
Abstract
Background:
Preoperative quadriceps and hamstring muscle weakness may predispose patients to strength deficits and prolonged recovery in the setting of anterior cruciate ligament (ACL) injury. Three-dimensional (3D) magnetic resonance imaging (MRI) analysis has been developed to provide a comprehensive assessment of the thigh musculature.
Purpose:
To (1) describe the magnitude of quadriceps and hamstring muscle weakness relative to the uninjured limb preoperatively in patients with known ACL tears, and (2) determine if preoperative quadriceps and hamstring muscle volume correlate with quadriceps knee extension strength and hamstring knee flexion strength.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Patients undergoing primary ACL reconstruction (ACLR) underwent MRI scans of the bilateral lower extremities and strength testing preoperatively within 7 days of ACLR. Three-dimensional MRI–based autosegmentation was used to measure the volume of individual quadriceps and hamstring muscles. Preoperative knee extension and flexion strength were assessed isometrically at 90° and isokinetically. Linear mixed-effects models were used to assess muscle volume by limb interaction effect on strength. Pearson correlation coefficients (r) were used to assess the association between muscle volume and strength in the injured and uninjured limbs.
Results:
In total, 72 patients were included (mean age, 26.6 ± 8.8 years; 64% male) with the median time to preoperative strength assessment and MRI within 90 days of injury. Comparing the ACL-injured limb to the uninjured limb, isometric knee extension and flexion strength demonstrated mean limb symmetry indices (LSIs) of 80.1% ± 18.5% (P < .001) and 83.7% ± 17.7% (P < .001), respectively. Additionally, measured quadriceps and hamstring volume demonstrated mean LSIs of 89.9% ± 8.8% (P < .001) and 95.4% ± 4.6% (P < .001), respectively. There was moderate to strong positive associations between individual muscle volume and strength in both the injured and uninjured limbs, regardless of the mode of strength assessment (r = 0.43-0.84; all P < .001).
Conclusion:
Preoperatively, a 20% deficit in isometric knee extension strength and a 10% deficit in quadriceps muscle volume was noted in the ACL-injured knee compared to the uninjured limb. A moderate to strong correlation between quadriceps strength and each individual quadriceps muscle volume measured by a 3D MRI platform was observed before ACLR. Findings suggest the utility of automated 3D MRI volumetric segmentation as an adjunct to complement formal preoperative strength assessment. Additionally, this method may be used to identify patients at risk for delayed and/or degraded functional outcomes after ACLR.
Keywords
Persistent quadriceps weakness after anterior cruciate ligament (ACL) reconstruction (ACLR) is common and has been acknowledged as a risk factor for persistent functional deficits after surgery.4,22 Eitzen et al 8 evaluated a cohort of 60 patients treated with bone–patellar tendon–bone (BTB) autograft for ACL injury and demonstrated that patients with preoperative quadriceps strength deficit >20% based on isokinetic knee extension strength testing continued to have persistent strength deficits 2 years after ACLR compared to the uninjured limb. Furthermore, Kim et al 11 demonstrated worse functional scores at 1 year post-ACLR based on severity of preoperative quadriceps strength deficit. Logerstedt et al 16 found preoperative quadriceps strength to be a positive predictor of self-reported International Knee Documentation Committee scores 6 months postoperatively after ACLR with hamstring autograft or allograft. Together, these studies suggest that there may be utility in preoperative assessments of quadriceps strength as a means of identifying patients who are at risk for worse functional outcomes after ACLR.
Multiple studies have indicated that increased quadriceps strength of the operative extremity both preoperatively and postoperatively is associated with improved subjective outcomes within 1 year after ACLR.1,4,7,8,12,17,23 Conversely, quadriceps muscle weakness has been associated with worse patient-reported outcome measures, lower rates of return-to-sport participation, and alterations in knee biomechanics 22 across a multitude of dynamic tasks including walking, 23 running1,12 and jumping. 17 While persistent quadriceps muscle weakness represents a key component in the ability of patients to return to their preinjury level of function and/or sport, there are fewer clear implications of how preoperative quadriceps weakness influences recovery after ACLR.
Isometric or isokinetic knee extension and flexion strength assessments, as measured by electromechanical dynamometers, represent the gold standard for assessing thigh muscle strength in patients undergoing ACLR. 3 However, such measurements may not be feasible either due to institutional limitations or in cases in which the patients’ capacity to participate in testing is limited secondary to pain and/or limited knee range of motion preoperatively. In light of these limitations, magnetic resonance imaging (MRI)–based analyses of thigh muscle volume have shown promise as either an adjunct or outright alternative to measurements of isometric and isokinetic strength. However, previously described MRI-based approaches using 2-dimensional (2D) assessments of thigh muscle volume estimated from cross-sectional area are limited in their ability to quantify the entirety of muscle units. Additionally, these measurements, commonly referred to as “segmentations,” are labor-intensive and costly, which limits their integration into routine clinical practice. Subsequent advancements in similar technology involving 3-dimensional (3D) measurements of thigh muscle volume using automatic segmentation performed by artificial intelligence (AI) address these shortcomings. 24 A deep learning algorithm for automatic 3D segmentation of hamstring musculotendon injury, 24 lower leg muscle, 26 and rotator cuff muscle 25 volume has proven to be feasible and comparable to ground-truth segmentation.
Thus, the novel 3D approach using automated segmentation is a comparable alternative to traditional approaches for strength measurements and could be more readily implemented in clinical practice as a means to identify patients at risk for post-ACLR muscle weakness. To date, this novel approach has not been validated against the objective isometric and isokinetic strength testing. Therefore, the purpose of this study was to determine if preoperative quadriceps and hamstring muscle volumes as measured by a novel 3D autosegmentation MRI–based assessment correlate with knee extension strength and knee flexion strength. It was hypothesized that quadriceps muscle volume would strongly correlate with knee extension strength in patients indicated for ACLR. Thus, 3D MRI–based automated segmentation may serve as a complement to traditional strength testing and provide an alternative approach as a means to identify patients at risk for post-ACLR muscle weakness.
