
Abstract
Objective:
To determine the clinical effect of continuous hemoperfusion with Cytosorb associated with standard Continuous Renal Replacement Therapy on hemodynamics and on clinically relevant outcome parameters in children with septic shock.
Design:
Retrospective analysis.
Setting:
Pediatric intensive care unit.
Patients:
Eight consecutive children with septic shock who received hemoperfusion with Cytosorb while on Continuous Renal Replacement Therapy.
Interventions:
Continuous hemoperfusion with Cytosorb (adsorber was changed every 24 h).
Measurements and main results:
Vasoactive-Inotropic Score was measured before and after the extracorporeal blood purification treatment. Bedside refractory septic shock score was calculated before the onset of the extracorporeal blood purification treatment. Time course of cytokines interleukin-6, interleukin-10, and tumor necrosis factor–alpha was measured at Time 0, then every 12 h until the end of blood purification treatment (72 or 96 h). Pediatric intensive care unit survival in our cohort was 90%. Median bedside refractory septic shock score was 2.1. Patients showed improved Vasoactive-Inotropic Score following blood purification (pre: 40.00 post: 8.89 p = 0.0076). Measurement of cytokines level showed a significant reduction of interleukin-6 plasma levels (7977.27–210.18 pg/mL, p = 0.0077) and interleukin-10 plasma levels (from 687.19 to 36.95 pg/mL, p = 0.0180). In those patients with detectable tumor necrosis factor–alpha plasma level, its reduction was not significant (p = 0.138). The median removal ratio was 80% for interleukin-6, 90% for interleukin-10, and 29% for tumor necrosis factor–alpha.
Conclusion:
The use of Cytosorb in combination with Continuous Renal Replacement Therapy as blood purification strategy in pediatric septic shock is associated with a rapid hemodynamic stabilization in the first 48 h of treatment and a significant reduction of interleukin-6 and interleukin-10.
Introduction
Septic shock and multiple organ failure remain a leading cause of pediatric mortality worldwide. Clinical application of well-established international guidelines and the goal directed therapy has been accepted as standard practice leading to an early recognition and treatment of children with sepsis.1,2 Nevertheless, pediatric patients affected by severe septic shock, in particular those who received extracorporeal therapies such as extracorporeal membrane oxygenation (ECMO) and renal replacement therapy (RRT), still present a high mortality rate.3,4
Mortality in septic shock is related to elevated concentrations of several cytokines released during the dysregulated host response to infection. 5 The cytokines storm, in fact, plays an integral part in the collapse of the vascular system 6 and the cumulative vasopressors load in patients with sepsis is correlated with intensive care mortality, occurrence of refractory shock, metabolic acidosis, and renal failure. 7 The study of novel interventions in sepsis research takes into consideration the blood removal of harmful mediators using extracorporeal techniques. 8 An ideal therapy should mitigate the cytokines storm and be directed against both the pro-inflammatory and anti-inflammatory mediators9,10 to restore the immuno-homeostasis. In a recent meta-analysis of the various forms of blood purification, only plasma exchange and hemoadsorption appeared to be potentially effective in the treatment of sepsis. 11 Cytosorb (CytoSorbents, Corporation, New Jersey, USA) is a hemoadsorption cartridge column containing hemocompatible porous polymeric beads with a total surface area of more than 40.000 m2. It is effective in removal molecules in the 5–60 kDa range and the majority of cytokines and other inflammatory mediators fall in this spectrum. The safety profile of Cytosorb was tested in more than 5000 clinical cases. 12 The “combination” of Cytosorb in series with the hemofilter in Continuous Renal Replacement Therapy (CRRT) represent an interesting strategy to remove inflammatory mediators while treating fluid overload and acute kidney injury (AKI) in children with septic shock. In addition, many authors mention the positive effect therapy associated with ECMO.13,14
The application of Cytosorb in pediatric population as adjunctive therapy in septic shock is still limited to isolated case reports.15–17 In this retrospective study, we report our single center experience of nine consecutive treatments of hemoperfusion with Cytosorb associated with CRRT in pediatric patients with septic shock describing the impact of this adjunctive therapy on hemodynamics and on clinically relevant outcome parameters. Furthermore, trends of pro-and anti-inflammatory biomarkers (interleukin (IL)-6, IL-10, tumor necrosis factor (TNF)-alpha) during the extracorporeal blood purification treatment (EBPT) has been measured.
Material and methods
Patient selection
The study was approved by the Institutional Review Board (IRB) of Children Hospital Bambino Gesù, Rome Italy.
We retrospectively reviewed all cases of pediatric septic shock (age between 1 month and 17 years) who received hemoperfusion with Cytosorb while receiving CRRT from January 2018 to May 2019.
