
Abstract
Background:
Cardiogenic shock is associated with significant mortality, morbidity, and healthcare cost. Utilization of extracorporeal membrane oxygenation in cardiogenic shock has increased in the United States. We sought to identify the rates and predictors of hospital readmissions in patients with cardiogenic shock after weaning from extracorporeal membrane oxygenation.
Methods:
Using the 2016 Nationwide Readmission Database, we identified all patients (⩾18 years) with cardiogenic shock (ICD-10 CM R57.0) that have been implanted with extracorporeal membrane oxygenation (ICD-10-PSC of 5A15223) and were discharged alive (January–November 2016). We explored the rates, causes, and predictors of all-cause readmissions within 30 days.
Results:
Out of 69,040 admissions with cardiogenic shock, 1641 (2.4%) underwent extracorporeal membrane oxygenation (581 were implanted during or after cardiac surgery). A total of 734 (44.7%) patients of all extracorporeal membrane oxygenations survived to discharge, and 661 were available for analysis. Out of those, 158 (23.9%) were readmitted within 30 days of discharge. More than 50% of these readmissions happened within the first 11 days. Out of 158 patients who were readmitted, 12 (7.4%) died during the readmission hospitalization. Leading causes of readmission were cardiovascular (31.6%) (heart failure: 24.1%, arrhythmia: 20.6%, neurovascular: 10.3%, hypertension: 10.3%, and endocarditis: 6.8%), followed by complications of medical/device care (17.7%), infection (11.3%), and gastrointestinal/liver (10.1%) complications. Factors associated with readmissions include the following: discharge to skilled nursing facility or with home healthcare (odds ratio: 2.10; 95% confidence interval: 1.18–3.74), durable ventricular assisted device implantation, asthma, and chronic liver disease.
Conclusion:
Patients with cardiogenic shock who underwent extracorporeal membrane oxygenation had a readmission rate. Identifying patients at high risk of readmissions might help improve outcomes.
Introduction
Despite improvements in heart failure therapies, cardiogenic shock (CS) remains associated with notable morbidity, mortality, and healthcare costs. Extracorporeal membrane oxygenation (ECMO) is increasingly utilized for management of refractory CS.1,2 Mortality of CS remains high, especially for patients treated with ECMO approaching 35%–60%.3–6
In addition to considering the morbidity and mortality from disease processes and related treatment modalities, there is a continued emphasis on reducing readmission rates. 7 Evidence of such emphasis can be seen in the practice of using readmission as a measure of quality, which is a practice utilized by the Centers for Medicare and Medicaid Services. 8 While morbidity (such as bleeding, neurological, and vascular complications) and mortality related to ECMO have been assessed previously,2,9,10 readmissions among patients successfully weaned from ECMO are not well studied. With increasing efforts nationally to employ advanced therapies, such as ECMO, as treatment for CS, it is important to consider the factors that may contribute to and predict hospital readmissions. Delineating these factors may help to improve outcomes in this patient population.11,12 Therefore, we sought to identify the rates, causes, and predictors in readmissions in patients weaned from ECMO for CS.
Methods
Data set
The study cohort was derived from the 2016 Healthcare Cost and Utilization Project National Readmission Database (NRD), supported by the Agency for Healthcare Research and Quality. NRD is part of a family of databases and software tools developed for the Healthcare Cost and Utilization Project (HCUP). NRD contains data from approximately 17 million discharges each year. Weighted, it estimates roughly 36 million discharges. The patients can be tracked using unique linkage number. Patients’ admissions, length of stay, comorbidities, and procedures are reliably linked in the database.
Study population
We queried the NRD database for all adults (age ⩾ 18 years), and who have a diagnosis of CS (ICD-10 CM R57.0), who were discharged alive between January and November 2016. December discharges were excluded to allow sufficient time for 30-day follow-ups (Figure 1). The index admission was defined as the first admission with CS in 2016. We identified patients who underwent ECMO in the same hospitalization (ICD-10-PCS 5A15223), all 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10) codes are shown in Supplemental Table 2. We describe baseline characteristics and hospitalization events, procedures during index hospitalization, readmission within 30 days, and the primary diagnosis of readmission. Age, sex, discharge disposition, quartile of household income by ZIP code of residence, primary payer, admission status, length of stay, cost of stay, and admission day were available from the NRD database.
