
Abstract
Heart failure remains a disease of ever increasing prevalence in the modern world. Patients with end-stage heart failure are being referred increasingly for mechanical circulatory support. Mechanical circulatory support can assist patients who are ineligible for transplant and stabilise eligible patients prior to transplantation. It is also used during cardiopulmonary bypass surgery to maintain circulation while operating on the heart. While mechanical circulatory support can stabilise heart failure and improve quality of life, complications such as infection and thrombosis remain a common risk. Leukocytes can contribute to both of these complications. Contact with foreign surfaces and the introduction of artificial mechanical shear stress can lead to the activation of leukocytes, reduced functionality and the release of pro-inflammatory and pro-thrombogenic microparticles. Assessing the impact of mechanical trauma to leukocytes is largely overlooked in comparison to red blood cells and platelets. This review provides an overview of the available literature on the effects of mechanical circulatory support systems on leukocyte phenotype and function. One purpose of this review is to emphasise the importance of studying mechanical trauma to leukocytes to better understand the occurrence of adverse events during mechanical circulatory support.
Introduction
Leukocytes, commonly known as white blood cells (WBCs), are cells of the immune system responsible for host defence. 1 The main subsets of leukocytes can be defined as polymorphonuclear (PMN) – neutrophils, eosinophils and basophils collectively known as granulocytes – or mononuclear – monocytes and lymphocytes. Functional differences determine the contribution of each cell type to innate and adaptive immunity. These cell types share the feature of responding to various stimuli to produce signature pro- and anti-inflammatory mediators called cytokines that transduce cell responses in receptor-bearing target cells of both haematopoietic and non-haematopoietic origins. 1 Studies on the effects of mechanical shear stress on leukocytes tend to focus on neutrophils, monocytes and lymphocytes, especially T cells, because of their contribution to inflammation, thrombosis and immune regulation and their relative abundance in human blood.
Given the vital contribution of these cell types to host defence, changes in environmental conditions, such as mechanical shear stress, might alter leukocyte function with potentially catastrophic effects. Infection is a common complication in ventricular assist devices (VADs) and rates are reported to be approximately 7% in the HeartMate II (HMII; Abbott Laboratories, Lake Bluff, IL, USA) and HVAD (HeartWare Inc., Framingham, MA, USA),2,3 with the HeartMate 3 (HM3; Abbott Laboratories) showing rates of 22%–36%.4,5 This is often due to infection at the driveline exit site, but there is evidence that the immune system of patients receiving mechanical circulatory support (MCS) is compromised compared to healthy people. 6 For example, early studies reported reduced cellular immunity 7 and deactivation of leukocytes 8 in HeartMate XVE VAD patients leading to an impairment of leukocyte function and the inability to elicit an effective attack against bacterial and fungal infections leading to impaired recovery, sepsis and multiple organ failure.
High levels of artificial mechanical stress produced by a VAD disrupt cells leading to damage, apoptosis and stress-induced microparticle (MP) formation which have strong inflammatory and pro-thrombotic properties. 9 Device thrombosis is a common complication in VADs occurring in 2%–3% of patients.10–13 The most recent VAD to enter clinical use is the HM3 which, so far, has been free of device thrombosis 4 but ischaemic stroke remains a problem. 5
The purpose of this review is to provide an overview of the effects of MCS devices on leukocytes and consider the mechanisms by which shear stress might alter leukocyte phenotype and function. A quick reference table for the content is available in Table 1.
A quick guide to published literature on the effects of MCS on leukocytes (papers describing total leukocytes and those that report on specific subtypes categorised into in vitro, in vivo and clinical studies).
