
Abstract
Purpose:
Few data are available on the potential benefits and risks of red blood cell transfusion in patients undergoing extracorporeal membrane oxygenation. The aim of this study was to identify the determinants and prognosis of red blood cell transfusion in patients undergoing extracorporeal membrane oxygenation, with a special focus on biological parameters during extracorporeal membrane oxygenation treatment.
Methods:
We conducted a single-center retrospective cohort study including all consecutive patients who underwent extracorporeal membrane oxygenation between January 2010 and December 2015.
Results:
The 201 evaluated patients received a median of 0.9 [0.5–1.7] units of red blood cell per day. Significant and clinically relevant variables that best correlated with units of red blood cell transfused per day of extracorporeal membrane oxygenation were lower median daily prothrombin time in percentage (Quick) (t = –0.016, p < 0.0001), higher median daily free bilirubin level (t = 0.016, p < 0.0001), and lower pH (t = –2.434, p < 0.0001). In multivariate analysis, red blood cell transfusion was associated with a significantly higher rate of in-intensive care unit mortality (per red blood cell unit increment; adjusted odds ratio: 1.07, 95% confidence interval: 1.02–1.12, p = 0.005). It was also associated with higher rates of acute renal failure (p = 0.025), thromboembolic complications (p = 0.0045), and sepsis (p = 0.015).
Conclusion:
This study suggests that red blood cell transfusion may be associated with a higher mortality rate and with severe complications. However, we cannot conclude a direct causal relationship, as red blood cell transfusion may be only a marker of poor outcome. We recommend that physicians correct acidosis and hemolysis in patients undergoing extracorporeal membrane oxygenation whenever possible.
Introduction
Anemia is a common problem in intensive care unit (ICU), 1 especially in patients undergoing extracorporeal membrane oxygenation (ECMO).2–4 In this context, red blood cell (RBC) transfusion is often administered to improve oxygen content—and hence tissue oxygenation—and to restore adequate oxygen reserve. The beneficial effects of RBC transfusion on mortality have been demonstrated in situations such as hemorrhagic shock and severe malaria associated with respiratory failure.5,6 However, RBC transfusion is also associated with risks of alloimmunization, transfusion-related immunomodulation, transfusion-related acute lung injury, and microcirculatory dysfunction. 7 Moreover, RBC transfusion in ICU has been shown to be an independent risk factor for higher mortality, longer stay in hospital, sepsis, organ failure, and increased costs. 1 While this common treatment helps ICU patients cope with anemia, there are no guidelines for the management of RBC transfusion in ICU at present. 8
In spite of the above, few data are available on RBC transfusion in patients undergoing ECMO.2,3,9 Furthermore, bleeding and thromboembolic complications in patients receiving ECMO and anticoagulation treatment are frequent and associated with worse outcome.2,9 The aim of this study was to identify the determinants and prognosis of RBC transfusion in patients undergoing ECMO.
Materials and methods
This observational study was approved by the Institutional Review Board of the Committee of the French Intensive Care Society (No. CE SRLF17-19) and declared to the Commission nationale de l’informatique et des liberté (CNIL MR-003, No. 2000694). The need for informed consent was waived because of the observational and retrospective nature of the study.
Selection of the study sample
This observational and retrospective cohort study was conducted between January 2010 and December 2015 in a 23-bed mixed medical/surgical ICU of a French university hospital.
All ICU patients who underwent ECMO during this period were consecutively evaluated. The exclusion criteria were age <18 years old and duration of ECMO <2 days.
Anticoagulation management
Anticoagulation was performed with intravenous unfractionated heparin (IVUH) in all patients undergoing ECMO according to a standardized protocol. Anticoagulation efficacy was defined by an activated partial thromboplastin time (aPTT) ratio between 2 and 3. aPTT was checked 6 h after modification of the IVUH dose.
Following postcardiotomy or surgical bleeding, IVUH was started on the sixth postoperative hour in the absence of bleeding.
RBC transfusion was usually performed to maintain a hemoglobin level above 7 g/dL.
Prophylactic blood products were not routinely given to treat coagulation abnormalities. In the case of bleeding, platelet bags were administered to maintain a platelet count ⩾70 g/L, fresh frozen plasma to maintain prothrombin time in percentage (Quick) >50%, and fibrinogen concentrate to maintain fibrinogen plasma concentration ⩾1.5 g/L.
Data collection
The usual comorbidities were recorded at ICU admission. We also recorded the median daily values of the following biological parameters for each day of ECMO treatment: hemoglobin level, nadir hemoglobin (defined as the hemoglobin value prior to first RBC transfusion, or as the lowest hemoglobin value during ECMO in patients without RBC transfusion), platelet count, aPPT, prothrombin time in percentage (Quick), fibrinogen level, plasma urea level, free bilirubin level, and total bilirubin level.
Outcome measurements
The primary aim of the study was to evaluate the determinants of RBC transfusion in patients undergoing ECMO.
The secondary aim was to determine whether RBC transfusion was associated with increased in-ICU mortality.