These data were collected as part of a hospital audit about the efficacy and the safety of hemoperfusion with Cytosorb in children with pediatric septic shock.
Septic shock was identified as defined by the International Pediatric Consensus Conference and treated following the latest guidelines of the American College of Critical Care Medicine (ACCM). 18 AKI and its stage of severity have been defined according to the Kidney Disease: Improving Global Outcomes (KDIGO) 19 criteria and indications for CRRT were fluid overload, electrolyte imbalance, or both. Hemoperfusion treatment with Cytosorb was performed as a rescue therapy within 24 h after the proved or suspected diagnosis of septic shock in case of an inadequate response to standard therapy 18 (defined by an increase of lactate concentrations and/or an increased vasopressor requirements or additional need of inotropes) after an observational period of a maximum of 6 h or immediately in parallel to standard therapy 18 in patients with refractory septic shock. 20
CRRT and hemoadsorption with Cytosorb
A hemodialysis catheter was inserted into a central vein (internal jugular or femoral) as appropriate according to children size. CRRT was performed with standard hemofilter (Polyarylethersulphone or ANST69) combined with Cytosorb in continuous veno-venous hemofiltration (CVVH) or continuous veno-venous hemodiafiltration (CVVHDF) modality, using a pre-filter reinfusion and an effluent dose of 2000 mL/h/1.73 m2. Cytosorb was inserted in the CRRT circuit in series with the hemofilter in a post-filter position, both CRRT circuit and Cytosorb was flushed with saline solutions and primed with albumin, blood, or saline at discretion of the attending physicians. Anticoagulation was managed with a continuous infusion of unfractionated heparin (UFH) sodium (10–20 UI/kg/h) to achieve a post-filter activated clotting time (ACT) between 160 and 180 s. In case of contraindications to UFH, regional citrate anticoagulation has been used.
Cytosorb therapy was continued on the basis of the clinical course as well as laboratory surrogates (lactate concentrations, metabolic status including pH). The adsorber was changed every 24 h as recommended by the manufacturer and continued for a maximum of 96 h (mean 72 h).
In patients in ECMO, the CRRT access placed post-oxygenator and the CRRT return post-pump.
Study variables and definitions
Vasoactive-Inotropic Score (VIS)—Dopamine dose (µcg/kg/min) + Dobutamine dose (µcg/kg/min) + (100 × Epineph-rine dose (µcg/kg/min) × Milrinone dose (µcg/kg/min) × Vasopressin dose (units/kg/min) × Norepinephrine dose (µcg/kg/min)) 21 —was calculated prior the EBPT onset and 24 h after the end of the EBPT with Cytosorb. The proportion of reduction of vasopressors and inotropes dose was calculated every 24 h as a percentage respect to the onset of blood purification treatment. Bedside refractory septic shock score (bSSS)—based on 5 points, VIS > 200 mcg/kg/min = 1 point; arterial lactate > 8 mmol/L or its increase of 1 mmol/L after 6 h of care = 1 point; myocardial dysfunction defined as occurrence of a resuscitation-responsive cardiac arrest in pediatric intensive care unit (PICU) or cardiac ultrasound findings with left ventricle ejection fraction (LVEF) < 25% or a cardiac index < 2.2 L/min m2 = 3 points 20 —was calculated prior the EBPT onset in each treated patient.
As part of an in-hospital safety protocol for this adjunctive therapy cytokines IL-6, IL-10, and TNF-alpha were dosed at baseline (Time 0) and then every 12 h until the end of the EBPT (72 or 96 h). The removal ratio (RRAd%) is calculated = (Concentration at baseline (CB0) – Concentration at the end of the treatment (Cend)/CB0 × 100). 5
We reported survival at 28 days after PICU discharge and survival to hospital discharge.
Statistical analysis
Categorical data were represented as count and proportion, continuous data as median and interquartile range. VIS and cytokine data at different time were compared trough Wilcoxon signed-rank test. Differences were considered statistically significant at p < 0.05. All statistical analyses were performed using Stata 13.1.
Results
From January 2018 to May 2019, nine consecutive treatments of hemoperfusion with Cytosorb associated with standard CRRT were performed in eight patients with septic shock. Patients were submitted to EBPT by 24 h after the diagnosis of septic shock. All patients were mechanically ventilated for more than 48 h and the probability of death predicted by PIM3 score when admitted in PICU was 18% (interquartile range (IQR): 12; 28.9). Patient characteristics and details on the individual sources of infection and comorbidities are shown in Table 1.
Patients characteristics and details on the individual sources of infection and comorbidity.