Methods
Patient Selection
This study is a secondary analysis of cross-sectional data collected as part of a single-center randomized clinical trial that has been registered at ClinicalTrials.gov (ID No. NCT04519801). Specifically, this study utilized presurgical baseline data only. A cohort of patients between 15 and 45 years of age who sustained ACL tears indicated for primary ACLR were recruited and enrolled for this study between August 2022 and January 2025. All patients were diagnosed with an ACL tear based on a known injury with physical examination findings (abnormal Lachman, anterior drawer, and/or pivot-shift test) and a knee MRI study consistent with a complete ACL tear. Exclusion criteria consisted of revision ACLR procedures, bilateral knee injuries, multiligamentous knee injuries, and/or concomitant procedures at the time of ACLR that necessitated a nonweightbearing status postoperatively. This study was approved by the institutional review board and complied with Health Insurance Portability and Accountability Act guidelines. All patients provided written informed consent.
Preoperative Strength Testing
Preoperative knee extension and flexion strength was assessed isometrically at 90° of knee flexion and isokinetically at 60 deg/s and 180 deg/s using an isokinetic dynamometer within 7 days preoperatively of ACLR (Biodex System 4; Biodex Medical Systems) with torque sampled at 100 Hz. No patients were formally prescribed preoperative physical therapy. The hip was positioned at 85° of flexion. To standardize testing, patients underwent testing with supervision of the senior-level physical therapist, who provided instruction on how to perform assessments. For isometric and all isokinetic assessments, patients completed 3 submaximal effort practice repetitions (50%, 75%, and 90% of perceived maximal effort), followed by 2 maximal effort practice repetitions. After the practice set was completed, patients were given 2 minutes of rest. For maximal voluntary isometric contractions, a minimum of 3 repetitions were performed. Additional repetitions were completed if a continual increase in torque was observed between repetitions. For isokinetic testing, 5 repetitions of maximal concentric knee extension and flexion efforts were completed at 60 deg/s and 180 deg/s. Maximal knee extension and flexion torque were characterized by the highest value recorded across all 5 repetitions, normalized to body mass (N·m/kg), and used for the final analysis.
Three-Dimensional Segmentation and Volumetric Analysis of Quadriceps and Hamstring Musculature
All patients completed an MRI study within 7 days preoperatively of ACLR. MRI scans were acquired using a 3D axial spin-echo T1-weighted sequence capturing continuously from the L1 vertebra to the ankle joint bilaterally. Patients were scanned on a GE Medical Systems 3T Discovery MR750 MRI Scanner. The scan time was approximately 15 to 20 minutes per patient for muscle segmentation. The scanning parameters used include TE/TR/α of 3.38 msec/550 msec/70, field of view of 480 mm × 480 mm, slice thickness of 5 mm, and in-plane spatial resolution of 1.875 mm × 1.875 mm.
MRI scans were preprocessed to produce continuous, axial 3D images for all patients. Muscles and bones were then segmented from the images via labeling of each pixel using a combination of an AI-based algorithm and manual quality assurance (Springbok Analytics).9,20 The AI segmentation pipeline employed a modified 3D U-Net convolutional neural network architecture, trained to delineate muscle and bone boundaries from the MRI scans. All AI-generated segmentation labels were subsequently reviewed and refined by trained segmentation engineers using 3D Slicer to ensure anatomic accuracy and consistency across patients. In total, 88 individual muscles and bones