
Abstract
Purpose:
The purpose of this study was to assess the utility of a polyglycolic acid–collagen tube and to investigate its possible application in the field of facial nerve reconstruction.
Methods:
Wistar rats were used in this study. In the operation, a periauricular incision was made to expose the buccal and marginal branches of the facial nerve. Gaps of 10 mm were created by resection of a part of the nerve into the marginal branches and the buccal branch of the left facial nerve. The left marginal branch gap was bridged with a 10-mm polyglycolic acid–collagen tube or an autograft. At 12 weeks after the operation, nerve regeneration was assessed based on clinical, histopathological, and electrophysiological evaluations.
Result:
The functional recovery of the vibrissal muscle was observed with the polyglycolic acid–collagen tube. However, the functional recovery obtained with the use of the polyglycolic acid–collagen tube was inferior to that obtained with an autograft.
Conclusion:
We found that polyglycolic acid–collagen tubes could be applied in facial nerve gap reconstruction. However, further improvements will be necessary to achieve results that are equivalent to those obtained with autografts.
Introduction
In cases of facial nerve gap reconstruction, autologous nerve grafts are recognized as the only clinically effective choice.1–3 On the other hand, there have been a number of studies of artificial nerve development, and various products are currently in wide use in different countries.4–7 From 1980s, many biodegradable polymers’ conduit, including polylactic acid (PLA), polyglycolic acid (PGA), and polylactic-co-glycolic acid (PLGA) have been reported for peripheral nerve regeneration.4–7 An artificial nerve with a PGA tube containing a type I collagen sponge was first used in Japan in 2013. 8 At present, however, the function of the artificial nerve remains inferior to that of a traditional autologous nerve graft. Thus, this artificial nerve is mainly used in cases involving sensory nerve reconstruction and not for restoring the motor function. 9 Autologous nerve grafting is recognized as one of the most important procedures for facial nerve reconstruction.1–3 However, there are few studies on the utility of artificial nerve grafting in facial nerve reconstruction.6,10–12 This study aimed to assess the utility of a PGA–collagen tube and to investigate its possible application in this field.
Materials and methods
Animals
In this study, 10-week-old male inbred Wistar rats weighing between 200 and 250 g were used. All of the rats were purchased from KBT Oriental (Tokyo, Japan). The animals were caged individually, and their environments were maintained with a 12-h light/dark cycle. The animals used in this study received care in compliance with the Guide for the Care and Use of Laboratory Animals published by Oita University. All procedures were performed under general anesthesia combined with local anesthesia, and all efforts were made to minimize pain. During the operation, the animals were anesthetized with intraperitoneal pentobarbital (50 mg/kg) and xylazine hydrochloride (10 mg/kg). A total of 24 rats were used in this study. At 12 weeks after the operation, nerve regeneration was assessed based on clinical, histopathological, and electrophysiological evaluations. From our previous observation, we found that 12 weeks is necessary to find the difference of nerve regeneration between the groups.
The PGA–collagen tube
Nerbridge (Toyobo Co., Ltd, Osaka, Japan) is a novel PGA tube that is filled with collagen type I fibers. This product is commercially available with governmental approval for practical use in Japan. 13 The tube is biocompatible and is dissolved and absorbed in approximately 3 months. The collagen fiber used in this tube is a newly developed medical collagen (NMP Collagen PS; Nippon Meat Packers, Inc., Osaka, Japan) that is applied to the outside and inside of the conduit, which makes it easier to guide the blood vessels into the tube and thus provides a favorable environment for the regeneration and guidance of peripheral nerves. At the time of writing, this novel PGA–collagen tube is mainly used in Japan to repair peripheral sensory nerves.
