
Abstract
Introduction:
Suspected small bowel bleeding is frequently encountered in left ventricular assist device recipients and the identification of the culprit lesion may be challenging. Data regarding the safety and yield of small bowel capsule in the investigation of suspected small bowel bleeding are limited. We aimed to evaluate the safety and efficacy of small bowel video capsule endoscopy for the investigation of suspected small bowel bleeding among left ventricular assist device recipients.
Methods:
Patients with left ventricular assist device who underwent video capsule endoscopy for the investigation of suspected small bowel bleeding were identified. Suspected small bowel bleeding was defined as the presence of overt bleeding at least 30 days following left ventricular assist device implantation with no identifiable cause in upper and lower endoscopy.
Results:
A total of 10 patients with left ventricular assist device associated suspected small bowel bleeding performed 12 small bowel capsule endoscopies between January 2008 and December 2015 at our tertiary medical care facility. There were no cases of capsule retention or any other serious adverse events during the exams. A significant finding was identified in 8 out of 10 patients, including 3 cases of small bowel angioectasia, 2 cases of small bowel ulcers, 1 case of cecal polyp, and 2 cases of active bleeding with no apparent bleeding source. Small bowel enteroscopy identified and treated bleeding angioectasia in the latter two cases.
Conclusion:
Small bowel capsule endoscopy is safe and effective in the investigation of left ventricular assist device associated suspected small bowel bleeding.
Introduction
Left ventricular assist devices are a well-established modality for the treatment of end-stage cardiomyopathy. 1 While initially they were used as a bridge therapy for critically ill patients awaiting heart transplantation, the improved survival rate with their implantation has led to a prolonged and sustained left ventricular assist device treatment among selected patients. 2
The new generations of left ventricular assist devices are based on continuous-flow technology. 1 One of the most common adverse events associated with these devices is gastrointestinal bleeding.1,3 The lack of pulse pressure may cause local intestinal mucosal ischemia with compensatory angiogenesis and angioectasia formation. 3 Furthermore, the shearing stress caused by the non-pulsatile blood flow leads to an acquired Von-Willebrand factor deficiency due to the consumption of high-molecular-weight Von-Willebrand multimers.3,4 In addition, most of the left ventricular assist device recipients are treated with anticoagulants and antiplatelets agents in order to prevent thrombosis of the device and this may add considerably to their bleeding risk. The rate of bleeding originating in the gastrointestinal tract is estimated to be approximately 20%–40%, notably higher rates compared with the old-generation pulsatile left ventricular assist devices.5–9
The upper gastrointestinal tract is the most common source of bleeding in left ventricular assist device recipients (40%–50%), followed by the colon in 22% of cases. 8 Suspected small bowel bleeding formerly referred to as obscure gastrointestinal bleeding 10 is estimated to be the bleeding source of 35% of cases approximately. 8
Small bowel video capsule endoscopy is the first-line procedure for suspected small bowel bleeding evaluation due to its safety and high sensitivity and specificity for detecting small bowel bleeding lesions. 10 However, data regarding the safety and effectiveness of video capsule endoscopy in left ventricular assist device recipients are lacking, especially with the newer continuous-flow devices. Given imaging™ has included implanted electromedical devices in the list of contraindications to PillCam SB™ capsule endoscopy. 11 The American Society for Gastrointestinal Endoscopy technology review stated implantable cardiac devices as a relative contraindication for video capsule endoscopy investigation. 12
The concerns for using video capsule endoscopy in these patients were that radiofrequency transmissions from the capsule may interfere with function of implantable electromedical devices and also that the device may affect the capsule transmissions.
In this study, we describe the safety profile and utility of video capsule endoscopy investigation among a prospective cohort of left ventricular assist device recipients with suspected small bowel bleeding at a single tertiary medical center in Israel.
Methods
Study population
A cohort of patients aged 18 years and above who underwent left ventricular assist device implantation between August 2008 and March 2015 at a single tertiary medical center. All patients were treated and followed up at a dedicated heart failure unit. gastrointestinal bleeding was defined as the presence of overt gastrointestinal bleeding (melena, hematochezia, or hematemesis). Suspected small bowel bleeding was defined as the presence of gastrointestinal bleeding with no identifiable cause in upper and lower endoscopy. Patients who developed gastrointestinal bleeding which was resolved within 30 days of left ventricular assist device implantation were excluded from this study This study was approved by the institutional Helsinki ethics committee of Rabin Medical Center.
