
Abstract
Background
The Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) is a federal nutrition assistance program aiming to address food insecurity and improve health. Participation varies across marginalized groups (eg, Black, Hispanic, low-income, rural), likely due to WIC access barriers and satisfaction, limiting WIC's impact on health disparities.
Objective
Assess WIC access and satisfaction across marginalized groups to understand determinants of WIC participation in Missouri, where food insecurity is high (11% overall, 12% Hispanic, 26% Black) and WIC participation low (41%).
Methods
This cross-sectional study used data from the Missouri WIC Experience Survey (April 2022–June 2022). Bivariate and multivariate logistic regression assessed access (eg, clinic wait times, clinic hours, clinic location) and satisfaction (eg, nutrition education, meeting dietary needs, shopping experience) across race/ethnicity, income, and urbanicity.
Results
The sample (n = 2232) consisted of 69% White, 16% Black, and 8% Hispanic WIC-eligible households. Most had monthly incomes of $4000 or less (69%) and 32% lived in rural areas. Black households had 75% higher odds of experiencing barriers compared to White households. Compared to urban households, rural households experienced 30% lower odds of being satisfied overall with WIC, but 75% higher odds of being satisfied with WIC meeting dietary needs. Hispanic households had 85% higher odds than White households of being satisfied with WIC.
Conclusions
Findings offer considerations for addressing WIC access and satisfaction. WIC design and implementation should focus on barriers to access for Black households and improving overall satisfaction with WIC among rural and low-income households.
Plain language title
Describing differences in WIC participation across racial, ethnic, rural, and low-income groups
Plain language summary
The Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) supports families with low household incomes to purchase healthy food. WIC is not always easy to access, and families may not be satisfied with WIC benefits, leading to less participation in the program. Some groups such as Black, Hispanic, lower-income, and rural, may be more likely to experience barriers to WIC access and less satisfaction; however, less is known about these differences. We analyzed a survey of Missouri households who are eligible for WIC to understand their program experiences. Missouri is an important state to study because of the low levels of WIC participation. We asked about WIC access barriers such as clinic wait times, locations, and hours. We asked about satisfaction with using WIC such as finding WIC items in the store, WIC education, and WIC meeting dietary needs. Overall, 2232 people took the survey. Most were White (69%), but many were Black (16%) and Hispanic (8%). About 32% were rural and most (69%) made $4000 or less a month. Black households were more likely to face challenges accessing WIC services than White households. When using WIC, rural households were generally less satisfied than urban households but were more likely to feel like WIC met their dietary needs. Hispanic households were more satisfied with WIC overall, compared to White households. Differences in access and satisfaction with WIC are important to know how to improve WIC and make it better for everyone. If WIC is more accessible and people are satisfied, more people will benefit from WIC. Also, WIC may reduce food insecurity and improve health.
Introduction
The Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) is a federal nutrition assistance program that aims to increase food access for pregnant, postpartum, and breastfeeding people, infants, and children up to age 5 among economically disadvantaged (ie, low socioeconomic status) groups.1,2 Eligible individuals must meet income requirements, ranging from 100% to 185% of the federal poverty guidelines, as set by each state. 1 WIC applicants must live within the state where they become eligible and recertify their eligibility every 6 to 12 months. 3 WIC participants receive financial support to purchase WIC-approved food items, nutrition education, and breastfeeding support. 1 Participation in WIC has been associated with improvements in overall health and increased food security.4–8 Food and nutrition policies, such as WIC, are important for achieving health equity since they increase access to healthy foods and reduce associated health disparities among economically disadvantaged groups. 6
To reduce health disparities and improve food security and health outcomes, WIC needs to be accessible and acceptable to all eligible families, especially those from historically marginalized populations (eg, Black, Hispanic, Rural, low-income). However, WIC participation among eligible families remains low. In 2020, around half of eligible people participated in WIC, with the coverage rates varying across geography (ie, states), race and ethnicity, and participant category (ie, pregnant persons, infants, children).3,9 While coverage rates are higher among Black, Hispanic, and multiracial and ethnic groups compared to White populations, rates are still low (50%–64%) and have been declining. 10
