
Abstract
Background:
Osteochondral defects result in persistent knee pain and functional impairment, and remain a clinical challenge to repair effectively.
Purpose:
To evaluate the efficacy of an autologous inverted subchondral bone-periosteum composite graft for osteochondral reconstruction.
Study Design:
Controlled laboratory study.
Methods:
A total of 30 mature New Zealand White rabbits were randomly assigned to 3 groups: microfracture (MF) (n = 10), osteoperiosteal composite graft (OPC) (n = 10), and untreated control (n = 10). A 2 mm–diameter osteochondral defect was created in the control and MF groups and left untreated in the control group. In the MF group, microfracture was then performed by creating four 4 mm–deep perforations in the defect bed using Kirschner wires. A cylindrical osteochondral autograft (2 mm diameter × 4 mm height) was aseptically harvested from the intercondylar fossa using a calibrated coring drill only in the OPC group. Group-specific treatments included defect creation without reparative intervention (control), defect creation followed by subchondral perforation (MF), and inverted autograft implantation with periosteal wrapping (OPC). Animals were euthanized at 6 and 12 weeks postoperatively (n = 5 per group per time point) for gross and histological evaluation.
Results:
At 6 weeks, fibrocartilaginous tissue partially filled the defects in all groups. By 12 weeks, the OPC group exhibited a significant reduction in defect area compared with the preoperative baseline, with >75% of the defect depth filled, significantly outperforming the control group. Histological analysis confirmed the superior regenerative performance of the OPC group, with scores of 26.20 ± 1.48, compared with 21.80 ± 2.68 in the MF group and 15.60 ± 2.61 in controls (OPC vs MF, P = .0280; OPC vs Control, P <.0001).
Conclusion:
The osteoperiosteal composite graft promotes osteochondral regeneration by synergistically enhancing progenitor cell recruitment and chondrogenic differentiation.
Clinical Relevance:
This single-stage procedure offers a biomimetic, surgically practical, cost-effective, and arthroscopically compatible strategy for repairing osteochondral lesions.
Osteochondral lesions, often caused by trauma (eg, sports injuries) or degeneration, 11 contribute to osteoarthritis and chronic joint pain. Because of the avascular nature of mature cartilage, these defects are inherently irreparable and tend to progress to irreversible degeneration. Epidemiological data show that >19% of patients undergoing knee arthroscopy present with cartilage lesions. 1 When conservative treatments fail, surgical intervention is necessary. 39
Current surgical options include marrow stimulation (eg, microfracture), 4 autologous chondrocyte implantation (ACI), 32 and osteochondral autograft transfer (OATS). 12 However, each has important limitations. Microfracture is technically simple but often results in fibrocartilaginous repair tissue and may show inferior durability over time.19,25 ACI requires a staged procedure and is associated with a higher cost. 31 In contrast, OATS is limited by donor-site morbidity and graft availability.3,22 In clinical practice, treatment selection depends on multiple factors—including lesion size, location, tissue quality, patient symptoms, activity demands, and surgeon preference. 6 In more advanced degenerative disease, arthroplasty may be considered in selected patients, but treatment decisions are not determined by defect size alone.2,29
Osteochondral remodeling follows a pathological sequence: thinning of the subchondral plate, trabecular deterioration, and eventual sclerosis with marrow loss. 26 These changes impair biomechanics and regeneration, further hindered by dysfunctional mesenchymal progenitors in the lesion. The periosteum has shown promise in cartilage repair because of its chondrogenic potential. Its bilayer structure, with a fibrous outer layer and a cambium layer rich in multipotent progenitors, 17 supports site-specific osteochondral regeneration. 10 The periosteum, as a source of stem cells, plays a significant role in the repair process of bone and cartilage injuries. Periosteum has also been explored in human musculoskeletal repair because of its stem cell-rich cambium layer and regenerative potential. However, its clinical application remains limited by technical and biological challenges. Animal studies confirm that periosteum transplantation restores cartilage and remodels subchondral bone. One recent study also showed that periosteal grafts improve tendon-bone healing, 8 supporting their role as regenerative scaffolds when combined with viable subchondral bone. However, because of their characteristic differentiation, periosteal cells may lead to ectopic ossification, which affects joint mobility. Moreover, a simple periosteal transplantation is difficult to fix, which limits its application in the repair of bone and cartilage injuries.
In this study, we propose a novel technique involving in situ inversion of the osteochondral defect's bony core and periosteal suturing. This single-stage method creates an autologous osteoperiosteal composite scaffold as a proof-of-concept strategy for focal osteochondral repair in a rabbit model. We hypothesized that this construct would promote osteochondral regeneration by providing mechanical support and delivering progenitor cells.
