
Abstract
Purpose:
To evaluate the safety and effectiveness of a modified polymethyl methacrylate-silicone keratoprosthesis and its operation method in alkali-burned rabbit model.
Methods and materials:
The polymethyl methacrylate-silicone keratoprostheses were implanted into seven alkali-burned rabbit corneas by a special operation method using autologous graft as the keratoprosthesis (Kpro) carrier. The long-term postoperative outcomes were evaluated.
Results:
During a postoperative study period of 16 months, except for one Kpro extruded at 3 months, all Kpros were in good position and were kept transparent without Kpro extrusion, keratolysis, infection, endophthalmitis, or retinal detachment. The postoperative complications included elevated intraocular pressure in two cases and temporary retroprosthetic membrane formation in two cases.
Conclusion:
The modified polymethyl methacrylate-silicone Kpro and its operation method is a relatively safe and effective choice for alkali-burned rabbit eyes. Elevated intraocular pressure is the main complication needing to be resolved.
Introduction
There are millions of medicable blinds due to corneal diseases all over the world. Some of the corneal lesions are severe with massive vascularization and scarring. For these severely damaged corneas, keratoprosthesis (Kpro) is the only solution. Boston Kpro (B-Kpro) is currently the most widely used Kpro around the world. 1 But B-Kpro needs a relatively healthy allograft corneal graft as its carrier (supporter), and, furthermore, it is not suitable for a very dry ocular surface because of the high likelihood of epithelial breakdown and stromal melting in the carrier donor cornea.2,3 In the developing world, donor cornea is not easy and cheap to get, which limits the application of Kpro. Efforts have been made to use recipients’ own corneas as Kpro supporter. Osteo-odonto-keratoprosthesis (OOKP) is the most successful procedure. 4 OOKP has a very long retention time without extrusion or keratolysis, because it changes the corneal surface completely by adding a very thick corneal covering (mucosal membrane) in front of the damaged cornea. Moreover, it uses the recipient’s own tooth and bone to support the polymethyl methacrylate (PMMA) Kpro. OOKP can resist any dry ocular surface and lasts for a long period. However, its implantation procedure is complicated and time-consuming. Thus, we consider combining B-Kpro and OOKP Kpro together using the recipient’s own cornea as the Kpro supporter. In order to do this, there are several concerns to be addressed. One of them is that severely damaged corneas have different thicknesses, while the length of B-Kpro’s optical cylinder (stem) is fixed. During the process of assembling, the B-Kpro may not perfectly fit the different thicknesses of corneal lesions. Furthermore, in some cases, the burned corneas are too thin or too dry to support the Kpro, so an autologous conjunctival or mucosal transplantation is mandatory to reinforce the cornea before the Kpro implantation. 1 This procedure will also greatly thicken the cornea. Moreover, after Kpro operation, the cornea and its covering conjunctival or mucosal tissue will shrink or swell a little, which may change the total thickness of the corneal tissue. So we need a new Kpro to fit all kinds of thicknesses of the recipient’s corneal tissue. We present here a modified and self-fitting PMMA-silicone Kpro and its special operation method.
Materials and methods
The establishment of animal model
Eight Japanese white rabbits aged about 4 months and weighing about 3 kg were included in the study. The unilateral eye corneas of eight rabbits were burned by alkali (NaOH, 1 M) for 20 s. About 3 months later, one rabbit was excluded because of corneal perforation at 1 month, the remaining seven corneas had leucoma and vascularization in different degrees. Additional conjunctival transplantations were performed in two of the seven rabbit corneas because their corneas were too thin. Approval was obtained from the animal ethics committee of Kunming medical university and the declaration of Helsinki was followed during our animal study.
PMMA-silicone keratoprosthesis
Similar to B-Kpro, our modified PMMA-silicone Kpro was also made of two plates. The front plate was made of PMMA with a central transparent optical cylinder (stem), while the back plate was made of silicone gel (from ophthalmic silicone rubber for retinal detachment surgery). The dimensional details are shown in the schematic diagram in Figure 1. All the parts were manufactured and modified in the Ikarui optical instrument company of Kunming.