The whisker pad palsy model and the transplantation of a PGA–collagen tube into a gap in the marginal branch of the facial nerve
A periauricular incision with a marginal mandibular extension was made on the left face of a rat. The buccal and marginal branches of the facial nerve were exposed. Gaps of 10 mm were created by resection of a part of the nerve into the marginal branches of the left facial nerve. To block the signal to the whisker pad, 10-mm gaps were also introduced into the buccal mandibular branch of the left facial nerve, and the proximal stump of the buccal branch was ligated with 9-0 Nylon. The left marginal branch gap was bridged with a 10-mm PGA–collagen tube. The tube was sutured with 9-0 Nylon under a surgical microscope. Two sutures were introduced on each of the distal and proximal ends of the marginal and proximal branches with a PGA–collagen tube (Figure 1).
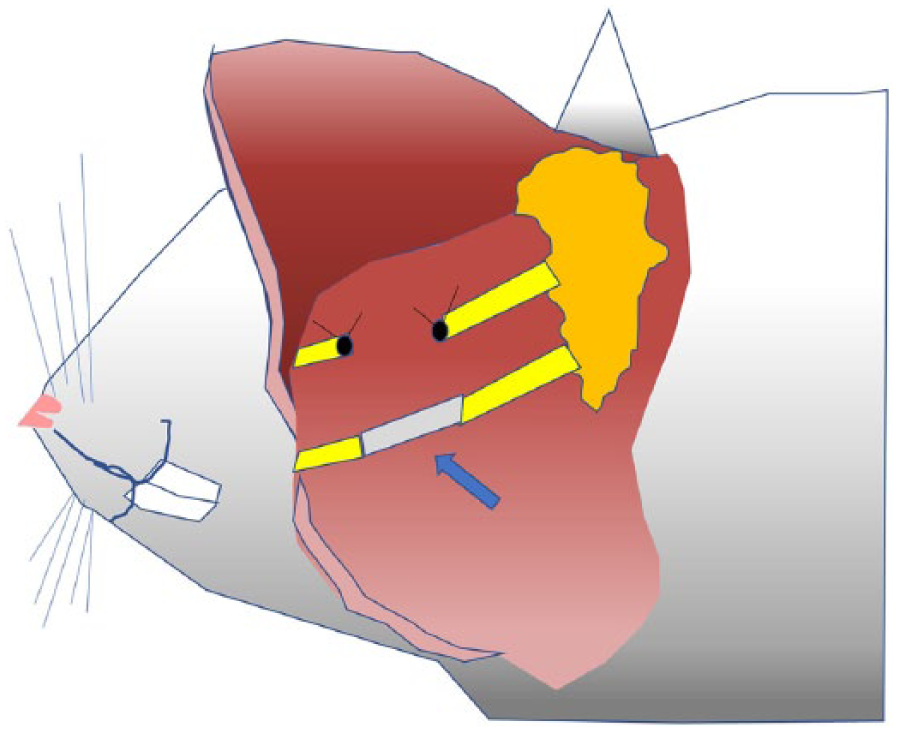
A schematic diagram of the operation. The buccal branch was removed and the proximal end was ligated. 10 mm of the marginal branch was resected and the gap was reconstructed with a PGA–collagen tube or an autograft that had been harvested from the buccal branch. Blue arrow indicates the reconstructed marginal branch.
The clinical evaluation of the recovery of facial palsy using an image analysis software program
Three groups were created for this study. In Group 1, the nerve gap was not reconstructed; this group was used as a control group (n = 8). In Group 2, the nerve gap of the marginal branch was reconstructed with a 10-mm autograft. The autograft was harvested from the buccal branch (n = 8). In Group 3, the nerve gap was reconstructed with a PGA–collagen tube, as described previously (n = 8). In each group, the whisker movement was recorded on a weekly basis using a video camera. These video files were assessed using an image analysis software program (TEMA; Photron, Tokyo, Japan). The functional recovery of the marginal branch of the facial nerve was assessed by the recovered range of motion (ROM; Figure 2).
