
Abstract
Background:
To investigate whether preoperative short-term extracorporeal life support therapy in patients undergoing continuous-flow left ventricular assist device implantation has an impact on the outcome regarding survival and adverse events.
Methods:
Between January 2011 and May 2018, 100 consecutive patients received HeartMate II, HeartWare, or HeartMate III for end-stage heart failure. Mean age was 64.2 ± 10.3 years. Three patient groups were identified: without preoperative extracorporeal life support (non-extracorporeal life support group, n = 80), with preoperative extracorporeal life support due to postcardiotomy shock after conventional cardiac surgery (postcardiotomy shock group, n = 9), and with preoperative extracorporeal life support without previous surgery (non-postcardiotomy shock group, n = 11). The primary endpoint was overall survival after device implantation. Secondary endpoints were adverse events during the follow-up period.
Results:
Survival was significantly different between the groups (p < 0.05): 30-day, 6-month, and 1-year survival rates were 85%, 68%, and 61% for non-extracorporeal life support group; 44%, 22%, and 22% for postcardiotomy shock group; and 45%, 27%, and 24% for non-postcardiotomy shock group, respectively. Furthermore, in both extracorporeal life support groups (postcardiotomy shock and non-postcardiotomy shock), there were a higher incidence (p < 0.05) of postoperative right heart failure (30% vs 66.7% vs 54.5%), acute renal failure requiring dialysis (20% vs 77.8% vs 54.5%), and respiratory failure (31.3% vs 88.9% vs 81.8%).
Conclusion:
Continuous-flow left ventricular assist device implantation with prior extracorporeal life support appears to have a worse outcome regarding survival, right heart failure, renal and respiratory dysfunction (p < 0.05). Future studies have to be done to evaluate the outcome after extracorporeal life support bridge pre-left ventricular assist device, especially as ultima ratio in postcardiotomy shock patients.
Keywords
Introduction
Heart failure (HF) is one of the leading causes of death in the developed world. 1 In stage D of HF, after exhaustion of medical therapy, either cardiac transplantation or mechanical circulatory support (MCS) is recommended. 2 Moreover, the importance of assist devices as destination treatment measure by left ventricular failure grows continuously due to a shortage of donor’s hearts and the accepted use as destination therapy (DT). From all long-term MCS devices, over 95% are left ventricular assist devices (LVADs). 3 The implantation of LVAD still represents a high-risk procedure, which is related to severe adverse events, such as right heart failure (RHF), cerebrovascular accident, infection, pump thrombosis, and hemolysis. 4 Expanding the indications for LVAD implantation leads to offering this therapeutic option to even older and sicker patient population. To this end, LVADs are increasingly implanted in high-risk patients as ultima ratio.
In this particular article, we will focus on the use of extracorporeal life support (ECLS) as a bridge to LVAD in patients with cardiogenic shock (CS), who belong to profile I or II, according to the current classification of the Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS). 5 The morbidity and mortality remain high in this cohort. 6 ECLS serves to stabilization of shocked patients to a more stable INTERMACS category and allows recovery of end-organ function before proceeding the LVAD implantation. 7 However, it benefits remain controversial, and the topic remains underinvestigated. There is still no clear treatment strategy for patients presenting INTERMACS I or II. Existing studies mostly concentrated on the ECLS therapy as bridge to LVAD in shocked patients without prior open-heart surgery. There are only a few studies aimed to investigate the outcome of patients who first undergone conventional cardiac surgery, developed then postcardiotomy shock (PCS), obtained ECLS as bridge to recovery and afterwards, after failed stabilisation and the impossibility of ECLS weaning received LVAD implantation under ongoing ECLS.
Our study aimed to investigate the effect of ECLS bridge on the outcome in patients undergoing LVAD implantation. We compared LVAD patients without preoperative short-term MCS to those with preoperative ECLS bridge. Meanwhile, we distinguished between two indications for ECLS therapy during the study—PCS and CS without previous cardiac surgery.
Materials and methods
Study population
At our institution, from January 2011 to May 2018, a total of 100 patients received a long-term LVAD because of HF by cardiomyopathy, PCS, or acute myocardial infarction as DT, bridge to transplantation (BTT), and bridge to candidacy (BTC) strategy. The indication for the operation was made following the current guidelines. 8 We used one of three LVAD models: HeartMate II (HM II), HeartMate III (HM III; Thoratec Corp., Pleasanton, CA, USA), and HeartWare (HVAD; HeartWare International Inc., Framingham, MA, USA). Choice of VAD was based on the availability of the device in the clinic and the personal decision of the surgeon. Thus, from January 2011 to November 2015, we used the HM II and from November 2015 to 2018, we used either the HM III or the HVAD.
Study design
The study is a retrospective review of prospectively collected data. Data collected as part of the institutional Mechanical Circulatory Support Database included detailed information on patients’ demographics, baseline clinical characteristics, and their laboratory, echocardiographic and hemodynamic parameters, as well as intraoperative variables and postoperative outcomes. The follow-up data collected by a periodic (once a month) presentation of the patients in our VAD clinic. The study was approved by the local ethics committee.
