
Abstract
Background:
Attachment-sparing anterior cruciate ligament reconstruction (ACLR) is gaining acceptance over the use of free grafts because of reported early graft ligamentization in both animals and humans. However, the literature regarding clinical outcomes and the correlation of early graft healing is unclear.
Hypothesis:
Tibial attachment-sparing hamstring graft (AS) results in earlier graft maturation, which correlates with a better clinical outcome than a free hamstring graft (FG).
Study Design:
Randomized controlled trial; Level of evidence, 1.
Methods:
A total of 56 patients were randomly assigned to 2 groups at the commencement of the study. Of these patients, 25 (AS group) underwent ACLR using the attachment-sparing technique, while 25 patients (FG group) underwent ACLR using the free hamstring graft technique. Prospective sequential magnetic resonance imaging (MRI) evaluations were performed at 3, 6, and 9 months to document graft maturation, characteristics, orientation, and tunnel dilation. Clinical evaluation was done at 3, 6, 9, and 12 months to document Lysholm, International Knee Documentation Committee (IKDC), and Tegner scores and anterior tibial translation (ATT) by KT-2000 arthrometer, by independent observers.
Results:
The overall follow-up rate was 78% (19 cases and 20 controls of 25 in each group). MRI Figueroa scores demonstrated significant differences between the AS and FG groups, with the AS group showing consistently higher scores at all timelines. The earliest noticed graft maturation in the case group was at 3 months (26.3% had Figueroa score 4), compared to 6 months for the controls. In the AS group, all participants attained a Figueroa score of 5 at the final assessment, whereas only 10% of the FG group achieved that. The AS group maintained nearly the same graft diameters, but the FG group showed increased diameter (graft swelling) at all follow-up time points. A significant increase in tibial tunnel diameter over time was observed in both groups, with a greater increase in the AS group. A significant improvement was observed in Lysholm score, IKDC score, and ATT in both groups.
Conclusion:
Tibial attachment-sparing hamstring grafts result in earlier and complete graft maturation on MRI as compared to free hamstring grafts for ACLR.
Registration:
Clinical Trials Registry – India (CTRI/2022/10/046620).
Keywords
Anterior cruciate ligament reconstruction (ACLR) is a commonly performed reconstructive sports surgery. Two grafts used for hamstring graft harvesting are the free autogenous graft and the tibial attachment-preserving graft. The free autogenous graft is known to undergo phases of necrosis, revascularization, cellular proliferation, and remodeling.5,12 Use of tibial attachment-sparing hamstring graft has been documented to bypass the phase of necrosis and revascularization in animal models,13,16 thus reducing the possibility of graft tear in the phase of revascularization when the graft is weakest, 1 while the patient is undergoing aggressive rehabilitation.
The technique of preserving the tibial insertion of the hamstring donor tendons maintains the biological insertion strength (4 zones of seamless blending of the tendon to bone), which has the potential to become stronger with cyclic loading over time. 7 The healing of the tendon-bone interface is by fibrocartilage growth (under the influence of M2 macrophages) if the hamstring insertion is preserved, as compared to fibrous healing in a free graft.11,14 It has already been demonstrated that the pes anserinus tendon insertion is well vascularized and richly innervated; this neurovascular network continues along the length of the pes tendons.19,23 Maintenance of the neurovascular supply may help in early maturation of the newly reconstructed anterior cruciate ligament (ACL) graft. It has been documented in animal models on magnetic resonance imaging (MRI) that a significantly elevated graft signal is present between the 6th and 12th weeks, correlating to the least tensile strength of the graft (estimated to be around 7%-16% of the time with zero values). 21 There are reports of successful clinical results with attachment-sparing hamstring grafts.4,15,17,18,22 Vari et al 20 reported that at 1 year postoperatively, remodeling of the attachment-sparing hamstring graft and clinical outcome were better than those of the free hamstring graft. However, there is no literature regarding the difference in maturation of attachment-sparing graft in vivo from free graft prospectively at sequential time intervals. Attachment-sparing grafts have the potential for an earlier graft maturation, which could lead to a favorable clinical outcome.
This study was conducted with the primary aim of assessing the difference in graft maturation on MRI at prospective, sequential time intervals, and the secondary objective of correlating it with clinical outcome, between 2 methods of hamstring graft usage in arthroscopic ACLR (attachment-sparing vs free hamstring graft harvest).
Methods
This study was a randomized controlled trial conducted at a tertiary care teaching hospital, after institutional ethics board approval and registration in the Clinical Trials Registry – India (CTRI/2022/10/046620) in 2022. All consenting adults, with a unilateral ACL tear with or without meniscal injury, between 18 and 30 years of age, were included. Patients with any other associated musculoskeletal injury, multiligament injury, chondral injury, revision ACLR, any prior surgery on the ipsilateral knee, or systemic medical problems were excluded. The sample size was calculated based on the work of Ruffilli et al. 17 The mean and standard deviation of the MRI Figueroa score was used as reference. With a pooled standard deviation of 0.6, alpha of 95%, and power of 85%, the calculated sample size was 16 cases in each group. The effect size was estimated to be 0.67. Because of the stringent timeline-based follow-up, greater than expected loss to follow-up was anticipated. To compensate for follow-up loss, 56 patients were randomized to the 2 groups (31 in the AS group and 25 in the FG group) without any prior analysis of outcomes. The patients were randomized into 2 groups based on a computer-generated randomization sequence by a nurse not involved in participation recruitment or assessment (Figure 1). This was done after confirming eligibility for participation and obtaining informed consent. The surgeon (S.S., K.C.A., A.P.B.) and sports medicine specialists (H.U., K.S.V.) assessing the participants were blinded to the type of graft used. The AS group represented patients undergoing attachment-sparing ACLR, while the FG group represented patients undergoing free graft ACLR.
