
Abstract
Background:
The prognosis of hematologic malignancies has improved over the past three decades. However, the prognosis in hematologic malignancies with severe acute respiratory distress syndrome has remained poor. Initial reports regarding the utility of extracorporeal membrane oxygenation in hematologic malignancies have been controversial, with limited evaluations of acute leukemia patients supported by extracorporeal membrane oxygenation.
Methods:
We conducted a retrospective review of patients with acute leukemia who developed acute respiratory distress syndrome requiring veno-venous extracorporeal membrane oxygenation support at our facility from July 2015 through August 2017.
Results:
Four cases of acute myelogenous leukemia with respiratory failure and acute respiratory distress syndrome treated with veno-venous extracorporeal membrane oxygenation while undergoing induction chemotherapy were identified. All patients completed induction therapy with addition of extracorporeal membrane oxygenation support, with two patients dying secondary to their acute leukemia and the other two surviving to allogeneic hematopoietic stem cell transplant. Overall, 75% (three of four) survived to decannulation with a 1-year survival rate following extracorporeal membrane oxygenation of 50% (two of four).
Conclusion:
Currently, the use of extracorporeal membrane oxygenation in patients with hematologic malignancies who develop severe acute respiratory distress syndrome remains controversial. Although extracorporeal membrane oxygenation in post-allogeneic hematopoietic stem cell transplant is associated with poorer outcomes, our data suggest that salvage extracorporeal membrane oxygenation support is a viable option to manage moderate to severe acute respiratory distress syndrome while completing therapeutic chemotherapy and following in the peri-induction phase of acute leukemia.
Keywords
Background
The overall prognosis of hematologic malignancies (HM) has improved with novel chemotherapeutic regimens, stem cell transplantation, and improved supportive care. However, the prognosis of those HM requiring mechanical ventilation or extracorporeal membrane oxygenation (ECMO) has remained poor with mortality rates of up to 85%.1–4
The underlying etiology for respiratory failure in acute leukemia (AL) varies from other HMs. In AL, non-infectious etiologies such as leukocyte infiltration, immune activation, and pulmonary edema account for 45%–60% of all respiratory events with potential progression to acute respiratory distress syndrome (ARDS).5,6 Mechanical ventilation is required in 60% of AL patients admitted to the intensive care unit (ICU) and ARDS develops in 37%.7,8 Survival to ICU discharge is 62%, and 1-year survival ranges from 16% to 29%.7–10 It is in the setting of these poor outcomes that ECMO can provide respiratory support while a patient receives appropriate chemotherapy.
We describe the use of ECMO as a salvage respiratory support in four AL patients who developed ARDS during induction chemotherapy.
Materials and methods
We performed chart reviews of four consecutive adult patients with AL who developed ARDS requiring rescue therapy with veno-venous ECMO (VV-ECMO) at our institution from July 2015 through August 2017. This retrospective review was approved by the IRB (Protocol C.2017.152d).
The San Antonio Military Medical Center’s (SAMMC) ECMO service provides consultation and support for patients with life-threatening hypoxemia refractory to conventional therapy. In patients with refractory hypoxemia/ARDS despite optimal medical management, ECMO cannulation may be offered. For patients outside our facility, we send a team to include a specialist, coordinator, and cannulating physician to initiate ECMO at the referring hospital before transporting the patient back to SAMMC.
While receiving ECMO therapy, a maximally achievable lung rest ventilation strategy is attempted. Our lung rest strategy incorporates pressure control ventilation with goal of positive end-expiratory pressure (PEEP) of 10–15 cm H2O, inspiratory pressures less than 25 cm H2O, and a fraction of inhaled oxygen (FiO2) less than 0.4. Tidal volume goal is maintained at less than 4 cm3/kg ideal body weight until there is evidence pulmonary recovery. Heparin infusion is titrated to an anti-Xa level of 0.1–0.4 IU/mL so long as activated partial thromboplastin time (aPTT) remains less than 80 s. Anticoagulation is held with severe thrombocytopenia or significant bleeding, at the discretion of the ECMO physician. Weaning from ECMO is performed according to Extracorporeal Life Support Organization (ELSO) guidelines.