were segmented for each patient. For this study, the quadriceps musculature (rectus femoris [RF], vastus medialis [VM], vastus intermedius, and vastus lateralis [VL]) and hamstring musculature (biceps femoris short head and long head, semimembranosus, and semitendinosus muscles) were the focus (Figure 1). Muscle volume was found by summing the total number of pixels labeled for that segmented muscle's boundary and multiplied by the pixel's voxel volume. All volumes were normalized to the height and mass product. Asymmetry was computed as the percent difference in muscle volume between the injured and uninjured sides, defined as the limb symmetry index (LSI).
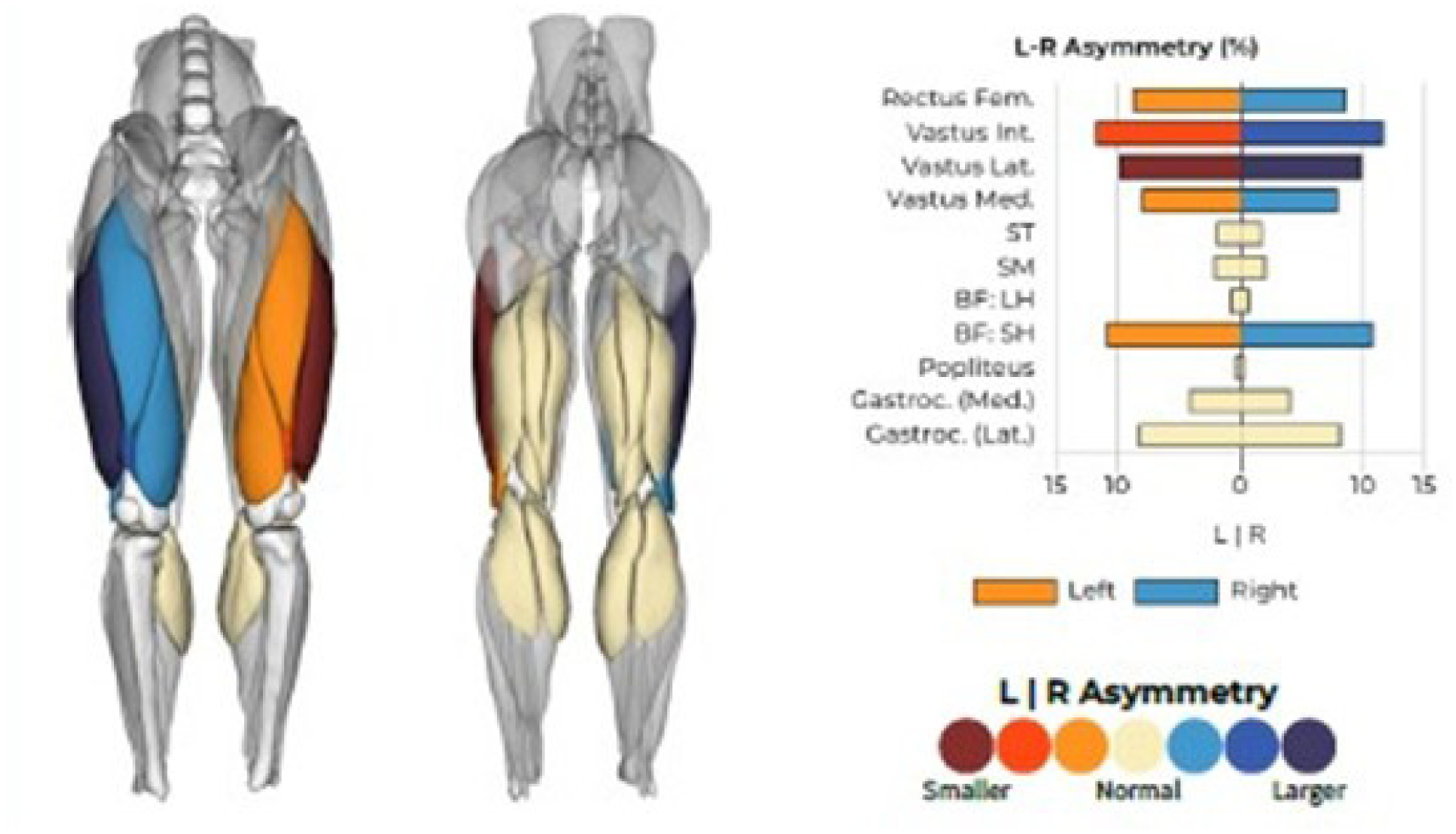
Demonstration of 3-dimensional magnetic resonance imaging volumetric segmentation of the quadriceps and hamstrings musculature and comparison of symmetry between the injured and uninjured limbs. The muscles are color-coded to represent their asymmetry levels, with darker colors indicating greater asymmetry. Blue signifies the larger side, while red represents the smaller side. These color thresholds are muscle specific and were determined by analyzing the typical asymmetry levels of each muscle in a cohort of healthy adults and calculating deviations from the mean. 9 BF:LH, biceps femoris, long head; BF:SH, biceps femoris, short head; L, left; R, right; Rectus Fem, rectus femoris; SM, semimembranosus; ST, semitendinosus; Vastus Int, vastus intermedius; Vastus Lat, vastus lateralis; Vastus Med, vastus medialis.
Statistical Analysis
Pearson correlation coefficients (r) were used to assess the association between quadriceps and hamstring muscle volume and strength in both the injured and uninjured limbs. An a priori power analysis (power = 0.8; alpha = .05) determined that a sample of 64 patients was needed to detect an r value of 0.3. Standard criteria were used to indicate the strength of correlation as weak (r < [0.39]), moderate (r = [0.4] to [0.69]), or strong (r > [0.7]). 27 For visualization, scatterplots and simple linear regression by limb were plotted for the comparison of strength to muscle volume measures. With limb, muscle volume, and their interaction included as fixed effects, linear mixed-effects models were used to assess for a muscle volume by limb interaction effect on strength, and the patient was included as the random effect. If a significant interaction was not observed, it was removed from the model. Marginal R2 values (total variance explained by the fixed effects) are reported. 19 A statistical level of significance of alpha value <.05 was used. Analyses were conducted using R (Version 4.4.0; R Foundation for Statistical Computing).
Results
Patient Characteristics
A total of 72 patients, 46 males (64%) and 26 females (36%), were included in the final analysis with a mean age of 26.6 ± 8.8 years (Table 1). The median times from injury to preoperative strength testing and MRI were 94 days (IQR, 53, 158 days) and 90 days (IQR, 53, 160 days), respectively. MRI was performed at a median of 1 day (IQR, −1, 1.25 days) before strength testing. Means, standard deviations, and LSIs are reported for all strength and muscle volume measures in Table 1. Comparing the ACL-deficient knee to the uninjured limb, isometric knee extension and flexion strength demonstrated mean LSIs of 80.1% ± 18.5% (P < .001) and 83.7% ± 17.7% (P < .001), respectively. Additionally, quadriceps and hamstring muscle volumes demonstrated mean LSIs of 89.9% ± 8.8% (P < .001) and 95.4% ± 4.6% (P < .001), respectively. There was a significant difference in LSI among muscle volume comparison of the ACL-deficient knee to the uninjured limb in all the individual quadriceps and hamstring musculature (all P < .02), except for the short head of the biceps femoris muscle (P = .53).
