
Abstract
Background
Vitamin A (VA) deficiency affects approximately 15% of preschool-aged children in the Philippines (serum retinol <0.7 μmol/L). Data on school-aged children are lacking.
Objective
To characterize intake of VA-rich foods and VA status among school-aged children in 3 areas of the Philippines at high risk of undernutrition.
Methods
We conducted a cross-sectional study, randomly selecting n = 520 children from primary schools in 3 high-risk provinces. We collected data on household characteristics, past-week food intake, and children's weights and heights. Venous blood samples were drawn and analyzed for plasma retinol, C-reactive protein, and α1-acid glycoprotein.
Results
Most children (96.7%) had consumed preformed VA-rich foods at least once in the prior week, mainly eggs and fortified foods, with a median consumption frequency of 7 times [p25, p75: 4, 12]. While 93.7% had consumed proVA-rich foods—mainly dark green leafy vegetables—the frequency was lower (5 times [2, 9]). Approximately one-quarter took multinutrient supplements (median 600 μg retinol equivalents [400, 1185]). The mean (± SD) plasma retinol concentration was 0.95 ± 0.23 μmol/L. The prevalence of VA deficiency (retinol <0.70 μmol/L) was 13.6% (4.9% adjusted for inflammation), and 59.0% (52.0% adjusted for inflammation) had marginal status (0.70-1.05 μmol/L).
Conclusions
The VA status of school-aged children in high-risk areas was similar to that of preschool-aged children nationally. Despite adjusting for inflammation, most children were classified as having marginal VA status that could be improved by increasing intake of the available preformed and proVA-rich foods in the study area.
Plain language title
Vitamin A intakes and status of school-aged children in high-risk areas of the Philippines
Vitamin A (VA) deficiency is a nutritional concern in the Philippines, affecting about 15% of young children nationally. However, there has been little research on VA deficiency among school-aged children. This age group may be at particular risk as they are not targeted with interventions like high-dose VA supplements. Our study focused on school-aged children in 3 areas of the country known for high rates of undernutrition. We examined their intake of VA-rich foods and measured their VA status. We found that ∼14% of schoolchildren were affected by VA deficiency, similar to the prevalence found among younger children. Additionally, a large proportion of children with marginal VA levels could benefit from increased intake of the VA-rich foods available in this setting. For example, while some children were consuming eggs and milk, the frequency of consumption was low. Our findings highlight the importance of ensuring that children have regular access to VA-rich foods, particularly in areas where undernutrition is prevalent. Incorporating more VA-rich foods into school-based feeding programs could be a crucial step in addressing this nutritional gap and improving the health of school-aged children in the Philippines.
Introduction
Vitamin A deficiency (VAD) has been a long-standing nutritional concern in the Philippines. The country has successfully reduced deficiency-related mortality and virtually eliminated nutritional blindness through interventions like high-dose vitamin A (VA) supplementation, targeted to children 6 to 59 months of age. Since the introduction of the Philippine Food Fortification Act of 2000 (Republic Act No. 8976), preformed VA-fortified foods have also become widely available. This has been achieved through the mandatory fortification of cooking oil and wheat flour, and the voluntary fortification of other processed foods under the Department of Health's Sangkap Pinoy Seal Program. Data from the Philippine National Nutrition Surveys suggest that these interventions have led to substantial reductions in the prevalence of deficiency among young children over the past 15 years, with estimates of VAD decreasing from 40% in 2003 to 15.5% by 2019.1,2
However, despite these achievements, there are disparities in VA status, particularly at the provincial level, between rural versus urban populations, and across different wealth quintiles. 2 For instance, recent provincial-level data from the National Nutrition Survey indicate a wide range of VAD prevalence, from 1% to 40% depending on the province. Additionally, urban areas show a lower prevalence of VAD (13.6%) compared to rural areas (16.9%), and children from the lowest wealth quintile are disproportionately affected (22.4%) compared to those from the highest wealth quintile (5.5%). As inflammation biomarkers are not currently measured in national surveys, the extent to which these prevalence estimates are influenced by inflammation is unknown.
School-aged children, a group not specifically targeted by current VA interventions, remain largely understudied. Although dietary surveys suggest that up to 65% of children in this age group may have inadequate VA intakes, there is a lack of comprehensive data on status, particularly regarding the impact of inflammation on these estimates. This gap is crucial because school-aged children do not benefit from high-dose supplements and rely on dietary sources, which may not be consistently available or adequately consumed.
