
Abstract
Dietary vitamin A inadequacy remains a serious public health problem, especially among young children. Food and condiment fortification programs and policies are in place in many countries to address this issue, but degradation of the vitamin A added via fortification can reduce the quantity of vitamin A reaching consumers. We modeled the impacts of vitamin A degradation on program effectiveness and cost-effectiveness in fortified wheat flour, sugar, and (hypothetical) bouillon cubes in Nigeria. We used secondary data to estimate the prevalence of vitamin A inadequacy among young children (6-59 months), and the programs’ modeled contributions to reducing vitamin A inadequacy at selected levels of vitamin A degradation. The Lives Saved Tool was used to estimate child-lives saved. Program costs were estimated using activity-based models. Vitamin A degradation had a large negative impact on program effectiveness. Over the 0% to 80% vitamin A degradation range, accounting for other existing programs, fortification of sugar (7.5 mg/kg), wheat flour (2 mg/kg), and bouillon cubes (96 mg/kg) would reduce inadequacies among children by 2.9 to 0.7 percentage points, 3.9 to 0.7 percentage points, and 20.6 to 9.6 percentage points, respectively. Over the same vitamin A degradation range, average annual child-lives saved ranged from 3984 to 769 (sugar), 3036 to 739 (wheat flour), and 15 301 to 7153 (bouillon cubes); estimated cost/child-life saved ranged from US$ 550 to US$ 2848 (sugar), US$ 1039 to US$ 4271 (wheat flour), and US$ 944 to US$ 2018 (bouillon cubes). Vitamin A fortificant selection, technological innovations in vitamin A fortificants, and/or changes in premix and fortified food handling and storage could reduce degradation; these options could increase program costs, but merit consideration.
Plain Language Title
The Modeled Impacts of Vitamin A Degradation on the Performance of Wheat Flour, Sugar, and Bouillon Fortification Programs in Nigeria
Plain Language Summary
Dietary vitamin A inadequacy remains a serious public health problem, especially among young children. Food and condiment fortification programs are in place in many countries to address this issue, but degradation of vitamin A can reduce program impacts and efficiency. We estimated the impacts of vitamin A degradation on fortified wheat flour, sugar, and (hypothetical) bouillon cubes in Nigeria. We focus on vitamin A inadequacy and mortality among young children (6-59 months of age), and fortification programs’ contributions to reducing inadequacy and mortality at different levels of vitamin A degradation. Program costs are included in this analysis. Vitamin A degradation had large negative effects on program impacts and efficiency. Technical and policy options exist for reducing vitamin A degradation; these options could increase program costs, but all merit consideration.
Highlights
Vitamin A fortification programs and policies can reduce dietary inadequacies and hence child morbidity and child mortality; in the context of Nigeria, these programs cost millions of US$ per year.
Vitamin A is known to degrade when exposed to heat, light, and/or high humidity.
We provide the first modeled estimates of the impacts of vitamin A degradation on the effectiveness and cost-effectiveness of wheat flour, sugar, and (hypothetical) bouillon fortification programs in the context of Nigeria.
While some programs generate higher levels of nutritional and child mortality benefits than others, vitamin A degradation can substantially undermine the impacts and cost-effectiveness of all of the fortification programs examined.
Policy and technological options exist for reducing vitamin A degradation.
Degradation of vitamin A can seriously undermine the impacts and cost-effectiveness of food fortification programs. If vitamin A losses were 0, a hypothetical bouillon cube fortification program in the context of Nigeria aiming to contribute 30% of Codex Nutrient Reference Value for vitamin A per 2.5 g/p/d for adults would save an estimated ∼153k child-lives over 8 years at a cost of US$ 944 per child-life saved; if 80% of vitamin A were lost, only ∼72k child-lives would be saved at a cost of US$ 2018 per child-life saved. Improved premix and fortified food storage and handling practices, and perhaps especially technological advances to stabilize vitamin A, could help reduce vitamin A degradation and increase the benefits of these programs to all consumers.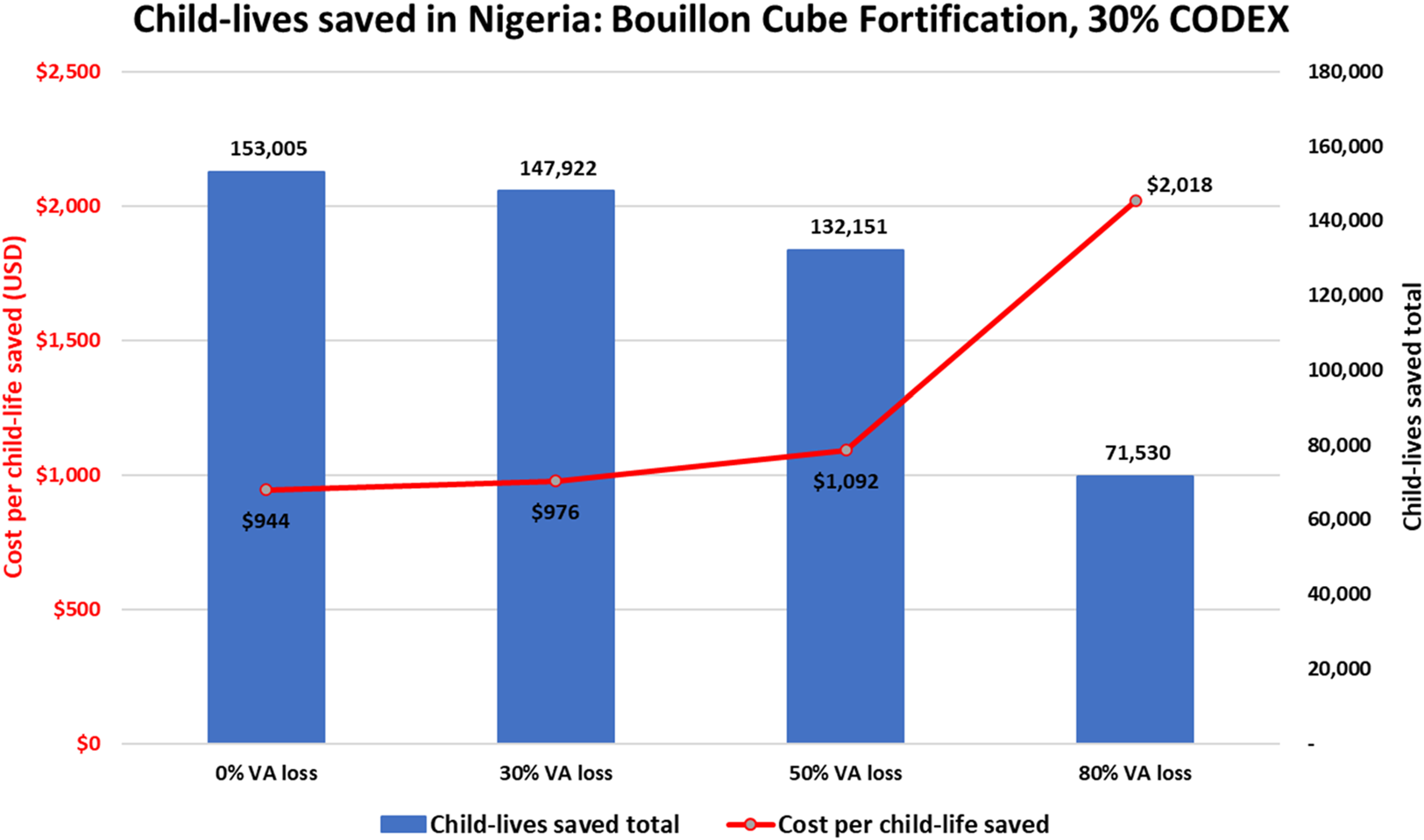
Introduction
Micronutrient deficiencies remain a major public health concern in most low- and middle-income countries (LMICs)1,2 with important consequences for child health and development3–7 and, for vitamin A in particular, child mortality.8,9 Dietary inadequacies are major contributors to these deficiencies and are also prevalent in LMICs. 10 An array of food and agricultural policies is available for addressing these dietary inadequacies, 11 some focus on consumers, 12 others focus on food producers and domestic food markets,13,14 and still others focus on international trade.i,15 Specific examples include biofortification of staple crops, 17 breastfeeding promotion, 18 and large-scale food fortification (LSFF) programs. ii None of these policy choices is costless, and their effectiveness will depend on the key program characteristics that will determine the amounts of micronutrients delivered to targeted consumers over time, and at what cost. This paper focuses on LSFF programs, which have been designed and implemented in many LMICs to help close the gaps between dietary intake and nutritional needs. 19 For example, every country in West Africa mandates that one or more staple foods be fortified with vitamin A, eg, Nigeria mandates the fortification of five vehicles for vitamin A (wheat flour, maize flour, edible oils, sugar, and margarine) and recently introduced a voluntary bouillon fortification program.20–25 Hence, many tons of vitamin A are being added to foods in Nigeria every year. iii For example, full compliance of the mandated fortification of wheat flour alone in Nigeria would require an average of 123MT tons of premix per year, 5% (6.15MT) of which would be vitamin A.iv,26 All of these programs require human and financial resources to establish and manage, and one of the main drivers of operational costs is premix purchases.
