
Abstract
Introduction:
Pump thrombosis of left ventricular assist devices remains a devastating complication with high morbidity and mortality. Despite the improvements made, the matter affects many patients and the treatment options are limited to thrombolysis and surgical replacement. An alternative approach using the aspiration Indigo catheter was tested.
Methods:
An Indigo thrombectomy catheter was used within an in vitro model to assess the direct aspiration of prefabricated clots from three different positions within the HeartWare HVAD (inlet, outlet, and housing). The experiments were conducted with a straight and an angled catheter. The aspiration pressure was constant. The flow, power consumption, and pressure head of the left ventricular assist devices were measured at pre-defined measuring points.
Results:
The device was more effective (success rate 71%) at inlet and outlet of the left ventricular assist device. In addition, the duration of aspiration and the aspiration volume were shorter in comparison to the aspiration in the housing (inlet M = 19.75 s, outlet M = 60.50 s, and housing M = 38.75 s). Moreover, the aspiration volume was associated with the aspiration duration and the weight of thrombi but not with their volume. Noteworthy, the angled catheter showed an improved performance compared to the straight one (67%–33%). The recorded parameters showed no major changes during the use of the catheter. After application of the Indigo catheter, flow and pressure head of the pump could be restored.
Conclusions:
The aspiration system showed promising results under specific conditions for the treatment of pump thrombosis in an in vitro model. However, further examination, including in vivo experiments, will justify its effectiveness.
Keywords
Introduction
Over the last years, left ventricular assist devices (LVAD) have been established as a therapeutical option in patients with end-stage heart failure. 1 Implantation of a continuous-flow LVAD reduces mortality and improves the quality of life. 2 In addition, an LVAD can be implanted as a bridge to transplantation in eligible patients for heart transplant to improve end-organ function and physical capacity. 3 However, LVAD devices are associated with adverse events 2 including bleeding, infection, stroke, hemorrhagic complications, right ventricular failure, and pump thrombosis (PT).3,4 The incidence of PT in adult patients with a continuous-flow device is 2%–13% and 2% with centrifugal flow. 1
Apart from the cost-intensive and hazardous device replacement, the pharmacological treatment (thrombolysis) remains the only available treatment strategy. However, high rate of stroke and mortality as well as low technical success rate remain important limitations of the technique.
The aim of this study was to investigate the use of percutaneous transluminal aspiration mechanical thrombectomy as an alternative, minimally invasive, potential treatment for LVAD thrombosis in an experimental model for the first time in the literature.
Methods
Thrombus production
Two series of experiments with different thrombi size and positions were conducted. In all, 16 S-Monovettes® (Sarstedt, Nümbrecht, Germany) with human blood from healthy donors were provided from the blood transfusion department of Hannover Medical School. A volume of 340 μL of citrated blood (sodium citrate 3.2%, 0.105 M) was recalcified with 20 μL of 0.2 M CaCl2. 5 This ratio was maintained and adapted to larger volumes to produce red stagnation thrombi, which do not contain a structured fibrin net.
For the first experimental set (small-volume thrombus test), blood from 10 monovettes was transferred with a pipette (Eppendorf AG, Hamburg, Germany) into 20 reaction vessels. A total of 20 thrombi were produced from 4.1 mL of blood and 250 μL of calcium chloride. For the second experimental set (large-volume thrombus test), six monovettes containing 8.2 mL whole blood were recalcified with 500 μL calcium chloride. Monovettes with a diameter of 15 mm (thrombi outflow graft) and 16 mm (thrombi inflow cannula and pump housing) were used as reaction vessels for thrombus production.
The reaction vessels were heated up to reach a temperature above 30°C to a maximum of 32°C for 1 h. Vessels with formed thrombi were stored at room temperature for the first 24 h and then at 5°C for 96 h. The storage in blood and calcium chloride promoted a stabilization of the thrombus formation. The size of the thrombi was determined by their volume and weight. The weight was measured with a digital scale and their volume was determined by the displaced volume within a measuring cylinder. Thereafter, the thrombi were stored in phosphate-buffered saline solution to maintain a constant pH.
