
Abstract
Background:
Anterior cruciate ligament (ACL) injury significantly increases the risk for developing knee osteoarthritis (OA), yet the early contributors to cartilage degeneration remain poorly understood. While range of motion (ROM) deficits after ACL reconstruction (ACLR) are associated with long-term development of radiographic OA, the association between early ROM recovery and cartilage composition has not been established.
Hypothesis:
Knee extension ROM deficits at 2 months after ACLR would be associated with worsening tibiofemoral and patellofemoral cartilage T2 relaxation times at 6 months.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
A total of 30 participants (15-35 years) were enrolled within 1 month of ACL injury and before ACLR. At 2 months post-ACLR, active knee extension ROM was measured in the supine position using a goniometer. An extension deficit was considered >3° less extension in the injured knee compared to the uninjured side. Quantitative magnetic resonance imaging–based T2 relaxometry of the injured knee was performed preoperatively and at 6 months post-ACLR to measure percent change in mean T2 relaxation times in predefined tibial and femoral cartilage regions. Independent t tests were used to compare changes in T2 values between participants with and without an extension deficit.
Results:
The mean age of the participants was 18.8 ± 3.9 years, and 63.3% were female. Fifteen (50.0%) participants exhibited an extension deficit at 2 months. Those with an extension deficit demonstrated a greater increase in T2 relaxation time in the anterior (mean difference, 10.21% [95% CI, 3.67%-16.76%]; P = .003) and weightbearing (mean difference, 6.14% [95% CI, 2.19%-10.09%]; P = .004) cartilage of the medial femoral condyle. No significant group differences were observed in other cartilage regions (all P > .05).
Conclusion:
Knee extension ROM deficits at 2 months post-ACLR are associated with early compositional changes in the medial femoral cartilage, indicating a potential relationship between limited extension and OA risk.
Keywords
Of individuals who undergo anterior cruciate ligament reconstruction (ACLR), 50% develop knee osteoarthritis (OA) within 5 to 15 years of surgery.30,31,37 Given the substantial long-term incidence of OA, early identification of individuals at high risk for OA is critical to intervene and prevent irreversible joint degeneration and functional decline. Although the mechanisms underlying knee OA development after anterior cruciate ligament (ACL) injury are not fully understood, current evidence implicates a combination of structural, biological, and mechanical factors in the degradation of the extracellular matrix and impaired matrix repair.7,28,35,43 These changes ultimately lead to cartilage loss and joint deterioration.
Return of full knee range of motion (ROM), particularly extension, is considered a critical early milestone in ACLR rehabilitation. 6 Extension deficits ≥3° have been independently associated with poor long-term outcomes, including increased risk for radiographic OA and persistent functional limitations.49,50,52 These deficits may alter joint loading patterns and increase mechanical stress on cartilage, accelerating degeneration. Despite these associations, the relationship between early ROM deficits and subsequent cartilage compositional changes has not been well characterized. Clarifying this link will strengthen the evidence supporting early restoration of knee extension as a critical rehabilitation goal after ACLR, with potential implications for long-term joint health.
Previous studies linking knee extension ROM deficits to knee OA have relied on radiographic measures such as the Kellgren scale.49,50,52 However, altered biomechanics and symptoms like pain and declining function often precede radiographic changes, making such methods insufficient for early detection. Quantitative magnetic resonance imaging (MRI) such as T2 relaxation time mapping offers a more sensitive, noninvasive approach to detecting early cartilage degeneration.10,41 T2 relaxation times reflect changes in water content and collagen organization within the cartilage. Elevated baseline T2 values have cross sectionally been associated with OA severity and predicted OA progression and morphological changes.10,29 Furthermore, longitudinal increases in T2 relaxation times have been observed within populations at risk of OA progression and after ACLR, with these early T2 changes being associated with later cartilage loss.12,33,57
The purpose of this study was to determine if knee extension ROM at 2 months post-ACLR is associated with tibiofemoral and patellar cartilage composition at 6 months. We hypothesized that knee extension ROM deficits would be associated with worsening tibiofemoral and patellar cartilage T2 relaxation times, a possible indicator of early OA development.
Methods
Study Design and Ethical Approval
This study is a secondary analysis of a prospective cohort study that was approved by an institutional review board (IRB No. 416-17-FB). Participants at least 19 years of age provided written informed consent. Minors provided assent with written consent from a parent or legal guardian.