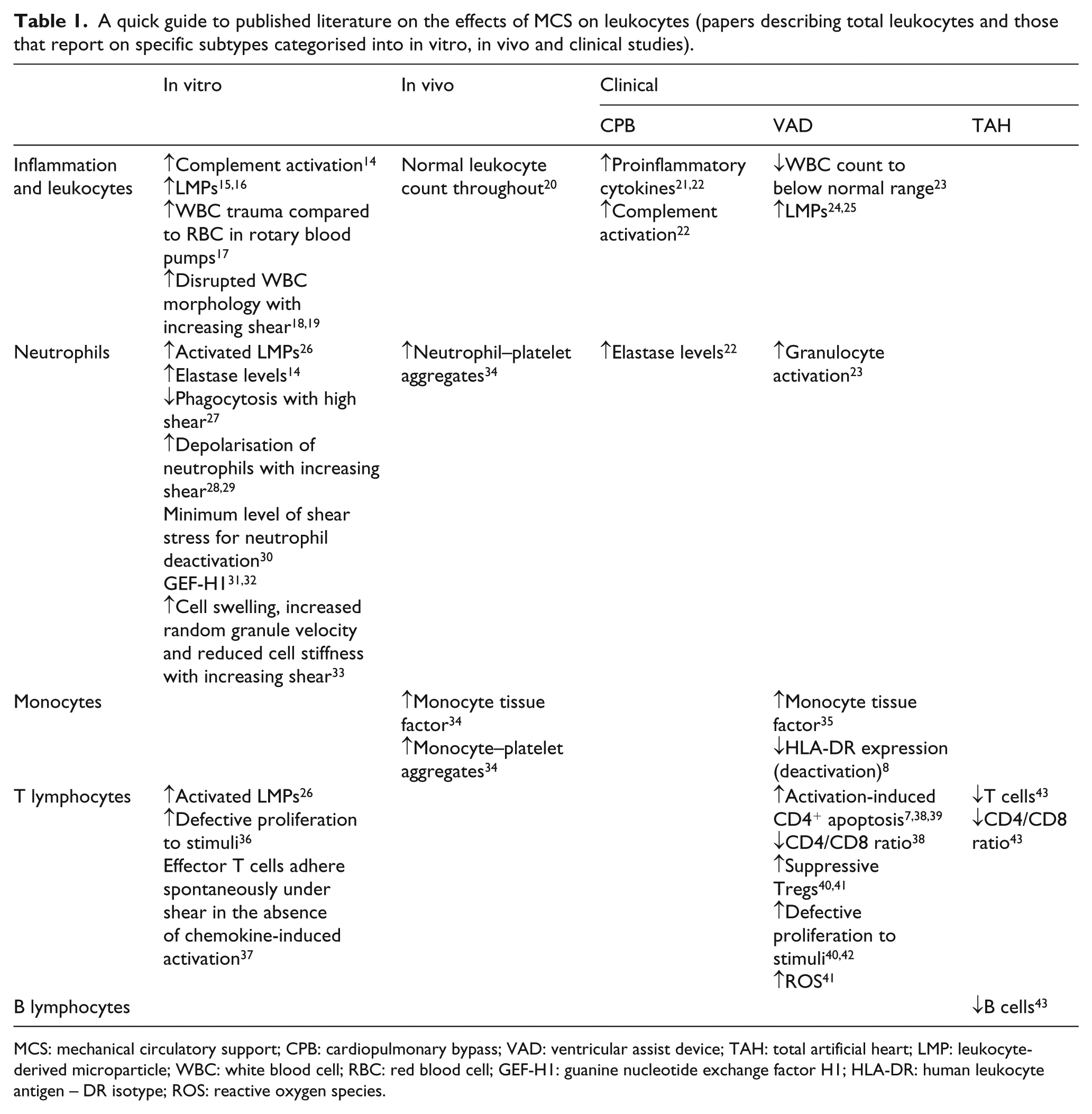
MCS: mechanical circulatory support; CPB: cardiopulmonary bypass; VAD: ventricular assist device; TAH: total artificial heart; LMP: leukocyte-derived microparticle; WBC: white blood cell; RBC: red blood cell; GEF-H1: guanine nucleotide exchange factor H1; HLA-DR: human leukocyte antigen – DR isotype; ROS: reactive oxygen species.