Participation in WIC is often determined by accessibility (how easy or difficult it is to enroll and obtain benefits) and acceptability (how well the program meets participants needs and how easy or difficult it is to use benefits). There are likely multiple mechanisms through which WIC accessibility and acceptability varies across race, ethnicity, urbanicity, and income. One mechanism occurs through administrative burdens. Administrative burdens include learning costs (eg, determining eligibility and requirements for enrollment), compliance costs (eg, spending time and money on documentation and completing forms, scheduling and time off work, transportation and travel to appointments), and psychological costs (eg, stress, frustration, loss of autonomy, and stigma).11–13 Among economically disadvantaged groups, these burdens are often disproportionately experienced by historically marginalized populations (eg, Black, Hispanic, rural, lowest-income), leading to disparities in participation.11,12
When considering accessibility, compliance costs related to clinic location, clinic hours, and clinic wait times may be more common for rural communities that live further away from WIC agencies or for lower income WIC participants who may be more likely to have employment with less flexibility for time off to reload benefits.9,14 Low-income groups may also not know they are eligible, thinking the income requirements are for very low-income groups. 9 Hispanic populations may face additional compliance cost burdens related to immigration status and language barriers.9,11,12 Eligible Black participants may be more likely to experience administrative burdens across safety net programs due to racism and discrimination experienced while managing compliance costs. 11
Numerous barriers to acceptability (ie, satisfaction of using WIC) include among others, aspects of food shopping such as checkout experiences, choices of food options approved by WIC, finding food items in the store, and ease of navigating WIC benefits.15–18 WIC benefit food packages may be less likely to meet cultural preferences for Hispanic WIC participants. 19 Low-income, Black, and Hispanic WIC participants may experience stigma while using WIC benefits, reducing satisfaction, and impeding use of and participation in WIC.12,17,19 Additionally, rural residents may have less access to stores that accept WIC or to the diversity and availability of WIC approved foods.9,20,21 Equitable WIC use through a reduction of barriers (ie, administrative burden) to access benefits and improvement in satisfaction with WIC is essential to maximize WIC's impact on health equity.
As a state-administered Federal program, WIC participation rates vary widely.10,22 Missouri is an important state to assess as it relates to WIC accessibility and acceptability. In 2020, 40.6% of eligible Missourians participated in WIC, which is lower than the national average of 50.2%.1,23 Missouri also experienced the second most severe decline in WIC participation (18.9%) in the U.S. during COVID-19. 14 While most states expanded flexibilities, 9 states including Missouri maintained in-person benefit re-authorization appointment requirements. 24 The in-person benefit re-authorization appointment requirement is likely a major factor in creating compliance burdens for WIC participants. Findings from this study may provide insight into variation in WIC experiences across marginalized groups for other states with similar WIC policies. Beyond WIC administration, Missouri experiences high rates of food insecurity, especially among racial and ethnic groups at risk. In 2020, the food insecurity rate in Missouri (11.4%) was higher than the national average, 25 and Black and Hispanic food insecurity rates in Missouri were even higher than the Missouri average, at 26% and 11.6% respectively. 4
Previous research shows there are differences in WIC coverage rates across racial, ethnic, rural, and low-income groups. 9 Qualitative and theoretical work has explored accessibility and acceptability as potential mechanisms driving these differences in WIC use;11,12,19,26,27 however, little quantitative research has assessed accessibility and acceptability across these groups. Most research on satisfaction looks at WIC participants collectively or by eligibility status (eg, pregnant, postpartum). 28 The National WIC Association has made calls for research priorities that focus on better understanding participant experiences to improve WIC reach and use. 29
We fill this research gap using a survey on WIC access of over 2000 residents of Missouri who use WIC or live in a household with someone who uses WIC. The aims of this paper are to 1) describe the barriers to accessing WIC; 2) describe satisfaction with using WIC; and 3) explore differences in barriers and satisfaction by race, ethnicity, income status, and urbanicity. We hypothesize that barriers to accessing WIC and satisfaction will vary across race, ethnicity, income, and urbanicity.