Some LSFF intervention programs have been shown to be impactful and cost-effective.27–32 To be impactful, they must be designed to reach vulnerable populations and managed to deliver policy-determined amounts of micronutrients. 33 There are many challenges associated with designing LSFF programs, eg, choosing appropriate food/condiment vehicles, developing appropriate and agreed-upon standards,27,34–37 and identifying and securing agreement on which stakeholder groups will pay program costs. 26 There are also many challenges associated with implementing and managing LSFF programs, eg, securing consistent adherence to fortification standards.29,38–40
One vexing and understudied challenge associated with LSFF program design and management is the potential for some micronutrients included in premixes to degrade—this is especially challenging in the context of vitamins. In particular, vitamin A is known to degrade when exposed to light, high heat, and high humidity, conditions that are common in markets and food distribution systems in LMICs.41–46 Losses can also occur during cooking. 47 Fortification programs often mandate that “overages” be included at the point of fortification to compensate for these losses, 27 thereby increasing technical challenges and the cost of fortification.
It may be possible to help protect vitamin A from degradation by modifying the durations and conditions of storage, and/or by technical innovations in vitamin A fortificants.45,48 However, these changes in transportation or storage durations or conditions, or technological changes, may have different costs, so it is important to know the impacts of degradation on the public health problems that vitamin A fortification is meant to address in order to assess the wisdom of intervening at 1 or more stages along the vitamin A fortification pathway.
The analysis and results presented here focus on the neglected issue of the potential impacts of vitamin A degradation on the effectiveness and cost-effectiveness of vitamin A fortification programs. More specifically, in the context of young children in Nigeria, we estimate the potential impacts of vitamin A degradation on the effectiveness and cost-effectiveness of existing wheat flour and sugar fortification programs, and on a hypothetical bouillon fortification program. v
Materials and Methods
Modeling Nutritional Benefits
We estimated the nutritional impacts of fortification programs based on modeling of household food consumption data, with particular focus on the population of young children 6 to 59 months of age. vi First, we matched household food consumption data from the 2018 to 2019 Nigeria Living Standards Survey (recall of quantities of each of 99 prespecified foods, including most of the fortified foods and the condiment included in this analysis and products containing them, consumed by household members in the past 7 days)49,50 with food composition estimates from the West African Food Composition Table, 51 supplemented with entries from the Nutrition Coordinating Center Nutrient Database for Standard Reference 52 and the Malawian food composition table. 53 Then, based on estimates of household daily apparent energy and vitamin A intake, we estimated the vitamin A density of the household diet (vitamin A per 1000 kcal) 54 in the absence of LSFF or other micronutrient intervention programs.
To account for vitamin A provided (in the form of retinyl palmitate 250 CP) via existing LSFF programs in Nigeria vii (target values are: refined edible oils, 6 mg/kg; sugar, 7.5 mg/kg; margarine, 7.8 mg/kg; wheat flour, 2 mg/kg; and maize flour, 2 mg/kg),viii,55 we multiplied daily household consumption of each food vehicle by the estimated average additional amount of vitamin A provided by LSFF based on current estimated compliance with industry standards and recalculated the vitamin A density of the household diet. 56 To estimate dietary vitamin A adequacy based on only baseline diets or baseline diets plus the amount of vitamin A contributed by existing LSFF, we compared the vitamin A density of the household diet to the critical vitamin A densities of children 6 to 59 months of age; critical vitamin A densities were calculated as the age- and sex-specific estimated average requirement (EAR) divided by the age- and sex-specific energy requirement, expressed in per 1000 kcal. Vitamin A requirements were from the US Institute of Medicine.57,58 Energy requirements were from the Food and Agricultural Organization. 59 Using household food consumption data and the nutrient density method to assess dietary adequacy depends on the assumptions that food is distributed in the household according to age- and sex-specific energy requirements, and that individuals in the household are meeting their age- and sex-specific energy requirements.
We modeled the impacts of vitamin A degradation separately for each of the three food/condiment delivery vehicles included in this analysis. For example, to model the marginal contribution of vitamin A-fortified wheat flour over a range of potential levels of vitamin A degradation, we began by estimating the vitamin A density of household diets, accounting for the vitamin A contributions to diets of existing LSFF programs except fortified wheat flour. Then, we modeled the additional contribution of wheat flour fortification at the national standard (2 mg vitamin A per kg of wheat flour), assuming 75% of fortifiable wheat flour would be fortified to this level. ix The fortification level was then adjusted down in a series of different modeling scenarios to account for potential vitamin A degradation of 0% (ie, no vitamin A degradation) to 80%. That is, for each vitamin A loss scenario, we multiplied daily apparent household consumption of wheat flour (grams) by the average additional vitamin A provided per gram of fortified wheat flour, recalculated the vitamin A density of the household diet, and compared the density to critical vitamin A densities.
For sugar, we similarly began with the vitamin A density of diets accounting for existing LSFF except sugar fortification, and then we modeled the additional contribution of sugar fortification at the national standard (7.5 mg/kg), assuming 75% of fortifiable sugar would be fortified to this level and adjusted this level down for potential vitamin A degradation of 0% to 80%.
Because bouillon is not currently mandated to be fortified with vitamin A in Nigeria, the starting point for bouillon fortification was the vitamin A density of diets accounting for all existing LSFF programs. Then, we modeled the additional contribution of bouillon, assuming a target fortification level of 96 mg/kg, equivalent to meeting 30% of the Codex nutrient reference value (NRV), 60 calculated assuming 2.5 g of bouillon consumption per day among adultsx,56 again assuming 75% of bouillon would be fortified to this level (modeled by adjusting the fortification level down by 25%). Note that we assumed 96% of wheat flour and 100% of sugar and bouillon in the food system in Nigeria are industrially processed and hence fortifiable. Also note that the Nigeria Living Standards Survey did not collect data on household bouillon consumption, so we relied on the estimates of bouillon consumption reported in the final report of the 2021 National Food Consumption and Micronutrient Survey. 50 Specifically, we imputed bouillon consumption based on the zone-specific median bouillon consumption per 1000 kcal as summarized in the report. 56
The effectiveness of wheat flour, sugar, and bouillon fortification programs (assessed separately) under each modeled level of vitamin A degradation was based on the percentage and number of children effectively covered, which was calculated as the prevalence of inadequacy (assessed separately) in the absence of wheat flour, sugar, or bouillon fortification, minus the prevalence of inadequacy with wheat flour, sugar, or bouillon fortification. We converted the percent of children effectively covered to the number of children effectively covered by multiplying effective coverage (%) by the estimated total population of children 6 to 59 months in each year of the 10-year time horizon. 61 Note that because we assumed a 2-year startup period for bouillon fortification, effective coverage was set to 0 in years 1 and 2.