Study Participants
A total of 30 participants between the ages of 15 and 35 years were enrolled in the study within 1 month of acute ACL injury before ACLR. Individuals <15 years were excluded due to possible skeletal immaturity, and individuals >35 were excluded due to potential baseline OA already present before ACL injury. Exclusion criteria included a previous injury or surgery to either knee, concomitant grade 3 tear to other knee ligaments, meniscal tear with anticipated meniscectomy by the treating orthopaedic surgeon, acute chondral lesions or degenerative cartilage changes identified on postinjury MRI, or open growth plates requiring an altered ACLR technique (ie, physeal sparing). Additional exclusion criteria included history of inflammatory disease, immune compromise, chronic use of nonsteroidal inflammatory drugs, history of cortisone injection during the prior 3 months, current pregnancy, or contraindications to MRI. Participants completed rehabilitation according to their surgeon's postoperative protocol; rehabilitation content and adherence were not standardized or monitored during the study period.
Participant Characteristics
Participants reported age, sex, race, patient-reported outcomes (International Knee Documentation Committee Subjective Knee Form 200023,24,46 and Knee injury and Osteoarthritis Outcome Score),8,40 and preinjury cutting and pivoting activity level (level 1: soccer, basketball, etc; level 2: tennis, baseball, etc; level 3: walking, cycling)17,21 utilizing REDCap (Research Electronic Data Capture). REDCap is a secure, web-based application designed to support data capture for research studies. 19 Height and weight were measured barefoot using a portable stadiometer before ACLR. Graft type and concomitant surgical procedures were obtained from each participant's operative report.
Extension ROM
Active knee extension ROM for each limb was measured at 2 months post-ACLR with the participant lying supine with the heel of the foot placed on a bolster to allow for potential hyperextension (Figure 1). A standard goniometer was aligned with the greater trochanter and lateral malleolus, as described by Shelbourne et al. 52 An extension difference >3° in the injured knee compared to the uninjured side was used to define an extension deficit, consistent with previous reports and the intrarater minimal detectable change of a standard goniometer.34,51

Knee extension range of motion measurement in the supine position.
MRI Acquisition and T2 Relaxation Time
MRI was performed on the injured knee within 1 month of ACL injury (before ACLR) and at 6 months post-ACLR. Before MRI was performed, participants sat for 30 minutes due to acute effects of knee loading on T2 relaxation time. 53 To control for the effect of daily activity on quantitative MRI markers, each MRI scan began between 4:15 and 5:45 PM. A 3-T Philips Ingenia MRI scanner (Philips North America Corporation) equipped with a 16-channel transmit/receive knee coil was used with the knee in slight flexion and neutral rotation. For T2 mapping, a multi-spin-echo (MSE) sequence was acquired with parameters as specified in Wellsandt et al. 56 MRI-based T2 mapping is effective for detecting changes in cartilage health before radiographic changes by measuring variations in T2 relaxation time.12,33,57 In addition to MSE, a fat-suppressed proton density–weighted spin-echo (SE) sequence in axial, coronal, and sagittal orientations and a sagittal T1-weighted SE sequence were included in the MRI protocol.
Voxel-wise MSE data were fitted to the signal equation Si = S0exp(−TE i /T2) to generate T2 maps via the Levenberg-Marquardt nonlinear least squares algorithm using Interactive Data Language (Harris Geospatial Solutions Inc), where Si is the signal at echo time TE i and S0 is the signal at a TE of 0. To minimize the errors due to stimulated echoes, the first echo data were not used in T2 relaxation time estimation. 32
ITK-SNAP software was used for manual cartilage segmentation as previously described.56,59 Briefly, the lateral and medial tibiofemoral compartments were defined using the center of the intercondylar notch for both the femur (lateral femoral condyle [LFC], medial femoral condyle [MFC]) and the tibia (lateral tibial condyle, medial tibial condyle) (Figure 2). Cartilage within each femoral and tibial compartment was further divided into anterior, weightbearing, and posterior regions of interest (ROIs). The weightbearing region was defined by the borders of the anterior and posterior meniscal horns in the sagittal plane. Anterior and posterior regions of the tibial articular cartilage were not used for analysis due to small cartilage volumes in these regions. Before 6-month cartilage segmentation, a manual and affine registration technique was used to register the 6-month image to the preoperative image using 3D Slicer software. 14 The purpose of this registration was to compare similar cartilage ROIs across time.