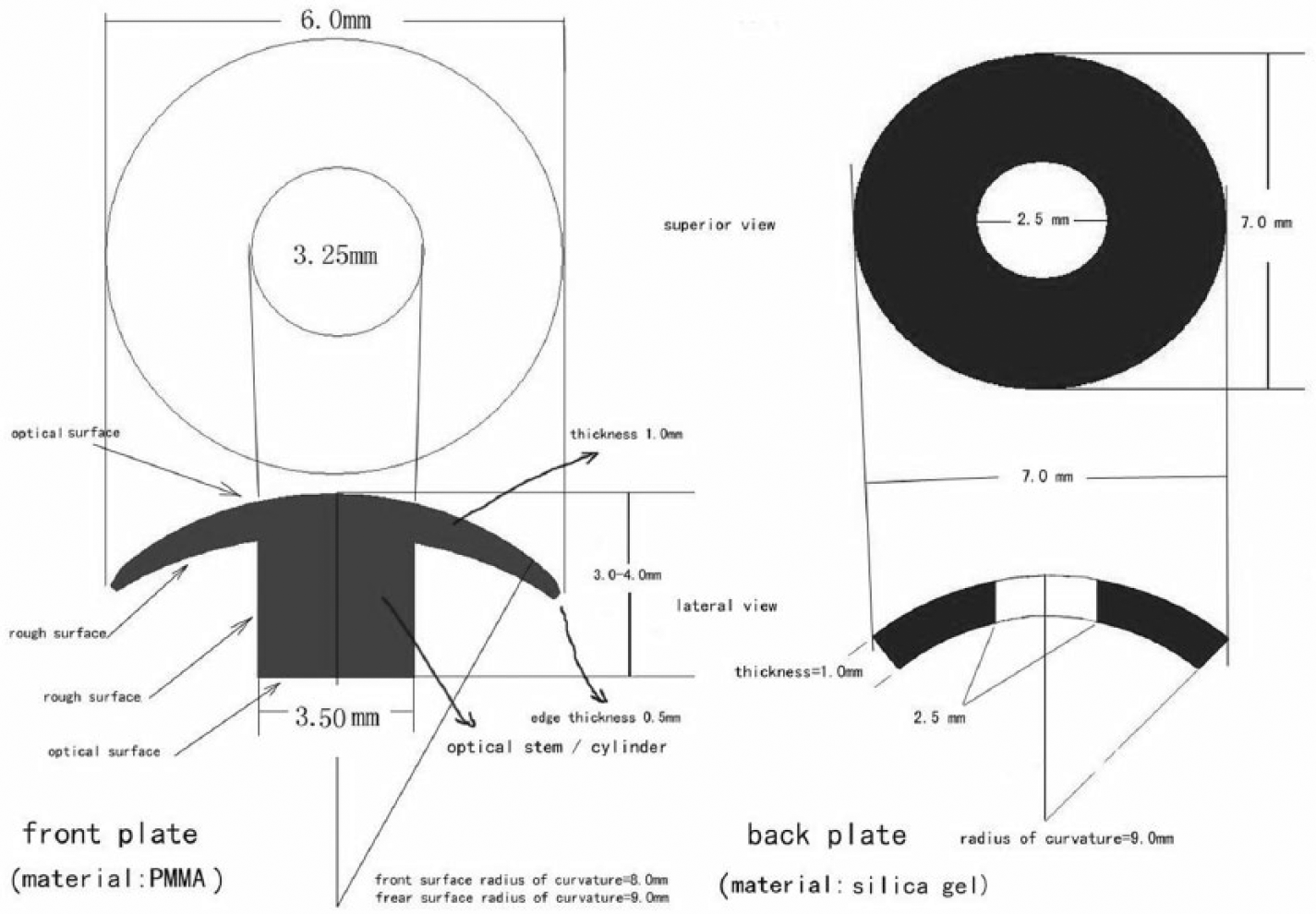
Schematic diagram of the PMMA-silicone Kpro with anterior and lateral views.
The operation method and postoperative management
The cornea (or with its conjunctival covering) was cut open with about a 270° opening, and then a corneal flap was lifted (see Figure 2). At the center of the cornea, a hole (3.0 mm in diameter) was trephined. After that, the PMMA-silicone Kpro was assembled in situ. The lens was removed completely. Partial iridectomy was performed in several cases. The anterior vitreous body was cut off. The cornea opening was then closed with 10–0 sutures. The anterior chamber was formed with saline solution and viscoelastics. Antibiotic and steroid eye ointment was applied to the eye after operation. Tobramycin and dexamethasone ophthalmic ointment was administrated daily for 2 weeks. The postoperative results were observed by slit lamp biomicroscopy and B-scan ultrasonography for any leakage, melting, membrane formation, infection, hemorrhage, or retinal detachment. Intraocular pressure (IOP) was tested by finger palpation.