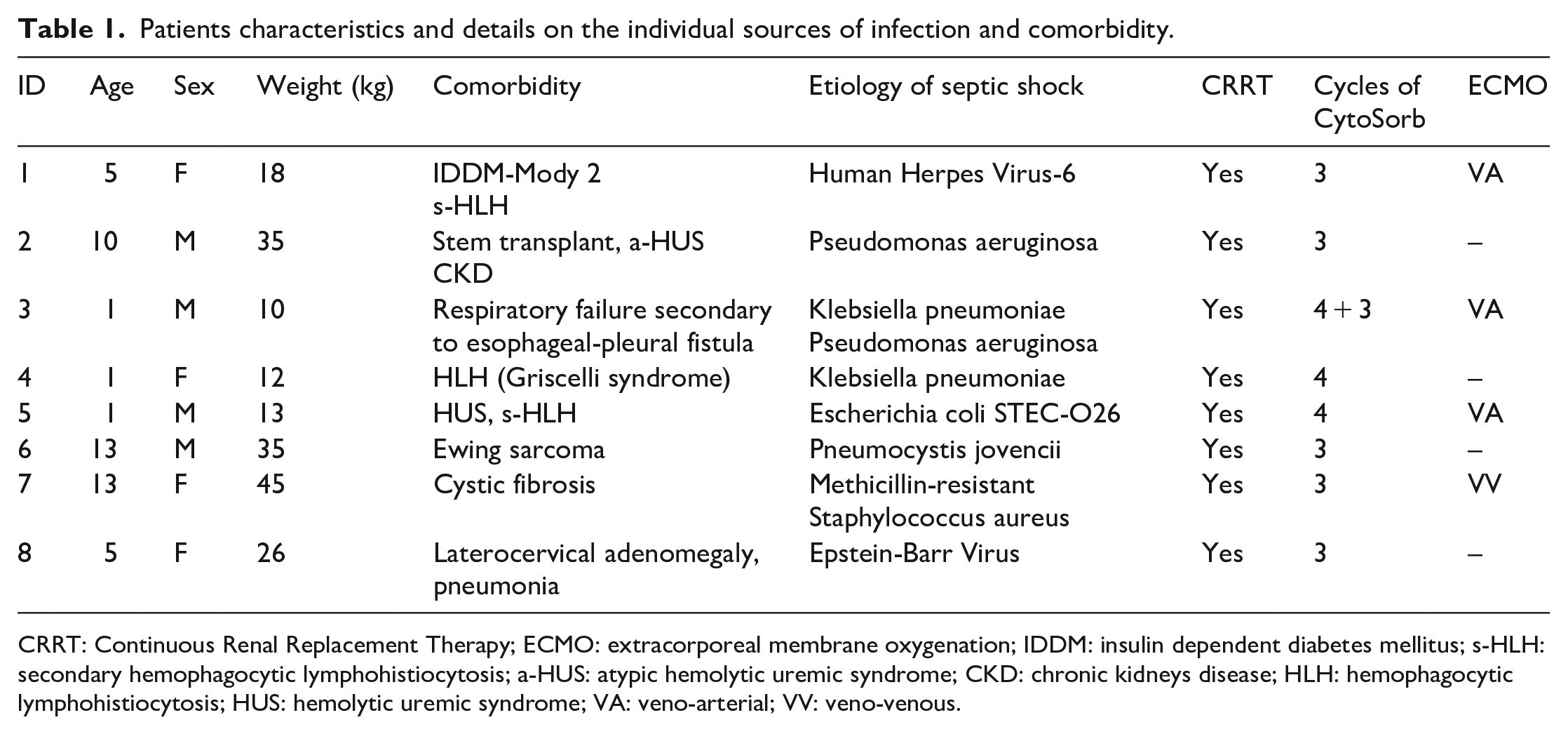
CRRT: Continuous Renal Replacement Therapy; ECMO: extracorporeal membrane oxygenation; IDDM: insulin dependent diabetes mellitus; s-HLH: secondary hemophagocytic lymphohistiocytosis; a-HUS: atypic hemolytic uremic syndrome; CKD: chronic kidneys disease; HLH: hemophagocytic lymphohistiocytosis; HUS: hemolytic uremic syndrome; VA: veno-arterial; VV: veno-venous.
Four of the eight patients received an ECMO support (three veno-arterial (VA) ECMO and one veno-venous (VV) ECMO). Patient 3 required an ECMO support for 60 days and received two cycles of hemoperfusion with Cytosorb due to two distinct episodes of septic shock. Patient 5 required resuscitation for an in-hospital cardiac arrest prior to VA ECMO. Patient 7 was the only patient on VV ECMO as bridge to lung transplant but developed a refractory septic shock few days after ECMO initiation. The median duration of ECMO support was 20.5 (IQR: 8.5; 49.75) days. The median duration of CRRT treatment was 12.5 (IQR: 4.75; 26.5) days.