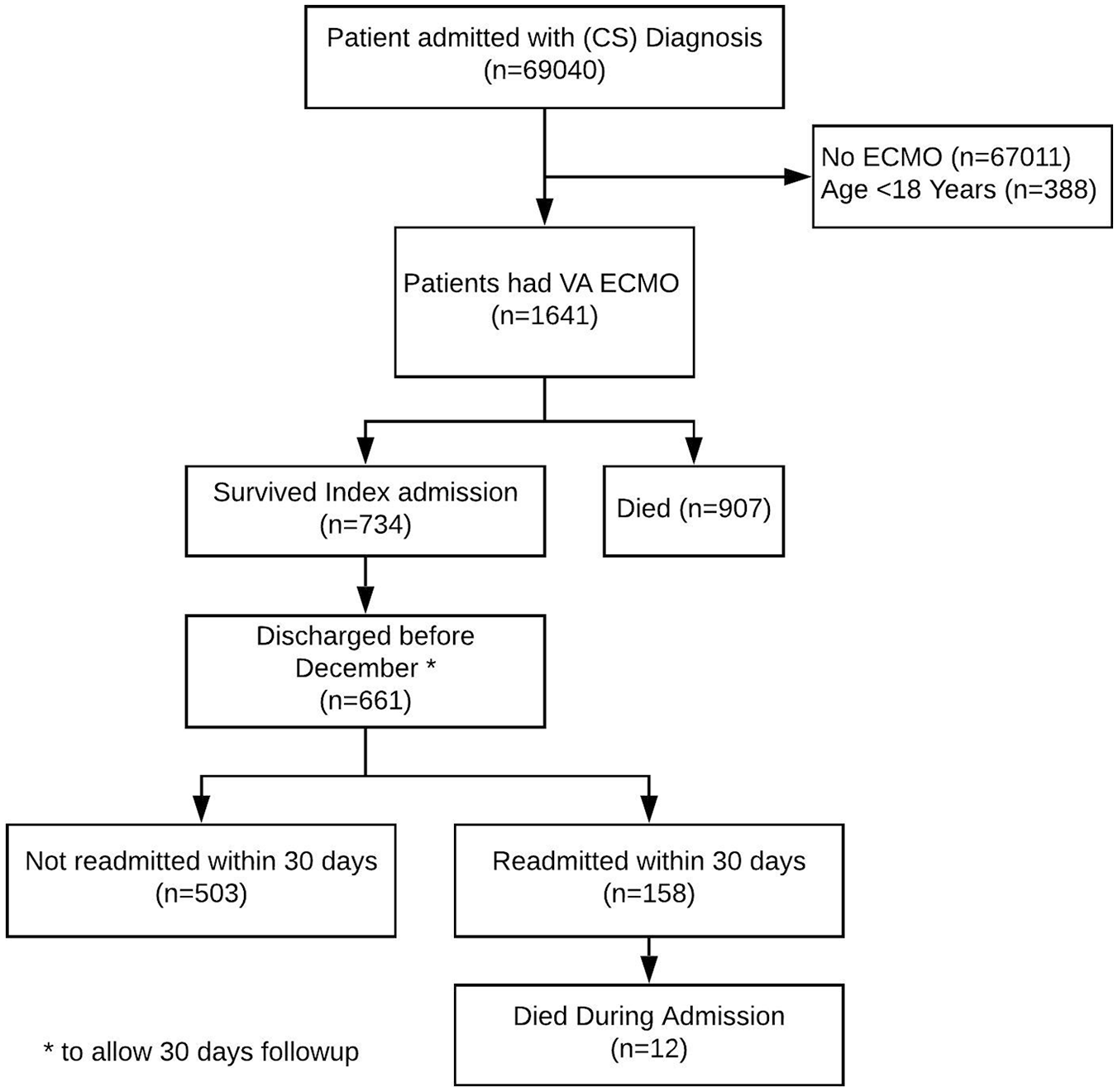
CONSORT diagram.
Outcomes
The primary outcome was 30-day readmission postdischarge from the index admission. Secondary outcomes include readmission primary diagnosis, length of stay, hospital charges, and inpatient death.
Statistical analysis
Categorical data are expressed as counts and percentages, continuous variables as mean ± standard deviations or median and interquartile range as appropriate. Categorical variables were compared using chi-square tests, and continuous variables were compared using t-test. Predictive modeling was done using multivariate logistic regression with forward variable selection (p < 0.05). All tests are two-sided and p < 0.05 was considered statistically significant. Statistical Package for Social Sciences (SPSS, version 24.0, IBM) was used for analyses.
Results
Baseline characteristics for patient who underwent ECMO
Out of 69,040 CS admissions, 1641 (2.37%) were supported with ECMO (Figure 1). A total of 581 (35.4%) patients were placed on ECMO after cardiac surgery: valve replacement (n = 250, 43%), coronary artery bypass surgery (CABG) (n = 177, 30.5%), ventricular assist device (VAD) place-ment (69, 11.9%), or other cardiac surgery (n = 85, 14.6%) (Figure 2). Mean age of patients who underwent ECMO was 55.74 ± 14.8 years. Median length of stay for index admission was 17 (6–36) days, 551 (33.6%) were females, and 248 (15.1%) were electively admitted initially. Median hospital charges of the index admission were (US$586,727). Median admission day to ECMO placement was 2 days. In this cohort, 267 (16.3%) patients had percutaneous left ventricular assist device (pLVAD) support and 512 (31.2%) had intra-aortic balloon pump (IABP) support. A total of 386 (23.5%) of these temporary mechanical support devices were placed after ECMO placement (Figure 3). Out of patients who underwent ECMO, 734 (44.7%) survived their index admission.