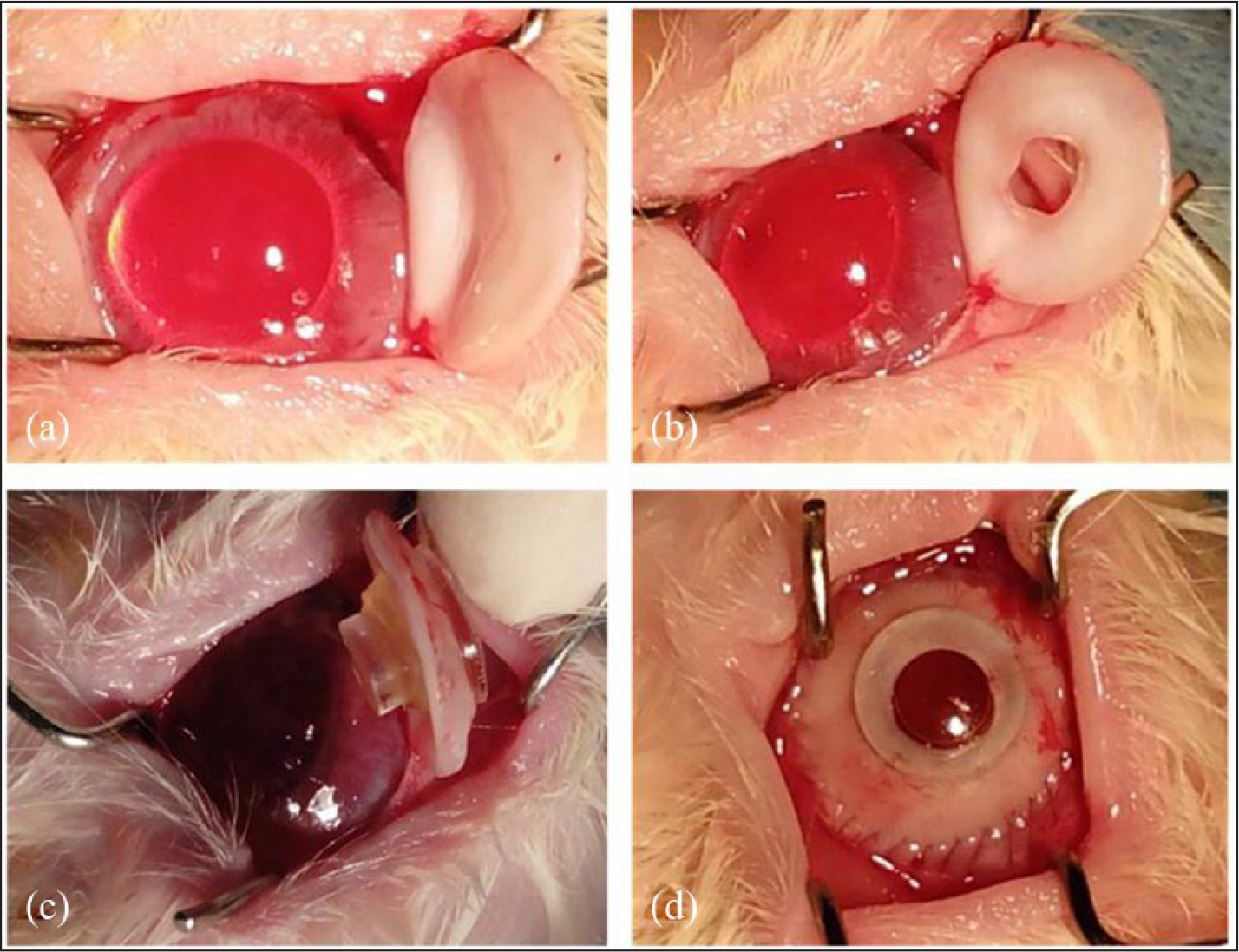
The operation procedure: (a) cut and flip the cornea with a 270° opening; (b) a 3.0-mm hole is trephined in the center; (c) assemble the front plate and the back plate before lens removal, vitrectomy, and partial iridectomy; and (d) suture the incision.