Materials and Methods
Participants and Recruitment
Data for this study comes from the WIC Experience Survey, administered by Operation Food Search, a Missouri-based hunger-relief organization between April and June 2022. The survey is a cross-sectional survey of Missouri residents who use or have used WIC in the last 3 years, live with someone who currently uses WIC has used WIC in the last 3 years, or is eligible but not participating in WIC. Participants were recruited in 3 ways: 1) the WIC Shopper App, a third-party mobile app used by WIC recipients to manage WIC benefits; 2) partnering nonprofit organizations serving low-income families; and 3) the Missouri WIC Facebook page.
Survey Administration
The survey was designed and administered using Qualtrics, and the median response time was 19 min. As an incentive for participation, survey respondents could enter a raffle for a $25 VISA gift card. Respondents were required to be residents of Missouri and provide zip codes as part of survey data collection. The survey was anonymous which reduced the potential for certain biases, such as social desirability. However, due to the anonymous nature of the survey it was not possible to ensure more than 1 person from a household did not take the survey. As part of the response quality checks, duplicate survey responses (ie, from the same respondent) were flagged and removed. The survey was only offered in English. In total, 2850 participants completed the survey. Of these participants, 2232 completed all demographic and related items on the survey for WIC access and satisfaction—this group constitutes the analytic sample for this study. A non-human subject research determination was obtained for this research from the Washington University in St. Louis Institutional Review Board.
Survey Instrument
Development
The survey was developed using a mix of already validated measures and internally developed measures. Internally developed measures were piloted and revised for clarity and understanding with a group of WIC eligible participants, the staff at a local hunger relief non-profit organization, and the Missouri WIC state office.
Measures
Barriers to WIC access – To assess experience with potential barriers and burdens in accessing WIC, the survey asked participants to respond with ‘Yes,’ ‘No,’ or ‘Not sure’ to “Have any of the following been barriers to you being able to access a WIC clinic?” Enrollment barriers included clinic locations, clinic hours of operation, and clinic wait times. We combined ‘No’ and ‘Not sure’ for the analysis to create a dichotomous outcome (‘Yes,’ and ‘No/Not sure’). These barriers constitute structural aspects of WIC delivery that can be intervened upon to improve access.
Satisfaction with using WIC – Participants responded on a five-point Likert scale (very dissatisfied to very satisfied) regarding satisfaction with WIC nutrition education and WIC breastfeeding education. For the analysis, we combined breastfeeding and nutrition education to create an overall measure of WIC education (satisfied, dissatisfied/neutral). Participants were considered satisfied with WIC education if they responded that they were very or somewhat satisfied with both the breastfeeding education and nutrition education components of WIC, or if they did not respond to breastfeeding education, and indicated satisfaction with nutrition education.
To explore WIC benefit use, the survey asked participants to respond on a five-point Likert scale (strongly disagree to strongly agree) to “agree or disagree with statements such as, “WIC approved items are always in stock,” “WIC approved items are easy to find,” and “Cashiers are knowledgeable about WIC approved items.” For analysis, we dichotomized measures into agree (strongly agree and somewhat agree) and disagree/neutral (neither agree nor disagree, somewhat disagree, and strongly disagree). For meeting dietary needs, the survey asked participants if WIC met their family's cultural and dietary needs, which we dichotomized into yes or a little/no. Participants were also asked how satisfied they were with the food options covered by WIC. Response options included a five-point Likert scale from very satisfied to very dissatisfied. For analysis we dichotomized the measure into satisfied (very satisfied and somewhat satisfied) and dissatisfied/neutral (neutral, somewhat dissatisfied, very dissatisfied).
Demographics – Participants were asked to check all that apply for race and/or ethnicity including White/Caucasian, Black/African American, Hispanic/Latinx, Asian, or other. If they selected “other” they were prompted to specify their race/ethnicity in text. Participants were asked to select their monthly pre-tax income from a set of options ranging from $0–$500 to more than $8000. For this analysis, income categories were collapsed into ($2000 or less, $2001–$4000, more than $4000) based on the distribution of the data. Urbanicity was based on rural-urban commuting area codes (RUCA) calculated from participant zip codes. 30 Participants were identified as urban if they fell under codes 1–3 and rural if they fell under codes 4–10. Participants were asked to select the number of children (people under the age of 18) in a household and the number of adults (people aged 18 and older) including them in a household from a drop-down menu.
