. 45
Based on the encouraging data in animal models, the first clinical studies investigated the effects of zoledronic acid after arthroscopic RC repair in patients with osteoporosis.27,28 Recently, a single-center, prospective, randomized, placebo-controlled, triple-blinded phase II trial showed a significant reduction of early retears in patients without osteoporosis undergoing arthroscopic RC repair with a systemic single-dose of zoledronic acid. 47
Epigenetics play a crucial role in the development of RC tendinopathy or RC tears and are eventually involved in the healing process. 17 Papalia et al 40 summarized the current understanding of the involvement and dysregulation of miRNAs related to inflammation, fibrosis, and tendon-to-bone healing in RC injuries and healing. Because a single miRNA has multiple targets, which are in turn involved in various (patho-)physiological processes with positive as well as negative feedback loops,16,56 the direct involvement of a single miRNA needs to be interpreted with caution. Nevertheless, the combination of different miRNA expression patterns offers a broader view for the interpretation of cellular pathways involved in tendon-to-bone healing after RC repair.
This study presents the results of a comprehensive investigation of circulating miRNAs in patients undergoing arthroscopic RC repair. Data were collected in course of a single-center, prospective, randomized, placebo-controlled, triple-blinded (investigator, surgeon, patient) phase II trial, which showed a significant reduction of early RC retears. 47 This experimental study presents miRNA analysis of the same patient cohort with recently published radiological, clinical, and functional outcomes. 47 Six signature miRNAs were identified to have significant changes in the plasma of patients treated intraoperatively with a single-dose of zoledronic acid, which controls the expression of various genes involved in shoulder pathologies (Figure 4).
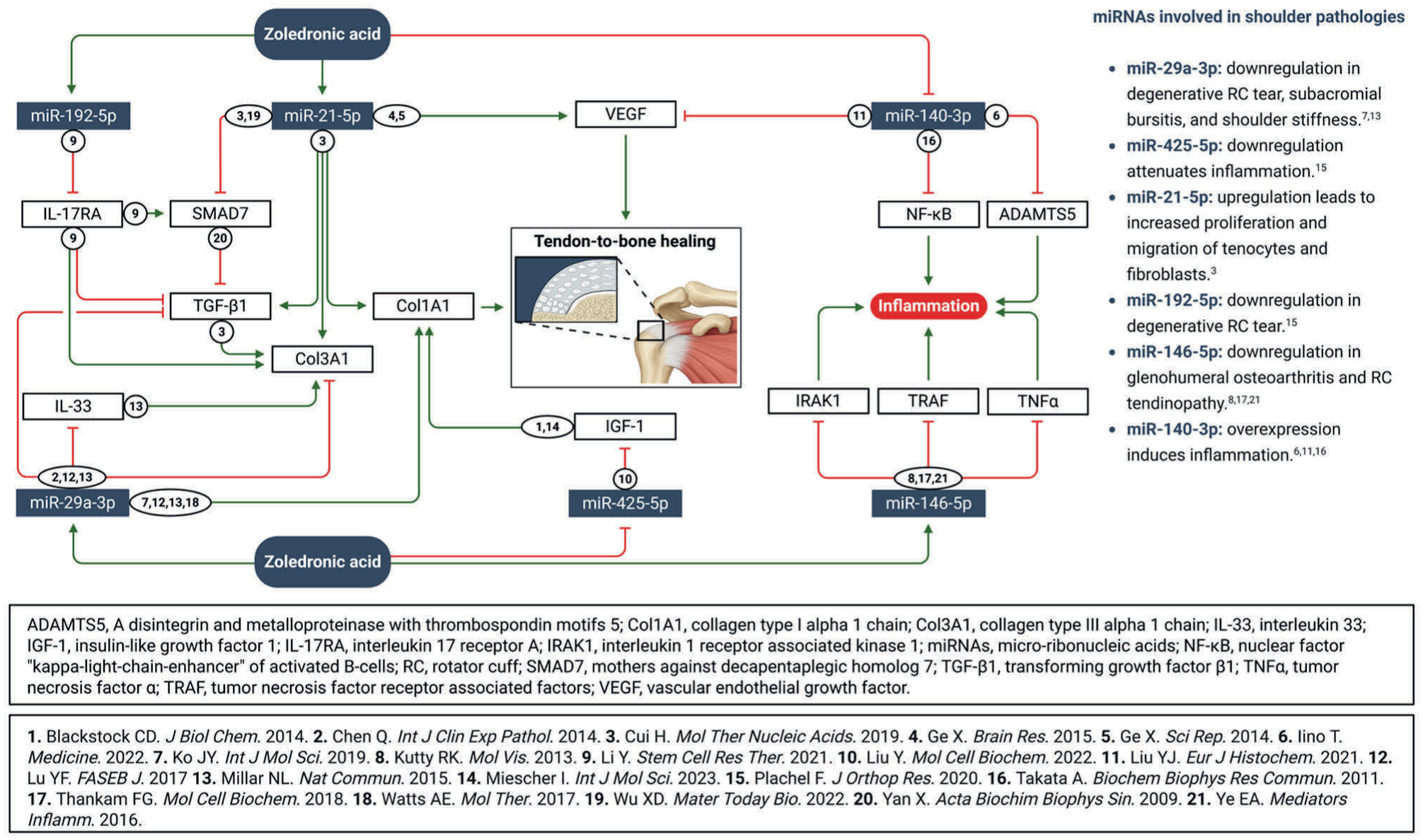
Interactions between zoledronic acid and micro-ribonucleic acid expressions and their effects on pathways involved in tendon-to-bone healing.