We found that the combined application of CVVH/CVVHDF and Cytosorb was associated with a significant decrease in catecholamines demand and a hemodynamic stabilization in the patients. Median VIS score calculated prior the onset EBPT and after the last EBPT with Cytosorb showed a significant reduction (pre: 40.00 (IQR: 27.00; 40.00); post: 8.89 (IQR: 5.00; 11.00), p = 0.0076) and the median VIS decreased nearly 4.5-fold following blood purification treatment (Table 2).
Hemodynamic characteristics of the patients treated.
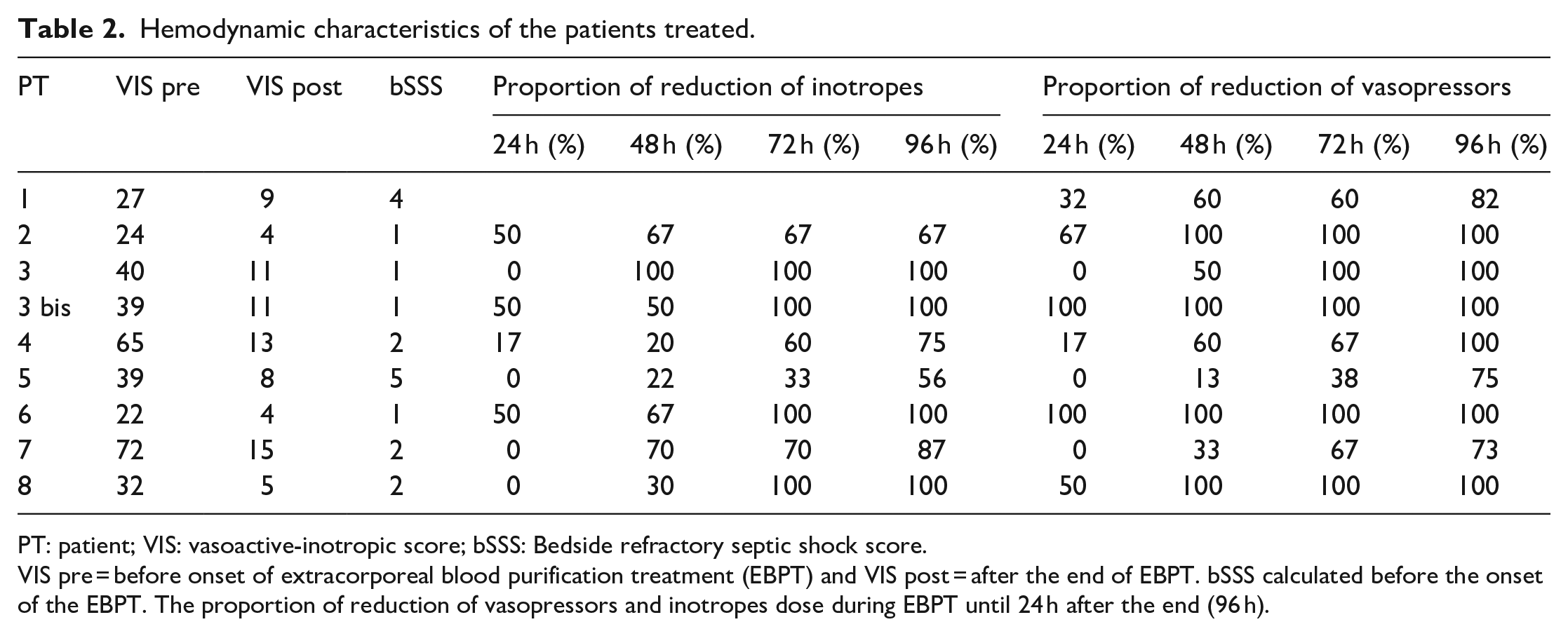
PT: patient; VIS: vasoactive-inotropic score; bSSS: Bedside refractory septic shock score.
VIS pre = before onset of extracorporeal blood purification treatment (EBPT) and VIS post = after the end of EBPT. bSSS calculated before the onset of the EBPT. The proportion of reduction of vasopressors and inotropes dose during EBPT until 24 h after the end (96 h).
In total, 65% and 70% of the patients showed a reduction of ⩾50% of vasopressors and inotrope, respectively, after 48 h of blood purification treatment (Table 2). The median bSSS score was 2.11. Patients 1, 5, and 8 presented a severe myocardial dysfunction (FE 5%–20%), but during the 72–96 h, they showed a progressive improvement of cardiac function (Figure 1).