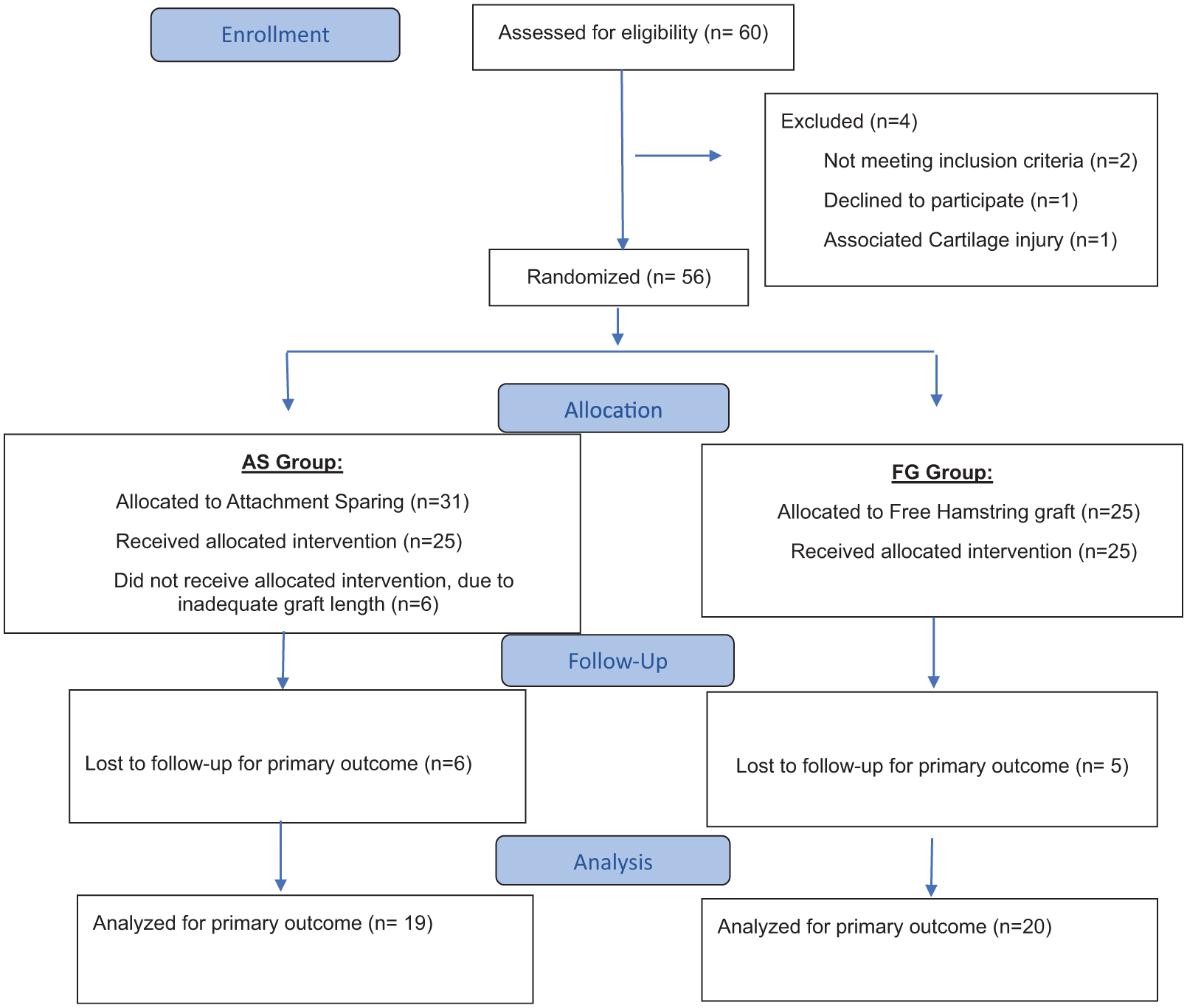
CONSORT (Consolidated Standards of Reporting Trials) flow diagram.
Attachment-sparing ACLR was performed after sterile preparation, through a 3-cm incision over an anteromedial aspect of the leg starting at the level of the tibial tuberosity. The sartorius facia was split, and the semitendinosus and gracilis tendons were harvested with an open tendon stripper, leaving the tibial insertion intact, as shown in Figure 2. The tendons were cleared of muscle tissue, and the free ends of both were whip-stitched using Ethibond No. 5. The dimensions (diameter and length) of the prepared graft were measured, and the graft was placed back subcutaneously in the wound. Arthroscopy ACLR was done through the standard anterolateral and anteromedial portals. An arthrex tibial guide and transportal femoral guide were used to create the tibial tunnel and femoral socket. The sutured free end of the graft was passed through the adjustable loop device (Stryker). The free end of the graft was secured to the tibia using a titanium staple (as described by Ruffilli et al 17 ), with the graft length adjusted to prevent bottoming at the femoral socket. The adjustable loop was shuttled from the tibia to the femur, the button was flipped, and the graft passage was performed by shortening the loop in 20° of knee flexion. Cycling was done and the graft tensioned in the same knee position. Then the wound was closed.
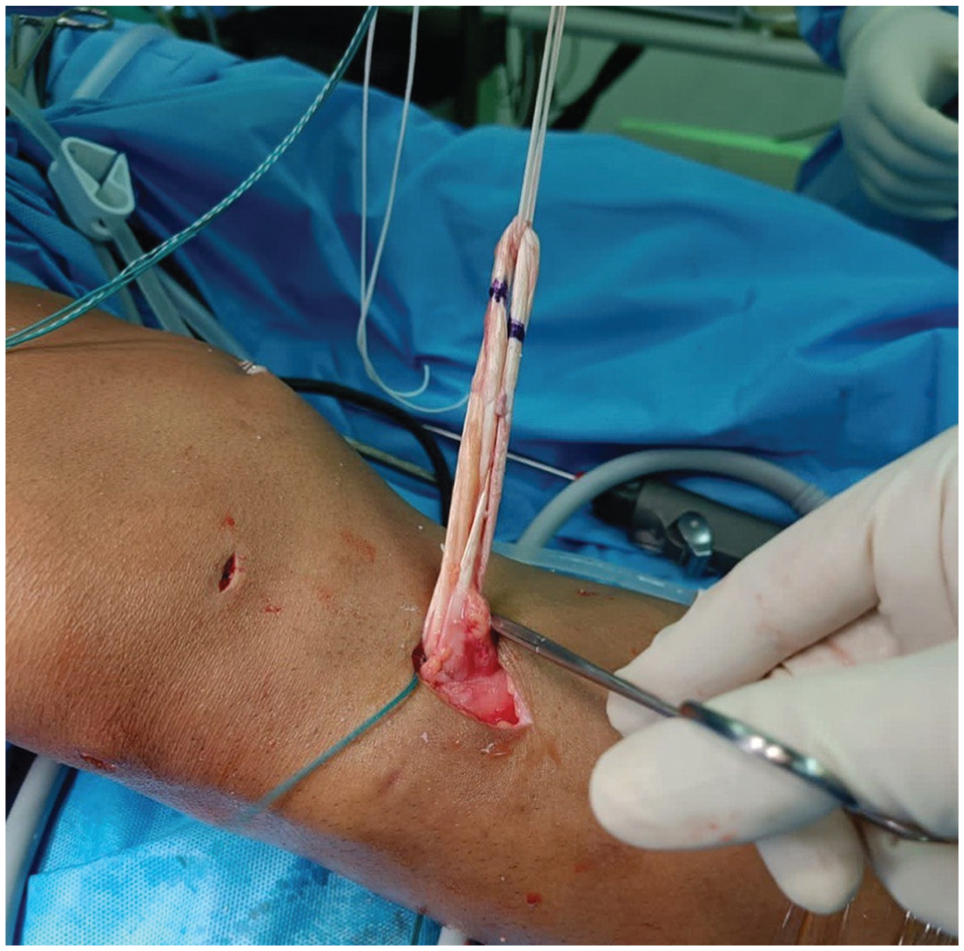
Photograph of attachment-sparing hamstring graft.