Patients’ characteristics are further detailed in Table 1.
Patients’ characteristics.
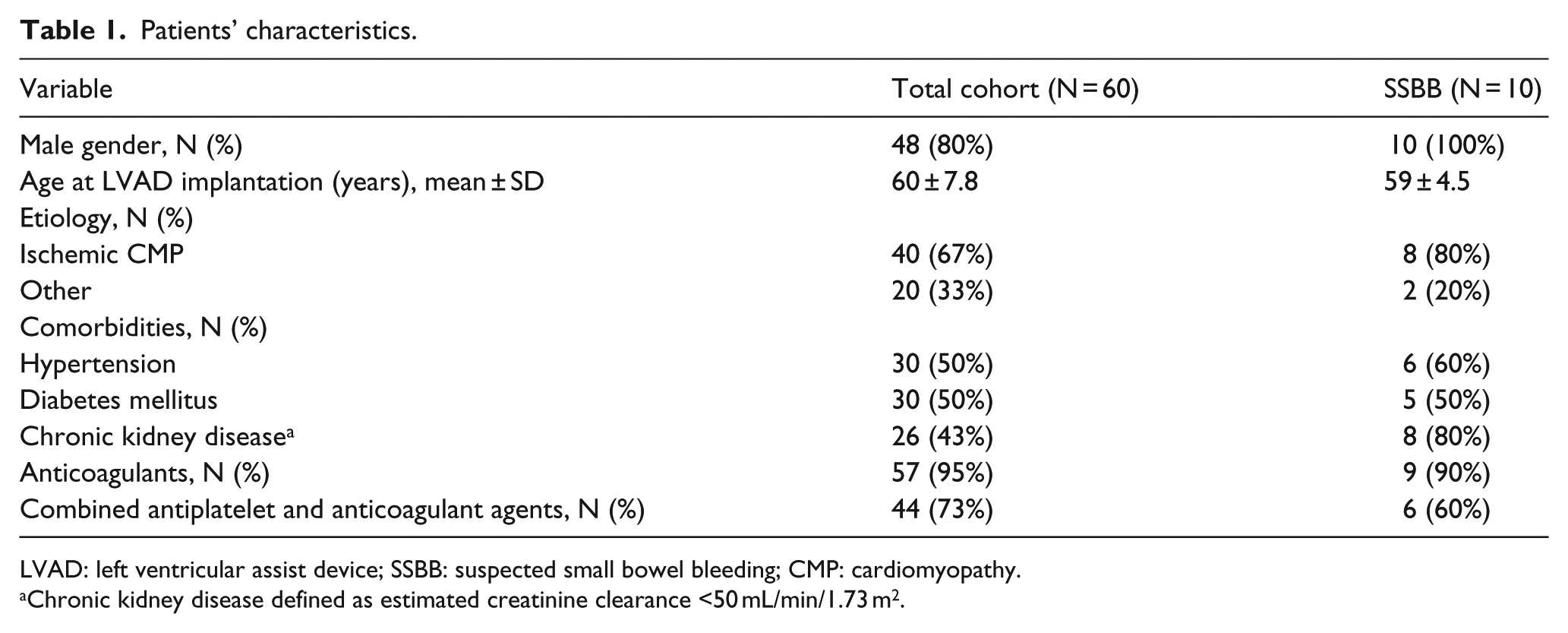
LVAD: left ventricular assist device; SSBB: suspected small bowel bleeding; CMP: cardiomyopathy.
Chronic kidney disease defined as estimated creatinine clearance <50 mL/min/1.73 m2.