Results
All seven rabbits survived the operation without intraoperative complications. One rabbit’s Kpro extruded 3 months after operation because of elevated IOP. At the end of the experiment (16 months after operation), six rabbits’ Kpros were in good position with transparent central optic cylinder, without keratolysis, extrusion, infection, hemorrhage, or retinal detachment (see Figures 3 and 4). The elevated IOP was found in two rabbit eyes (including the extruded one). The retroprosthetic membrane formation was found in two rabbit eyes at about 1 month postoperatively, but was absorbed automatically 1 month later without any management.
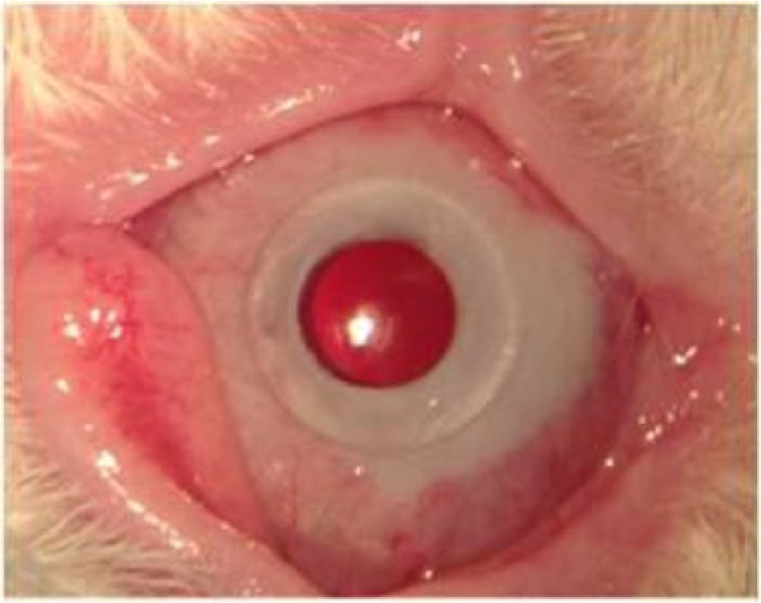
One month after operation.

Sixteen months after operation.
Discussion
Modification of Kpro design
Kpro is an optimum choice for severely diseased corneas. B-Kpro is currently the most commonly used Kpro around the world with a remarkable 5-year retention rate of about 90%.1,5,6 However, it needs a relatively healthy donor graft as Kpro’s carrier and, in developing countries, this donor graft is not easy and cheap to get. 7 Another drawback is that B-Kpro is not suitable for a very dry ocular surface because it can cause donor graft cornea melting or breakdown.2,3 The OOKP is another widely used Kpro with a lesser 5-year retention rate of about 60%.4,8 For its design, it adds a very thick corneal covering (mucosal membrane) in front of diseased cornea before OOKP implantation, so it can be applied to any dry ocular surface. Although it doesn’t need a donor cornea as the Kpro carrier, this procedure needs to harvest the recipient’s bone and/or a tooth to support the Kpro and is time-consuming (it needs three stages).
Given all these disadvantages, in our design, we tried to combine these two kinds of Kpros together. To the best of our knowledge, there is no design similar to ours so far. We continued to use B-Kpro’s two-plate “collar button” idea. Instead of using a donor corneal graft, we used the recipient’s own cornea as the Kpro carrier. Used in this way, we would face the challenge that the diseased corneas with their proliferative connective tissue and scarring would have quite different thicknesses. So it is difficult to use the B-Kpro, as the length of its optical cylinder (stem) is fixed. Because of this, we changed the Kpro’s back plate from PMMA to silicone gel, which has been used in retinal detachment repair for a long time. Since the silicone gel was elastic, we didn’t need to make the screw thread (like on nuts and bolts) to fix it onto the optical cylinder of the front plate. It could be fixed at any position on the optical cylinder tightly to fit different thicknesses of the corneas and/or their covering (conjunctival or mucosal membrane). There were three designs to prevent loosening of the silicone gel back plate. The first design was that the central hole of the silicone gel back plate was much smaller (diameter = 2.5 mm) than the optical cylinder (diameter = 3.5 mm), which increased the friction to avoid loosening of the back plate. The second design was the side surface of the optical cylinder was made so rough that it also increased the friction. The third design was that the size of the upper part of the optical cylinder (diameter = 3.25 mm) was slightly smaller than the size of the lower part of the optical cylinder (diameter = 3.50 mm), which was to make sure that the silicone gel back plate wouldn’t slide off from the optical cylinder. In our study, no loosening of the silicone gel back plate was found, even in the extruded case.