For each of the delivery vehicle-specific model simulations, the “background” contributions of diets and of existing LSFF programs (somewhat different for each simulation) to vitamin A intake were included. For example, when modeling the impacts of vitamin A degradation in fortified wheat flour, “background contributions” did not account for the fortification of wheat flour, but did include the contributions of the four other LSFF programs currently in place in Nigeria (sugar, refined edible oils, maize flour, and margarine). Similarly, sugar was excluded from the “background contributions” when modeling the impact of vitamin A degradation in fortified sugar.
Finally, we did not account for high-dose vitamin A supplementation received via either the campaign-based Maternal, Newborn, and Child Health Week (MNCHW) platform or via the clinic-based routine platform in modeling the prevalence of vitamin A inadequacy. The MNCHW platform, in particular, is generally considered a temporary intervention, maintained until diets change and LSFF programs mature.
Modeling the Effects of Vitamin A Fortification on Child Mortality Using LiST
Estimates of affected fraction (ie, the proportion of the target population with nutrient density of the household diet below the critical nutrient density) and effective coverage (ie, the proportion of the population that achieves nutrient density above the critical density via one of the fortification scenarios listed above) described above were used as inputs into the Lives Saved Tool (LiST) to generate estimates of child-lives saved due to fortification with vitamin A. The methods used to link these estimates to the LiST model have been described in greater detail in Thompson et al. 9 A summary is provided below.
The LiST model is a deterministic model developed to estimate the effects of public health intervention programs on maternal and child mortality in low- and middle-income countries (https://www.livessavedtool.org/). The structure of the LiST model has been described previously.62,63 To summarize, the LiST model estimates child-lives saved due to an intervention by multiplying the following; the number of cause-specific deaths that could be averted by a given intervention, the change in coverage of that intervention, the affected fraction (proportion of the population to which the intervention benefits are applied), and the effectiveness of the intervention on cause-specific mortality.
Methods have been developed to adapt the LiST model to estimate the impact of LSFF programs on child mortality. 64 In addition to the use of estimates of affected fraction and effective coverage in the LiST model, intervention effectiveness estimates were changed to reflect the estimated impact of achieving dietary adequacy on child mortality rather than the effect of supplementation on child mortality, as is the default in the LiST model. Specifically, the vitamin A supplementation pathway was used to estimate lives saved among children 6 to 59 months of age. Default LiST parameters were replaced with country-specific estimates of apparent vitamin A inadequacy (affected fraction) and effective coverage for each modeled vitamin A degradation scenario. xi
Modeling Vitamin A Fortification Program Costs
An ingredient- and activity-based approach was used to estimate the economic costs of planning, designing, launching, and operating bouillon fortification programs in Nigeria from a societal perspective.26,65,66 A similar approach was used to estimate the costs of existing wheat flour and sugar fortification programs, except these programs do not face any start-up costs in the context of Nigeria. This approach focuses exclusively on the marginal costs of fortification for governments, industry, and consumers who, in the end, may pay all fortification program costs via increased retail prices for fortified foods and/or taxes. Several steps are involved in estimating program costs: (1) estimating the average annual consumption of fortifiable products, (2) determining how much vitamin A is included in the premixes, the prices of the selected vitamin A fortificant and the total cost of premix, including shipping, handling, and storage, (3) estimating the proportions of products that are locally produced versus imported, (4) estimating the government start-up and operational costs, and (5) estimating industry start-up and operational costs. 26 All of these costs were assessed on an annual time-step and summed over the temporal extent of the model, which is 10 years; this temporal extent allows time for up-front investments required to design and implement some LSFF programs, and to incorporate changes in population size and age structure over time. Bouillon fortification, in particular, was assumed to have a 2-year start-up period during which costs are paid but no nutritional benefits accrue.
Key cost model assumptions and parameters included the assumption that the vitamin A fortificant was retinyl palmitate—250 000 IU/g (dry), and the price of the fortificant was US$ 35/kg. xii No overages were included in calculating premix costs (overages for vitamin A in wheat flour and in sugar were assumed to be included in the current mandatory standards, and there is currently no mandatory or voluntary standard requiring the addition of vitamin A to bouillon). All costs are presented in 2021 US dollars.
Linking nutritional and child mortality benefits to fortification program costs requires temporal synchronization and spatial harmonization. Temporally, all of the estimates generated by the nutritional benefits, child mortality, and cost models represent the same simulation time period (in this case, 2021-2030). In addition, the temporal flows of benefits are tied to the specific time periods during which such nutritional benefits are expected to flow, eg, for bouillon fortification, no benefits are generated during the assumed 2-year bouillon fortification program start-up periods, although costs will be incurred during these 2 years. Spatially, for this analysis, all results are reported at the national level.
Vitamin A Pathway—From Fortificant Production to Consumption
Vitamin A follows a long pathway between production and final absorption in consumers’ bodies, and degradation can occur anywhere along that pathway (Figure 1). This pathway involves a series of steps beginning (at T = 0) with fortificant quality when produced and upon receipt by premix producers, and over time through various stages of the premix supply chain, through the production and marketing of fortified foods, and finally through to the purchase/preparation/consumption by individuals in households. At each step, the duration and quality of the treatment of the fortificant, the premix, or the fortified food can influence vitamin A degradation. 46 In the context of most LMICs, this pathway begins internationally with the importation of fortificants or finished premixes; these imported products generally arrive with certificates attesting to the content and purity of products. Beyond this point in the pathway, little is known about where along this pathway degradation occurs, the extent of degradation, or how this might vary across vitamin A delivery vehicles. Wherever data are available on degradation, they should be used, but this (general) gap in knowledge can impede the development of specific policies and practices to reduce degradation.67,68 The methods described above and the evidence presented below correspond to a few stages along the pathway: (1) cost estimates are generated from the perspective of the food/condiment producer (third box along the horizontal axis of Figure 1) and represent the marginal costs of designing and managing LSFF programs which can be dominated by premix costs, and (2) the nutritional and mortality benefits are generated from the perspective of purchasing households (fifth box) and consumers within them (sixth box). But vitamin A degradation could occur at stages before and/or between them, and therefore influence private-sector and public-sector opportunities for reducing degradation.