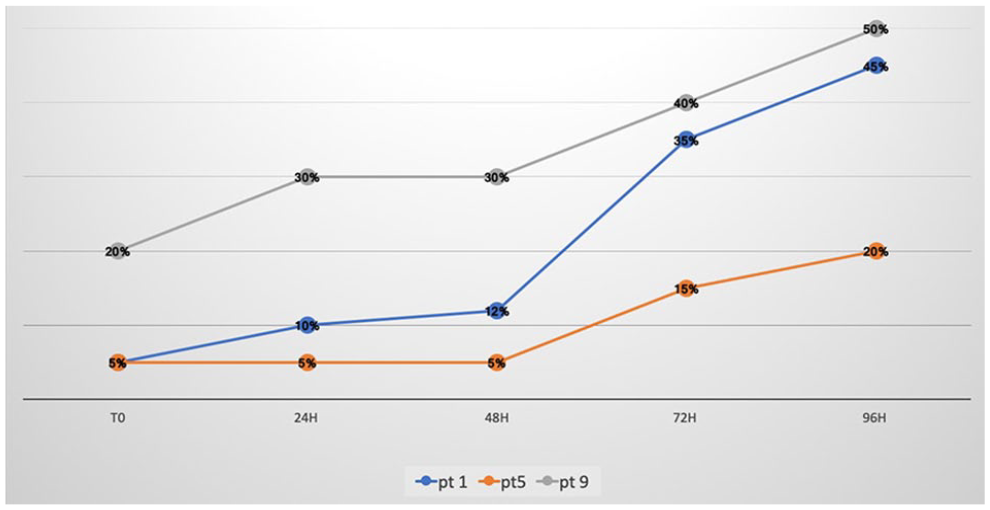
Trend of ejection fraction (FE%) during Extracorporeal Blood Purification Therapy (EBPT) in patients with severe myocardial dysfunction.
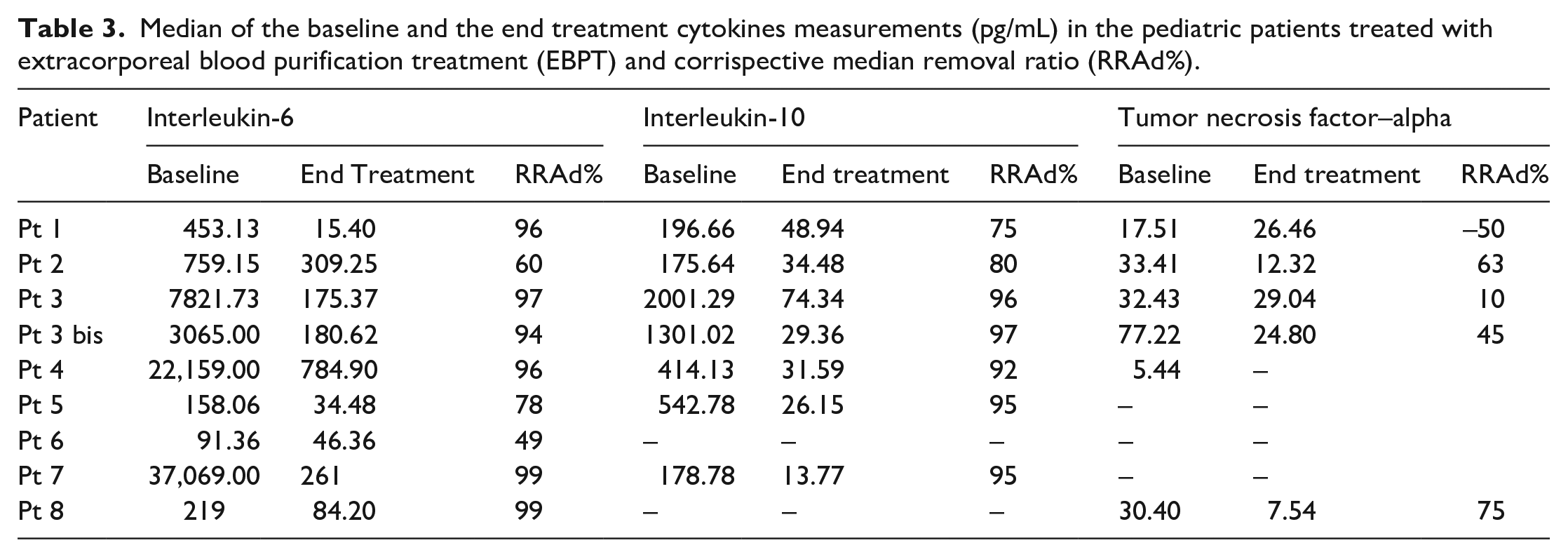
Measurement of cytokines during EBPT evidenced a significant reduction of IL-6 plasma levels (7977.27 (IQR: 219.00; 7821.73) to 210.18 pg/mL (IQR: 43.39; 273.06), p = 0.0077) and IL-10 plasma levels (from 687.19 (IQR: 187.72; 921.9) to 36.95 pg/mL (IQR: 27.755; 41.71), p = 0.0180). In four patients, plasma level of TNF-alpha was not detectable at baseline and afterward, in the others plasma reduction of TNF-alpha was not significant (p = 0.138; Table 3). The median removal ratio (RRAd%) was 80% for IL-6, 90% for IL-10, and 29% for TNF-alpha. In Figure 2, we report the time course of cytokines IL-6, IL-10, and TNF-alpha during EBPT in each treated patient.