The pivotal role of leukocytes in MCS outcomes
The primary function of the immune system is to protect the body from foreign invaders. MCS devices fit into the category of foreign invaders and how leukocytes respond to these highly influences the outcome. The most abundant human blood leukocytes are neutrophils (50%–60%) with that are essential for the innate immune response. Neutrophils typically are the first leukocyte recruited to an inflammatory site where their role is elimination of pathogens through phagocytosis, production of reactive oxygen species (ROS) and the activity of granule contents, for example, myeloperoxidase, elastase and defensins. 44
Neutrophils are the first leukocyte type to interact with MCS devices and their response is dependent largely on biomaterial and microenvironment which affects the subsequent events. 45 The pre-existing inflammatory state of the recipient might prime neutrophils for exacerbated activation upon exposure to mechanical shear stress. Such excessive stimulation of neutrophils by MCS might contribute to the occurrence of sepsis, multiple organ failure 46 and the formation of thrombosis. 47
Monocytes account for 2%–10% of all blood leukocytes and quickly follow neutrophils to infected or damaged tissues. On migration into tissues, monocytes undergo differentiation into macrophages which provide protection through phagocytosis, cytokine production and antigen presentation. Macrophages are central to the resolution of inflammation via phagocytosis of dying neutrophils and provide a link to the adaptive immune response through antigen presentation. 48 However, MCS devices due to their size cannot be removed in the same fashion as pathogens, leading to ‘frustrated phagocytosis’ by macrophages and the creation of an impermeable layer between host and device. 45 This layer can grow to block the device and cause failure, and emboli can break off leading to stroke. In addition, activated monocytes/macrophages express tissue factor (TF), an activator of the intrinsic coagulation cascade. 49 Shear stress causes the formation of monocyte-derived TF-bearing MPs that can contribute to thrombosis. 9
Cells of the adaptive immune system affect the outcomes of MCS through a less direct approach. Lymphocytes provide antigen specificity to the immune response with T lymphocytes (T cells) being critical in cell-mediated immunity. The CD4+ T helper subset provides cytokines and co-stimulation/inhibition to instruct the tenor of the adaptive immune response and the CD8+ cytotoxic T cell subsets kill the infected host cells. 48 Damage to lymphocytes can cause drastic MCS outcomes such as immunosuppression in patients, thereby increasing the prevalence of opportunistic infections. 38
Mechanical trauma observed in clinical and animal studies
Cardiopulmonary bypass is pro-inflammatory and activates neutrophils
