
Abstract
Background:
Anterior cruciate ligament (ACL) rupture frequently occurs alongside meniscal injury, together altering the intra-articular environment. While ACL injury triggers an inflammatory cascade within synovial fluid, meniscal injury may intensify these responses, contributing to joint degeneration. However, little is known about how combined ACL and meniscal injuries shape the synovial inflammatory milieu or whether these profiles influence long-term outcomes.
Purpose/Hypothesis:
The purpose was to characterize synovial fluid inflammatory phenotypes at the time of ACL reconstruction with concomitant meniscal injury and assess their association with patient-reported outcome measures (PROMs) and clinically meaningful improvement. It was hypothesized that (1) distinct inflammatory phenotypes would exist, (2) these phenotypes would correlate with symptom severity and recovery, and (3) individual biomarkers’ effects on outcomes would vary by phenotype.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients undergoing arthroscopic ACL reconstruction with concomitant meniscal injury were prospectively enrolled between July 2011 and January 2024. Synovial fluid was aspirated before incision, and the concentrations of 10 biomarkers were quantified. Unsupervised k-means clustering identified high- and low-inflammation phenotypes. PROMs were collected preoperatively on the day of surgery (baseline) and at long-term follow-up. Linear regression assessed biomarker associations with PROMs, with interaction models evaluating effect modification by inflammation phenotype. Minimal clinically important difference (MCID) achievement thresholds were calculated using a distribution-based approach (0.5 × baseline SD) and compared between clusters.
Results:
A total of 97 patients were stratified into high-inflammation (n = 66) and low-inflammation (n = 31) clusters. Patient and surgical characteristics were similar, but the high-inflammation cluster demonstrated significantly worse baseline pain and function (all P≤ .008). At a mean follow-up of 8.2 ± 2.5 years, postoperative PROMs were similar, but the high-inflammation cluster experienced greater improvements in VAS pain (−13.5 vs 3.1; P = .008) and Lysholm (28.6 vs 8.9; P = .002) scores. Monocyte chemoattractant protein-1 (MCP-1) demonstrated strong, phenotype-dependent associations with PROMs, and patients with high inflammation were more likely to achieve the MCID for VAS pain score (57.6% vs 17.6%; P < .05).
Conclusion:
Synovial fluid biomarker profiles at the time of ACL reconstruction with concomitant meniscal injury identified distinct inflammatory phenotypes associated with baseline symptom severity and differential patterns of clinical improvement. Although long-term PROMs were similar between groups, phenotype-dependent biomarker associations, particularly involving MCP-1, suggest that the biological context of recovery differs across inflammatory profiles.
Keywords
Anterior cruciate ligament (ACL) rupture is among the most common serious knee injuries in young and athletic populations, affecting >200,000 people annually in the United States. 31 Despite technically successful reconstruction, clinical recovery is highly variable, with some patients experiencing persistent pain, functional limitations, and incomplete return to preinjury activity levels. Traditional predictors of outcomes, including graft type, surgical technique, and rehabilitation, only partially explain this heterogeneity, suggesting that biological factors intrinsic to the joint environment may play an important role in recovery and ultimate outcomes. 35
One key contributor to this biological response is the acute intra-articular inflammatory cascade triggered by the initial ACL injury, characterized by the release of cytokines, chemokines, matrix-degrading enzymes, and growth factors.22,37 Prior work has demonstrated that elevated inflammatory mediators in synovial fluid at the time of ACL reconstruction are associated with worse baseline symptoms, worse patient-reported outcome measures (PROMs) at 2 years, and progression of cartilage degradation at 3 to 5 years.2,25,30 However, inflammation is not uniformly detrimental; controlled inflammatory signaling is necessary for debris clearance, graft incorporation, and tissue healing. Accordingly, recovery after ACL reconstruction likely depends not only on the magnitude of inflammation but also on the overall balance between pro-inflammatory, anti-inflammatory, and reparative pathways. 20 Recent orthopaedic research has therefore shifted toward identifying molecular “inflammation phenotypes” rather than relying on single biomarkers.22,43 Understanding whether these biological profiles modify the relationship between biomarkers and outcomes may clarify why some patients improve dramatically after reconstruction while others experience persistent symptoms despite similar surgical care.
One important and common source of this biological heterogeneity is concomitant meniscal injury, which accompanies ACL rupture in 37% to 46% of patients and further alters the intra-articular biological environment.3,31,34 Among concomitant injuries, the meniscus is uniquely positioned to influence joint homeostasis because of its roles in load distribution, joint stability, and chondroprotection, and its disruption has been consistently linked to worse long-term clinical outcomes. Specifically, concomitant meniscal injuries at the time of ACL reconstruction are associated with worse PROMs at 5 to 10 years, particularly for pain, sports and recreation function, and quality of life.3,6,34 Meniscal damage also increases synovial activation, augments cytokine production, and accelerates degenerative pathways, potentially amplifying variability in the patient response to injury and surgery.7,43 While other concomitant findings such as chondral lesions and bone marrow edema are also common, these are often heterogeneous, more difficult to quantify reproducibly at the time of surgery, and less consistently associated with synovial fluid biology and long-term outcomes. In contrast, meniscal pathology represents a well-defined, clinically relevant, and biologically active modifier of the intra-articular environment.
Therefore, rather than comparing patients with and without meniscal pathology, the purpose of the current study was to characterize synovial fluid inflammatory phenotypes at the time of ACL reconstruction specifically in patients with concomitant meniscal injury, a common and biologically influential co-pathology, and to determine whether biomarker-defined inflammation profiles are associated with baseline symptoms, long-term PROMs, and clinically meaningful improvement. We hypothesized that (1) distinct inflammatory phenotypes would exist within this population, (2) these phenotypes would be associated with baseline symptom severity and magnitude of recovery, and (3) the relationship between individual biomarkers and postoperative outcomes would differ according to inflammation phenotype.
Methods
Study Design
This was a retrospective cohort study derived from a database of patients whose synovial fluid had been prospectively collected and analyzed as part of an institutional review board–approved study (No. 24-00387) between July 2011 and January 2024. The patients selected from the databases had undergone arthroscopic knee surgery at a large urban academic medical center. Eligible participants were adults (≥18 years of age) requiring surgical management for ligamentous, meniscal, or focal cartilage injuries who consented to intraoperative synovial fluid collection. To minimize selection bias, all consecutive patients meeting eligibility criteria during the study period were prospectively enrolled in the institutional synovial fluid registry. Data collection, including synovial fluid sampling and PROMs, followed standardized institutional protocols. Patients were included in the present study if they had a concomitant ACL and meniscal injury and a preoperative synovial fluid sample available for biomarker analysis. Exclusion criteria included concomitant posterior cruciate ligament, medial collateral ligament, lateral collateral ligament, posterolateral corner injuries, multiligament knee injuries, osteochondral fractures requiring fixation, advanced chondral lesions requiring separate cartilage restoration procedures, prior diagnosis of autoimmune or inflammatory disease, receipt of an intra-articular injection in the operative knee within 3 months of surgery, use of immunomodulatory medications in the preceding year, or an inadequate volume of synovial fluid for analysis. Because this study was derived from an existing prospective synovial fluid registry and included all eligible patients with available biomarker and long-term PROM data, an a priori power analysis was not feasible. The present study should therefore be considered exploratory and hypothesis generating.
Participants completed 4 validated PROMs: visual analog scale (VAS) (from 0 to 100) to assess pain, Lysholm scale, Tegner Activity Scale, and Knee injury and Osteoarthritis Outcome Score–Physical Function Short Form (KOOS-PS). These assessments were administered at baseline (day of surgery) and again at a minimum of 5 years after the index procedure. These tests were chosen as they have been validated in patients with ACL and meniscal injury.12,29,38,44,45
For the present investigation, descriptive information including age, sex, and body mass index (BMI) at the time of surgery was abstracted from the electronic medical record. A total of 97 patients met inclusion and exclusion criteria and were included in analyses of synovial fluid biomarker concentrations. Patients without long-term follow-up PROM data were excluded from PROM outcome analyses, leaving 60 patients for postoperative outcome assessment, with 41 in the high-inflammation cohort and 19 in the low-inflammation cohort. Of these patients, 50 also had baseline preoperative PROMs available and were therefore included in minimal clinically important difference (MCID) responder analyses, with 33 in the high-inflammation cohort and 17 in the low-inflammation cohort (Figure 1).