Median of the baseline and the end treatment cytokines measurements (pg/mL) in the pediatric patients treated with extracorporeal blood purification treatment (EBPT) and corrispective median removal ratio (RRAd%).
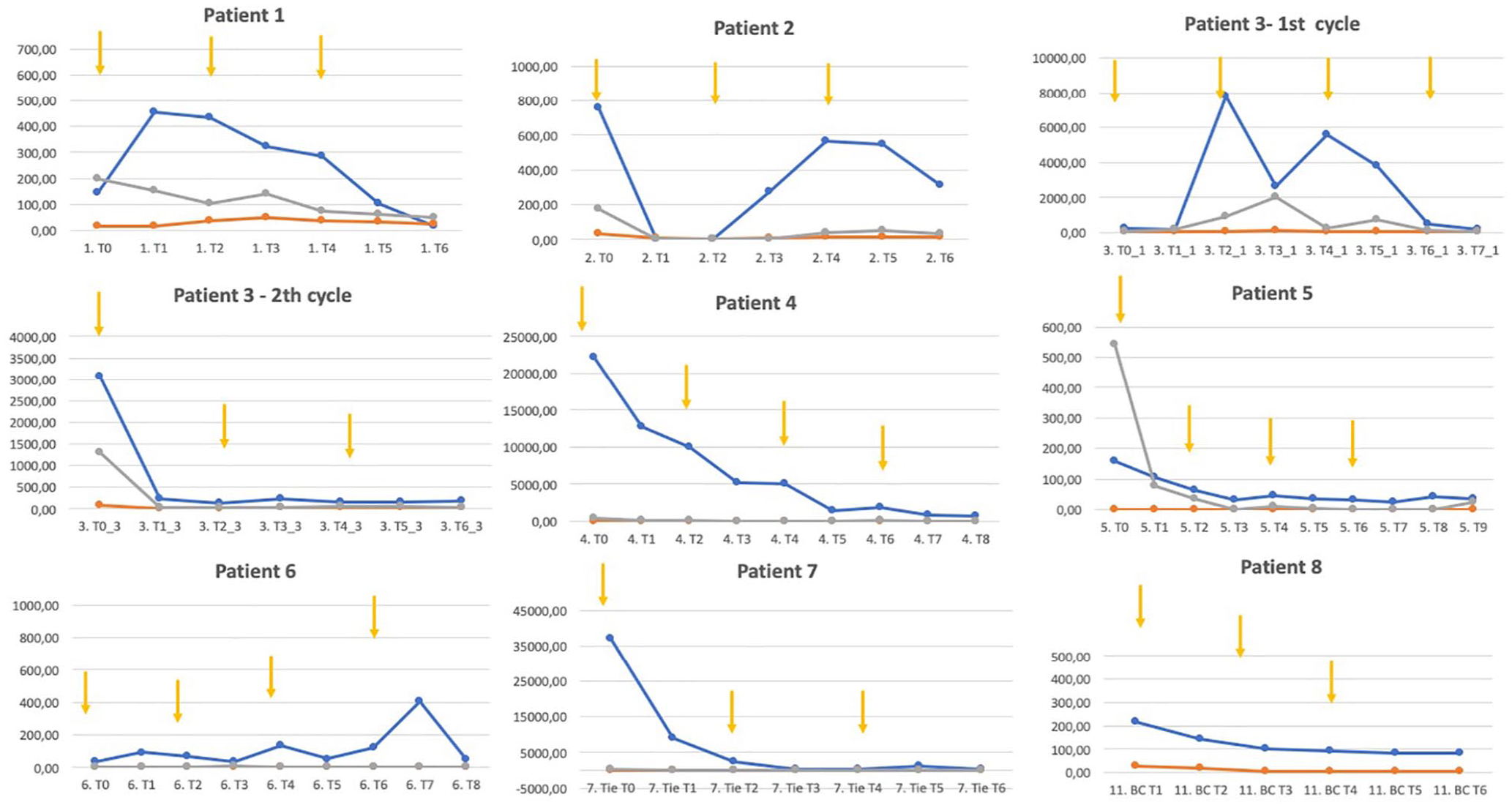
Time course of cytokines IL-6, IL-10, and TNF-alpha during Extracorporeal Blood Purification Therapy (EBPT) in each patient treated.