Study groups
All the subjects were divided into three groups: group 1—patients without ECLS prior to LVAD implantation (non-ECLS, n = 80), group 2—patients with ECLS due to PCS after previous cardiac surgery (PCS, n = 9), and group 3—patients with ECLS due to CS without previous surgery (non-PCS, n = 11).
Outcome measures
The primary endpoint was overall survival after device implantation at 30 days, 1 year, and 2 years. Secondary endpoints were adverse events and other postoperative characteristics during the follow-up period. Patients were censored after their death or at the cutoff of the study.
Variables and definitions
Variables were evaluated, including baseline characteristics, as well as further preoperative clinical data, preoperative laboratory parameters, intraoperative data, postoperative variables, and follow-up data. PCS was defined as the inability to wean a patient from cardiopulmonary bypass (CPB) requiring an ECLS support at any point during the hospital stay. The adverse events definitions were mostly based on the “INTERMACS Adverse Event Definitions.” 9 Major bleeding was defined as an episode of suspected internal or external bleeding that resulted in re-operation (need for revision), hospitalization, or transfusion of packed red blood cells (PRBCs) as follows: ⩾4U PRBC within any 24-h period during first 7 days post-implant or a transfusion of PRBC after 7 days following implant. Major infection was defined as an episode of localized non-device infection, percutaneous site, and/or pocket infection or sepsis. Respiratory failure was defined as impairment of respiratory function requiring reintubation, tracheostomy, or the inability to discontinue ventilatory support within 6 days (144 h) post-LVAD. RHF was defined as a need for post-implant inotropes continued beyond post-op day 14 following LVAD implant, right ventricular assist device at any time following LVAD implant or delayed chest closure due to hemodynamic instability. Hepatic dysfunction was defined as an episode of an increase in any two of the following hepatic laboratory values—total bilirubin, aspartate aminotransferase, and alanine aminotransferase—to a level greater than three times the upper limit of normal, beyond 14 days post-implant. Acute renal dysfunction was defined as an episode of abnormal kidney function requiring dialysis (including hemofiltration) in patients who did not require this procedure prior to implant, or a rise in serum creatinine of greater than three times baseline or greater than 5 mg/dL sustained for over 48 h. Neurological dysfunction was defined as an episode of transient ischemic attack, ischemic stroke, or acute intracranial hemorrhage.
Surgical technique
We cannulated ascending aorta and right atrium for a central ECLS and femoral artery and vein for a peripheral ECLS. An additional left ventricular vent for central ECLS was inserted through the right upper pulmonary vein. All LVAD procedures were performed via full sternotomy. After systemic heparinization, cannulation for CPB was performed either in standard fashion via ascending aorta and right atrium or the procedure was performed on ECLS, without conversion to CPB. For patients, who needed a concomitant tricuspid valve surgery, a bicaval cannulation was performed. Cardioplegia was used in patients needing concomitant procedures according to each procedure. Concerning the LVAD implantation directly, the inflow cannula of the assist device was implanted into the heart apex according to the manufacturer’s instructions. The outflow graft was connected to the ascending aorta via an end-to-side anastomosis in a standard manner. The driveline was undermined subcutaneously in a double-tunnel technique. After that, CPB was weaned and the chest was closed in a standard manner. In cases with acute right-sided HF, short-term right ventricular assist device (ST-RVAD) was implanted through the right atrium and the pulmonary artery. In a few cases, the chest closure was delayed because of hemodynamic instability.
Anticoagulation protocol
At ⩾12 h post-implantation, when the chest tube drainage decreased to ⩽50 mL per hour, and the coagulation profile returned to normal or near-normal levels, intravenous heparin infusion was commenced to maintain an activated partial thromboplastin time between 60 and 80 s. Aspirin, 100 mg for HM II and HM III groups, and 300 mg for the HVAD group, once daily was commenced after extubation. After removal of the chest drains and starting oral medication, phenprocoumon was administered to maintain an INR between 2.0 and 2.5 for HM II and HM III patients and between 2.3 and 2.8 for HVAD patients. Heparin infusion was continued until the international normalized ratio (INR) target range was attained.
Statistical analysis
The data were analyzed using IBM SPSS version 25 (IBM Corp., Chicago, Ill., USA). We used the Kolmogorov–Smirnov test to prove the data for normal distribution. Quantitative data are expressed as the mean and standard deviation (SD) for normally distributed variables and as the median and interquartile range for not normally distributed variables. Categorical data are expressed as frequency and percentage. We used the Kruskal–Wallis test to compare mean values and the chi-square test to examine the distribution of categorical variables between the groups. We used the Kaplan–Meier method to analyze the survival. The significance of survival differences between the groups was assessed with Log-Rank and Breslow tests. A value of p < 0.05 was considered to be statistically significant.
Results
Baseline characteristics
In the entire cohort of 100 patients (20% females), the most frequent etiologies of HF were ischemic cardiomyopathy in 52 patients (52%), dilated cardiomyopathy in 28 patients (28%), and PCS in 11 patients (11%). There was a significant difference in primary diagnosis between the study groups; PCS led to LVAD implantation in all patients of group 2. Groups 2 and 3 were INTERMACS 1 to 3 exclusively, were ventilated and had an intraaortic balloon pump preoperatively more often than group 1 (p < 0.05) (Table 1). Furthermore, groups 2 and 3 showed significantly higher preoperative levels of white blood cell (WBC), C-reactive protein (CRP), total bilirubin, alanine aminotransferase (ALT), and lactate dehydrogenase (LDH) (Table 2).
