
Abstract
Background:
Return to work (RTW), particularly return to full-duty occupational function, is a clinically meaningful outcome after sports-related orthopaedic surgery. However, reporting across procedures is heterogeneous and often lacks occupational context.
Purpose:
To synthesize full-duty RTW outcomes after common sports-related orthopaedic procedures in civilian populations. Secondary objectives were to describe the time to RTW and to evaluate outcomes stratified by occupational intensity and workers’ compensation (WC) status.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. Civilian studies reporting RTW outcomes after meniscectomy, meniscal repair, anterior cruciate ligament (ACL) reconstruction (ACLR), rotator cuff repair (RCR), distal biceps repair, biceps tenodesis, or hip arthroscopy were included. Data were extracted at the cohort level. Full-duty RTW rates were calculated using sample-size weighted pooled estimates. Time to RTW was summarized using the median of reported cohort-level mean RTW times. Occupational intensity-specific and WC-specific outcomes were analyzed descriptively when reported separately at the cohort level.
Results:
A total of 87 unique studies met the inclusion criteria. Pooled full-duty RTW rates exceeded 90% after meniscectomy, meniscal repair, ACLR, and distal biceps repair. In contrast, pooled full-duty RTW rates after biceps tenodesis, RCR, and hip arthroscopy ranged from 74.2% to 76.7%. The median time to RTW ranged from 33 days after meniscectomy to 185 days after RCR. Across procedures with available data, WC cohorts and higher occupational intensity were associated with prolonged RTW timelines.
Conclusion:
Full-duty RTW outcomes vary by procedure type, with longer rehabilitation procedures demonstrating lower pooled RTW rates and longer median RTW timelines. WC status and higher occupational intensity were consistently associated with delayed RTW. Standardized reporting of occupational intensity, RTW definitions, and WC status is needed to improve clinical counseling and enhance comparability in future orthopaedic outcomes research.
Keywords
Return to work (RTW) after orthopaedic surgery represents a critical milestone for patients. While return to sport is often emphasized, return to full-duty occupational function is frequently more consequential for long-term functional independence and financial stability. Despite increasing interest in RTW outcomes, interpreting the existing literature remains challenging due to substantial variability in definitions of successful RTW, follow-up durations, and methods for classifying occupational physical demand. Many investigations report overall RTW rates without accounting for job-specific physical demands, limiting their applicability for individualized patient counseling and cross-procedure comparisons.
Several procedure-specific systematic reviews have synthesized RTW outcomes within isolated domains. Blaeser et al 3 performed a systematic review and meta-analysis of a combined military and civilian population to evaluate RTW after hip arthroscopy. They reported high overall RTW rates, although only approximately half of patients returned to full preinjury work duties, and time to RTW varied substantially by job intensity and workers’ compensation (WC) status. Rubinger et al 9 reported high rates of full RTW after distal biceps tendon repair, with a mean return time of approximately 100 days. However, reporting of occupational demands and WC status was inconsistent across included studies. Similarly, Haunschild et al 5 conducted a systematic review and meta-analysis on RTW after rotator cuff repair (RCR). They found that higher occupational physical demands were associated with lower RTW rates and longer recovery timelines, while operative technique had minimal influence on work outcomes. To date, no systematic review has synthesized RTW outcomes across multiple common sports-related orthopaedic procedures within a unified, civilian-only framework stratified by occupational physical demand and WC status. Stratification by occupational physical demand and WC status is critical, as both are well-established determinants of RTW outcomes. Military cohorts differ substantially from civilian populations in occupational demands, injury mechanisms, mandated duty requirements, and institutional return-to-duty policies. These differences may systematically influence full-duty RTW outcomes and limit direct extrapolation of military outcomes to civilian patients.
Importantly, return to any work capacity (including modified or restricted duty) is not equivalent to return to unrestricted, full-duty occupational function. Full-duty RTW more accurately reflects restoration of baseline occupational capacity and is often the primary concern of working-age patients. However, many studies do not distinguish between modified-duty and unrestricted return, contributing to heterogeneity in reported outcomes.
The purpose of this systematic review was to descriptively synthesize full-duty RTW rates after common sports-related orthopaedic procedures in civilian populations. Secondary objectives included describing the time to RTW and, when reported, stratifying by occupational intensity and WC status. The authors hypothesized that procedures requiring longer postoperative rehabilitation (RCR, biceps tenodesis, and hip arthroscopy) would be associated with lower full-duty RTW rates and longer time to RTW compared with procedures associated with faster functional recovery, such as meniscectomy, meniscal repair, anterior cruciate ligament (ACL) reconstruction (ACLR), and distal biceps repair.