This study aimed to address these gaps by characterizing the intake of VA-rich foods and the VA status of school-aged children in 3 high-risk areas of the Philippines. By focusing on these areas with historically high levels of undernutrition, we sought to provide information that can inform future nutritional interventions and policies targeted at this vulnerable age group.
Methods
Study Design and Site Selection
This study was carried out to guide the selection of a research site for a randomized controlled trial of Golden Rice, which has been designed as a VAD control intervention. Golden Rice has been genetically engineered to express β-carotene in the grain. The trial will enroll up to 1000 children in a school-based feeding intervention. It targets schoolchildren as this age group does not regularly receive other VA interventions. We first conducted a scoping exercise using extant data to identify regions and provinces likely at risk of VAD based on proxy indicators (eg, food insecurity, dietary inadequacy, anemia, and stunting) and where rice production and consumption would facilitate the eventual deployment of Golden Rice. We excluded areas with existing ordinances against genetically modified organisms or promoting organic agriculture, as well as areas where infrastructure or security concerns would make a trial infeasible. Within selected provinces, we selected municipalities with lower socioeconomic status based on a fourth, fifth, or sixth class government designation 3 and school enrollment with more than 1000 kindergarten through grade 3 students. Input from local government unit officials and a site visit to assess the receptiveness of the environment and feasibility (ie, infrastructure, human resources) guided the final site selection: 2 municipalities in the Province of Antique (Region VI), 1 municipality in the Province of Northern Samar (Region VIII), and 1 municipality in the Province of Sorsogon (Region V).
Sample Size and Power Calculations
Our primary aim was to characterize VA status. Based on available data from the Philippine Expanded National Nutrition Survey, we anticipated a prevalence of ∼25%. Assuming an α = 0.05 and a desired precision of ±5%, this required a sample size of 288 children. We increased this figure by 25%, to 360, to account for refusals or other loss-to-follow-up. Dividing the sample between the 2 sites, we would have ∼88% power to detect a 0.1 μmol/L difference in mean serum retinol between sites, assuming an SD = 0.3 μmol/L and α = .05. This would constitute a meaningful difference in status to drive site selection for the trial. We subsequently added a third site for a total sample size of 520 children, giving us ∼80% power to detect a 10-percentage point difference at 1 of the sites.
Participant Recruitment
Public primary or elementary schools with a minimum of 20 students were considered eligible for selection. Private schools, those with low enrollment or facing potential closure, or those identified as hard-to-reach or as serving primarily indigenous communities, were ineligible. (Golden Rice is not intended for deployment in the latter due to legal safeguards protecting heirloom rice varieties.) We purposively selected from among eligible schools based on school health data (stunting, thinness) provided by the Department of Education. We conducted multiple Parent-Teacher Association meetings in eligible schools to describe the problem of VAD and the planned study. A recruitment script was read to parents or guardians by the research team. Parents with children enrolled in kindergarten through grade 3 of eligible schools who were interested in participating were requested to provide their name and contact details, as well as their child's name, date of birth, sex, and grade level. This listing constituted our sampling frame. We used interval sampling to randomly select children from this listing.
Data Collection
We collected data in Antique and Northern Samar from October to November 2022 and in Sorsogon from November to December 2023. A team of trained data collectors first visited households to describe the study to parents or guardians and to obtain consent and permission for their child's participation. We obtained verbal assent from the child in the presence of their parent or guardian. For consenting households, we administered a questionnaire to capture information on the type of housing, household demographics, and asset ownership. We assessed food security using the Household Food Insecurity Access Scale. 4 We then asked about the number of times each of a list of 7 categories of VA- (milk, organ meat, eggs, fortified foods) or proVA-rich (dark green leafy vegetables, yellow or orange vegetables, orange fruits) foods and supplements were consumed by the child in the prior 7 days and then any illnesses the child experienced during that same period. Nutrient content of supplements was sourced from packaging.
Within 1 to 2 weeks of the household visit, a team visited the child's school. We measured the child's weight on a Seca 874 digital scale and height using a Seca 217 portable stadiometer as per standard protocols. 5 The certified medical technologist then collected a 5-mL venous blood sample into an EDTA vacutainer using antecubital venipuncture in dim light conditions. Blood remaining in the tubing was used to measure hemoglobin concentration using a portable HemoCue Hb 301 photometer (HemoCue). We referred children with a hemoglobin concentration of <90 g/L for treatment at a local clinic. Blood samples in vacutainers were stored on ice for transport.