Baseline characteristics of the study patients.
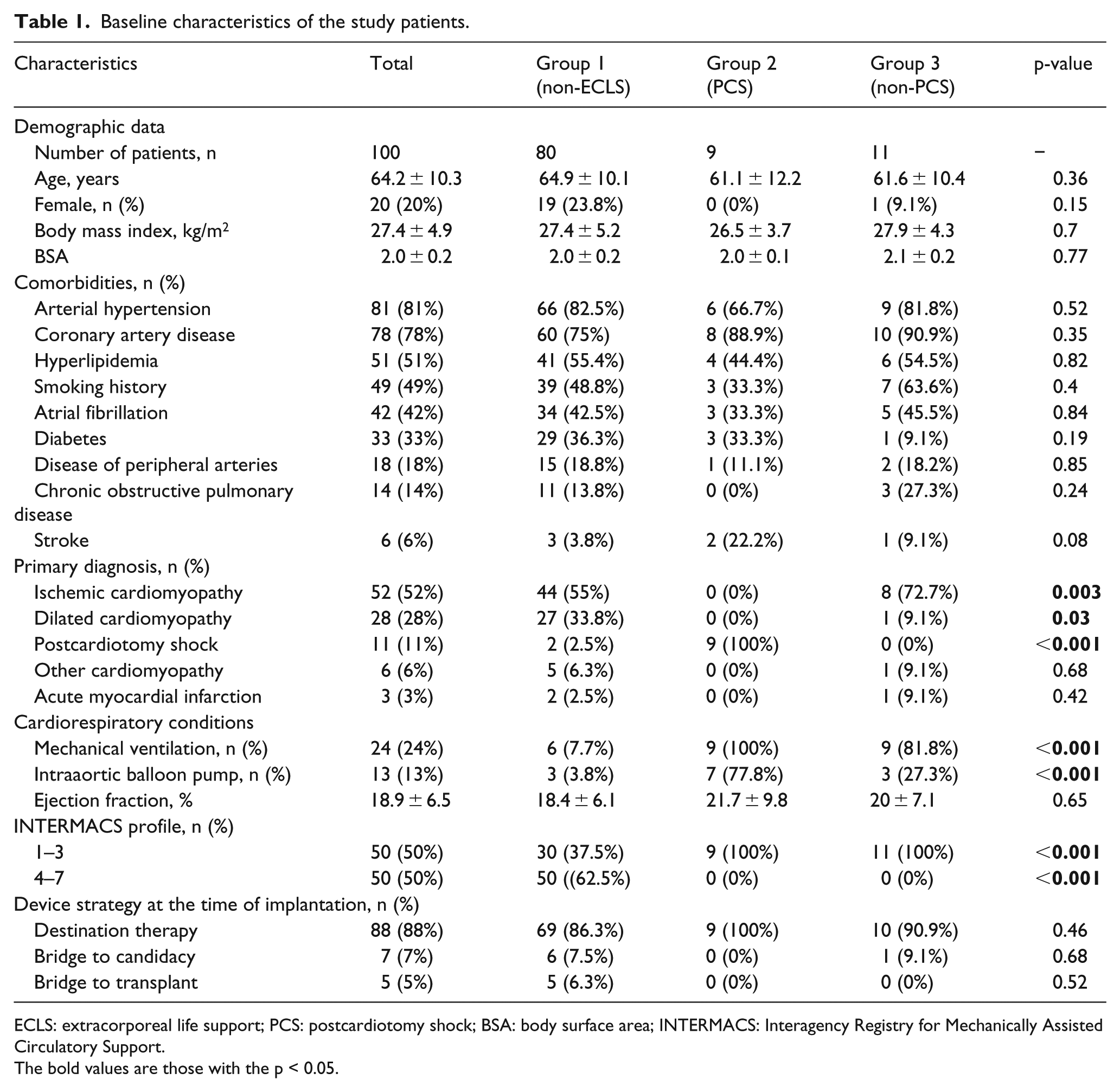
ECLS: extracorporeal life support; PCS: postcardiotomy shock; BSA: body surface area; INTERMACS: Interagency Registry for Mechanically Assisted Circulatory Support.
The bold values are those with the p < 0.05.
Preoperative laboratory parameters.