We also collected data on severe morbid complications: thromboembolic event during stay in ICU, major bleeding event during ECMO, severe sepsis or septic shock during stay in ICU, and acute renal failure requiring renal replacement therapy during stay in ICU.
Thromboembolic event was defined as transient ischemic attack, ischemic stroke, systemic embolism, acute myocardial infarction, intracardiac thrombosis, deep venous thrombosis, pulmonary embolism, and circuit/membrane oxygenator change due to thrombus formation.
Major bleeding was defined according to the criteria of the Extracorporeal Life Support Organization: 10 bleeding responsible for death, intracranial bleeding, bleeding requiring hemostatic procedure (surgery, embolization, or gastroscopy), or bleeding associated with administration ⩾2 RBC units in 24 h.
Severe sepsis was defined as sepsis with sepsis-induced organ dysfunction or tissue hypo-perfusion, and septic shock was defined as sepsis-induced hypotension persisting despite fluid resuscitation. 11
Statistical analysis
Results were expressed as total number (percentage) for categorical variables and as median [25th–75th percentiles] or mean ± standard deviation (SD) for continuous variables, as appropriate. Continuous variables were compared using the Mann–Whitney U test or the Kruskal–Wallis test, as appropriate. Categorical variables were compared using chi-square test or Fisher’s exact test, as appropriate. Spearman’s rank correlation coefficient analysis was performed to assess the correlation between units of RBC transfused per day of ECMO and continuous variables. The variables independently correlating with units of RBC transfused per day with p < 0.1 were then entered into multiple multivariate logistic regression analyses. Furthermore, risk factors for in-hospital mortality with p < 0.1 in bivariate analysis were entered into a multivariate logistic regression analysis using backward selection with p < 0.05. Collinearity between independent risk factors was tested; when collinearity was identified between two risk factors, the most clinically relevant factor was selected to construct the multivariate models. A p value < 0.05 was considered significant. Analyses were performed using SAS statistical software (8.2, Cary, NC, USA).
Results
Study population
Over the study period, 4878 patients were hospitalized, of whom 242 (5%) underwent ECMO. Among these 242 patients, 41 were excluded (9 were <18 years old, and 32 received ECMO <2 days). The remaining 201 patients formed the cohort of this study.
Patient characteristics at ICU admission and study inclusion are shown in Tables 1 and 2.
Clinical characteristics at admission.
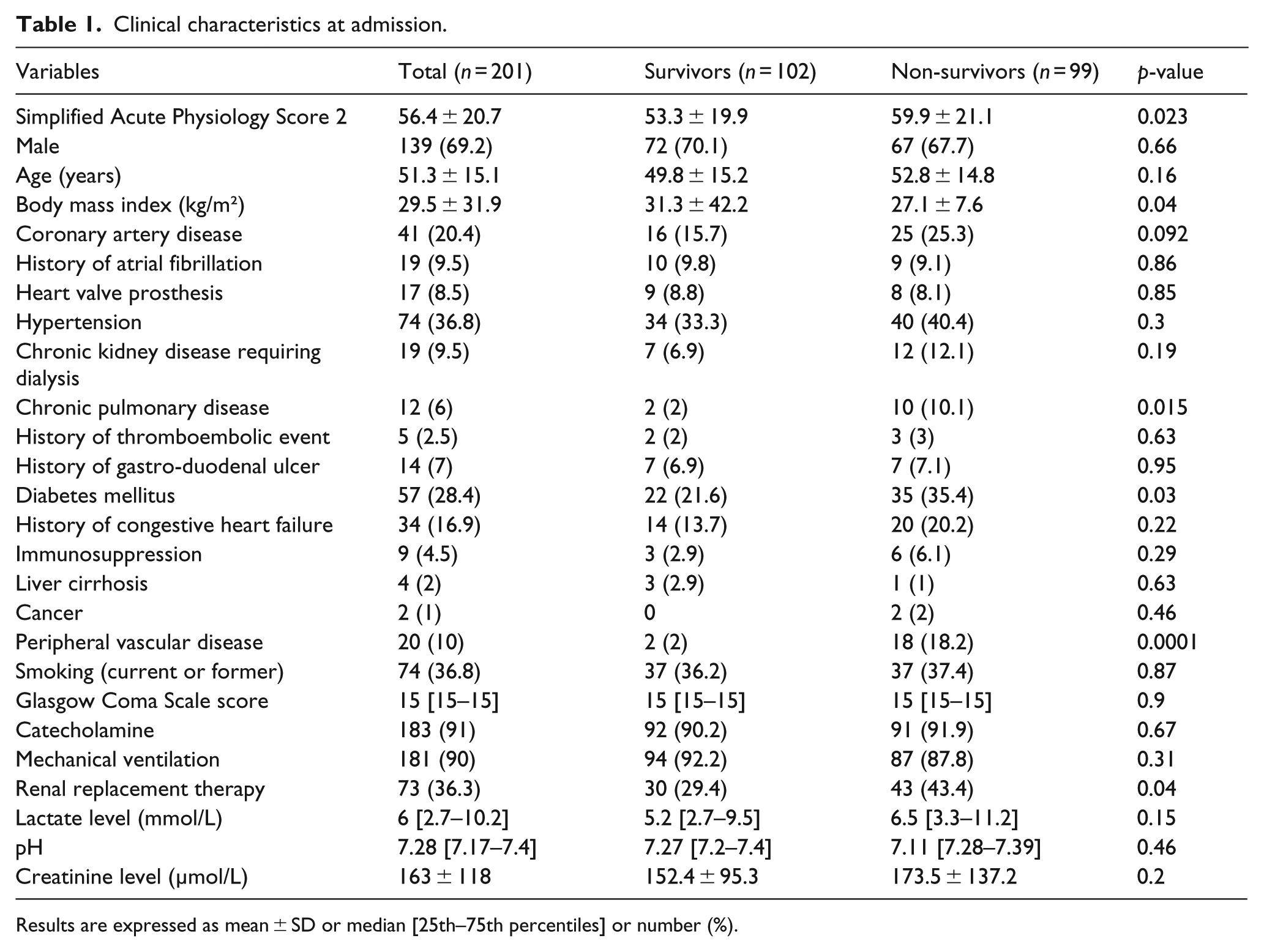
Results are expressed as mean ± SD or median [25th–75th percentiles] or number (%).