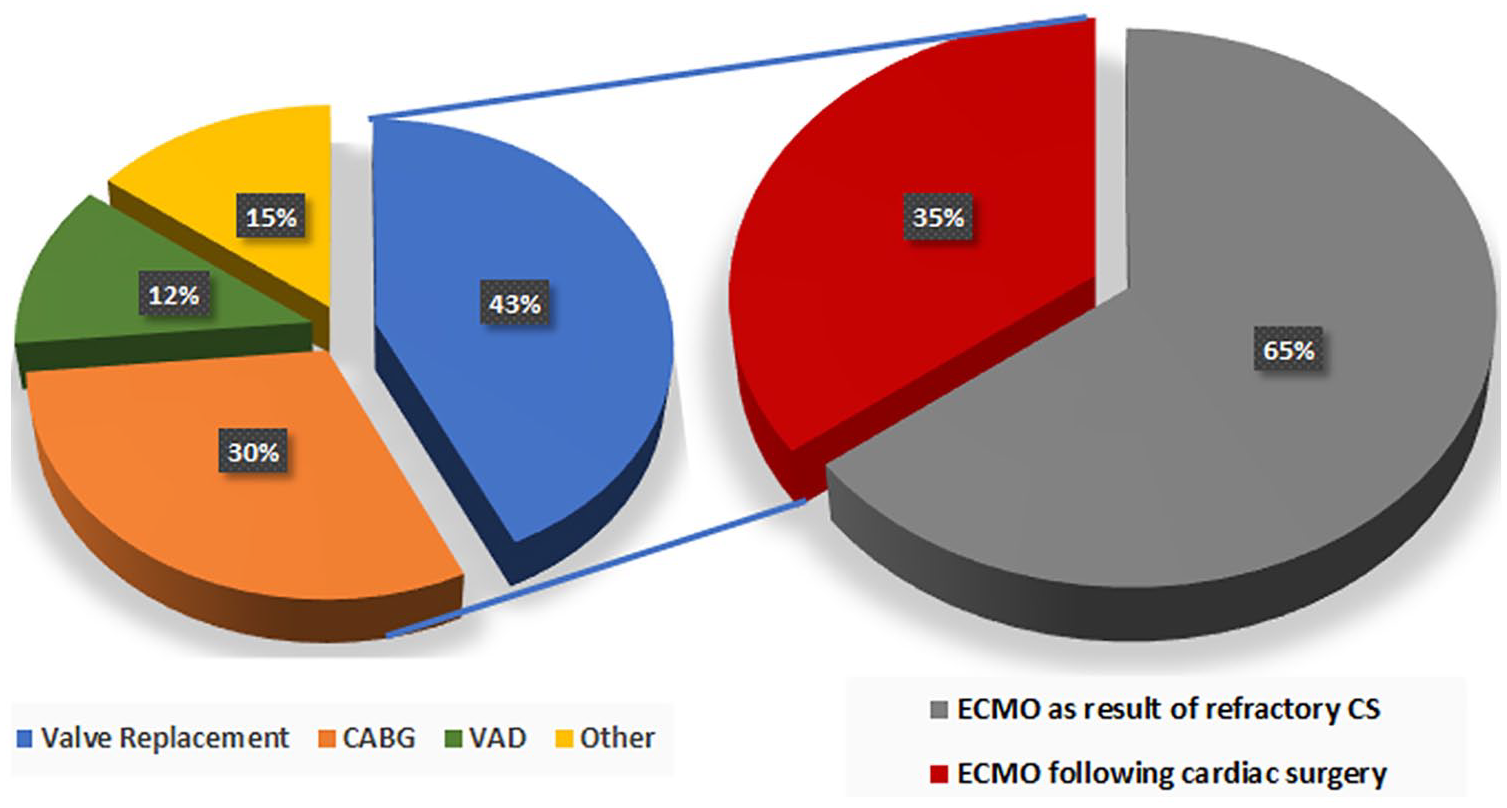
Distribution of cardiac surgery occurring during the index hospitalization for patients admitted with cardiogenic shock and received extracorporeal membrane oxygenation (n = 1641).