Patient Characteristics a
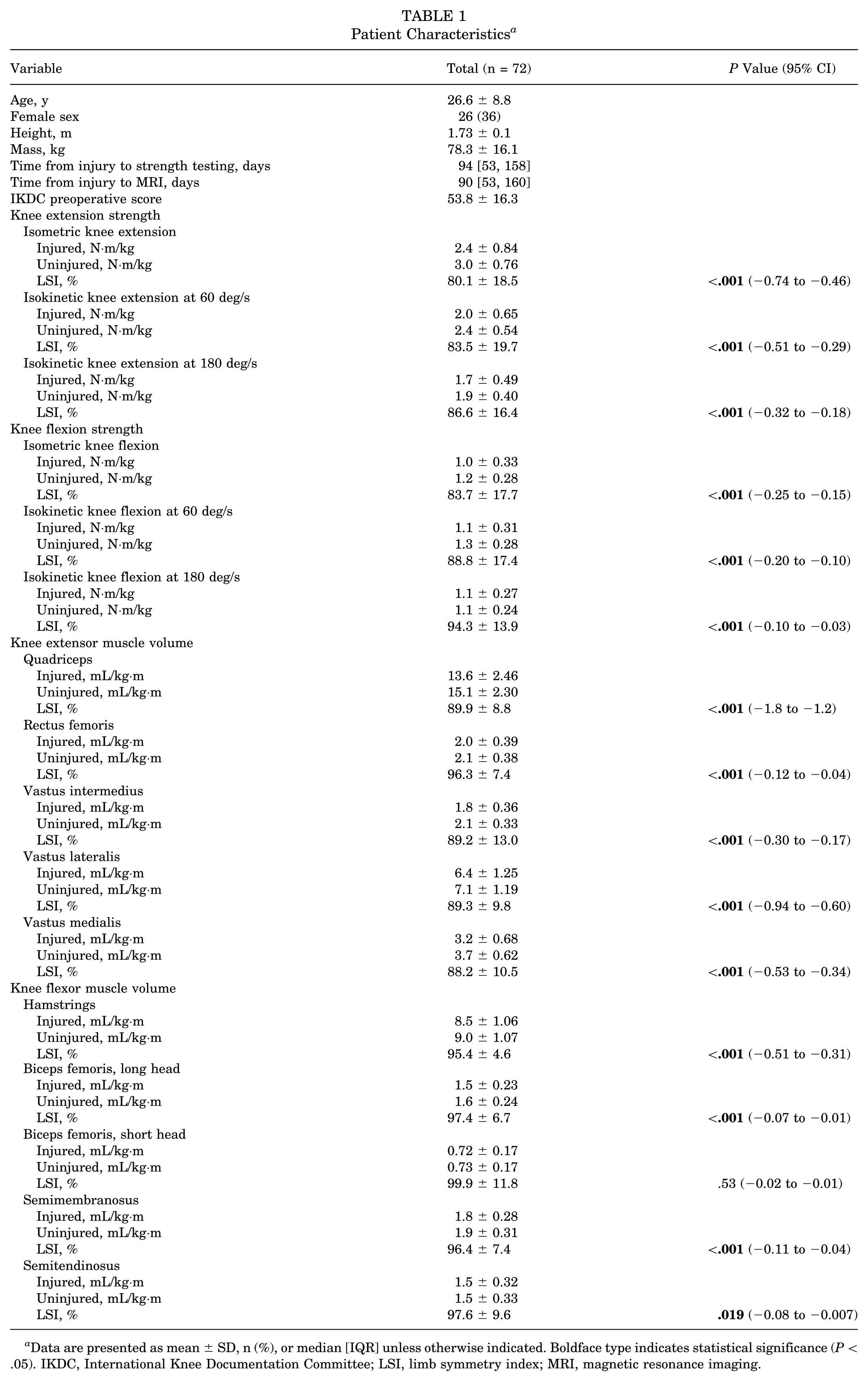
Data are presented as mean ± SD, n (%), or median [IQR] unless otherwise indicated. Boldface type indicates statistical significance (P < .05). IKDC, International Knee Documentation Committee; LSI, limb symmetry index; MRI, magnetic resonance imaging.
Limb by Strength Assessment
Based on the linear mixed-effects models, there were no significant limb by muscle volume interaction effects detected (all P > .19) (Supplemental Table 1). As such, the relationship (slope) between muscle volume and strength metrics did not differ between the injured and uninjured limbs. For the combined quadriceps muscle volume influence on quadriceps strength (isometric), there was a significant effect observed for muscle volume (P < .001) and limb (P = .03). For every 1.0 mL/kg·m there was an associated 0.30-N·m/kg (95% CI, 0.26-0.33) increase in quadriceps strength (isometric) when accounting for limb. The injured limb had a mean lower quadriceps strength of 0.15 N·m/kg (95% CI, 0.05-0.24) compared to the injured limb, when accounting for quadriceps muscle volume. The overall model explained 74% of the variance in quadriceps strength (isometric). This general relationship can be appreciated in Figure 2, where the lines for the injured and uninjured limbs have the same slope (no interaction effect), but the injured limb is slightly lower than the uninjured limb (limb main effect). Fixed effects and marginal R2 values for each model are reported in Supplemental Table 2 for isokinetic 60 deg/s and Supplemental Table 3 for isokinetic 180 deg/s.
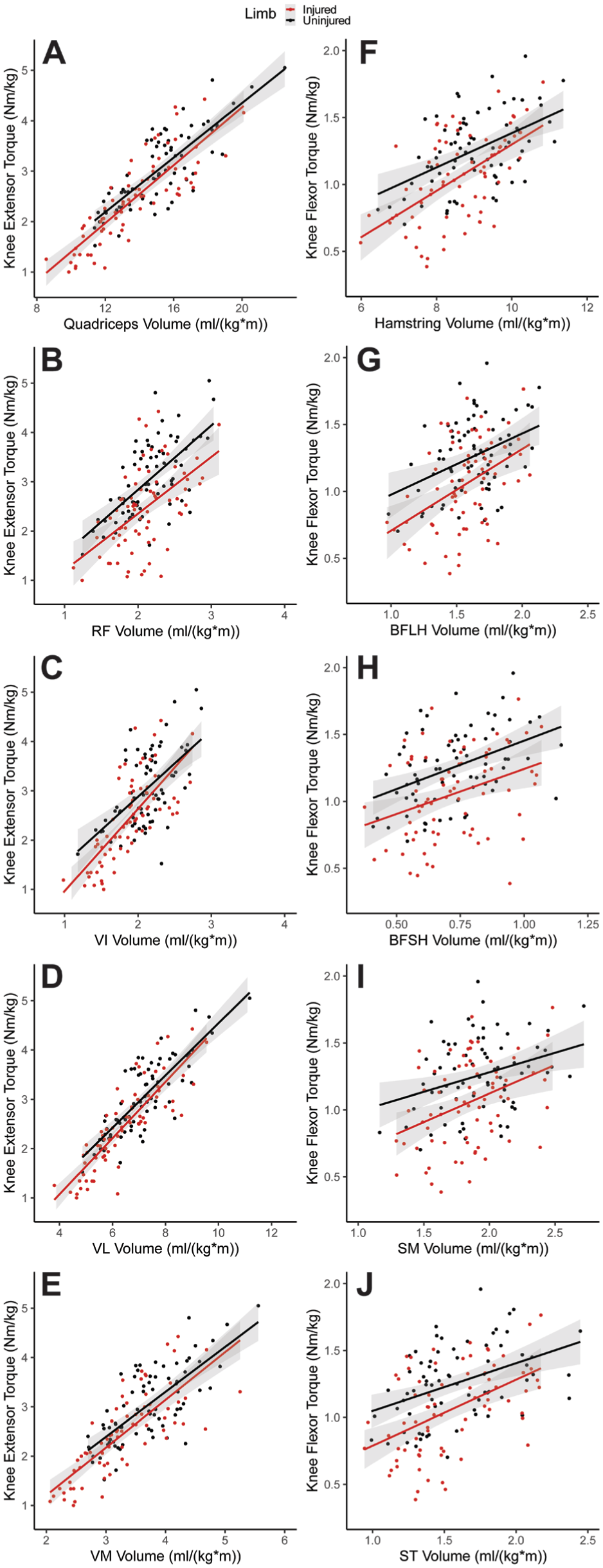
The linear relationship (A-E) between isometric knee extension strength and all quadriceps muscle volumes and (F-J) between isometric knee flexion strength and all hamstring muscle volumes. BFLH, biceps femoris, long head; BFSH, biceps femoris, short head; RF, rectus femoris; SM, semimembranosus; ST, semitendinosus; VI, vastus intermedius; VL, vastus lateralis; VM, vastus medialis.