Clinical and biological parameters during ECMO treatment.
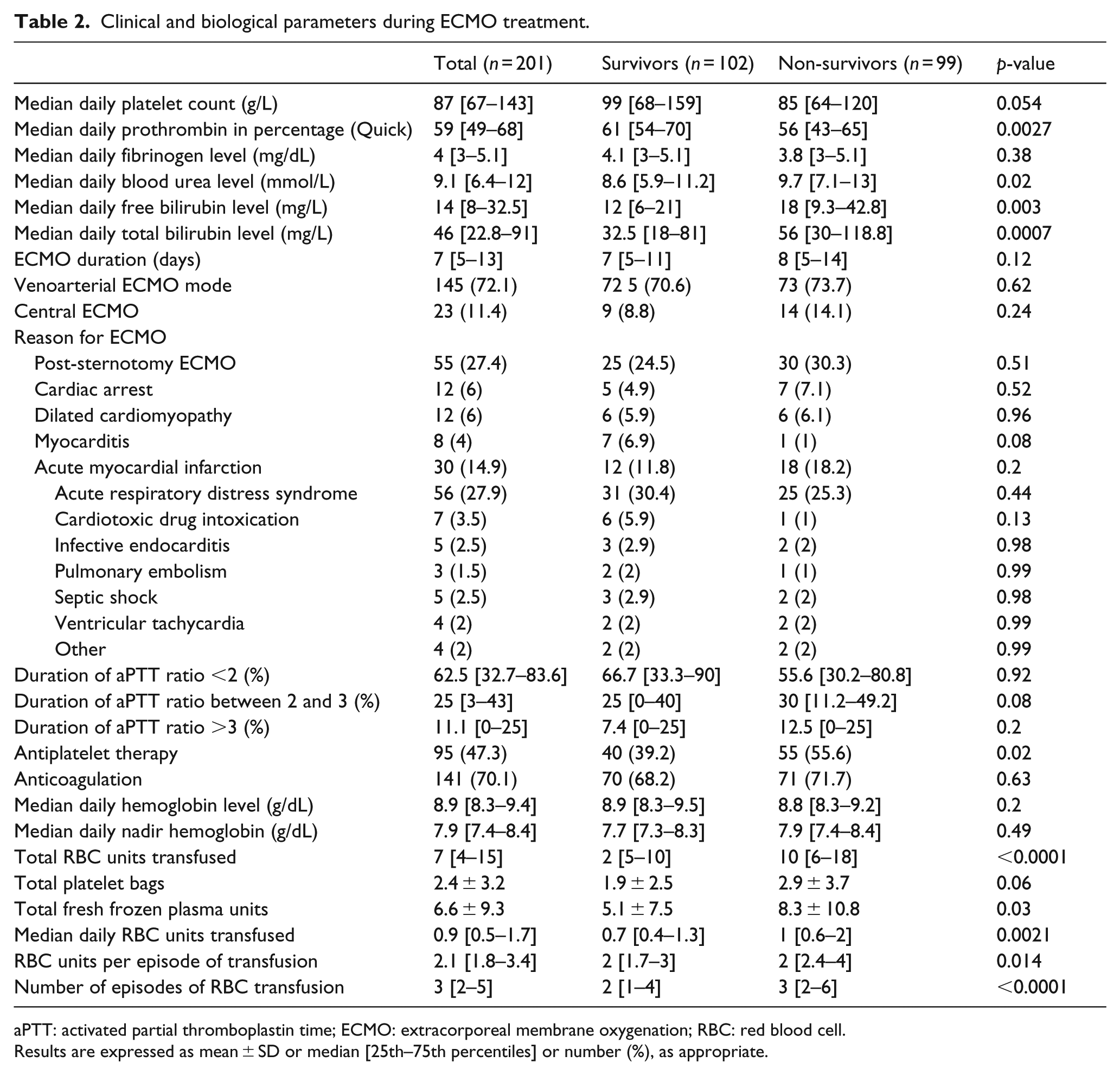
aPTT: activated partial thromboplastin time; ECMO: extracorporeal membrane oxygenation; RBC: red blood cell.