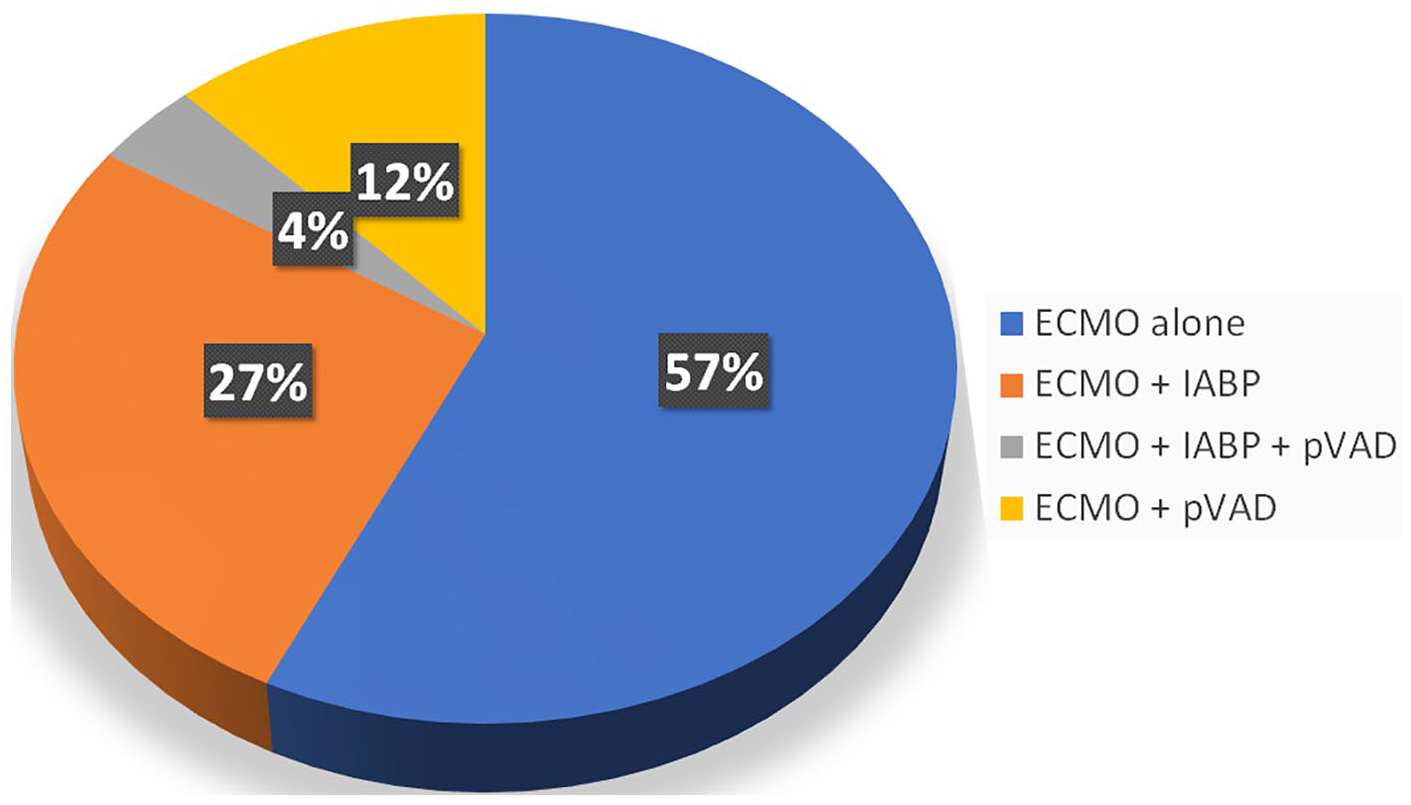
Mechanical support device utilization among CS patients implanted with ECMO (n = 1641).
Thirty-day readmission, cause, cost, and length of stay
A total of 661 patients who survived their index admission and were discharged before December 2016 were included for analysis of readmissions. Of these 661 patients, 158 (23.9%) were readmitted within 30 days.
More than 50% of these readmissions happened within the first 11 days after discharge (Figure 4). There was no difference in readmission rates between patients discharged from higher (>median of 23/year) and lower (⩽median of 23/year) ECMO volume centers (23.9% vs 23.9%, p > 0.99). Twelve patients (7.4%) died during rehospitalization.
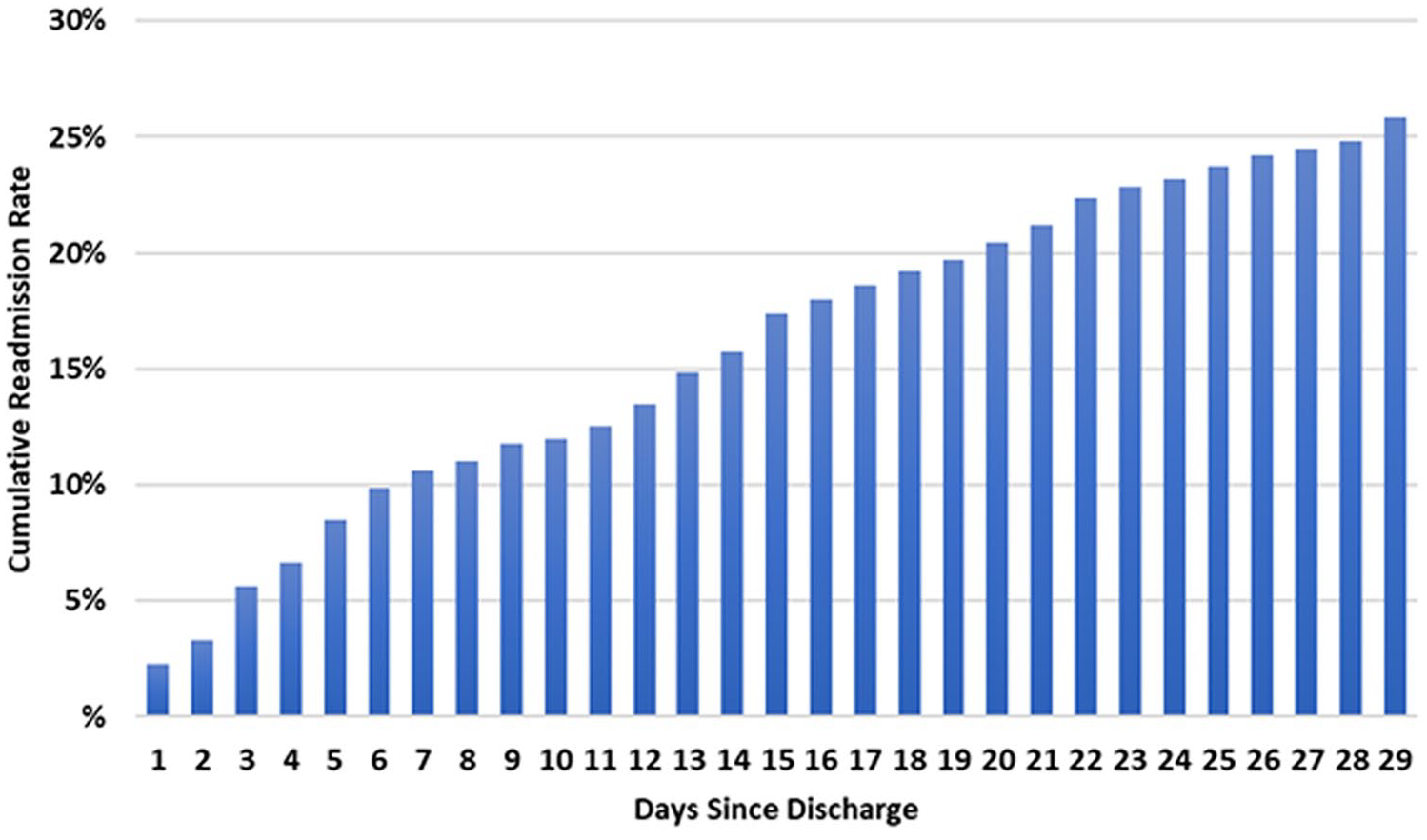
Cumulative incidence of readmission postdischarge from index hospitalization.