Methods
Search Strategy
A systematic literature search was performed in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 2020 guidelines 8 in PubMed, Scopus, and Embase from January 2000 through November 2025. The review protocol was developed a priori and registered with PROSPERO (CRD420261319899). Search terms combined controlled vocabulary and keywords related to RTW, occupational outcomes, and sports-related orthopaedic procedures. The full electronic search strategy is provided in Appendix 1 (available in the online version of this article). Reference lists of included studies were manually screened to identify additional eligible articles. The full search strategy is summarized in Figure 1.
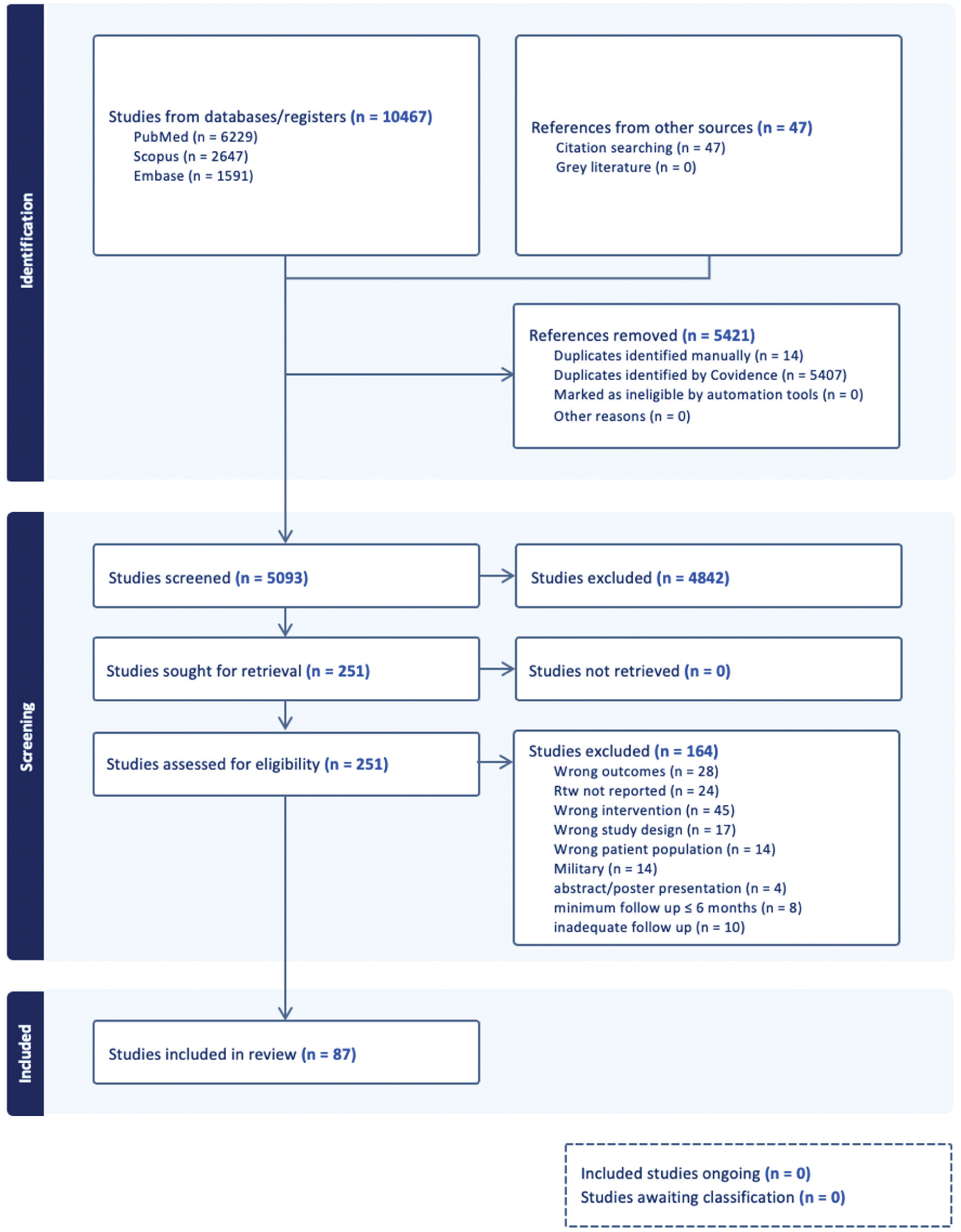
PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Eligibility Criteria
Studies were included if they reported RTW outcomes, including full-duty RTW rates and/or time to RTW in civilian adults undergoing meniscectomy, meniscal repair, ACLR, RCR, distal biceps repair, biceps tenodesis, or hip arthroscopy. These procedures were selected a priori based on their prevalence in sports-related orthopaedic practice and the availability of sufficient RTW data within the literature to allow meaningful descriptive synthesis. Studies involving exclusively military cohorts or mixed civilian-military cohorts without separable data were excluded. Studies that combined RTW and return-to-sport outcomes without separately reported cohort-level data were also excluded. A publication year limit (≥2000) was applied to reflect contemporary surgical techniques, rehabilitation protocols, and workplace demands. A minimum follow-up of 6 months was required for all procedures. For RCR, a minimum follow-up of 12 months was required due to longer recovery timelines associated with tendon healing and RTW after repair. 5
Study Design and Reporting
The objective was to provide a descriptive pooled synthesis of RTW outcomes after common sports-related orthopaedic procedures in civilian cohorts. Studies were cross-referenced for similar author and institution groupings to minimize potential patient overlap. Two independent reviewers (T.N. and S.L.) screened titles, abstracts, and full-text articles using the online software program Covidence (Veritas Health Innovation Ltd). Disagreements were resolved through discussion with a third senior author (A.H.) to achieve consensus.
