
Abstract
Background:
Smoking has been linked to alterations in cellular inflammatory pathways and adverse outcomes in orthopaedic procedures. It is unclear how patient smoking affects the intra-articular microenvironment in the setting of symptomatic meniscal tears.
Purpose:
To investigate the association between tobacco use and variation in cytokine concentrations in knee synovial fluid in patients undergoing arthroscopic knee surgery for symptomatic meniscal injury.
Study Design:
Cohort study; Level of evidence, 3
Methods:
Patients who underwent knee arthroscopy for meniscal injury were prospectively enrolled between July 2011 and June 2019. Synovial fluid was aspirated and the concentrations of 10 biomarkers were measured by immunoassay. Smoking status, pack-years, and time since smoking cessation were collected. Log-normalized biomarker concentrations and smoking status were analyzed using analysis of variance (ANOVA) and linear regression.
Results:
A total of 297 patients (mean age, 45.7 ± 12.5 years; mean body mass index, 28.3 ± 5.3 kg/m2; 55.6% male) were included. Patients were divided into current smokers (n = 27), former smokers (n = 54), and nonsmokers (n = 216). No descriptive differences between groups were found. ANOVA showed significant differences (P < .01) in regulated on activation, normal T cell expressed and secreted (RANTES), monocyte chemotactic protein-1 (MCP-1), macrophage inflammatory protein-1β, vascular endothelial growth factor, tissue inhibitors of metalloproteinases 1 and 2, interleukin-1 receptor antagonist (IL-1Ra), matrix metalloproteinase (MMP-3), and basic fibroblast growth factor (bFGF) between cohorts. Post hoc analysis revealed a significant difference between nonsmokers and former smokers for all biomarkers, aside from interleukin (IL)–6, that showed a significant difference on ANOVA testing. Significant differences were also found between smoker and nonsmoker cohorts for biomarkers MCP-1, MIP-1β, IL-1Ra, MMP-3, and bFGF. Linear regression analysis demonstrated a significant negative association between pack-years in the current smoker group and RANTES (β = −0.5115; P = .0358), and a positive association between time since quitting and IL-6 (β = 0.3842; P = .0084).
Conclusion:
Smoking status was found to be significantly associated with alterations in synovial fluid biomarker profiles in patients undergoing arthroscopic knee surgery for meniscal injury. RANTES was negatively associated with pack-years in current smokers, and IL-6 was positively associated with time since smoking cessation in former smokers. These findings suggest that smoking may have lasting effects on joint inflammation after injury, and that biomarker profiles can provide insight into local tissue responses influenced by smoking history.
Tobacco use has been linked to alterations in several biological processes critical for postoperative wound healing.2,17 Tobacco is known to inhibit the function of platelets, macrophages, and fibroblasts, while causing tissue ischemia due to the induction of adrenergic vasoconstriction—all functions vital to proper healing and tissue formation after surgery.8,10 Perioperative smoking cessation is therefore routinely advised and has been shown to be effective when initiated at various time points. 2
In the realm of orthopaedic surgery, prior investigations have found that smoking may adversely affect bone density, fracture fixation, and postoperative anterior cruciate ligament (ACL), meniscal, and cartilage healing. 2 Smoking has been associated with particularly unfavorable outcomes after meniscal repair, including higher rates of adverse events and hospital readmission. 6 Previous research has characterized the inflammatory response pathway after meniscal injury and how alterations in the synovial environment may affect postoperative outcomes.7,8,10,11 Relatedly, tobacco exposure has previously been shown to affect inflammation on a cellular level, which may potentially affect synovial fluid biomarker expression after meniscal injury.14,15 Prior studies have demonstrated that smoking induces inflammatory biomarker interleukin (IL)–1β in synoviocytes of patients with rheumatoid arthritis and IL-1α, IL-1β, IL-6, and IL-8 in synoviocytes.1,16 However, the relationship between smoking and the intra-articular microenvironment in the setting of symptomatic meniscal tears has not yet been investigated.
Therefore, the purpose of the current study was to investigate the association between tobacco exposure and variation in cytokine profile concentrations in knee synovial fluid in patients undergoing arthroscopic knee surgery for symptomatic meniscal injury. We hypothesized that smokers, former smokers, and never-smokers would demonstrate distinct profiles of pro-inflammatory and anti-inflammatory cytokines at the time of arthroscopy, with smokers demonstrating higher concentrations of pro-inflammatory synovial fluid biomarkers.
Methods
Study Design
This was a retrospective analysis of a prospectively collected database of biospecimens and clinical data approved by the institutional review board (IRB No. 15-00929), and all patients who underwent arthroscopic surgery for symptomatic meniscal injuries at a large urban academic medical center between July 2011 and June 2019 were included. Eligible patients required operative management for meniscal injuries and consented to synovial fluid collection from the operative knee on the day of surgery for biomarker analysis. Exclusion criteria included a history of inflammatory or autoimmune disease, history of blood-borne illness, intra-articular injection in the operative knee within 90 days before surgery, immunomodulatory therapy within the past year, concomitant ligamentous or chondral injuries, or insufficient synovial fluid volume obtained at aspiration. Patients with isolated meniscal injuries identified as current or former smokers via chart review at the time of surgery were selected for analysis. Smoking status was determined by a patient's documented status at the time of surgery in the chart; there was no minimum cessation time required to be considered a former smoker, but time since cessation, if available, was recorded for former smokers. The 2 smoking types gathered included cigarettes/cigars/pipes and e-cigarettes. Smoking pack-years was retrospectively quantified for current smokers. Patients were matched by age, sex, and body mass index (BMI) in a 1:2:8 ratio of current smokers, former smokers, and nonsmokers based on the naturally occurring distribution in our cohort and relatively small numbers of current smokers. Descriptive data including age, sex, and BMI at surgery were additionally obtained.