The median length of stay for readmission was 7 (4–14) days, and 20 (12.7%) of these readmissions were elective. Median hospitalization charges for readmission were US$72,715. Table 1 shows the characteristics of patients with or without 30-day readmission. Patients with index admissions longer than 30 days, who underwent left ventricular assist device (LVAD), had vascular complications, or were discharged to skilled nursing facility (SNF) or Home Care with agency were more likely to be readmitted. There was no difference between patients who had mechanical support, chronic medical conditions, ischemic versus non-ischemic etiologies, sex, age, or ZIP income quartile.
Baseline characteristics of patients who underwent VA-ECMO during the index admission.
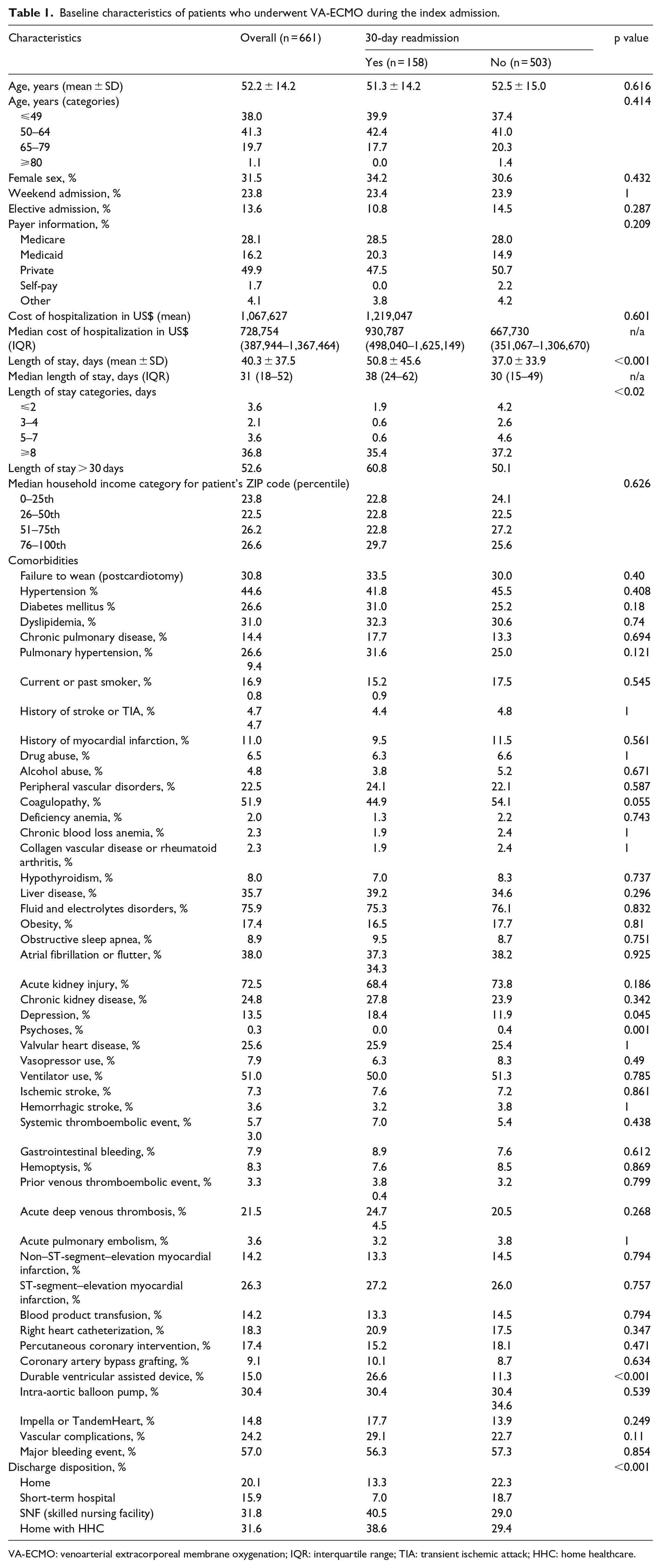
VA-ECMO: venoarterial extracorporeal membrane oxygenation; IQR: interquartile range; TIA: transient ischemic attack; HHC: home healthcare.