Data Extraction
Data were extracted independently by 2 reviewers (T.N. and S.L.) using a predefined standardized form. Extracted variables included study characteristics, RTW definitions, full-duty RTW rates, mean time to RTW, occupational intensity-specific RTW outcomes, and WC-specific RTW outcomes. Cohorts without reported occupational intensity were excluded from intensity-stratified analyses to avoid misclassification bias. Discrepancies were resolved by consensus. Data were extracted at the cohort level. When both limited-duty and full-duty RTW were reported, full-duty data were used. Studies reporting mixed WC and non-WC cohorts without separable data were excluded from the WC-specific subanalyses but were retained in the overall pooled analyses when otherwise eligible. All 87 included studies with descriptive data are included in Appendix Table A1 (available online).
Mean RTW times were standardized to days. Values reported in weeks were multiplied by 7 and those reported in months by 30.44. Occupational intensity categories were consolidated into light/sedentary, moderate, and heavy classifications based on study definitions found in Appendix Table A2 (available online).
Quality Assessment
The level of evidence was assessed using the Oxford Centre for Evidence-Based Medicine criteria. 7 Non-randomized prospective and retrospective study quality assessment was performed with the Methodological Index for Non-Randomized Studies (MINORS) criteria. 10 Randomized controlled trials were assessed using the Cochrane Risk of Bias Tool 2.0 (RoB 2). 6 Quality assessment was performed to characterize the methodological rigor of the included literature and to inform interpretation of findings; studies were not excluded based on risk of bias. RoB 2 and MINORS are shown in Appendix Tables A3 and A4 (available online).
Data Synthesis
A descriptive pooled synthesis was performed. Full-duty RTW percentages were calculated using sample size-weighted, cohort-level estimates:

Due to inconsistent reporting of dispersion measures across studies, a formal meta-analysis of time to RTW was not performed. Instead, the primary summary metric for RTW timing was the median of reported cohort-level mean RTW times for each procedure. This approach was selected to reduce the influence of extreme cohort-level means and to provide a stable descriptive summary in the setting of heterogeneous reporting. Unweighted mean RTW times and ranges of reported cohort-level mean RTW times were presented descriptively. No inferential comparisons were conducted.
Results
Study Selection
A total of 87 unique studies were included in the qualitative synthesis. The number of studies contributing to pooled RTW rates versus pooled mean time differed across procedures due to inconsistent reporting for each outcome.
Full-Duty RTW Outcomes by Procedure
Full-duty RTW rates and time to RTW differed by procedure (Table 1). Across procedures, pooled full-duty RTW rates ranged from 74.2% to 98.6%, while the median time to RTW ranged from 33 days after meniscectomy to 185.3 days after RCR. Reported cohort-level mean RTW times demonstrated substantial variability across procedures (Table 1).