Analysis
To accomplish study aims 1 and 2 describing barriers to accessing WIC and satisfaction using WIC, we ran descriptive frequencies for WIC barriers (clinic location, clinic hours, and wait times), WIC satisfaction (WIC education, food options, availability of WIC-approved items, ease of finding WIC-approved items, and cashier knowledgeability of WIC approved items), and demographic variables (race/ethnicity, income, urbanicity, number of children, number of adults). To accomplish study aim 3, we examined the relationship between WIC barrier and satisfaction measures and sociodemographic factors through the use of Chi-square tests. Finally, multivariate logistic regression models examined the associations between race/ethnicity, income, and urbanicity with WIC barriers and WIC satisfaction, controlling for family size (number of adults and number of children).
Results
Descriptive statistics for the analytic sample (n = 2232) are presented in Table 1. Most sample participants were White (69%), 15% were Black, less than 8% were Asian or other racial group, and 8% were Hispanic. Thirty-seven percent of households had a monthly income of $2000 or less, 32% had an income between $2001 and $4000, and 31% had an income greater than $4000. Almost 70% of participants lived in urban areas.
Descriptives for WIC Experience Survey Participants (n = 2232).
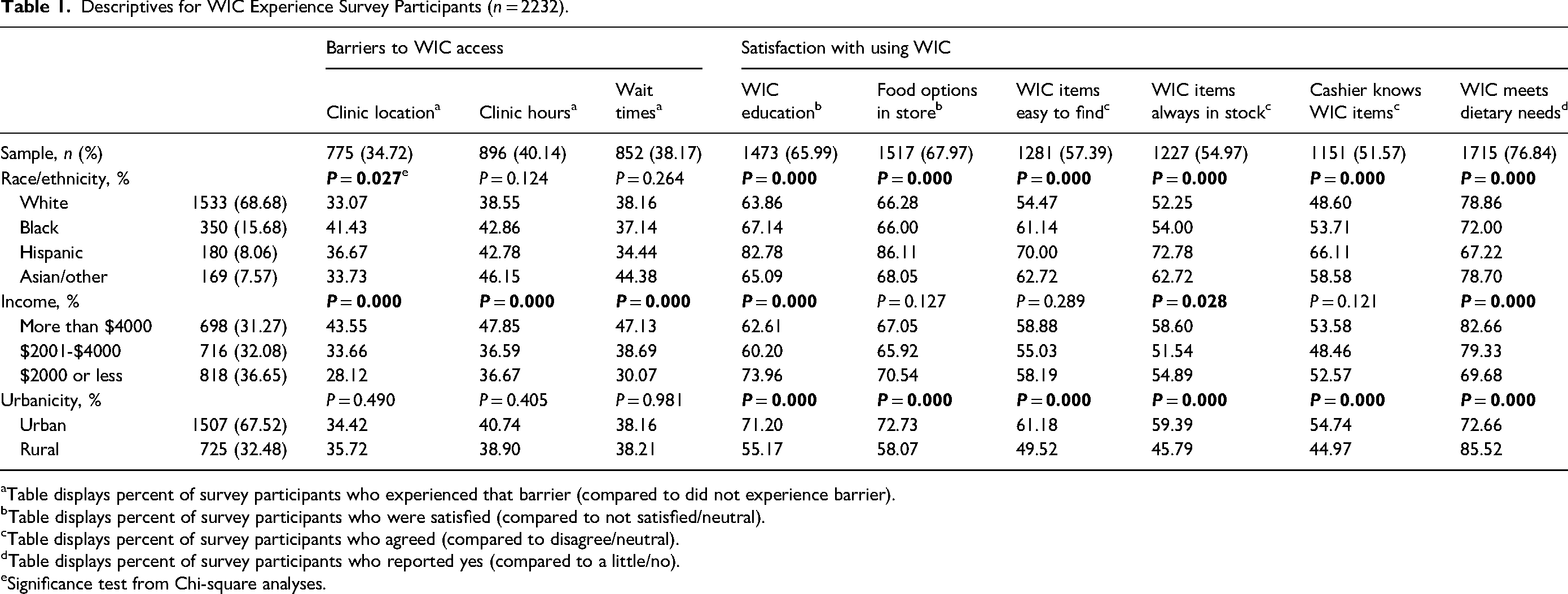
Table displays percent of survey participants who experienced that barrier (compared to did not experience barrier).