For ACLR in the FG group, an autogenous hamstring graft was prepared on the back table and measured. A femoral socket and tibial tunnel similar to those of the AS group were created. Graft fixation on the femoral side was the same as that in the AS group, and bioresorbable interference screw fixation was performed at the tibial tunnel. A single senior surgeon performed all surgeries. Postoperatively, patients were subjected to an identical standard rehabilitation protocol.
MRI of the operated knee after ACLR was done sequentially at 3, 6, and 9 months to record the qualitative and quantitative differences of the grafts of both groups. For graft measurement, proton-density 3-dimensional cube acquisition on a 3-T GE MRI scanner, with 3 mm–thick slices and 0.3 mm overlap, was used. To measure ACL graft signal intensity, the signal-to-noise quotient was calculated. For graft diameter measurement, a multioblique technique to isolate the ACL graft and create sections perpendicular to the axis of the graft was used, and the graft was measured at 3 intra-articular points in both the coronal and sagittal planes. Any case with a graft angle out of the normal range of inclination was excluded (sagittal >60°; coronal >75°). 10 Tibial tunnel dilation was also measured in both the coronal and sagittal planes. Figueroa scoring was done. 9 MRI evaluation was done by 2 musculoskeletal radiologists, who were blinded to the type of graft technique used. All quantitative values were measured 3 times, and the best value was recorded. All qualitative values were measured by both radiologists concurrently. The interrater reliability in Figueroa scores between the 2 musculoskeletal radiologists was calculated using analysis of variance to determine the intraclass correlation coefficient (ICC). The interrater reliability was 0.93.
The clinical outcome was assessed by 2 sports medicine specialists not involved in surgery and blinded to group, using Lysholm, International Knee Documentation Committee (IKDC), and Tegner scores, which were measured preoperatively and at 3, 6, 9, and 12 months after ACLR. Objective measurement of anterior tibial translation (ATT) using the KT arthrometer was done at 6, 9, and 12 months. Each reading was taken three times, and the highest value of the 3 was documented. Subjective and objective instability (positive Lachman or pivot-shift test; ATT >5 mm) at 1 year were considered as failed surgery. Patients were followed up for 1 more year to determine any incidence of graft tear.
Statistical analysis was done using the SPSS software Version 27 (IBM). Descriptive data are presented as number with percentage or mean with standard deviation. Baseline comparability between groups was assessed using independent t tests or Mann-Whitney U tests for continuous variables and chi-square tests for categorical data. Nonnormally distributed continuous variables were compared between groups using the Wilcoxon-Mann-Whitney test. Correlation between variables was assessed using the Spearman rank correlation coefficient (r). The strength and direction of association were interpreted based on r values, and statistical significance was determined using corresponding P values <0.05.
Results
Of 31 patients in the AS group, 6 patients did not receive the intended intervention because the length of attachment-sparing hamstring graft fell short, leading to 25 patients in each group. Six patients in the AS group and 5 in the FG group could not complete the MRI evaluations on the scheduled timeline and were excluded. The follow-up rate was 78% (39/50 patients), 19 in the AS group and 20 in the FG group. Both groups were comparable for baseline characteristics such as age and sex distribution, suggesting adequate group homogeneity, as depicted in Table 1. The mean graft diameter at the time of surgery was 7.95 ± 0.44 in the AS group compared to 8.48 ± 0.73 in the FG group (Table 2).