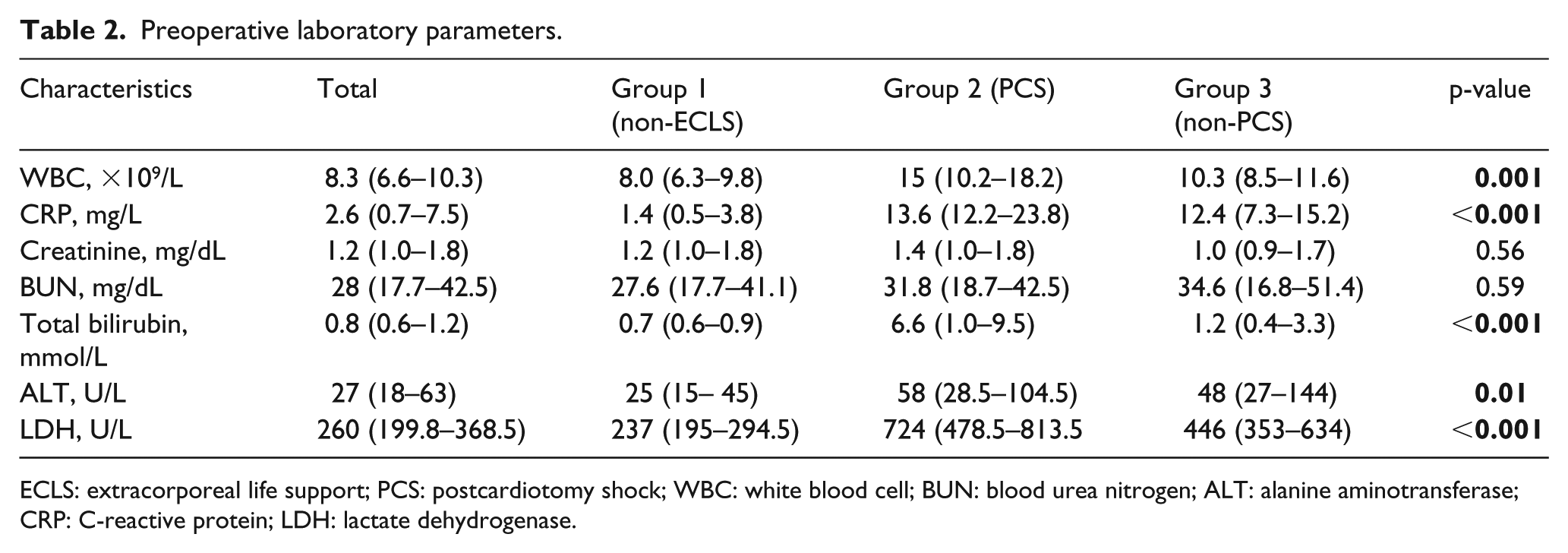
ECLS: extracorporeal life support; PCS: postcardiotomy shock; WBC: white blood cell; BUN: blood urea nitrogen; ALT: alanine aminotransferase; CRP: C-reactive protein; LDH: lactate dehydrogenase.
The median length of ECLS bridge pre-LVAD was 5 days (interquartile range 3—8 days). In PCS group, ECLS was implanted intraoperatively in seven patients (77.8%) and postoperatively in two patients (22.2%). The previous surgery leading to PCS was distributed as follows: coronary artery bypass grafting—six patients (66.7%), aortic valve replacement, mitral valve replacement, and removal of a left ventricular thrombus—one patient (11.1%), respectively. Among groups 2 and 3, a central ECLS was performed in 12 patients (60%) and a peripheral ECLS in 8 patients (40%). We used an additional left ventricular vent in six patients with central ECLS.