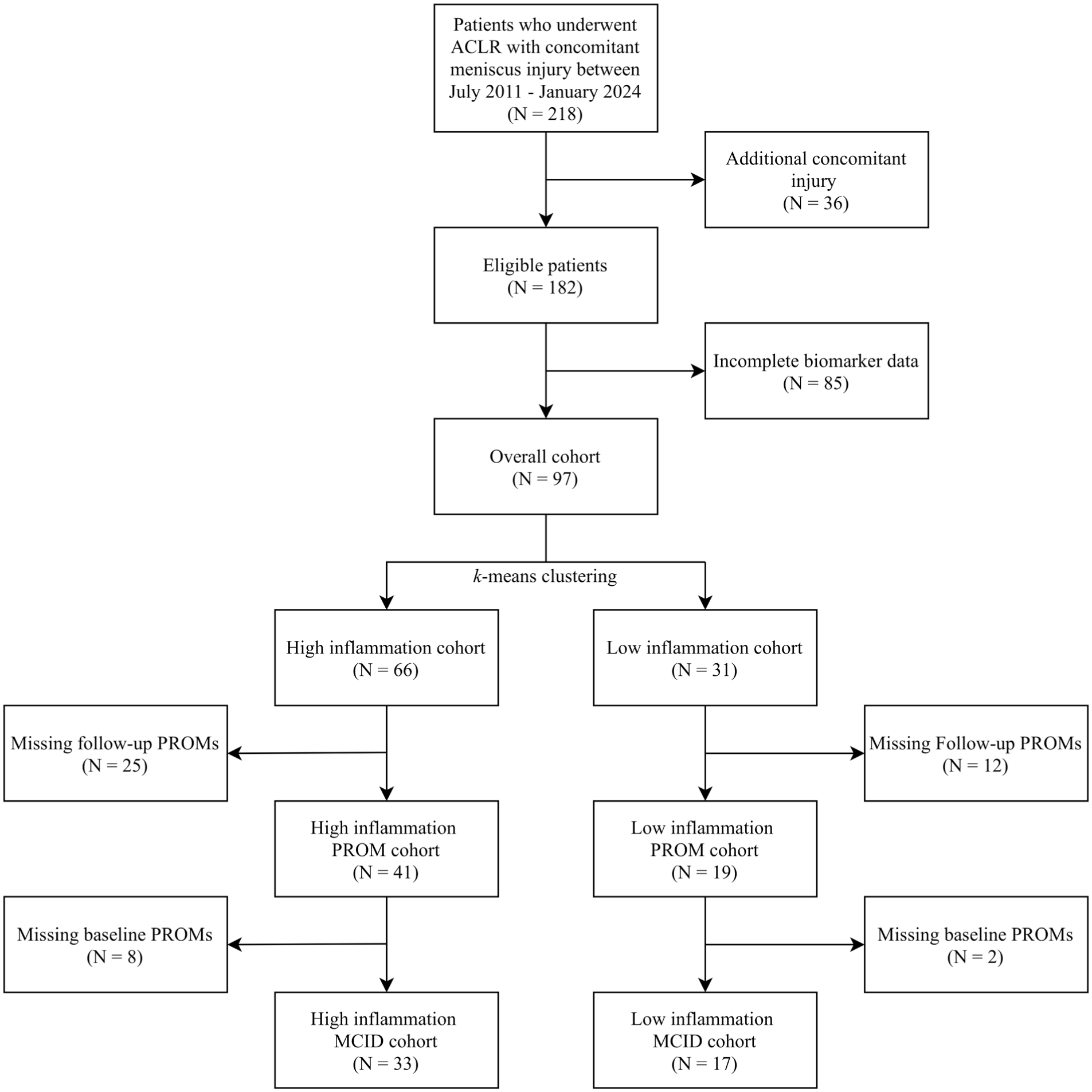
Flow diagram of patient inclusion. ACLR, anterior cruciate ligament reconstruction; MCID, minimal clinically important difference; PROM, patient-reported outcome measure.
Synovial Fluid Collection and Analysis
On the day of surgery, at least 500 µL of synovial fluid was aspirated from the operative knee before incision using an 18-gauge needle and a 20-mL syringe under sterile technique. The aspirated fluid was immediately transferred into a sterile tube with a protease inhibitor cocktail (Halt Protease Inhibitor Cocktail, EDTA-free; Pierce Biotechnology) at a ratio of 10 µL of inhibitor per 1000 µL of synovial fluid. Samples were centrifuged at 3820 rpm for 10 minutes at 4°C, and the resulting supernatant was divided into sterile cryotubes and stored at −80°C until further processing.
Ten biomarkers (Appendix Table A1, available in the online version of this article) were selected for analysis: basic fibroblast growth factor (bFGF), interleukin-6 (IL-6), interleukin-1 receptor antagonist (IL-1Ra), monocyte chemoattractant protein-1 (MCP-1), macrophage inflammatory protein-1 beta (MIP-1β), matrix metalloproteinase-3 (MMP-3), regulated on activation, normal T cell expressed and secreted (RANTES), tissue inhibitor of metalloproteinases 1 and 2 (TIMP-1 and TIMP-2), and vascular endothelial growth factor (VEGF). Concentrations were quantified using a combination of custom and commercially available precoated multiplex enzyme-linked immunosorbent assay (ELISA) plates (Meso Scale Discovery [MSD]). Thawed samples were run in duplicate, and signal detection was performed with an MSD QuickPlexSQ120 reader.
Synovial fluid biomarkers were selected to capture complementary aspects of the intra-articular environment relevant to arthroscopic knee pathology. IL-6 was included as a pro-inflammatory cytokine associated with acute synovitis and cartilage catabolism after ligamentous and meniscal injury.5,41 MCP-1, MIP-1β, and RANTES were selected as chemokines involved in monocyte, macrophage, and T-cell recruitment and persistent synovial inflammation.9,36 MMP-3 was included as a marker of extracellular matrix degradation, with synovial fluid concentrations consistently elevated in operative knee samples.10,11 IL-1Ra was evaluated as an endogenous anti-inflammatory regulator that suppresses IL-1–mediated inflammation.13,14 VEGF and bFGF were included for their roles in angiogenesis, fibroblast proliferation, and proliferative/reparative signaling. 10 TIMP-1 and TIMP-2 were selected to assess regulation of matrix metalloproteinase activity and tissue remodeling balance. 10 These biomarkers have been previously implicated in ACL injury, meniscal pathology, and cartilage degeneration, and synovial fluid cytokine profiles using this panel have been shown to explain >50% of variance in intermediate-term patient-reported outcomes.21,43 Because the original prospective registry was designed to evaluate inflammatory synovial phenotypes rather than cartilage-specific degeneration, biomarkers such as CTX-II and COMP were not included, representing an important limitation and area for future investigation.
Statistical Analysis
Statistical analyses were performed using RStudio (Version 2025.09.0+387; Posit). Analyses were performed using a complete-case approach for biomarker clustering because k-means clustering requires complete biomarker profiles for accurate cluster assignment. Therefore, only patients with complete synovial fluid biomarker measurements across all included analytes were eligible for inclusion in the clustering analysis and subsequent stratification into high- and low-inflammation groups. Because all downstream analyses were performed within these predefined inflammatory clusters, subsequent outcome analyses were limited to patients who could be assigned to a cluster.
For PROM analyses, patients without long-term follow-up outcome data were excluded from postoperative outcome comparisons. All patients with long-term follow-up PROMs also had complete baseline preoperative PROMs and were therefore included in MCID responder analyses. Loss to follow-up was addressed by restricting each outcome analysis to patients with available data for that specific endpoint. This complete-case approach was selected to preserve consistency of inflammatory phenotype classification across all analyses, although it may introduce selection bias and is acknowledged as a limitation.
Continuous variables are summarized as means with standard deviations, and categorical variables are summarized as counts and percentages. Baseline patient and clinical characteristics were compared between inflammation clusters using independent-samples t tests or Mann-Whitney U tests for continuous variables, as appropriate, and chi-square tests or Fisher exact tests for categorical variables.
Preoperative and postoperative PROMs, as well as change scores from baseline to follow-up, were compared between inflammation clusters using independent-samples t tests. The proportion of patients achieving the MCID for each PROM was compared between clusters using chi-square tests or Fisher exact tests, with results displayed graphically. MCID thresholds were calculated using a distribution-based approach (0.5 × SD of baseline scores) from the full preoperative cohort: 10.1 for VAS pain, 9.0 for Lysholm, 10.3 for KOOS-PS, and 0.7 for Tegner.
Inflammation clusters were derived using an unsupervised k-means clustering approach based on synovial fluid biomarker concentrations. Before clustering, biomarker values were natural-log transformed and standardized to account for differences in scale. K-means clustering was performed in R (R Foundation for Statistical Computing) using Euclidean distance, with the number of clusters prespecified as 2 to identify groups representing relatively high and low inflammatory profiles. Alternative cluster solutions, including a k value of 3, were explored; however, the 3-cluster solution produced substantial overlap and did not improve clinical interpretability. In contrast, a k value of 2 demonstrated clearer separation across multiple inflammatory mediators and was therefore selected for subsequent analyses. Importantly, cluster assignment was derived in an unsupervised manner based solely on synovial fluid biomarker concentrations, independent of clinical characteristics and outcomes, and was not intended to represent injury severity classification. Rather, clusters reflect relative intra-articular inflammatory states at the time of sampling.
Resulting clusters demonstrated clear separation in multiple inflammatory mediators, supporting their classification as high- and low-inflammation groups. These clusters were used for all subsequent stratified and interaction-based analyses. Principal component analysis (PCA) was performed as a post hoc dimensionality reduction technique to visualize separation between inflammatory phenotypes. PCA was not used in cluster derivation or model training.
To evaluate associations between biomarker concentrations and postoperative PROMs, multivariable linear regression models were constructed separately within each inflammation cluster. Each model included one biomarker as the primary independent variable and was adjusted for age, sex, BMI, symptom duration, meniscal laterality, and meniscal surgical treatment. Symptom duration, defined as time from injury to synovial fluid aspiration on the day of surgery (in months), was included both as a baseline comparison between inflammation clusters and as an adjustment variable in all multivariable regression models because of its known association with inflammatory biomarker expression after ACL injury. Regression coefficients (β), 95% confidence intervals, and corresponding P values were reported, with full model outputs including standard error, adjusted R2, and overall model fit statistics provided in the Appendix (available online). Model assumptions for all multivariable linear regression analyses were assessed using standard diagnostic procedures, including evaluation of linearity, normality of residuals, homoscedasticity, multicollinearity, and influential observations. Residual and Q-Q plots were visually inspected, and variance inflation factors were reviewed to assess collinearity among covariates. No major violations were identified that required model restructuring.
Conditional process (moderation) analysis was performed using multivariable linear regression models including biomarker × inflammation cluster interaction terms, consistent with an effect modification framework. Multivariable linear regression models were adjusted for age, sex, BMI, symptom duration, meniscal laterality, and meniscal surgical treatment. A statistically significant interaction term was interpreted as evidence of effect modification by inflammation cluster.
All statistical tests were 2-sided, and statistical significance was defined as a P value <.05. No adjustments were made for multiple comparisons given the exploratory nature of the biomarker analyses. This study focused on within-cohort comparisons of biomarker expression, as reliable and standardized synovial fluid reference values in uninjured knees are not well established due to limited fluid availability and interassay variability across studies.
Results
Patient Characteristics
A total of 97 patients met inclusion criteria and were stratified into high-inflammation (n = 66) and low-inflammation (n = 31) clusters based on k-means clustering of synovial fluid biomarker profiles. Baseline patient and clinical characteristics were comparable between groups (Table 1). No significant difference in symptom duration was observed between high- and low-inflammation clusters (3.9 ± 8.5 and 8.2 ± 13.6 months, respectively; P = .112). Because symptom duration is known to influence synovial inflammatory activity after ACL injury, it was also included as an adjustment variable in all multivariable regression models. For patients with long-term PROM data, the mean follow-up time was 8.2 ± 2.5 years and did not differ between clusters (8.0 ± 2.7 years for high vs 8.5 ± 2.0 years for low; P = .452).