Demographic and Clinical Parameters a
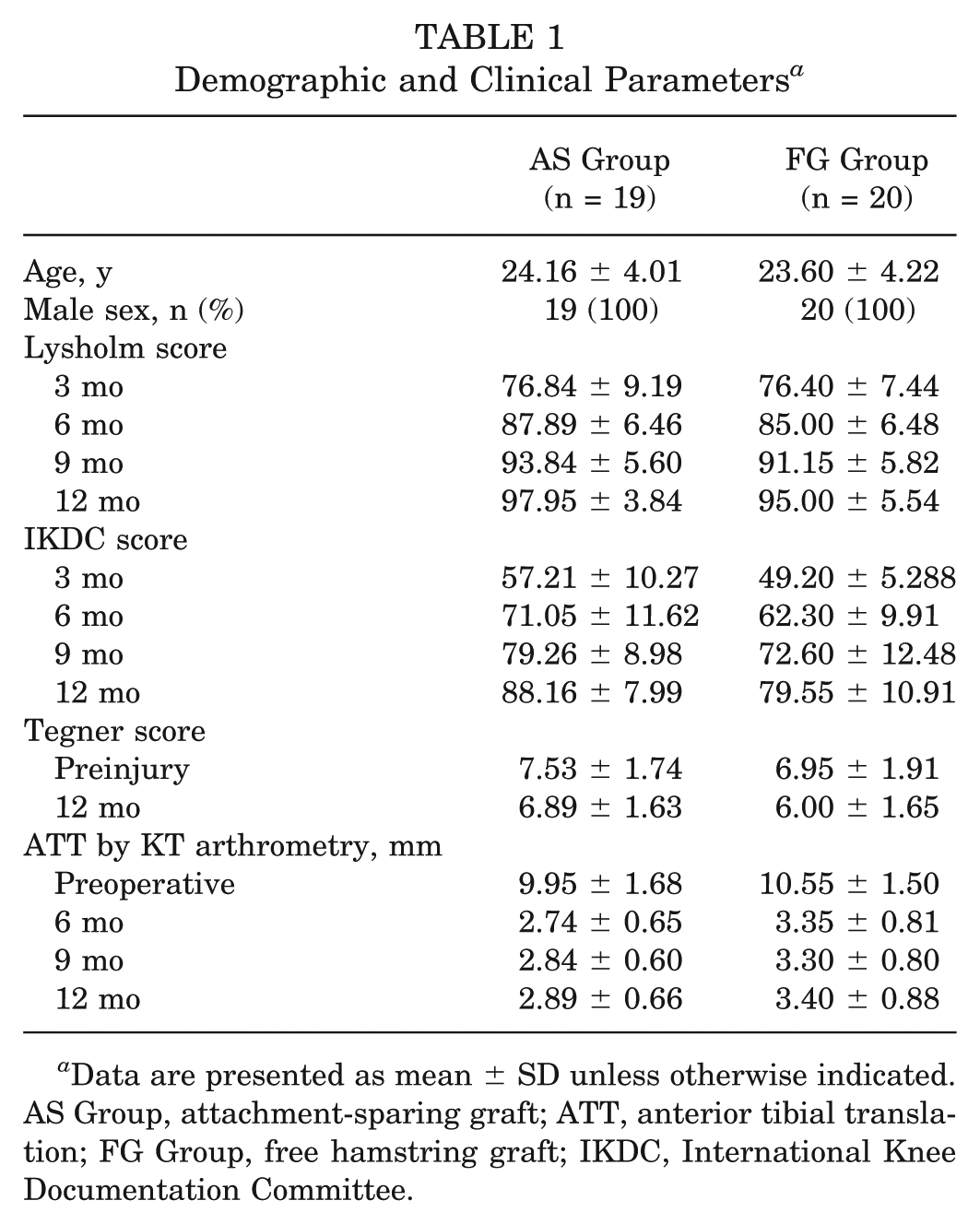
Data are presented as mean ± SD unless otherwise indicated. AS Group, attachment-sparing graft; ATT, anterior tibial translation; FG Group, free hamstring graft; IKDC, International Knee Documentation Committee.
Hamstring Graft Characteristics a

Data are presented as mean ± SD. AS, attachment-sparing graft; FG, free hamstring graft.
The orientation angle of the graft in the coronal and sagittal planes was within normal limits in both groups. MRI Figueroa scores improved in both groups at all timelines but were significantly higher in the AS group compared to FG group, with this difference becoming more pronounced at 6 and 9 months. The achievement of an MRI Figueroa score of 5 was accelerated in the AS group, with 79% achieving this milestone by 6 months compared to 0% in the FG group (P < .001) (Figures 3 and 4).
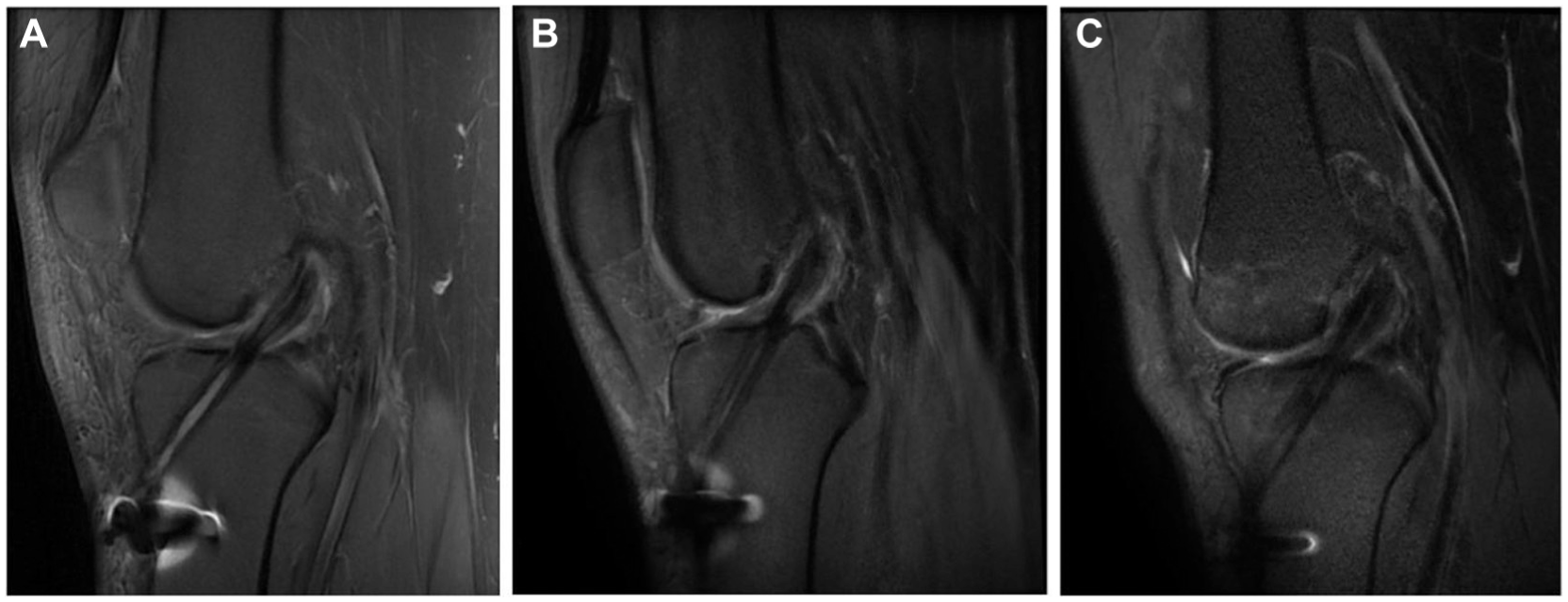
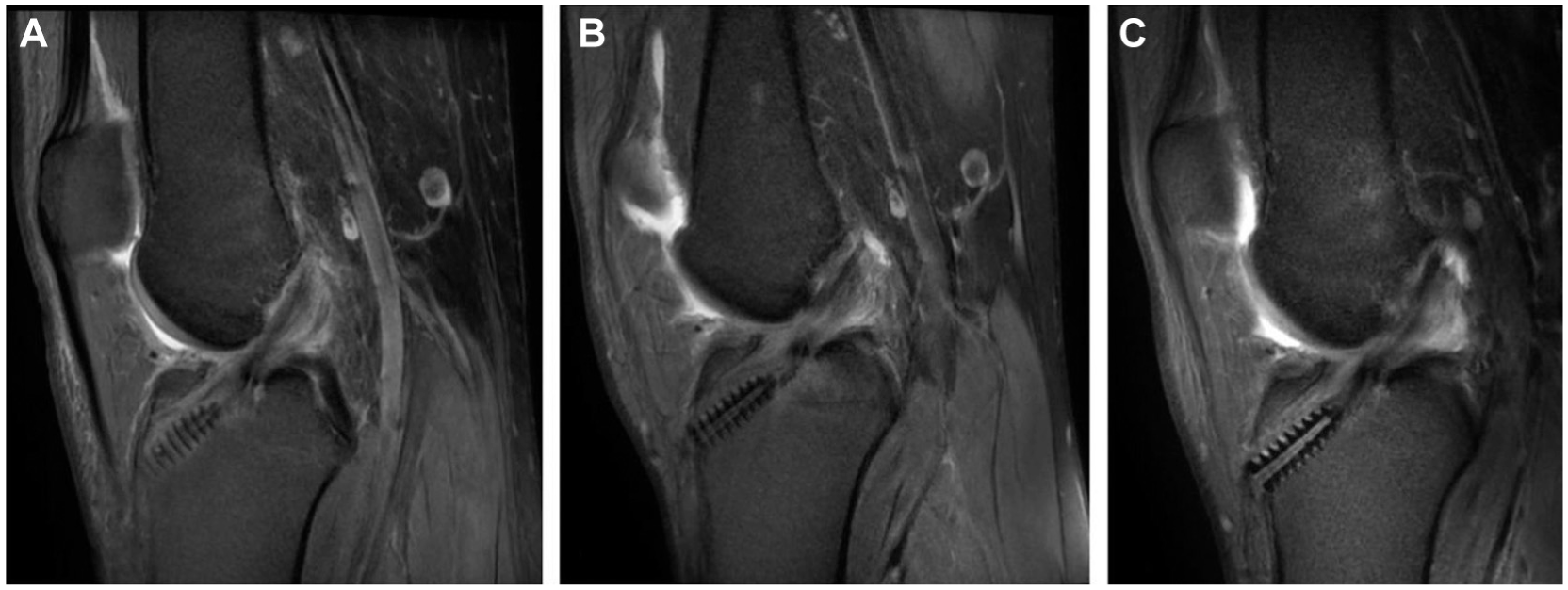