The short-term effects of shear stress on leukocytes can be observed in cardiopulmonary bypass (CPB). Leukocyte activation is evidenced as an increase in pro-inflammatory cytokines such as tumour necrosis factor (TNF)-α, interleukin 6 (IL-6) and interleukin 8 (IL-8) over time during CPB, albeit not significantly for TNF-α. 21 These increases are evident when using both centrifugal flow pumps (CFPs) and roller pumps (RPs). 22 However, neutrophil activation appears more prominent in CFP with more elevated levels of elastase and IL-8 than RP after 2 h. 22 Reasons for pump differences remain speculative, but one suggestion is that pulsatile perfusion, as slightly by RP, 50 offers less cellular disruption through better preserving microcirculation. 51
VADs generate MPs
CPB temporarily introduces high levels of shear stress to the circulation; VADs do so permanently and the effects on leukocytes are more likely to cause complications (Figure 1). VADs introduce foreign biomaterials with varying surface finishes that are known to cause leukocyte activation.52,53 While this foreign body response may resolve itself through the building of an ‘inert’ biological layer on the device, the non-physiological shear stresses remain constant. High levels of shear stress cause MP release from platelets (platelet-derived microparticle (PMP)), leukocytes (leukocyte-derived microparticle (LMP)) and endothelial cells (endothelial cell–derived microparticle (EMP)) 25 and patients implanted with the HMII and HVAD all have increased LMPs. 24 Given that these devices are very different in terms of design (HMII – a titanium alloy axial flow pump with ceramic (ruby) bearings; 54 HVAD – a titanium alloy centrifugal pump with parts made from zirconia 55 ), it is likely that a high shear stress introduced by VADs causes LMP release regardless of design features. Consequently, an increase in LMPs independently of leukocyte counts has been suggested as a biomarker for vascular inflammation. 25
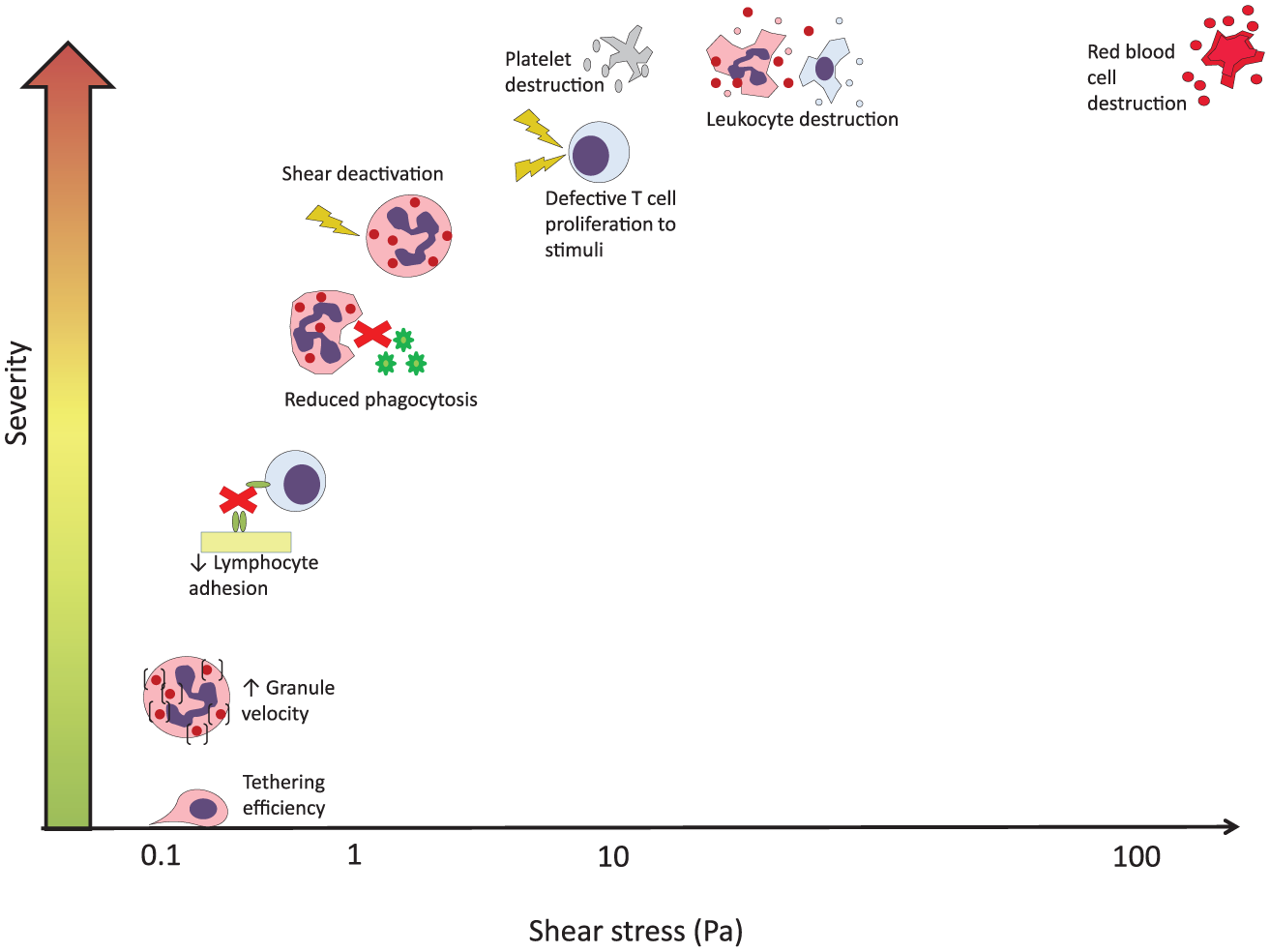
Relationship between shear stress and changes in leukocyte morphology and function. Leukocytes are accustomed to physiological shear stress (0.05–1 Pa) throughout the circulation allowing them to remain in a resting state until activated by pathogenic stimuli. Above these shear levels, leukocyte function is altered through diminished phagocytic ability (>0.6 Pa 27 ), deactivation by shear (2.5 Pa 30 ) and defective proliferation responses by T cells to stimuli (>10 Pa 36 ). Shear above 10 Pa destroys platelets and leukocytes leading to the production of MPs. RBCs remain more tolerant to high shear as destruction occurs around 150 Pa. 19
MPs are both pro-inflammatory and pro-thrombotic so they are potentially involved in VAD-related thrombosis and chronic systemic inflammation. 56 In VAD patients, monocyte TF expression increases within the first week and returns to the normal range within a month. 35 Monocyte TF is a potential source of thrombin generation 35 and monocytes can produce TF-bearing MPs. Significantly increased levels of MPs in VAD patients could be predictive of adverse events 57 although there are yet to be conclusive studies on whether these are biomarkers of MCS or vascular inflammation in general.