Indigo® aspiration mechanical system
The Indigo® aspiration mechanical system set (Penumbra, Inc., Alameda, CA, USA) consists of a vacuum-assisted pump (Pump MAX™) which can be connected to the Indigo catheter. There are many catheter types regarding either the configuration (straight or angled) or the size. The catheter can be inserted at the upper or lower extremities on both arterial and venous system. Complimentary, a separator can be used for the fragmentation of the thrombi in order to maximize the effectivity and the aspiration power and to prevent clogging of the aspiration tip. Through its atraumatic profile with a soft tip, the Indigo catheter has flexibility and can also be used without a guide wire. Specifically, the angled catheter with the longest tip length (XTorq) provides a circumferential aspiration for vessels up to 25.4 mm. For the small-volume thrombus tests, the angled Indigo catheter was used (CAT8 XTorq, 8F), while for the large-volume thrombus tests, saw the use of a straight one (CAT8, 8F). A separator (SEP8) was used in all experiments.
Experimental setup
Figure 1 shows the schematic experimental setup of the in vitro model. The mock circulation loop represents the left ventricle and the systemic circulation, with silicone tubes modeling the inlet (1/2″) and outlet (3/8″) cannula. The Indigo catheter can be inserted through an introducer sheath (8F), located in Y-connectors representing the venous and arterial side. An explanted HVAD® (HeartWare Inc., Framingham, MA, USA) was put into operation with a typical speed known from clinical practice (2500 r/min). The whole system was filled with 42% glycerin solution, which possesses blood-like viscosity and hence flow conditions. To avoid any damage of the Indigo catheter, the thrombi were aspirated from the pump housing, while the VAD was switched off. The thrombus positioned in the pump housing mimics a thrombus suctioned from the left atrium or left ventricle into the pump components. There was no need to fixate the thrombi inside the pump housing. The thrombus was introduced into the pump housing through the inlet cannula.
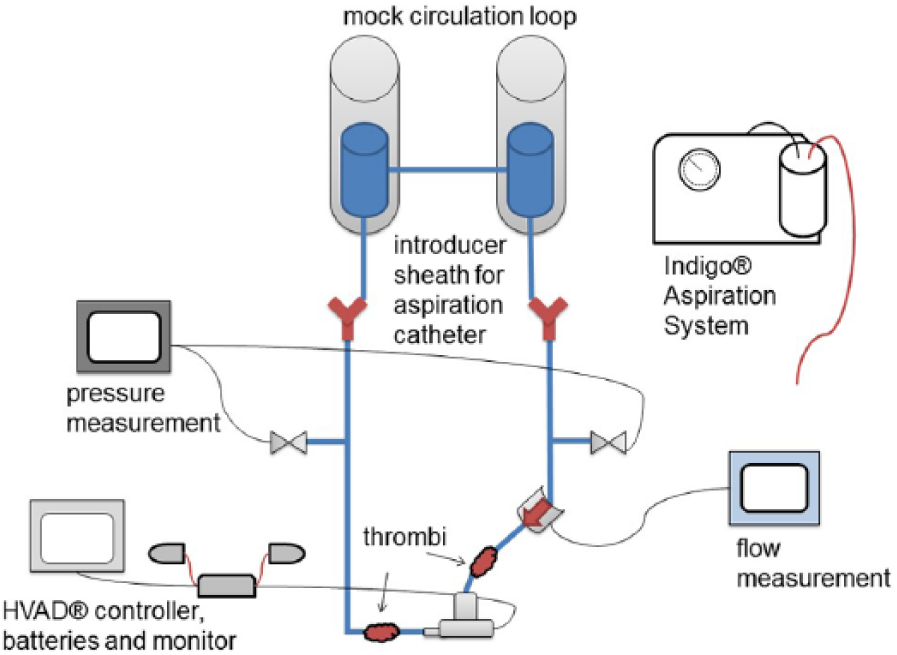
Schematic experimental setup of the in vitro model.
The thrombi positioned at the inlet and outlet were immobilized with a 3-way stopcock and a polycarbonate I-connector. A hole was drilled in the lid of the 3-way stopcock opposite to the Luer Lock connector. The lid was sealed with silicone (Ecoflex® 0030/2 silicone rubber; KauPo, Plankenhorn e.K., Spaichingen, Germany) and a rubber stopper. The thrombus was secured with a wire which was inserted through the hole within the connector. The wire was not removed during the removal of the thrombi using the Indigo catheter. The different attachment positions allowed a flow between 100 and 200 mL/min. A hose clamp ‘stop-it with Easy-click’ (Buerkle, GmbH, Bad Bellingen, Germany) was used as a throttle.For each experiment, the in vitro model was filled with the same amount of fluid.