Leading causes of readmissions are summarized in Figure 5 as follows: cardiovascular events (31.6%) were the most prominent causes of readmission, followed by complications of medical/device care (17.7%), infection (11.3%), and gastroenteric/liver (10.1%) complications. Cardiovascular readmission causes were further characterized as follows: heart failure (24.1%), arrhythmia (20.6%), neurovascular (10.3%), hypertension (10.3%), and endocarditis (6.8%) (Figure 5).
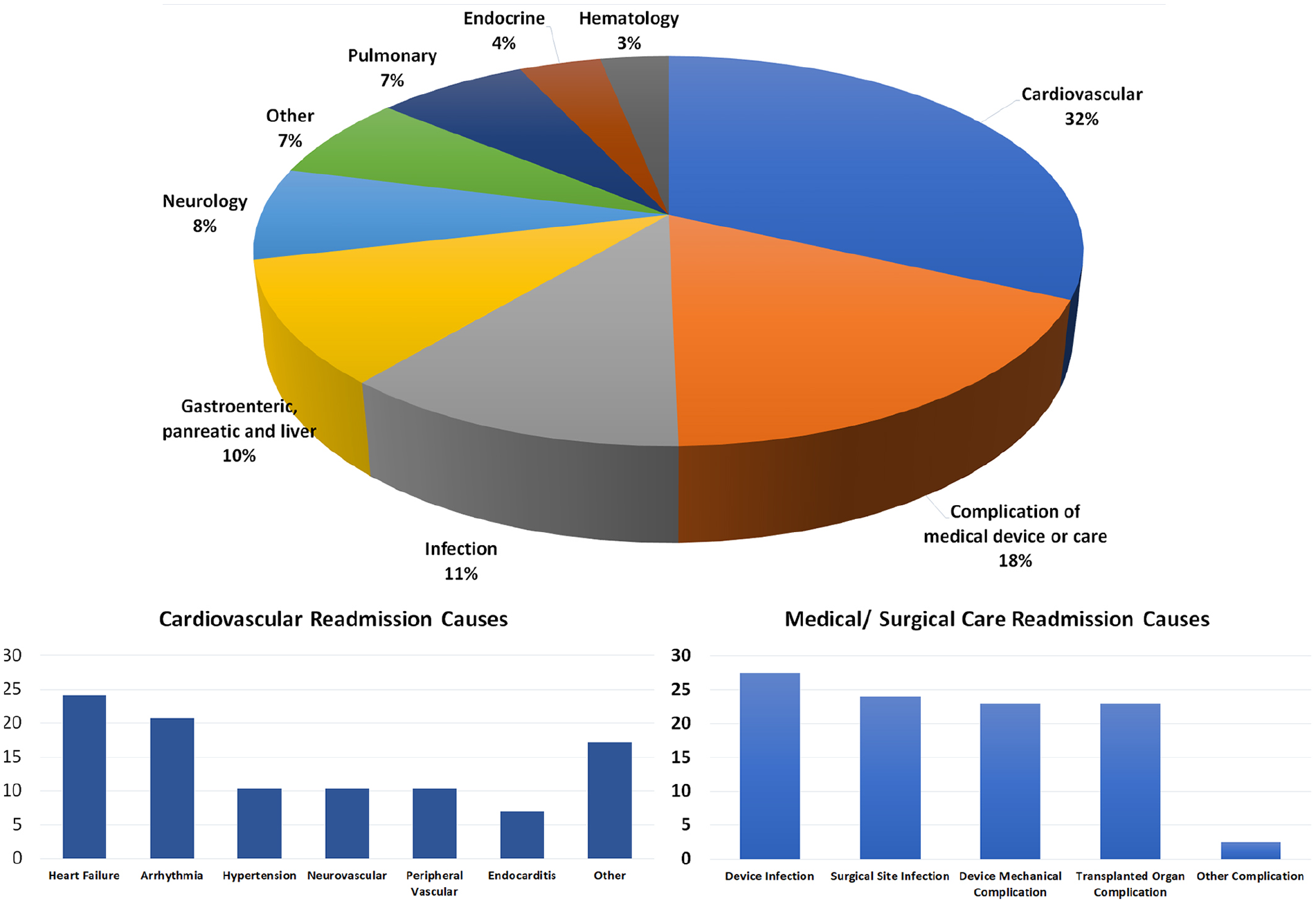
Primary diagnosis of 30-day readmissions.