Video capsule endoscopy
Video capsule endoscopy is a noninvasive technology which allows visualization of the entire small bowel. This technology includes single-use swallowed capsule, 11 × 26 mm in size, which contains a camera, a light source, and a battery, which lasts for at least 8 h. It captures up to six frames per second and delivers them wirelessly to an external recorder. The frames are then read by an experienced gastroenterologist, who interprets the findings by direct visualization of the bowel mucosa, as is done in invasive endoscopy. The capsule used in our center is the PillCam SB™ (Given Imaging, Israel). In order to clean the small bowel from content and improve visualization, patients are required to fast and to ingest a purgative agent (polyethylene glycol) 12–15 h before the procedure. The more advanced version of the PillCam SB3™ allows better image resolution and a higher frame rate than the previous version, the SB2™. This software includes the Suspected Blood Indicator, a system that identifies frames that contain a few red pixels, potentially aiding the exam interpreter in locating bleeding sources. 13 The median small bowel transit time according to one study was 254 min. 14 When video capsule endoscopy detects a potential source of bleeding, a following invasive therapeutic procedure is considered, such as deep enteroscopy or surgery.
Left ventricular assist device recipients who had suspected small bowel bleeding underwent small bowel video capsule endoscopy for further investigation. Patients were admitted to the cardiology intermediate intensive care ward during the entire investigation and were constantly supervised using a cable-based electrocardiogram monitor. Telemetric electrocardiogram recording was prohibited during the video capsule endoscopy recording in order to minimize recording interference.
Video capsule endoscopy was performed using the PillCam SB2™ and SB3™ capsule (Given Imaging, Israel) and its recordings were interpreted by two experienced gastroenterologists. Video capsule endoscopy findings were classified according to the P0–P2 classification, where P0 lesions are considered to harbor no bleeding potential, P1 lesions are of uncertain bleeding potential (for example, mucosal erosion), and P2 lesions which are considered to have high bleeding risk (such as angiodysplasia or active bleeding with no identified source).15,16 P2 lesions were considered as significant findings. Figure 1 presents typical video capsule endoscopy findings.
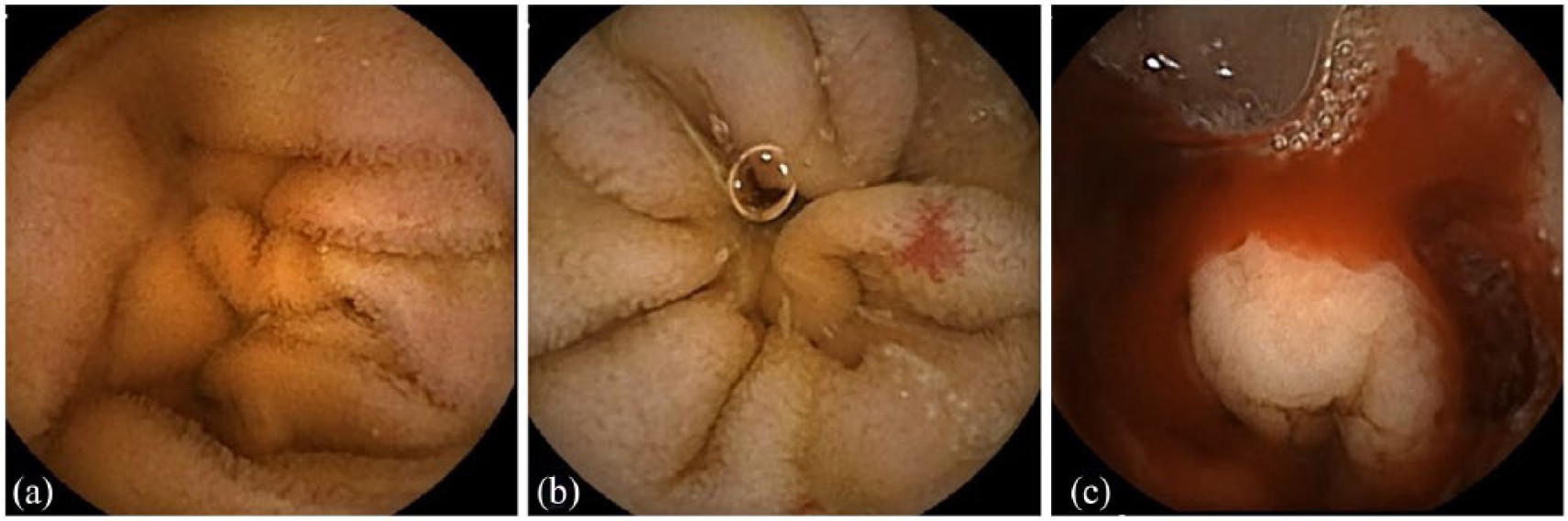
Typical video capsule endoscopy findings: (a) normal small bowel mucosa, (b) angioectasia, and (c) active bleeding.