Synovial Fluid Collection and Biomarker Analysis
On the day of surgery, a minimum of 100 µL of synovial fluid was aspirated from the operative knee before incision using an 18-gauge needle and 20-mL syringe under standardized sterile conditions (chlorhexidine gluconate/70% isopropyl alcohol). Samples were immediately transferred to sterile tubes containing Halt Protease Inhibitor Cocktail (ethylenediaminetetraacetic acid-free; Pierce Biotechnology) at a ratio of 10 µL of inhibitor per 1000 µL of synovial fluid. After centrifugation at 3820 rpm for 10 minutes at 4°C, supernatants were aliquoted into sterile cryotubes and stored at −80°C until assay. For the duration of this study, all methods remained consistent; there were no changes in synovial fluid storage conditions, assay methods, or clinical practice that may have changed biomarker results.
Synovial fluid samples were thawed and analyzed in duplicate using custom and commercially available precoated multiplex enzyme-linked immunosorbent assay (ELISA) plates from Meso Scale Discovery (MSD). Quantification of biomarker concentrations was performed using the MSD QuickPlex SQ120 Plate Reader/Scanner. Ten biomarkers were evaluated (Table 1): basic fibroblast growth factor (bFGF), regulated on activation, normal T cell expressed and secreted (RANTES) (C-C motif chemokine ligand 5), IL, IL-1 receptor antagonist (IL-1Ra), monocyte chemotactic protein-1 (MCP-1), macrophage inflammatory protein-1β (MIP-1β), matrix metalloproteinase (MMP)–3, tissue inhibitors of metalloproteinases (TIMPs) 1 and 2, and vascular endothelial growth factor (VEGF).
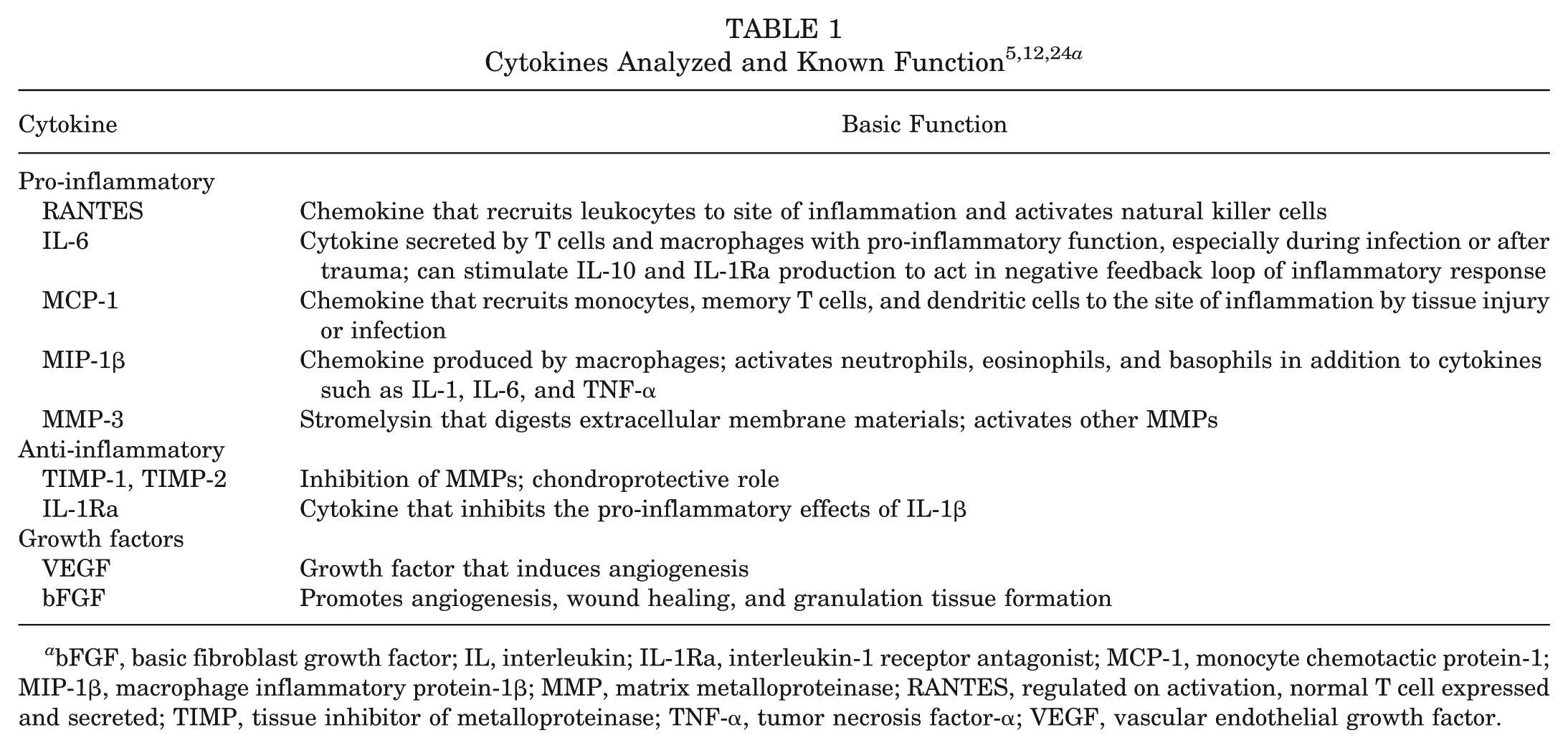
bFGF, basic fibroblast growth factor; IL, interleukin; IL-1Ra, interleukin-1 receptor antagonist; MCP-1, monocyte chemotactic protein-1; MIP-1β, macrophage inflammatory protein-1β; MMP, matrix metalloproteinase; RANTES, regulated on activation, normal T cell expressed and secreted; TIMP, tissue inhibitor of metalloproteinase; TNF-α, tumor necrosis factor-α; VEGF, vascular endothelial growth factor.