Baseline Characteristics and Cytokine Profiles of Entire Cohort by Inflammation Cluster a
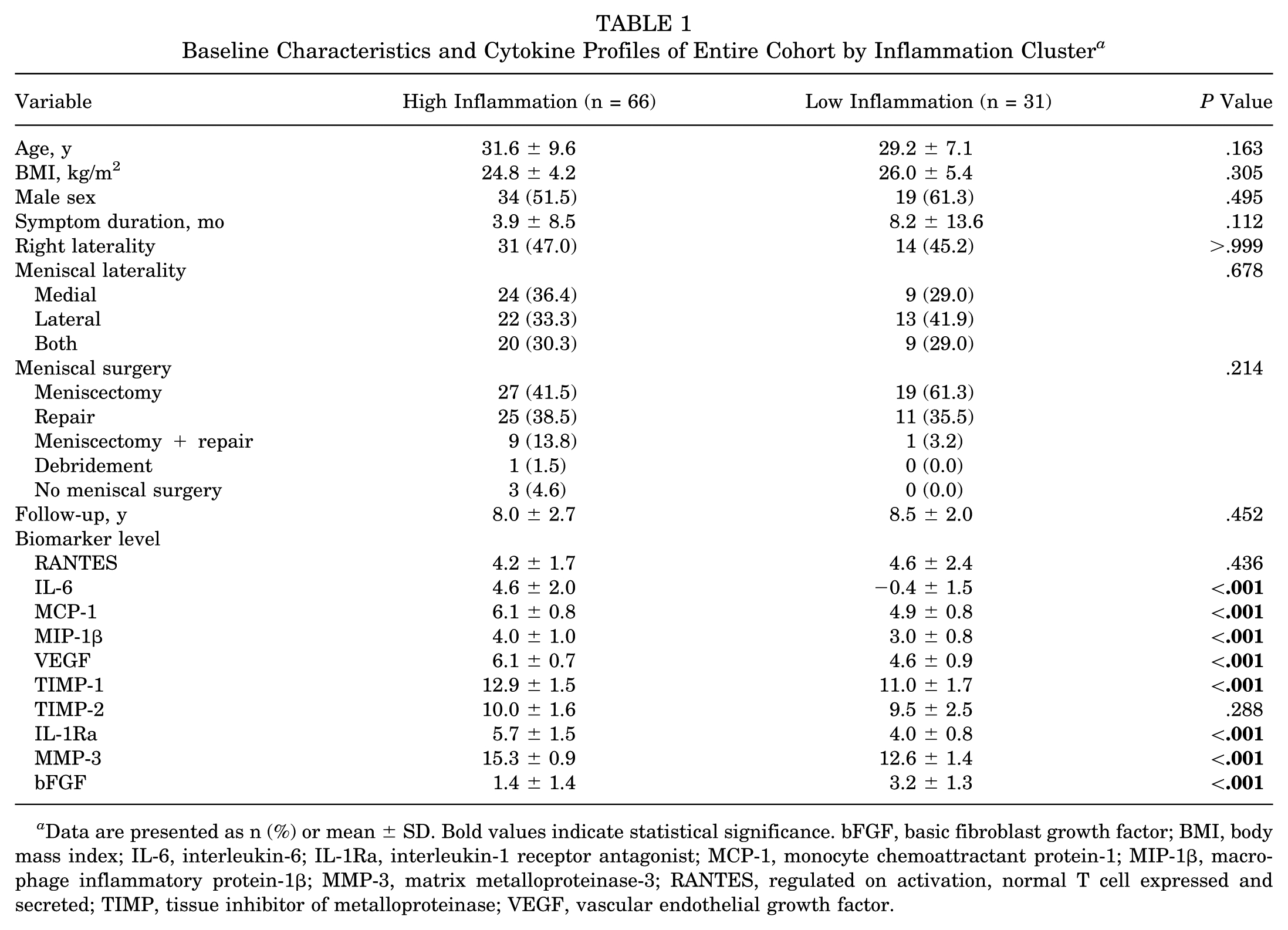
Data are presented as n (%) or mean ± SD. Bold values indicate statistical significance. bFGF, basic fibroblast growth factor; BMI, body mass index; IL-6, interleukin-6; IL-1Ra, interleukin-1 receptor antagonist; MCP-1, monocyte chemoattractant protein-1; MIP-1β, macrophage inflammatory protein-1β; MMP-3, matrix metalloproteinase-3; RANTES, regulated on activation, normal T cell expressed and secreted; TIMP, tissue inhibitor of metalloproteinase; VEGF, vascular endothelial growth factor.
As expected, patients in the high-inflammation cluster demonstrated significantly elevated concentrations of multiple pro-inflammatory and catabolic biomarkers, including IL-6, MCP-1, MIP-1β, VEGF, TIMP-1, IL-1Ra, and MMP-3 (all P < .001). In contrast, bFGF levels were significantly higher in the low-inflammation cluster (P < .001). No differences were observed in RANTES or TIMP-2 levels between groups.
To further illustrate separation between inflammatory phenotypes and the biomarker patterns driving cluster assignment, PCA was performed on standardized synovial fluid biomarker concentrations. As shown in Figure 2, patients demonstrated clear separation along the first principal component, which accounted for 40.6% of the variance and reflected coordinated pro-inflammatory and catabolic signaling. The second principal component explained 16.8% of variance and captured additional heterogeneity in biomarker expression.
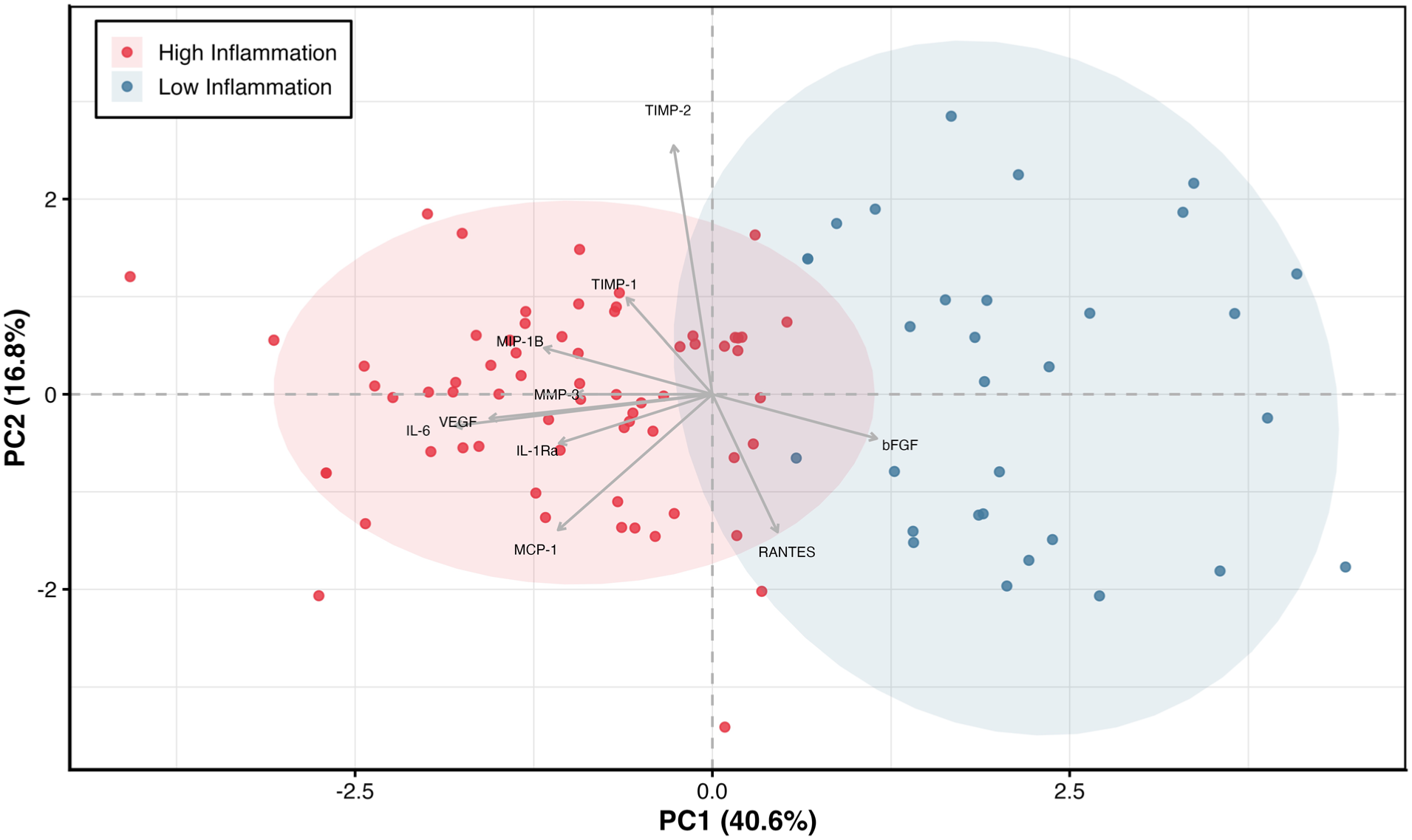
Principal component analysis of standardized synovial fluid biomarker concentrations used to visualize separation of inflammatory phenotypes identified via k-means clustering. Each point represents an individual patient, with shaded ellipses indicating cluster dispersion. Arrows indicate the contribution of individual biomarkers to the overall inflammatory profile. Principal component 1 (PC1; 40.6% variance explained) represents a composite axis of coordinated inflammatory activity, with higher levels of pro-inflammatory and catabolic biomarkers clustering on one side of the plot. Principal component 2 (PC2; 16.8%) captures additional variability in biomarker expression. bFGF, basic fibroblast growth factor; IL-6, interleukin-6; IL-1Ra, interleukin-1 receptor antagonist; MCP-1, monocyte chemoattractant protein-1; MIP-1β, macrophage inflammatory protein-1β; MMP-3, matrix metalloproteinase-3; RANTES, regulated on activation, normal T cell expressed and secreted; TIMP, tissue inhibitor of metalloproteinase; VEGF, vascular endothelial growth factor.