Methods
Animal Study
A total of 30 male New Zealand White rabbits (mean weight, 2.5 kg; age, 2 months) were used in this study. The animals were randomly assigned to 3 groups 30 (n = 10 per group): (1) control; (2) microfracture; and (3) composite.
In the control group, a 2 mm–diameter osteochondral defect was created and left untreated (Figure 1). In the microfracture group, the same defect was first created, followed by microfracture of the defect bed using 4 Kirschner wire perforations, each 4 mm deep. No osteochondral column was removed and reimplanted in the microfracture group. In the composite group, a cylindrical osteochondral column (2 mm diameter × 4 mm depth) was harvested, inverted, reimplanted into the original defect site, and covered with periosteum (Figure 2, A-C).
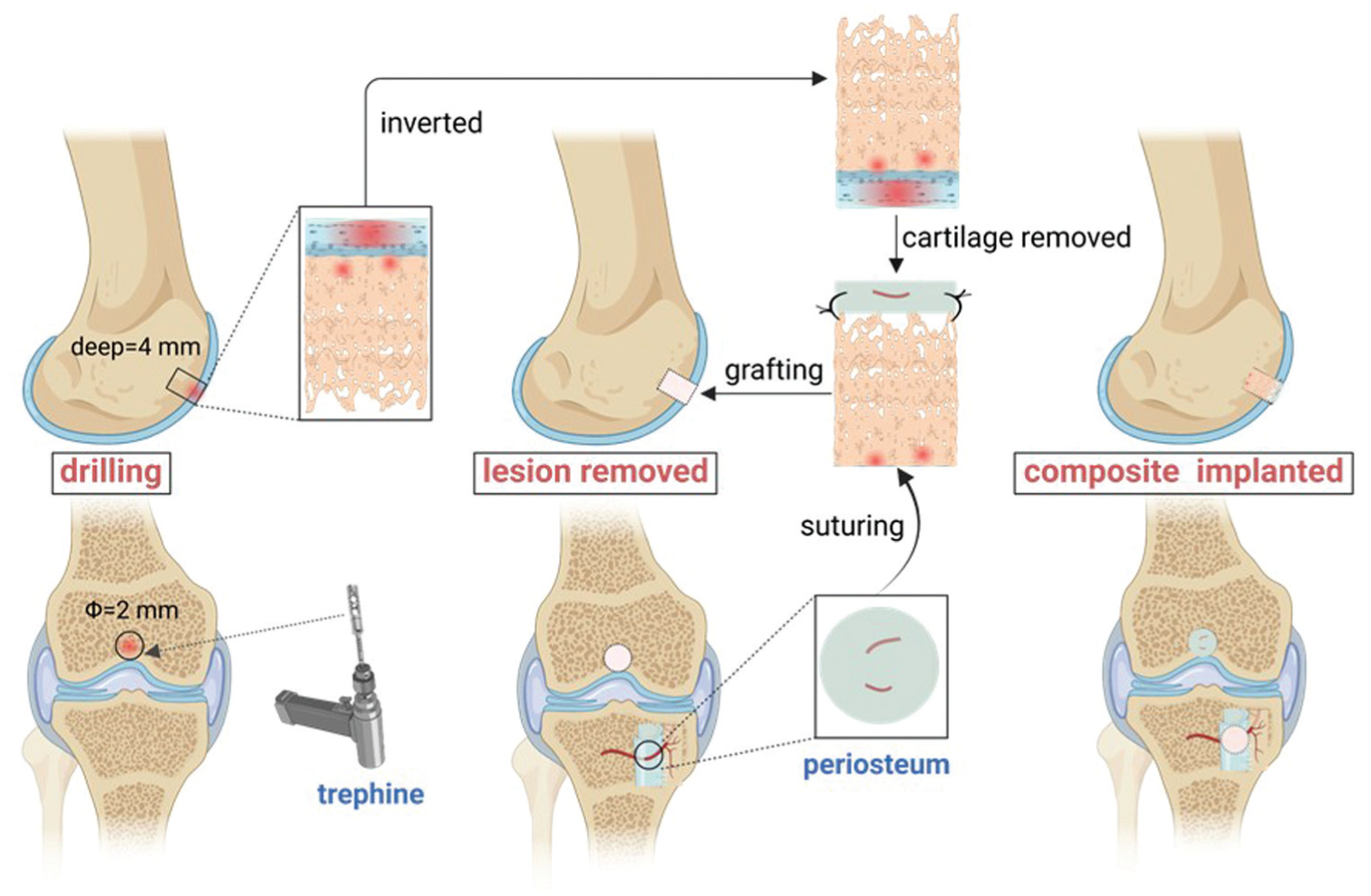
A cartilage column was carefully excised from the superior aspect of the femoral condyle. The cartilage block was inverted and placed into the cartilage defect. The periosteum was sutured to the surface of the defect.