Study design
Mechanical thrombectomy of the small (n = 5) and large (n = 2) thrombi using the straight- and angled-tip Indigo catheter, respectively, was examined at three different thrombus positions (inlet, outlet, and pump housing) each. Power consumption P (W), aspirated volume (mL), and the duration of aspiration (s) were documented. Two pressure transducers (Codan System DPT-6000) were used to measure the pressure (mmHg) before (P1) and after (P2) the pump. The pressure difference Δp (= P1 – P2) was calculated. Furthermore, a flow sensor (Sono TT Flow Clamp on Transducer; em-tec, GmbH, Finning, Germany), placed before the inflow cannula of the VAD, was used to measure the pump volume flow Q (mL/min; Figure 2). The aspiration success was evaluated visually, whereas technical success was defined as complete thrombus removal from the system.
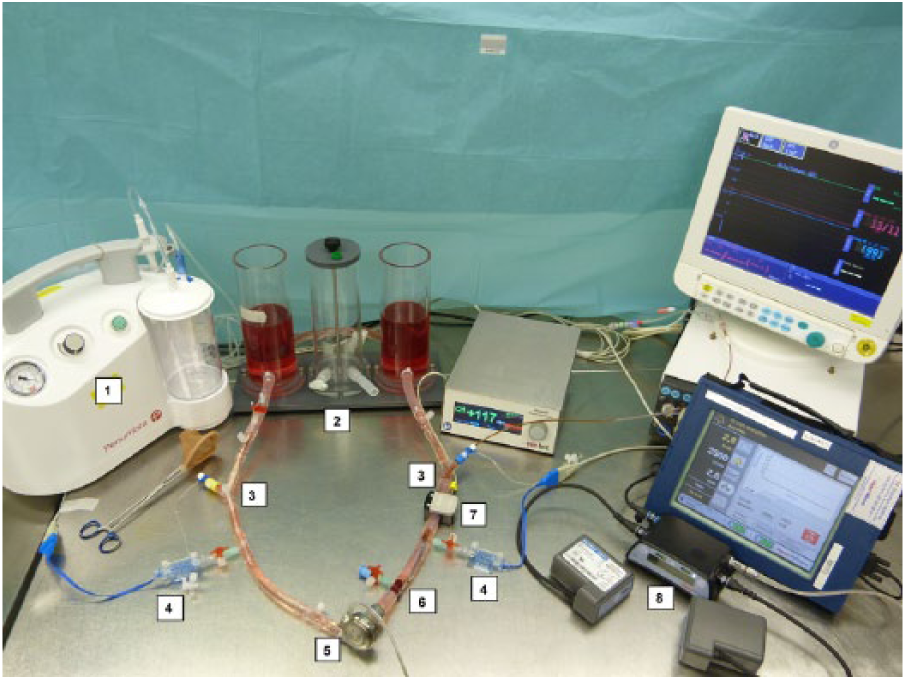
Experimental setup (1. Indigo aspiration system; 2. Mock circulation loop; 3. Introducer sheath; 4. Pressure sensor; 5. HVAD; 6. Thrombus; 7. Flow sensor; 8. HVAD controller, batteries, and monitor).
Five different measurement conditions were compared and data were recorded for 5 min for each condition:
Baseline: parameters without thrombi in the system;
Catheter Insertion: parameters with Indigo® catheter in the system;
Thrombus Placed: parameters with thrombi in the system;
Aspiration: parameters during catheter application (aspiration);
Post-thrombectomy: parameters after catheter application with Indigo® catheter in the system.
Statistical methods
Data collection and analysis were performed with SPSS Statistics 24.0 (IBM Corp., Armonk, NY, USA). The correlation was determined by the Bravais–Pearson correlation coefficient. Categorical and continuous variables (Q, Δp, and P) were summarized as mean with standard deviation (M ± SD). Non-parametric Wilcoxon signed-rank test was used to compare measurement conditions. Two-tailed p values ≤0.05 were considered significant.
Results
In small-volume thrombus tests, 10 out of 15 thrombi (67%) were completely aspirated. Five experiments were defined as technical failure because rigid and dark red colored components remained in the system (Figure 3). This included three experiments with thrombi in the pump housing, one experiment with thrombus at the outlet, and one with thrombus at the inlet. In large-volume thrombus tests, only one experiment showed technical success (thrombus at the outlet). There was no contact between the Indigo® System and the impeller of the VAD during the aspiration. The catheter and the separator remained intact even at the cases with technical failure. Removal of thrombi from the pump housing was more difficult because parts of the thrombus became detached and settled down in the edges of the impeller. There was no risk of catheter damage as the VAD was switched off.