Baseline and Follow-up PROMs by Inflammation Cluster
Preoperative PROMs differed significantly between inflammation clusters (Table 2, Figure 3). Patients in the high-inflammation cluster reported worse baseline pain and function, including higher VAS pain score and lower KOOS-PS, Lysholm, and Tegner values compared with the low-inflammation cluster (all P≤ .008). At the final follow-up, however, no significant differences in PROMs were observed between clusters for VAS pain, KOOS-PS, Lysholm, or Tegner values (all P > .40), indicating convergence of outcomes despite differing baseline symptom severity.
Pre- and Postoperative Outcome Scores of Entire Cohort by Inflammation Cluster a
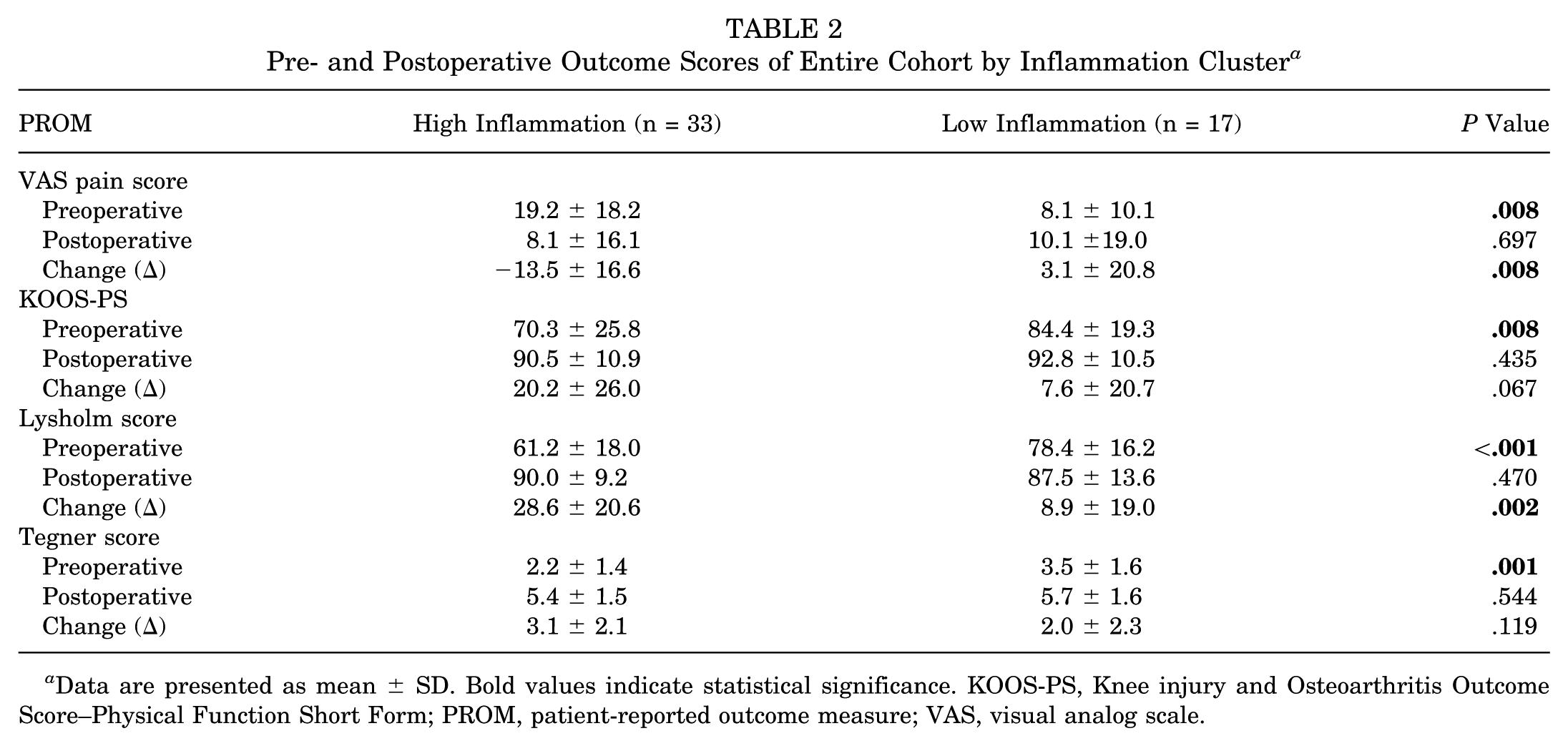
Data are presented as mean ± SD. Bold values indicate statistical significance. KOOS-PS, Knee injury and Osteoarthritis Outcome Score–Physical Function Short Form; PROM, patient-reported outcome measure; VAS, visual analog scale.
Patients in the high-inflammation cluster demonstrated greater improvements from baseline to follow-up for several PROMs despite worse baseline scores (Table 2). The high-inflammation cluster experienced significantly greater reductions in VAS pain score (−13.5 vs 3.1; P = .008) and greater improvements in Lysholm score (28.6 vs 8.9; P = .002) compared with the low-inflammation cluster. Improvements in KOOS-PS and Tegner values did not differ significantly between groups.
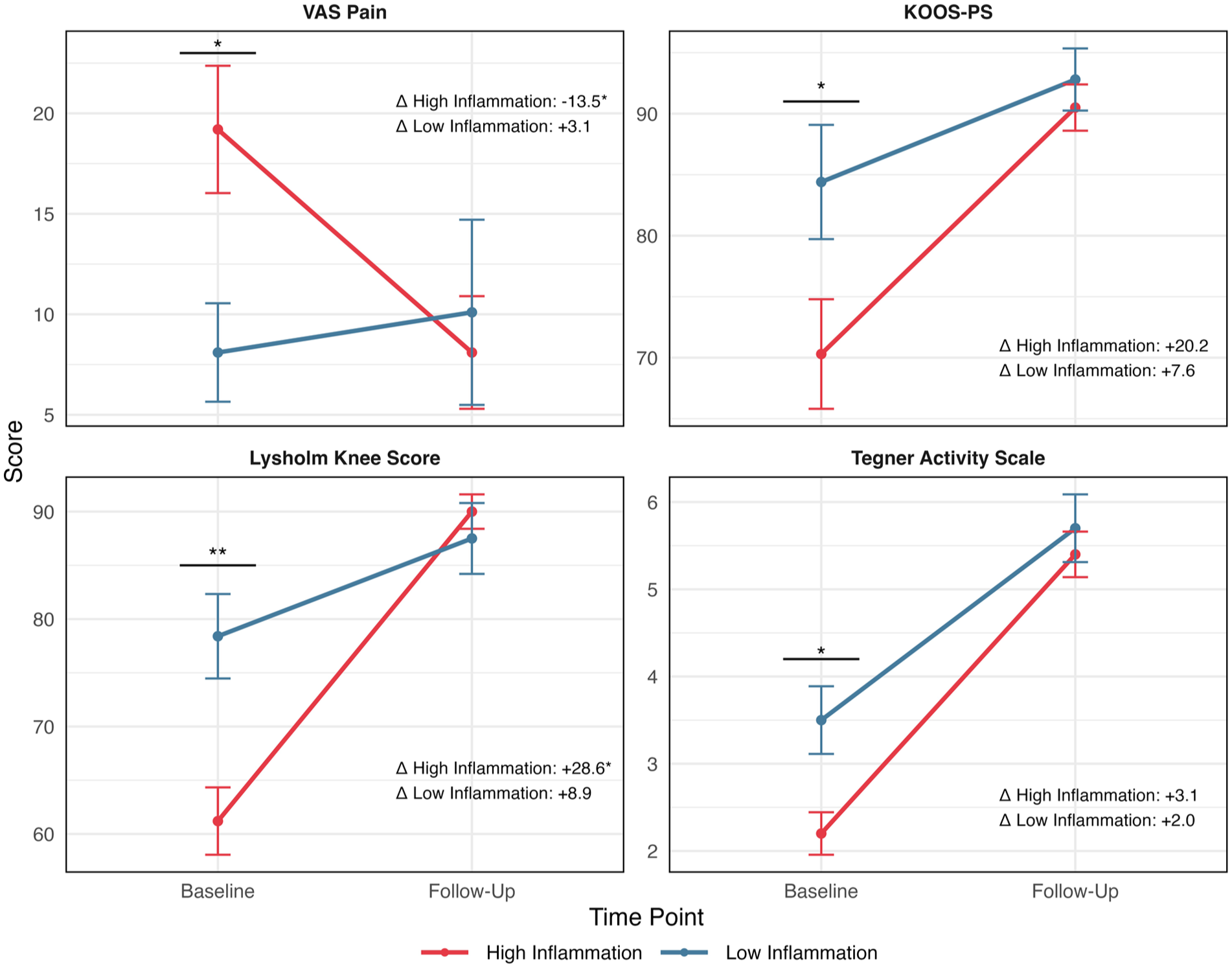
Preoperative and postoperative patient-reported outcome measures (PROMs) stratified by inflammatory phenotype. Line plots demonstrate mean scores with standard error bars for high- and low-inflammation groups across PROMs. The high-inflammation group showed a greater magnitude of change for VAS pain and Lysholm scores (P < .01). Asterisks above the baseline values indicate significant baseline differences between groups (*P < .01; **P < .001). Change (Δ) values represent mean change from baseline to follow-up scores within each group. KOOS-PS, Knee injury and Osteoarthritis Outcome Score–Physical Function Short Form; VAS, visual analog scale.
Associations Between Biomarkers and PROMs
In the overall cohort, associations between baseline biomarker concentrations and PROMs at follow-up were generally weak and not statistically significant (Appendix Table A2, available online). No biomarkers demonstrated a significant relationship with VAS, KOOS-PS, or Lysholm values. Notably, bFGF showed a significant negative association with Tegner scores (β = −0.286; P = .008), indicating that higher baseline bFGF concentrations were related to lower activity levels at follow-up. No significant associations were observed between bFGF and VAS pain, KOOS-PS, or Lysholm values. Other biomarkers did not exhibit statistically significant associations with Tegner scores.