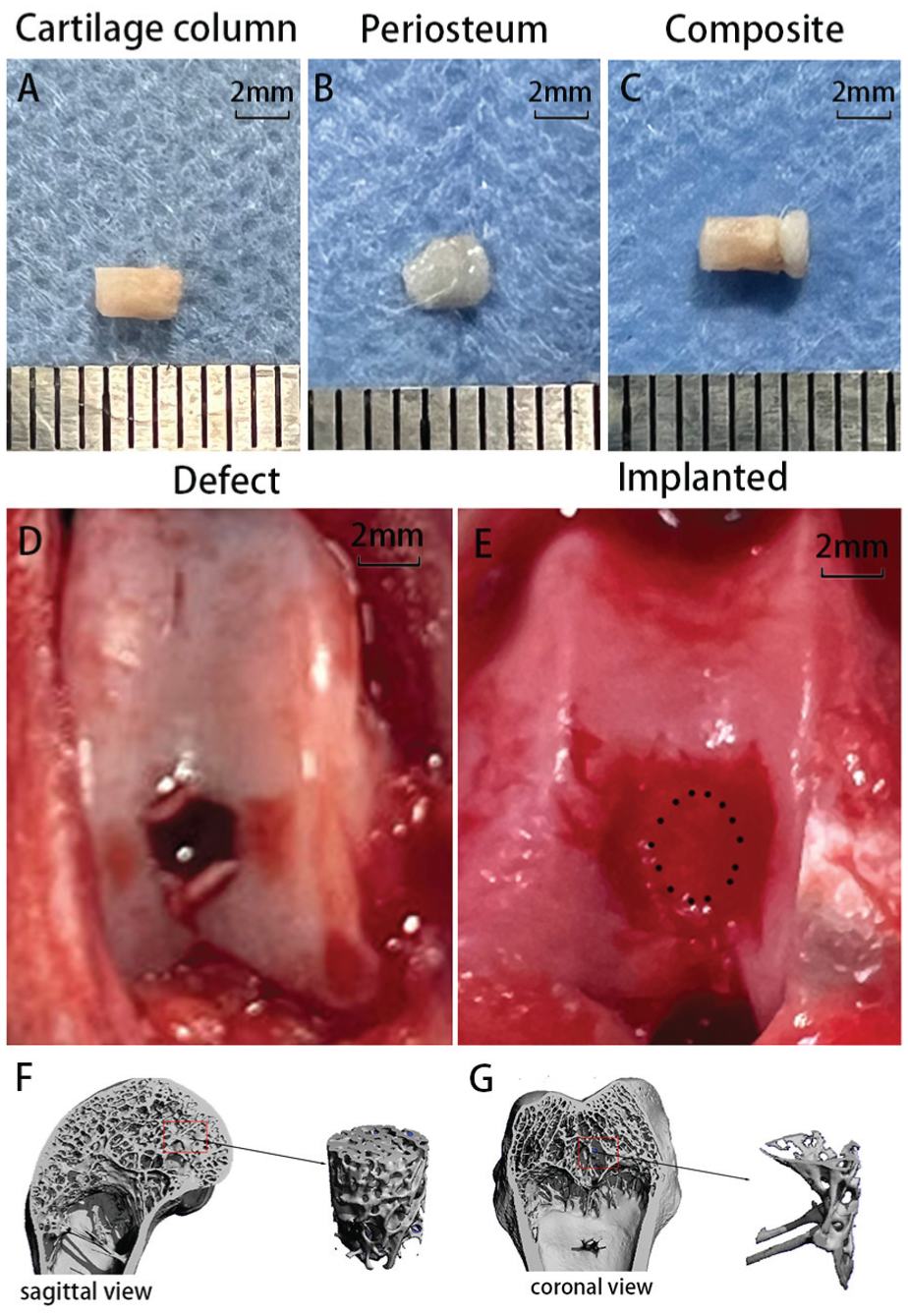
(A) Cartilage column measuring 4 mm in length and 2 mm in diameter. (B) Periosteal flap with a diameter of 2 mm. (C) Constructed cartilage-periosteum complex. (D) An osteochondral defect was created on the femoral condyle. (E) The cartilage-periosteum complex implanted into the defect site. (F) Lateral cortical bone section in sagittal view. (G) Inner cancellous bone structure in coronal view.
Animals were euthanized at 6 and 12 weeks postoperatively (n = 5 per group per time point) for gross and histological evaluation. All procedures were approved by the Institutional Animal Care and Use Committee of the Zhejiang Provincial People's Hospital (Ethics Approval No. ZJCLA-IACUC-20010627). Except for a small number of acute injuries, the occurrence and progression of osteochondral injuries are usually a chronic process of damage, and it is more common in the elderly population. This study used an acute-injury animal model solely for preliminary validation within a short timeframe to assess the therapeutic protocol proposed in this research for osteochondral injury repair.