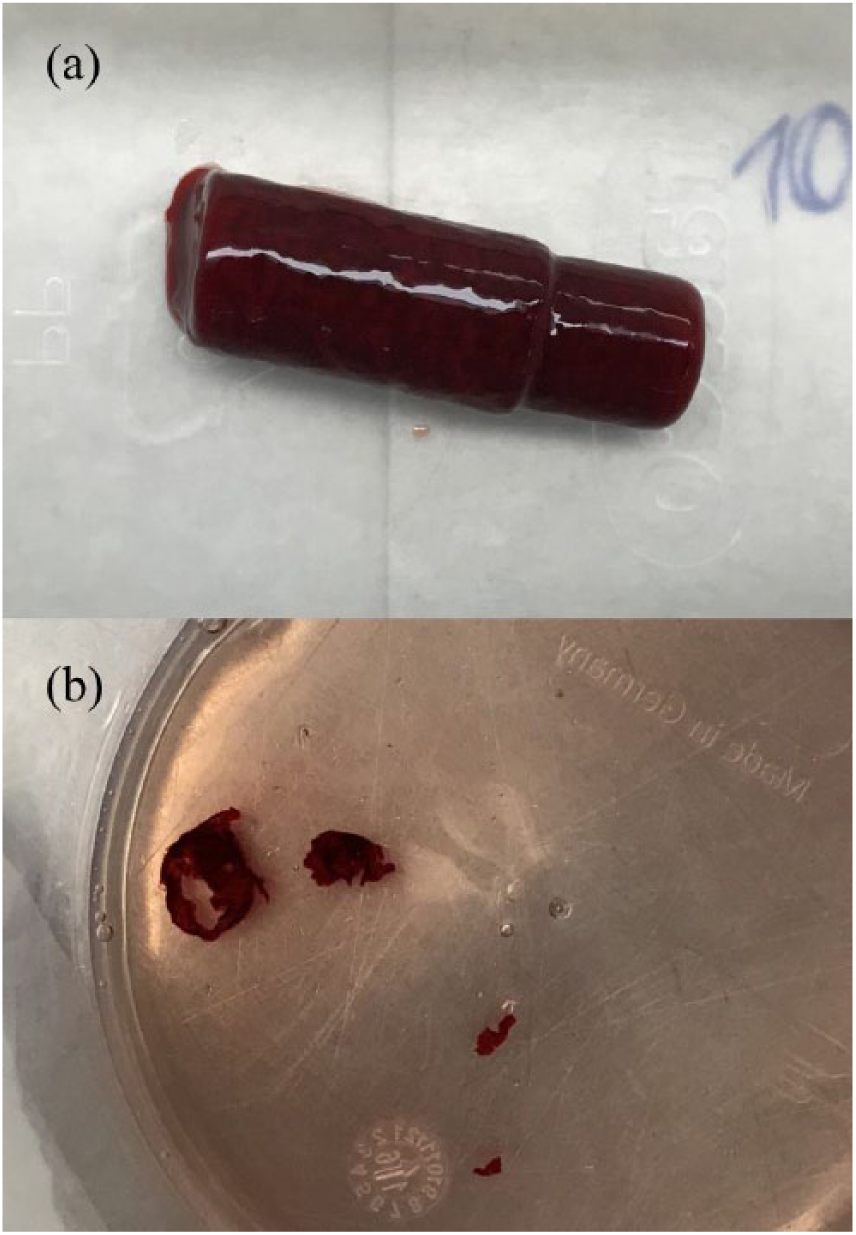
(a) Produced thrombus for small-volume thrombus tests positioned inside the pump housing. (b) Remaining parts of the same thrombus shown in Figure 3(a) after unsuccessful catheter application.
Formation of the thrombi and the required aspiration
Regarding the aspiration duration, outliers were identified and not included in the further evaluation. These outliers were experiments in which only hard, rigid thrombus components remained and further attempts were made to remove those. These thrombi did not meet the set requirements for thrombi used in this study (red stagnation thrombus, not structured nor consolidated).
The duration of the aspiration was significantly shorter while aspirating thrombi from inlet M = 19.75 s (SD = 19.60 s) in comparison to the pump housing M = 38.75 s (SD = 7.37 s) and at the outlet M = 60.50 s (SD = 20.63 s; Table 1).
Thrombus production, comparison of the produced thrombus and their aspiration profiles (I = inlet, O = outlet, and H = housing) for both test series (M ± SD).