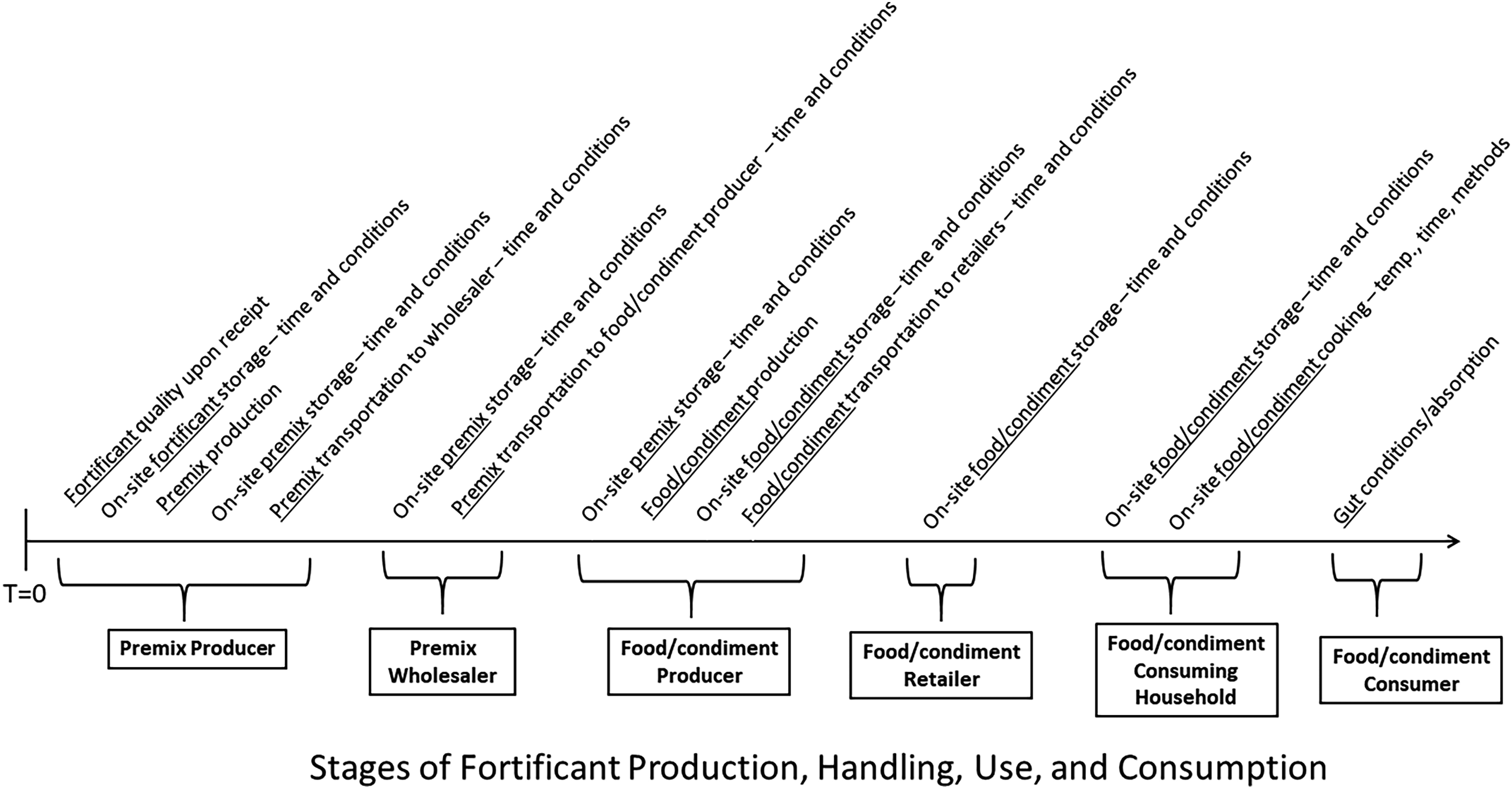
Vitamin A supply chain and potential sources of degradation.
Results
Figure 2 through Figure 4 summarize the results of model simulations focused on assessing the impacts of alternative vitamin A degradation scenarios in fortified wheat flour, sugar, and bouillon cubes in terms of effective coverage (Panel A) and child-lives saved (Panel B).
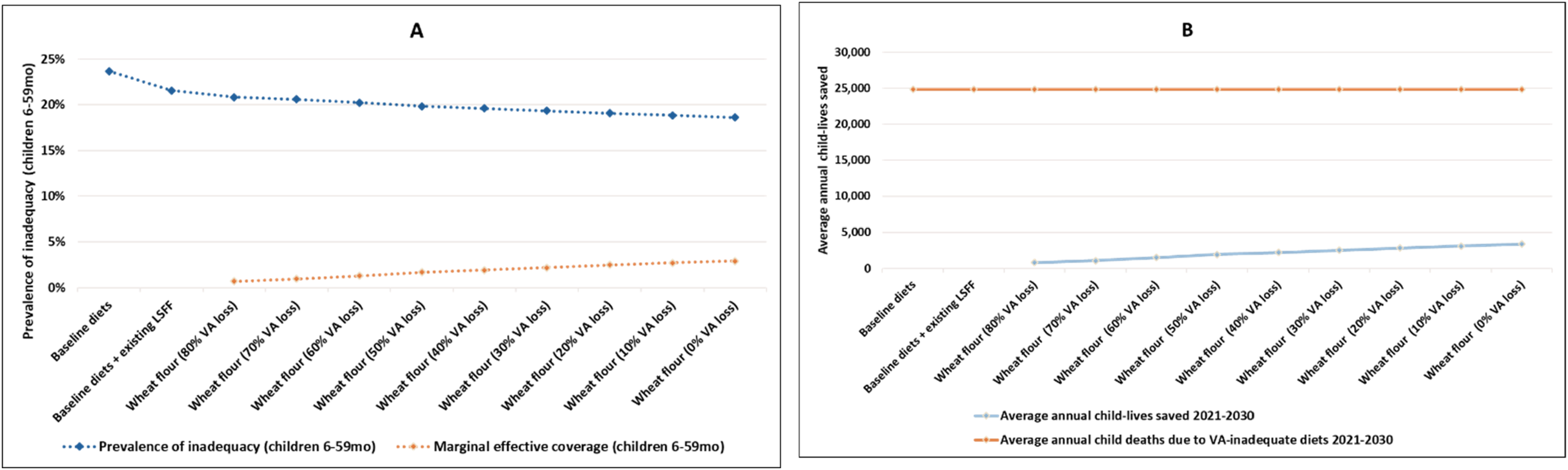
Modeled effects of vitamin A degradation on vitamin A inadequacy (A) and child-lives saved (B) via wheat flour fortification.
Wheat Flour
Figure 2, Panel A reports the baseline level of dietary inadequacy of vitamin A among children (∼24% in the absence of five existing LSFF programs, and ∼22% once the contributions of these programs are accounted for), and the estimated impacts of alternative assumptions regarding vitamin A degradation in wheat flour (from 0% loss to 80% loss, reading right to left) in terms of marginal effective coverage among children 6 to 59 months of age xiii (dotted orange line) and the percentage of children at risk for dietary VA inadequacy (dotted blue line). The marginal effective coverage curve suggests that even if there were no vitamin A degradation (far righthand side of Panel A), the marginal contribution of vitamin A-fortified wheat flour to reducing dietary inadequacy among young children would be small (<5 percentage points) over the 10-year model simulation period in the context of Nigeria, and that vitamin A degradation systematically erodes that maximum modest contribution to 0.7 percentage points.
Figure 2, Panel B depicts the estimated impacts of vitamin A degradation in terms of the average number of child-lives saved per year, based on the accumulated child-lives saved over the entire 10-year modeling time horizon (as was the case for effective coverage, the marginal child mortality reduction benefits of reductions in vitamin A degradation for wheat flour begin to accrue in year 2) and under the same set of vitamin A degradation assumptions. Approximately 30 000 child-lives over the 10-year simulation period could be saved if vitamin A degradation were zero; this number drops to ∼7000 as vitamin A degradation rates reach 80%. xiv
Sugar
Figure 3, Panel A reports the results of alternative assumptions regarding the degradation of vitamin A in fortified sugar on marginal effective coverage (dotted orange line) and the percentage of vitamin A-inadequate children (dotted blue line). Marginal effective coverage ranges from 0.7 percentage points at 80% of vitamin A degradation to 3.9 percentage points at 0% degradation.