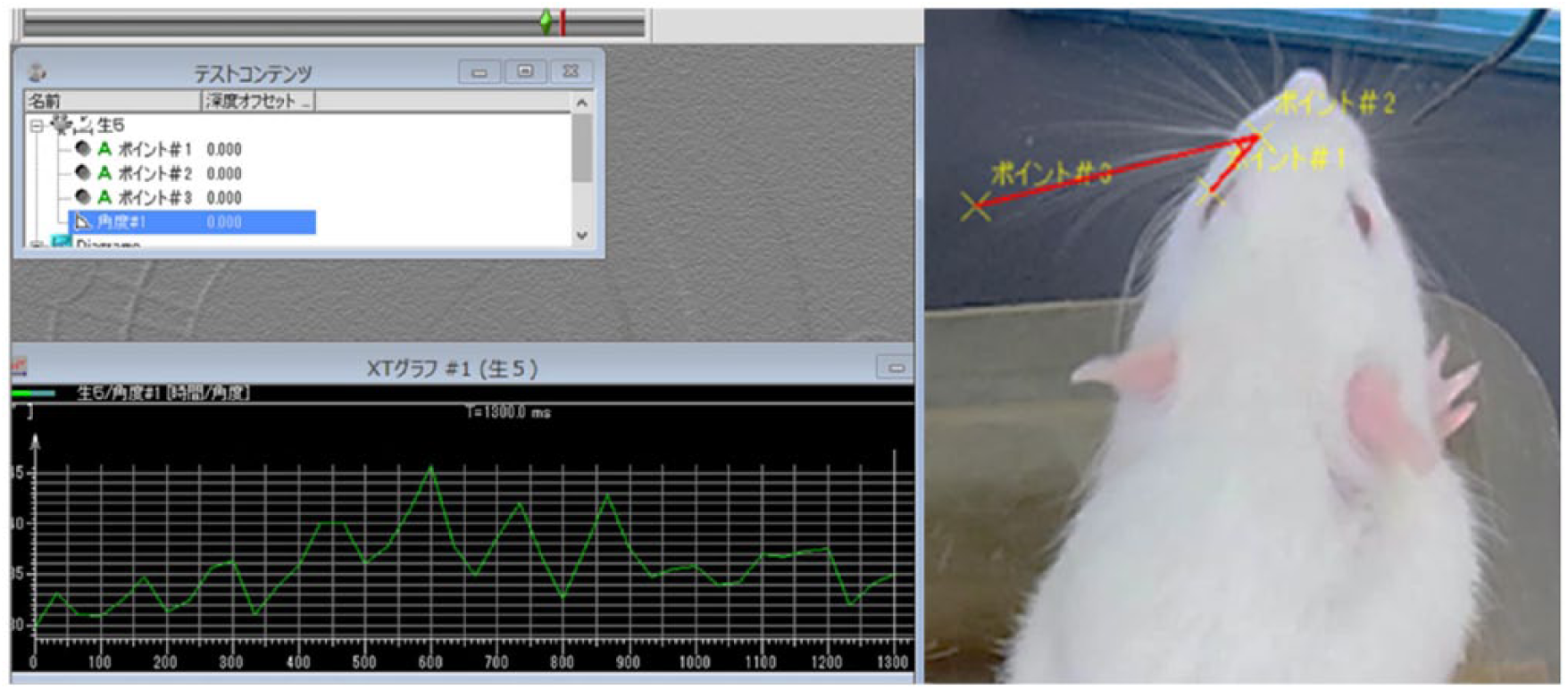
The recovery of whisker movement was assessed using an image analysis software program (TEMA; Photron, Tokyo, Japan). The range of whisker movement was measured and shown on the left of the figure.
The compound muscle action potential recordings of the vibrissal muscles in the regenerated nerve
At 12 weeks after the operation, an electrophysiological analysis of the compound muscle action potentials was conducted to compare the effect of nerve regeneration in Groups 1 (control group), 2 (autograft), and 3 (PGA–collagen tube). The compound muscle action potentials of the vibrissal muscles were recorded in each group. Electrical stimulation on both nerve types always elicited large and reliable movements of the mystacial whiskers and pads.