Laboratory Analysis
At the project laboratory, whole blood samples were centrifuged at 3000 rpm for 10 min to separate plasma and then aliquots were stored at −20 °C. At the close of data collection, plasma aliquots were shipped on dry ice to the Department of Science and Technology-Food and Nutrition Research Institute (DOST-FNRI) in Manila. At DOST-FNRI, we measured plasma retinol using high-performance liquid chromatography. We measured C-reactive protein (CRP) and α1-acid glycoprotein (AGP) by immunoturbidimetric assay on a COBAS Integra 400 plus clinical chemistry analyzer (Roche Diagnostics).
Data Analysis
To characterize nutritional status, we first calculated body mass index (BMI) by dividing the child's weight (kg) by his or her height squared (m2). We used the World Health Organization Stata macro 6 to derive anthropometric indices using sex-specific reference data for children aged 5 to 19 years7,8 and classified children as stunted based on a height-for-age Z (HAZ) <−2. They were classified as thin, at risk of thinness, normal, or overweight/obese based on BMI-for-age Z (BAZ) <−2, −2 to −1, −1 to 1, >1 Z, respectively. We calculated anemia prevalence as the proportion of children with hemoglobin <11.5 g/dL. Inflammation was defined based on CRP >5 mg/L or AGP >1 g/L. For plasma retinol, we used linear regression to estimate an inflammation-adjusted plasma retinol concentration based on methods published by Larson et al, 9 including both CRP and AGP in the regression equation. We calculated the prevalence of VAD and marginal VA status for both unadjusted and adjusted plasma retinol using cutoffs of <0.70 and 0.70 to 1.05 μmol/L, respectively. Retinol concentrations ranging from 0.70 to 1.05 μmol/L are indicative of risk for VA deficiency; status in this range can be improved through the consumption of VA-rich foods.10,11
Ethical Considerations