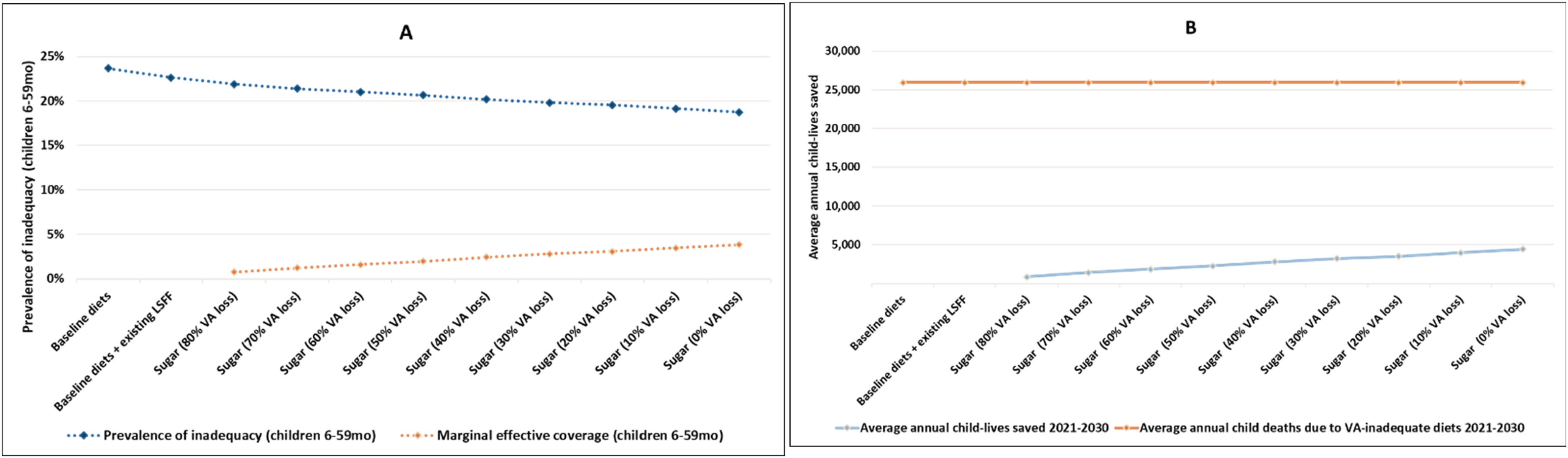
Modeled effects of vitamin A degradation on vitamin A inadequacy (A) and child-lives saved (B) via sugar fortification.
Figure 3, Panel B depicts the results on the average number of child-lives saved per year over the entire 10-year modeling time horizon, under the same set of alternative vitamin A loss assumptions. The total number of child-lives saved at zero vitamin A degradation is ∼40 000 over the 10-year simulation period; that number falls to ∼7500 child-lives saved if 80% of the vitamin A is lost.
Both panels in Figure 3 suggest that even at 0% vitamin A loss, the marginal contribution of sugar fortification to addressing vitamin A inadequacy in children would be relatively small and, consequently, reductions in child mortality are also relatively small.
Bouillon Cubes
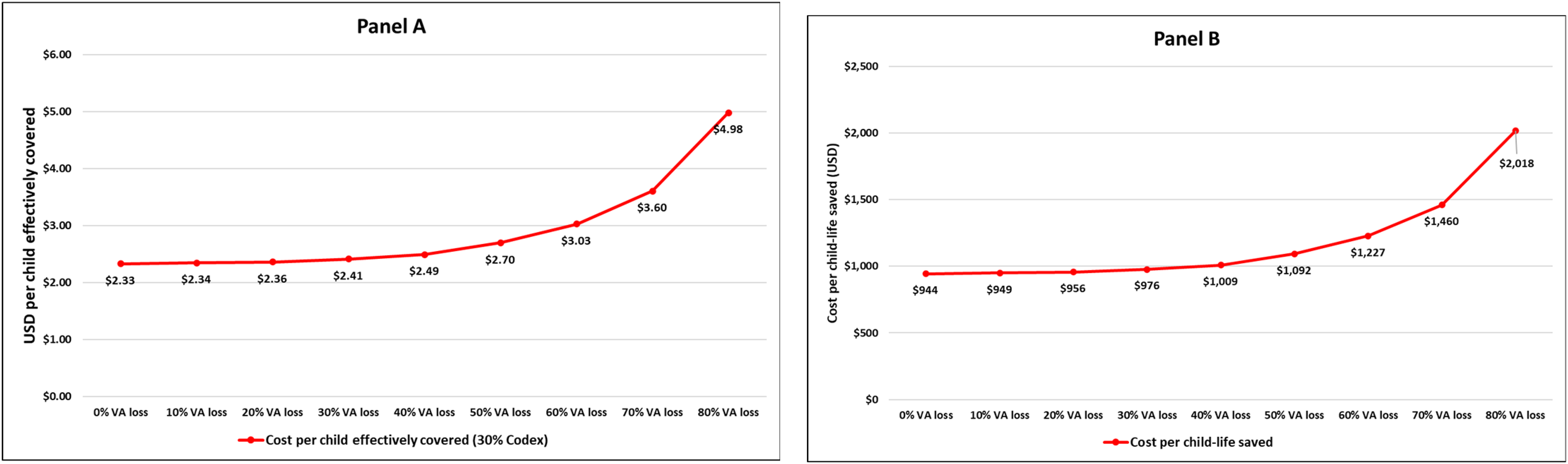
In what follows, we examined the potential impacts of hypothetical bouillon fortification with vitamin A on the vitamin A adequacy of young children and on child-lives saved, again along a gradient of assumed vitamin A losses due to fortificant degradation. Figure 4, Panel A reports the changes in the modeled prevalence of vitamin A inadequacy among children (blue dotted line) and the marginal effective coverage (orange dotted line) of alternative assumptions regarding the degradation of vitamin A, a widely consumed condiment in Nigeria, 56 assuming a level of fortification equivalent to 30% of Codex NRV in 2.5 g of bouillon (96 mg/kg). The far right-hand side of Panel A represents the maximum potential contribution of the modeled fortified bouillon cube; without any vitamin A losses due to product degradation, this bouillon cube has the potential to reduce vitamin A inadequacy among children to practically 0. Vitamin A degradation reduced those gains substantially, but even if 80% of vitamin A were lost, the remaining 20% would make a substantial reduction in vitamin A inadequacy among children (from ∼22% {baseline diets plus existing LSFF programs} to ∼10%). The same pattern of benefits was evident in the case of child-lives saved; vitamin A losses of less than roughly 30% would essentially achieve the maximum potential number of vitamin A-preventable deaths in children (∼157 200 over 10 years), but even if 80% of vitamin A were lost in the fortified bouillon cubes, ∼72 000 child-lives would be saved.
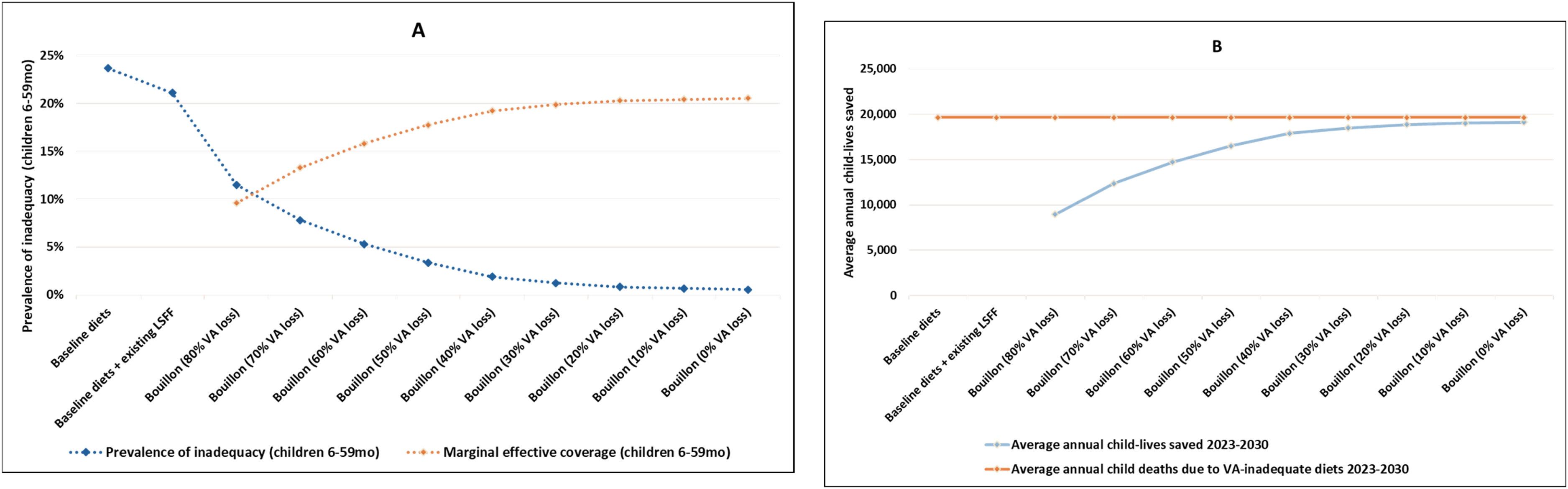
Modeled effects of vitamin A degradation on vitamin A inadequacy (A) and child-lives saved (B) via bouillon fortification.