The histological evaluation of facial nerve regeneration
Nerve biopsies were taken from the midpoint of the reconstructed nerve at 12 weeks after the operation for a histological evaluation. To assess nerve regeneration, the number of regenerated myelinated axons of >3.5 µm diameter were counted by S-100 protein staining. The difference in the number of axons was compared between Groups 2 (autograft) and 3 (PGA–collagen tube). The myelinated fibers in the middle portion (5 mm from the proximal end) of the transplanted autograft and the regenerated nerve in the PGA–collagen tube were counted with a NanoZoomer 2.0-HT scanner (Hamamatsu Photonics, Shizuoka, Japan) and its software program (NDP.view 1.2.25; Hamamatsu Photonics, Shizuoka, Japan), and the mean number of myelinated fibers was calculated.
Statistical analysis
All of the results were expressed as mean ± standard deviation. In the clinical evaluation, the data were compared, and intergroup differences were analyzed with the unpaired t-test and multiple comparison test. The statistical analysis was performed using the GraphPad Prism 4 software program (GraphPad Software Inc., San Diego, CA, USA). p values < 0.05 were considered to indicate statistical significance.
Results
The recovery of whisker movement was observed after nerve reconstruction using the PGA–collagen tube
In Groups 1 and 2, the recovery of whisker movement was observed weekly until 12 weeks after the operation. In Group 1 (control group), the ROM recovered slightly. The average ROM of the whiskers in Group 1 (control) at 12 weeks after the operation was approximately 4.63 ± 0.51°. In Group 2 (autograft), the ROM of the whiskers recovered well. The average ROM of the whiskers in Group 2 at 12 weeks after the operation was approximately 22.75 ± 4.30°. In contrast, in Group 3 (PGA–collagen tube), the ROM recovered to 16.38 ± 3.45° (Figure 3).
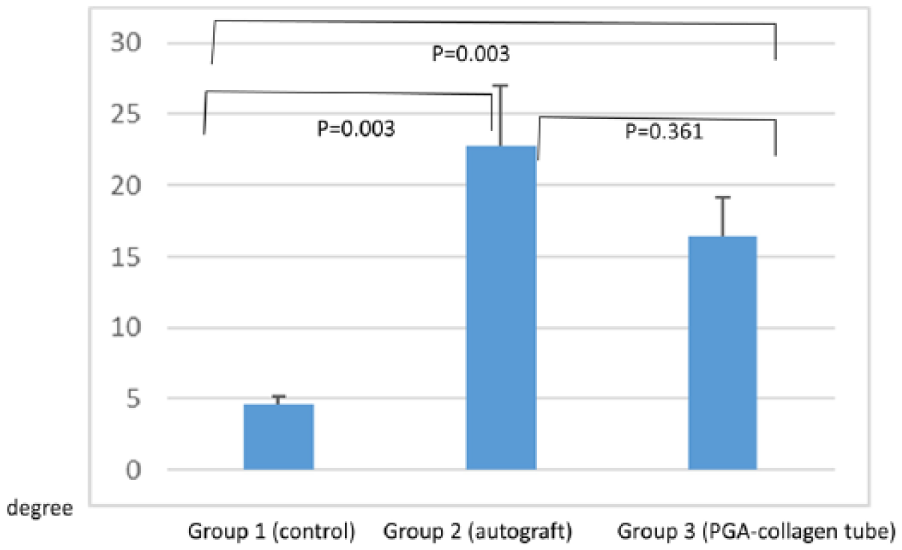
The recovery of whisker movement after nerve reconstruction using a PGA–collagen tube or an autograft. The range of whisker motion in Group 3 (PGA–collagen tube) was lower in comparison to Group 2 (autograft).