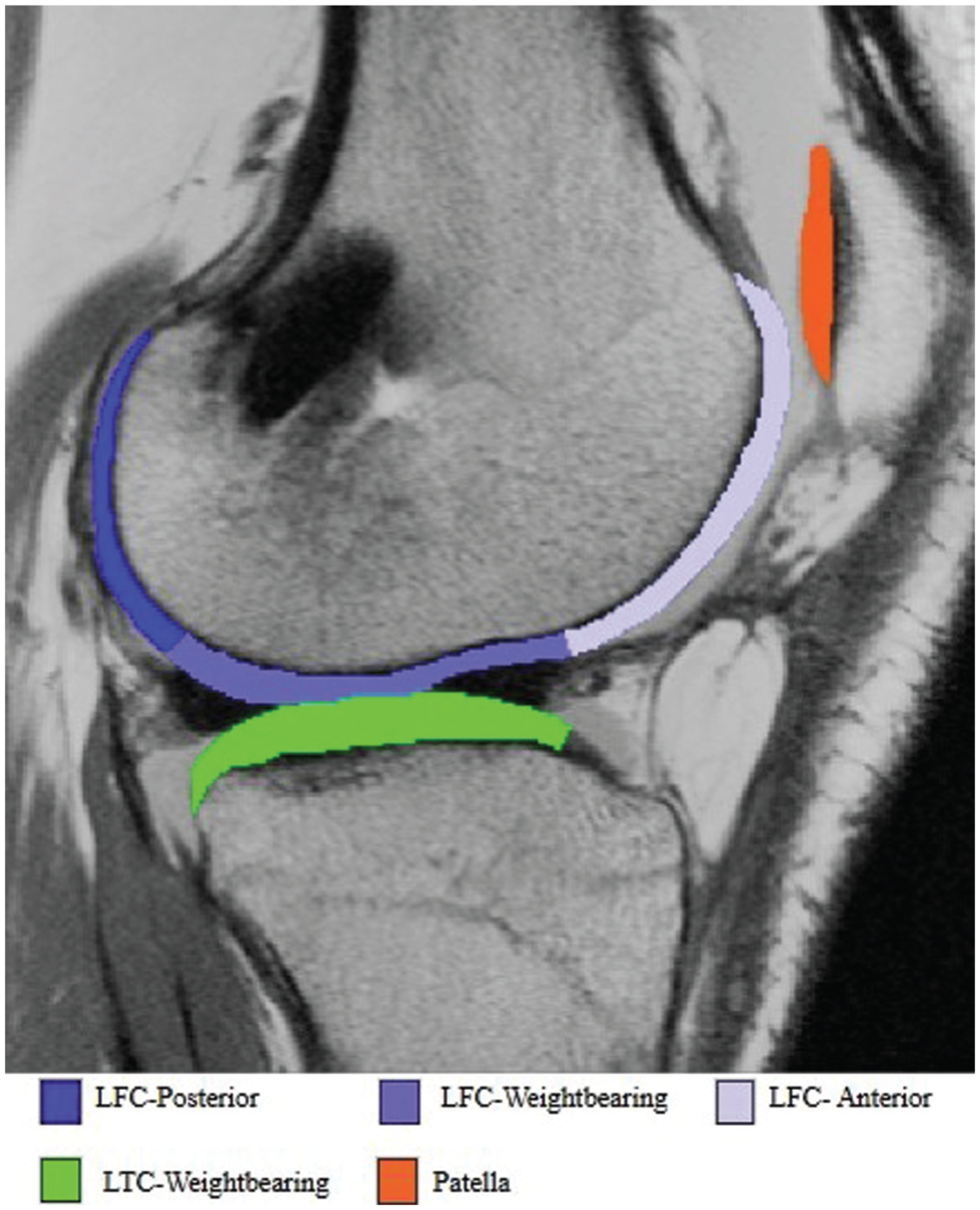
Segmentation of cartilage in the lateral tibiofemoral compartment and patella. Similarly, segmentation of the medial tibiofemoral cartilage was also completed, resulting in 13 segmentation regions created: 6 femoral, 6 tibial, and 1 patellar. The borders of the tibial and femoral segmentations were defined by the borders of the meniscal horns. The anterior and posterior segmentations of the tibial cartilage were not used in our analysis. LFC, lateral femoral condyle; LTC, lateral tibial condyle.