Quadriceps Muscle Volumetric Analysis
In evaluation of the injured limb, the strongest correlation between quadriceps volume and strength was observed with the VL, which demonstrated a strong positive correlation in terms of preoperative knee extension strength at 90° isometric (r = 0.85; 95% CI, 0.77-0.90), 60 deg/s isokinetic (r = 0.78; 95% CI, 0.66-0.85), and 180 deg/s isokinetic (r = 0.80; 95% CI, 0.70-0.87) testing (all P < .001) (Table 2). The weakest correlation was observed with RF in terms of preoperative knee extension strength, demonstrating a moderate correlation at 90° isometric (r = 0.53; 95% CI, 0.34-0.68), 60 deg/s isokinetic (r = 0.51; 95% CI, 0.32-0.67), and 180 deg/s isokinetic (r = 0.55; 95% CI, 0.36-0.69) testing (all P < .001).
Preoperative Muscle Volume and Strength of Quadriceps Musculature in Injured and Uninjured Limbs Before ACLR a
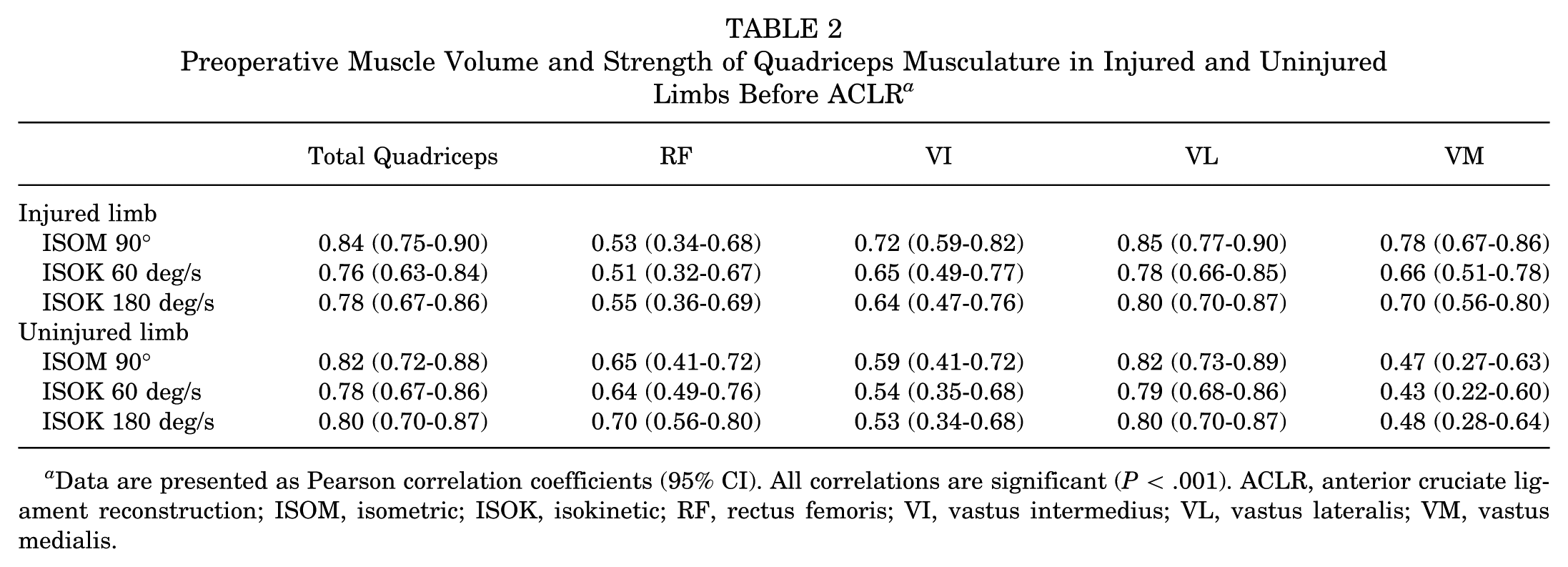
Data are presented as Pearson correlation coefficients (95% CI). All correlations are significant (P < .001). ACLR, anterior cruciate ligament reconstruction; ISOM, isometric; ISOK, isokinetic; RF, rectus femoris; VI, vastus intermedius; VL, vastus lateralis; VM, vastus medialis.
In evaluation of the uninjured limb, the strongest correlation between quadriceps volume and preoperative knee extension was also established with VL, which demonstrated a strong positive correlation in terms of preoperative knee extension strength at 90° isometric (r = 0.82; 95% CI, 0.73-0.89), 60 deg/s isokinetic (r = 0.79; 95% CI, 0.68-0.86), and 180 deg/s isokinetic (r = 0.80; 95% CI, 0.70-0.87) testing (all P < .001) (Table 2). The weakest correlation was established with VM in terms of preoperative knee extension strength, demonstrating a moderate correlation at 90° isometric (r = 0.47; 95% CI, 0.27-0.63), 60 deg/s isokinetic (r = 0.43; 95% CI, 0.22-0.60), and 180 deg/s isokinetic (r = 0.48; 95% CI, 0.28-0.64) testing (all P < .001). Across all modes of knee extension strength assessments, the total quadriceps muscle volume demonstrated a strong positive association with preoperative strength (r = 0.76-0.84; all P < .001). The relationships between isometric knee extension strength and all quadriceps muscle volumes are represented in Figure 2 (A-E) as scatterplots and simple linear regressions. Isokinetic plots for the quadriceps musculature are visualized in Supplemental Figure 1.