We did not observe any adverse event due to extracorporeal adsorption therapy neither during the priming, nor during continuous hemoperfusion and the end of the EBPT.
Seven of eight patients survived. Patient 4 overcame the septic shock but she died 10 days later due to a reactivation of the familiar hemophagocytic lymphohistiocytosis (F-HLH). In Patient 1, ECMO was stopped on the 7th day and she was discharged from PICU on the 12th day. Patient 3 required a total of 60 days of VA ECMO and Patient 5 required 30 days of VA ECMO: both were discharged from PICU after more than 28 days. Table 4 reported the most relevant outcome variables (PIM3 score, bSSS score, survival at 28 days after PICU discharge and survival to hospital discharge) in each patient treated.
Principal outcome variables in each patient treated.
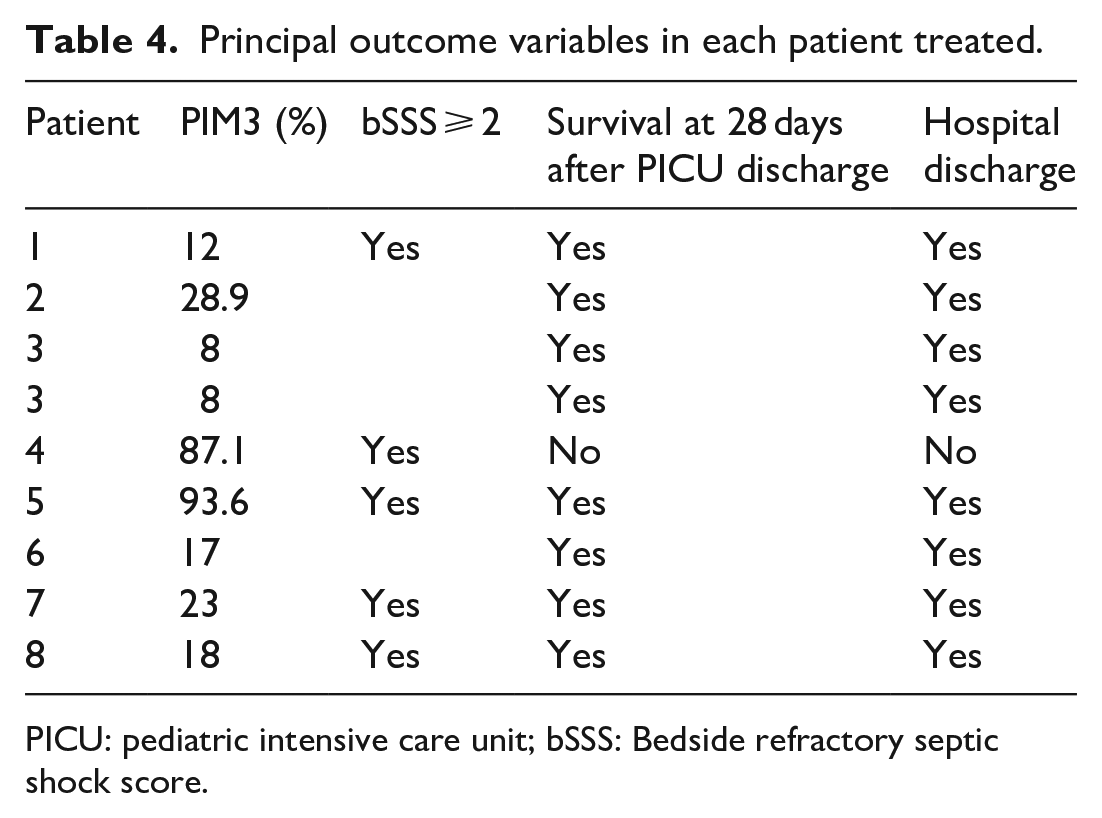
PICU: pediatric intensive care unit; bSSS: Bedside refractory septic shock score.