A board-certified and fellowship-trained musculoskeletal radiologist (M.M.) confirmed ROI boundaries and the accuracy of segmentation masks. The mean T2 relaxation time within each ROI was extracted by overlaying cartilage masks on T2 maps (6 femoral, 2 tibial, and 1 patellar). Pixels with T2 relaxation times <10 milliseconds or >90 milliseconds were excluded as outliers due to fitting errors. 57 The variable of interest was the percent change in mean T2 relaxation time from before ACLR (pre-ACLR) to 6 months after ACLR for each ROI (6 months − pre-ACLR/pre-ACLR).
Statistical Analysis
Nominal data are described using counts and proportions. Continuous data are described using means, standard deviations, and 95% confidence intervals. A P value of .05 was set a priori as the threshold for statistical significance. Independent t tests and Fisher exact tests were used to determine if participant and surgical characteristics differed between those with and without an extension deficit at 2 months post-ACLR. Additionally, independent t tests were used to determine if percent change in cartilage T2 relaxation time at 6 months post-ACLR was different between those with and without a knee extension deficit at 2 months. Data were normally distributed, as assessed by histograms. There was homogeneity of variances for T2 relaxation times across all cartilage regions for those with and without an extension deficit, as assessed by the Levene test for equality of variances (all P > .05). Outliers were assessed by inspection of a box plot for values >3.0 box lengths from the edge of the box. If an outlier was detected, sensitivity analyses were conducted with outliers removed. A Bonferroni adjustment was applied to account for multiple comparisons across the 9 cartilage ROIs (a = 0.05/9 = 0.0056).
Results