Ethical oversight for this study in the Philippines was carried out by the Single Joint Ethics Review Board, the Eastern Visayas Health Research and Development Consortium, and the St. Cabrini Medical Center – Asian Eye Institute Ethics Review Committee. The Institutional Review Board of the Johns Hopkins Bloomberg School of Public Health also approved this protocol. We obtained written consent from parents or guardians and oral assent from children.
Results
We selected a total of 32 schools across the 3 provinces, from which we randomly selected 540 children. Of these, 520 parents (96%) consented to their child's participation and provided data on household characteristics and their child's diet and morbidity. During the school visits, we obtained assent from 482 children (89%) and collected venous blood samples from 471 children (87%).
Household characteristics: The mean ± SD household size was 5.8 ± 2.1 people (Table 1), with most families owning their own homes (84.4%) and close to one-quarter (22.9%) owning farmland. Most households had access to a protected source of drinking water (only 5.4% unprotected). Asset ownership ranged from 21.9% for a bicycle to mobile phone ownership by 89.2% of households. Moderate and severe food insecurity were prevalent, at 39.1% and 25.6%, respectively. Almost half of the parents were married (49.9%) and most mothers had received at least some secondary education or greater (>50%).
Characteristics of Selected Households in Antique, Northern Samar, and Sorsogon Provinces (n = 520).a
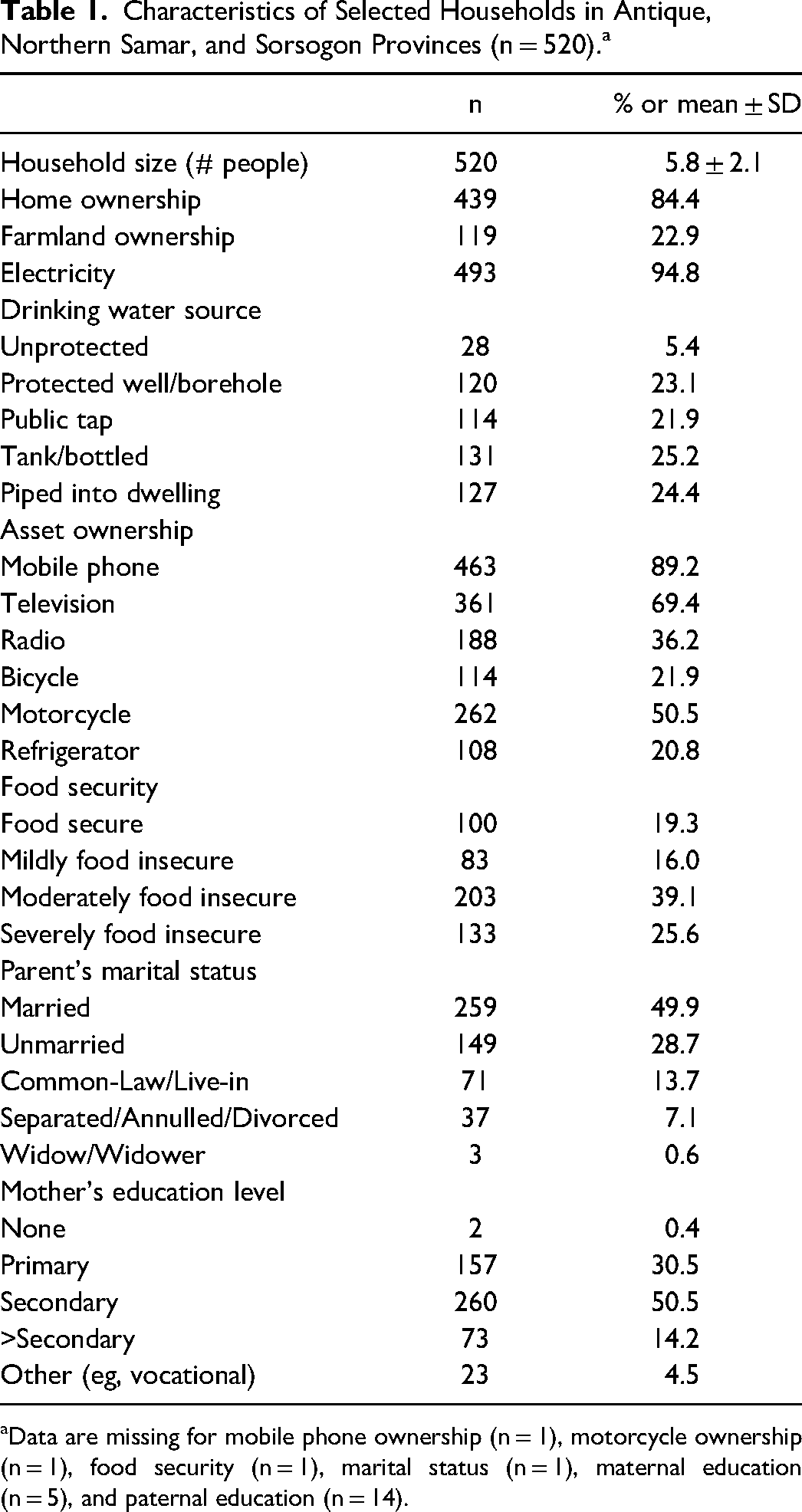
Data are missing for mobile phone ownership (n = 1), motorcycle ownership (n = 1), food security (n = 1), marital status (n = 1), maternal education (n = 5), and paternal education (n = 14).