In evaluation of the injured limb, knee flexion strength had the strongest correlation with the biceps femoris and semitendinosus muscle volumes, which demonstrated a moderate positive correlation in terms of preoperative knee flexion strength at 90° isometric, 60 deg/s isokinetic, and 180 deg/s isokinetic testing (P < .001) (Table 3). A weak correlation was established with the semimembranosus muscle in terms of preoperative knee flexion strength at 90° isometric (r = 0.36; 95% CI, 0.15-0.55), 60 deg/s isokinetic (r = 0.29; 95% CI, 0.07-0.49), and 180 deg/s isokinetic (r = 0.33; 95% CI, 0.10-0.52) testing (all P < .01).
Preoperative Muscle Volume and Strength of Hamstring Musculature in Injured and Uninjured Limbs Before ACLR a
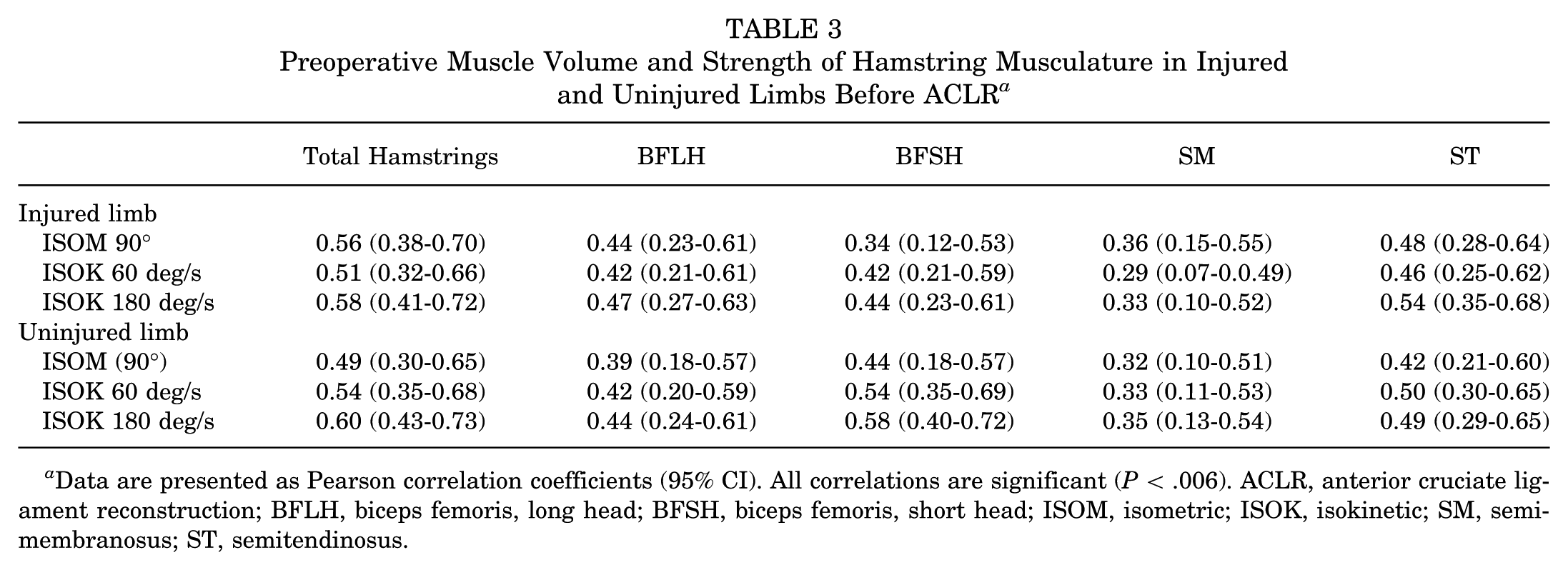
Data are presented as Pearson correlation coefficients (95% CI). All correlations are significant (P < .006). ACLR, anterior cruciate ligament reconstruction; BFLH, biceps femoris, long head; BFSH, biceps femoris, short head; ISOM, isometric; ISOK, isokinetic; SM, semimembranosus; ST, semitendinosus.
Similarly, in evaluation of the uninjured limb, there was a moderate positive correlation between the hamstring volume of the biceps femoris and semitendinosus muscles and preoperative knee flexion strength at 90° isometric, 60 deg/s isokinetic, and 180 deg/s isokinetic testing (all P < .006) (Table 3). A weak correlation was also demonstrated in the uninjured limb of the semimembranosus muscle in terms of preoperative knee flexion strength at 90° isometric (r = 0.32; 95% CI, 0.10-0.51), 60 deg/s isokinetic (r = 0.33; 95% CI, 0.11-0.53), and 180 deg/s isokinetic (r = 0.35; 95% CI, 0.13-0.54) testing. Across all modes of knee flexion strength assessments, the total hamstring muscle volume demonstrated a moderate positive association with preoperative knee flexion strength (r = 0.49-0.60; P < .001). The relationships between isometric knee flexion strength and all hamstring muscle volumes are visualized in Figure 2 (F-J). Isokinetic plots for the hamstring musculature are visualized in Supplemental Figure 2 (available in the online version of this article).
Discussion
The purpose of the current study was to determine if preoperative quadriceps and hamstring muscle volumes as measured by a novel MRI-based 3D autosegmentation technique correlated with knee extension and flexion muscle strength. Moderate to strong correlations between 3D MRI measurements of preoperative muscle volume and strength were observed in a population of patients indicated for ACLR. Thus, our hypothesis was confirmed. These results validate the use of this AI-automated image-based modality in assessing preoperative muscle function and as an adjunct to improve the identification of patients at risk for persistent post-ACLR strength deficits and worse functional outcomes.