Proton-density fat-saturated sagittal images obtained in a 26-year-old male (AS group) after receiving an anterior cruciate ligament graft at (A) 3, (B) 6, and (C) 9 months, demonstrating magnetic resonance imaging Figueroa scores of 3, 5, and 5, respectively.
Proton-density fat-saturated sagittal images obtained in a 21-year-old male (FG group) after receiving an anterior cruciate ligament graft at (A) 3, (B) 6, and (C) 9 months, demonstrating magnetic resonance imaging Figueroa scores of 2, 3, and 4, respectively.
The graft diameter revealed a consistent and statistically significant difference between groups (P < .001) at all follow-up times (Table 3). The mean increase in graft diameter (difference between baseline and maximum swollen graft) was significantly lower in the AS group (2.68 ± 1.02 mm) compared to the FG group (7.78 ± 1.53 mm), and this difference was also statistically significant (P < .001) (Table 2).
Comparison of MRI Parameters Between Groups a
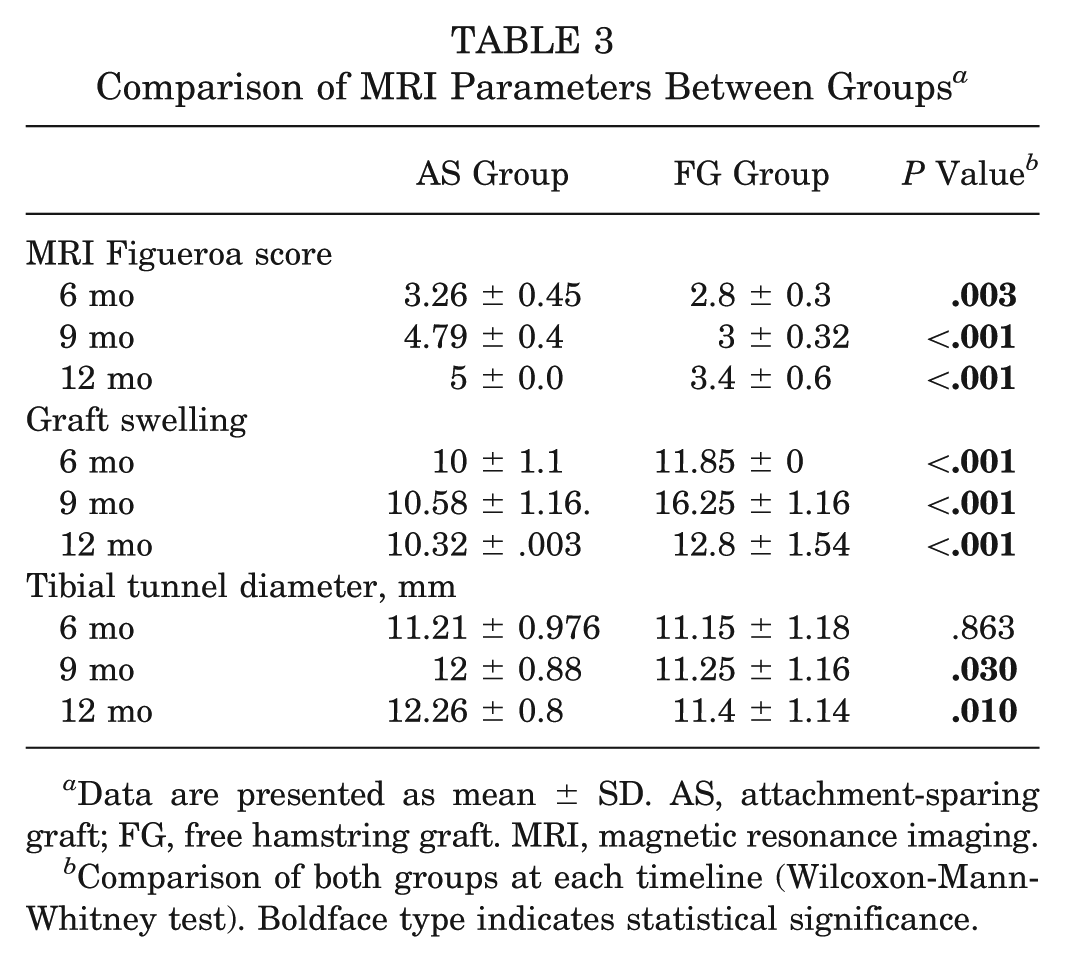
Data are presented as mean ± SD. AS, attachment-sparing graft; FG, free hamstring graft. MRI, magnetic resonance imaging.
