
Abstract
Objectives:
Weight change after left ventricular assist device implantation may influence outcomes and can affect transplant candidacy. We questioned if there is a systematic weight change after left ventricular assist device implantation and examined the evolution in functional capacity.
Methods:
A retrospective analysis of 84 patients who received a left ventricular assist device in Universitaire Ziekenhuizen Leuven between 2008 and 2016 was performed. Patients were divided into four groups based on their baseline body mass index, and we also examined weight evolution for patients presenting with new-onset heart failure versus those suffering from chronic heart failure. Body mass index was assessed at baseline, 6, 12, 18, and 24 months. To indicate the functional capacity, we analyzed the results of routine 6-Minute Walk Test performed at 6, 12, and 18 months.
Results:
During the first 6 months after surgery, the underweight patients evolved to normal weight and the body mass index of the obese patients reduced significantly. Afterward, all patients gained weight. The weight loss of the obese was not maintained over time. The weight of patients with normal weight and overweight evolved to overweight and obesity, respectively. No body mass index changes were demonstrated for patients presenting with new-onset heart failure, and the body mass index of patients suffering from chronic HF significantly increased. There was a significant improvement in functional capacity at 6 months, but this level remained unchanged at 12 and 18 months after surgery.
Conclusion:
Although the initial 6 months evolve beneficial, all patients gain weight in the second year and do not further improve their exercise capacity.
Introduction
The relation between obesity and heart failure (HF) is complex. Although obese people have twice the risk to develop HF, obesity is protective in patients with established HF, a phenomenon termed “the obesity paradox.”1–4 Despite this, many of these patients proceed to stage D HF. Morbid obesity (defined as a body mass index (BMI) ⩾ 35 kg/m2) is a limitation to candidacy for heart transplantation (HTx) and those who are obese (defined as a BMI ⩾ 30 kg/m2) and undergo HTx have worse outcomes.5,6 Left ventricular assist device (LVAD) therapy is often considered in these patients who are not currently transplant candidates. Associated with LVAD therapy, an improved functional capacity is expected, which would facilitate weight loss. However, an analysis of the INTERMACS data revealed that obese patients did not experience weight change after LVAD implantation. 7 In addition, they have higher rates of device-related infection, thromboembolic events, and rehospitalization.8–13
We questioned if there is a systematic weight gain after LVAD implantation. Therefore, we analyzed our institutional data to identify potential subgroups. Moreover, we sought to examine the evolution in functional capacity after LVAD implantation.
Methods
Data of all patients who received an LVAD (type HeartMate II or HeartWare) in our institution between 2008 and 2016 were prospectively entered into a database and retrospectively assessed for this study. Patients of whom data were available for a follow-up period of at least 6 months were included.
BMI was assessed at baseline during hospitalization before LVAD implantation and at the time of outpatient visit 6, 12, 18, and 24 months after LVAD implantation. We considered the BMI at the moment of LVAD implantation as the baseline BMI. All patients were advised by the dietician to eat healthy, but no specific diet instructions were given.
To indicate the functional capacity, a 6-Minute Walk Test (6MWT) was assessed routinely at baseline (if possible), 6, 12, and 18 months after LVAD implantation. At 6, 12, and 18 months, a cardiopulmonary exercise test (CPET) was performed. Patients were divided into four groups based on their baseline BMI, as follows: underweight (BMI < 20 kg/m2), normal weight (BMI 20 to 24.9 kg/m2), overweight (BMI 25 to 30 kg/m2), and obese (BMI > 30 kg/m2).
It is intuitive to expect a different behavior for patients presenting with new-onset (“de novo”) HF versus those suffering from chronic HF (cHF). New-onset HF may present acutely, for example, as a consequence of acute myocardial infarction. It may also present in a subacute fashion, for example, in patients with a dilated cardiomyopathy, who often have symptoms for weeks or months before the diagnosis become clear. Patients who have had HF for some time are said to have cHF. 14 We focused on patterns in weight evolution within these subgroups over time.
Data analysis
BMI is expressed as absolute value and as percentage compared to the individual baseline. The 6MWT and CPET are expressed as percentage compared to age and sex-specific reference standards. Change in BMI, 6MWT, and CPET were analyzed using a two-tailed paired student t-test, considering a p < 0.05 as significant.
Results
Patient population
The total number of patients included for the study was 84. Baseline characteristics of patients are shown in Table 1.
Baseline characteristics.