Fortification Program Costs and Cost-Effectiveness
Next, we estimate fortification program costs and then link them with estimated program benefits—marginal effective coverage and child-lives saved—and then assess the impacts of vitamin A degradation on the cost-effectiveness of these programs.
Total 10-year costs of each LSFF program in the context of Nigeria are reported in Table 1. Note that there are start-up costs for the hypothetical bouillon fortification program, but not for the existing LSFF programs, even though there is a one-year delay in generating benefits in these cases.
Ten-Year Program Costs for Selected Vitamin A LSFF Programs.
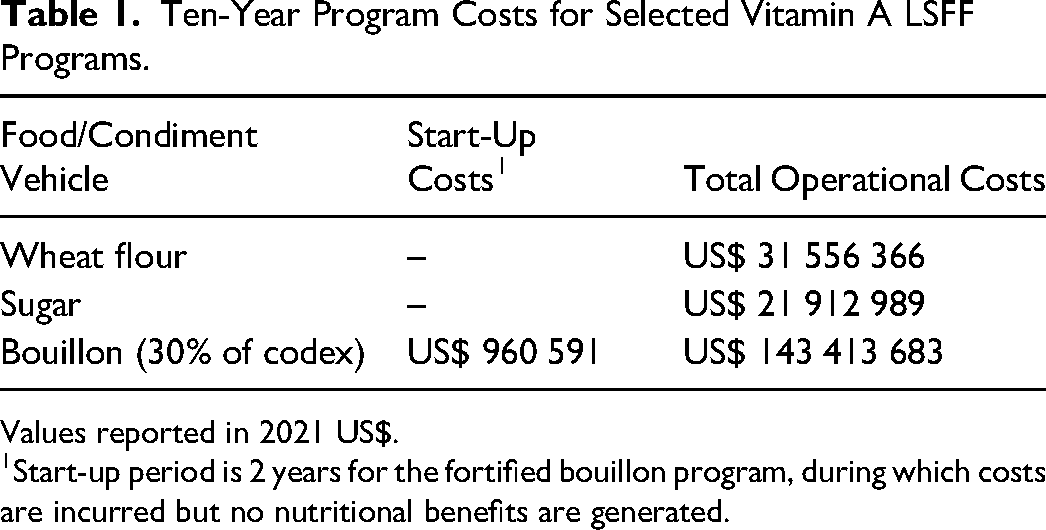
Values reported in 2021 US$.
Start-up period is 2 years for the fortified bouillon program, during which costs are incurred but no nutritional benefits are generated.
Program costs will not change with alternative assumptions regarding vitamin A degradation (the same amount of the fortificant would be purchased at the same price), but the cost-effectiveness of the program will change because vitamin A degradation will directly affect dietary inadequacy and indirectly affect child mortality. Figure 5 reports cost-effectiveness results in the context of wheat flour fortification (again with vitamin A contributions by the fortified sugar and other existing LSFF programs included in baseline diets). Under an assumption of zero degradation, the cost per effectively covered child is US$ 2.90 (Panel A). This cost per child effectively covered rises continuously as assumed degradation levels rise, reaching US$ 11.93 if vitamin A degradation reaches 80%.
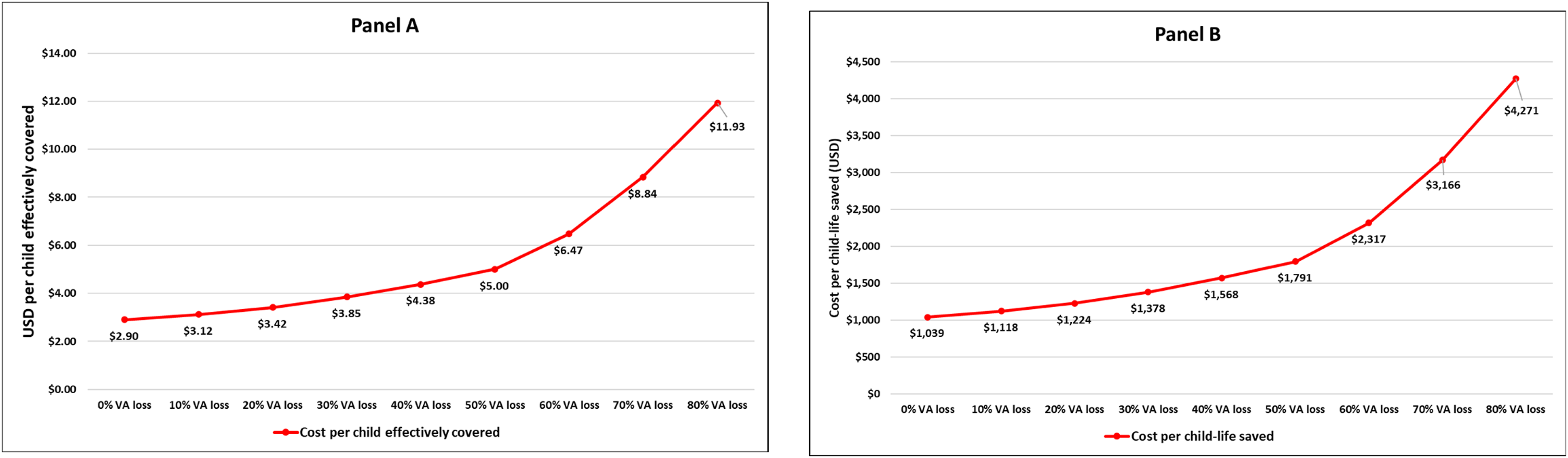
Modeled effects of vitamin A degradation in fortified wheat flour on cost per child effectively covered (Panel A) and cost per child-life saved (Panel B).
A similar pattern emerges for the cost-effectiveness of vitamin A in saving child-lives. Figure 5, Panel B reports the cost-effectiveness of wheat flour fortification at different assumed levels of vitamin A loss. Estimates of cost per child-life saved vary from US$ 1039 to US$ 4271 depending on the level of vitamin A degradation.
Figure 6 reports cost-effectiveness results in the context of sugar fortification. Under an assumption of zero degradation, the cost per effectively covered child is US$ 1.53 (Panel A). The cost/child effectively covered rises continuously as assumed degradation levels rise, reaching US$ 7.91 at a degradation level of 80%.