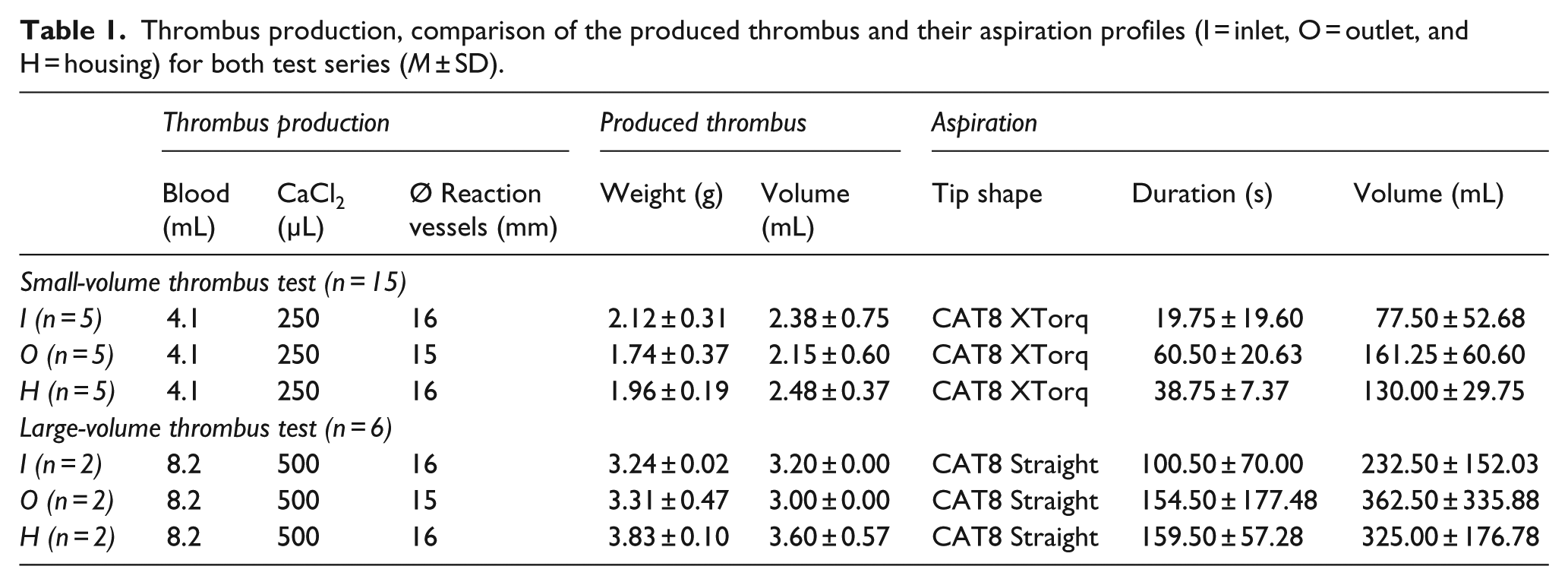
A high correlation between the duration of aspiration and the aspirated volume (rP = 0.97) was recorded, as could be expected. The weight of the thrombus and the duration of aspiration showed a medium correlation (rP = 0.66). Last but not least, there was a medium correlation between the volume of the thrombus and the duration of aspiration (rP = 0.48).
Recorded parameters
During the evaluation of the flow Q and the pressure difference Δp, a strongly deviating data recording was noted during one experiment (thrombus at the outlet). The data were falsified because half of the thrombus had come off and had settled in front of the tube clamp. Another outlier was identified in tests with large-volume thrombus with thrombus in the pump housing. The flow displayed negative values (approximately −100 mL/min). These outliers were not included in the further evaluation.
The parameters of the measurement conditions differ between the three thrombus positions (Figure 4). The large SD at condition Thrombus Placed (thrombus at the inlet and outlet) is attributable to the fact that thrombi allowed different levels of flow. Therefore, the flow had to be readjusted via the hose clamp. This is also reflected in the SD of condition Aspiration and Post-thrombectomy. All three thrombus positions showed an increased flow while using the catheter (aspiration). The pressure difference Δp fluctuates only slightly during the experiment. The pressure difference decreased by ~20 mmHg at Thrombus Placed (thrombus at the inlet and outlet). Even with thrombi within the pump housing, the pressure difference decreased at Thrombus Placed. There was no particular variation in the applied power P of the VAD.