VADs affect leukocyte counts
In patients implanted with a pneumatic ventricular assist device (PVAD; Abbott Laboratories), HMII or HVAD, leukocyte counts increased significantly from already greater than usual preoperative levels to above the normal range at postoperative day (POD) 14. Comparatively, patients who undergo CPB display an increased leukocyte count, but this returns to normal by POD 5. 58 Woolley et al. 23 speculate that the surgery- and device-induced systemic response is substantial as a reduction in the inflammatory response is expected to reduce the number of circulating leukocytes by this time. Given that ‘frustrated phagocytosis’ is a feature of biomaterial implantation, any delayed clearance of neutrophils would prolong their presence and might sustain their recruitment. 45 By POD 60, leukocyte counts fall significantly below preoperative levels in all VAD types 23 which could indicate VAD-mediated recovery to normal healthy leukocyte counts, or more concerning, leukocyte reduction due to damage. Controversially, in vivo studies of HVAD implanted in sheep showed that the WBC count remained within the normal range throughout the long-term (90-day) study. 20 Notably, there are species differences in the relative abundance of different leukocyte subsets with lymphocytes being the most abundant leukocyte in sheep and neutrophils in humans. 59 Analysis of total WBC count only in sheep might mask VAD-related effects on neutrophils. 26
VADs activate leukocytes in a device-dependent manner
As the first line of defence against foreign bodies such as VADs, granulocytes are predisposed to upregulation and expression of activation markers. Macrophage antigen-1 (MAC-1) is a granulocyte marker for systemic inflammation and has been used as a biomarker in CPB and sepsis.46,47 MAC-1 expression on granulocytes was increased significantly in HMII at POD 14 and did not return to preoperative levels until POD 120. 23 On the other hand, HVAD patients had only a small increase in MAC-1 expression at POD 14 which had returned to preoperative levels by POD 60. 23 Patients implanted with HMII also experienced higher rates of infection than the HVAD, likely related to increased MAC-1 expression and MAC-1-induced apoptosis of granulocytes. Shear stress rather than biomaterial/surface choice here is the more likely explanation for the increased granulocyte activation in HMII as the operating speed is three to four times greater than that of the HVAD with smaller gaps and twice the range of turbulent stresses. 60
In animal studies, activation of leukocytes and subsequent aggregation with platelets was measured in cows implanted with the HMII. Increases in monocyte TF, monocyte–platelet and granulocyte–platelet aggregates occurred within the first few days postoperatively. While the levels decreased over the next 30 days, they remained greater than the preoperative levels and are suggestive of increased risk of thrombosis. 34 Again, the presence of small gaps and turbulent stresses in the HMII is likely responsible with thrombus formation around the bearings as a result. 61
VAD use can lead to immunosuppression
Severe side effects of VADs include sepsis and multiple organ failure which are associated with chronic inflammation and immunosuppression. 46 Potential deactivation of monocytes through reduced expression of human leukocyte antigen, especially HLA-DR, has been observed in VAD recipients. Loss of HLA-DR has been postulated as a biomarker for increased risk of patient mortality as patients who died had fewer HLA-DR-positive monocytes than those who survived. 8 This might also be indicative of immunoparalysis which hampers tissue repair for end-organ recovery. 62 The deactivation of monocytes by VADs might be more likely in patients with pronounced systemic inflammation, with introduction of the device activating monocytes to the point of exhaustion. 8
The effects of MCS on T and B cells are much less studied. Implantation of the first-generation pulsatile flow VADs in humans has been described to cause a selective reduction in CD4+ T cells, defective CD3+ T cell proliferative responses to stimuli and higher levels of apoptosis in both CD4+ and CD8+ T cells; the link between these and mechanical stress is supported by in vitro studies of the effects of shear stress on T cells.7,38,40,42 The effects of continuous-flow devices on lymphocytes, while less studied, are suspected to be less severe than pulsatile flow devices. The one available study showed increased apoptotic activity in CD4+ T cells up to 4 weeks postoperatively which normalised to baseline after 7 weeks 39 rather than sustained excessive CD4+ T cell apoptosis linked to a drastic reduction in circulating CD4+ T cells in pulsatile devices. 38 More recently, a study of infection rates in continuous-flow ventricular assist device (CF-VAD) patients found that patients with infection had much higher numbers of circulating regulatory T (Treg) cells than those without infection. 63 Oxidative stress was also prominent in CF-VAD patients and when combined with increased Treg cells it could lead to immunosuppression and pathogen persistence. 63
There is very little information on the effects of total artificial hearts (TAHs) on leukocytes. In one study that observed two patients sustained with long-term TAH, granulocyte function remained intact, but both patients became B and T lymphopenic with an initial decrease in the ratio of helper to cytotoxic T cells. 43 While identifying changes in leukocytes by MCS is beneficial to modifying care during use, understanding the mechanisms behind these changes benefits design changes by developers.