miR-29a-3p is the most widely studied miRNA in tendon tissue, as it promotes tendon-to-bone healing by reducing tendon adhesion formation and fibrosis after injury and accelerating tenogenic differentiation by inhibition of transforming growth factor-β1 (TGF-β1).3,22,33,36,54 Elevated levels of miR-29a-3p directly promote collagen type I alpha 1 chain (Col1A1) and inhibit collagen type III alpha 1 chain (Col3A1), resulting in an improved collagen I/collagen III ratio and less scar tissue formation.3,22,33,36,54 Furthermore, miR-29a-3p directly inhibits interleukin 33 (IL-33) expression; thus, downregulation of miR-29a-3p is associated with an increased expression of IL-33. In case of repeated tendon microinjuries, IL-33 is constantly upregulated by the suppression of miR-29a-3p, resulting in a decrease of tendon tensile strength and load to failure. 36 Moreover, downregulation of miR-29a-3p in blood samples and the subacromial bursa was associated with increased bursitis and shoulder stiffness in patients with RC lesions. 22 In case of exogenous application of miR-29a-3p, Col3A1 and fibrotic tissue development were significantly reduced, resulting in improved tendon-to-bone healing. 22 In the present study, a significant decrease in miR-29a-3p was observed in the control group postoperatively, while miR-29a-3p remained unchanged at a high level in the zoledronic acid group, potentially reflecting a higher regenerative environment. These findings are consistent with a previously reported improvement of tendon-to-bone healing after RC repair with zoledronic acid. 47
Insulin-like growth factor 1 (IGF-1) plays a key role in growth, development, and cell differentiation, with distinct effects on tendon-to-bone healing by the promotion of Col1A1 synthesis, resulting in improved mechanical properties of the enthesis.2,7,35 While overexpression of miR-425-5p leads to suppression of IGF-1, downregulation of miR-425-5p actively induces IGF-1. 30 In the present study, postoperative downregulation of miR-425-5p was observed under zoledronic acid, while the expression in the control group remained unchanged at higher levels. This might affect tendon-to-bone healing via IGF-1, as a significant reduction of early RC retears was reported after an augmentation with zoledronic acid. 47
The mothers against decapentaplegic homolog (SMAD) genes are strongly linked to TGF-β1 and play a crucial role in collagen expression and fibrogenesis. An overexpression of SMAD7 inhibits fibrosis mediated by TGF-β1, inducing proliferation and migration of fibroblasts and tenocytes. 59 miR-21-5p associates with the TGF-β/SMAD pathway, as an overexpression of miR-21-5p directly inhibits SMAD7, thus promoting Col3A1 expression via TGF-β1.6,57 On the other hand, miR-21-5p also targets the proliferation and migration capacity of fibroblasts and tenocytes with increased levels of Col1A1 at messenger RNA and protein levels, responsible for improved tendon-to-bone healing. 6 Furthermore, overexpression of miR-21-5p actively induces vascular endothelial growth factor (VEGF),12,13 which is crucial for tendon-to-bone healing by tenogenic differentiation of tendon-derived stem cells, collagen formation, and angiogenesis. 53 Two days after surgery, a significant downregulation was observed in the control group, while circulating miR-21-5p remained unchanged at high levels under zoledronic acid. Activation of Col1A1 and VEGF synthesis mediated by miR-21-5p might be a reason for improved tendon-to-bone healing, as previously reported. 47
Plachel et al 41 reported a significant reduction of miR-192-5p in patients with degenerative RC tears, compared to healthy controls. This effect might be explained by the interaction of miR-192-5p and interleukin 17 receptor A (IL-17RA). While an overexpression of IL-17RA promotes Col3A1 via the TGF-β/SMAD pathway, suppression of IL-17RA alleviates fibrosis. miR-192-5p directly targets IL-17RA, reducing Col3A1 via TGF-β1. 29 In the present study, a significant postoperative downregulation of miR-192-5p was observed in the control group, while consistently high levels were detectable throughout the study under zoledronic acid. This suggests that zoledronic acid might prevent a detrimental decrease of miR-192-5p in the plasma, thus resulting in improved tendon-to-bone healing. 47
miR-146a-5p is predominantly downregulated in case of glenohumeral arthritis and RC tendinopathy, as miR-146a-5p is a potent inhibitor of inflammation by direct suppression of tumor necrosis factor receptor associated factors, tumor necrosis factor α, and interleukin 1 receptor associated kinase 1. Therefore, reduced levels of miR-146a-5p are commonly observed in a pro-inflammatory environment.24,51,60 In the present study, a downregulation of miR-146a-5p was solely observed in the control group, while expression of miR-146a-5p remained unchanged at increased levels under zoledronic acid. This suppression of an early inflammatory response after RC repair might have had a positive effect on tendon-to-bone healing, explaining the significant reduction of retears using zoledronic acid. 47