Both isometric and isokinetic assessments have been described to assess quadriceps strength post-ACLR. 2 Isometric testing is performed at a single, fixed joint angle to quantify peak torque, whereas dynamometers can be utilized to perform isokinetic testing of knee extension torque throughout the knee range of motion.5,6,29,30 In a direct comparison of isometric and isokinetic assessments in knee extension, Cobian et al 3 demonstrated strong agreement between the 2 modalities, supporting the use of either contraction type for clinical strength assessment in athletes after ACLR. While isokinetic and isometric strength assessments are a direct measure of torque production ability, these measurements can also be influenced by factors other than muscle volume, such as neural activation and pain inhibition. Deficits in these measures of quadriceps muscle strength among patients with ACL injuries have previously been observed.7,15 We observed a 20% mean deficit in isometric knee extension strength testing (LSI: 80.1% ± 18.5%; P < .001; 95% CI, −0.74% to −0.46%) and a 10% deficit in quadriceps volume (LSI: 89.9% ± 8.8%; P < .001; 95% CI, −1.8% to −1.2%) compared to the uninjured limb. These data corroborate previous observations made in comparably sized cohorts and should amplify awareness for the prevalence of these preoperative deficits, which have been shown to drive postoperative functional outcomes.
While moderate to strong correlations between 3D MRI measurements of preoperative quadriceps and hamstring muscle volume and strength were observed in the patient cohort, quadriceps muscle volume demonstrated a stronger positive correlation with knee extension strength testing (r = 0.42-0.86) compared to the hamstring muscle volume correlation with knee flexion strength testing (r = 0.26-0.64) across all modes of strength assessment and limb in our current study. We observed weaker correlations among hamstring muscle volumes and knee flexion strength across all modes of strength assessment and limbs. Additionally, we observed diminished magnitudes of strength deficits with respect to hamstring strength and muscle volume, with a 15% deficit in isometric knee flexion strength testing (LSI: 83.7% ± 17.7%; P < .001; 95% CI, −0.25% to −0.15%) and a 5% deficit in hamstring volume (LSI: 95.4% ± 4.6%; P < .001; 95% CI, −0.51% to −0.31%) compared to the uninjured limb These findings suggest that deficits in quadriceps musculature volume may be more representative of associated strength deficits as compared to hamstring musculature. This may be explained by the majority of the quadriceps musculature being uniarticular compared to the majority of the hamstring musculature, which is biarticular. The hamstrings (except the short head of the biceps femoris muscle) cross both the hip and knee joints, so in vivo operating lengths depend on simultaneous hip and knee angles, where hip flexion changes fiber length far more than knee flexion alone. 10 This biarticular complexity and resulting length-tension variability reduce the direct predictability of total hamstring volume to isolated knee flexion strength—unlike the quadriceps, where functional testing aligns better with their primary monoarticular function and more uniform structure. As such, it is likely that the muscle physiology (fiber length, orientation, and distribution of muscle volume) may influence the strength differences observed.
Previous studies have observed strong correlations between quadriceps muscle cross-sectional area, as measured by 2D MRI, and muscle strength testing, suggesting an alternate, accurate, and reliable method for assessing quadriceps muscle strength.13,14 Marcon et al 18 measured muscle volume and mean fat-signal fraction with 2-point Dixon-based MRI in a subset of 33 patients after ACLR with BTB autograft demonstrating a persistent loss of 10% of VM volume. Nevertheless, several limitations have subsequently been highlighted by this 2D MRI–based assessment. Two-dimensional assessments are limited by the fact that only partial muscle volume measurements can be made, and these approaches additionally rely on labor-intensive manual segmentation, limiting the feasibility of readily integrating such analyses into routine clinical practice.18,21,22,28 It is not surprising that the VL demonstrated the strongest correlation with knee extension strength assessment, as this muscle accounts for more than half of the quadriceps volume. However, it is also not surprising that the RF demonstrated the weakest correlation with knee extension strength assessment, as this is the only biarticular quadriceps muscle. The utility of the novel MRI-based 3D approach for volumetric analysis in the current study is that it provides a more comprehensive assessment of the entire lower extremity musculature by allowing further investigation of the involvement and contribution of each individual muscle, muscle group, and/or group ratio in their entirety.
There are limitations to the current study. The median times from ACL injury to functional testing and MRI were 94 and 90 days, respectively, which could lead to a variable degree of muscle volume and/or strength impairments from the time of injury among patients. The temporal delay from injury to assessment in this patient cohort may reflect COVID-19 pandemic-related degradations in institutional capacity. It should be noted that the muscle volume assessments were derived from the MRI study that was repeated, along with strength testing, within 7 days of ACLR to mitigate the likelihood of temporal confounding between the primary variables of interest within this study. The contralateral leg was used as the baseline standard, which is comparable to existing literature. However, this assumes that both limbs are equal in strength preinjury, not affected by dominance, and that the uninjured leg is not also atrophied as a result of injury. The applicability and generalizability of 3D MRI AI segmentation and volumetric analysis may be limited in widespread clinical practice. Further efforts should continue to develop a computer learning algorithm that is easily accessible and user-friendly in providing rapid clinical information that can guide treatment algorithms and provide prognostic value. Lastly, future efforts are required to investigate any potential correlation of quadriceps and hamstring 3D MRI–based volumetric analysis with functional strength analysis in the postoperative setting.
As the results from our study suggest, there is a strong association between 3D MRI–based quadriceps volumetric analysis and knee extension strength testing, and, therefore, automated measurements of muscle volume may be a way to gain further insight into quadriceps strength. The further value of 3D MRI may be found in its utility as a potential adjunct or alternative for strength assessment when quadriceps strength assessments are not feasible, as in cases of significant postinjury pain, limited range of motion, and/or institutional impediments to strength testing. As the results of this study demonstrate the correlation between 3D MRI volumetric automated analysis and quadriceps strength, preoperative 3D MRI may be useful in identifying preoperative strength deficits and aid in risk stratification for postoperative strength deficits.
Conclusion
Preoperatively, a 20% deficit in isometric knee extension strength testing and a 10% deficit in quadriceps musculature volume was noted in the ACL-deficient knee compared to the uninjured limb with a median time from injury to preoperative strength assessment and MRI within 90 days. A moderate to strong correlation between knee extension and flexion strength testing and each individual quadriceps and hamstring muscle volume as measured by a 3D MRI platform was observed preoperatively in the setting of ACL injury. These findings suggest the utility and feasibility of 3D MRI volumetric autosegmentation as a complement to formal preoperative strength assessments. The potential use of this preoperative quantitative assessment serves as an adjunct to individualized hypertrophy-based rehabilitation and a tool to guide patient expectations during postoperative recovery after ACLR. While variable strength of correlation exists between individual muscles of the quadriceps, further investigation is required to determine if targeting individual muscles is feasible and clinically significant.