Statistical Analysis
All statistical analyses were performed using GraphPad Prism (Version 10.6.0) and RStudio (Version 2026.01.2+418; Posit). Descriptive variables (age, sex, and BMI) were compared across groups using analysis of variance (ANOVA) with post hoc comparisons. Synovial fluid biomarker concentrations were log-normalized to evaluate skewness and standardized by Z score to facilitate regression comparison. ANOVA was performed for each biomarker variable among the current smokers, former smokers, and nonsmokers with pairwise comparisons performed for significant findings. Post hoc pairwise comparisons were adjusted using Bonferroni correction. A minimum detectable effect size (MDES) analysis was performed based on observed variance and sample sizes, assuming an α value of .05 and 80% power. Regression analyses examining the association between pack-years as a continuous predictor and individual biomarkers were considered secondary and exploratory. To provide a clear and consistent assessment of effect magnitude and precision, these analyses are presented unadjusted, with unadjusted P values accompanied by effect sizes and 95% confidence intervals. Multiple testing correction was not applied, as the emphasis was on the size and direction of associations rather than on strict statistical significance, allowing the results to inform hypothesis generation for future studies. Statistical significance was defined as P value <.05 for all analyses.
Results
Patient Characteristics
There were 994 patients identified who underwent surgery for a meniscal injury between the years of 2011 and 2024. Of these, 479 patients had isolated meniscal injury, and 443 had no previous ipsilateral surgery. A total of 297 patients with isolated meniscal injury requiring arthroscopy had smoking status available, a sufficient synovial fluid amount for testing, and complete ELISA biomarker data (Figure 1). The final cohort included patients who underwent biomarker testing between 2011 and 2019; patients until 2024 were screened, but results beyond 2019 were not analyzed due to incomplete biomarker results. In addition, patients who currently or formerly used e-cigarettes were excluded due to low prevalence. The patients were divided into groups based on a 1:2:8 ratio of current smokers (n = 27), former smokers (n = 54), and nonsmokers (n = 216) based on the natural distribution of the cohort. The mean age at the time of surgery was 45.7 ± 12.5 years, the mean BMI was 28.3 ± 5.3 kg/m2, and 55.6% of the patients were male. There were no significant differences in the distributions of age, sex, and BMI among the 3 groups (Table 2).
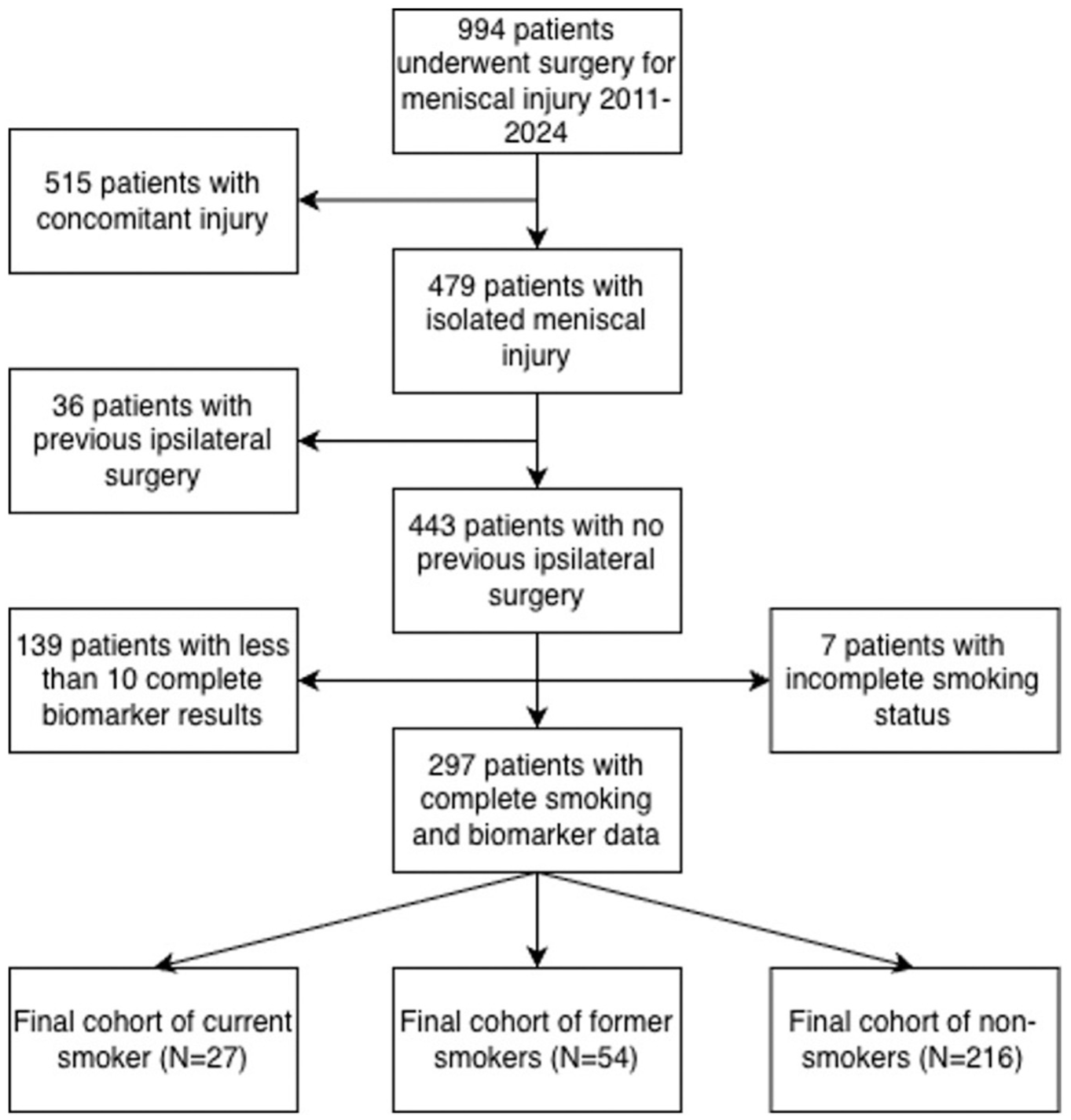
Diagram of included patients.
Cohort Characteristics a
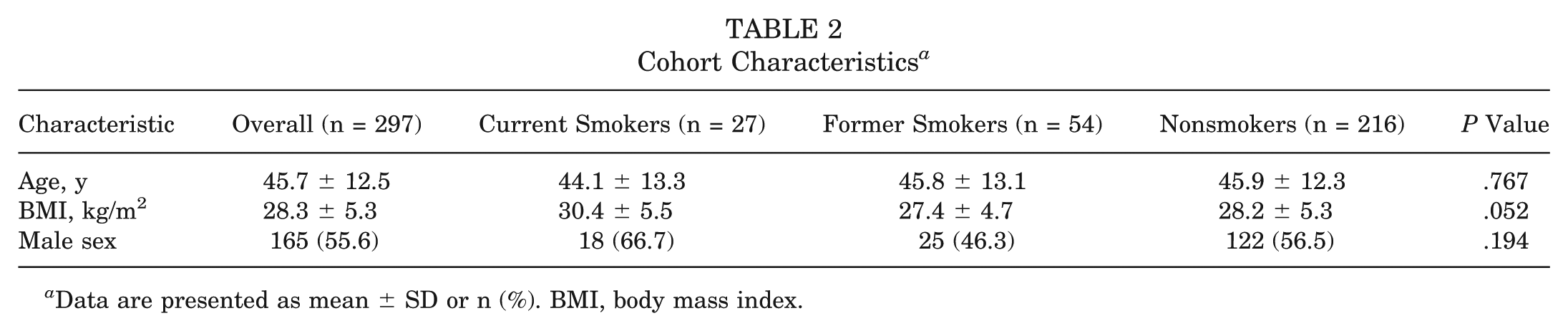
Data are presented as mean ± SD or n (%). BMI, body mass index.
Patients in the current smoker and former smoker groups were found to have means of 10.2 ± 8.5 and 12.6 ± 14.3 pack-years (P = .54), respectively. Of the former smokers, the mean time since quitting before surgery was 15.9 ± 13.6 years (median, 15.0 years; IQR, 22.5 years).
ANOVA of Biomarkers
ANOVA showed significant differences (P < .01) in biomarker concentrations between groups for every biomarker, besides IL-6 (Table 3).