Associations Between Biomarkers and PROMs Within Inflammation Clusters
Within the high-inflammation cluster, multivariable linear regression analyses demonstrated limited associations between individual biomarker concentrations and long-term PROMs (Table 3). Elevated bFGF levels were independently associated with worse KOOS-PS values (β = −2.93; P = .042) and lower Tegner activity levels (β = −0.53; P < .001) within the high-inflammation cluster, despite mean bFGF concentrations being higher in the low-inflammation group overall. No significant association between bFGF and postoperative PROMs was observed within the low-inflammation cluster, suggesting that the clinical relevance of bFGF may depend on the broader inflammatory phenotype rather than absolute concentration alone. No other biomarkers showed consistent or statistically significant associations with pain or functional outcomes in this cluster.
Associations Between Biomarker Concentrations and PROMs at Follow-up in the High-Inflammation Cluster a
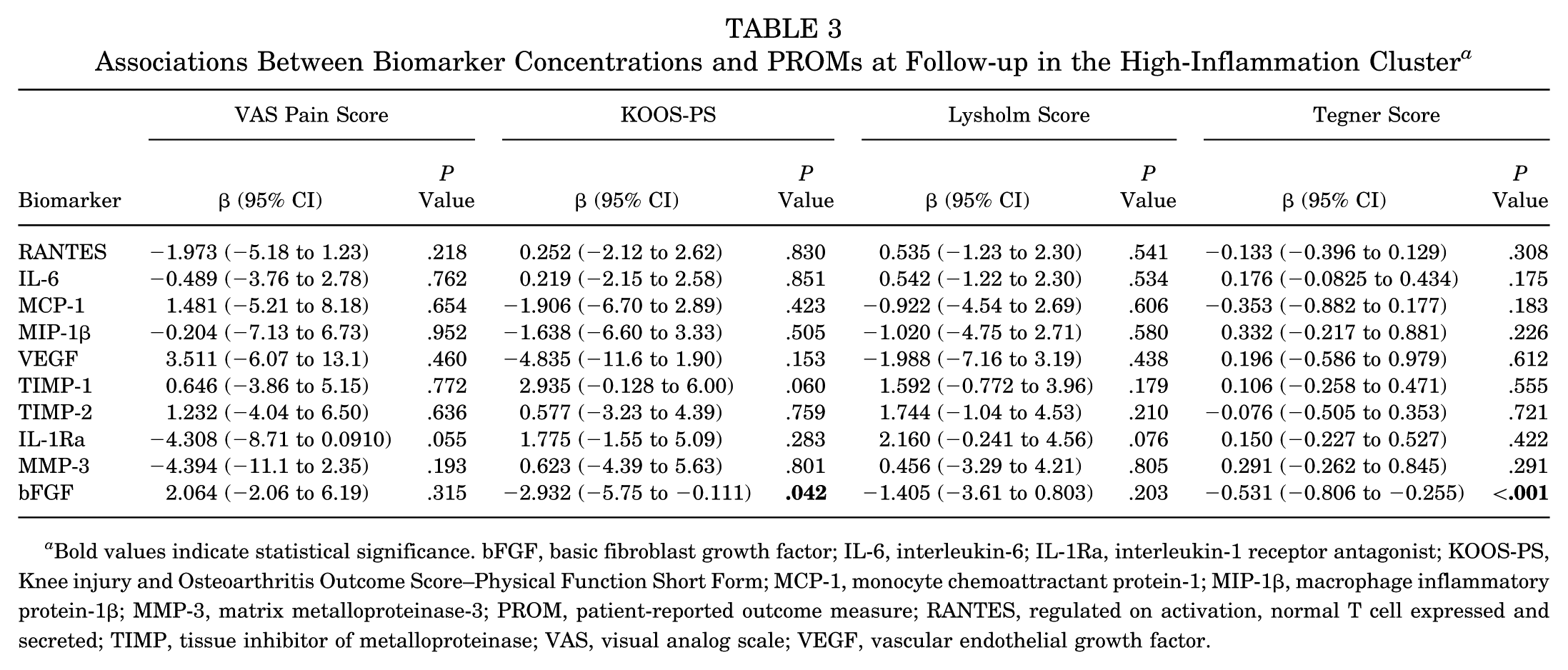
Bold values indicate statistical significance. bFGF, basic fibroblast growth factor; IL-6, interleukin-6; IL-1Ra, interleukin-1 receptor antagonist; KOOS-PS, Knee injury and Osteoarthritis Outcome Score–Physical Function Short Form; MCP-1, monocyte chemoattractant protein-1; MIP-1β, macrophage inflammatory protein-1β; MMP-3, matrix metalloproteinase-3; PROM, patient-reported outcome measure; RANTES, regulated on activation, normal T cell expressed and secreted; TIMP, tissue inhibitor of metalloproteinase; VAS, visual analog scale; VEGF, vascular endothelial growth factor.
In contrast, within the low-inflammation cluster, MCP-1 showed strong and consistent links with long-term outcomes (Table 4). Higher MCP-1 levels were associated with lower VAS pain scores (β = −20.37; P < .001), higher KOOS-PS values (β = 9.97; P = .007), and higher Lysholm scores (β = 13.87; P = .002). Although baseline MCP-1 concentrations were significantly higher in the high-inflammation cluster overall, MCP-1 demonstrated significant positive associations with long-term outcomes only within the low-inflammation phenotype. No significant associations were observed within the high-inflammation cluster, suggesting that elevated MCP-1 may be beneficial only within a lower-inflammatory environment rather than as an isolated marker of greater inflammation. No significant associations were observed between bFGF or other biomarkers and PROMs in this cluster.
Associations Between Biomarker Concentrations and PROMs at Follow-up in the Low-Inflammation Cluster a
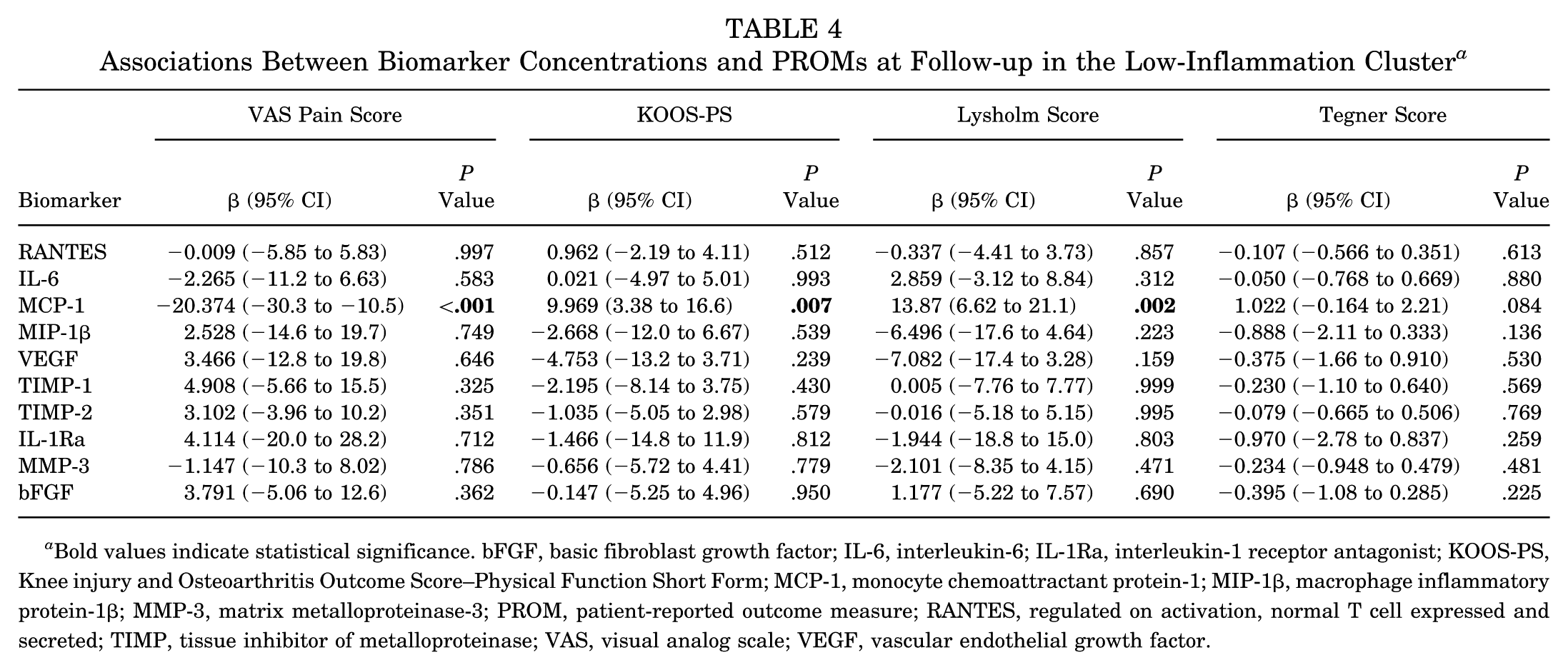
Bold values indicate statistical significance. bFGF, basic fibroblast growth factor; IL-6, interleukin-6; IL-1Ra, interleukin-1 receptor antagonist; KOOS-PS, Knee injury and Osteoarthritis Outcome Score–Physical Function Short Form; MCP-1, monocyte chemoattractant protein-1; MIP-1β, macrophage inflammatory protein-1β; MMP-3, matrix metalloproteinase-3; PROM, patient-reported outcome measure; RANTES, regulated on activation, normal T cell expressed and secreted; TIMP, tissue inhibitor of metalloproteinase; VAS, visual analog scale; VEGF, vascular endothelial growth factor.
To facilitate visualization of these within-cluster associations, regression coefficients from Tables 3 and 4 are displayed graphically in Figure 4. Complete regression modeling data are included in Appendix Tables A3 and A4 (available online).