Micro-computed Tomography
Rabbits from the 3 groups were euthanized, and the femoral condyles were carefully removed intact. All samples were analyzed using a micro-computed tomography (micro-CT) scanning system 5 (Bruker SkyScan 1176). Briefly, the specimens were scanned with a pixel size of 10 μm, a current of 250 μA, and a maximum voltage of 40 Kv. 5 After scanning, 3-dimensional images were reconstructed. The bone volume/total volume (BV/TV) fraction was calculated using dedicated software. 35
Construction of the Osteoperiosteal Composite and Implantation
All in vivo procedures were performed by a single experienced operator (Q.B.) under general anesthesia. A medial parapatellar arthrotomy was performed on both hindlimbs. After lateral dislocation of the patella, a cylindrical osteochondral column (2 mm in diameter × 4 mm in depth, Figure 2A) was harvested from the central femoral trochlear groove using a surgical micromotor system (NSK SurgicPro) equipped with a trephine bur. The superficial hyaline cartilage was subsequently removed, and the defect area was irrigated with 0.9% saline to minimize thermal damage.
The harvested osteochondral column was stored in 0.9% saline before reimplantation. The subchondral portion was inverted and implanted back into the original defect site. A 2 mm–diameter periosteal graft was harvested from the proximal tibia and sutured over the inverted column using 5-0 polydioxanone (PDS) sutures. After implantation, the patella was repositioned, and the surgical wound was closed in layers. Postoperatively, all rabbits received enrofloxacin (10 mg/kg) for 2 days and were housed individually without immobilization.
Macroscopic and Histological Evaluation
At 6 and 12 weeks postoperatively, rabbits were euthanized via intravenous injection of a lethal dose of pentobarbital sodium (Figure 3). The distal femurs were exposed, and digital images were taken to document the surgical sites. Gross repair of the defects was assessed using the International Cartilage Repair Society (ICRS) macroscopic scoring system (Appendix Table A1 range, 0-12 points, available in the online version of this article).
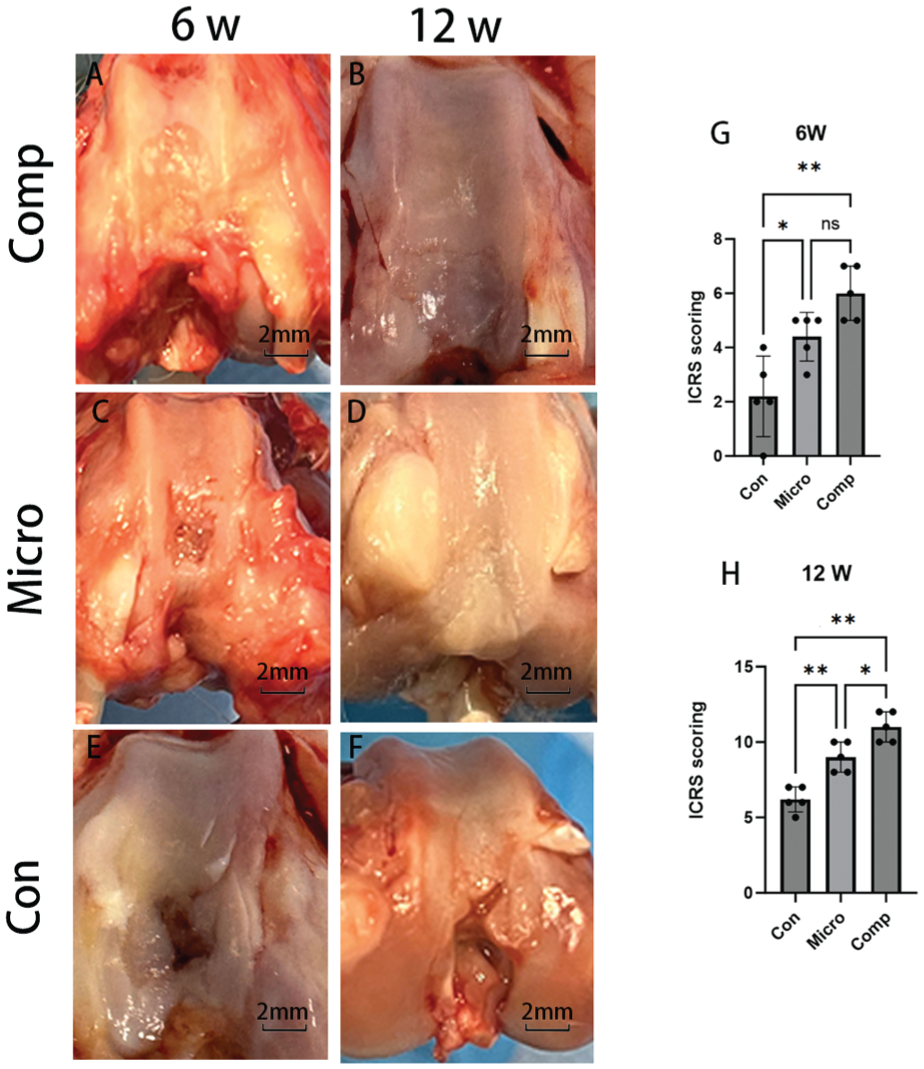
Macroscopic appearance at 6 weeks (A, C, and E) and 12 weeks (B, D, and F) postoperatively. (A and B) The composite group. (C and D) The microfracture group (E and F). The Control group. (G and H) Quantitative analysis of cartilage repair using the ICRS scoring system. Data are presented as mean ± standard deviation. Significant differences: P < .01, P < .05, ns = P > .05; n = 5 at 6 weeks, n = 5 at 12 weeks. Comp, composition; Con, control; ICRS, International Cartilage Repair Society; Micro, microfracture.