Statistical analysis
Statistical analysis was generated using SAS Software, Version 9.4. Continuous variables were presented by mean ± standard deviation. Categorical variables were presented by (N, %).
Results
Between August 2008 and March 2015, a total of 60 patients underwent continuous-flow left ventricular assist device transplantation at the Rabin Medical Center in Israel. All of the left ventricular assist devices were either Heartmate™ II or HeartWare™. In all, 25 patients (41%) developed gastrointestinal bleeding at least 30 days following left ventricular assist device implantation and 10 patients (16%) were diagnosed with suspected small bowel bleeding.
A total of 12 video capsule endoscopies were performed in 10 patients with suspected small bowel bleeding, 8 patients underwent one video capsule endoscopy, and 2 patients underwent two video capsule endoscopies, each several days apart due to improper bowel preparation at the first examination.
There were no cases of capsule retention or any other serious adverse events during the examinations, and no cases of video capsule endoscopy recording interruptions were noted.
A significant small bowel finding (P2) was identified in 7 out of 10 patients, including 3 cases of small bowel angioectasia, 2 cases of small bowel ulcers, and 2 cases of active bleeding with no apparent bleeding source. In the latter two cases where ongoing bleeding was noted with no apparent source identified, small bowel enteroscopy identified and treated bleeding angioectasias. Another significant colonic lesion was identified in 1 patient with a large cecal polyp (not identified at previous colonoscopy; Figure 2).
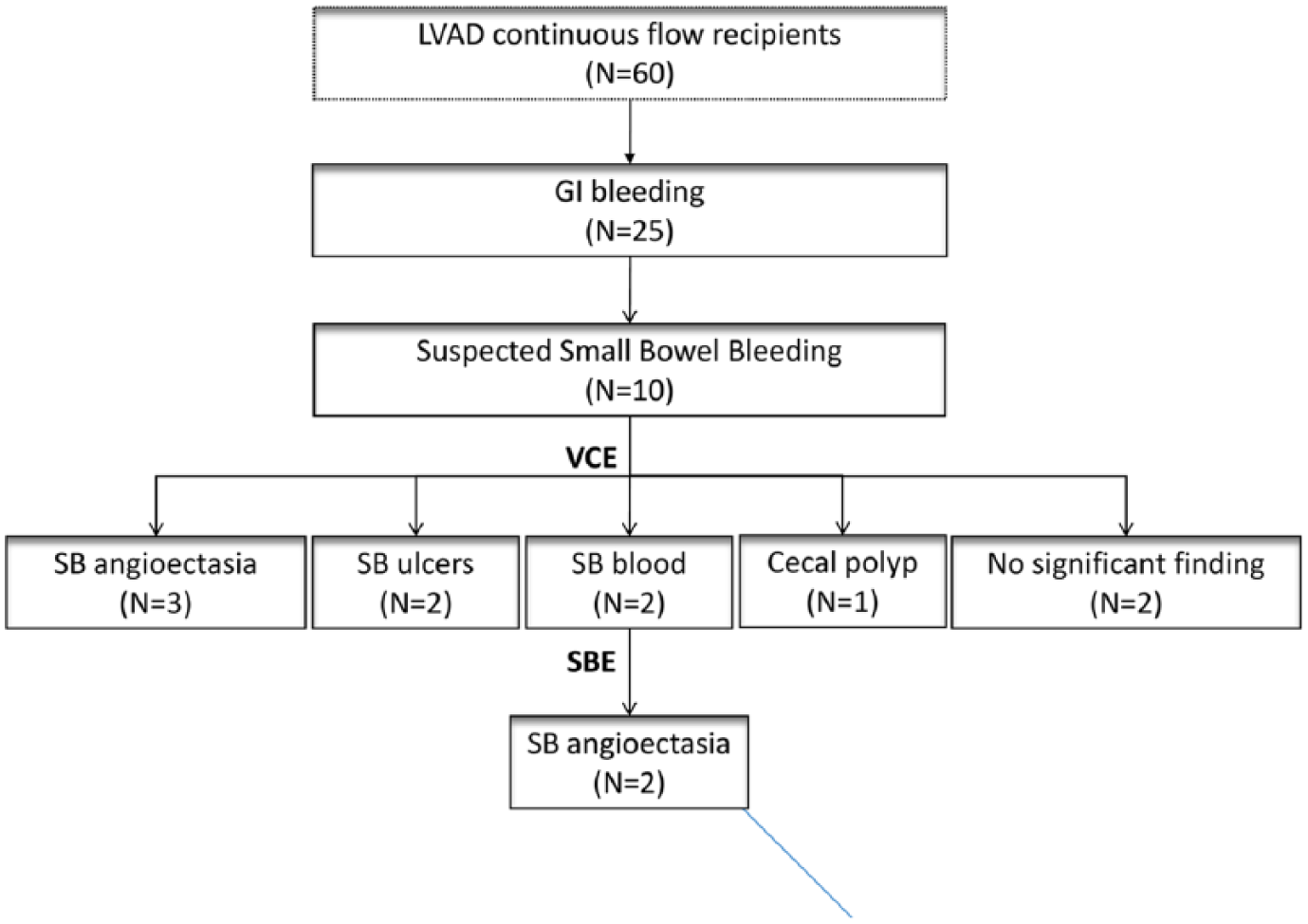
Flow diagram of study patients.
Discussion
Video capsule endoscopy offers the advantage of non-invasive small bowel endoscopy with a diagnostic yield of 38%–83% and a good safety profile. 10 However, its use in continuous-flow left ventricular assist device recipients with suspected small bowel bleeding has been limited mainly due to safety concerns.11,12,17,18 In this cohort of continuous-flow left ventricular assist device recipients, 41% developed at least one episode of gastrointestinal bleeding and 40% of those had suspected small bowel bleeding. Video capsule endoscopy identified the apparent bleeding source in 80% of patients with suspected small bowel bleeding with no adverse events and no documented electromechanical interference.
Several studies have reported similar results. Hanson et al. 19 described their experience with 34 video capsule endoscopies performed in left ventricular assist device recipients with 55% positive findings and no clinically significant cardiac adverse events.