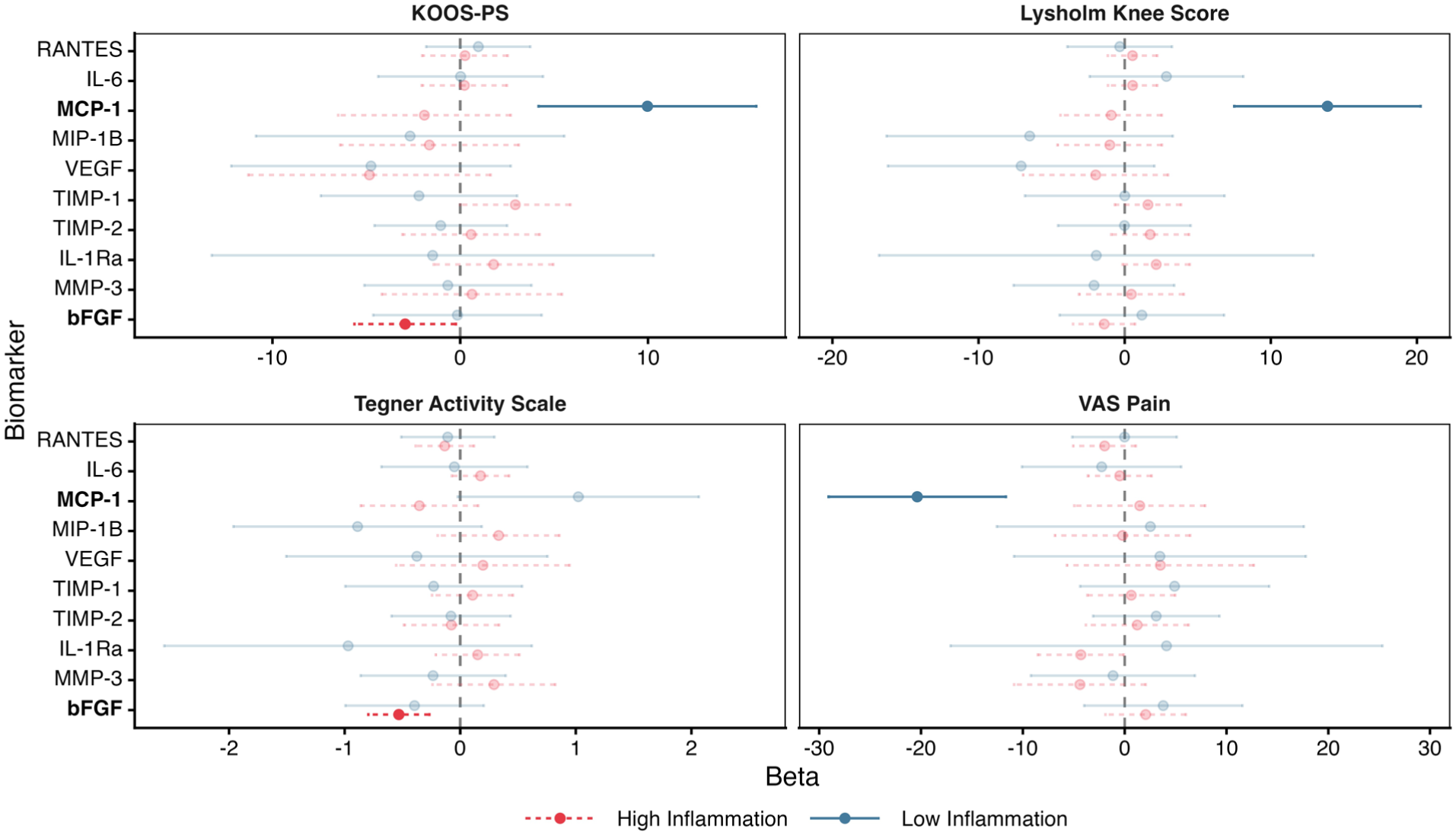
Forest plots displaying adjusted regression coefficients (β) and 95% confidence intervals for associations between baseline synovial fluid biomarker concentrations and long-term patient-reported outcomes, analyzed separately within each inflammatory phenotype. Nonmuted (darker) points and lines indicate statistically significant associations (P < .05), whereas faded elements denote nonsignificant results. bFGF, basic fibroblast growth factor; IL-6, interleukin-6; IL-1Ra, interleukin-1 receptor antagonist; KOOS-PS, Knee injury and Osteoarthritis Outcome Score–Physical Function Short Form; MCP-1, monocyte chemoattractant protein-1; MIP-1β, macrophage inflammatory protein-1β; MMP-3, matrix metalloproteinase-3; RANTES, regulated on activation, normal T cell expressed and secreted; TIMP, tissue inhibitor of metalloproteinase; VAS, visual analog scale; VEGF, vascular endothelial growth factor.
Effect Modification by Inflammation Cluster
Conditional process analysis confirmed that inflammation cluster status significantly moderated the relationship between select biomarkers and PROMs (Table 5). MCP-1 demonstrated significant cluster-dependent effects across all outcome measures, including VAS pain, KOOS-PS, Lysholm, and Tegner values (all P≤ .042) (Figure 4). Additional moderation effects were observed for TIMP-1 with KOOS-PS (P = .042) and MIP-1β with Tegner activity score (P = .015), although these associations were less consistent across outcomes.
Conditional Process Analysis: Biomarker Versus PROM With Effect Moderation by Inflammation Cluster
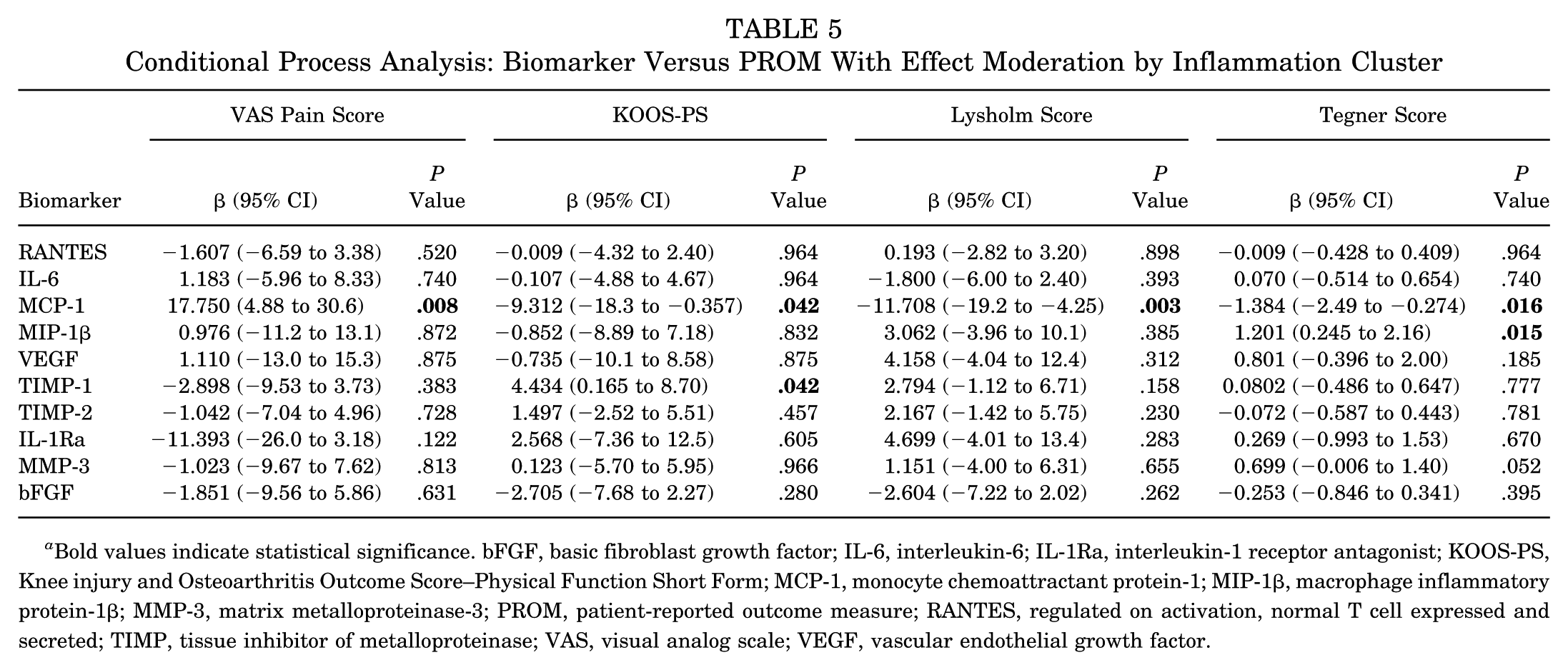
Bold values indicate statistical significance. bFGF, basic fibroblast growth factor; IL-6, interleukin-6; IL-1Ra, interleukin-1 receptor antagonist; KOOS-PS, Knee injury and Osteoarthritis Outcome Score–Physical Function Short Form; MCP-1, monocyte chemoattractant protein-1; MIP-1β, macrophage inflammatory protein-1β; MMP-3, matrix metalloproteinase-3; PROM, patient-reported outcome measure; RANTES, regulated on activation, normal T cell expressed and secreted; TIMP, tissue inhibitor of metalloproteinase; VAS, visual analog scale; VEGF, vascular endothelial growth factor.
To further illustrate the observed effect modification, the interaction between MCP-1 and inflammation phenotype on long-term patient-reported outcomes is visualized in Figure 5. Complete regression modeling data are included in Appendix Table A5 (available online).