Intraoperative data
There were no significant differences in procedure durations, distribution of LVAD models, and concomitant procedures between the groups (Table 3).
Intraoperative data.
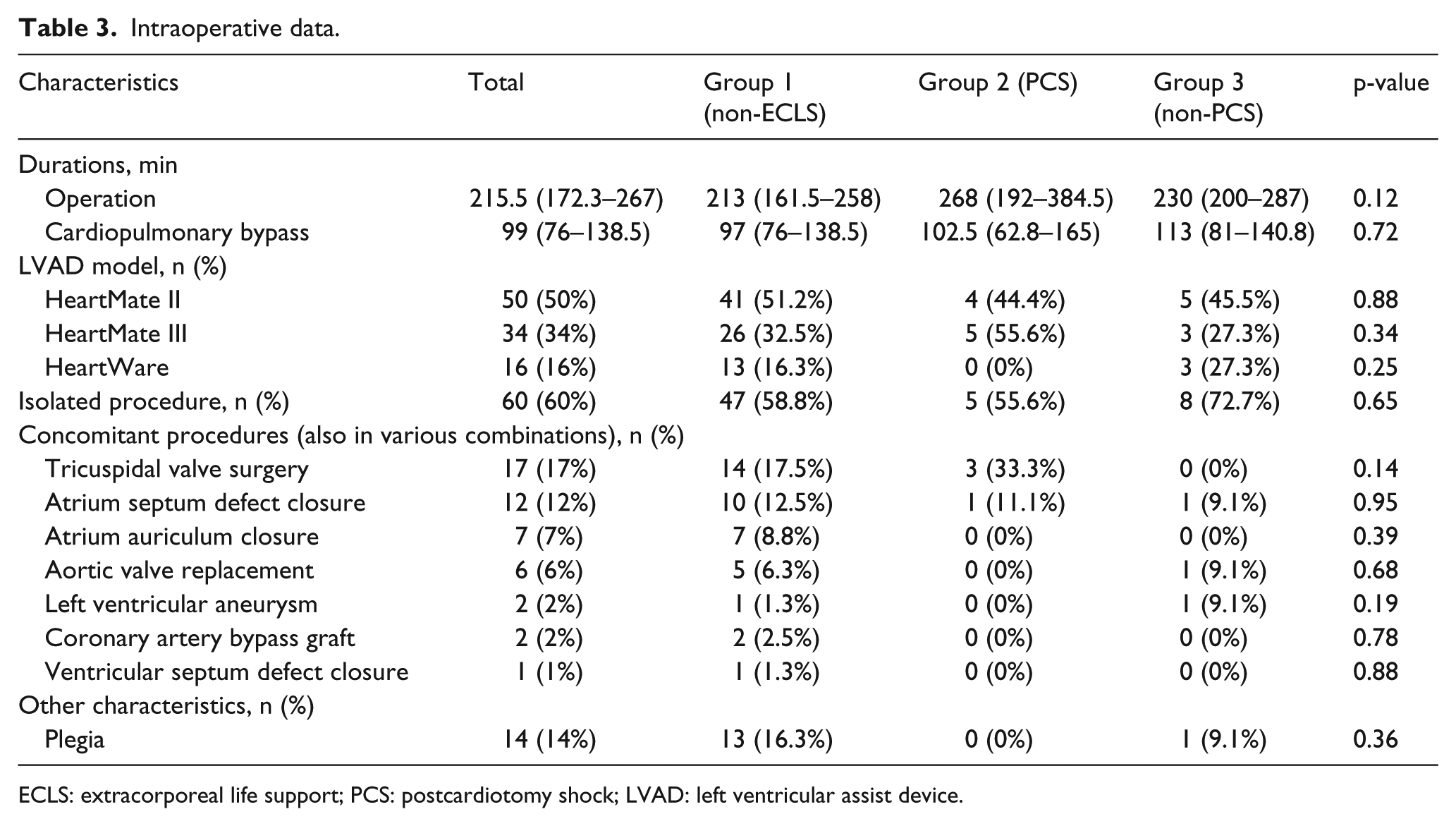
ECLS: extracorporeal life support; PCS: postcardiotomy shock; LVAD: left ventricular assist device.
Survival data and adverse events
There was a significant difference in the survival rates for groups 1 and 2 in hospital, at 30 days, 1 year, 2 and 5 years after surgery; furthermore, there were differences regarding the cause of death (COD): group 2 showed a higher rate of infection, and groups 2 and 3 showed a higher rate of multiorgan failure as COD (Table 4). Figure 1 depicts the Kaplan–Meier estimate of overall survival comparing groups.
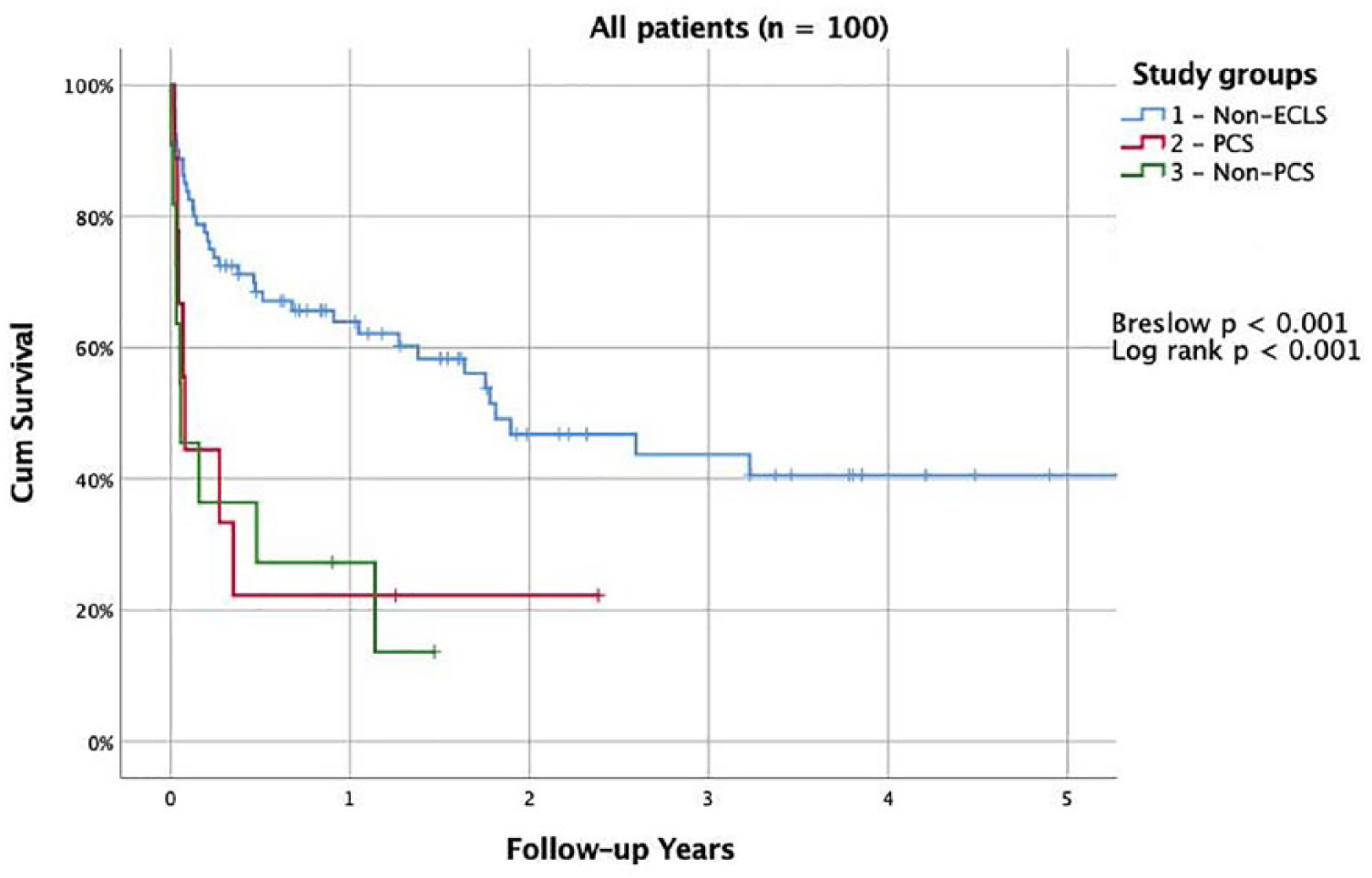
Kaplan–Meier survival estimate comparing groups 1–3.