Child characteristics: Children had a mean age of 7.2 ± 1.2 years and 48.3% of enrolled children were girls (Table 2). The most prevalent sign or symptom of illness in the past week was a cough or cold, reported for 62.9% of children. The mean ± SD of HAZ score was −1.6 ± 1.0, with 37% of children classified as stunted. Based on BAZ scores, 11.2% of children were classified as thin. A further 38.0% of children were classified as at-risk for thinness, 46.6% were classified as normal, and 4.2% were classified as overweight or obese.
Characteristics of Selected Children in Antique, Northern Samar, and Sorsogon Provinces (n = 520).a
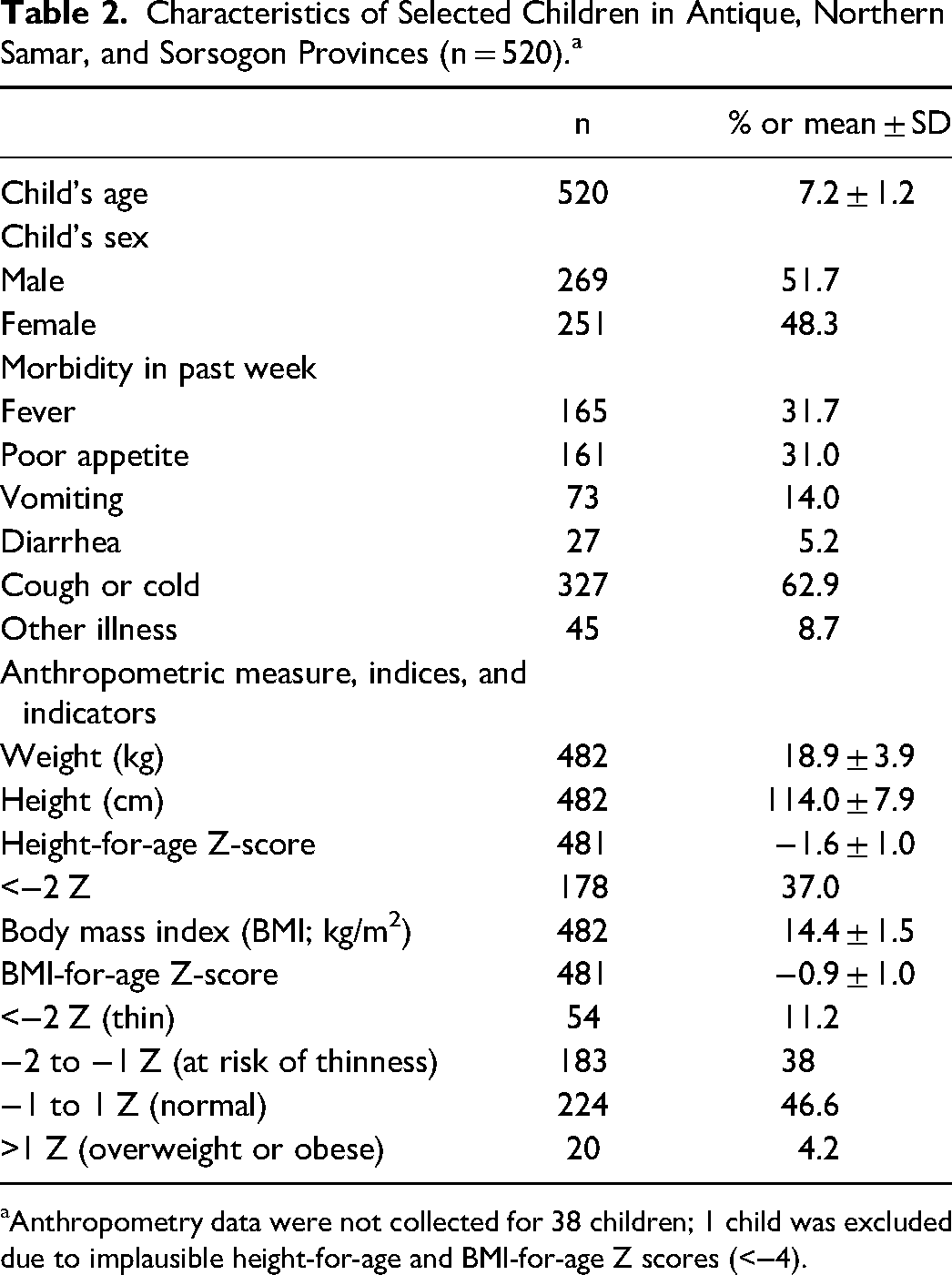
Anthropometry data were not collected for 38 children; 1 child was excluded due to implausible height-for-age and BMI-for-age Z scores (<−4).
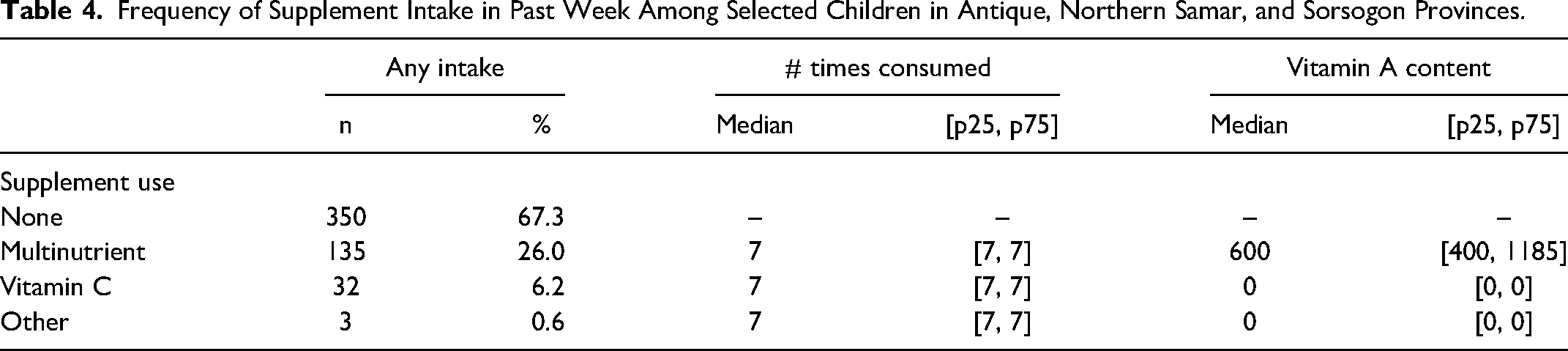
Diet and supplement intake: As shown in Table 3, most children had consumed food containing preformed VA at least 1 time in the prior week. The median frequency of consumption was 7 times [25th percentile, 75th percentile: 4, 12]. Eggs were the most common source of preformed VA. They were consumed at least 1 time in the past week by 93.2% of children, with a median frequency of consumption of 3 times [2, 5]. Fortified foods were also consumed at least once in the past week by 69.6% of children, although the median intake was only 1 time [0, 1]. Consumption of proVA carotenoid sources was lower. Although 93.7% had consumed proVA-rich foods at least once in the past week, the median frequency was 5 times [2, 9]. These were most commonly dark green leafy vegetables, consumed at least once by 82.1% of children (median = 3 times [1, 5]). About one-third of children had consumed supplements in the past week (Table 4), with a median frequency of 7 times [7, 7]. Most of the reported brands contained multiple vitamins and minerals. The median VA content of multinutrient supplements was 600 μg retinol equivalents [400 μg, 1185 μg].