Overall Full-Duty RTW Outcomes by Procedure a
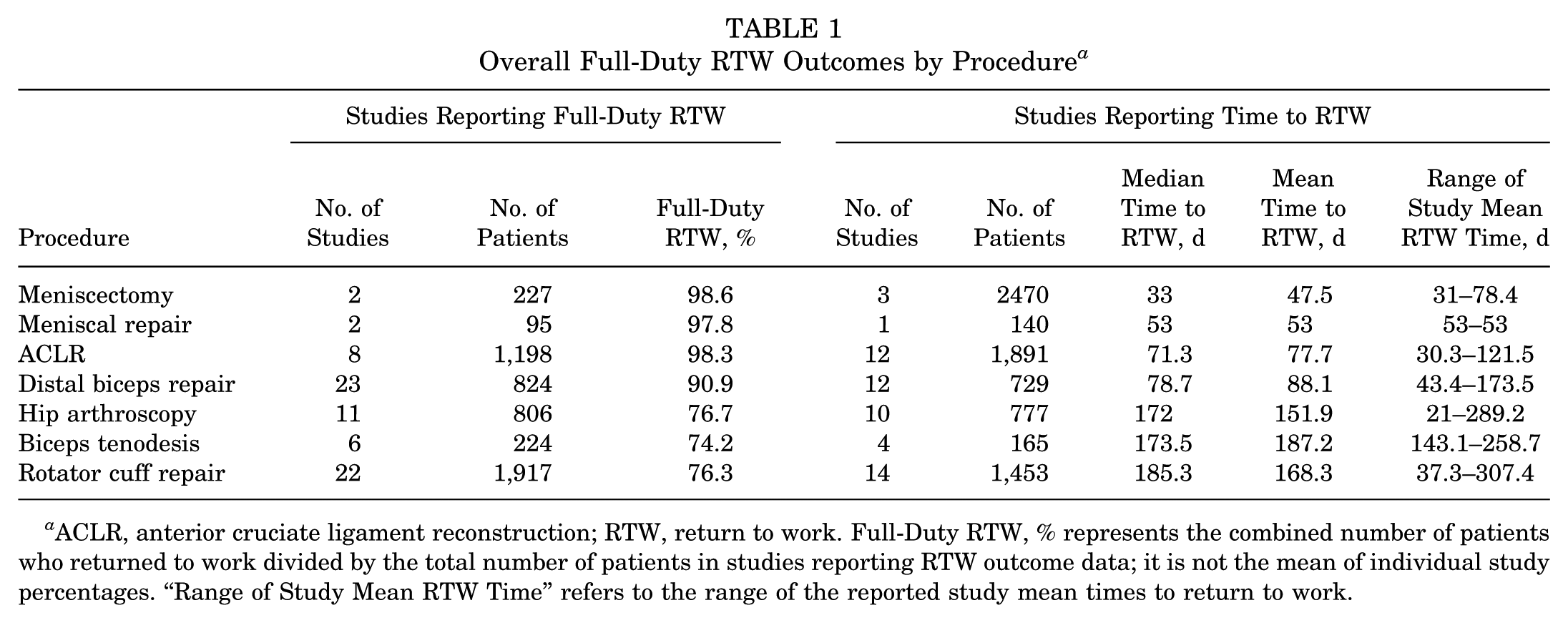
ACLR, anterior cruciate ligament reconstruction; RTW, return to work. Full-Duty RTW, % represents the combined number of patients who returned to work divided by the total number of patients in studies reporting RTW outcome data; it is not the mean of individual study percentages. “Range of Study Mean RTW Time” refers to the range of the reported study mean times to return to work.
Occupational Intensity-Stratified Outcomes
Occupational intensity-specific outcomes were variably reported (Table 2). Occupational intensity-stratified data were most complete for RCR and hip arthroscopy. In these procedures, RTW rates and mean time to RTW differed across moderate- and heavy-duty cohorts where stratified data were available (Table 2). However, complete intensity strata were unavailable for several procedures, limiting cross-procedure comparisons of occupational intensity effects.