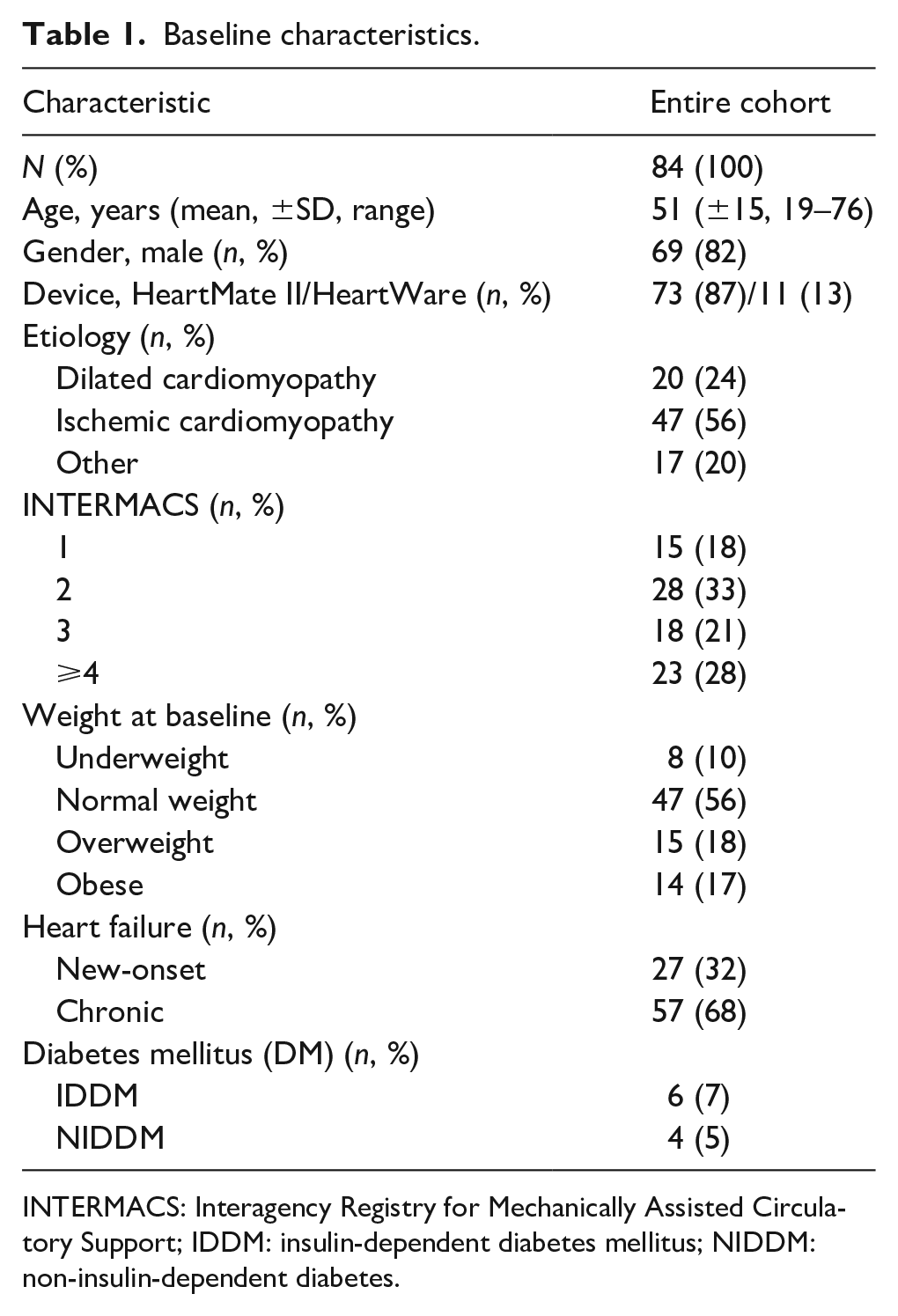
INTERMACS: Interagency Registry for Mechanically Assisted Circulatory Support; IDDM: insulin-dependent diabetes mellitus; NIDDM: non-insulin-dependent diabetes.
BMI change over time
The BMI change over time of the study population is shown in Figure 1. The mean baseline BMI is at the upper end of the normal range (BMI = 24.8). There is an increase in BMI, which sustains up to 24 months after LVAD implantation. Significant changes in BMI are observed between baseline and 18 months (BMI = 26.1, p = 0.032) and between baseline and 24 months (BMI = 27.0, p = 0.002) after LVAD implantation.