Moreover, after the operation, the tightness of our Kpro would also be adjustable. If the corneal tissue became thicker (e.g. swelling), the silicone gel back plate could step back automatically. On the contrary, if the corneal tissue became thinner (e.g. shrinkage), the silicone gel back plate position could be adjusted (fastened) easily by a single forceps. In order to do so, we could insert one foot of a forceps into the anterior chamber (behind the silicone gel back plate) through a small incision while putting another foot of the forceps in front of the front plate, and then clamp the front and back plates together.
Modification of operation method
Some researchers have successfully used the patient’s autologous corneal graft as the Kpro carrier.9,10 In our study, we carried out a similar method. Our PMMA-silicone Kpro’s assembling procedure was quite different from B-Kpro’s. Because our silicone gel back plate was elastic without a screw thread, we didn’t need to cut the whole cornea off for assembling the cornea-Kpro complex. We just made an opening of 270°, or less (a pedicle flap), to finish the assembling procedure in situ. There were three advantages to this special implantation method. First, as we had known, there was no need for a donor corneal graft as the Kpro carrier, which is rare and expensive in developing countries. Second, no graft rejection happened at all, which could cause corneal melting or Kpro extrusion. Third, the blood supply was better and the healing time was faster. Given that the silicone gel back plate was easy to assemble in situ, a flap of more than 90° corneal tissue was untouched. This remained a part of the corneal blood vessels, which gave corneas an instant blood supply after operation. The faster healing and better blood supply could help corneas resist leakage and melting after operation.
Some further tips from our study should be mentioned here. For example, the trephined central corneal hole (3.0 mm) should be slightly smaller than the optical cylinder (3.5 mm), which is a simple procedure. Because the corneal tissue was elastic and could be enlarged a little, a smaller corneal hole and its late shrinkage would decrease the gap between the central corneal hole and the optical cylinder. In our study, no leakage was found (even in the extruded case). Another tip was, if the cornea had its conjunctival covering, we suggested opening the cornea and its covering tissue together, because separating the covering tissue from its underlying cornea would cause more damage to the cornea and its blood supply. Our experience proved that this procedure was not difficult. But mucosal covering might be different because it is too thick.
Complications
What we were most concerned with in the autograft operation method was the elevated IOP. It has been a common challenge in B-Kpro (from 30% to 65%)5,6,11,12 and in OOKP (10%). 8 In our study, two rabbit eyes suffered from elevated IOP (of them one Kpro extruded because of this). We analyzed that the same sizes of the corneal button and bed might shallow the anterior chamber which would cause the anterior synechia of iris and the postoperative angle-closed glaucoma.13,14 In order to avoid glaucoma, as well as lens removal and anterior vitrectomy, we considered that complete iridectomy would be essential. Akpek et al. 15 had reported that B-Kpro implantation in aniridia cases was feasible. Whether the iridectomy can cease the elevated IOP is a subject of future study.
Retroprosthetic membrane formation was another concern we confronted. It was also a common complication after B-Kpro implantation.16,17 In our study, it happened in two cases, but it existed only temporarily. It was absorbed spontaneously 1 month later. We inferred inflammation to be a major cause for retroprosthetic membrane formation. Maybe a long optical cylinder, a thorough anterior vitrectomy, and iridectomy would reduce its incidence.
In the future, instead of an open-sky (large incision) operation method, we propose a smaller corneal incision (8 mm), which is enough for inserting a folded silicone gel back plate and assembling the Kpro in situ (like a folded artificial lens). After the assembling, lensectomy, anterior vitrectomy, and iridectomy can be performed through 25G incisions. Better results could be achieved with minimal damage to the eye, lesser inflammation, and quicker healing.
Conclusion
We have provided here a new PMMA-silicone Kpro and its operation method. We used the donor’s own cornea as the Kpro carrier, which did not need to open the whole cornea for assembling and could fit to various thicknesses of corneal lesions. It is relatively safe, effective, and cost-saving, and is also suitable for use in the developing world.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the applied basic research project of Yunnan province (No. 2013FB158), the scientific research fund project of the education department of Yunnan province (No. 2013C230), and the health science and technology plan project of Yunnan province (No. 2014NS040).