RTW Outcomes Stratified by Occupational Intensity a
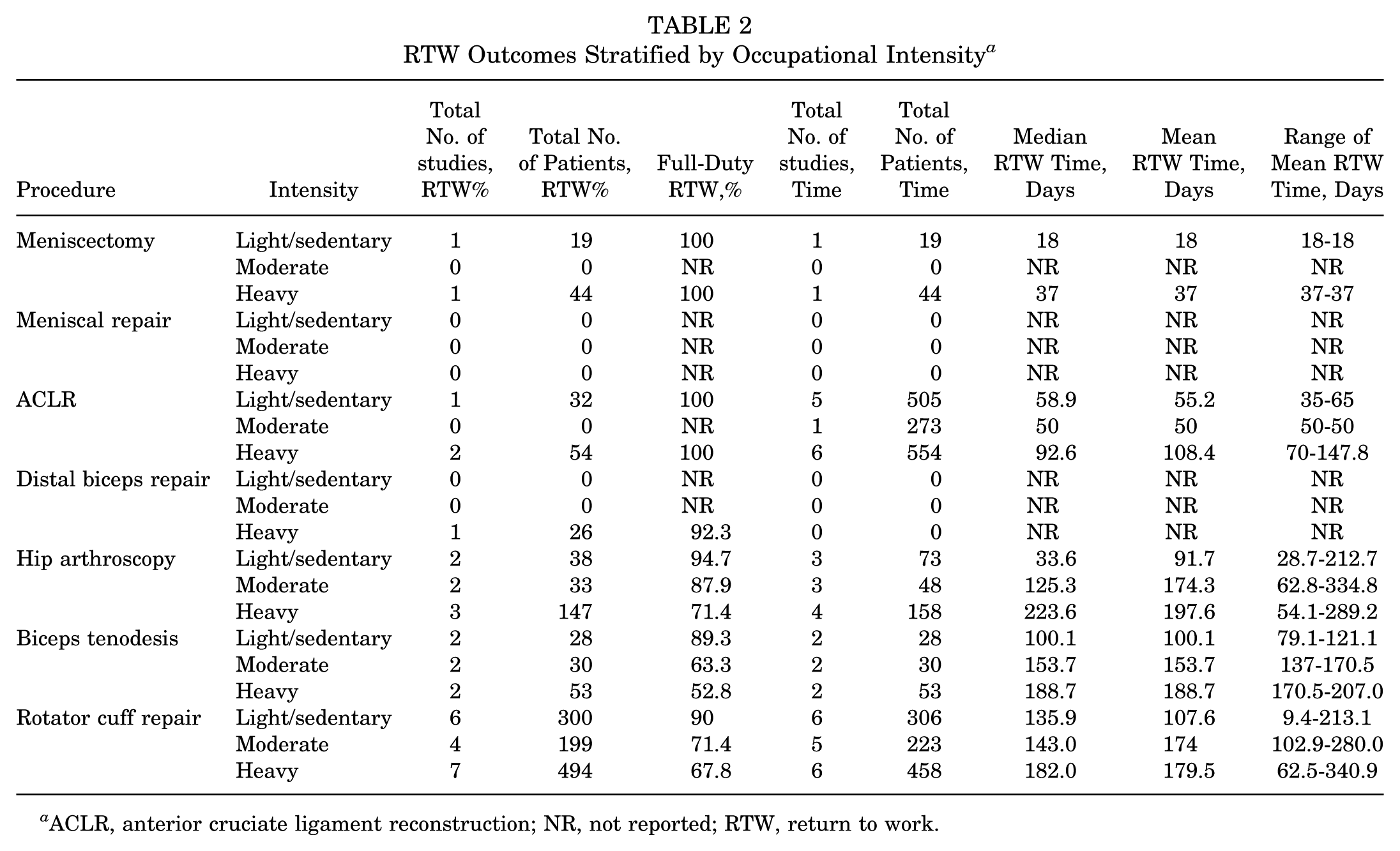
ACLR, anterior cruciate ligament reconstruction; NR, not reported; RTW, return to work.
WC Outcomes
WC-specific RTW outcomes were available for a subset of included studies in which WC and non-WC cohorts were reported separately at the cohort level; studies with mixed, nonseparable cohorts were excluded from these subanalyses. Across procedures with available data, the median time to RTW was consistently longer in WC cohorts than in non-WC cohorts (Figure 2, Tables 3 and 4). WC cohorts demonstrated prolonged RTW times across all procedures. No formal comparisons were performed.
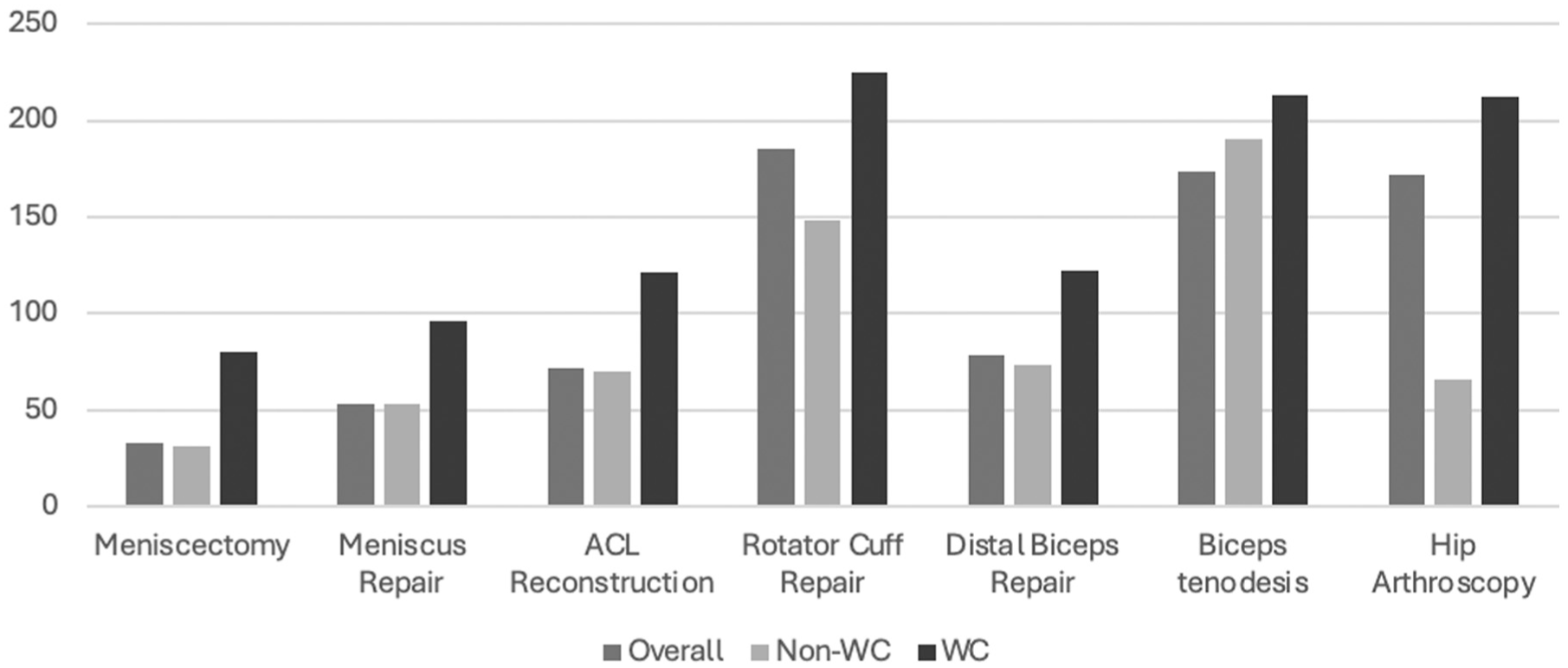
The median time to RTW by procedure and WC status. Grouped bar graph demonstrating the median RTW time in days for overall cohorts, non-WC cohorts, and WC cohorts. ACL, anterior cruciate ligament; non-WC, non-workers’ compensation; RTW, return to work; WC, workers’ compensation.