Frequency of Vitamin A-Rich Food Intake in Past Week Among Selected Children in Antique, Northern Samar, and Sorsogon Provinces.a
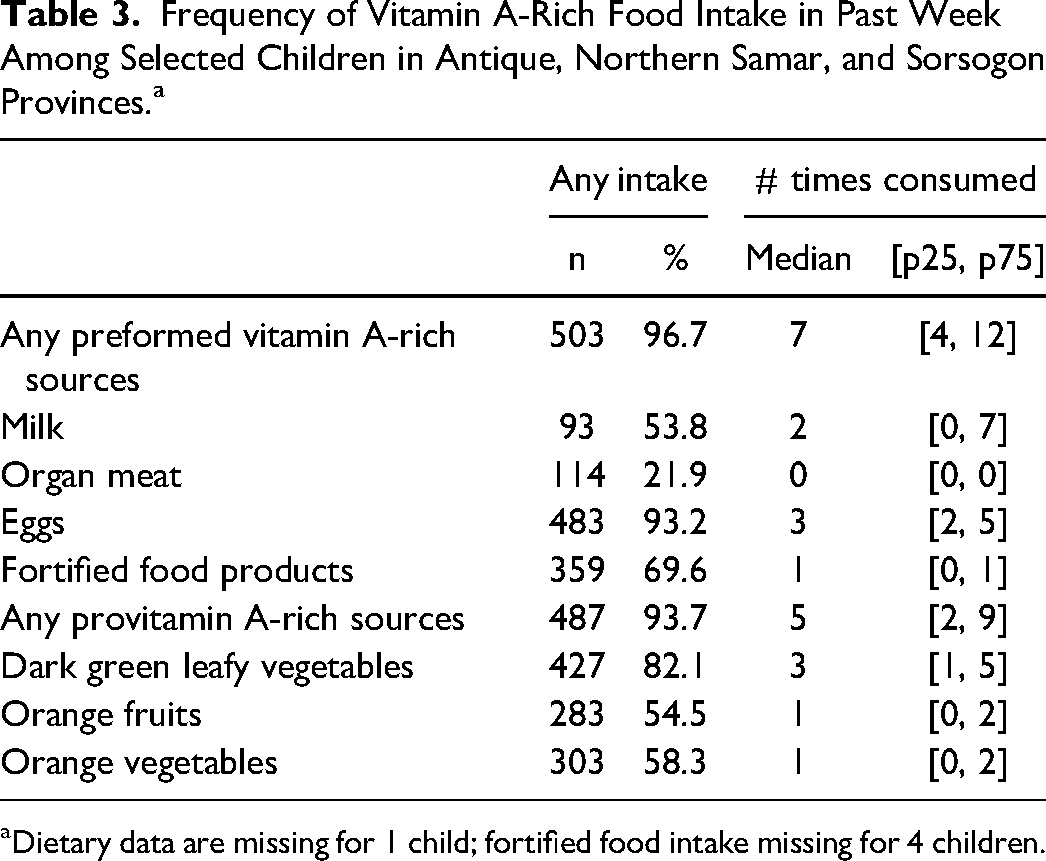
Dietary data are missing for 1 child; fortified food intake missing for 4 children.
Frequency of Supplement Intake in Past Week Among Selected Children in Antique, Northern Samar, and Sorsogon Provinces.
VA and hemoglobin status: The mean plasma retinol concentration was 0.95 ± 0.23 μmol/L, with 13.6% of children classified as deficient and 59.0% with plasma retinol concentration ranging from 0.70 to 1.05 μmol/L, indicating marginal VA status (Table 5). The prevalence of elevated CRP was 10.4% and 20.8% had elevated AGP. After adjustment for inflammation, the prevalence of VAD was 4.9% and 56.9% of children were classified as either deficient or marginal in status. The mean hemoglobin concentration was 12.8 ± 0.9 g/dL and 7% of children were anemic.