Results are expressed as mean ± SD or median [25th–75th percentiles] or number (%), as appropriate.
Mean age was 51.3 ± 15.1 years old, and mean Simplified Acute Physiology score 2 at admission was 56 ± 21 (Table 2).
A total of 145 patients (72.1%) received venoarterial ECMO. The main indications for ECMO were acute respiratory distress syndrome in 56 cases (27.8%) and cardiogenic shock following post-cardiotomy in 55 cases (27.4%).
Determinants of RBC transfusion
During a median of 7 [5–12.3] days of ECMO support, 0.9 [0.5–1.7] units of RBC were transfused each day. A total of 15 patients did not receive RBC transfusion (7.5%) during ECMO support.
The factors associated in univariate analysis with units of RBC transfused per day of ECMO with a p-value less than 0.1 are shown in Tables 3 and 4.
Clinical characteristics at admission correlating with units of red blood cell transfused per day of ECMO.
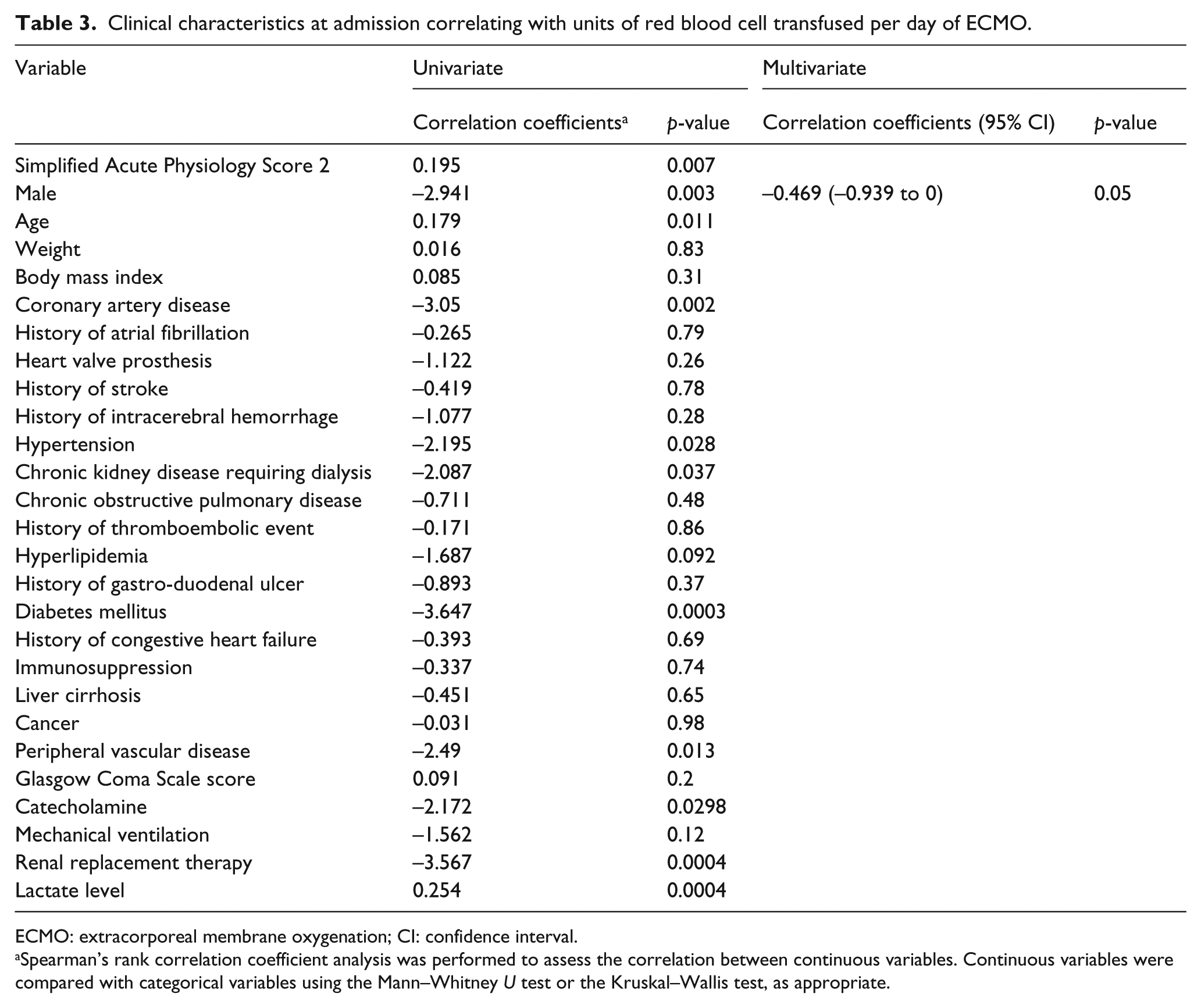
ECMO: extracorporeal membrane oxygenation; CI: confidence interval.