WC-Specific RTW Outcomes by Procedure a
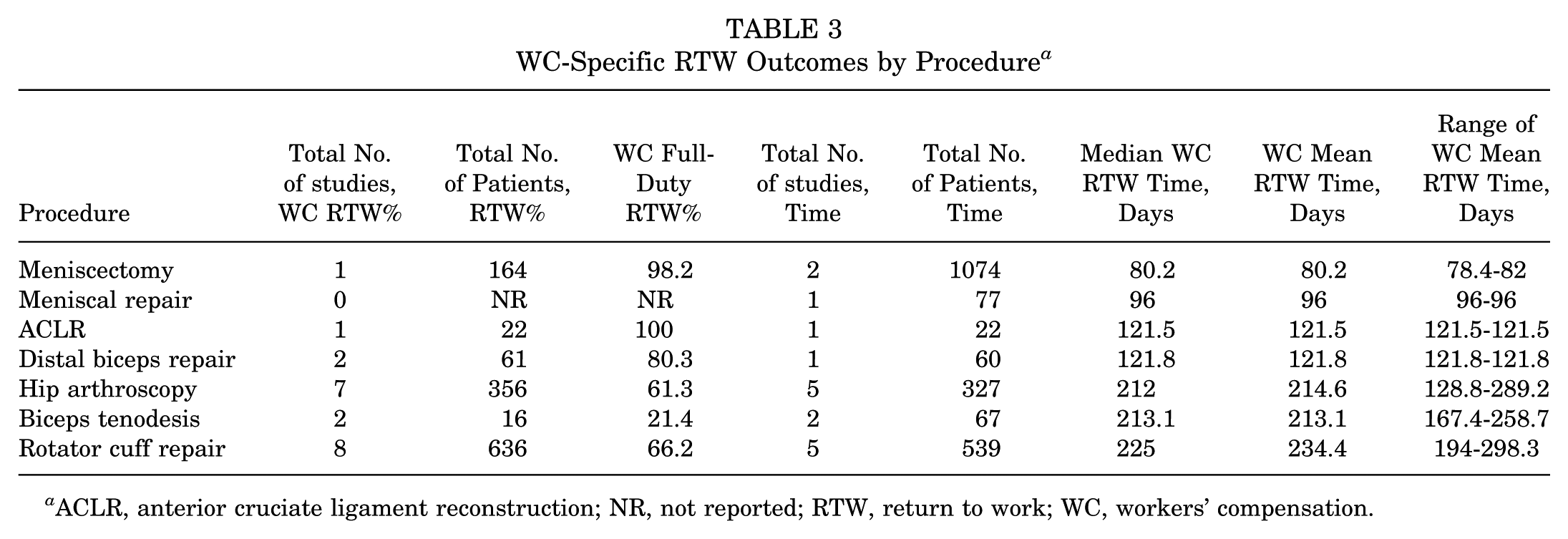
ACLR, anterior cruciate ligament reconstruction; NR, not reported; RTW, return to work; WC, workers’ compensation.