At baseline, age, gender, cytogenetics, time of diagnosis, type, and timing of treatments were recorded. The underlying etiology of respiratory failure was noted when known. Secondary markers of acuity such PaO2/FiO2 ratio (PFR) and lactate were recorded at initiation of ECMO. Daily laboratory values to include platelet count, coagulation function, renal, and liver function were recorded. Requirements for ECMO, ventilator, and continuous renal replacement therapy (CRRT), transfusions, vasopressor therapies, and chemotherapeutic regimens were analyzed. Hematopoietic stem cell transplantation (HSCT), hospital discharge, and death were recorded and are presented as the primary outcome.
Case series
Patient 1
A 54-year-old African American female was admitted with respiratory symptoms and labial cellulitis. Peripheral smear at admission was suggestive of myeloid malignancy. Bone marrow biopsy on Hospital Day (HD) 3 confirmed acute myelogenous leukemia (AML). On HD7, patient was transferred to the medical intensive care unit (MICU) for increased work of breathing in setting of acute kidney injury (AKI) and disseminated intravascular coagulopathy. Induction chemotherapy with idarubicin and cytarabine was started on HD10. On HD11, her respiratory status worsened and she was intubated. Her respiratory status continued to decline with worsening bilateral infiltrates and she developed severe ARDS (PFR = 63) despite optimal medical management. On HD15, VV-ECMO was initiated. She continued her induction chemotherapy and on HD20 patient was decannulated with documented remission on HD32. Her lung function continued to improve and she was discharged to an acute rehabilitation facility on HD60. She subsequently underwent consolidation with intermediate dose cytarabine followed by allogeneic HSCT. She lived independently following transplantation for 8 months but died 12 months after her initial AML diagnosis secondary to infectious complications and relapsed AML.
Patient 2
A 63-year-old African American male presented with right toe pain and swelling. Evaluation was concerning for AML and bone marrow biopsy performed on HD3 confirmed the diagnosis. On HD5, he developed multifocal lung opacities. Induction chemotherapy with idarubicin and cytarabine was started on HD6. He was intubated for ARDS on HD7. Over the following 12 days, his ARDS progressed (PFR = 85) despite neuromuscular blockade and he was initiated on VV-ECMO and CRRT therapy on HD19. The clinical course was complicated by recurrent fevers and prolonged neutropenia but responded to granulocyte transfusions and antifungal therapy. Decannulation occurred on HD33 followed by lung protective ventilation via tracheostomy. He remained ventilator dependent and was discharged to a long-term care facility on HD76 without receiving consolidation therapy. After 6 months of his initial AML diagnosis, he was discharged home on supplemental oxygen independent in activities of daily living.
His AML relapsed 12 months after initial diagnosis. He required two inductions to achieve repeat remission. At the time of this submission, he is undergoing matched related HSCT, 18 months from his initial diagnosis of AML.
Patient 3
A 33-year-old Caucasian male presented to an outside hospital with a 2-day history of hemoptysis and fatigue with evaluation suggestive of AML. Upon admission, he developed hypoxemic respiratory failure requiring intubation and mechanical ventilation. Optimal medical management strategies were unsuccessful with a PFR of 108. He was cannulated at the outside hospital by the SAMMC ECMO team and transported back to SAMMC. He started chemotherapy on HD2 with idarubicin and cytarabine. On HD4, he was extubated and was decannulated on HD13. Patient remained oliguric and required reintubation for hypoxia secondary to pulmonary edema from HD15–20. On HD21, repeat peripheral blood flow cytometry demonstrated refractory disease. Salvage chemotherapy failed on HD30. The patient elected to pursue comfort measures and died on HD46.