The femoral specimens were fixed in 4% paraformaldehyde in phosphate-buffered saline at 4°C for 72 hours, followed by decalcification in 20% ethylenediaminetetraacetic acid (EDTA) (pH 7.4) at 4°C for 4 weeks. Decalcified tissues were embedded in paraffin, and 4-μm-thick longitudinal sections were obtained through the center of the defect. Sections were stained with hematoxylin and eosin (H&E) and safranin O for histological evaluation. Both grafted and nongrafted sites were assessed according to the Histological Scoring System (Appendix Table A2, available online) described by Niederauer.
Statistical Analyses
Statistical analysis was conducted with SPSS 19.0 (IBM Corp), and a 2-tailed P < .05 was considered statistically significant. Gross and histological scores were independently assessed by 3 professional researchers from the Animal Research Institute of Zhejiang Provincial People's Hospital, all of whom were blinded to group allocation at the time of evaluation.
Data are presented as the mean ± standard deviation. Intergroup comparisons were performed using the Ordinary 1-way analysis of variance (ANOVA), followed by the Tukey multiple comparisons test, with a single pooled variance for pairwise comparisons separately.
Results
Micro-computed Tomography
In our in vivo study, we removed the femoral condyles of rats and observed the bone conditions of the inner and outer layers of the femur using micro-CT. We also conducted quantitative analysis on the micro-CT data. The above indicators confirmed the different bone microstructure states of cortical bone and cancellous bone. We found that the BV/TV of the cortical bone group was 23.55%, while that of the cancellous bone group was 6.12%, which was only 25.98% of the outer cortical bone (Figures 2, F and G).
Macroscopic Evaluation
At 6 weeks postoperatively, the microfracture group exhibited inadequate soft tissue filling at the defect site and only limited integration between the repair tissue and the surrounding cartilage. In contrast, the composite group showed partial graft-cartilage integration, with the defect filled by translucent, whitish tissue suggestive of early formation of cartilage-like repair tissue. Overall intergroup differences in total ICRS macroscopic scores were significant at 6 weeks (1-way ANOVA, P = .0008; Appendix Table A3, available online). The composite group also showed better surface regularity than the control group. Quantitative scores were as follows: control = 2.20 ± 1.48, microfracture = 4.40 ± 0.89, and composite = 6 ± 1. Data are presented as the mean ± standard deviation.
At 12 weeks, distinct healing patterns were evident among the groups. The control group exhibited partial defect closure, primarily filled with soft tissue, although residual defects remained. Both the microfracture and composite groups demonstrated complete defect filling with well-integrated repair tissue (Figure 3). Overall intergroup differences in total ICRS macroscopic scores remained significant at 12 weeks (1-way ANOVA, P < .0001; Appendix Table A3, available online). Quantitative scores were as follows: control = 6.20 ± 0.84, microfracture = 9 ± 1, and composite = 11 ± 1. Data are presented as the mean ± standard deviation.
Histological Evaluation
At 6 weeks, histological sections from the microfracture group showed weak Safranin O staining (Figure 5) and reduced chondrocyte density in the central graft region. In contrast, the composite group retained stronger Safranin O staining, moderate cellular proliferation, and cartilage-like morphology. Overall intergroup differences in total Niederauer histological scores were significant at 6 weeks (1-way ANOVA, P < .0001; Appendix Table A4, available online). The composite group showed more favorable structural features and Safranin O staining intensity than the control group. Data are presented as the mean ± standard deviation.