Non-WC-Specific RTW Outcomes by Procedure a
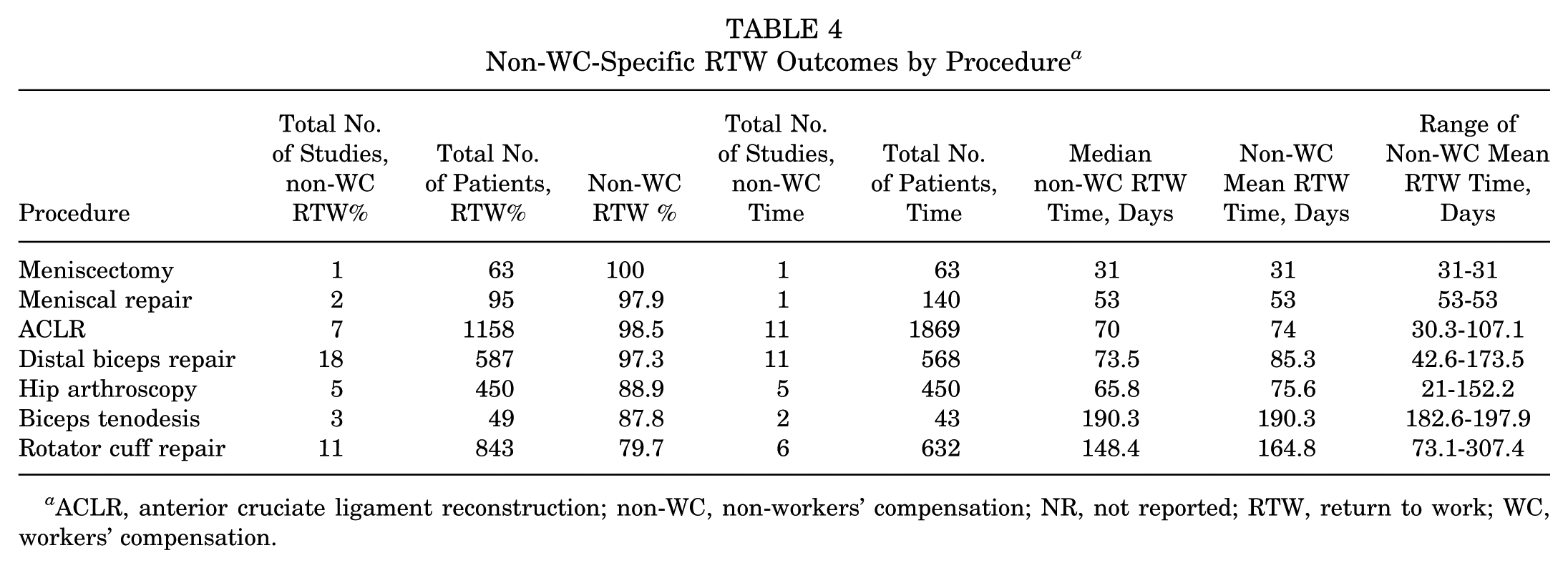
ACLR, anterior cruciate ligament reconstruction; non-WC, non-workers’ compensation; NR, not reported; RTW, return to work; WC, workers’ compensation.
Discussion
This systematic review provides a comprehensive descriptive synthesis of full-duty RTW outcomes after 7 common sports-related orthopaedic procedures in civilian populations. Procedures associated with shorter rehabilitation timelines, such as meniscectomy (98.6%; 33 days), meniscal repair (97.8%; 53 days), ACLR (98.3%; 71.3 days), and distal biceps repair (90.9%; 78.7 days), demonstrated consistently high pooled full-duty RTW rates and a short median time to RTW. In contrast, biceps tenodesis (74.2%; 173.5 days), RCR (76.3%; 185.3 days), and hip arthroscopy (76.7%; 172 days) were associated with lower pooled RTW rates and longer recovery time. Across procedures with available data, WC cohorts demonstrated longer median RTW times compared with non-WC cohorts. Variability in reporting resulted in differing numbers of studies contributing to RTW rate versus timing estimates, which should be considered when interpreting cross-procedure comparisons.
A key conceptual distinction in the RTW literature is the difference between return to any work capacity and return to unrestricted, full-duty occupational function. While overall RTW rates are frequently high, inclusion of modified or restricted duty may overestimate true functional recovery. By prioritizing full-duty RTW, this review provides a more clinically meaningful benchmark for counseling working-age patients whose primary concern is restoration of preinjury occupational capacity. Additionally, reporting of modified duty was inconsistent across studies and often not reported at comparable time points with full-duty return. In certain settings, particularly within WC systems, early return to modified duty may be influenced by employer or insurer expectations, which may shorten reported RTW timelines and introduce bias in the interpretation of outcomes.
Differences in full-duty RTW rates and timelines likely reflect variation in rehabilitation demands, occupational physical requirements, and inconsistent RTW definitions across studies. Previous civilian systematic reviews of distal biceps repair report high rates of return to previous work without permanent restrictions and predictable RTW timelines, which is consistent with the range of full-duty RTW rates and time-to-RTW estimates observed in the present review. 9 In contrast, RCR has been associated with a lower likelihood of return to the previous work level among patients in physically demanding occupations, consistent with the intensity-stratified findings observed here. 5
Similarly, previous hip arthroscopy literature demonstrates variability in RTW definitions, with high rates of return to some work but less predictable return to full-duty, particularly among patients in higher-demand occupations. 3 Differences between previously published estimates and those observed in the present review may reflect the exclusion of military cohorts and a higher proportion of civilian WC populations. A civilian cohort study after biceps tenodesis reported decreasing full-duty RTW rates with increasing job intensity, reinforcing the influence of occupational demand. 1 Civilian ACLR cohorts likewise demonstrate delayed RTW among patients performing knee-demanding work. This supports the observation that even procedures with high overall RTW likelihood may involve delayed work resumption in heavier-demand occupations.2,4 By synthesizing RTW outcomes across multiple procedures using a unified framework stratified by occupational intensity and WC status, this review extends previous procedure-specific literature. It provides a comparative context not previously available.