Vitamin A and Hemoglobin Status of Selected Children in Antique, Northern Samar, and Sorsogon Provinces.a
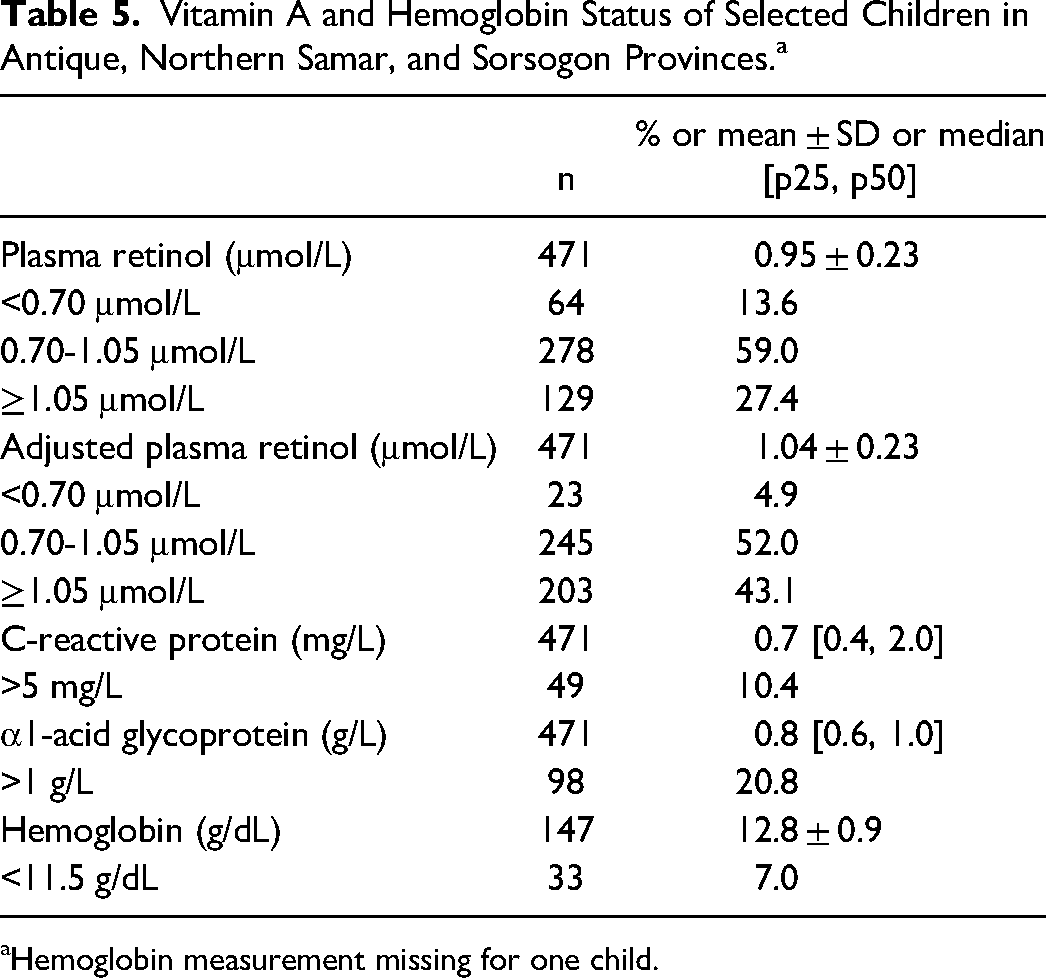
Hemoglobin measurement missing for one child.
Discussion
National surveys in the Philippines have shown consistent improvements in both dietary VA intake and in VA status over the past 20 years.1,2 The most recent national-level data indicate that ∼15% of preschool-aged children are deficient. 2 Our study, while not representative of the entire population, found a similar prevalence among school-aged children. It is important to note that inflammatory biomarkers are not currently measured as part of the biochemical component of the National Nutrition Survey, so inflammation-adjusted prevalence estimates are unavailable. Adjusting for inflammation in our data reduced the prevalence of VAD from 13.6% to 4.9%. Even after adjustment, more than half of all children had plasma retinol concentrations <1.05 μmol/L, indicative of deficient to marginal VA status.