Spearman’s rank correlation coefficient analysis was performed to assess the correlation between continuous variables. Continuous variables were compared with categorical variables using the Mann–Whitney U test or the Kruskal–Wallis test, as appropriate.
Clinical, biological, and hemostasis parameters correlating with units of red blood cell transfused per day of ECMO.
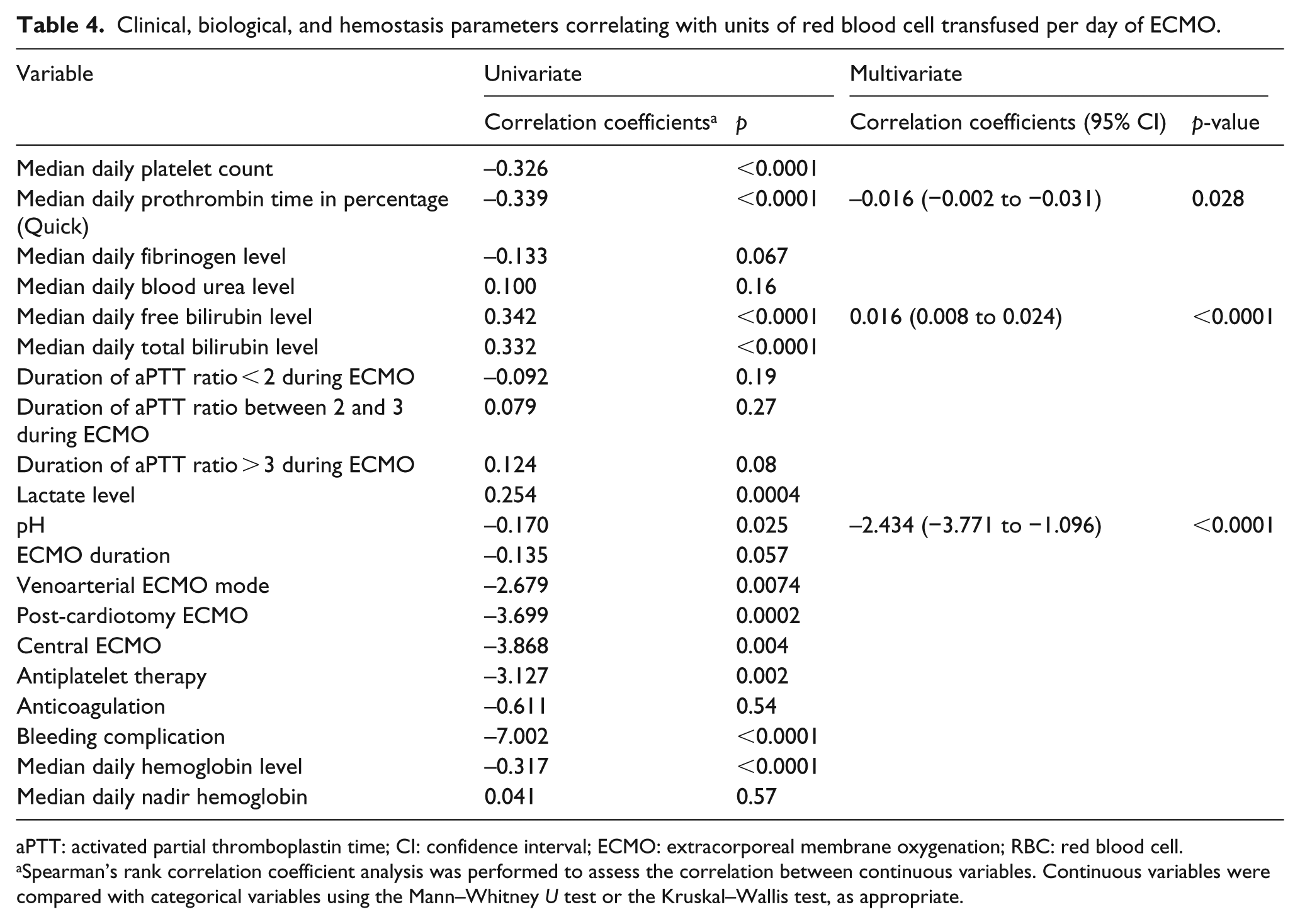
aPTT: activated partial thromboplastin time; CI: confidence interval; ECMO: extracorporeal membrane oxygenation; RBC: red blood cell.
Spearman’s rank correlation coefficient analysis was performed to assess the correlation between continuous variables. Continuous variables were compared with categorical variables using the Mann–Whitney U test or the Kruskal–Wallis test, as appropriate.
In multiple multivariate analyses, units of RBC transfused per day of ECMO were independently associated with lower median daily prothrombin time in percentage (Quick; t = –0.016, p < 0.0001), higher median daily bilirubin level (t = 0.016, p < 0.0001), and lower pH (t = –2.434, p < 0.0001) during ECMO support (Table 4).