Supplemental Material
sj-docx-1-ajs-10.1177_03635465261456991 – Supplemental material for MRI-Based Volumetric Analysis of the Quadriceps Muscles Correlation With Knee Extension Strength in Patients Undergoing Anterior Cruciate Ligament Reconstruction
Supplemental material, sj-docx-1-ajs-10.1177_03635465261456991 for MRI-Based Volumetric Analysis of the Quadriceps Muscles Correlation With Knee Extension Strength in Patients Undergoing Anterior Cruciate Ligament Reconstruction by Mikalyn T. DeFoor, Keith A. Knurr, Bryan Heiderscheit, Lara Riem, Daniel J. Cognetti, Joshua Shaw, Marc Blaylock, Ivan J. Antosh, Asheesh Bedi and Andrew J. Sheean in The American Journal of Sports Medicine
Supplemental Material
sj-docx-2-ajs-10.1177_03635465261456991 – Supplemental material for MRI-Based Volumetric Analysis of the Quadriceps Muscles Correlation With Knee Extension Strength in Patients Undergoing Anterior Cruciate Ligament Reconstruction
Supplemental material, sj-docx-2-ajs-10.1177_03635465261456991 for MRI-Based Volumetric Analysis of the Quadriceps Muscles Correlation With Knee Extension Strength in Patients Undergoing Anterior Cruciate Ligament Reconstruction by Mikalyn T. DeFoor, Keith A. Knurr, Bryan Heiderscheit, Lara Riem, Daniel J. Cognetti, Joshua Shaw, Marc Blaylock, Ivan J. Antosh, Asheesh Bedi and Andrew J. Sheean in The American Journal of Sports Medicine
Supplemental Material
sj-docx-3-ajs-10.1177_03635465261456991 – Supplemental material for MRI-Based Volumetric Analysis of the Quadriceps Muscles Correlation With Knee Extension Strength in Patients Undergoing Anterior Cruciate Ligament Reconstruction
Supplemental material, sj-docx-3-ajs-10.1177_03635465261456991 for MRI-Based Volumetric Analysis of the Quadriceps Muscles Correlation With Knee Extension Strength in Patients Undergoing Anterior Cruciate Ligament Reconstruction by Mikalyn T. DeFoor, Keith A. Knurr, Bryan Heiderscheit, Lara Riem, Daniel J. Cognetti, Joshua Shaw, Marc Blaylock, Ivan J. Antosh, Asheesh Bedi and Andrew J. Sheean in The American Journal of Sports Medicine
Supplemental Material
sj-tif-4-ajs-10.1177_03635465261456991 – Supplemental material for MRI-Based Volumetric Analysis of the Quadriceps Muscles Correlation With Knee Extension Strength in Patients Undergoing Anterior Cruciate Ligament Reconstruction
Supplemental material, sj-tif-4-ajs-10.1177_03635465261456991 for MRI-Based Volumetric Analysis of the Quadriceps Muscles Correlation With Knee Extension Strength in Patients Undergoing Anterior Cruciate Ligament Reconstruction by Mikalyn T. DeFoor, Keith A. Knurr, Bryan Heiderscheit, Lara Riem, Daniel J. Cognetti, Joshua Shaw, Marc Blaylock, Ivan J. Antosh, Asheesh Bedi and Andrew J. Sheean in The American Journal of Sports Medicine
Supplemental Material
sj-tif-5-ajs-10.1177_03635465261456991 – Supplemental material for MRI-Based Volumetric Analysis of the Quadriceps Muscles Correlation With Knee Extension Strength in Patients Undergoing Anterior Cruciate Ligament Reconstruction
Supplemental material, sj-tif-5-ajs-10.1177_03635465261456991 for MRI-Based Volumetric Analysis of the Quadriceps Muscles Correlation With Knee Extension Strength in Patients Undergoing Anterior Cruciate Ligament Reconstruction by Mikalyn T. DeFoor, Keith A. Knurr, Bryan Heiderscheit, Lara Riem, Daniel J. Cognetti, Joshua Shaw, Marc Blaylock, Ivan J. Antosh, Asheesh Bedi and Andrew J. Sheean in The American Journal of Sports Medicine
Footnotes
Acknowledgements
The authors acknowledge all surgeons who contributed their patients to be included in this cohort study, including Rachel Cuenca, MD, Matthew Schmitz, MD, Jeanne Patzkowski, MD, Joshua Tadlock, MD, and David Tennent, MD. Additionally, the authors thank Joshua McKinley, PTA, for his treatment contributions in this study population.
Submitted December 24, 2025; accepted April 30, 2026.
One or more of the authors has declared the following potential conflict of interest or source of funding: This study was partially funded by NIH award KL2TR002374 (to K.A.K.) and the Congressionally Directed Medical Research Program (CDMRP), Peer Reviewed Orthopaedic Research Program (PRORP) (to A.J.S.). M.T.D. is a board or committee member of the American Academy of Orthopaedic Surgeons and Society of Military Orthopaedic Surgeons, and is on the editorial board of Arthroscopy. B.H. is an advisory board member of and has stock options in Springbok Analytics; receives IP royalties from the NBA, NFL, and GE Healthcare; has an ownership interest in Science of Running Medicine; and is on the editorial board of Orthopedics Today. L.R. is a salaried employee of and receives stock options in Springbok Analytics. D.J.C. is a board or committee member of the Arthroscopy Association of North America, and is on the editorial board of Arthroscopy. I.J.A. receives personal fees from Arthrex. A.B. is an advisory board member of and has stock options in Springbok Analytics; is a paid consultant for Arthrex; receives publishing royalties and financial or material support from SLACK Incorporated and Springer; and is a board or committee member of the American Orthopaedic Society for Sports Medicine. A.J.S. is an advisory board member of and has stock options in Springbok Analytics; is a paid consultant for Stryker; is a board or committee member of the American Orthopaedic Society for Sports Medicine; and is on the editorial board of Arthroscopy.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.