ANOVA of Log-Normalized Biomarker Concentrations Between Groups a
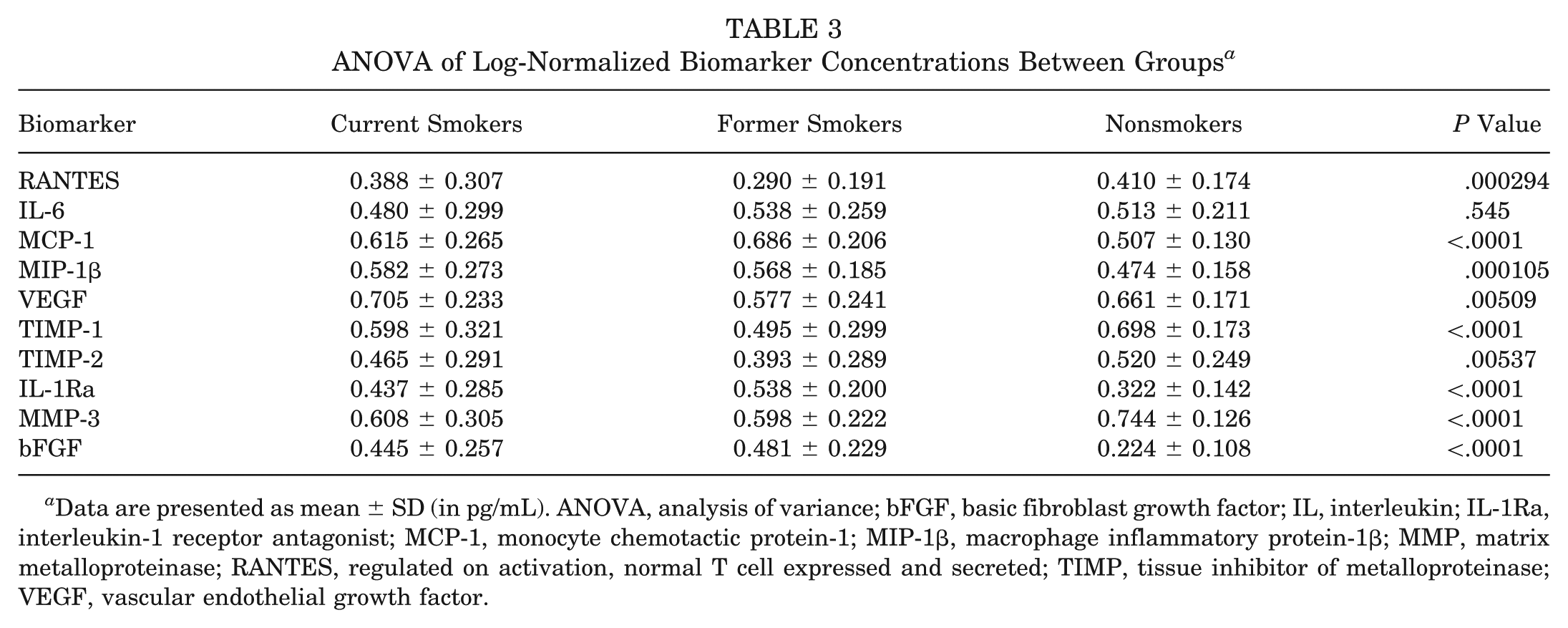
Data are presented as mean ± SD (in pg/mL). ANOVA, analysis of variance; bFGF, basic fibroblast growth factor; IL, interleukin; IL-1Ra, interleukin-1 receptor antagonist; MCP-1, monocyte chemotactic protein-1; MIP-1β, macrophage inflammatory protein-1β; MMP, matrix metalloproteinase; RANTES, regulated on activation, normal T cell expressed and secreted; TIMP, tissue inhibitor of metalloproteinase; VEGF, vascular endothelial growth factor.
Post Hoc Analysis of Biomarkers
Post hoc analysis revealed a significant difference between nonsmokers and former smokers for all biomarkers that had a significant difference on ANOVA testing (Table 4). Significant differences were also found between the current smoker and nonsmoker cohorts for biomarkers MCP-1, MIP-1β, IL-1Ra, MMP-3, and bFGF. Lastly, VEGF and IL1-Ra had significant differences on pairwise comparison between the smoker and former smoker cohorts (Table 4). The minimum detectable difference between current and nonsmokers ranged from 0.13 to 0.18 across biomarkers, corresponding to a standardized effect size of 0.57. For comparisons between current and former smokers, the minimum detectable difference ranged from 0.15 to 0.21, corresponding to a standardized effect size of 0.66.
Post Hoc Analysis of Biomarkers a
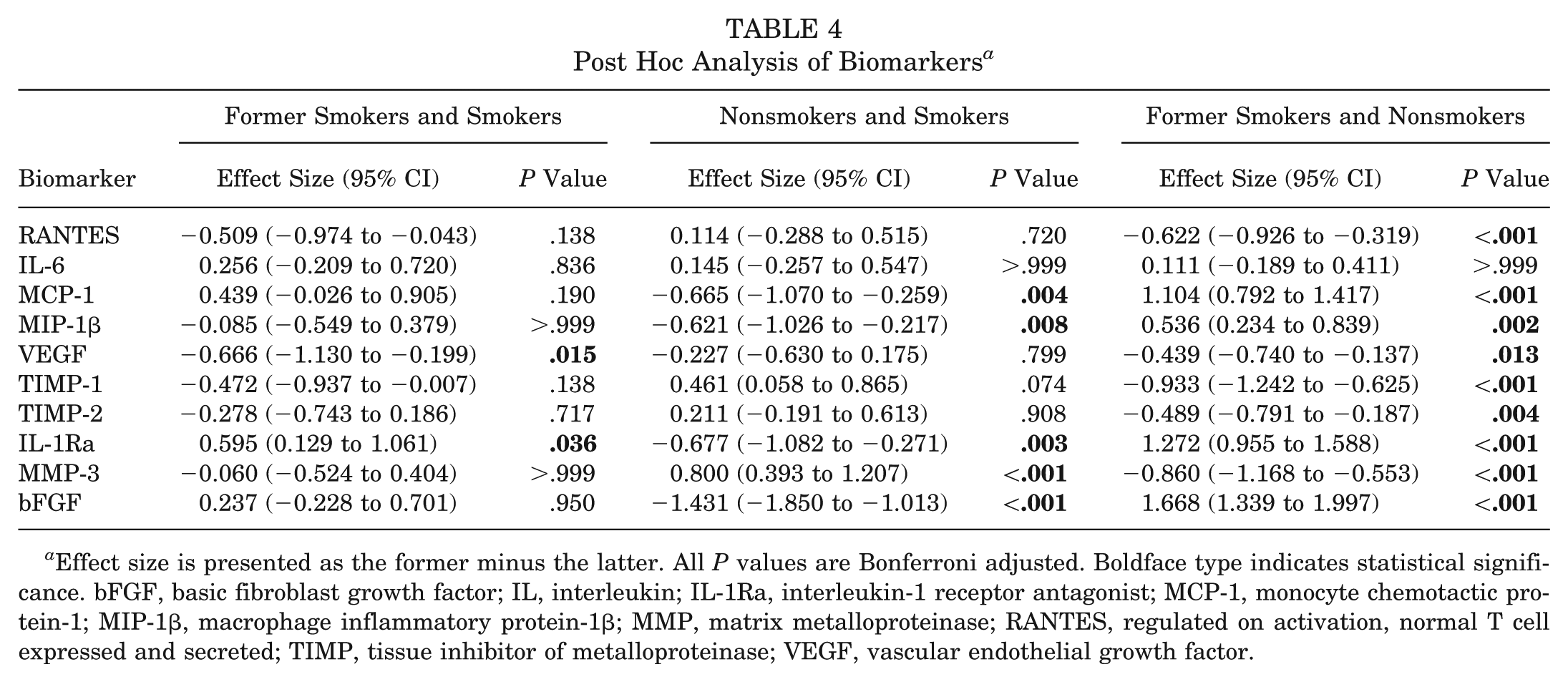
Effect size is presented as the former minus the latter. All P values are Bonferroni adjusted. Boldface type indicates statistical significance. bFGF, basic fibroblast growth factor; IL, interleukin; IL-1Ra, interleukin-1 receptor antagonist; MCP-1, monocyte chemotactic protein-1; MIP-1β, macrophage inflammatory protein-1β; MMP, matrix metalloproteinase; RANTES, regulated on activation, normal T cell expressed and secreted; TIMP, tissue inhibitor of metalloproteinase; VEGF, vascular endothelial growth factor.
Regression Analysis of Biomarkers
Linear regression analysis (Table 5) demonstrated a significant negative association between pack-years in the current smoker group and RANTES concentration (β = −0.5115; P = .0358); however, no association was found between pack-years in the former smoker group and any biomarker. There was a positive association between time since quitting and IL-6 concentration (β = 0.3842; P = .0084).