Amornsawadwattana et al. 16 also described 30 video capsule endoscopy records in left ventricular assist device patients with positive findings in 40% of cases and no adverse events.
Truss et al. 20 reported a 100% yield with nine video capsule endoscopies performed in eight left ventricular assist device patients with a reduction of blood products consumption and endoscopic procedure performed following video capsule endoscopy identification of bleeding source and subsequent endoscopic intervention.
Other studies performed on previous generations of left ventricular assist device and video capsule endoscopy reported similar results.21,22 Harris et al. 23 reported two cases of capsule recording interference with a former generation of video capsule endoscopy (M2A capsule, Given Imaging™) in 12 patients with left ventricular assist device. The reason for these interferences is unknown, but both seemed to occur when the capsule was in the upper abdomen close to the left ventricular assist device.
In this study, we describe a cohort of patients implanted with non-pulsatile left ventricular assist device presenting with gastrointestinal bleeding. We have shown that performance of video capsule endoscopy in these patients is both safe and effective in identifying the bleeding source. Finding of significant small bowel lesions in these patients may direct further therapeutic interventions. A considerable number of patients in the suspected small bowel bleeding group had chronic kidney disease (Table 1), a known risk factor for gastrointestinal bleeding and for angioectasia bleeding in particular.24,25 One of the problems we encountered in these patients is the presence of multiple small angioectasias that are not always visible or accessible on enteroscopy and are very difficult to treat. Further studies on the outcome of endoscopic and pharmacologic treatments in these left ventricular assist device recipients are required.
This study has two main limitations. First, the study is based on a single-center cohort, and the results might be different with other types of video endoscopy capsules and with other video capsule endoscopy readers, and second, the cohort is based on a relatively low number of patients.
Conclusion
Small bowel capsule endoscopy is safe and effective in the investigation of left ventricular assist device associated suspected small bowel bleeding and should be considered in the investigation of such cases.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.