In-ICU mortality
The in-ICU mortality rate was 49.3%. Univariate analysis revealed that RBC transfusion was associated with increased in-ICU mortality (the median number of units of RBC transfused per day was 0.7 [0.4–1.3] in survivors and 1 [0.6–2] in non-survivors, p = 0.002). Major bleeding complication was also associated with increased in-ICU mortality (62.4% vs 38%, p = 0.001). The other risk factors found to be predictive of in-hospital mortality (based on bivariate analysis with p < 0.1) are shown in Tables 1 and 2.
In multivariate analysis, in-hospital mortality was independently associated with RBC transfusion (per RBC unit increment; odds ratio (OR): 1.07; 95% confidence interval (CI): 1.02–1.12, p = 0.025) and peripheral vascular disease (OR: 11.4; 95% CI: 1.3–102.8, p = 0.03; Table 5). The Hosmer–Lemeshow goodness-of-fit test showed good calibration of the model (p = 0.703). The Nagelkerke and Cox/Snell R2 were 0.360 and 0.268, respectively.
Multivariate analysis of risk factors for in-ICU mortality.
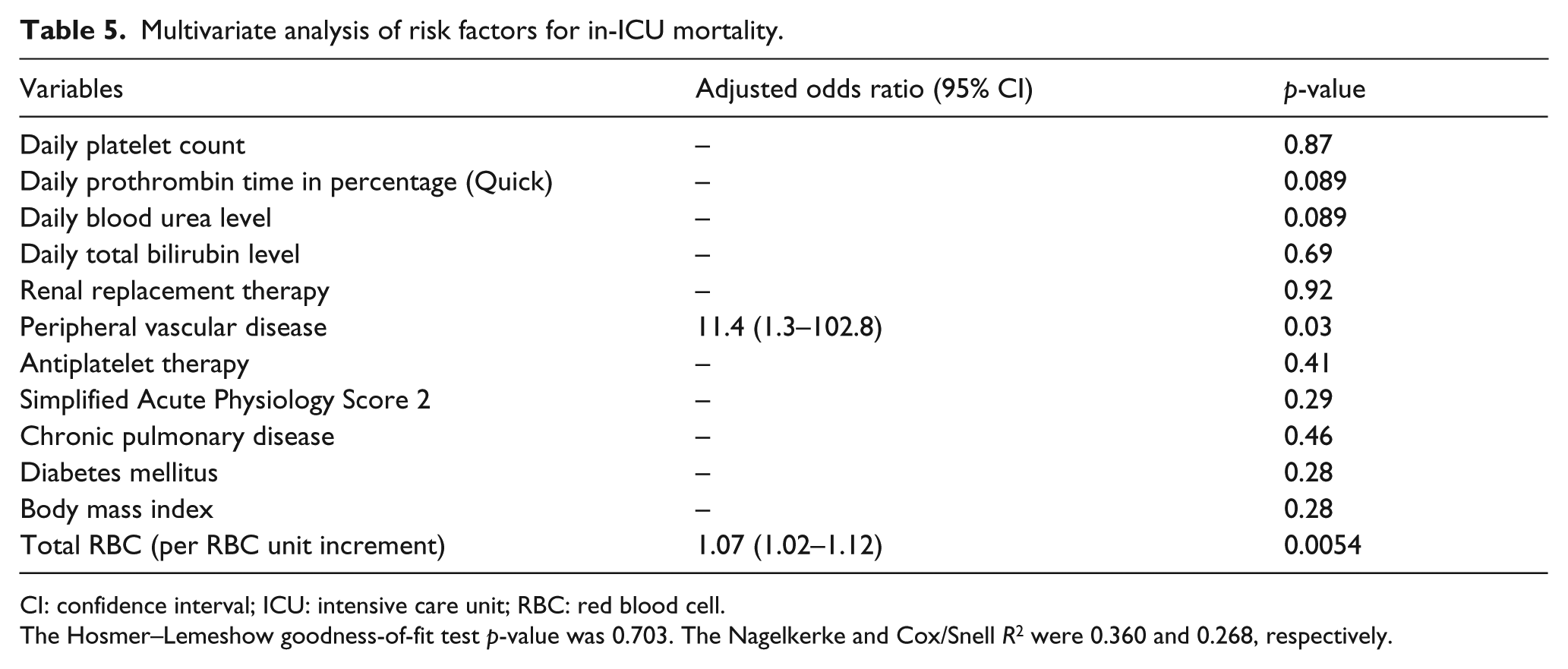
CI: confidence interval; ICU: intensive care unit; RBC: red blood cell.
The Hosmer–Lemeshow goodness-of-fit test p-value was 0.703. The Nagelkerke and Cox/Snell R2 were 0.360 and 0.268, respectively.
Severe morbidity
A total of 93 patients (46.3%) had ⩾1 major bleeding complication during ECMO support: 42 had bleeding from the ECMO cannula; 24 had bleeding from ear, nose, and throat; 15 had pericardial effusions or cardiac tamponade requiring surgery; 9 had hemoptysis; and 9 had intracranial hemorrhages.
Patients with major bleeding complications had higher units of RBC transfused per day of ECMO (1.4 [0.8–2.4] vs 0.6 [0.3–1], p < 0.0001).