Participants were a mean age of 18.8 ± 3.9 years, and 63.3% were female. Nearly all participants participated in level 1 cutting and pivoting sports before injury. Graft type included 26.7% quadriceps tendon autograft, 66.7% bone–patellar tendon–bone autograft, and 6.7% hamstring tendon autograft. Concomitant meniscal repair was performed in 56.7% of cases. No significant differences in demographics, surgical characteristics, or patient-reported outcomes were observed between groups based on extension deficit at 2 months post-ACLR. Additional participant characteristics are summarized in Table 1.
Characteristics of participants with and without an extension deficit at 2 months after ACLR
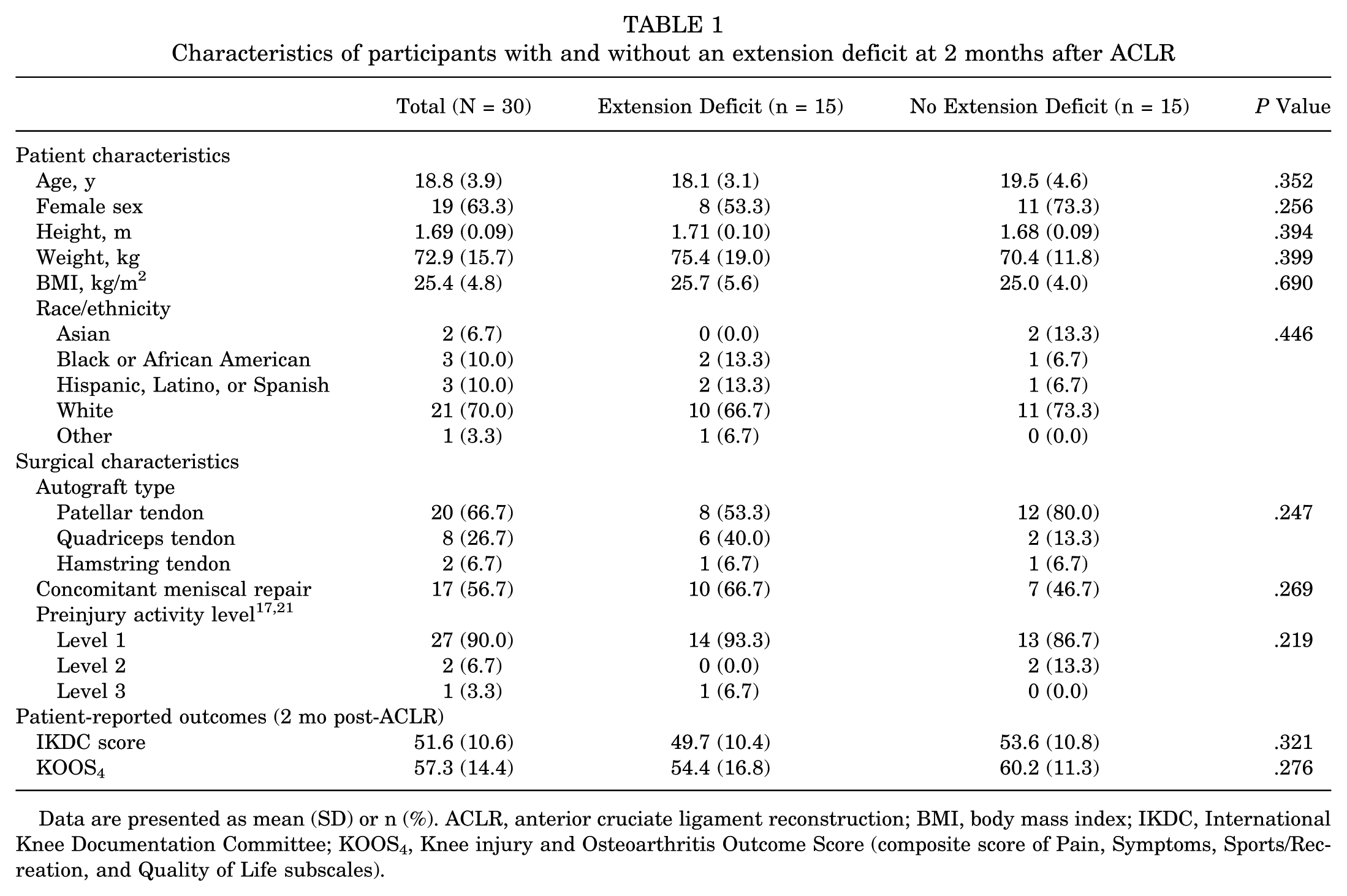
Data are presented as mean (SD) or n (%). ACLR, anterior cruciate ligament reconstruction; BMI, body mass index; IKDC, International Knee Documentation Committee; KOOS4, Knee injury and Osteoarthritis Outcome Score (composite score of Pain, Symptoms, Sports/Recreation, and Quality of Life subscales).
Fifteen of 30 (50.0%) participants had an extension deficit greater than 3° in the injured knee at 2 months after ACLR. The mean interlimb difference in participants with an extension deficit was 6.2°± 2.2° less in the injured knee compared to 0.1°± 3.2° less in those without an extension deficit (P < .001). Of the 15 participants with a 2-month extension deficit, 7 continued to demonstrate an extension deficit greater than 3° at 6 months post-ACLR.
Participants with an extension deficit had significantly greater (worse) percent changes in T2 relaxation time within the anterior cartilage of the MFC (P = .003; extension deficit: 16.20% ± 9.25%; no extension deficit: 5.99% ± 8.22%) and the weightbearing cartilage of the MFC (P = .004; extension deficit: 12.62% ± 4.66%; no extension deficit: 6.48% ± 5.83%), indicating worse cartilage composition at 6 months post-ACLR (Table 2 and Figure 3). Changes in T2 relaxation time did not differ between groups in other cartilage regions (all P > .05) (Table 2). One outlier in posterior LFC T2 relaxation time was identified in the group without an extension deficit. Removal of this outlier did not alter the findings, with no between group differences observed (P = .453; extension deficit: 10.22% ± 8.01%; no extension deficit: 8.02% ± 7.57%).