Survival data.
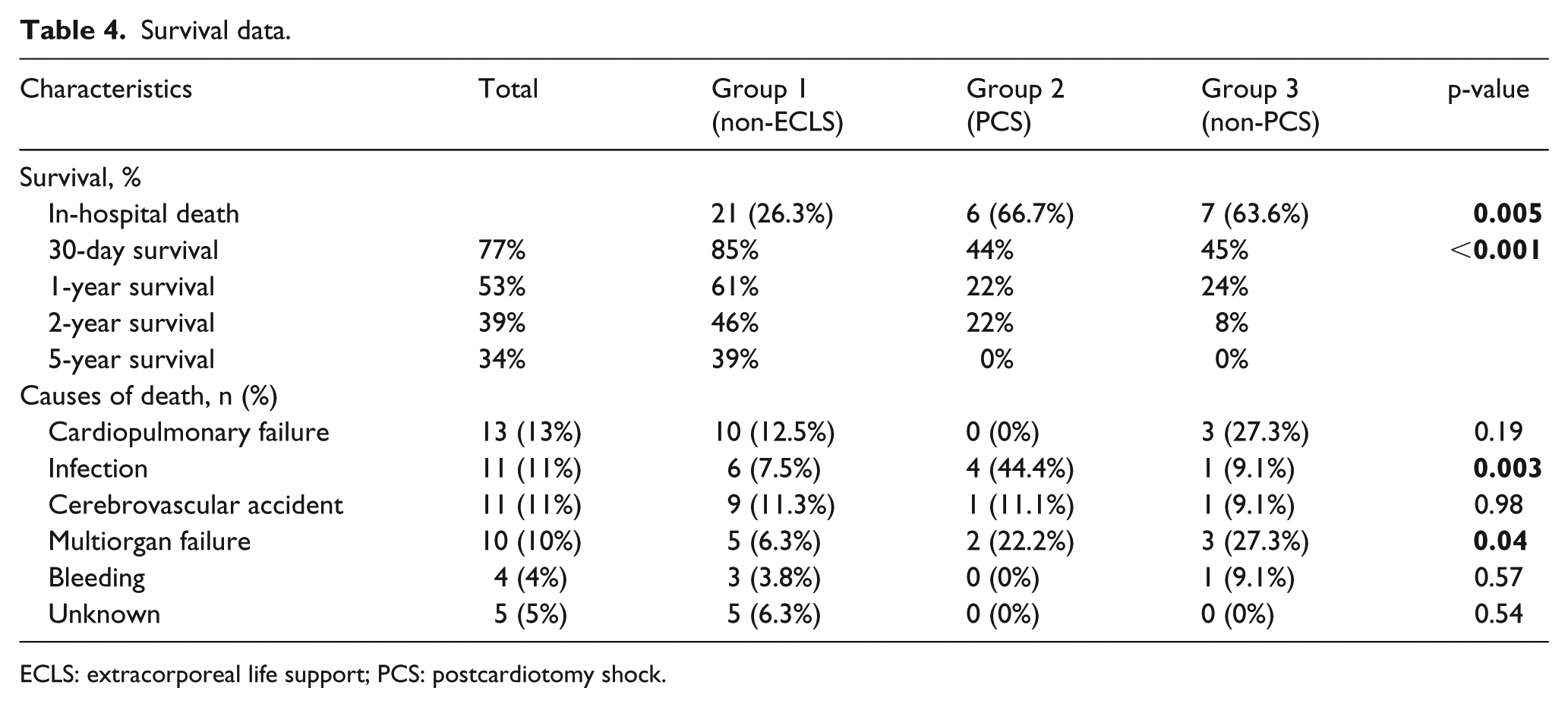
ECLS: extracorporeal life support; PCS: postcardiotomy shock.