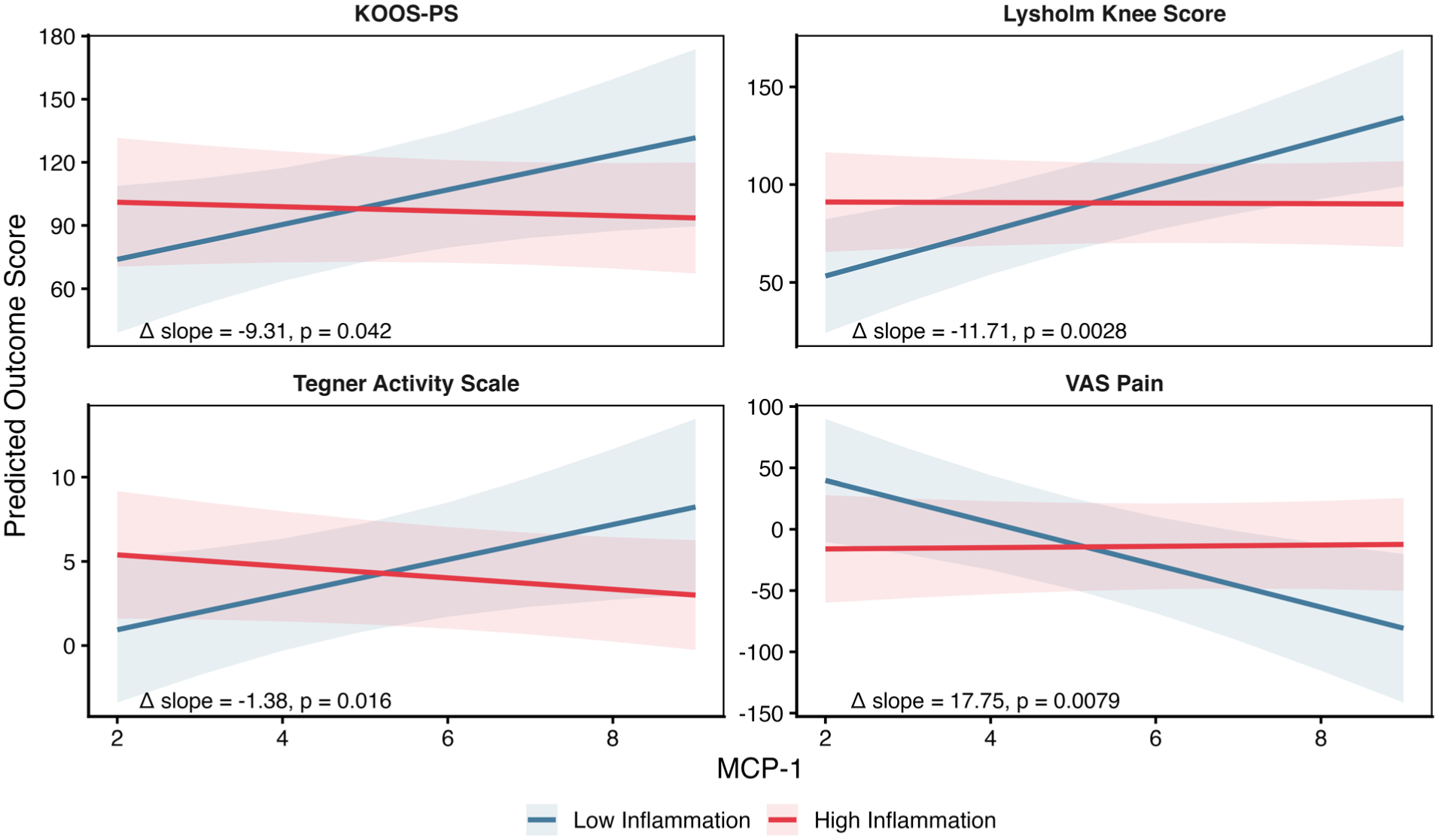
Predicted long-term patient-reported outcomes are plotted as a function of baseline monocyte chemoattractant protein-1 (MCP-1) concentration based on multivariable linear regression models including an interaction term between MCP-1 and inflammation phenotype (MCP-1 × cluster), adjusted for covariates. Lines represent model-predicted values for each phenotype, with shaded regions indicating 95% confidence intervals. The slope for the low-inflammation group reflects the main effect of MCP-1, while the slope for the high-inflammation group incorporates the interaction term (ie, deviation from the low-inflammation reference). The reported change (Δ) slope values represent the difference in MCP-1 effect between phenotypes. Significant interaction terms (P < .05) indicate that the effect of MCP-1 on outcomes depends on the underlying inflammatory milieu. KOOS-PS, Knee injury and Osteoarthritis Outcome Score–Physical Function Short Form; VAS, visual analog scale.
MCID Analysis
The proportion of patients achieving the MCID differed by inflammation cluster (Appendix Figure A1, available online). Patients in the high-inflammation cluster were more likely to achieve the MCID for the VAS pain score compared with those in the low-inflammation cluster (57.6% vs 17.6%; P < .05). No statistically significant differences in MCID achievement were observed for other PROMs.
Discussion
The principal finding of this study is that synovial fluid biomarker profiles at the time of ACL reconstruction with concomitant meniscal injury define biologically distinct inflammatory phenotypes that are associated with baseline symptom severity, magnitude of postoperative improvement, and biomarker-outcome relationships at long-term follow-up. Although patients in the high-inflammation cluster had significantly worse baseline pain and functional scores, long-term outcomes were comparable between clusters, suggesting convergence of recovery over time. However, the biological context in which recovery occurred differed between phenotypes, with cluster-dependent associations observed between specific biomarkers—most notably MCP-1—and long-term PROMs. These findings should be interpreted in the context that this study was not designed to evaluate structural joint degeneration, but rather to characterize biological inflammatory variation and its relationship to clinical recovery.
Patients in the high-inflammation cluster demonstrated significantly worse preoperative VAS pain, KOOS-PS, Lysholm, and Tegner values compared with the low-inflammation group. These findings are consistent with prior work demonstrating that elevated inflammatory mediators at the time of ACL injury are associated with greater symptom burden and cartilage metabolic activity.41-43 Clustering approaches using PCA and other multivariable techniques have been previously used to identify biologically distinct inflammatory phenotypes after knee injury, with these subgroups demonstrating differing symptom severity and recovery trajectories.2,20,43 For example, prior work has identified distinct inflammatory profiles associated with ACL injury, meniscal injury, and cartilage injury, with ACL and meniscal injuries displaying a pro-inflammatory phenotype characterized by elevated VEGF, IL-6, MMP-3, MIP-1β, and MCP-1, while more severe cartilage lesions were associated with reduced anti-inflammatory markers. 43 Additionally, a subset of patients have been shown to exhibit a “dysregulated inflammation” phenotype characterized by significantly greater concentrations of cartilage degradation biomarkers and a lower ratio of anti- to pro-inflammatory cytokines, independent of injury severity. 20 The elevated concentrations of IL-6, MCP-1, MIP-1β, VEGF, MMP-3, and IL-1Ra observed in the high-inflammation cluster reflect a coordinated pro-inflammatory and catabolic response, which likely contributes to nociceptive sensitization and functional impairment in the acute and subacute injury periods. Specifically, IL-6 has been positively correlated with pain after ACL injury and reconstruction (r = 0.52; P < .001), supporting the association between high inflammatory burden and worse baseline symptoms. 42 Furthermore, recent work has demonstrated that ACL and meniscal injuries display a pro-inflammatory phenotype characterized by elevated VEGF, IL-6, MMP-3, MIP-1β, and MCP-1, with this phenotype independently correlating with worse baseline knee function. 43
Importantly, these inflammatory phenotypes should not be interpreted as direct proxies for overall injury severity, as structural damage characteristics (eg, cartilage or bone injury severity) were not incorporated into the clustering algorithm. Instead, the identified clusters likely represent biologically distinct inflammatory responses to similar injury patterns rather than discrete structural severity strata.
However, inflammation is not purely detrimental. A degree of inflammatory signaling is essential, as it facilitates debris clearance, cellular recruitment, graft incorporation, and early tissue remodeling.26,33,46,49 Macrophages, recruited in part by chemokines, such as MCP-1, play essential roles in all phases of tissue repair by clearing damaged tissue, remodeling extracellular matrix, promoting angiogenesis, and supporting stem/progenitor cell activation.32,33,46 Although patients in the high-inflammation cluster demonstrated greater improvement in pain and Lysholm scores, the observational design precludes determining whether inflammation itself contributed to this improvement or simply reflects differences in injury timing, baseline symptom severity, or other unmeasured factors. Although symptom duration did not significantly differ between groups and was included as a covariate in regression analyses, the numerically longer interval in the low-inflammation group may still reflect temporal changes in inflammatory activity not fully captured by this study. Accordingly, the low-inflammation phenotype may partially represent a later stage of postinjury inflammatory resolution rather than a less severe initial injury. However, it may also represent a biologically distinct intra-articular environment with less acute inflammatory activation. This interpretation is supported by evidence that ACL reconstruction itself reinitiates an inflammatory response, with IL-1β and IL-6 concentrations increasing significantly in the first postoperative week, followed by increases in cartilage degradation markers at 4 weeks. 16 This “second inflammatory hit” may be necessary for graft healing and tissue remodeling, although excessive or prolonged inflammation can contribute to cartilage degradation. 24
Another possible explanation is that the high-inflammatory cluster started in a more painful preoperative state due to the exaggerated inflammatory response, but as the increased inflammation dampened over time, patients in the high cluster were able to reach the same level as those in the lower-inflammatory cluster. This would suggest that elevated inflammation is associated with preoperative pain but not long-term PROMs. Existing data are mixed on the effect of synovial fluid biomarkers on long-term PROMs; some studies have demonstrated associations between perioperative biomarker concentrations and PROMs at short- to intermediate-term follow-up,4,25,42 while others have found no significant relationship between biomarker profiles and symptom-based outcomes. 27
The most striking cluster-dependent finding involved MCP-1. Within the low-inflammation phenotype, higher MCP-1 levels were strongly and consistently associated with better long-term pain and functional outcomes. In contrast, MCP-1 demonstrated no significant associations within the high-inflammation cluster, and interaction models confirmed significant effect modification by phenotype across multiple PROMs. MCP-1 (CCL2) is a chemokine responsible for monocyte recruitment and macrophage activation. 50 While traditionally considered pro-inflammatory, MCP-1–mediated macrophage infiltration may also support tissue remodeling and debris clearance.33,46,50 Importantly, MCP-1 has been shown to be required for spontaneous articular cartilage regeneration postinjury in murine models, with MCP-1–deficient mice demonstrating impaired mesenchymal stem cell homing to injury sites and reduced regeneration. 19 In a relatively low-inflammatory environment, modest elevations in MCP-1 may reflect a more engaged reparative response, thereby supporting improved long-term recovery. Despite higher absolute MCP-1 concentrations in the high-inflammation cluster, MCP-1 was not associated with improved outcomes in that phenotype. This suggests that once inflammatory signaling is globally elevated, additional MCP-1 expression may not meaningfully alter downstream reparative processes because inflammatory pathways may already be maximally activated. MCP-1 may, in fact, contribute to excessive macrophage recruitment and prolonged inflammation, potentially inhibiting chondrogenesis of synovial mesenchymal progenitor cells, as demonstrated in vitro. 15
These findings underscore that the clinical implications of a given biomarker concentration cannot be interpreted in isolation; rather, its effect appears contingent on the broader inflammatory milieu. This phenotype-dependent behavior helps reconcile seemingly contradictory findings in the literature, where MCP-1 has been associated with both worse cartilage outcomes (when measured as changes from preoperative to 6 months post-ACL reconstruction serum levels) and prediction of cartilage lesions at 5 years (when measured in synovial fluid at time of surgery), yet not consistently associated with symptom-based outcomes in prior studies.15,28,30
The findings related to bFGF require careful interpretation. In the overall cohort, higher baseline bFGF concentrations were associated with lower Tegner activity levels at long-term follow-up. Within the high-inflammation cluster, bFGF was additionally associated with worse KOOS-PS values. When stratified by inflammatory phenotype, both relationships were observed only within the high-inflammation cluster, whereas no significant associations were detected within the low-inflammation group. Notably, mean bFGF concentrations were higher in the low-inflammation phenotype, indicating that absolute concentration alone does not explain its relationship with outcomes. These findings suggest that the clinical relevance of bFGF is context dependent, consistent with preclinical evidence demonstrating that FGF-2 overexpression worsened joint disease in inflamed but not noninflamed joints. 48 In human articular chondrocytes, bFGF activates FGFR1 to exert catabolic effects including upregulation of MMP-13, inhibition of proteoglycan synthesis, and antagonism of anabolic growth factors, and it cooperates synergistically with IL-17 to amplify inflammatory cytokine production in synovial fibroblast-like synoviocytes.17,39 IL-1β has also been shown to directly induce FGF-2 expression in chondrocytes, linking the inflammatory cascade to bFGF-mediated catabolic signaling. 8 Thus, within a high-inflammatory milieu, elevated bFGF may reflect amplified catabolic and pro-inflammatory synovial signaling rather than a reparative response. In lower-inflammatory settings, bFGF may reflect baseline fibroblast activity and tissue turnover without measurable functional impact, although the role of FGF-2 in human cartilage remains complex, with catabolic effects predominating via FGFR1 activation. 47
Despite substantial baseline differences, long-term PROMs were similar between clusters at a mean follow-up of >8 years. This convergence suggests that early differences in inflammatory phenotype were not reflected in long-term patient-reported outcomes in this cohort, resulting in comparable functional states between groups at follow-up. However, the pathway to that endpoint differed: the high-inflammation group improved more dramatically and was more likely to achieve the MCID for the VAS pain score. MCID values for the KOOS subscales after ACL reconstruction have been established as 12.1 for Sport and Recreation and 18.3 for Quality of Life, with clinically significant improvement typically occurring up to 1 year postoperatively.1,18 The higher rate of MCID achievement for VAS pain in the high-inflammation cluster was most likely driven by worse baseline pain scores and therefore greater opportunity for measurable improvement, rather than reflecting a true superiority in clinical recovery. Because patients in the low-inflammation cluster had less baseline pain, a ceiling effect likely limited their ability to achieve the MCID threshold despite comparable postoperative pain scores.