Following univariate analysis, patients with major bleeding complications had a higher rate of thromboembolic complications (29% vs 13%, p = 0.008) and a higher rate of acute renal failure requiring renal replacement therapy (62.4% vs 45.4%, p = 0.025). No statistically significant difference in rate of severe sepsis was observed in univariate analysis between patients with major bleeding complications (58.1%) and patients without major bleeding complications (44.4%, p = 0.07).
A total of 48 patients (23.9%) had ⩾1 thromboembolic event during their stay in ICU: 7 had an ischemic stroke, 11 had acute lower limb ischemia with thrombus, 12 had a circuit/membrane oxygenator change due to thrombus formation, 11 had intracardiac thrombus, 12 had inferior vena cava thrombus, and 8 had internal jugular vein thrombus.
In univariate analysis, RBC transfusion was associated with higher rates of thromboembolic complications (p = 0.0045), acute renal failure requiring renal replacement therapy (p = 0.025), and severe sepsis (p = 0.015).
Discussion
The main findings of our study are as follows: (1) the factors that correlated best with units of RBC transfused per day of ECMO were lower daily prothrombin time in percentage (Quick), higher daily free bilirubin level, and lower pH; and (2) RBC transfusion was associated with in-ICU mortality.
Few studies have evaluated the risk factors for RBC transfusion or for bleeding complications in patients undergoing ECMO. In a study evaluating 40 patients undergoing ECMO, Tauber et al. 3 found, as we did, that lower prothrombin time in percentage (Quick) significantly increases transfusion requirements. They also noted that impaired platelet function and increased creatinine level were associated with higher transfusion requirements. In the study by Aubron et al. 2 assessing the risk factors for bleeding complications in patients undergoing ECMO, higher aPTT was associated with bleeding complications in multivariate analysis. Similarly, in the study by Yeo et al. 4 evaluating 71 patients with ECMO, univariate analysis revealed that rates of major bleeding complications were higher in patients with conventional activated clotting time (between 180 and 220 s) than in patients with lower activated clotting time (between 140 and 160 s; p < 0.0001). In addition, daily RBC transfusion requirements were found to be lower in the conventional aPTT group than in the lower aPTT group (2.7 RBC units per day vs 1.3, p = 0.011). In this study, however, the number of patients was quite low and no multivariate analysis was performed.
In our study, a higher aPTT ratio was associated with a higher number of RBC units transfused per day of ECMO in univariate analysis but not in multivariate analysis. This could be due to a lack of power or the fact that few of our patients had a high aPTT ratio. Moreover, we found that higher free bilirubin level during ECMO was associated with a higher number of RBC units transfused. Free bilirubin level might be a marker of hemolysis, which could explain why we found a correlation between daily free bilirubin level and units of RBC transfused per day of ECMO. Note, however, that free bilirubin level was significantly higher in non-survivors than in survivors. This may suggest that hemolysis triggered transfusion and that free bilirubin level is a determinant of outcome rather than a surrogate marker of RBC transfusion. It has been recommended that physicians should screen patients with ECMO for hemolysis and that they should prevent risk factors for technical-induced hemolysis—for instance, by avoiding using high-flow velocity through small cannulas and by replacing the pump head if necessary (if it is partially clotted). 12 In our study, we found that lower pH and lower prothrombin time in percentage (Quick) were associated with a higher number of RBC units transfused. In the study by Shenkman et al., 13 metabolic acidosis was a risk factor for clot formation and impaired platelet function; moreover, it was associated with systemic disseminated intravascular coagulation. 14 In clinical practice, acidosis has been shown to be an independent risk factor for RBC transfusion. 15 However, the association between prothrombin time in percentage (Quick) and the number of RBC units transfused is difficult to interpret because patients received a large number of total fresh frozen plasma units during ECMO support (6.6 ± 9.3).
A number of studies suggest that RBC transfusion is an independent risk factor for higher mortality. In a multicenter study involving 146 hospitals and 3534 ICU patients, Vincent et al. 1 found that RBC was an independent risk factor for higher 28-day mortality (OR: 1.37, 95% CI: 1.02–1.84). In a study including only ECMO patients, Aubron et al. 2 showed that bleeding complication was an independent risk factor for higher in-hospital mortality (adjusted hazard ratio: 2.17, 95% CI: 1.07–4.41, p = 0.03); however, they did not evaluate the impact of RBC transfusion on mortality. In their study of RBC transfusion in patients undergoing ECMO, Tauber et al. 3 also failed to investigate the impact of RBC transfusion on mortality.
In univariate analysis, we found that RBC transfusion was associated with severe complications such as severe sepsis, thromboembolic event, and acute renal failure. Similarly, previous studies have suggested that RBC transfusion in ICU is an independent risk factor for nosocomial infection,16,17 renal failure,18,19 and thrombotic event.20,21
In order to limit RBC transfusion and its associated mortality, morbidity, and increased costs, it is necessary to develop the optimal transfusion strategy. In this perspective, many randomized controlled clinical trials in ICU have found that a restrictive RBC transfusion strategy was non-inferior to a liberal RBC transfusion strategy.22–25 Moreover, it has been suggested by Agerstrand et al. 26 that implementation of an RBC conservation protocol in patients undergoing ECMO for acute respiratory distress syndrome was associated with lower transfusion requirements without an increase in in-hospital mortality.