The compound muscle action potential recordings of the vibrissal muscles in regenerated nerve
An electrophysiological analysis of the compound muscle action potentials was performed to compare the nerve regeneration effect of Groups 1 (control group; n = 5), 2 (autograft; n = 5) and 3 (PGA–collagen tubes; n = 5). The compound muscle action potentials of the vibrissal muscles were recorded. The electrical stimulation of both types of nerves always elicited large and reliable movements of the mystacial whiskers and pads. The amplitudes of Groups 1(control group), 2 (autograft), and 3 (PGA–collagen tubes) were 9.86 ± 2.58, 3380.75 ± 1170.28, and 932.13 ± 39.57 µV, respectively. In this study, the electrophysiological analysis revealed that the reconstruction of the nerve gap with the PGA–collagen tube regenerated the nerve; however, the amplitude of the response was significantly lower than that observed in the group that received autograft transplantation (Figure 4).
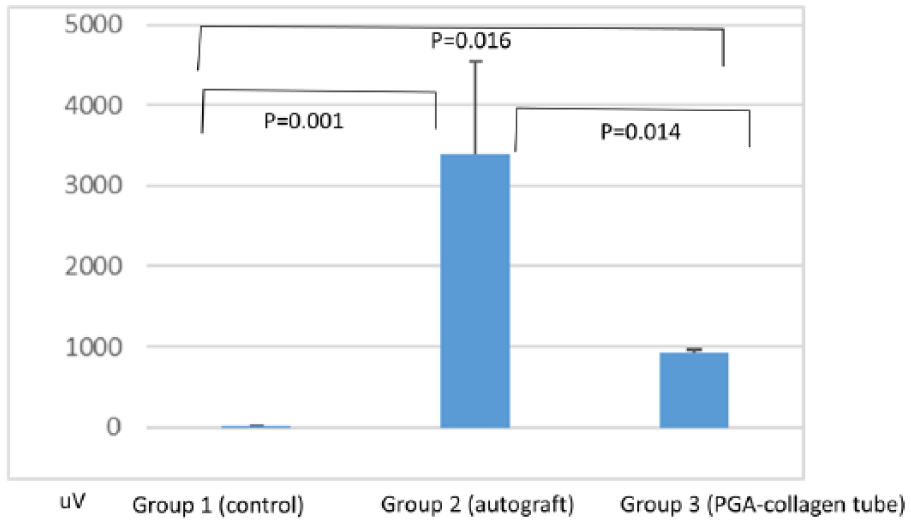
The compound muscle action potential of the whisker pad was compared among the groups. The compound muscle action potential of Group 3 (PGA–collagen tube) was higher than that of Group 1 (control), but lower than that of Group 2 (autograft).
Myelinated axonal regeneration was observed in histopathological examinations after PGA–collagen tube implantation or autograft transplantation
At 12 weeks after the operation, nerve specimens were taken from the rats in Groups 2 (autograft) and 3 (PGA–collagen tube). S-100 protein staining showed regeneration of the myelinated fibers in Groups 2 and 3 (Figures 5 and 6). In Group 2 (autograft), there were 1160.1 ± 96.3 axons of >3.5 µm diameter. In Group 3 (PGA–collagen tube), there were 319.5 ± 106.8 axons of >3.5 µm diameter; thus, fewer axons were observed in Group 3 (Figure 7).