Comparison of both groups at each timeline (Wilcoxon-Mann-Whitney test). Boldface type indicates statistical significance.
Temporal changes in tibial tunnel dimensions showed significantly larger tunnel diameters at 6 months and 9 months (P = .03 and P = .01, respectively) in the AS group (Table 3, Figures 5 and 6).
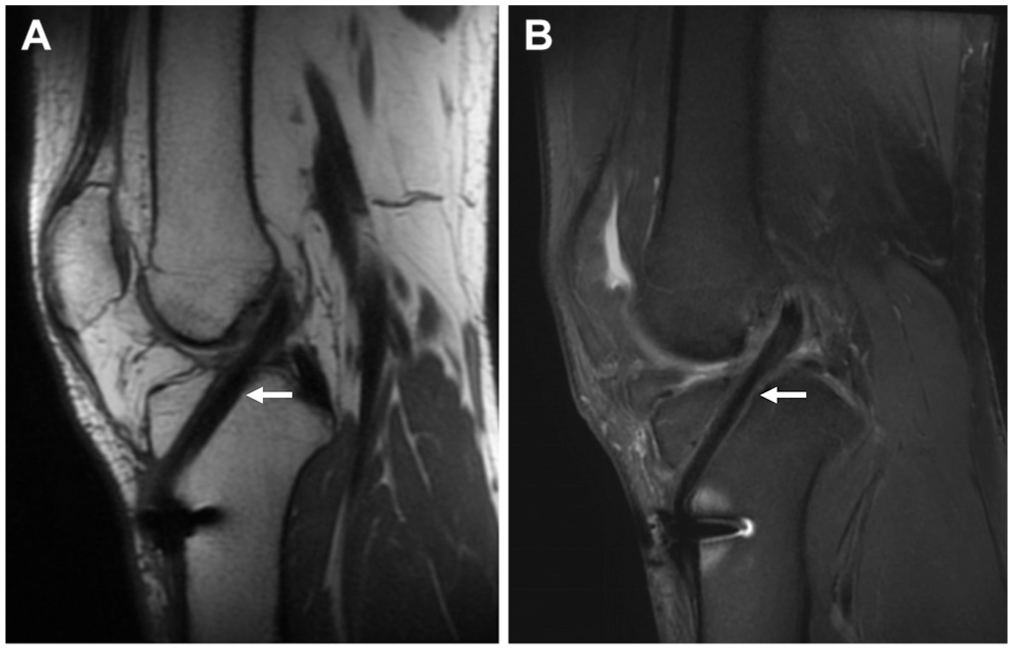
Proton-density (A) cube sagittal and (B) fat-saturated sagittal magnetic resonance imaging scans obtained in a 28-year-old male (AS group) 6 months after receiving an anterior cruciate ligament graft (attachment sparing), demonstrating hypointense graft signal (>50%) (arrow) indicating mature graft and no fluid at the graft-tunnel interface (Figueroa score 5).
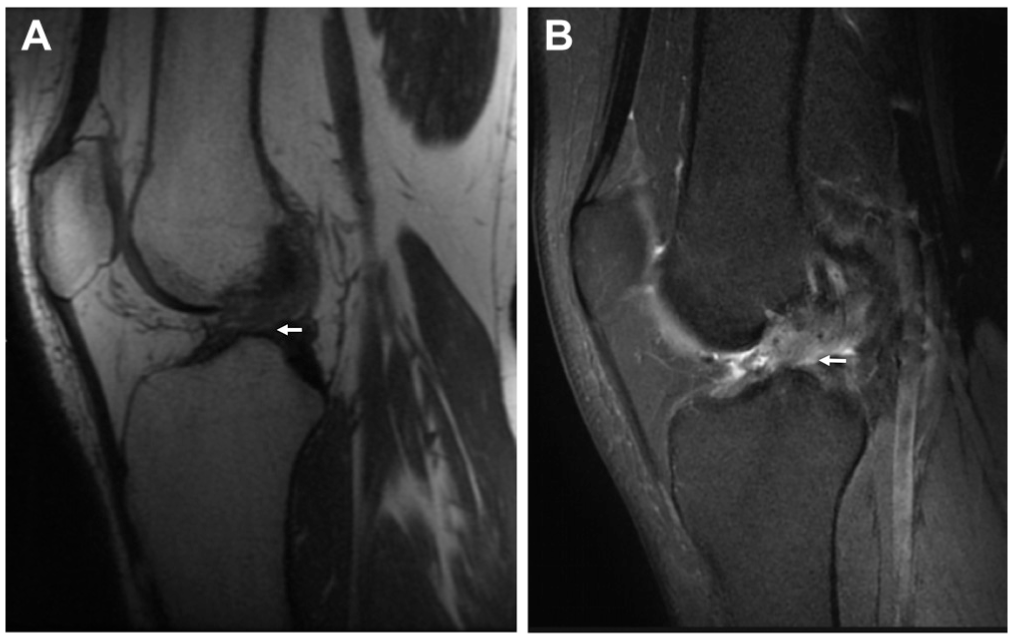
Proton-density (A) cube sagittal and (B) fat-saturated sagittal magnetic resonance imaging scans obtained in a 21-year-old male (FG group) 6 months after receiving an anterior cruciate ligament graft, demonstrating hyperintense graft signal (>50%) (arrow) indicating immature graft (Figueroa score 3).