Table displays percent of survey participants who were satisfied (compared to not satisfied/neutral).
Table displays percent of survey participants who agreed (compared to disagree/neutral).
Table displays percent of survey participants who reported yes (compared to a little/no).
Significance test from Chi-square analyses.
Overall, most participants were satisfied with WIC meeting dietary needs (77%), food options in the store (68%), and WIC education (66%). Participants were least satisfied with WIC items being easy to find (57%), WIC items always in stock (55%), and the cashier knowing WIC items (52%). Additionally, between 35% and 40% of participants experienced barriers to WIC access with nearly half (40%) experiencing clinic hours as a barrier to access. Thirty-eight percent experienced wait times as a barrier, and 35% reported clinic location as a barrier.
Table 1 shows how the WIC experience differs by race and ethnicity, income, and urbanicity. Over 40% of Black participants and 37% of Hispanic participants reported experiencing a barrier in clinic locations. More than 80% of Hispanic participants were satisfied with WIC education and food options in the store. Moreover, approximately 70% of Hispanic participants agreed that WIC items were easier to find, WIC items were always in stock, and the cashier knew WIC items. Almost 80% of White and Asian participants reported that WIC met their dietary needs.
More than 40% of participants with an income greater than $4000 experienced barriers in clinic location, clinic hours, and wait times. Over 70% of participants with an income of $2000 or less were satisfied with WIC education. However, almost 60% of participants with an income greater than $4000 agreed that WIC items were always in stock, and over 80% of participants with incomes greater than $4000 reported that WIC met their dietary needs.
More than 70% of participants in urban areas were satisfied with WIC education and food options in the store. Approximately 60% of urban participants agreed that WIC items were easy to find, WIC items were always in stock, and the cashier knew WIC items. Yet, 85% of rural participants reported that WIC met dietary needs.
Table 2 shows the results of the adjusted logistic regression models for barriers to WIC access by race and ethnicity, income, and urbanicity. Relative to White participants, Black participants had a 1.75 times higher odds of experiencing barriers in access to clinic locations (p < .001) and a 1.32 times higher odds of experiencing barriers in clinic hours (p < .05). Participants with incomes of $2001 to $4000 had 0.66 times lower odds of experiencing barriers in access to clinic locations (p < .001), a 0.64 times lower odds of experiencing barriers in clinic hours (p < .001), and a 0.72 times lower odds of experiencing barriers in wait times (p < .01), compared to participants with incomes of more than $4000. Participants with incomes of $2000 or less had 0.58 times lower odds of experiencing barriers in clinic locations (p < .001), a 0.69 times lower odds of experiencing barriers in clinic hours (p < .001), and a 0.55 times lower odds of experiencing barriers in wait times (p < .001), than participants with incomes of more than $4000.
Logistic Regression Models for WIC Barriers to Access and Satisfaction with WIC use (n = 2232).