Percent Change in Mean T2 Relaxation Time From Before ACLR to 6 Months Post-ACLR in Cartilage Regions of Interest a
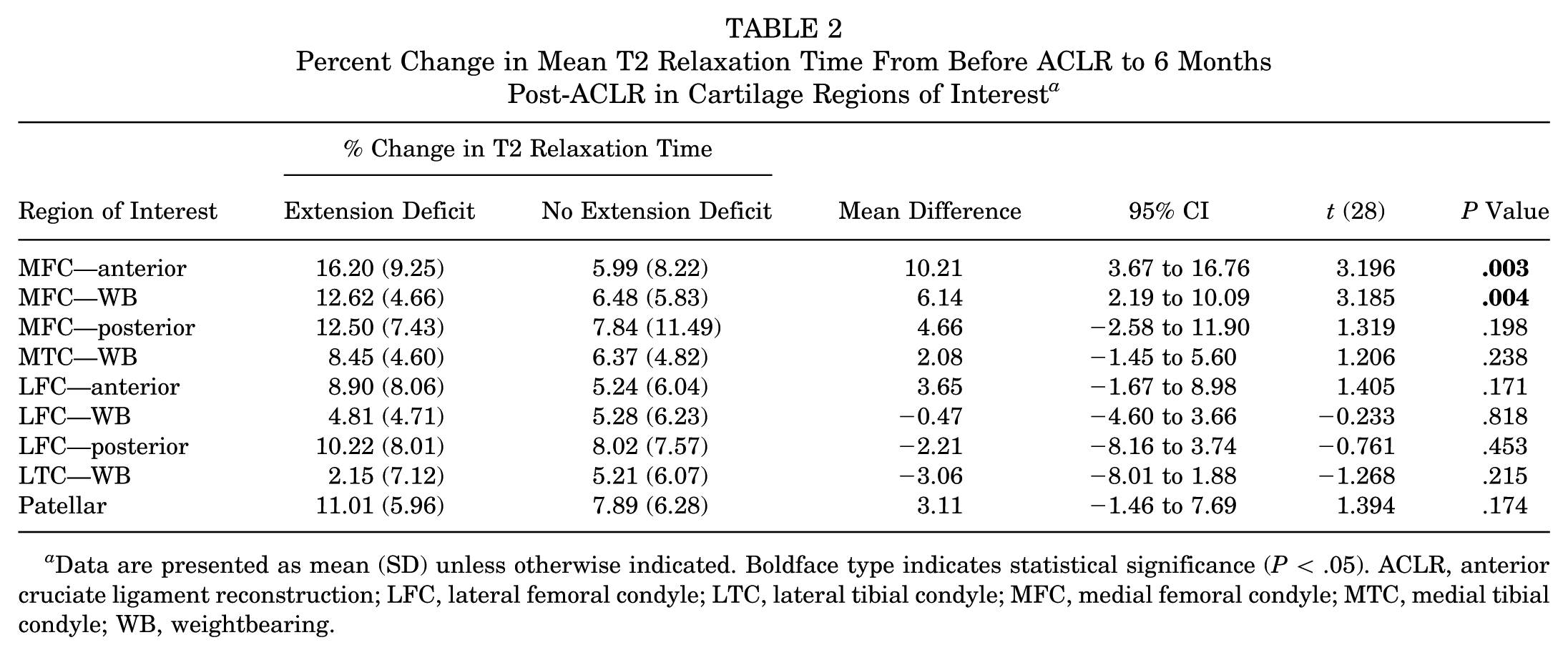
Data are presented as mean (SD) unless otherwise indicated. Boldface type indicates statistical significance (P < .05). ACLR, anterior cruciate ligament reconstruction; LFC, lateral femoral condyle; LTC, lateral tibial condyle; MFC, medial femoral condyle; MTC, medial tibial condyle; WB, weightbearing.
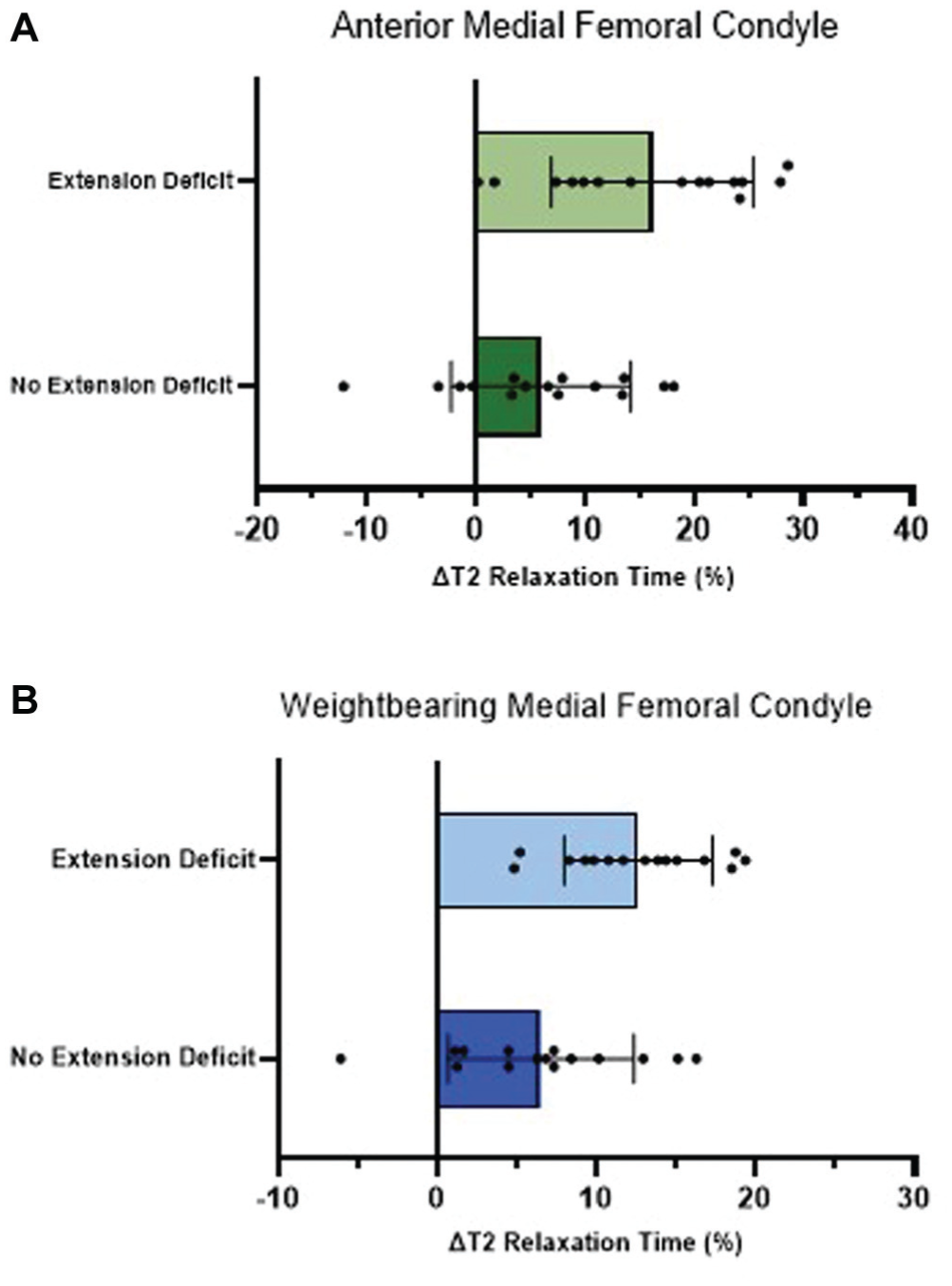
The mean percent change in T2 relaxation time from before anterior cruciate ligament reconstruction (ACLR) to 6 months post-ACLR was greater in participants with an extension deficit (n = 15) compared to those without (n = 15) in the (A) anterior cartilage (P = .003) and (B) weightbearing cartilage (P = .004) of the medial femoral condyle. Error bars represent ±1 standard deviation of the mean of the percent change in T2 relaxation time.
Discussion
The primary aim of this study was to determine whether knee extension ROM at 2 months post-ACLR is associated with tibiofemoral and patellar cartilage composition at 6 months. Our findings indicate that participants with an extension deficit at 2 months exhibited greater increases in T2 relaxation times in the anterior and weightbearing cartilage of the MFC at 6 months. These results suggest early compositional cartilage changes in the medial compartment among individuals with a knee extension impairment that is not resolved by 2 months. This pattern in the medial but not the lateral compartment aligns with prior research indicating that OA in both the general population and ACLR population often initiates medially before progressing to other regions of the knee.3,4,10,27,48 The absence of significant differences in the lateral compartment may reflect this early medial predominance in OA development.
Restoration of full knee extension has long been a foundational goal of ACLR rehabilitation. 2 Achieving full extension is associated with less pain, better functional scores, and improved long-term joint health; conversely, persistent extension loss is linked to inferior subjective and objective outcomes and higher odds of radiographic OA.49,50,52 Reported prevalence of loss of extension varies across studies owing to heterogeneous definitions