Lysholm and IKDC scores showed a sequential increase in both groups at all follow-up times, but a significantly better IKDC score was documented in AS group at 6 months (P = .022) and 12 months (P = .011). ATT, as measured by KT arthrometry, decreased in both groups. A significant difference emerged at 6 months (2.74 ± 0.65 mm for case vs 3.35 ± 0.81 mm for control; P = .023). There was no significant difference in Tegner score between groups at preinjury and 12 months (Table 1). No complications or graft failure was observed in the postoperative period until the last follow-up.
Clinicoradiological Correlation
Correlation analysis between MRI-derived parameters and clinical outcome scores was performed separately for the AS and FG groups at 3, 6, and 9 months (Table 4).
Correlation Analysis Between MRI-Derived Parameters and Clinical Outcome Scores a
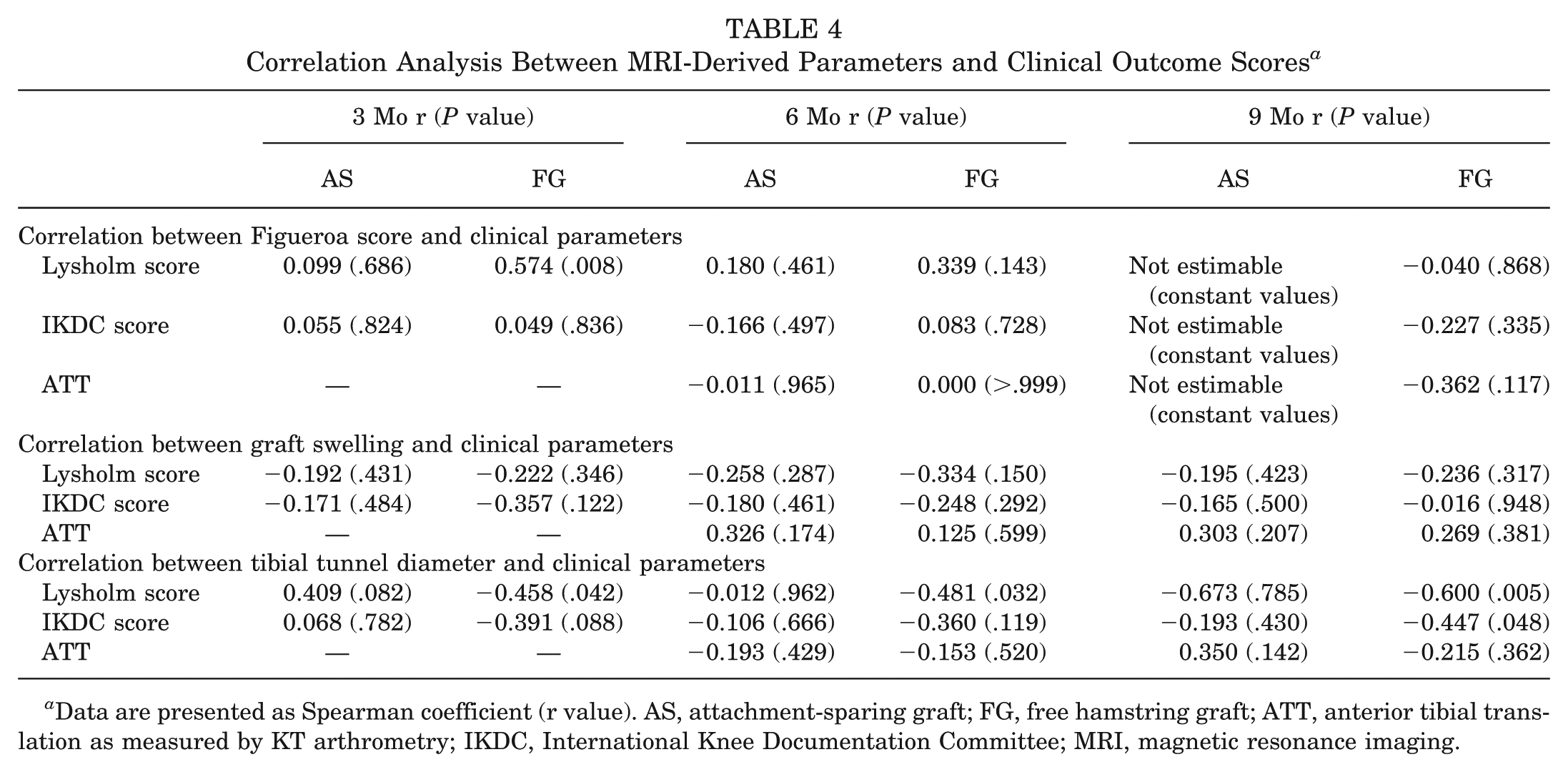
Data are presented as Spearman coefficient (r value). AS, attachment-sparing graft; FG, free hamstring graft; ATT, anterior tibial translation as measured by KT arthrometry; IKDC, International Knee Documentation Committee; MRI, magnetic resonance imaging.
In the AS group, Figueroa scores showed no correlation with Lysholm score (r = 0.099 [P = .686] at 3 months; r = 0.180 [P = .461] at 6 months) or IKDC score (r = 0.055 [P = .824] at 3 months; r = −0.166 [P = .497] at 6 months). The FG group, however, demonstrated a moderate and statistically significant positive correlation between the Figueroa and Lysholm scores at 3 months (r = 0.574; P = .008), while other associations were nonsignificant across time points.
No correlation between graft swelling and clinical outcomes was found in either group. In the AS group, graft diameter change had no correlations with Lysholm score (r = −0.192 to −0.195) or IKDC score (r= −0.171 to −0.165) over the follow-up period. Similarly, in the FG group, graft diameter did not correlate with Lysholm and IKDC scores.