There was a higher incidence of postoperative sepsis in group 2; the incidence of respiratory failure, RHF, hepatic dysfunction, acute renal dysfunction, and an intensive care unit length of stay were significantly higher in groups 2 and 3 (Table 5).
Major adverse events and ICU length of stay.
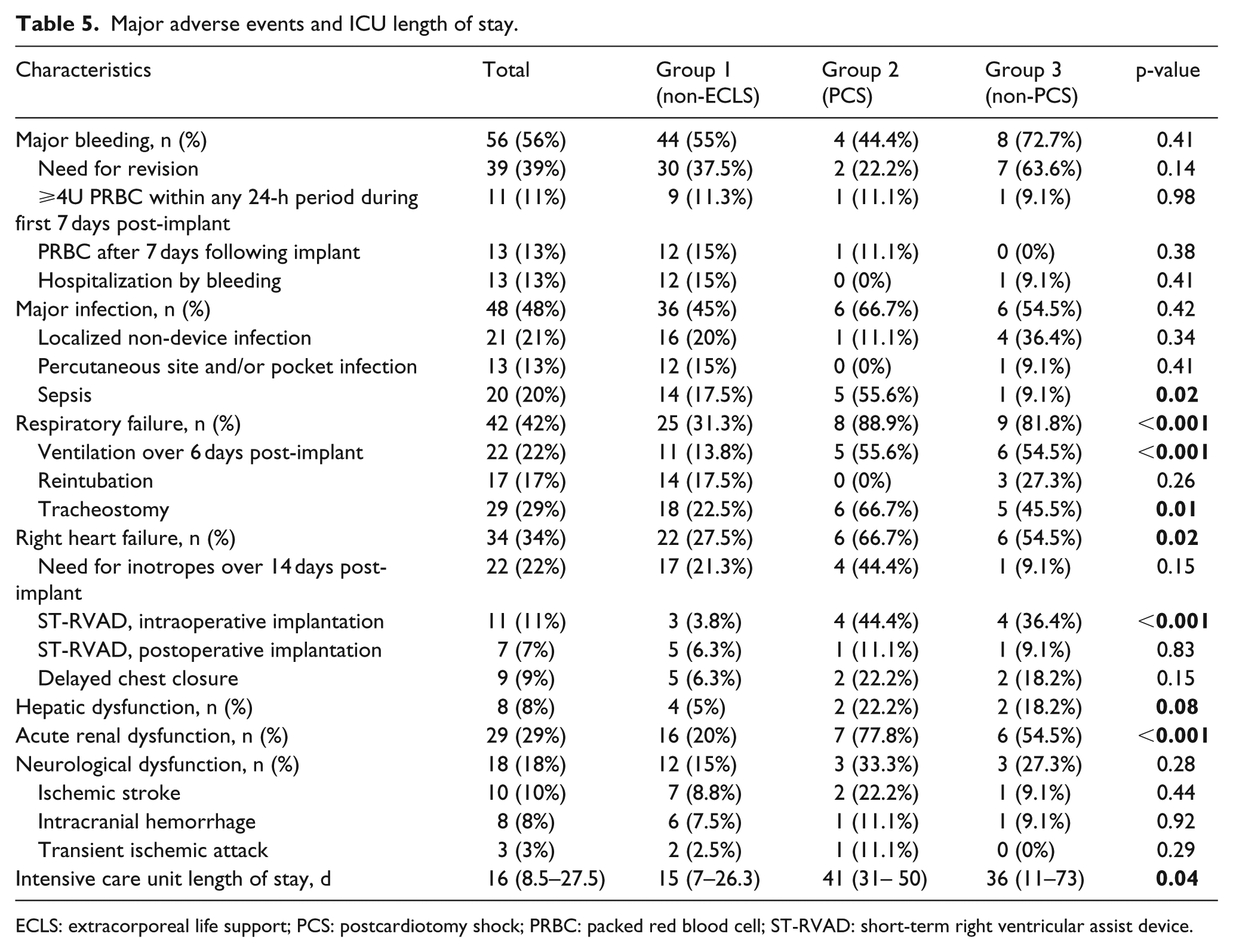
ECLS: extracorporeal life support; PCS: postcardiotomy shock; PRBC: packed red blood cell; ST-RVAD: short-term right ventricular assist device.
Discussion
LVAD implantation expands continuously as a therapeutic option in HF patients. 10 However, there are still no special guidelines for pre-, intra-, and postoperative management of long-term MCS, only several chapters with recommendations in the guidelines for management of HF. This study was conducted to expand still insufficiently accumulated evidence to consequences of ECLS bridge strategy before LVAD implantation.
The acceptance of LVAD support as DT led to a broad distribution of this procedure in non-transplant low-volume centers, and less selected patients received LVADs. 11 One of the most challenging subgroups of LVAD recipients is that with patients who were bridged with short-term MCS, such as ECLS. Those patients were previously associated with worse outcome. 12 In our study, the baseline characteristics showed expectedly significant differences between non-ECLS group 1 and more sicker ECLS groups 2 and 3.