Studies are now needed to compare anticoagulation regimens in this context with those applied in the context of heart valve disease. 27
Physicians should nevertheless keep in mind that the indication and thresholds for RBC transfusion may differ significantly between patients, conditions, type of ECMO, and situations. RBC transfusion should be adapted to each situation and to the tolerance of each patient (oxygen content, tissue oxygenation, oxygen reserve, etc.).
Our study presents a number of limitations. The retrospective nature of the analysis is clearly a weakness. Another limitation is a possible lack of power due to the relatively low number of patients and events evaluated. Our study population may be considered small; yet, to our knowledge, this is the largest cohort for whom the impact of certain biological variables was assessed on each day of ECMO support and RBC transfusion. The studies by Aubron et al., 2 Tauber et al., 3 and Yeo et al. 4 evaluated 40 patients, 147 patients, and 71 patients, respectively, and they investigated biological parameters at few time points. Other limitations of our study are worth noting: coagulation parameters during ECMO were not analyzed with rotational thromboelastometry, free hemoglobin was not routinely available at our center, and data on transfusion efficacy (post-transfusion Hb level or central venous oxygen, etc.) were not collected. Patients with venoarterial ECMO (including postcardiotomy and central ECMO) and venovenous ECMO were combined for analysis, as was the case in the studies by Aubron et al., 2 Tauber et al., 3 and Yeo et al. 4 This could be viewed as a major limitation of our study. However, the mean Simplified Acute Physiology Score 2 and the mortality rate did not differ between groups of patients; moreover, venoarterial ECMO, postcardiotomy ECMO, and central ECMO were not associated with higher units of RBC transfusion per day of ECMO in multivariate analysis. Finally, RBC transfusion was performed to treat anemia due to bleeding complications in several cases (46%), suggesting that RBC transfusion is merely a marker of bleeding complication.
In multivariate analysis, RBC transfusion was associated with a higher mortality rate. Yet this analysis may have presented a bias related to the use of covariates, as RBC transfusion was more common in patients with altered coagulation and acidosis. This suggests that RBC transfusion was more common in patients with multiple organ failure, which may explain why their mortality rate was higher.
Insofar as our study was not a randomized controlled trial comparing different RBC transfusion regimens, we cannot conclude a direct causal relationship between RBC transfusion and higher mortality or severe complications. Nevertheless, our assessment of the impact of RBC transfusion on mortality in patients undergoing ECMO is one of the first steps for launching an impact study. 28 In order to limit biases caused by the absence of randomization, we did not use a propensity matching score because our study sample was too small. It has indeed been shown that there is limited interest in performing a propensity score analysis in a study like ours.29,30 Yet, given that RBC transfusion is very common in ICU and that it is associated with well-known and severe side effects, analyzing the risk factors for RBC transfusion seems to us essential.
Conclusion
In our study, lower prothrombin time in percentage (Quick), higher free bilirubin level, and lower pH correlated best with units of RBC transfused per day of ECMO. Moreover, RBC transfusion in patients undergoing ECMO was very common (92.5%), as was the case in the study by Tauber et al. 3 (100%). We also found RBC transfusion to be associated with a higher mortality rate. However, we cannot conclude a direct causal relationship, as RBC transfusion may be only a marker of poor outcome. Prospective randomized studies are needed to determine the best anticoagulation and clinical regimen in patients undergoing ECMO and to assess the best strategy for RBC transfusion in this setting. We recommend that physicians correct acidosis and hemolysis in patients undergoing ECMO whenever possible.
Footnotes
Acknowledgements
N.A. and H.L.P. had full access to the study data and take responsibility for the integrity of the data and the accuracy of the data analysis. N.A., J.A., B.B., and H.L.P. contributed to study concept and design. H.L.P., N.A., B.B., R.P., O.M., C.B., D.V., B.D., L.D., G.B., and E.B. contributed to acquisition of data. N.A., J.A., H.L.P., R.P., O.M., C.B., D.V., B.D., L.D., and E.B. contributed to analysis and interpretation of data. N.A. and J.A. contributed to drafting of the manuscript. N.A., J.A., H.L.P., R.P., O.M., C.B., D.V., B.D., L.D., B.B., and E.B. contributed to critical revision of the manuscript for important intellectual content. J.A. and N.A. contributed to statistical analysis. N.A. and J.A. contributed to administrative, technical, or material support. N.A., J.A., B.B., and L.D. contributed to study supervision.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This observational study was approved by the Institutional Review Board of the Committee of the French Intensive Care Society (No. CE SRLF17-19) and was declared to the Commission nationale de l’informatique et des liberté (CNIL MR-003, No. 2000694).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Support was obtained solely from institutional and/or departmental sources. This work was internally funded.
Informed consent
The requirement for informed consent was waived given the retrospective nature of the study.