At 12 weeks, the composite group maintained robust Safranin O staining (Figure 5) and H&E staining (Figure 4), with well-preserved surface architecture and cartilage thickness similar to that of native tissue. Histology revealed seamless graft-host integration, with continuous trabecular bridging at the subchondral junction. In contrast, the microfracture group exhibited disrupted trabecular structures and reduced Safranin O staining intensity. Overall intergroup differences in total Niederauer histological scores remained significant at 12 weeks (1-way ANOVA, P < .0001; Appendix Table A4). Data are presented as the mean ± standard deviation.
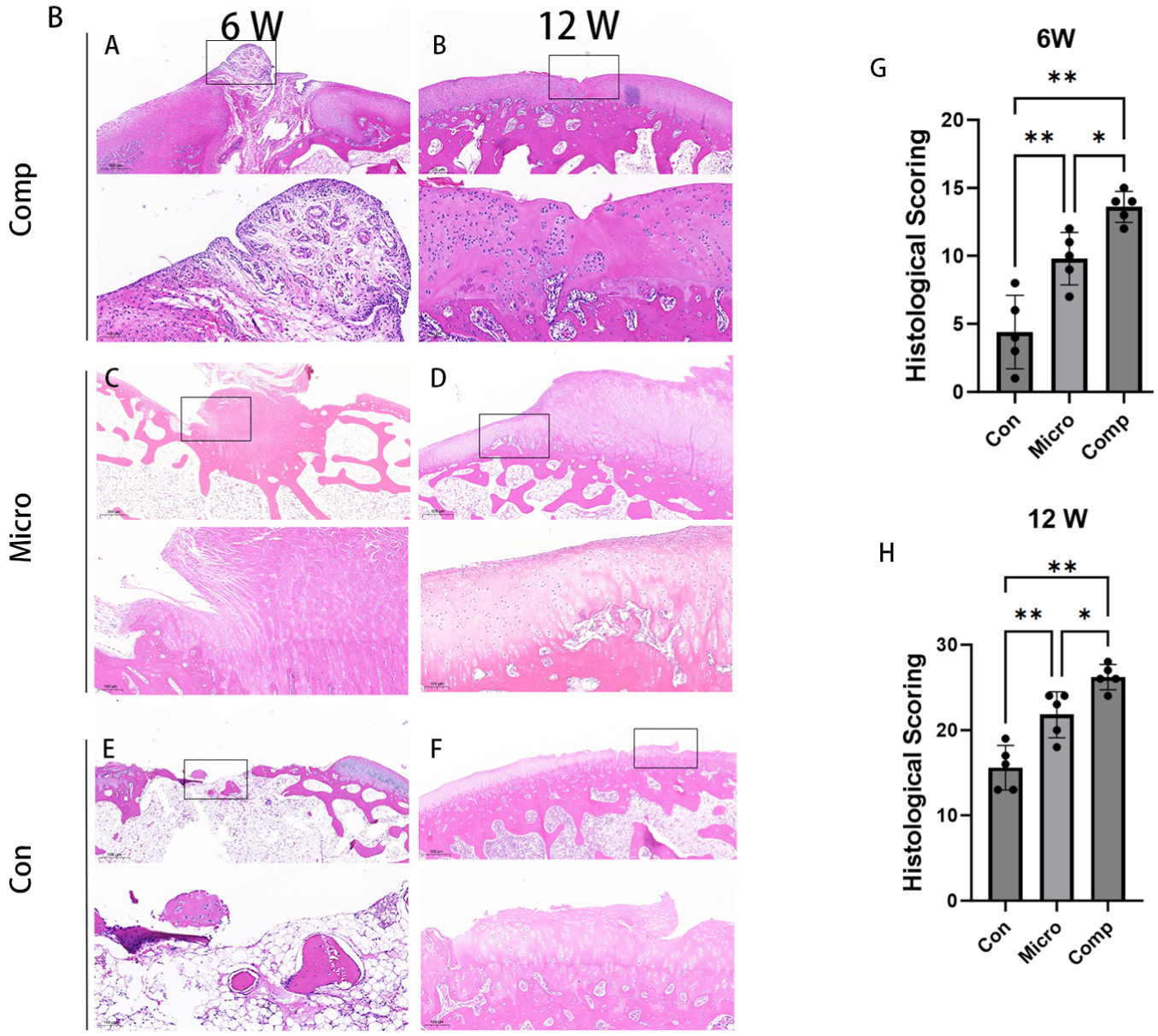
(A-F) H&E staining at 6 and 12 weeks postoperatively. Scale bar = 500 μm. (G and H) Quantitative analysis of cartilage repair using the histological scoring system of Niederauer. Data are presented as the mean ± standard deviation. Significant differences: P < .01, P < .05, ns = P > .05; n = 5 at 6 weeks, n = 5 at 12 weeks. Comp, composition; Con, control; H&E, hematoxylin and eosin; Micro, microstructure.