In vitro shear stress models
Several shearing devices have been used during in vitro studies to generate variable shear stress conditions and study their effects of leukocytes. Each device type has its advantages and disadvantages, but those used in leukocyte activation studies include the following:
Concentric cylinder viscometer. Blood is sheared in the annular gap between the inner bob and the outer cup.18,19
Cone and plate viscometer. Blood is sheared in the gap between the stationary plate and the perpendicular rotating cone. 64
Parallel plate viscometer. Blood is sheared in the gap between the stationary plate and the rotating parallel plate.27,65
Microfluidic devices. Blood is pushed through micrometre-sized channels using syringe pumps or other pumps to control flow. 33
Mock circulatory loops. Blood is circulated through a loop connected to MCS devices.15,26
The key findings include the lower tolerance threshold of leukocytes compared to red blood cells (RBCs). Using a concentric cylinder viscometer to shear whole blood in the range of 10–60 Pa for 10 min yielded a decrease in WBC viability and count, and increased enzyme release; this was at levels much lower than critical for detrimental effects on RBCs (~150 Pa).18,19 Lower shear stresses but still greater than physiological levels (>0.6 Pa) cause pseudopod retraction and condensed actin distribution. 27 Comparable results were seen using a cone-and-plate device wherein shear stress (0.15–0.5 Pa) applied to leukocytes adhered to a glass surface caused instant pseudopod retraction. 64
Retraction of pseudopods relates to the phagocytic ability of leukocytes. The phagocytic ability of neutrophils diminishes under high (>0.6 Pa) compared to low (0–0.2 Pa) shear stress. 27 Bacteria were seeded onto discs of cardiovascular device materials and isolated neutrophils were added to the discs which were then subjected to shear using a rotating disc system. Scanning electron microscopy (SEM) revealed that neutrophils subjected to high shear stress became compact and irregularly shaped, with condensed nuclei and F-actin, and were apparently incapable of interacting with the bacteria. 27 Those subjected to lower shear stresses maintained the characteristic multi-lobed nuclei with normal morphology and bactericidal activity. 27 Another study identified an immediate retraction of neutrophil pseudopodia on the application of ~0.04 Pa with neutrophil granule velocity being significantly enhanced by shear stress (0.1 Pa), indicating that the cytoplasm within the cell had become less viscous due to cell swelling. 33 The continuous application of shear stress enhances random granule velocity and reduces cell stiffness. These phenomena suggest that shear stress mediates water entry into the cell, thereby reducing F-actin, 33 causing cell swelling/lysis 19 and depressing T cell activation. 36
Rotary blood pumps tested for 6 h with human blood have shown WBC damage through trypan blue exclusion in the absence of haemolysis, further supporting that WBCs are more vulnerable to mechanical trauma than RBCs. 17 When circulated through the CentriMag™ and HMII (Abbott Laboratories), blood elastase concentration increased significantly over time, indicating granulocyte activation. 14 Our own studies using bovine blood circulating through the CentriMag, RotaFlow (MAQUET Holding B.V. & Co. KG, Rastatt, Germany) and VentrAssist™ (Ventracor Ltd, Sydney, Australia) for 6 h showed an increase in LMPs, indicative of mechanical damage.15,16 Characterisation of these LMPs using ovine blood circulated through the CentriMag identified CD11bbright/HLA-DR– and CD11bdull/HLA-DR+ populations of LMPs which we propose come from granulocytes – that were also significantly decreased in number – and T lymphocytes, respectively. 26
Mechanisms of mechanical (de)activation
The studies mentioned above show that shear stress greatly impacts leukocyte morphology and function whether it be high enough to cause destruction, 19 or just enough to reduce phagocytic ability. 27 Knowing how this happens can benefit the development of MCS to encourage leukocytes to work with rather than against the device. The mechanisms through which artificially high shear stress activates or deactivates leukocytes are yet to be fully understood. Much of the literature regarding the effects of shear stress is contradictory due mostly to variation in the methods used to apply shear stress and to measure its effects. The following section aims to summarise what is known about mechanotransduction effects in leukocytes.