Based on a VA-focused food frequency questionnaire, we showed that most children had access to sources of preformed VA, notably eggs, and that these were consumed a median of 7 times per week. These sources included fortified milk and foods bearing the Sangkap Pinoy Seal, used by food manufacturers to promote fortified products. While the inclusion of these foods in the diet is promising, the frequency of consumption was relatively low and may not have been sufficient to ensure adequate VA intake. For example, milk is available in the area and was consumed at least once by about half of children, but the median consumption was only 2 times in the past week. This finding aligns with national data from repeated 24-h recalls which show a high prevalence of dietary VA inadequacy (∼58%) in this age group. 12 It is worth noting that the analysis of national survey data accounted for only dietary sources. Our data suggest that daily supplements may be important contributors to overall VA intake in about one-quarter of children. It was notable that, among those receiving supplements, almost all children had consumed them 7 times in the past week. This regular consumption of supplements providing the Recommended Dietary Allowance or more is very likely to contribute to adequate VA status.
Although our primary focus was on VA intakes and status, our study also provides data relevant to the school health and feeding programs. Most children in our study came from households experiencing moderate to severe food insecurity, likely contributing to the 40% prevalence of stunting. Only ∼10% of children were classified as thin based on their BMI-for-age. This is notable because a low BMI-for-age is the indicator used to define eligibility for the Department of Education's school-based feeding program. However, a further 38.0% of children were at risk of underweight or thinness. Given this, the high prevalence of food insecurity suggests a greater need for interventions. We found that VA and proVA-rich food sources are available in these settings and consumed by children. Foods such as milk could be considered for inclusion in the school feeding menu to increase the frequency of consumption and usual VA intakes. Anemia is another school health priority in the Philippines. The low prevalence of anemia we report here is promising and lower than the ∼12% prevalence previously reported for Filipino school-aged children. 13 This may be attributable in part to school-based deworming, although there are disputes as to the effectiveness of this intervention in maintaining hemoglobin concentrations.14,15
Our study has limitations. It was designed to guide the selection of a research site for a future randomized controlled trial of a VAD control intervention. Therefore, provinces, municipalities, and schools were purposively selected based on a likely risk of VAD, and our findings are not representative of school-aged children in these areas or more broadly. Furthermore, the dietary data that we present here reflect solely the number of times each type of food was consumed in the prior week, without capturing the serving size. Thus, we were unable to estimate the usual intake of VA. Despite these limitations, our study provides novel data on intake of VA-rich or proVA-rich food sources and VA status among Filipino school-aged children, who are not covered in the national survey's biochemical assessment. Additionally, we were able to measure inflammatory biomarkers, allowing us to assess the influence of inflammation on plasma retinol concentrations.
In summary, our findings suggest that school-aged children in these high-risk areas have access to VA- and proVA-rich foods and supplements. However, they may not be consuming these frequently enough, resulting in the high prevalence of marginal VA status. School-based programs may provide an opportunity to incorporate additional sources of preformed VA such as fortified milk into children's diets. However, targeting these programs solely to children classified as thin based on a BMI-for-age <−2 Z does not adequately address the needs in communities where a further 38% could be considered at risk of underweight (−2 to −1 Z) and most households face moderate to severe food insecurity. Future interventions should consider these broader nutritional challenges to effectively improve VA status and overall health in this vulnerable population.
Footnotes
Acknowledgments
The authors are grateful for the strong support of the Department of Education, the Department of Health, the National Nutrition Council, and local government unit officials. The authors acknowledge members of our Technical Advisory Group and colleagues at the Department of Science and Technology-Food and Nutrition Research Institute for their input on this study. Most importantly, the authors thank the teachers in our selected schools and the participating children and their families.
Author Contributions
All authors contributed to the study design and implementation. GVCG, NLCS, and ACP wrote the first draft. All authors interpreted the data and reviewed and contributed to the manuscript.
Authors’ Note
Ethical Considerations: The Philippine Single Joint Ethics Review Board (Protocol # 2021-100; March 17, 2022), the Eastern Visayas Health Research and Development Consortium (Protocol # 2021-009; March 29, 2022), the Asian Eye Institute Ethics Review Committee (Protocol # 2022-008; April 22, 2022), and the Institutional Review Board of the Johns Hopkins Bloomberg School of Public Health approved our protocol (Protocol # 17000; June 20, 2022). Consent to Participate: Parents gave written consent and permission, and children gave verbal assent before starting interviews and assessments. Data Availability: The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded, in whole or in part, by the Bill and Melinda Gates Foundation [grant number INV-007261]. Under the grant conditions of the Foundation, a Creative Commons Attribution 4.0 Generic License has already been assigned to the Author Accepted Manuscript version that might arise from this submission.