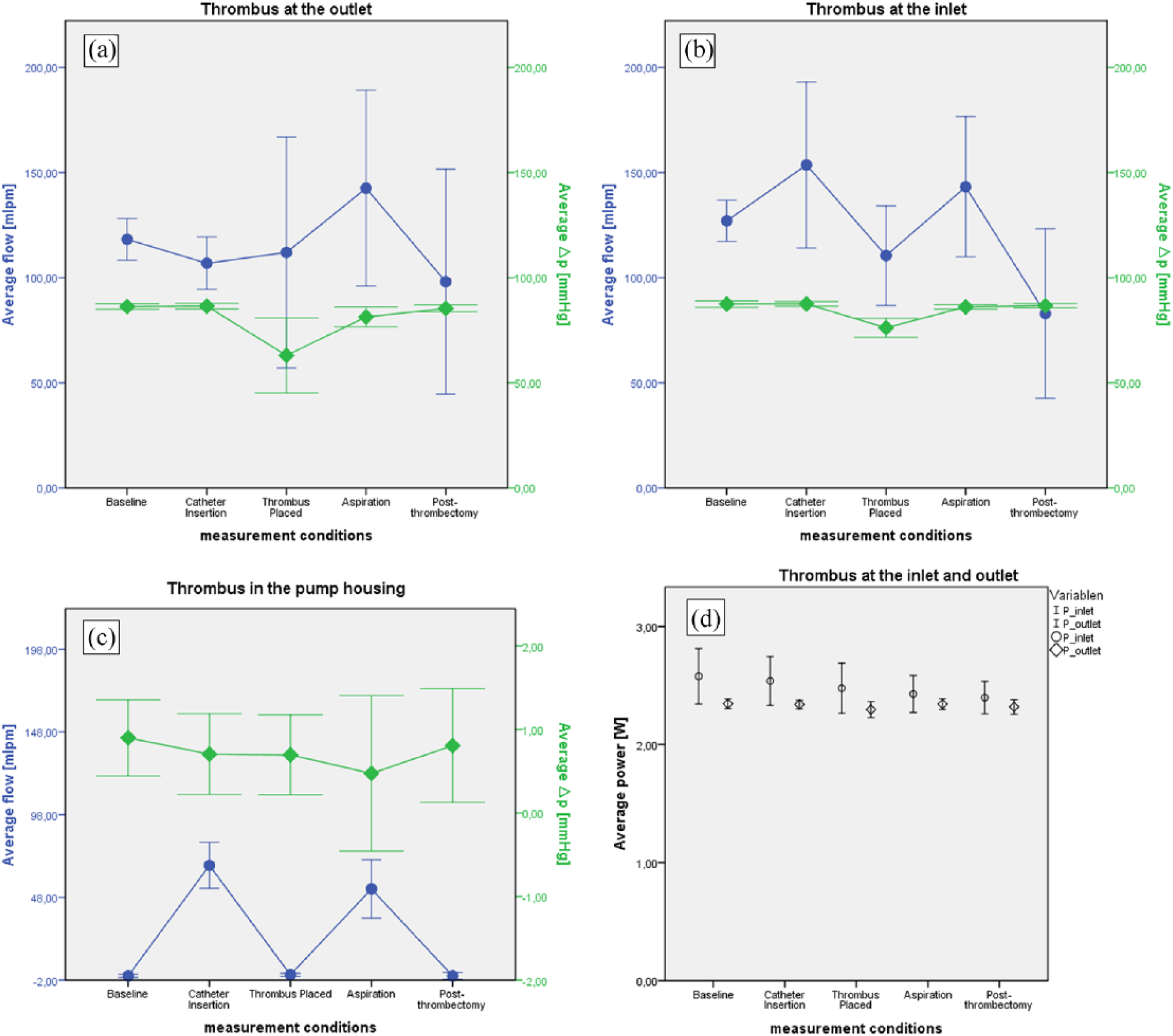
Comparison of the parameters of the three thrombus positions, both test series combined. The mean values of the defined measurement conditions are presented. The error bar indicates the standard deviation of the mean value. (a) Thrombus at the outlet, (b) thrombus at the inlet, (c) thrombus in the pump housing, and (d) average power at the inlet and outlet.