Patient 4
A 30-year-old Indian male reported to a local emergency department with increasing fatigue and evaluation suggestive of AML. On HD2, he had bilateral infiltrates and was intubated for ARDS. He started induction chemotherapy HD2 with daunorubicin and cytarabine. He progressed to severe ARDS despite optimal medical management (PFR = 74) and SAMMC ECMO was consulted on HD7. He was cannulated at the outside hospital and transported to SAMMC MICU.
At time of admission to SAMMC, the patient had pancytopenia with bloody secretions suggestive of diffuse alveolar hemorrhage (DAH) and hyperbilirubinemia. He was started on empiric antibiotics and high-dose corticosteroids. Over the subsequent days, he became progressively icteric and encephalopathic suggesting worsening organ failure. He developed renal failure requiring CRRT on HD10 and evidence of upper gastrointestinal bleed (UGIB) on HD14. On HD16, peripheral blood smear suggested induction failure. Given the multisystem organ failure, his family decided to withdraw life-sustaining treatment and the patient died on HD17.
Discussion
The use of ECMO in patients with HM who develop ARDS remains controversial. Although an initial report evaluating HM suggested positive conclusions, subsequent studies have been more guarded regarding outcomes; however, most do not differentiate AL from HSCT.4,11,12 In larger studies evaluating utilizing ECMO support in post-HSCT patients, an overall poor prognosis was noted.13,14 Most recently, Schmidt et al., evaluated the 6-month outcomes associated with the use of ECMO support in immunocompromised individuals. Although the outcomes of HM were <25% and the subset of AML/ acute lymphocytic leukemia (ALL) / myelodysplastic syndrome (MDS) also had a <10% 6-month survival, the subgroup of patients diagnosed <30 days prior to receiving ECMO support had a 50% 6-month survival rate. 10 Given the large heterogeneity in HM patients but potentially promising results in the recently diagnosed population, a more thorough evaluation of the utility of ECMO support specific to peri-induction AL is warranted.
The underlying etiology for respiratory failure in AL ranges from opportunistic infections to non-infectious etiologies. A study of high-risk AML patients suggested that >60% of respiratory events are associated with leukostasis, leukemic infiltration, or acute lysis pneumopathy with a 28-day mortality of 34.5% in this cohort. 15 Although the differential diagnosis of respiratory failure in HMs is similar to the AL subset, studies have suggested that a higher rate of infectious etiologies may be responsible for respiratory failure in HM patients.16,17 The AL cases described here suggested an ARDS etiology of leukemic infiltration, leukostasis, and lysis pneumopathy, with two cases also having chest radiographic features concerning for invasive fungal infections. These etiologies represent potentially reversible causes of respiratory failure—if patients are given appropriate respiratory support while receiving chemotherapeutic interventions.
Our cases of ECMO-AML patients treated at SAMMC demonstrated AKI requiring CRRT in all patients, with three of four requiring CRRT at time of ECMO initiation. Previous studies have associated AKI with receiving suboptimal chemotherapy and a lower 6-month complete remission rate. 18 When compounded with the uncertain effects of the ECMO and CRRT circuits, concern regarding adequate chemotherapeutic and antimicrobial levels has been suggested. 19 In our cases, patients 1 and 3 received chemotherapy while receiving ECMO support. For patient 3, there was a 50% dose reduction in chemotherapeutics due to concurrent liver and renal dysfunction, potentially resulting in his failure of induction therapy. Based on this experience, we suggest that chemotherapeutics continue while patient receive ECMO support, with no dose reductions for respiratory failure or renal failure while on CRRT and careful consideration regarding dose reductions in the setting of liver dysfunction.