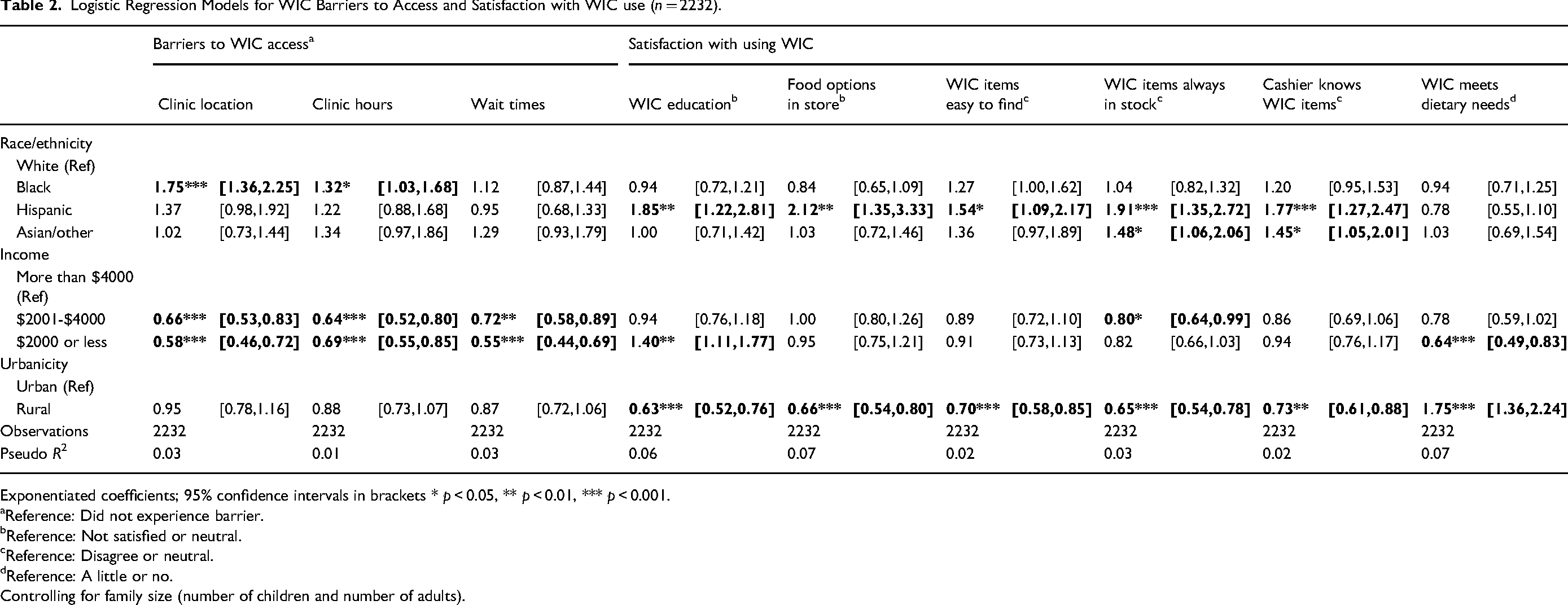
Exponentiated coefficients; 95% confidence intervals in brackets * p < 0.05, ** p < 0.01, *** p < 0.001.
Reference: Did not experience barrier.
Reference: Not satisfied or neutral.
Reference: Disagree or neutral.
Reference: A little or no.
Controlling for family size (number of children and number of adults).
Table 2 also shows the results of the logistic regression models for satisfaction with using WIC across ethnicity and race, income, and urbanicity. Relative to White participants, Hispanic participants had 1.85 times higher odds of being satisfied with WIC education (p < .01) and a 1.12 times higher odds of being satisfied with food options in the store (p < .01), than White participants. Also, Hispanic participants had a 1.54 times higher odds of agreeing that WIC items were easy to find (p < .05), a 1.91 times higher odds of agreeing that WIC items were always in stock (p < .001), and a 1.77 times higher odds of agreeing that the cashier knew WIC items (p < .001), compared to White participants. Relatedly, relative to White participants, Asian participants had 1.48 times higher odds of agreeing that WIC items were always in stock (p < .05) and a 1.45 times higher odds of agreeing that the cashier knew WIC items (p < .05), compared to White participants. Rural participants had a 0.63 times lower odds of being satisfied with WIC education (p < .001) and a 0.66 times lower odds of being satisfied with food options in the store (p < .001), compared to urban residing participants. Additionally, relative to urban participants, rural participants had a 0.70 times lower odds of agreeing that WIC items were easy to find (p < .001), a 0.65 times lower odds of agreeing that WIC items were always in stock (p < .001), and a 0.73 times lower odds of agreeing that the cashier knew WIC items (p < .01). Finally, rural participants had a 1.75 times higher odds of reporting that WIC met dietary needs (p < .001), compared to urban residing participants.