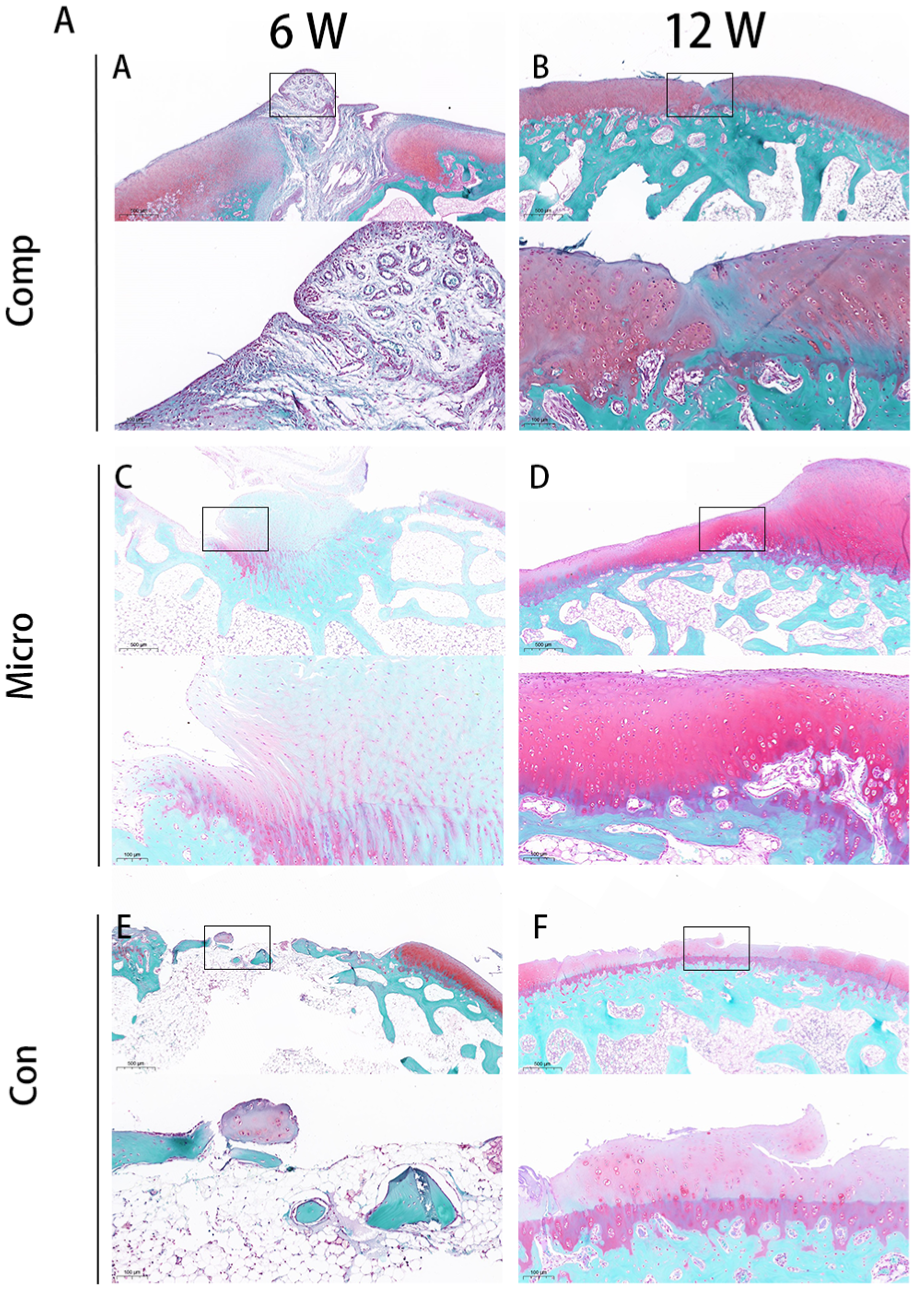
Safranin O staining at 6 and 12 weeks postoperatively. Scale bar = 500 μm. Comp, composition; Con, control; H&E, hematoxylin and eosin; Micro, microstructure.
Histological scores based on the Niederauer system further supported these findings: control = 16.60 ± 2.61, microfracture = 21.80 ± 2.68, and composite = 26.20 ± 1.48 (1-way ANOVA, P < .0001; Appendix Table A4, available online). Data are presented as the mean ± standard deviation.
Discussion
Osteochondral lesions in osteoarthritis remain a major clinical challenge. 21 This study presents a novel autologous reconstruction strategy that combines inverted osteochondral grafts with periosteal coverage, significantly enhancing regeneration. 33 The inverted graft offers a favorable microenvironment that may support osteochondral repair, while the periosteum may contribute biologically active cues through its cambium-derived stem cells. 7 Together, these components form a promising osteoperiosteal composite for osteochondral repair.