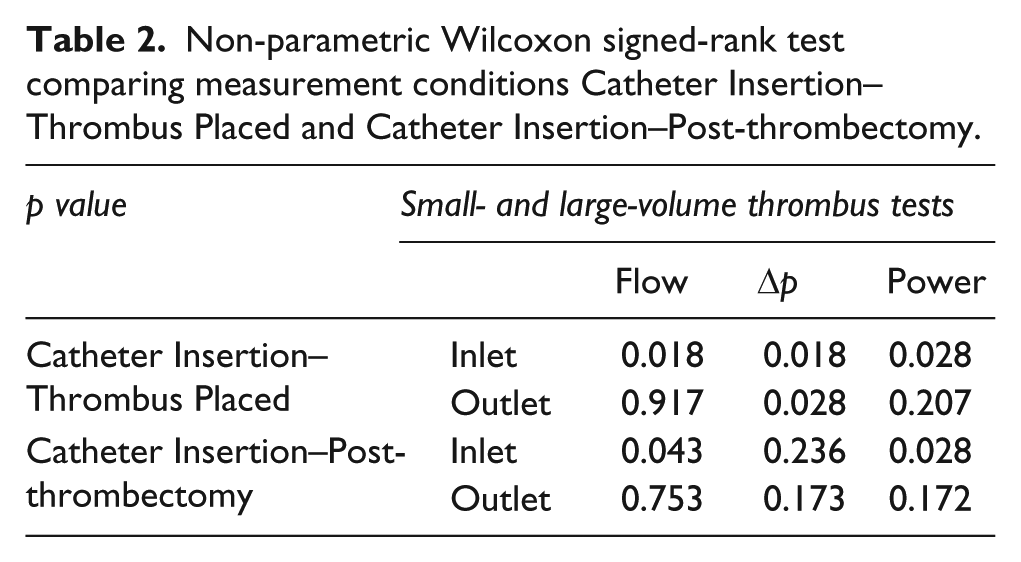
There was a significant difference between measurement condition Catheter Insertion and Thrombus Placed of the parameters (Q, Δp, and P) with thrombi at the inlet (Table 2). There was also a significant difference of Δp with thrombi at the outlet (p = 0.028, α = 0.05). The flow and power showed no significant difference (thrombi at the outlet). Besides the p value of the power with thrombi at the inlet (p = 0.028, α = 0.05), there is no significant difference between Catheter Insertion and Post-thrombectomy.
Non-parametric Wilcoxon signed-rank test comparing measurement conditions Catheter Insertion–Thrombus Placed and Catheter Insertion–Post-thrombectomy.
Discussion
LVAD PT remains a major problem. Thrombolysis is associated with high bleeding risk, whereas pump replacement or heart transplantation remain very invasive procedures with high costs and limited availability of the latter.
It was discovered that patient-related factors influence the development of PT. 3 A PT can cause thromboembolic events, LVAD malfunction or failure with life-threatening consequences. 1 Prasad et al. 6 reported two types of thrombi. In the first case, it was mostly settled around the inlet and outlet of the pump. These areas usually show low pressure or stagnation. 7 The soft clots consist of serum proteins, fibrin, and red blood cells (red thrombi). The fast appearance of red thrombi may cause acute catastrophic PT. The composition of the second type contains a firm and layered fibrin network with different densities (white thrombi). They are found on the rotor assembly within the pump housing. 6 They form slowly by shear activation of platelets caused by turbulence. 7 In addition, a thrombus can also be transported from the left atrium or left ventricle into the LVAD. 8 Literature provides little statistics on the distribution of the three thrombus locations. Scandroglio et al. 9 reported numbers for thrombus in pump, outflow and inflow obstruction (n = 70, 4, and 26, respectively) in an HVAD patient cohort (n = 524). The here proposed thrombectomy method is intended to address the soft clots, for example, forming in outlet graft obstructions and may be combined with other approaches. This could be a stent for more consolidated thrombus parts, which might be attached to the graft material. The produced thrombi used in this study were larger than clinical thrombi to evaluate the effectiveness of the Indigo system simulating a worst-case scenario.
LVAD patients have a high risk of bleeding due to the chronic anticoagulation and antiplatelet therapy. 1 Stulak et al. 10 reported that medical therapy is related to low success (48%) risk of stroke (21%) and death (10%) in a multicenter study. The surgical treatment includes replacement of the device 11 or heart transplantation. However, the availability of donors is limited and pump replacement is associated not only with the risk of perioperative morbidity and mortality but also with high costs. Novel LVAD implantation techniques with a minimal approach have several positive aspects, but adverse events like PT are still possible. 12 Another promising approach is a fully magnetically levitated left ventricular assist system, the HeartMate3.13,14 A multicenter study with 50 patients showed no major events such as PT, pump exchanges or pump malfunctions during the first 6 months after implantation. 15
The Indigo catheter was first used for stroke treatment. 16 Since then, there was an expansion of its uses at all vascular beds. It affords an endovascular approach for acute limb ischemia 17 or acute renovisceral ischemia, 18 as well as for the treatment of deep vein thrombosis or even pulmonary embolism. 19 There is also a dedicated catheter for vascular access.