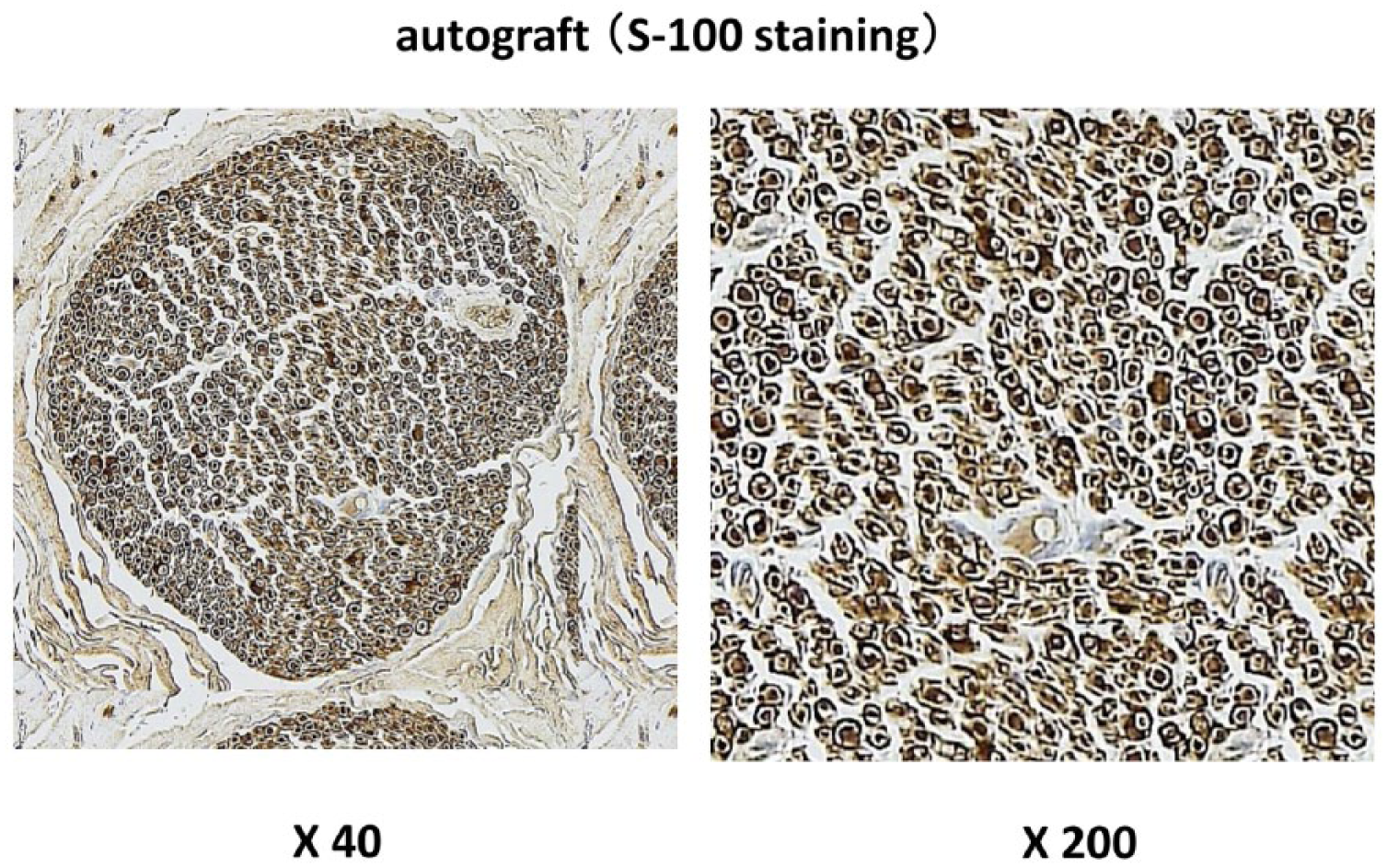
A nerve biopsy was performed at 12 weeks after the operation. The biopsy specimen was taken from the midpoint of the transplanted autograft. Myelinated axonal regeneration was observed.