Regression Analysis of Pack-Years and Years Since Quitting With Biomarkers a
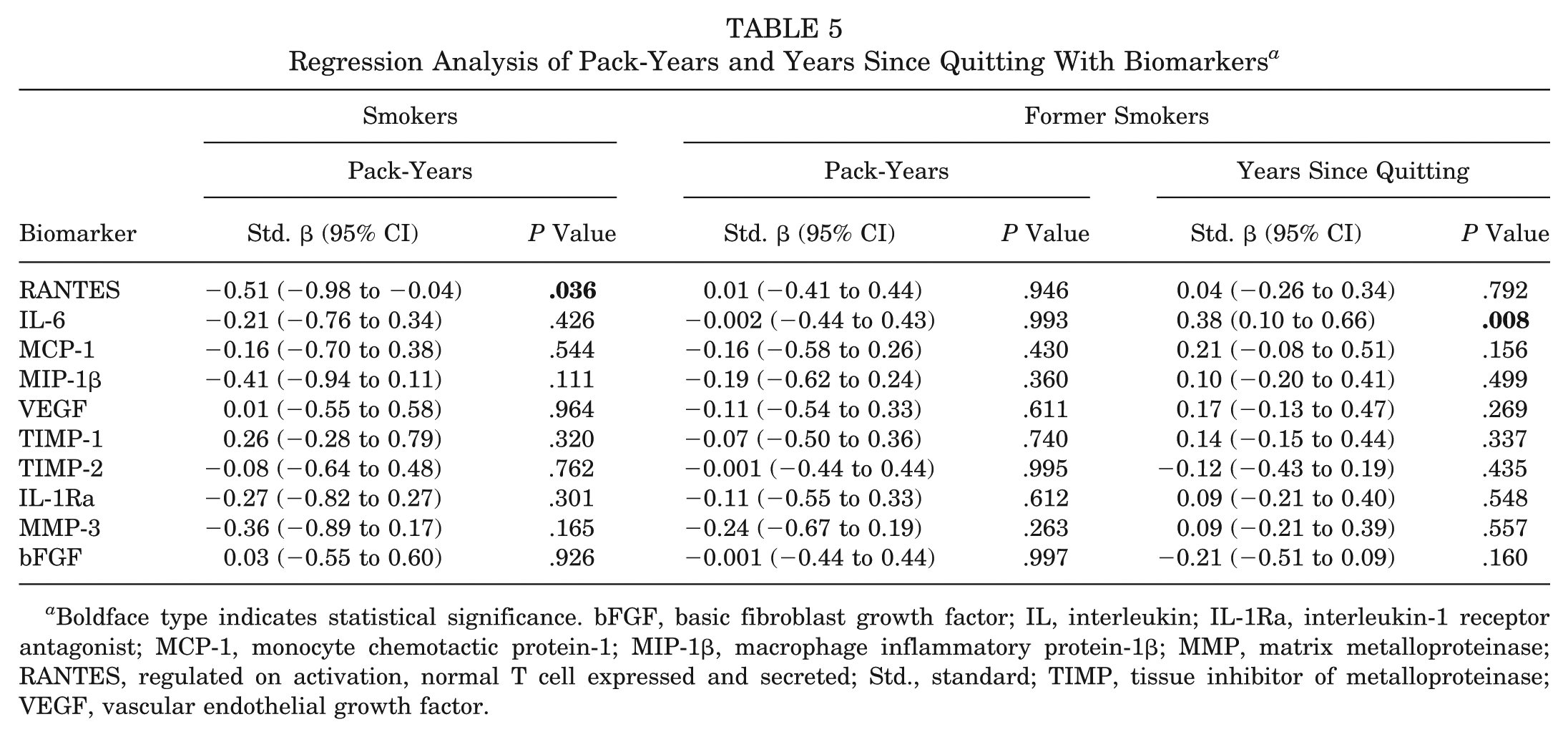
Boldface type indicates statistical significance. bFGF, basic fibroblast growth factor; IL, interleukin; IL-1Ra, interleukin-1 receptor antagonist; MCP-1, monocyte chemotactic protein-1; MIP-1β, macrophage inflammatory protein-1β; MMP, matrix metalloproteinase; RANTES, regulated on activation, normal T cell expressed and secreted; Std., standard; TIMP, tissue inhibitor of metalloproteinase; VEGF, vascular endothelial growth factor.
Discussion
The primary finding of this study is that in patients undergoing knee arthroscopy for meniscal tears, there were significantly different concentrations of synovial fluid biomarkers among current smokers, former smokers, and nonsmokers. In particular, these findings suggest that smoking is associated with a distinct alteration of the intra-articular environment in the setting of a symptomatic meniscal tear, potentially affecting leukocyte recruitment, immune cell signaling, angiogenesis, and extracellular matrix regulation within the knee joint. Prior studies of synovial fluid markers in the setting of knee injury have demonstrated that meniscal pathology is not merely a mechanical condition but is accompanied by a biologically active inflammatory response that correlates with symptoms and cartilage health.5,6,21 Furthermore, smoking cessation directly after surgery has been validated through rat in vitro and in vivo models to be associated with increased bone density and an improved fracture healing rate. 9 In ACL reconstructions, patient smoking has also been demonstrated to negatively impact functional outcome scores. 13 Our results extend this paradigm by identifying smoking as an important modifier of this synovial inflammatory response.
A key observation was the dose-dependent relationship between tobacco exposure and synovial chemokine signaling. Increasing pack-years was negatively associated with synovial RANTES concentration in current smokers. RANTES is a chemoattractant for leukocytes and natural killer T cells and plays an important role in coordinating inflammatory cell trafficking within injured joints.3,15 Reduced RANTES expression has previously been observed in contralateral knees that later develop pain patterns resembling those seen in advanced cartilage injury, suggesting a role in chronic joint disease pathophysiology. 