Our experiments showed a high success rate when the thrombi were located either at the outlet (71%) or at the inlet (57%) of the HVAD. The lower efficacy within the pump housing may be associated with the size of the catheter and the complex rotational mechanism inside the LVAD not allowing enough space for aspiration. In addition, thrombi developed inside the pump housing usually have a composition (white thrombi) differing from the thrombi used in this experiment (red thrombi). There was no risk of damage of the Indigo® catheter as the VAD was not in function during thrombi removal from the pump housing. A damaged catheter could lead to serious adverse events such as loose particles of the catheter, vessel injury, or pump damage. Therefore, in clinical transition, removal of thrombi within the pump housing should be considered to be done with the VAD switched off.
The Wilcoxon signed-rank test showed that thrombi at the inlet caused more significant differences between the flows of Catheter Insertion–Thrombus Placed than thrombi at the outlet (Table 2). Possible explanation could be that the flow sensor was placed on the side of the inlet cannula. The ultrasonic measurement method might be disturbed by the inserted catheter running through the measurement path. The high SD of Catheter Insertion and Aspiration with thrombi at the inlet and within the pump housing was probably caused by the positioning of the catheter inside the sono-transducer (Figure 4). After application of the Indigo catheter, the flow could be restored and there was no significant difference between measuring point Catheter Insertion and Post-thrombectomy. The power consumption with thrombi at the inlet showed a significant difference (p = 0.28, α = 0.05) between Catheter Insertion and Post-thrombectomy (Table 2). Goldstein et al. 8 and Kaufmann et al. 20 reported increased power consumption is indicative for PT. The recommended alarm level is 1.5–2 W above the mean power consumption. 20 Goldstein et al. described power consumption >10 W sustained >24 h as a possible sign for PT. The mean values of Catheter Insertion (M = 2.47 W, SD = 0.19) and Post-thrombectomy (M = 2.35 W, SD = 0.15) are extremely close. The significant difference in the data probably results from the small sample size and the standardized in vitro test method. The parameters showed no major differences during the use of the catheter (Aspiration). Therefore, there is no evidence of negative impact on HVAD by continuous aspiration.
The Bravais–Pearson correlation coefficient indicated that longer aspiration duration is needed for bigger thrombi. The amount of aspirated blood is acceptable (Table 1).
In comparison to the XTorq catheter, the straight one showed lower effectivity. The angled tip of the XTorq catheter allowed a circumferential aspiration at the affected area.
Limitations
The different blood donors lead to poor reproducibility. The varying compositions of the donor blood led to variance in thrombus morphology and the produced sample was small. In addition, there was no histological analysis or microscopic examination of clots. The thrombi were produced under controlled conditions and were judged as comparable to PT in LVAD patient by a cardiothoracic (CT) surgeon after visual examination. The possible effects of the simplification of silicone tubing instead of an outflow graft and the fixation by a wire mechanical integration and surface adhesion were not investigated. Moreover, the study only evaluates the outcome in HeartWare HVAD pumps. The transferability to other impeller systems (axial pumps) needs to be investigated and is a further limitation. As the Indigo catheter comes in different sizes and the circumferential aspiration of vessels up to 25.4 mm is feasible, there is no limitation according to the outlet and inlet dimensions. Therefore, the positive outcome can be transferred to HeartMate devices. Since PT is a very common adverse event in patients with an HVAD (8.1%) and there has been an increase in the incidence of PT in HeartMate II device, 21 the present feasibility study provides important insights for the development of a potential treatment option for PT.
Conclusion
Interpretability of the collected data of this feasibility study is limited because of the small sample size. The described novel mechanical aspiration system showed promising in vitro results for the treatment of PT. Mechanical thrombectomy using the Indigo catheter within an in vitro LVAD flow loop was successful in removing pre-cast, non-adherent, erythrocyte-rich thrombi inserted proximal or distal to the pump. However, further examination, including in vivo experiments, are required for further evaluation. All the study results indicate that Indigo catheter could be used to remove thrombi from the inflow cannula and outflow graft of an HVAD. Thus, further device exchanges and related complications could be prevented.
Footnotes
Acknowledgements
T.G. and E.B. share first authorship.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Bisdas received honoraria from Penumbra Inc.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The aspiration pump, all catheters, and separators used were provided free of charge by Penumbra Inc. Company.