Innate immune cells
Responding to changes in shear forces is a normal feature of leukocyte activity. During inflammation, circulating leukocytes must cross the endothelium and migrate into tissues. Leukocytes interact with and tether to the endothelial surface most efficiently at around 0.1–0.2 Pa. 66 Leukocytes must then produce pseudopodia to allow migration across the endothelium and into the tissue. In healthy vasculature, physiological shear of around 0.15 Pa 67 induces pseudopod retraction 33 which is dependent on the presence of RBCs.30,31 This serves to maintain circulating leukocytes in a spherical shape to prevent trapping in capillaries and allow normal passage through the microcirculation. 64 Therefore, the leukocyte shear stress response is a fundamental regulatory mechanism supporting normal blood flow and enabling the inflammatory response.
The principal consequences of neutrophil priming and activation include cell polarisation with the formation of lamellipodia at the leading edge and a uropod trailing edge, 68 increased cell deformability, expression of integrins/selectins, generation of superoxide anions and degranulation and release of lipid mediators. 28 Activation occurs through ligand-induced structural changes in receptor molecules that activate intracellular signalling cascades. These control neutrophil adhesion and migration, in part through local regulation of actin polymerisation and actin–myosin contraction. 31 The Rho family of small GTPases are well-established key mediators of ligand-induced cytoskeleton changes in motile cells.31,68 It has been suggested that shear stress activates leukocytes through structural changes in the same array of molecules in response to physical forces rather than ligand-induced signal transduction. 32 Examples include stretch-sensitive calcium ion channels, neutrophil polarisation through plasma membrane tension or swelling-induced inflammatory lipid mediator production from damaged host cells.32,69 More recently, guanine nucleotide exchange factor-H1 (GEF-H1) has been associated with shear stress activation of neutrophils. GEF regulates actin–myosin-dependent uropod contractility in leukocytes by promoting guanosine diphosphate (GDP)-to-guanosine triphosphate (GTP) exchange on the small GTPase RhoA. 70 GEF-H1 is activated in response to shear stress to promote spreading, crawling and transmigration of neutrophils. 31 Depolymerised GEF-H1 relocalises to the uropod to stimulate Rho signalling resulting in intracellular tension and cellular contractility. 32
Notably, repeated mechanical deformation of primed neutrophils can return them to a resting state. 29 Shear deactivation of neutrophils through retraction of pseudopods can occur at around 2.5 Pa, but prolonged exposure to fluid shear stress leads to visibly disrupted leukocyte structure. 30 The particular challenge of MCS devices is the combination of areas of high shear stress with low residence time, and areas of low shear stress with long residence times. If leukocytes can be differentially and negatively affected by both scenarios, simply lowering shear stress is not enough. Neutrophils are the primary effectors of the innate immune response and the negative effects on them will have downstream consequences.
It has been suggested that mechanotransduction mechanisms in monocytes are similar to neutrophils as they also form uropods during extravasation. 71 While F-actin becomes condensed in neutrophils, an increase in its synthesis in monocytes has been observed when applying 12 Pa shear stress using a microfluidic pump. 72 F-actin is used for pseudopod extension in phagocytosis 73 so it is possible that elevated shear stress underpins the ‘frustrated phagocytosis’ noted earlier.