Discussion
We surveyed over 2000 residents of Missouri who use WIC or live in a household with someone who uses WIC to contribute quantitative data on WIC accessibility and acceptability and to examine differences across racial, ethnic, rural, and low-income groups. While WIC programs have some variance across states, using data from Missouri WIC participants provides insight into accessibility and acceptability for states with similar WIC policy profiles (eg, requiring in-person reauthorization). We found participants were generally satisfied with WIC. More than half of participants reported satisfaction across all satisfaction measures in this study. Participants reported the most satisfaction with WIC meeting dietary needs (77%) and with the food options in the store (68%) and were least satisfied with cashiers knowing WIC items (52%) and with WIC items always being in stock (55%). Differences in satisfaction were experienced across race and ethnicity, income groups, and urbanicity.
Barriers to Access
While participants had reasonably high levels of satisfaction with WIC, we also document disparities in the barriers to accessing the program. We found that 35% to 40% of participants reported experiencing barriers to access associated with clinic location, clinic hours, and wait times and that these barriers were experienced differently across race and ethnicity and income groups.
Notably, our study suggests that Black participants were more likely to face barriers than White participants due to WIC office locations and clinic hours. Black participants reporting a higher likelihood of experiencing these barriers may be due to several reasons, such as the number of clinics in predominantly Black neighborhoods, access to transportation, and available time.11,12 Some research suggests administrative burdens related to access, such as time for appointments and applying or recertifying, may be racialized. For example, Black individuals may have higher utilization of means-tested programs that cumulatively require more time and thus act as a greater barrier. 11 Reducing these barriers is important since only 50% of WIC-eligible Black individuals receive WIC and rates of food insecurity and chronic disease are higher among Black individuals.4,9,25 Recent policy changes related to using digital tools for remote certification have shown promise in increasing WIC participation and may be beneficial for reducing barriers to WIC access among Black individuals in Missouri.2,23
Income also played a significant role, with lower-income earners less likely to report clinic location, clinic hours, and wait times as barriers. The results suggest WIC may be reaching some of the most financially at-risk groups, such as those living in poverty, who could benefit most from WIC participation. Limited research exists to explain these findings. One study found some WIC-eligible people may not participate because they believe their income is too high or note they do not have the available time. 31 It may also be the case they receive support from other programs, families, or friends. 31 It is also possible that WIC clinics are located in predominantly low-income neighborhoods, facilitating access to WIC clinics and reducing time and transportation burdens associated with WIC appointments.
Satisfaction with Using WIC
Overall, participants were satisfied with using WIC. However, some areas related to WIC use such as the cashier knowing WIC items, WIC items always being in stock, and WIC items being easy to find, could be improved. We found differences in satisfaction by race and ethnicity, income, and urbanicity, suggesting differences in how WIC is experienced across these groups. In particular, Hispanic participants were more likely to be satisfied with WIC than White WIC participants, except for satisfaction with WIC meeting dietary needs. Other research has found mixed experiences of satisfaction using WIC, specifically with WIC education and cultural acceptability of WIC-approved foods among Hispanic groups by primary language spoken.26,27,32 Language spoken may be an important factor related to satisfaction and speaks to the heterogeneity within ethnic groups. We did not collect information about primary language and unfortunately cannot explore this aspect of our findings. However, our findings of high satisfaction among Hispanic participants indicate WIC may be particularly useful for Hispanic WIC participants.
We also found differences in WIC satisfaction by income. Compared to participants in the highest income group (more than $4000), the lowest income group ($2000 or less) was more satisfied with WIC education but less satisfied with WIC meeting dietary needs. These results are important since nutrition and breastfeeding education may improve dietary behavior and increase breastfeeding, and the lowest income groups are at an increased risk of poor nutrition and associated chronic diseases.8,33 Policy changes related to the WIC food package such as increasing the cash value benefit for fruits and vegetables, increasing size flexibility across all food categories, and substitution flexibility for dairy products may improve satisfaction with WIC meeting dietary needs among lowest income groups.2,5 In general, more research is needed to better understand why the lowest income groups receiving WIC are less satisfied with WIC meeting dietary needs.