and measurement techniques. Compared to a recent meta-analysis and meta-regression that similarly defined loss of extension as a ≥3° deficit versus the contralateral limb, our sample had a higher prevalence of extension loss at 50% versus their prediction of 38.5% at 2 months post-ACLR. 47 When extension deficits persist, nonoperative management (terminal extension exercises, patellofemoral mobilization, effusion reduction, pain management, and monitoring for cyclops lesions) is recommended and effective.11,18,39 When nonoperative measures fail, escalation with manipulation under anesthesia, lysis of adhesions, and/or lesion excision may be required.13,25,38
ACLR does not consistently restore native tibiofemoral kinematics. Both in vivo and modeling studies have demonstrated persistent alterations in tibial rotation and anterior tibial translation, particularly when graft placement is nonanatomic.1,16,22,45,60 These deviations can disrupt medial-lateral load distribution and alter tibiofemoral contact forces, mechanical changes that have been implicated in the elevated risk of OA after ACLR.5,22,55,56 Superimposed on these ACLR-related changes, a knee extension deficit may further impair tibiofemoral alignment by limiting terminal extension and disrupting the screw-home mechanism, which involves progressive external tibial rotation during the final approximate 15° to 20° of open-chain extension or femoral internal rotation during closed-chain tasks. 26 This mechanism is essential for normal tibiofemoral contact mechanics. As a result, individuals with extension deficits may experience shift in the location of tibiofemoral contact forces compared to those without such deficits. These altered loading patterns are consistent with our findings of increased T2 relaxation time in the weightbearing MFC cartilage and align with prior studies linking altered cartilage loading with cartilage T2 relaxation changes.42,44,56 These findings suggest that even by 6 months post-ACLR, a knee extension deficit is associated with measurable changes in cartilage composition. It is unknown whether restoring extension loss early in rehabilitation will lead to improved cartilage health, or whether both an extension loss and worse cartilage microstructure underlie other deleterious outcomes.