No correlation between tibial tunnel diameter and clinical outcomes in the AS group was found across all timelines. Lysholm scores showed correlations ranging from r = 0.409 (P = .082) at 3 months to r = −0.012 (P = .962) at 6 months and r = −0.673 (P = .785) at 9 months. IKDC scores also demonstrated weak correlations (r = 0.068 [P = .782] to r = −0.193 [P = .430]). In the FG group, tibial tunnel diameter showed a negative correlation with Lysholm scores at 3 months (r = −0.458; P = .042), 6 months (r = −0.481; P = .032), and 9 months (r = −0.600; P = .005). IKDC scores demonstrated a significant negative correlation only at 9 months (r = −0.447; P = .048), while earlier follow-up remained nonsignificant.
KT arthrometry values did not show any significant correlation with tibial tunnel diameter, graft diameter, or MRI Figueroa scores in either group at both the 6- and 9-month follow-ups. All correlations were nonsignificant, indicating that knee laxity measured by KT arthrometry was not influenced by these radiological parameters during the postoperative period.
Discussion
The most pertinent finding of this study is that the attachment-sparing hamstring graft is associated with accelerated, earlier graft maturation, as evidenced by the maximum MRI Figueroa score of 5 in all cases of the attachment-sparing group at 9 months. A Figueroa score >3 is an indicator of graft maturation. 9 In the AS group, a Figueroa score of 4 was attained by 26.3% at 3 months and 79% at 6 months, but none in the FG group reached the same level. Although graft maturation was also a consistent finding in the FG group, the maximum Figueroa score of 5 was attained by only 10% of patients in the FG group and later in the timeline than the AS group.
The graft in the FG group underwent more swelling, as depicted by a significant increase in diameter until 6 months, after which a decrease was noticed, but the AS group showed less swelling and thus maintained smaller graft diameters throughout. This increased graft diameter in the FG group could be due to the inflammatory and revascularization response after graft necrosis of the free graft. The free graft undergoes necrosis with inflammation and inflammatory cellular accumulation with macrophages (M1) in the majority. When the ligamentization process matures the graft, it gradually becomes smaller in diameter, as shown by the improvement in the Figueroa score up to 9 months in the FG group. The observed differences in healing patterns between groups appear to emerge primarily at the 3-month period, suggesting that the differential effects of the interventions become more apparent during the early healing phase. These results contribute to the growing body of evidence regarding optimization of graft healing and early ligamentization after attachment-sparing ACLR.
The clinical outcome in terms of Lysholm, IKDC, and Tegner scores improved significantly in both groups at each sequential visit. The mean ATT and IKDC scores in the AS group were significantly better than those in the FG group at 6 months.
Similarly, the superiority of graft maturation and clinical outcome was reported by Vari et al 20 in a comparison between groups at the 1-year follow-up. However, the present study recorded clinicoradiological differences between groups prospectively at fixed sequential intervals to evaluate the differences between groups at each timepoint. It also correlated graft maturation with clinical outcome. The improvement in MRI parameters weakly correlated with improvement in all subjective and objective clinical parameters in both groups across the timeline.
Vari et al 20 used only the semitendinosus tendon, which was left attached to its tibial insertion and then folded into 4 bundles as a graft. They also applied an interference screw in the tibia. The reported technique of the current study differs in that both semitendinosus and gracilis tendons were used and no aperture fixation was done at the tibia. If an interference screw is applied to the tibia, it would crimp the graft, hampering the blood supply, providing only the mechanical benefit of stump preservation. The tibial side fixation in the present study was done as suggested by Ruffilli et al. 17
Ruffilli et al 17 reported better ligamentization at 6 months in the attachment-sparing group without any difference in clinical parameters. They suggested that an intermediate MRI evaluation be performed at 3 months to highlight the progression of the ligamentization. This parameter is fulfilled in our study. Zaffagnini et al 24 also found no difference in clinical outcome between the 2 groups. But in our study, a superior clinical outcome was documented in the AS group at 1 year, as also reported by Vari et al. 20
The graft maturation on MRI correlated to clinical outcome in a weak positive manner without statistical significance. Similar noncorrelation was reported by Bouguennec et al 2 at 2 years of follow-up. This is because the clinical outcome is multifactorial, depending on muscle strength, balance, range of motion, and psychological recovery rather than graft maturation alone. That is why there was no difference in the Tegner score at 1 year.
In addition, we noticed significant differences in tibial tunnel widening between groups, with more widening noticed in the AS group. This widening may be due to the windshield wiper effect because of surface fixation on the tibia that was away from the tibial aperture, and in the FG group, it was interference fixation. In contrast, Buda et al 3 reported a reduction in tibial tunnel diameter during follow-up of attachment-sparing ACLR. However, the clinical outcome was not noticed to be negatively affected by tibial tunnel widening in the present study. A similar noncorrelation of tunnel widening to clinical outcome was reported by DeFroda et al 6 and Eichinger et al. 8
Another drawback of this technique is dependence on adequate hamstring tendon length, especially the gracilis tendon (which is shorter than the semitendinosus tendon and is the determinant of quadrupled graft length), as the point of native tibial attachment of the hamstring is approximately 3 cm away from the external aperture of the tibial tunnel. Six patients (19%) had to be excluded because of a short graft and converted to a free hamstring graft ACLR.
We noticed that the early phase of graft healing and maturation showed weak association with improvement in clinical parameters in both groups. The strength of the study is randomized prospective sequential measurements of radiological and clinical criteria by neutral observers not involved in surgery. The differences elicited by serial analysis of both methods could translate to clinical application. This evidence of early and complete graft maturation can be utilized for accelerated rehabilitation for early return to sport, as the risk of intrasubstance tear of the graft minimizes with ligamentization.
The limitations of this study are the limited sample size, narrow age range (18-30 years), absence of female patients, different fixation techniques on the tibial side in the 2 groups, and surgery by a single surgeon, which limits generalization but also minimizes 1 confounding factor in outcome. The study's power was calculated based on Figueroa score only, so its application to other outcome measures is limited even though the differences were statistically analyzed. One aspect that needs further investigation is the difference in retear rate after reinjury post–return to sports in the long term.
Conclusion
The tibial attachment-sparing hamstring graft results in earlier and complete graft maturation on MRI in comparison to free hamstring graft for ACLR in patients 18 to 30 years of age.
Footnotes
Submitted December 8, 2025; accepted April 30, 2026.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval was obtained from Institutional Ethics Committee of Vardhman Mahavir Medical College & Safdarjung Hospital – IEC/VMMC/SJH/Project/08-2022/CC-273 dated 29-09-2022.