7 Furthermore, RANTES has been implicated as a crucial mediator of rheumatoid arthritis, with a study by Stanczyk et al 18 demonstrating high concentrations and chemotactic associations of RANTES in patients with rheumatoid arthritis, a finding consistent with other similar studies.22,23 The present findings indicate that smoking may induce similar suppression of RANTES signaling within the injured knee, supporting broader immunological literature demonstrating that cigarette smoke exposure disrupts chemokine gradients and immune cell recruitment despite systemic pro-inflammatory effects. 4 This dysregulated inflammatory signaling may impair appropriate synovial responses to meniscal injury and contribute to altered pain perception.
Former smokers demonstrated a distinct biomarker profile compared with nonsmokers, with time since smoking cessation positively associated with synovial IL-6 concentration. Although IL-6 levels did not differ significantly between groups at the cohort level, this association suggests that the synovial inflammatory milieu remains dynamic and responsive to smoking behavior over time. IL-6 is cytokine central to nociception and chronic synovial inflammation. Multiple studies have identified IL-6 as one of the strongest molecular correlates to pain and functional limitation after knee injury, including associations with Knee injury and Osteoarthritis Outcome Score, Lysholm, and pain values.11,14,19 The observed relationship between cessation duration and IL-6 supports the concept that smoking-related immune modulation may persist after cessation and evolve rather than normalize immediately. The positive association may reflect that the joint's IL-6–mediated immune response is suppressed by smoking, and smoking cessation revealed a meaningful return of this immune function. However, given the wide range in cessation, this may reflect residual confounding by age or joint degeneration rather than a persistent isolated effect of prior smoking. While these results should be considered primarily exploratory, these findings reinforce the importance of encouraging early smoking cessation as part of preoperative counseling, as even partial reduction in smoking may restore some pro-inflammatory signaling, evidenced by a negative association between RANTES and pack-years.