Beyond tibiofemoral load redistribution, early postoperative gait adaptations also influence patellofemoral joint loading. Many patients exhibit a “stiff-knee” gait early after ACLR, characterized by reduced stance-phase flexion and a diminished knee extensor moment. Because patellofemoral joint reaction force increases with both knee flexion angle and quadriceps demand, this reduced flexion commonly seen after ACLR can lead to underloading of the patellofemoral cartilage during level walking.20,36 Contributing factors in addition to extension deficits likely include pain, effusion, quadriceps inhibition and weakness, and fear of movement, each known to disrupt gait symmetry and knee loading.15,54 Importantly, underloading of the patellofemoral joint and altered gait mechanics at 3 months after ACLR have been associated with subsequent patellofemoral cartilage degeneration over 2 years, aligning with our observation that early extension loss was associated with increased T2 changes in the cartilage of the anterior MFC.44,58 Similar T2 relaxation changes were not observed in patellar cartilage, consistent with findings from Savage et al. 44 Further research is needed to determine whether cartilage thickness moderates susceptibility to T2 changes and eventual OA development, as suggested by Savage et al, 44 or if this relationship is isolated to the patellar cartilage.
This study has several strengths. It used a prospective design with quantitative MRI assessments of cartilage composition at an early postoperative time point, allowing for the detection of subtle changes that may precede radiographic OA. The use of T2 relaxation time mapping provides a sensitive, noninvasive biomarker of cartilage health. However, limitations should be acknowledged. The sample size was relatively small, which may limit generalizability to all individuals who experience ACL injury (and may have resulted in type 2 errors due to decreased power). Our patient population had a high proportion of concomitant meniscal repair, which could alter joint contact forces within the knee.5,9 Standing radiographs to assess joint alignment and analyses of bone bruising using MRI data were not obtained in this study, and differences in mechanical axis (particularly varus) and injury severity (bone bruising) may have influenced our results. Additionally, while we observed significant changes in the medial femoral cartilage, longer follow-up is needed to determine whether these early compositional changes predict long-term structural degeneration or clinical symptoms. Longer follow-up may also be needed to determine if extension deficits are related to degeneration in the lateral femoral and patellar cartilage beyond 6 months post-ACLR.
Conclusion
Knee extension ROM deficits at 2 months post-ACLR are associated with compositional changes in the medial femoral cartilage at 6 months, suggesting that limited extension may contribute to early signs of OA risk. Restoring full knee extension early in ACLR rehabilitation is a modifiable target that may help preserve cartilage health and reduce long-term OA risk. Routine monitoring and individualized interventions to address extension deficits should be prioritized early in the postoperative recovery process.
Footnotes
Submitted November 23, 2025; accepted May 28, 2026.
One or more of the authors has declared the following potential conflicts of interest or sources of funding: E.W. is funded by the National Institutes of Health (U54GM115458, R01AR080346, R15AG085105) and the Arthritis Foundation (Osteoarthritis Clinical Trials Network [OACTN]). M.T. serves on the editorial board for Current Review in Musculoskeletal Medicine; receives research funding from Moximed; provides consulting for NewClip, Moximed, and Vericel; and owns stock in Overture, Pinotage Healthcare, and NeAT Surgical.
Ethical approval was obtained from the University of Nebraska Medical Center's institutional review board (IRB No. 416-17-FB).