An additional left ventricular decompression was used in half of the patients with central ECLS. This technique was found beneficial to avoid pulmonary edema, left heart distension and facilitate myocardial recovery in refractory CS. 13 Three different LVAD models were included in our study. Most patients received the axial-flow HM 2, as the placement of the centrifugal pumps, HM III and HVAD, started in 2015 in our institution. The evaluation period stretched throughout 7 years. This limiting factor might be potentially a source of criticism. However, as previously published by our group, 14 the device implanted in the examined cohort had no significant effect on the outcome.
The patients in ECLS bridge groups received LVAD either with CPB or directly on ECLS support without converting to CPB. Abdeen et al. 15 demonstrated that the CPB machine could be safely omitted when a long-term VAD is implanted on veno-arterial extracorporeal membrane oxygenation (VA-ECMO) support, with similar survival rates between both strategies.
We have seen significantly higher mortality and morbidity rates in ECLS groups 2 and 3. Group 2 included PCS patients. The reported in-hospital mortality of the PCS patients remains high, consistently over 50%, despite ongoing refinements of MCS technology. 16 The mortality of PCS was previously described as much higher than that of any other CS etiologies. 17 PCS was also found to be an independent predictor of mortality in other studies describing CS. 18 Group 3 represented with CS patients caused mostly due ischemic cardiomyopathy and myocardial infarction. The mortality of CS with ECLS support was also reported high, and CS remains the leading cause of death in patients hospitalized because of myocardial infarction. 19 However, the use of ECLS in CS was associated with an absolute increase in survival compared with patients in which ECLS was not used. 20
The 30-day mortality and during the follow-up period as well as the adverse events rates are higher in our group than those in the INTERMACS and European Registry for Patients with Mechanical Circulatory Support (EUROMACS) registries, 3 , 21 but this has several reasons due to the extremely high preoperative risk in our patients compared to the patient population captured in the above-mentioned databases. While patients with INTERMACS class I only comprised 15.2% of the INTERMACS registry and 12% of the EUROMACS registry, this subgroup of patients comprised 24% of our patients. Moreover, 20% needed preoperative ECLS. All those factors were found to be reliable predictors of mortality and morbidity after LVAD implantation.
The evidence of other significant previous studies is controversial to our findings. On the other hand, there is a lack of evidence for ECLS bridge pre-LVAD in PCS patients with status after conventional cardiac surgery; most studies evaluated ECLS support in shocked patients without previous cardiac intervention. Marasco et al. 22 conducted a retrospective review for 58 patients implanted with continuous-flow left ventricular assist device (CF-LVAD); 23 required ECLS support pre-LVAD while 35 patients underwent LVAD implantation without an ECLS bridge. The ECLS group was noticeable with increased postoperative intensive care duration, blood loss, blood product use, and postoperative renal failure, but without negative impact on survival when compared with the no ECLS group.
Han et al. 23 performed a retrospective review of patients who received CF-LVADs. Subjects were INTERMACS class 1 patients divided into ECMO bridge (18 patients) and non-ECMO bridge (17 patients) cohorts. There was no difference in rates of adverse events. Survival at 30 days postoperative and 1 year was similar. Schibilsky et al. 24 presented a 30-day survival of 93.3% in 15 patients on ECLS therapy for CS prior to LVAD implantation. The survival at the end of the study (follow-up 810.7 ± 338.9 days) was 86.7%.
Ljajikj et al. compared 30-day and 1-year mortality of patients who underwent LVAD implantation after extracorporeal cardiopulmonary resuscitation (CPR) with the aid of an ECLS system (CPR+ group; n = 40) with CS patients in which the ECLS system was implanted under non-CPR conditions (CPR– group, n = 68). The CPR+ group was associated with higher 30-day and 1-year mortality (p < 0.05). Lebreton et al. reported a non-inferiority of the ECLS pre-LVAD concept. They analyzed 97 patients assisted by various long-term MCS. The implantation was the first-line intervention in 48 patients and was performed after a period of ECLS support in 49 others. The long-term survival rate was 51.6%, with a mean follow-up of 30.7 months, and there were no differences for biological parameters between the two groups. Popov et al. 25 presented a 76% mid-term survival rate after CF-LVAD implantation in patients with end-stage HF.
Weymann et al. showed in their cohort of patients a safe usage of ECLS in critical CS as a bridge to implantation of the Berlin Heart Excor ventricular assist device. This was associated with improvement in end-organ function leading to similar excellent early and long-term survival and incidences of major complications as in patients without the need for preoperative ECLS support. 26
Study limitations
This study is a retrospective non-randomized analysis of a relatively small number of CF-LVAD patients from a single medical center over a span of 7 years. Clinical decisions were made in a nonblinded fashion.
Conclusion
In our cohort of patients, CF-LVAD implantation with prior short-term ECLS therapy appears to have a worse outcome regarding survival, RHF, renal and respiratory dysfunction (p < 0.05). Future studies have to be done to evaluate the outcome after ECLS bridge pre-LVAD, especially as ultima ratio in PCS patients.
Footnotes
Acknowledgements
K.Z.: conception and design, data analysis and interpretation, manuscript writing, final approval of manuscript. M.S., A.M., S.M., D.S., S.E.: data collection, analysis and interpretation, manuscript writing. J.E., J.E., H.C.E., A.W.: surgical team, final approval of manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.