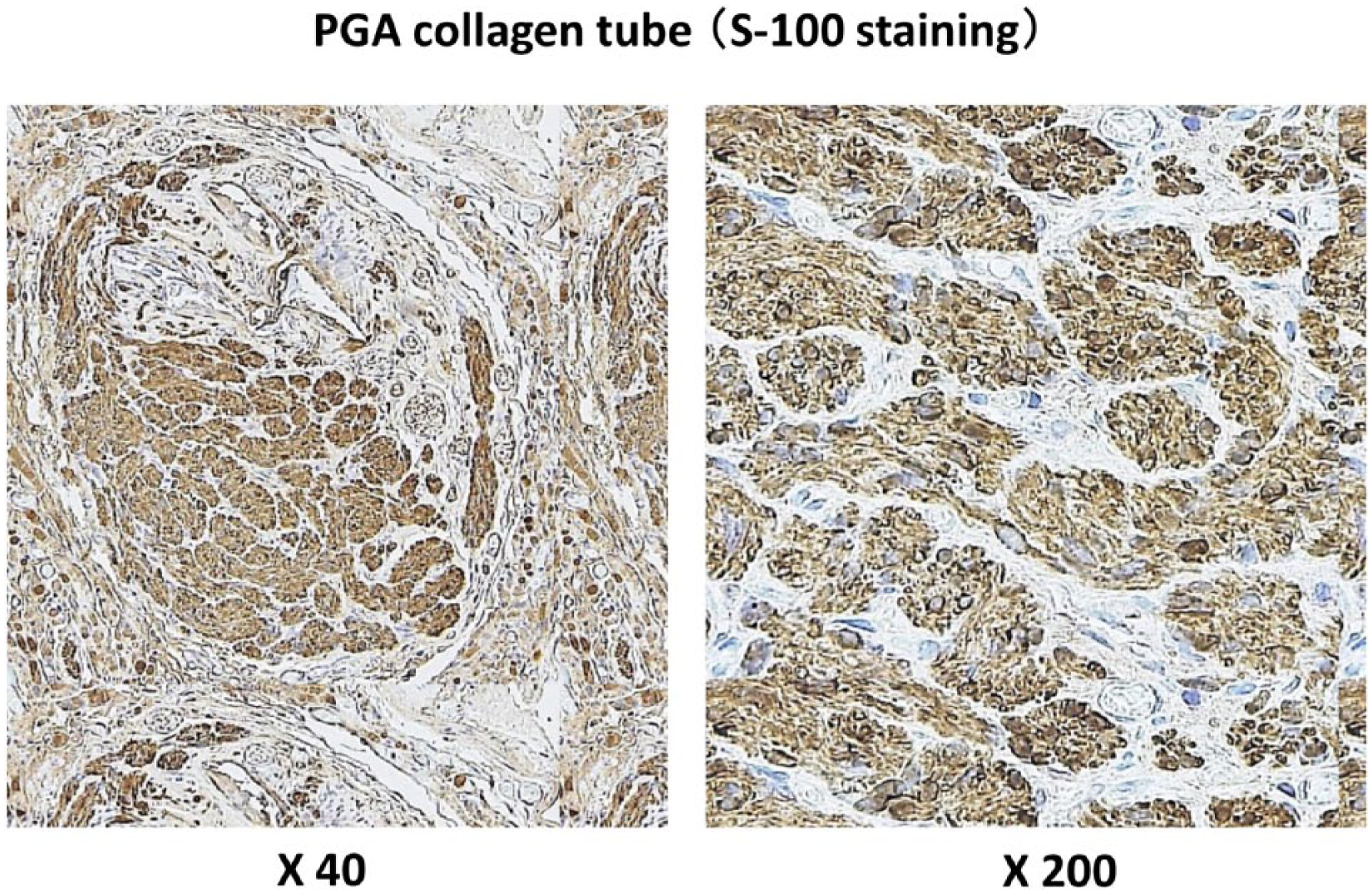
A nerve biopsy was performed at 12 weeks after the operation. The biopsy specimen was taken from the midpoint of the implanted PGA–collagen tube. Myelinated axonal regeneration was observed; however, fewer axons were observed in comparison to the autograft group. The size of the axons was also smaller in comparison to the autograft group.