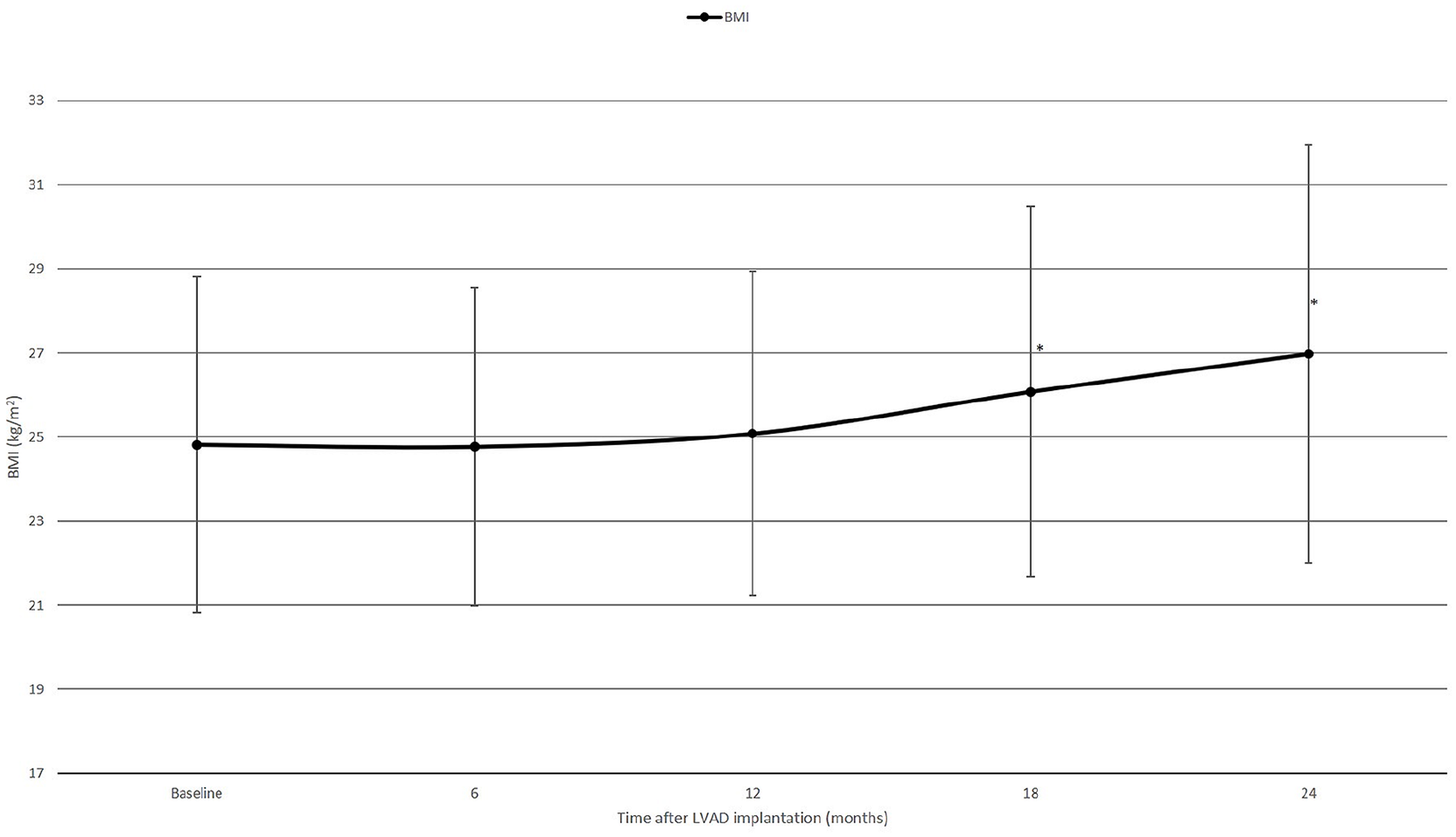
Mean (±SD) BMI change over time of the entire cohort (n = 84).
Figure 2(a) and (b) shows, respectively, BMI change and percent BMI change over time for the four subgroups based on their baseline BMI. Underweight patients gained the most weight after LVAD implantation. Significant change in BMI is demonstrated between baseline (BMI = 18.9) and 12 months (BMI = 21.1, p = 0.022). Patients with normal baseline weight evolved toward overweight over time. This effect was significant between baseline (BMI = 23.1) and 24 months (BMI = 25.2, p = 0.044). For the obese patients, there was a significant decrease in BMI initially at 6 months (BMI = 30.2, p = 0.012). However, this weight loss was not maintained over time.