Discussion
Our retrospective study confirms the data coming from previous reports6,22 showing that continuous hemoperfusion with Cytosorb is able to reduce the catecholamines doses in patients with septic shock. We detected a significant reduction in median VIS score 24 after completing the EBPT compared to the VIS score at time 0 before the onset of EBPT. It is relevant that this clinical effect was observed even in pediatric patients with a bedside SSS score ⩾ 2 and according to the last ESPNIC definition, the mortality of patients with an bSSS score ⩾2 is between 45% and 55%. 21 The survival rate of our cohort was 90% definitively higher than the survival rate reported for this group of patients on the basis of bSSS score. The median PIM3 score in our cohort was only 18% (IQR: 12; 28.9), but this can be explained, PIM3 score does not take into account the impact of the extracorporeal supports (ECMO and CRRT) on mortality. Conversely, the latest scientific evidences clearly showed the relevant role of the extracorporeal supports on the mortality outcome in pediatric population with septic shock.4,23 In terms of discharge from PICU at 28 days, it is possible that ECMO patients have influenced this result: four patients in our cohort were supported on ECMO, two of them experienced a longer stay in PICU.
In our cohort, we also demonstrated a significant reduction of IL-10 and IL-6 serum levels and these data are consistent with previous studies in vitro, ex vivo, and in vivo24,25 on the ability of Cytosorb to capture IL-10 and IL-6. Furthermore, the progressive and constant reduction of cytokines’ concentrations during the blood purification treatment evidences not only the importance of a continuous hemoperfusion along 72–96 h but also the high compatibility of the cartridge excluding an inflammatory response secondary to the device itself.
Two patients showed higher levels of IL-10 than IL-6, and we can speculate that both pro-inflammatory and anti-inflammatory cytokines should be monitored in patients with septic shock because of different patterns of inflammation. Considering that in literature, it has been suggested that both high level of pro-inflammatory and anti-inflammatory cytokines correlates with high mortality in these patients5,9,10 to monitor only IL-6 could not only underestimate the dysregulated host response but also the efficacy of the hemoperfusion in those patients with a prevalent anti-inflammatory response.
Concerning the possible rule of ECMO and CRRT in the cytokines adsorption, many authors have already described the ECMO support itself can induce and maintain an inflammatory response through various mechanisms, 13 this response is mainly caused by exposure of blood cells and molecules to the artificial surfaces of tubings, rotor, and oxygenator of the ECMO circuit. 26 This effect is especially relevant in children, as the extracorporeal blood volume exposed to foreign surfaces often exceeds the total blood volume of the pediatric patient. 13 Furthermore, in our small cohort, only four out of eight patients received an ECMO support, and we observed the same significant reduction of IL-6 and IL-10 in patient without ECMO support. Regarding the role of CRRT in removal of cytokines, we highlight that on the basis of the technical characteristics of ANST69 and scientific evidences about its clinical application in septic patients, these hemofilters are able to remove only small molecules (cut off 35 kDa) with a limited capacity of adsorption. 27
Finally, we believe that the high adsorption surface (>40.000 m2) of Cytosorb compared to the body surface and the blood volume of pediatric patients has a significantly impact on the cytokines removal in septic shock: Cytosorb efficacy is primarily based on a longer time of membrane saturation by the target molecules than a standard hemofilter. Consequently, according to our experience a continuous hemoperfusion on 24 h is probably more effective than a shorter cycle as reported in other clinical experiences. 28
The adsorbing column has shown to be very biocompatible: we did not observe major adverse events neither in term of bradykinin reactions neither in term of hemodilution or severe piastrinopenia after the onset of the EBPT. However, we have accurately followed the known safety keys points of pediatric patients receiving extracorporeal support.29,30
There are several limitations of our work: first, this is a retrospective study and we did not compare our results with a cohort control; second, it is a single institution study with a limited numbers of patients; thus, these limits make it difficult to draw definitive conclusions on outcome. Finally, the rate of removal of antibiotics and others micro and macronutrients was not investigated in this study.
Conclusion
To our knowledge, this is the first case series reporting the use of Cytosorb therapy in pediatric patients with septic shock. Treatment with Cytosorb was associated with a rapid stabilization in hemodynamics and with a significant reduction in inotropes and vasopressors doses. No adverse effects related to the use of Cytosorb has been evidenced. Two of the most important cytokines involved in septic shock, IL-6 and IL-10, were significantly reduced after the blood purification treatment.
Our findings have showed a potential promising adjunctive therapy in septic shock, but since this is a very small patient cohort, we cannot definitely conclude that the EBPT was the cause of the clinical improvement in our patients. The results of this retrospective study indicate that there is a need for further investigations on extracorporeal blood purification therapies in pediatric patients with septic shock. 31 Future case-control studies comparing CRRT versus CRRT plus hemoadsorption will better address the impact of this depurative therapies on patient outcome.
Footnotes
Author’s note
All research materials related this paper can be accessed.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.