The observed alterations in matrix remodeling cytokines and angiogenic mediators further support the biological relevance of smoking-related synovial changes. MMP-3, TIMP-1, and TIMP-2 regulate cartilage matrix turnover and tissue homeostasis, while VEGF and bFGF are critical for angiogenesis and reparative responses. Prior studies of knee injury and early cartilage degeneration have demonstrated associations between synovial MMPs, TIMPs, and clinical outcomes, suggesting that imbalance in these pathways may predispose patients to progressive joint degeneration. 14 BFGF has been implicated in synovitis and pain sensitization after intra-articular injury. 20
Taken together, these findings suggest that smoking history—both active exposure and prior use—is associated with durable alterations in the synovial inflammatory environment in patients with isolated meniscal injury. These molecular differences may provide a mechanistic explanation for the reported worse symptoms often observed in smokers undergoing arthroscopic knee surgery. The persistence of biomarker alterations in former smokers underscores the importance of early smoking cessation counseling and suggests that smoking-related joint effects may extend well beyond cessation. Importantly, BMI approached statistical significance between groups (P = .052), with the highest values observed in the current smoker cohort, including an extreme outlier. Obesity has previously been shown to impact distribution of inflammatory cytokines in addition to its known impact on joint biomechanics. 25 Given the relationship between BMI and inflammation, this may have influenced biomarker levels; however, adjustment for BMI in regression models likely mitigated this effect, although residual confounding remains possible.
Furthermore, the findings in this study may be useful in preoperative counseling when discussing smoking status with patients. Although long-term outcomes and complications were not the focus of this paper, it is important to discuss with patients that smoking has been shown to significantly alter the joint environment through a variety of inflammatory cytokines. In addition, smoking cessation was shown to be associated with another distinct alteration in cytokine profile, including the return of IL-6. Clinicians may discuss that longer duration of smoking cessation is generally advisable, although the precise duration at which biomarker levels respond remains unclear. Importantly, these findings reinforce the broader benefits of smoking cessation for joint health and postoperative recovery.
Limitations
The findings of this study must be understood through the context of its limitations. The single-center design, retrospective review of smoking status, and modest sample size may limit generalizability. In particular, there was a small cohort of current smokers (n = 27) due to the relatively low numbers of smokers in our outpatient surgery facility and preoperative smoking cessation counseling. Although our MDES demonstrated that our study was powered to detect moderate differences in synovial fluid biomarker levels, nonsignificant results involving this group should be interpreted with caution, as our study may have been underpowered to detect a change. Biomarkers and patient-reported outcomes (PROs) were measured at a single time point, precluding assessment of dynamic changes and distinguishment between transient and sustained effects of smoking in the postoperative period, which may be better observed with serial biomarker concentrations and PRO assessments. In addition, the study of our 10 chosen biomarkers may not capture the full interaction of cytokines in the inflammatory environment. Additional matrix degeneration and extracellular inflammatory biomarkers such as IL-1β and ADAMTS (a disintegrin and metalloproteinase with thrombospondin motifs) are important areas of future study. Tobacco exposure was collected via retrospective chart review of patient-reported smoking history, which may introduce recall bias. Additionally, while all patients follow a similar postoperative protocol, potential confounders such as baseline systemic inflammation, comorbidities, or lifestyle factors were not fully controlled. Additionally, several clinically important factors, such as tear chronicity, tear morphology, meniscal laterality, degenerative versus traumatic origin, surgical technique, and baseline cartilage status were not included in the adjusted models because of the limited sample size of the current smoker cohort and the heterogeneity across these factors, which would have resulted in unstable estimates. Given their potential influence on synovial inflammatory profiles, omission of these variables may limit the strength of causal inference and raises the possibility of residual confounding. The use of e-cigarettes and vapes was not included in the study; additional research stratifying biomarkers in patients engaging with alternative smoking methods would broaden the applicability to the current patient population and their smoking habits as smokeless tobacco remains popular. Future longitudinal studies with larger cohorts and serial sampling are needed to elucidate the temporal relationship between smoking, synovial biomarkers, and clinical outcomes.
Conclusion
Smoking status was found to be significantly associated with alterations in synovial fluid biomarker profiles in patients undergoing arthroscopic knee surgery for symptomatic meniscal injury. Increased cumulative smoking exposure was associated with reduced RANTES levels in current smokers, while longer time since quitting was linked to higher IL-6 levels in former smokers. These findings suggest that smoking may have biologically relevant effects on joint inflammation, and that biomarker profiles can provide insight into local tissue responses influenced by smoking history. Data from the current study may be utilized to inform preoperative counseling and to generate further hypotheses surrounding smoking and the dynamic synovial microenvironment.
Supplemental Material
sj-docx-1-ajs-10.1177_03635465261459231 – Supplemental material for The Effect of Smoking History on Inflammatory Biomarkers in Synovial Fluid of Patients Undergoing Arthroscopic Knee Surgery for Meniscal Injury
Supplemental material, sj-docx-1-ajs-10.1177_03635465261459231 for The Effect of Smoking History on Inflammatory Biomarkers in Synovial Fluid of Patients Undergoing Arthroscopic Knee Surgery for Meniscal Injury by Jessica L. Kurtz, Mallory Ehlers, Samuel R. Montgomery, Daniel J. Kaplan and Eric J. Strauss in The American Journal of Sports Medicine
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.