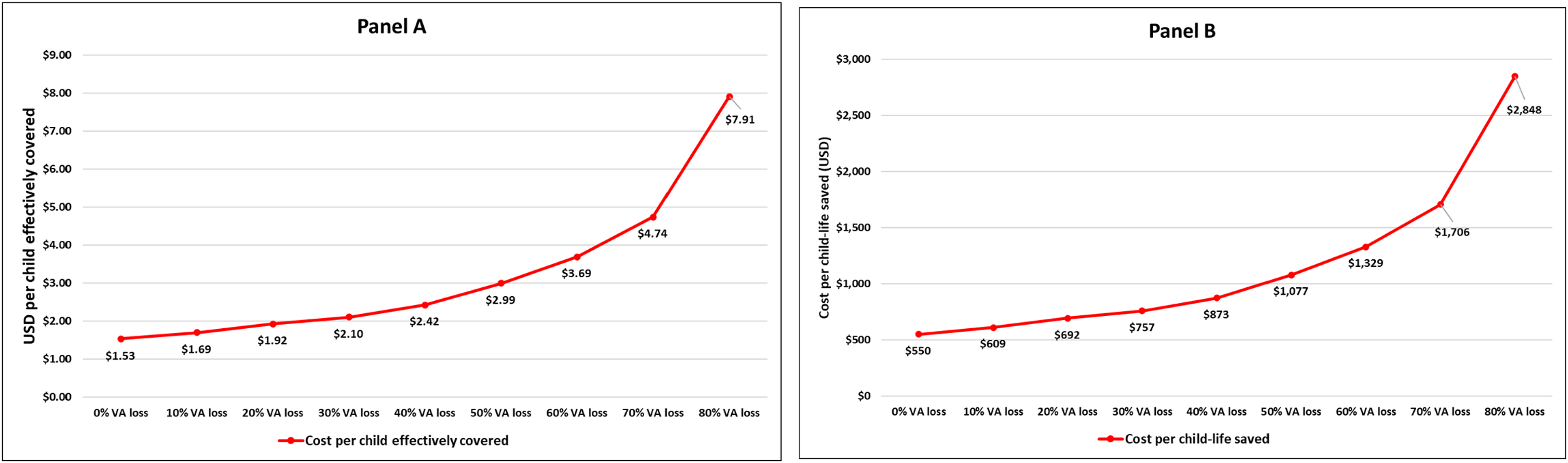
Modeled effects of vitamin A degradation in fortified sugar on the cost per child effectively covered (Panel A) and cost per child-life saved (Panel B).
Figure 6, Panel B reports the cost-effectiveness of wheat flour fortification at different assumed levels of vitamin A loss. Estimates of cost per child-life saved vary from US$ 550 (0% loss) to US$ 2848 (80% loss).
Lastly, we examined the effects of bouillon fortified at 30% of Codex in 2.5 g of bouillon on the cost-effectiveness of achieving vitamin A adequacy and on saving children's lives. Figure 7, Panel A reports cost per child effectively covered, again under alternative vitamin A loss assumptions. Cost per child effectively covered is US$ 2.33 at zero vitamin A degradation, rising to US$ 4.98 at 80% vitamin A degradation. Cost per child-life saved (Figure 7, Panel B) increases from US$ 944 (zero degradation) to US$ 2018 (80% degradation).
Modeled effects of vitamin A degradation in fortified bouillon (30% of codex NRV) on the per child effectively covered (Panel A) and cost per child-life saved (Panel B).
Table 2 reports the ranges of modeled impacts and cost-effectiveness for each delivery vehicle included in this study, at 0% and 80% levels of vitamin A degradation. The effects of vitamin A degradation vary across delivery vehicles, but both the impacts and efficiency of fortification programs fall in all cases as degradation increases, and clearly dwarf any cross-vehicle comparisons based on efficiency.
Ranges of Impacts of Vitamin A Degradation; Wheat Flour, Sugar, and Bouillon.
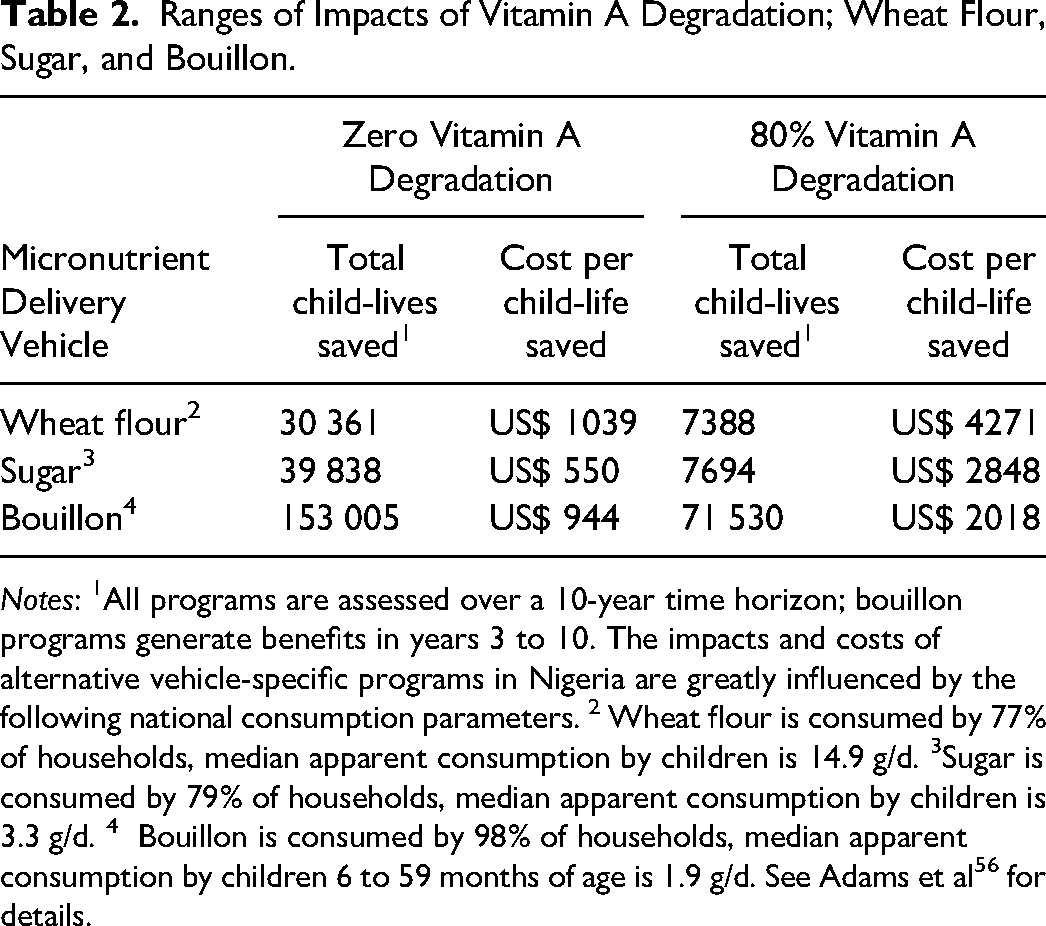
Notes: 1All programs are assessed over a 10-year time horizon; bouillon programs generate benefits in years 3 to 10. The impacts and costs of alternative vehicle-specific programs in Nigeria are greatly influenced by the following national consumption parameters. 2 Wheat flour is consumed by 77% of households, median apparent consumption by children is 14.9 g/d. 3Sugar is consumed by 79% of households, median apparent consumption by children is 3.3 g/d. 4 Bouillon is consumed by 98% of households, median apparent consumption by children 6 to 59 months of age is 1.9 g/d. See Adams et al 56 for details.
Discussion
Vitamin A deficiency remains a serious public health problem in LMICs, especially in the context of young children who suffer increases in morbidity and mortality.8,9 Dietary inadequacy is a key contributor to vitamin A deficiency, and governments, with the assistance of the international community, have responded, in part, by designing and implementing LSFF programs. There are recent/ongoing efforts to recommit to and strengthen existing programs, with particular attention paid to improving government monitoring and evaluation activities.69,70
While vitamin A is known to be sensitive to heat and light in some matrices,46,48 there is limited information on the extent to which vitamin A degradation influences program effectiveness and cost-effectiveness. It is unclear whether current recommendations regarding overages27,71 fully compensate for losses due to degradation. We used existing data and modeling tools to estimate the impacts, in the context of Nigeria, of various levels of vitamin A degradation in fortified wheat flour, sugar, and bouillon cubes (hypothetically) on vitamin A inadequacy in preschool children and on child mortality. We also estimated the impacts of vitamin A degradation to various degrees on the cost-effectiveness of these vitamin A fortification programs.