Bleeding complications represent the most common and potentially disastrous complication associated with ECMO. The ECMO circuit has been suggested to alter the coagulation cascade, increasing the risk of both bleeding and clotting. The standard approach to anticoagulation varies widely, to include dosing regimens of heparin as well as the use of alternatives such as argatroban and bivalirudin. 20 In HM, induced cytopenias and associated coagulopathies further complicate the anticoagulation balance. Our institution utilizes a heparin-based protocol with a combined targeted aPTT and anti-Xa level along with a restrictive transfusion protocol. In patients with HM thrombocytopenia and bleeding, risk must be balanced with the need for anticoagulation. During periods of profound thrombocytopenia, less than 10,000 or acute bleeding, anticoagulation was held at the discretion of the ECMO provider—a total of 11 days in our cohort. Three of four patients had bleeding events to include DAH, UGIB, and hematuria. No events of intracranial, intrathoracic, or retroperitoneal hemorrhage were noted (Tables 1 and 2).
Review of cases seen at our institution from January 2014–June 2017.
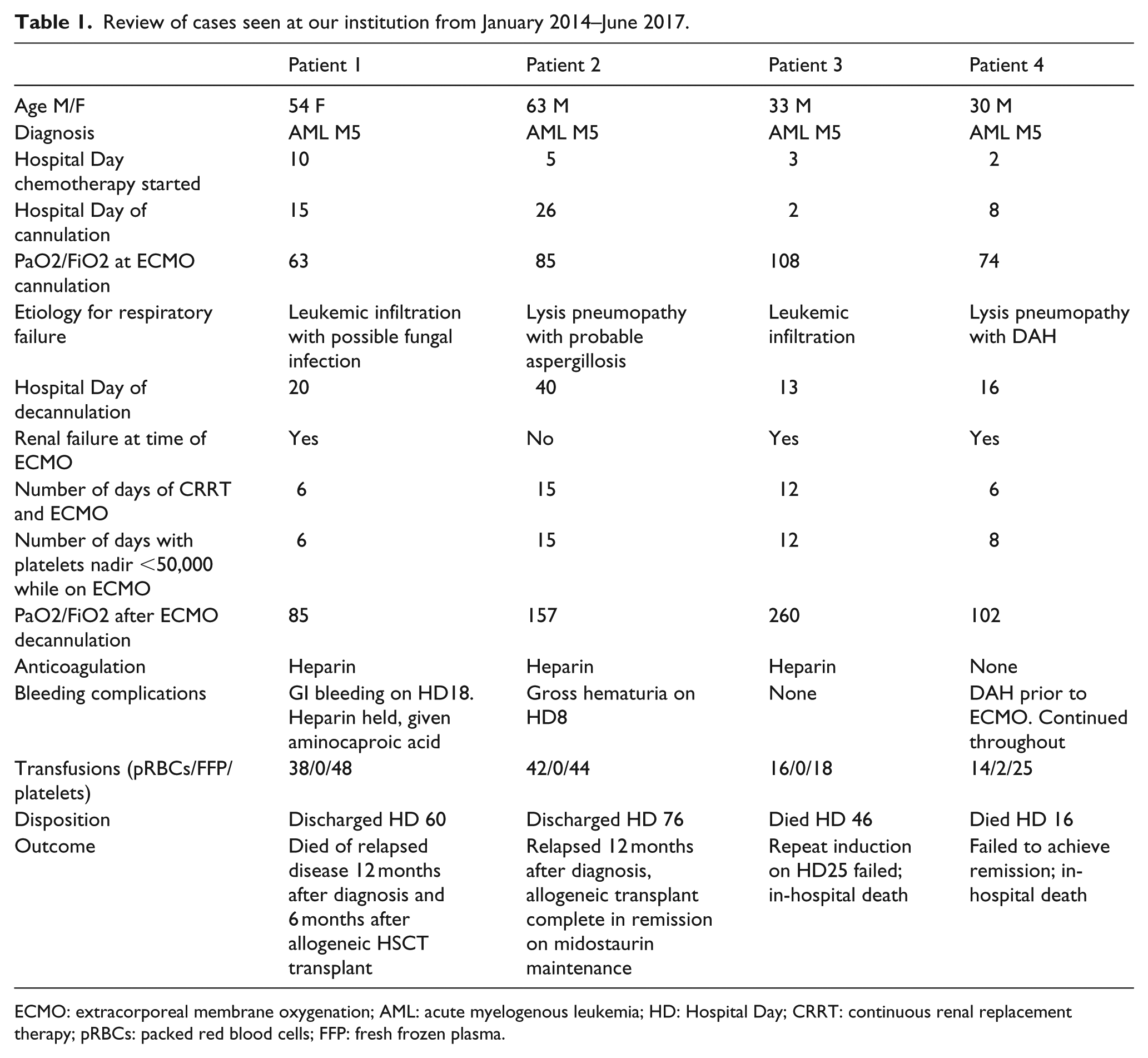
ECMO: extracorporeal membrane oxygenation; AML: acute myelogenous leukemia; HD: Hospital Day; CRRT: continuous renal replacement therapy; pRBCs: packed red blood cells; FFP: fresh frozen plasma.