An ideal scaffold must be biocompatible, osteoconductive, and osteoinductive to support mesenchymal stem cell
The grafted cancellous matrix replaced damaged subchondral bone, thereby facilitating cartilage repair. 9 Integrating periosteum with the cancellous base created a biphasic scaffold mimicking native osteochondral tissue. In vivo, this construct promoted cartilage regeneration and seamless tissue integration. 23 The cambium layer, rich in pluripotent cells and signaling molecules, served as a natural inducer of chondrogenesis. 36 The periosteum, composed of an outer fibrous layer and an inner cambium layer, 37 has long been recognized for its regenerative properties. Recent evidence highlights its dynamic stem cell populations regulated by molecular cues. 14 Fixation orientation remains debated. However, placing the germinal layer toward the defect interface enhances chondrogenesis, likely by facilitating nutrient diffusion and cell migration. Our findings support this approach, with improved fibrocartilage formation and histological outcomes in the periosteum-augmented group.
Despite MSC multipotency, effective differentiation requires a supportive niche. 14 The osteoperiosteal group showed superior tissue quality and biomechanics, likely due to the conducive microenvironment formed. 28 All constructs were autologous, avoiding immune rejection, and ensuring excellent 27 biocompatibility and biodegradability. Unlike allografts or xenografts, which carry immunogenicity and infection risks, 16 autologous grafts offer safer alternatives, 24 although limited by donor tissue availability and surgical complexity. 15
This study has several limitations: (1) It used an acute osteochondral defect model, whereas clinical OA involves chronic degeneration 38 ; future studies should evaluate this technique in chronic or degenerative models that better reflect the clinical setting. (2) The defect used in this study (2 mm in diameter × 4 mm in depth) represented a practical focal lesion for an initial proof-of-concept experiment in the rabbit trochlea, but the study did not include a direct comparison with osteochondral autograft transfer or other established restorative procedures. Future studies using larger defect models and clinically relevant comparators, including OATS, are needed to better define the translational role of this technique. (3) Differences in rabbit and human biomechanics may limit translation, although rabbits are widely used in OA models. (4) The mechanisms of periosteal stem cell-driven chondrogenesis warrant further investigation. (5) Immunohistochemical confirmation of the repair tissue phenotype was not available in the current study. Therefore, conclusions regarding hyaline cartilage characteristics should be interpreted with caution. (6) This study was conducted exclusively in male rabbits, and sex-related differences in healing and immune responses may influence regenerative outcomes. Future studies should include both sexes to better assess the potential impact of sex on osteochondral repair. (7) This article focuses on observation rather than mechanistic investigation, and cytokine production, inflammatory markers, and other mechanistic indicators of local tissue remodeling were not evaluated in the present study. Therefore, the biological mechanisms by which this periosteal-cartilage composite graft promotes osteochondral repair remain to be clarified in future work. Nonetheless, the proposed strategy offers a promising single-stage, autologous approach to osteochondral repair.
Conclusion
Bone regeneration is strongly regulated by the physicochemical microenvironment. This study demonstrates that autologous osteochondral-periosteal transplantation, combining periosteum-derived stem cells, an autologous subchondral bone scaffold, and local growth factors, effectively enhances osteochondral repair in the knee. This integrated, single-stage approach meets key tissue-engineering criteria and offers a promising strategy for treating degenerative cartilage lesions with high clinical-translational potential.
Supplemental Material
sj-pdf-1-ajs-10.1177_03635465261456227 – Supplemental material for A Novel Autologous Osteoperiosteal Composite for Osteochondral Regeneration
Supplemental material, sj-pdf-1-ajs-10.1177_03635465261456227 for A Novel Autologous Osteoperiosteal Composite for Osteochondral Regeneration by Longtao Yao, Senbo Zhu, Yifan Wu, Gangcheng Ye, Guorong Wang, Zexuan Niu, Sheyuan Ding, Zhihui Xiang, Qiong Zhang, Qing Bi and Prof Ruijian Yan in The American Journal of Sports Medicine
Footnotes
Submitted August 13, 2025; accepted April 19, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was supported by the Zhejiang Provincial Medical and Health Science and Technology Project (2024KY1083, 2021KY506, 2021KY035, 2020KY029), the Zhejiang Provincial Basic Public Welfare Research Program (LBY24H180001, LY22H060002, LGF20H280011), and the Key R&D Project of the Zhejiang Provincial Science and Technology Department (2021C03078).
Ethical approval was obtained from the Institutional Animal Care and Use Committee of the Zhejiang Provincial People's Hospital (Ethics Approval No. ZJCLA-IACUC-20010627).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.