We found differences across the three food vehicles examined regarding their relative contributions to reducing vitamin A inadequacy, even with no vitamin A degradation. The overall modeled impacts of vitamin A fortification of wheat flour and of sugar were small relative to those of fortified bouillon. These differences are attributable to differences in estimated baseline dietary vitamin A inadequacy, vehicle-specific consumption patterns, and to the absolute amounts of vitamin A added to wheat flour and sugar. 56 The contributions of these programs could be increased if more vitamin A were added; indeed, in some settings, the fortification of sugar alone has greatly reduced vitamin A inadequacy, 37 so wheat flour and sugar fortification standards in Nigeria might merit review. That said, regardless of these differences, vitamin A degradation had negative impacts on the effectiveness and cost-effectiveness of each of these programs. Compared to the scenario with no vitamin A degradation, at 80% vitamin A loss, xv the cost per child-life saved was over 300% higher for fortified wheat flour, >400% higher for sugar, and >100% higher for vitamin A-fortified bouillon.
These results supplement the literature on the effectiveness and cost-effectiveness of LSFF programs.26,72–75 Some of these studies undertook sensitivity analyses associated with program benefits (usually measured in terms of achieving dietary adequacy in specific micronutrients), but they did not systematically examine micronutrient degradation or its consequences.
These results have several policy implications. First, it is important to know the potential magnitude of the vitamin A degradation and its implications for achieving fortification program policy objectives. In the context of Nigeria examined here, we discovered that the modeled impacts of existing wheat flour and sugar fortification programs were small in absolute terms and very small relative to hypothetical bouillon fortification; revising standards for these existing programs could narrow this gap. Second, and related, the effects of vitamin A degradation on modeled program impacts and cost-effectiveness varied across the three delivery vehicles examined here, suggesting that the effects of changes in policies and investments aiming to reduce vitamin A degradation generally will not be uniform across programs. This is not surprising, but if interventions to reduce degradation are vehicle-specific, this information may help prioritize policy focus. Third, and again related, all of the cost-effectiveness curves were curvilinear, ie, as levels of vitamin A degradation fell from 80%, the marginal gains in terms of program efficiency decreased. Therefore, collecting the data required to situate each program on the vitamin A degradation continuum will be an important first step in determining if policy action and investments to reduce degradation are needed, and which program(s) to focus on. Fourth, if a large vitamin A degradation problem exists, there are several alternative responses, which are not mutually exclusive, eg, standards can be revised to require the use of more and/or more stable forms of vitamin A. Either response will likely increase premix costs, but also may prove to be more cost-effective; policy instruments exist for addressing these higher costs. Fifth, private investments in premix shipping and storage (eg, refrigeration, in both cases) will likely reduce vitamin A degradation; public policy can help focus and facilitate these investments. Monitoring and evaluation of premixes (alongside current efforts to monitor and evaluate fortified products) could help identify additional places along the vitamin A pathway where degradation is occurring and provide entry points for policies and improved practices to reduce vitamin A losses. 77
This study has several limitations. First, we focused only on vitamin A; other vitamins will likely display different degradation patterns under similar storage conditions, and their degradation may also have public health consequences. Second, we focused only on the benefits to preschool children; other consumers of fortified products will also benefit from fortification programs and improvements in them, especially women of reproductive age. Third, this study focused on Nigeria; due to the size of the Nigerian population, the results in other West African contexts surely would be smaller in terms of the total numbers of children achieving dietary adequacy and child-lives saved. The modeled impacts of vitamin A degradation on program effectiveness and cost-effectiveness might also be different from the Nigerian patterns identified above, owing to differences in the existence and performance of LSFF programs, dietary intake patterns, dietary gaps, and consumption of fortified foods and condiments. 27 Fourth, all of the vitamin A needs assessments, and the estimates of the contributions of LSFF programs to meeting these needs were based on household-level food consumption and expenditure data that were collected over the 2018 to 2019 period, and supplemented with more recent estimates of bouillon consumption. These diets varied substantially across households in the data underlying this analysis, but for given households, we assumed diets did not vary over the 10-year simulation period used in this study. Fifth, LSFF program costs are in part driven by premix costs, which are influenced by fortificant prices; in this case, the price of retinyl palmitate. The price of this fortificant was held constant over the modeling time horizon, but variations in this fortificant price would not affect the general patterns of the results presented here. Sixth, nutrition analyses were based on household consumption and expenditure data that are available for essentially all LMICs and can be used to inform policy discussions, but have known strengths and shortcomings.78,79 Finally, as previously mentioned, policies to reduce vitamin A degradation anywhere along the pathway will have associated costs, which are not reflected in our cost-effectiveness analyses. Once more is known about where along the vitamin A pathway losses are occurring and the policy options to address them are identified, cost-effectiveness analysis can be used to identify the most efficient policy solutions.
Conclusions and Implications for Policy
Increasing young children's dietary intake of vitamin A can save lives and contribute to their health and development. Indeed, many LMICs have designed and implemented large-scale food and condiment fortification programs to help meet their populations’ vitamin A needs, with special attention paid to preschool children and women of reproductive age. However, vitamins in general, and vitamin A in particular, are known to be unstable, especially when exposed to light, heat, and humidity. Standards for fortification often include overage amounts for vitamins to compensate for assumed losses from the point of fortification to consumption. However, vitamin A degradation rates may exceed those taken into consideration when setting fortification standards and overages. If this is true, then the expected nutritional and mortality reduction benefits associated with current fortification programs might be overestimated.
In the context of Nigeria, modeled results suggest that high levels of vitamin A degradation would reduce the expected marginal benefits of fortification programs, especially the (hypothetical) fortified bouillon program, which was the most impactful of the three examined here. That said, high levels of vitamin A degradation very substantially reduced the cost-effectiveness of all LSFF programs, leading in some cases to 4-fold increases in cost per child-life saved.
Policy changes and investments to increase vitamin A stability, and potentially the stability of other vitamins, too, would increase the streams of nutritional and other benefits generated by LSFF programs, and further research could provide insights into their relative cost-effectiveness.
Finally, the results presented here identify a gradient of negative impacts associated with vitamin A degradation. A logical next step would be to measure the vitamin A content in premixes and fortified foods/condiments along delivery-vehicle-specific vitamin A pathways. Then, the modeled results could be used in policy discussions aimed at identifying alternative investments (technological change, premix storage conditions, fortified product packaging and storage, etc.) and the associated policy changes needed to cost-effectively reduce vitamin A degradation and its consequences.
Footnotes
Acknowledgments
We gratefully acknowledge the contributions of colleagues at the Institute for Global Nutrition and the Department of Agricultural and Research Economics, University of California, Davis. We acknowledge the fundamental contributions made by those involved in the development of the models used in this paper, most notably Helen Keller International, Johns Hopkins University, the members of the Nigerian MINIMOD modeling team, and the members of the Nigerian Bouillon Country Working Group. We are especially indebted to Quentin Johnson for his insights into and information on large-scale food fortification programs, premix production processes, and premix ingredient prices. Finally, we acknowledge the very substantial technical input from the Particles for Humanity team, especially Judith Ternes, Caro Confort, Rachael Deraney, Sam Brady, Don Chickering, and Sherri Oberg. This research was funded, in part, by a grant from the Gates Foundation [INV-050527], via Particles for Humanity.
Author Contributions
All authors contributed to the design of the study; KPA and LT, respectively, undertook the dietary analyses and child mortality analyses; MJ and SV undertook the cost analyses; KP and SV prepared the first draft of the manuscript; all authors reviewed the draft manuscript and approved the final version of the manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Bill and Melinda Gates Foundation (grant number INV-050527).
Supplemental Material
Supplemental material for this article is available online.