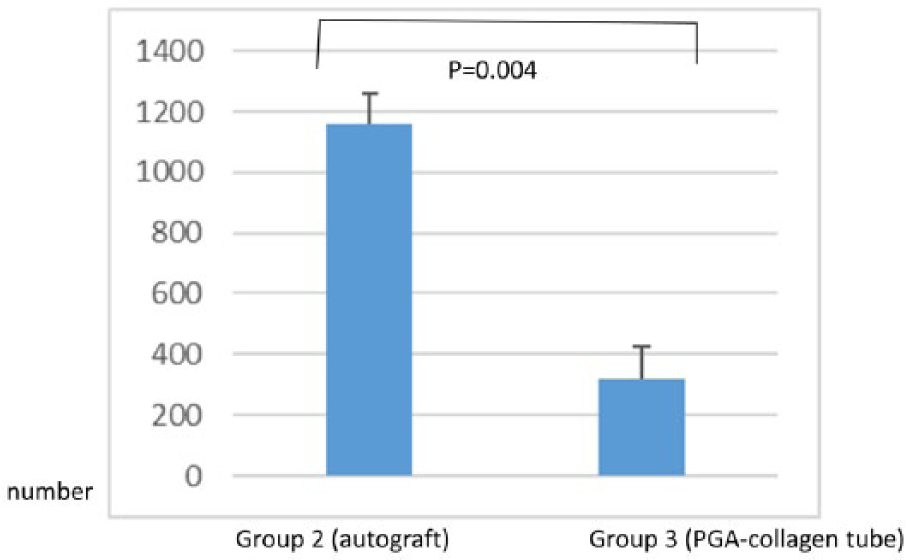
The number of myelinated axons was counted. The number of myelinated axons in Group 3 (PGA–collagen tube) was lower in comparison to that in Group 2 (autograft).
Discussion
Autologous nerve grafting has been recognized as one of the best procedures for reconstructing peripheral nerve gaps.1–3 The disadvantage of autologous nerve grafting is that the procedure causes some donor site morbidity, including pain, as well as scar formation and sensory disorders at the donor site. An ideal procedure would repair the peripheral nerve gap without any donor site morbidity. One alternative is nerve allograft transfer. Recently, Mackinnon et al. 14 reported the utility of nerve allograft, and this procedure is now widely used. Artificial nerve grafting is another potential alternative that may be used to overcome these problems. As mentioned before, there have been some studies about the development of artificial nerves and various products have been used in different countries.4–7,15 In 1970s, Lundborg reported the trial to reconstruct the nerve gap using a silicone tube. 16 In 2003, Yoshii reported the utility of a collagen-containing tube for peripheral nerve regeneration using the canine model. 17
A previous report showed the utility of PGA tubes for sensory nerve reconstruction. In 2016, Suzuki et al. 8 reported the utility of PGA tubes for reconstructing the laryngeal nerve in a rat model. However, there are no reports of its utility in the reconstruction of facial nerves.
In our study, the movement of the whisker pad was observed by clinical observation and electromyography. Furthermore, a histopathological study showed axonal regeneration at 12 weeks after the operation. However, the extent of recovery of whisker pad movement, compound muscle action potential, and axonal regeneration (as assessed by a histopathological study) were inferior in comparison to autograft reconstruction. The reason for this difference was thought to be the lack of a cellular component, including Schwann and endothelial cells. It is said that Schwann cells produce certain cytokines, including nerve growth factor (NGF) and vascular endothelial growth factor (VEGF).17–19
Several attempts have been made to improve the potential of axonal regeneration in artificial nerves.6,11,12,17–19 In 2014, Sakaki et al. 11 reported that a silicone tube containing dental pulp cells and gelatin enhanced the nerve regeneration observed by clinical evaluation and electromyography in a rat model. In 2016, Matsumine et al. 10 reported the facial nerve regeneration ability of a hybrid artificial nerve conduit containing an adipose-derived stromal vascular fraction in a rat model.
As we mentioned previously, PGA–collagen tubes have a collagen type I sponge structure inside the lumen of the PGA tube that can act as a scaffold for nerve regeneration. Furthermore, this can serve as a scaffold for cells that would be useful for nerve regeneration. 16 We therefore believe that this novel PGA–collagen tube has high potential for use in hybrid methods.
The limitation of this study is that the nerve gap was just short as 10 mm in this model. In clinical situation, the nerve gap is much longer in many cases. Further studies are necessary in a large animal model to investigate its potential in this regard.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.