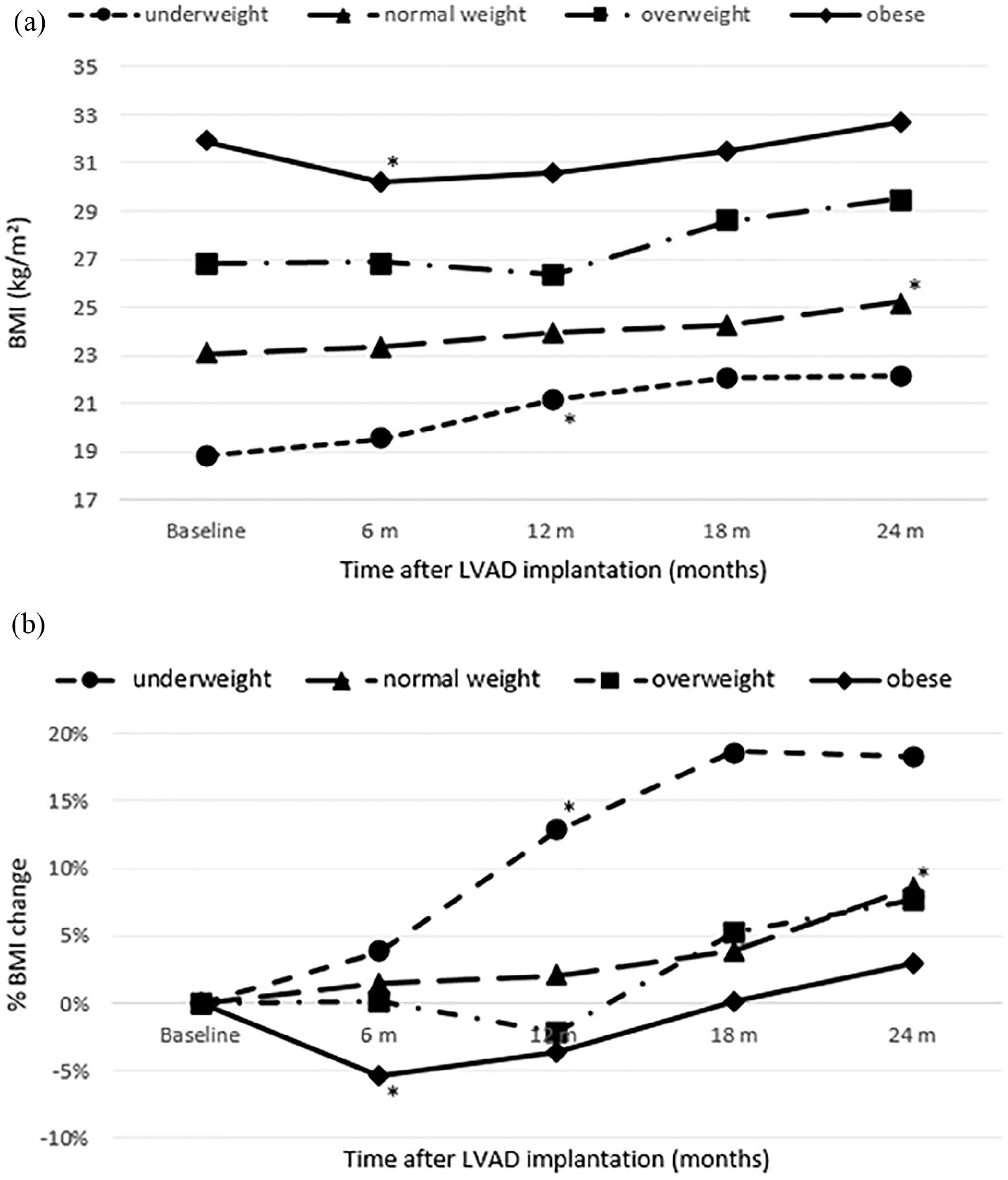
Mean BMI change (a) and mean percentage BMI change (b) over time in the underweight, normal weight, overweight, and obese subgroups.
Figure 3(a) and (b) shows, respectively, BMI change and percent BMI change over time based on LVAD implantation as a result of new-onset versus chronic HF. Baseline BMI for both groups is not significantly different (BMI = 24.5 vs BMI = 25.0, respectively, p = 0.6).