The miR-140-3p/miR-140-5p family plays a key role in modulation of inflammation and age-related diseases by targeting a disintegrin and metalloproteinase with thrombospondin motifs (ADAMTS5) and nuclear factor “kappa-light-chain-enhancer” of activated B-cells (NF-κB).19,31,49,52 Furthermore, miR-140-3p is downregulated in RC tendinopathy as well as degenerative RC tears. 41 ADAMTS5 is commonly overexpressed in a pro-inflammatory environment, such as osteoarthritis or large full-thickness RC tears.19,52 Synovial fluid and inflamed RC tendon tissue with increased levels of ADAMTS5 show low expressions of miR-140-3p. 19 As NF-κB is a central mediator of inflammation commonly observed in tendon injuries, the suppression of NF-κB improves healing after tendon repair.25,37 Similar to ADAMTS5, miR-140-3p directly suppresses NF-κB activity, thus reducing inflammation.31,49,52 Moreover, suppression of miR-140-5p leads to an upregulation of VEGF to promote tenogenic differentiation of tendon-derived stem cells. 31 Interestingly, in the present study a downregulation of miR-140-3p was observed in the zoledronic acid group. As a single-dose of zoledronic acid led to a significant reduction of early retears after arthroscopic RC repair, 47 the downregulation of miR-140-3p could be expected in the control group in order to suppress inflammation. On the other hand, zoledronic acid induces an acute phase reaction with increased levels of C-reactive protein, 5 which was also observed in the prospective, randomized, placebo-controlled trial. 47 Therefore, it remains unclear whether the reduction of miR-140-3p in the zoledronic acid group is related to postoperative inflammation possibly impeding healing after administration of zoledronic acid, or if it can be explained by the acute phase reaction after zoledronic acid treatment.
The different expression patterns of miRNAs between the 2 study groups shortly after RC repair (downregulation of miR-425-5p in the zoledronic acid group; downregulation of miR-29a-3p, miR-21-5p, miR-192-5p, and miR-146a-5p in the control group) suggest reduced inflammation and fibrosis at the enthesis with increased collagen 1 synthesis, possibly resulting in improved tendon-to-bone healing with zoledronic acid. These findings are in line with magnetic resonance imaging (MRI) outcomes, as retears were significantly lower in the zoledronic acid group compared to the control group. 47
Limitations
Although miRNA analyses revealed significant differences between the 2 study groups, indicating a decrease of inflammation and fibrosis eventually resulting in improved tendon-to-bone healing using zoledronic acid, this cannot be completely confirmed in this study, as no downstream gene expression, histological or morphometric analyses were performed. However, differences in miRNA expression patterns might explain the significantly higher healing rates in MRI scans in the zoledronic acid group. During the miRNA discovery phase, the zoledronic acid group was significantly older with higher FRAX values compared to the control group, which might have influenced the results of miRNA expressions between the 2 study groups. However, this can be neglected, as the validation phase analyzing the whole study cohort without any differences in descriptive data between the 2 study groups showed significant differences in miRNAs linked to tendon-to-bone healing.
Conclusion
Longitudinal miRNA expression patterns suggest a reduction of inflammation and fibrosis at the enthesis as well as increased collagen synthesis and vascularization, possibly resulting in improved tendon-to-bone healing mediated by an intraoperative single-dose augmentation using zoledronic acid, recently confirmed in a prospective, randomized, placebo-controlled, triple-blinded phase II trial. In addition, such miRNAs can be used as diagnostic tools to identify and monitor patients undergoing RC repair. Ultimately, intravenous zoledronic acid is a safe and easy-to-apply augmentation technique for patients undergoing arthroscopic RC repair.
Footnotes
Acknowledgements
The authors cordially thank the Center for Clinical Studies in Regenerative Medicine (CCSRM) of the Ludwig Boltzmann Institute for Traumatology–The Research Center in Cooperation with AUVA; Ortrun-Maria Neuper, Verena Waechter, and Carlos Rodriguez-Torres for the study coordination and monitoring of the study visits; Susan Netzl and her team from the laboratory of the AUVA Trauma Center Vienna–Meidling for blood collection at all study visits; and all secretaries of the AUVA Trauma Center Vienna–Meidling for the documentation of all study visits.
Submitted January 20, 2026; accepted April 19, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: The study was financially supported by the AGA Society for Arthroscopy and Joint Surgery Research Grant (project No. 104). M.H. is a co-founder and shareholder of TAmiRNA GmbH, which holds patents related to the diagnostic use of micro-RNAs. J.G. is a co-founder and shareholder of TAmiRNA GmbH. R.B. is an employee of TAmiRNA GmbH.
Ethical approval was obtained from the local ethics committee of the AUVA (EK-No. 06/22) as well as the Austrian Agency for Health and Food Safety.