Looking at urbanicity, participants in rural areas were less satisfied than participants living in urban areas across all satisfaction measures with 1 exception – rural participants were more likely to report satisfaction with WIC meeting dietary needs than urban participants. 3 Some of these differences may be due to distance to food retailers, which tend to be farther in rural areas. Additionally, rural participants may be able to purchase more fruits and vegetables using the cash value benefit due to lower food costs in rural areas. 3
Limitations
There are a few important limitations to report for this study. First, this is a cross-sectional study that cannot speak to potential causes of differences in WIC access and use across race and ethnicity, income, and urbanicity. Additionally, the survey used RUCA codes to capture urbanicity. This measure may not accurately represent who identifies as a rural or urban resident. This is a sample of Missouri residents, and findings may not be broadly generalizable beyond Missouri, though findings may be informative for other states with similar WIC policies. Additionally, survey participants may differ from those who opted not to take the survey, introducing selection bias, and the sample may not be representative of all Missouri WIC participants, introducing sample bias. According to the USDA, roughly 60% of WIC-eligible participants in Missouri are White; however, roughly 70% of our sample is White, which suggests that our sample is not entirely representative of the population of WIC-eligible persons in Missouri. 34 While this study uses a convenience sample, recruiting participants in 3 ways potentially increased reach for a wide range of WIC-eligible respondents. Further, the survey and analysis did not distinguish or account for people having different benefit packages based on breastfeeding or languages spoken. Due to the sample size, we were unable to look at intersectionality across race, ethnicity, urbanicity, and income.
Policy and Program Implications
The findings in this study suggest certain policies and programs may be important for increasing participation among marginalized groups within the WIC eligible population. WIC policies which simplify the enrollment and recertification process, provide flexible scheduling, and offer digital tools and remote certification may be useful in reducing compliance cost burdens for Black participants.3,9,23 Specifically, these findings provide support for states like Missouri, which maintain in-person enrollment and re-authorization, to adopt policies offering telephone and videoconference appointments. Given our findings that Hispanic and lowest income participants were less satisfied with WIC meeting dietary needs, WIC should focus on implementing policies and programs that allow for flexibilities in food package substitutions related to sizes and forms of food items.2,9 These policies can support cultural preferences, dietary needs, and more autonomy around what participants spend WIC benefits on, which may increase satisfaction with WIC and likelihood of continuing participation in WIC. Our study indicates rural residents in Missouri were less satisfied with the WIC shopping experience. WIC policies that offer online shopping options, ensure access to grocery stores accepting WIC, and use technology such as apps to help participants identify WIC eligible food items may be useful. 9 Many of these policies and programs are being tested and implemented across states. Ongoing research should continue to assess how these policies and programs influence accessibility, acceptability, and ultimately participation for marginalized groups among WIC eligible families.
Conclusion
Our study has several strengths. First, our study uses a large sample of residents from Missouri, a state with limited WIC reach and high rates of food insecurity. Additionally, we were able to look at differences in both WIC access and satisfaction across race and ethnicity, socioeconomic status, and urbanicity. While additional research is necessary to further understand relationships between racial/ethnic, income, and place-based disparities in WIC barriers and satisfaction, the current study identifies disparities in accessing and using WIC. Future research should explore why these disparities exist and ways to intervene.
Footnotes
Author Contributions
Contributed to conceptualization and design S.R., J.J., D.F., A.G.; Contributed to acquisition, analysis, or interpretation A.G., D.F., S.R., J.J.; Drafted the manuscript A.G., T.F, L.M, N.W; Critically revised manuscript A.G., D.F., T.F., S.R., J.J., N.W.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Data Availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
A non-human subject research determination was obtained for this research from the Washington University in St. Louis Institutional Review Board. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Helsinki Declaration.
Funding
This work was supported by the National Heart, Lung, and Blood Institute (NHLBI) Grant [T32 HL130357, 2024] and Operation Food Search and Missouri Foundation for Health. The National Heart, Lung, and Blood Institute (NHLBI) Grant, Operation Food Search, (grant number T32 HL130357).
Correction (August 2025):
Article updated online to add the missing information at the two Blinded places(one in the Materials and Methods section and the other in the Ethical Approval section) in the article.