Predictors of 30-day readmission
In multivariate analyses, among those who survived to discharge, discharge to SNF (odds ratio (OR): 2.50; 95% confidence interval (CI): 1.41–4.44; p < 0.002) or with home healthcare (OR: 2.10; 95% CI: 1.18–3.74; p < 0.001), durable VAD implantation (OR: 2.66; 95% CI: 1.64–4.31; p < 0.001), asthma (OR: 2.32; 95% CI: 1.00–5.37; p < 0.049), and chronic liver disease (OR: 2.68; 95% CI: 1.21–5.97; p < 0.01) were associated with 30-day readmissions. Figure 6 shows the independent predictors of 30-day readmissions after index admission for CS. A separate analysis for LVAD versus non-LVAD patients is included in Supplemental Table 2.
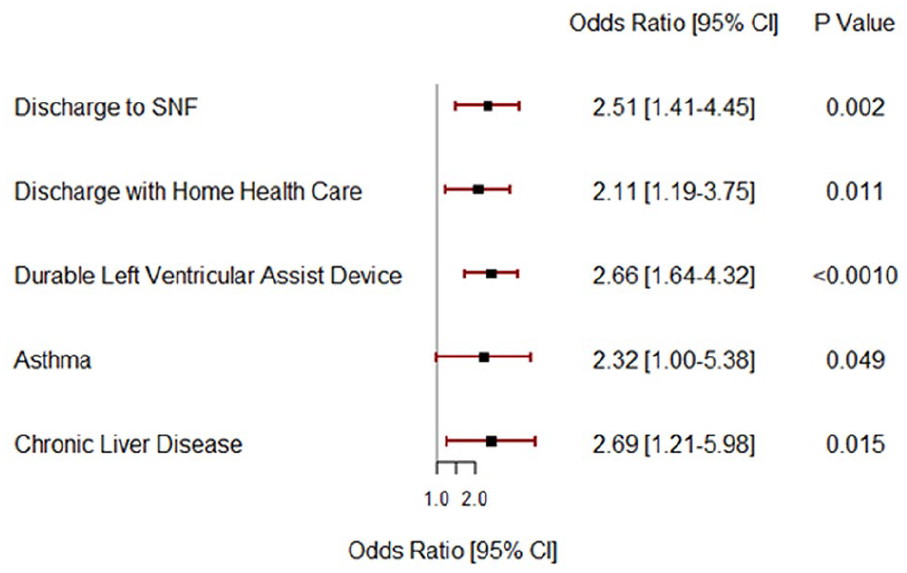
Independent predictors of 30-day readmission after index admission for cardiogenic shock requiring ECMO implantation.
Discussion
To our knowledge, this is the largest study to investigate the rates and causes of readmissions among patients weaned from ECMO for CS. We found that 24% of patients who are discharged alive are readmitted within 30 days. The majority of these admissions were due to cardiovascular causes, especially worsening heart failure and arrhythmia. Readmissions were associated with high inpatient mortality (7%) and charges (approximately US$70,000). Factors associated with readmissions include discharge to SNF, home care, durable LVAD implantation, asthma, and chronic liver disease.
Although CS represents a small percentage of all heart failure patients, the mortality rate can be well over 50% and the cost to treat these patients is often exorbitantly high, with readmission rates well above the all-cause rates for both Medicare and commercial populations.13–15 One of the principal methods for restoring hemodynamic stability in CS patients is via mechanical hemodynamic support, which was traditionally achieved with IABP, percutaneous LVAD, or if necessary, ECMO.16,17 There has been a substantial increase in the use of ECMO for management of refractory CS in the past decade. For example, the rate of ECMO cases per million adult discharges increased 433% from 11.4 in 2006 to 60.9 in 2011. 18 Thirty-day readmission is a measure used by the Centers for Medicare and Medicaid Services to gauge hospital performance as readmissions are associated with high cost, morbidity, quality of life, and poor long-term outcomes. Thus, it is important to identify patients who are at high risk of readmissions and allocate resources to reduce this risk.