Adaptive immune cells
T lymphocytes, the most studied lymphocyte subtype in terms of shear stress, differ fundamentally to neutrophils and monocytes as they crawl against blood flow. 74 Adhesion of T lymphocytes to the blood vessel wall occurs rapidly and firmly – cells must arrest at the endothelium and resist shear stress once tethered, which relies on polarised adhesion. 74 In one study, increasing shear stress from 0.03 to 0.12 Pa decreased the fraction of adherent lymphocytes suggesting disruption of the adhesive mechanism between T lymphocyte and endothelium. 75 When subjected to significantly higher than physiological shear stress (10–20 Pa) for 10 min, T lymphocytes were no longer able to proliferate on stimulation with the lectin phytohaemagglutinin-P (PHA-P) and IL-2 production was diminished. 36 This relates to the studies in VAD patients that identify defective proliferative responses to stimuli in T cells leading to immunosuppression. 38 Lectin binding to the T cell surface induces a rise in intracellular calcium ions, accompanied by depolarisation of the membrane and acquisition of IL-2 receptors. 36 This suggests that high shear disrupts T cell activation through interfering with lectin binding or prohibits an IL-2 feedback loop through another mechanism. The cellular and molecular mechanisms underpinning this are largely unknown and warrant investigation given the severity of the complications. 37
Summary
The use of mechanical circulatory devices has revolutionised cardiac surgery and the treatment of heart failure. Such devices introduce artificially higher shear stress to the circulatory system for prolonged times and can cause cell damage. Research in this area has focused mainly on RBC damage through haemolysis measurements. 76 However, RBC tolerance to shear is relatively high in comparison to that of leukocytes, and also of platelets. 77
MCS devices affect all leukocyte types, but neutrophils appear to be the most affected. CPB activates neutrophils as measured through increased elastase which is a marker of degranulation. 22 CPB has also been associated with increased circulating pro-inflammatory cytokines, particularly IL-8, which chemoattracts neutrophils and prolongs the inflammatory response. 21 Inflammation rapidly mobilises the release of neutrophils from the bone marrow into the blood, leading to an increase in leukocyte count which returns to normal a few days after CPB. 58 However, leukocyte counts remain elevated at POD 14 in VAD patients suggesting a substantial device-induced systemic response that might be affected by the introduction of foreign biomaterials, various surface finishes, as well as artificial shear stress.23,53
Shear stress affects neutrophils independently of biomaterials as evidenced by increased activation of granulocytes in HMII patients compared to the HVAD. 23 It is suggested that the physical forces of non-physiological shear stress cause structural changes that activate granulocytes. 32 Activation is marked by an increase in MAC-1 expression as observed in the HMII patients. 23 Equally, non-physiological shear can return granulocytes to a resting state where they are no longer responsive to inflammatory stimuli. 29 This is problematic in that a reduction in phagocytic ability by granulocytes leaves patients vulnerable to infection and might be why HMII patients suffer recurrent infections.23,27
Chronic infection, sepsis and multiple organ failure are also related to shear stress effects on other leukocyte types. Monocytes can react to biomaterials through ‘frustrated phagocytosis’ 45 and high shear on monocytes induces F-actin synthesis for pseudopod extension. 72 This might be why monocyte deactivation occurred. 8 Immunosuppression can also occur through effects on T cells. In vitro studies have shown that shear stress mediates water entry into cells which can cause cell swelling/lysis and depress T cell activation.19,36 Shear-induced swelling of T cells would go towards explaining the high levels of CD4+ and CD8+ cell apoptosis in VAD patients. 38 Exposure to high shear also diminishes the T cell response to inflammatory stimuli 36 which is suggested to be caused by interference with lectin binding by mechanical forces. This has also been noted in VAD patients who showed defective T cell proliferative responses to stimuli. 7
The mechanisms through which shear stress causes activation, and perhaps eventually exhaustion, of multiple leukocyte populations are not fully understood. Better understanding of these processes would provide data to optimise MCS design and minimise detrimental effects on leukocyte function as well as the adverse events that currently accompany the clinical use of blood-handling medical devices.
Future outlook
The development of new test devices that allow modifications of gap size, residence time, shear stress, biomaterial types and surface finish for leukocyte analysis in vitro would prove highly beneficial. Such devices would improve the design of MCS devices long before implantation through providing more information on cellular activation. While studies on RBCs and platelets are clearly beneficial, leukocytes are far more complex in their interactions due to their variety and diverse functions. Leukocytes play a role in both infection and thrombosis – two common complications of MCS usage – so including the analysis of these cell types should improve optimisation of device design in terms of thrombogenicity and potentially reduce recurrent infection rates.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship and/or publication of this article: G.R. and S.A. are employees of Calon Cardio-Technology Ltd (Calon). I.L.P. is employed by Scandinavian Real Heart AB.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.