Chemotherapeutic characteristics of AL patients seen at our institution from January 2014–June 2017.
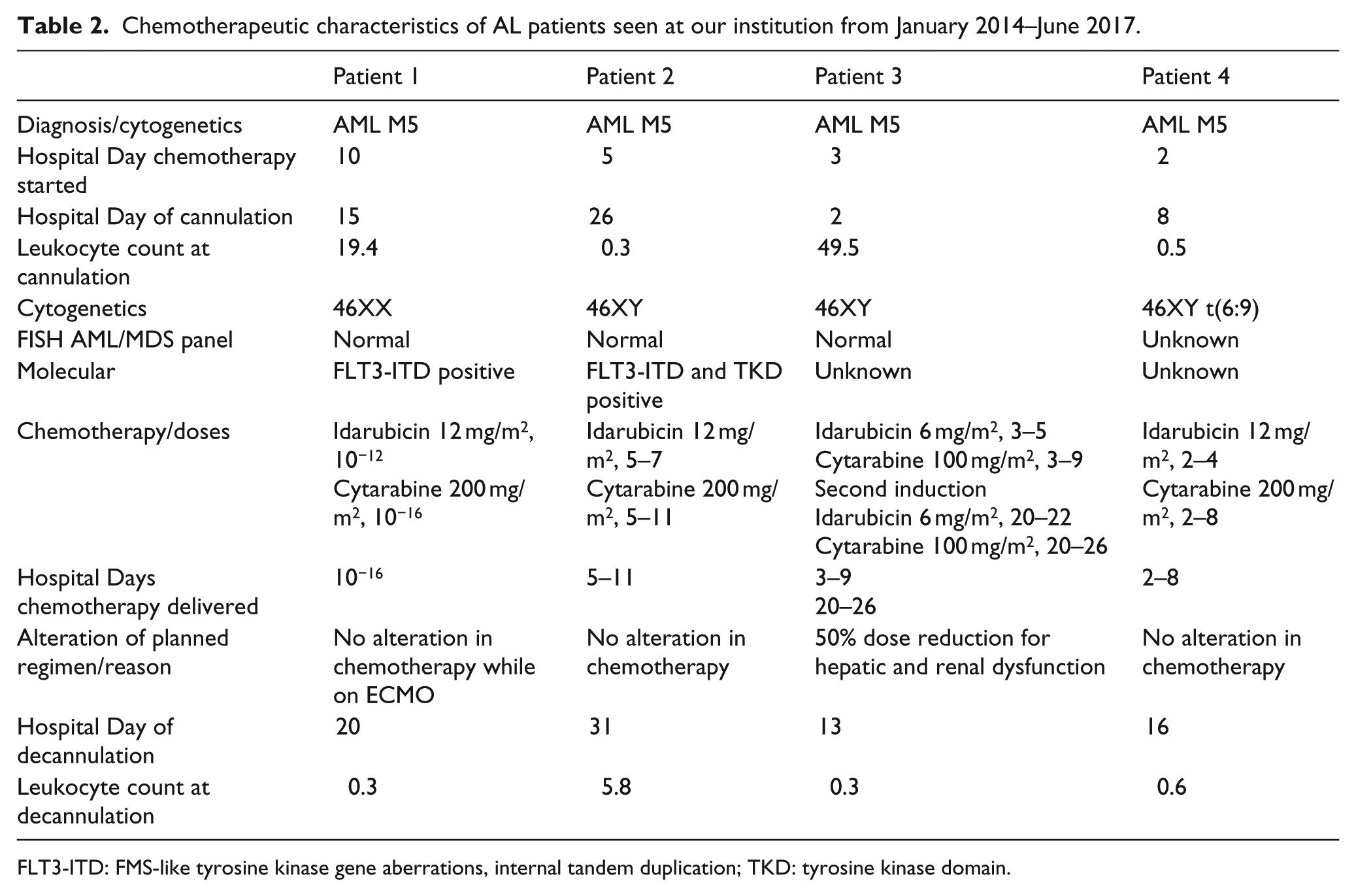
FLT3-ITD: FMS-like tyrosine kinase gene aberrations, internal tandem duplication; TKD: tyrosine kinase domain.
Limitations
SAMMC ECMO offers consultative services to a large demographic area and it is likely only those patients determined to have a higher chance at survival are referred. For those patients treated at SAMMC, a single team of providers with a unified approach is present; however, many of the therapies are at the discretion of the provider. Variations in practice, including transfusion thresholds, chemotherapy agents, and the use of alternative renal replacement therapies such as intermittent hemodialysis and continuous veno-venous hemodiafiltration, may play a role in outcomes and/or complications that are not realized in this assessment.
Currently, there is limited literature regarding the use of ECMO support in AL. Published reports often group AL with HSCT patients. A more precise analysis of these patient compared to those at SAMMC would be ideal but are currently not available. An analysis conducted through use of the ELSO registry may offer a more complete picture of these patients. In addition, technological advances regarding use of ECMO has occurred over the past decade. We remain in the early phases of ECMO therapy and many of the previously targeted goals, including transfusion and anticoagulation requirements, continue to be modified. With these modifications, this therapy can be offered to additional groups of patients previous deemed unfit for ECMO.
Conclusion