Previous studies based on nationwide registry data showed an overall 30-day readmission rate of 20.3% in patients with acute myocardial infarction complicated by CS 11 and 22.6% 30-day readmission rate for patients with non-AMI associated CS. 19 This study shows that the 30-day readmission rate for patients with CS who underwent venoarterial extracorporeal membrane oxygenation (VA-ECMO) was 23.9%. This higher readmission rate is expected, considering the extreme severity of illness for patients who usually undergo VA-ECMO. In an analysis of 132 Medicare patients with CS treated with ECMO between 2011 and 2012, 34.1% were readmitted within 30 days. 20 In another analysis of ECMO survivors 2007–2015 in Pennsylvania state hospitals, Huesch et al. 1 found that 43.8% were readmitted within 30 days. The readmission rates in these two studies are considerably higher than the 30-day readmission rate (23.9%) observed in our study. This difference between the studies is likely due to sicker patient population included in the prior studies as it was restricted to Medicare population, but it can also indicate improved outcomes in CS patients treated with ECMO.2,18
We show that cardiovascular causes accounted for 32% of readmission principal diagnosis. Similar findings were outlined among several studies that looked at CS readmissions.11,19 Among the cardiovascular reasons, heart failure was the leading cause of readmissions followed by arrhythmia and hypertension; similar findings were found in comparable studies.11,15,19 Given that these patients undergo invasive procedures and LVAD implantation/heart transplantation, the second major cause of readmission was complications of medical care/surgical procedures (including but not limited to LVAD infection, transplant rejection, surgical site infection, etc.). These areas represent a potential for improvement by establishing closer follow-up after discharge and enhancing care during admission. The third leading cause of readmission was infectious etiologies; this was also similar to finding in prior studies.11,12,19 Patients with healthcare-associated infections are at increased risk of rehospitalization across all medical conditions including surgical and non-surgical hospitalizations. This has a significant impact on health outcomes and should be addressed with improved infection prevention efforts. 21
Discharging patients to SNF or with home healthcare was associated with higher 30-day readmission rate. This is likely due to the poor functional status and inadequate social support for patients who were discharged to SNF or with home healthcare. This finding offers an important opportunity to reduce readmissions in this high-risk population. Closer follow-ups, SNF specialty care, and telemonitoring should be studied in this population to improve outcomes. Long-term VAD was also a significant predictor of higher 30-day readmission rate. Patients with long-term VAD are at higher risk of readmission both from cardiovascular and non-cardiovascular causes including infection, bleeding, and device-related complications, 22 especially early after implantation.
As a result of our study outcomes, we believe that follow-up is essential in the care pathway for ECMO patients. Given that some of the most common causes of readmission are heart failure, arrhythmia, infection, and rejection, close follow-up care for a patient discharged status-post-ECMO could include regular office visits, frequent home nursing visits, and/or follow-up phone calls with the purpose of evaluating the patient for early signs and symptoms associated with these causes of readmission. For patients discharged from the hospital after successful ECMO decannulation, monitoring for and detection of the early signs and symptoms of complications may be able to reduce readmission rates. If readmission rates are reduced, overall financial burden of ECMO utilization may be reduced.
ECMO utilization is associated with high costs. Our study demonstrated an initial admission mean cost of (US$586,727) over a median length of stay of 31 days or (US$18,927) per day. As nearly one-quarter of patients who received ECMO after CS were subsequently readmitted, the additional cost of readmission (US$72,715) should be considered when determining the overall financial burden of ECMO. Prior studies have demonstrated that alternatives to ECMO (e.g. percutaneous ventricular assist device (pVAD)) may be associated with lower cost when combined with readmission costs. 20 Given the high financial burden of ECMO, there is a need for a model that accurately predicts patient outcome and better selection of patients in order to reduce readmissions and ultimately lower cost.
Limitations
This study had potential limitations that should be considered. First, this is a retrospective analysis of a national administrative data set, with its inherent limitations related to coding and reporting. The ICD-10 code that was used to define ECMO did not differentiate between veno-venous ECMO and VA-ECMO, and included both centrally and peripherally placed ECMOs. The use of concomitant code for CS makes VA-ECMO much more likely. Second, the data set lacks essential data to identify level of illness such as hemodynamics, laboratory values, weaning from ECMO circumstances, and medications used. Third, we did not have information on out-of-hospital deaths, which may underestimate the 30-day readmission rates. Because of the calendar year reporting of the NRD, this study did not examine data on long-term outcomes beyond 30 days, which would be a potential target for future studies.
Conclusion
Patients with CS who underwent ECMO had significant readmission rates within 30 days, mainly due to cardiovascular diseases and complications of index hospitalization. Readmissions are associated with high cost and mortality. Identifying high-risk patients may help establish methods to improve outcomes.
Supplemental Material
Supplemental_table – Supplemental material for Causes and predictors of 30-day readmissions in patients with cardiogenic shock requiring extracorporeal membrane oxygenation support
Supplemental material, Supplemental_table for Causes and predictors of 30-day readmissions in patients with cardiogenic shock requiring extracorporeal membrane oxygenation support by Nour Tashtish, Sadeer G Al-Kindi, Mohamad Karnib, Erica Zanath, Steven Mitchell, Christopher Di Felice, Michael Zacharias, Guilherme H Oliveira, Benjamin Medalion, Francis Lytle and Chantal Elamm in The International Journal of Artificial Organs
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.