These data suggest that both excessive and insufficient inflammatory responses may influence recovery in different ways. A balanced inflammatory environment—rather than simply suppression of inflammation—may be critical to optimizing joint health and long-term outcomes.2,20 Serial sampling and integration with imaging biomarkers of cartilage health may further clarify the mechanistic links between early inflammation and later structural degeneration. Future work should examine whether targeted modulation of specific inflammatory pathways could optimize recovery without impairing necessary reparative processes, particularly given emerging evidence that biological agents such as mesenchymal stem cells and growth factors may enhance ACL healing and graft incorporation.23,40 Furthermore, structural imaging-based assessment of cartilage integrity and radiographic progression of posttraumatic osteoarthritis were not included in this study, as the primary objective was to evaluate synovial fluid inflammatory phenotypes in relation to patient-reported outcomes. Future studies integrating longitudinal imaging with synovial fluid biomarker profiling will be essential to determine whether early inflammatory phenotypes are associated with structural joint changes over time.
Limitations
This study should be interpreted through the context of its limitations. First, the modest sample size and single-center design may limit generalizability and reduce statistical power, particularly for subgroup and interaction analyses. Although statistically significant moderation effects were observed, the relatively small number of patients with complete long-term PROMs (n = 50) increases the risk of type 2 error for smaller associations and may limit the stability of regression estimates. In addition, a formal a priori power analysis was not performed, and the study may therefore be underpowered to detect more modest effects, particularly in the setting of loss to follow-up. Second, the absence of a comparator group (eg, patients without meniscal injury or with alternative injury patterns) limits the ability to determine the specificity and generalizability of the observed inflammatory phenotypes. Accordingly, our findings should be interpreted as describing heterogeneity within patients with combined ACL and meniscal injury rather than the isolated effect of ACL or meniscal pathology itself. Third, time from injury to surgery (symptom duration) was included as a covariate in all analyses; however, this variable may not fully capture the dynamic and nonlinear nature of postinjury inflammatory changes over time. Fourth, loss to follow-up introduces the potential for selection bias. Patients who completed long-term PROM assessments may differ systematically from those lost to follow-up in ways that were not captured in available covariates. Fifth, biomarker concentrations were measured at a single intraoperative time point. ACL injury and reconstruction initiate dynamic inflammatory and reparative processes that evolve over weeks to months. A single measurement cannot capture longitudinal fluctuations in cytokine expression or identify delayed dysregulation patterns. Serial sampling would provide a more comprehensive understanding of temporal inflammatory trajectories. Sixth, although biomarker assays were performed using validated multiplex ELISA platforms, variability in assay sensitivity, interassay reproducibility, and preanalytic sample handling may influence measured concentrations. While standardized processing protocols were used, minor technical variability cannot be excluded. Finally, PROMs are inherently subjective and may be influenced by psychosocial, socioeconomic, or behavioral factors not accounted for in this analysis. While validated instruments were used, patient perception of pain and function may not directly reflect underlying biological processes.
Conclusion
Synovial fluid biomarker profiles at the time of ACL reconstruction with concomitant meniscal injury define distinct inflammatory phenotypes that are associated with baseline symptom severity and differences in magnitude of improvement in patient-reported outcomes. Although long-term PROMs were similar between phenotypes, biomarker-outcome relationships varied by inflammatory profile. MCP-1 demonstrated significant phenotype-dependent associations with long-term outcomes, with higher concentrations associated with better pain and functional outcomes only within the low-inflammation phenotype. These findings suggest that the biological context in which recovery occurs differs across inflammatory phenotypes and may contribute to heterogeneity in clinical outcomes.
Supplemental Material
sj-docx-1-ajs-10.1177_03635465261459225 – Supplemental material for Knee Synovial Fluid Biomarker Type and Concentration With Long-Term Outcomes After ACL Reconstruction With Concomitant Meniscal Injury
Supplemental material, sj-docx-1-ajs-10.1177_03635465261459225 for Knee Synovial Fluid Biomarker Type and Concentration With Long-Term Outcomes After ACL Reconstruction With Concomitant Meniscal Injury by Mallory Ehlers, Layne C. Estes, Kendall Derry, Daniel J. Kaplan and Eric J. Strauss in The American Journal of Sports Medicine
Supplemental Material
sj-docx-2-ajs-10.1177_03635465261459225 – Supplemental material for Knee Synovial Fluid Biomarker Type and Concentration With Long-Term Outcomes After ACL Reconstruction With Concomitant Meniscal Injury
Supplemental material, sj-docx-2-ajs-10.1177_03635465261459225 for Knee Synovial Fluid Biomarker Type and Concentration With Long-Term Outcomes After ACL Reconstruction With Concomitant Meniscal Injury by Mallory Ehlers, Layne C. Estes, Kendall Derry, Daniel J. Kaplan and Eric J. Strauss in The American Journal of Sports Medicine
Supplemental Material
sj-docx-3-ajs-10.1177_03635465261459225 – Supplemental material for Knee Synovial Fluid Biomarker Type and Concentration With Long-Term Outcomes After ACL Reconstruction With Concomitant Meniscal Injury
Supplemental material, sj-docx-3-ajs-10.1177_03635465261459225 for Knee Synovial Fluid Biomarker Type and Concentration With Long-Term Outcomes After ACL Reconstruction With Concomitant Meniscal Injury by Mallory Ehlers, Layne C. Estes, Kendall Derry, Daniel J. Kaplan and Eric J. Strauss in The American Journal of Sports Medicine
Supplemental Material
sj-docx-4-ajs-10.1177_03635465261459225 – Supplemental material for Knee Synovial Fluid Biomarker Type and Concentration With Long-Term Outcomes After ACL Reconstruction With Concomitant Meniscal Injury
Supplemental material, sj-docx-4-ajs-10.1177_03635465261459225 for Knee Synovial Fluid Biomarker Type and Concentration With Long-Term Outcomes After ACL Reconstruction With Concomitant Meniscal Injury by Mallory Ehlers, Layne C. Estes, Kendall Derry, Daniel J. Kaplan and Eric J. Strauss in The American Journal of Sports Medicine
Supplemental Material
sj-docx-5-ajs-10.1177_03635465261459225 – Supplemental material for Knee Synovial Fluid Biomarker Type and Concentration With Long-Term Outcomes After ACL Reconstruction With Concomitant Meniscal Injury
Supplemental material, sj-docx-5-ajs-10.1177_03635465261459225 for Knee Synovial Fluid Biomarker Type and Concentration With Long-Term Outcomes After ACL Reconstruction With Concomitant Meniscal Injury by Mallory Ehlers, Layne C. Estes, Kendall Derry, Daniel J. Kaplan and Eric J. Strauss in The American Journal of Sports Medicine
Supplemental Material
sj-docx-6-ajs-10.1177_03635465261459225 – Supplemental material for Knee Synovial Fluid Biomarker Type and Concentration With Long-Term Outcomes After ACL Reconstruction With Concomitant Meniscal Injury
Supplemental material, sj-docx-6-ajs-10.1177_03635465261459225 for Knee Synovial Fluid Biomarker Type and Concentration With Long-Term Outcomes After ACL Reconstruction With Concomitant Meniscal Injury by Mallory Ehlers, Layne C. Estes, Kendall Derry, Daniel J. Kaplan and Eric J. Strauss in The American Journal of Sports Medicine
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.