Currently, the use of ECMO in patients with HM who develop ARDS remains controversial. Although ECMO post-allogeneic HSCT is associated with poorer outcomes, the four cases of AL requiring ECMO support had a 75% decannulation rate and 50% 1-year survival. The addition of ECMO support allowed all patients to complete induction therapy, with two patients dying secondary to their AL and the other two surviving to receive allogeneic HSCT.
ECMO support may be considered as a salvage maneuver in AL patients who fail conventional mechanical ventilation strategies to allow completion of induction chemotherapy and for respiratory support in the peri-induction period. A concerted effort should be made to capture these patients in the ELSO registry and be reported on a regular basis.
Footnotes
Acknowledgements
N.A.H.: study design, data analysis; primary manuscript author. M.R.P.: data analysis; primary manuscript author. J.D.D.: protocol design, study design; data analysis; secondary manuscript author. V.G.S.: protocol design; secondary manuscript editor. J.H.L.: protocol design; secondary manuscript editor. R.J.W.: data analysis; secondary manuscript author. M.B.O.: study design; senior manuscript editor. K.K.C.: study design; secondary manuscript editor. P.E.M.: data analysis; senior manuscript editor. The view(s) expressed herein are those of the author(s) and do not reflect the official policy or position of Brooke Army Medical Center, the US Army Medical Department, the US Army Office of the Surgeon General, the Department of the Army and Department of Defense or the US Government.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.