Occupational intensity-stratified RTW timing differed across reported intensity categories. These outcomes were inconsistently reported, leading to differences in the number of studies contributing to RTW percentages versus time-to-RTW estimates. Similarly, WC outcomes were variably reported and are therefore presented as secondary descriptive findings without formal comparison.
These findings support procedure-specific preoperative counseling regarding RTW expectations and highlight the need for standardized reporting of occupational intensity, RTW definitions, and WC status stratification in orthopaedic outcomes research. While RTW rates and timelines may differ by surgeon, this systematic review provides a contemporary civilian benchmark to inform discussions of expected recovery timelines. Procedures such as meniscectomy and ACLR are commonly associated with relatively rapid RTW. In contrast, RCR or hip arthroscopy often warrants counseling regarding prolonged work restrictions, particularly in physically demanding occupations or patients with WC claims. Importantly, RTW rate and time to RTW represent distinct dimensions of recovery and should not be interpreted interchangeably.
Limitations
This systematic review has important limitations. First, RTW outcomes were heterogeneously reported, with substantial variability in outcome definitions, occupational classifications, follow-up intervals, and denominators. Many studies reported dichotomous RTW without corresponding time data, while others reported mean RTW time without corresponding measures of dispersion. As a result, not all studies contributed to each pooled estimate, and several stratified analyses were derived from a limited number of studies, including single-study strata. These estimates should therefore be interpreted within the context of reporting heterogeneity. Furthermore, the absence of standardized postoperative timepoints for assessing RTW within procedures limits the ability to determine whether differences reflect true recovery variation or differences in follow-up structure.
Second, a formal inferential meta-analysis was not performed due to marked clinical and methodological heterogeneity and inconsistent reporting of variance measures (standard deviation or confidence intervals). A descriptive pooled approach using the median of reported cohort-level mean RTW times was therefore selected to summarize outcomes while avoiding inappropriate statistical assumptions.
Third, baseline employment status, preinjury occupational demands, psychosocial factors, and workplace accommodations were inconsistently reported and could not be controlled for, despite their known influence on RTW outcomes. Additionally, RTW outcomes were frequently self-reported rather than verified through employer or registry data, introducing potential recall or reporting bias.
Fourth, although WC status and occupational intensity were examined when reported, many studies included mixed cohorts that could not be separated at the cohort level, limiting the number of studies eligible for WC-specific subanalyses.
Fifth, patient-level demographic variables, including age, were not consistently reported or controlled for across studies and may have influenced RTW outcomes.
Finally, detailed surgical and intra-articular characteristics, including tear size, chronicity, degree of tendon retraction, cartilage status, presence of concomitant pathology (eg, labral tears, chondral lesions, meniscal extrusion), tissue quality, and technical variables, were inconsistently described or absent in many studies. This limits the ability to contextualize RTW outcomes within specific anatomic or technical subgroups and may contribute to variability in reported RTW rates and time-to-RTW across studies.
Conclusion
Full-duty RTW outcomes vary by procedure type, with longer rehabilitation procedures demonstrating lower pooled RTW rates and longer median RTW timelines. WC status and higher occupational intensity were consistently associated with delayed RTW. Standardized reporting of occupational intensity, RTW definitions, and WC-status is needed to improve clinical counseling and enhance comparability in future orthopaedic outcomes research.
Supplemental Material
sj-docx-1-ajs-10.1177_03635465261455044 – Supplemental material for Return to Work Outcomes After Common Sports-Related Orthopaedic Procedures: A Systematic Review Stratified by Occupational Intensity and Workers’ Compensation Status
Supplemental material, sj-docx-1-ajs-10.1177_03635465261455044 for Return to Work Outcomes After Common Sports-Related Orthopaedic Procedures: A Systematic Review Stratified by Occupational Intensity and Workers’ Compensation Status by Tanner Nishioka, Shaan Lalvani, Napatpong Thamrongskulsiri, Amelia Hummel, Jacob T. Morgan, Logan D. Moews, Tomás F. Vega, Felipe Casanova, Jourdan M. Cancienne, Nikhil N. Verma and Jorge Chahla in The American Journal of Sports Medicine
Footnotes
Submitted February 22, 2026; accepted April 24, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.C. has received support for professional activities from Smith & Nephew, Inc. N.N.V. has received royalties from Arthrex, Smith & Nephew; consulting fees from Stryker Corporation; and is a Board member of the MLB Team Physician Society. J.M.C. has received consulting fees from Arthrex Inc, MicroPort Orthopedics, Regeneration Technologies, Inc, and Smith & Nephew.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.