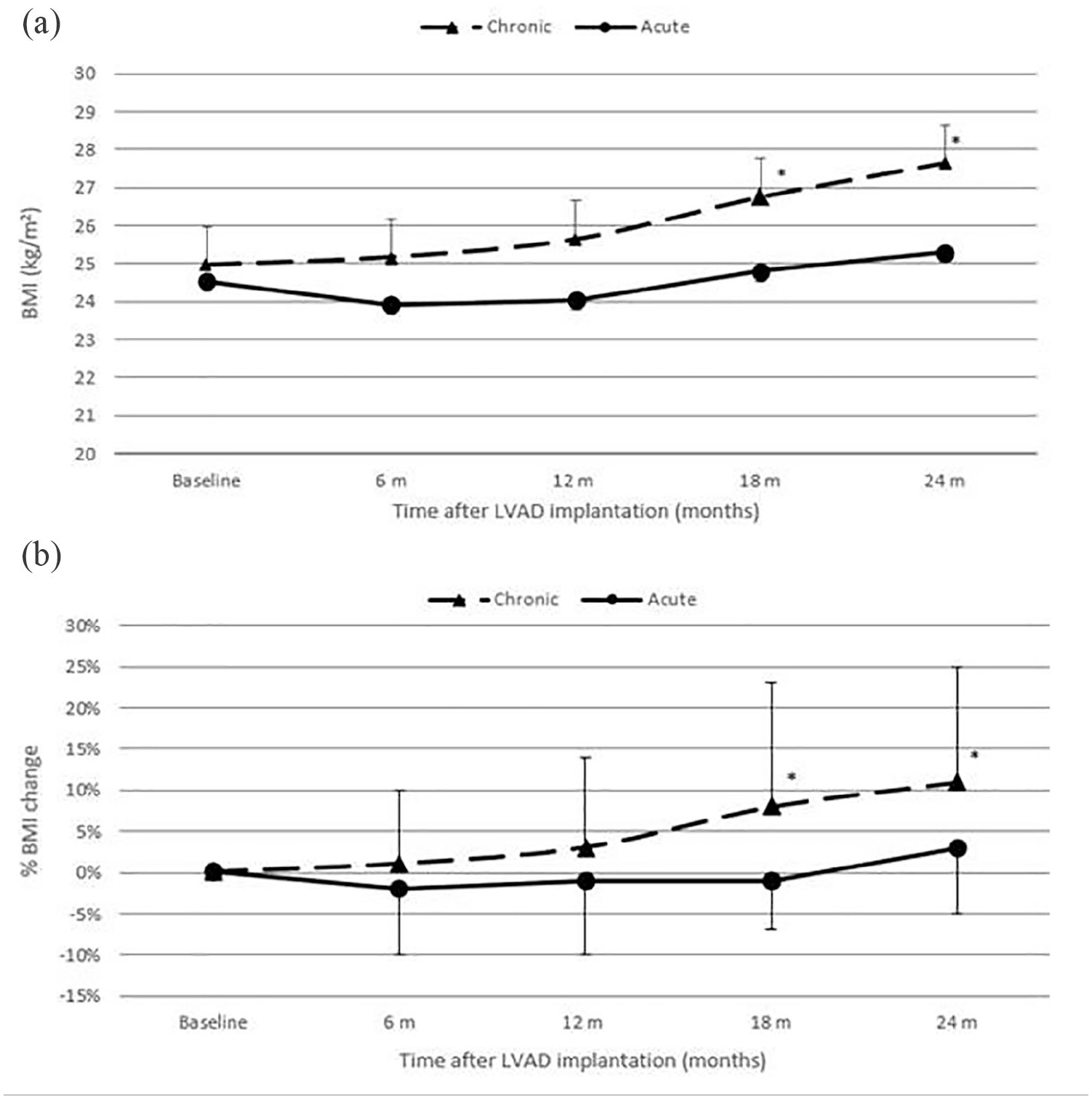
Mean (±SD) BMI change (a) and mean percentage BMI change (b) over time for patients with new-onset and chronic HF.
There are no significant changes in BMI demonstrated during the course of LVAD support for patients who received an LVAD as a result of new-onset HF.
The BMI of patients who suffered from cHF before LVAD implantation increased up to 24 months to a level of 11% of their baseline BMI. Significant changes are demonstrated between baseline and 18 months (BMI = 26.8, p = 0.009) and between baseline and 24 months (BMI = 27.7, p = 0.003) after LVAD implantation.
Evolution of functional capacity
The evolution in functional capacity, expressed by the 6MWT as a percentages compared to age and sex-specific reference standards, is shown in Figure 4. There was a significant improvement in functional capacity from baseline (20%) to 6 months after LVAD implantation (63%, p = 0.001), but the level of functional capacity remained unchanged at 6, 12, and 18 months after surgery.
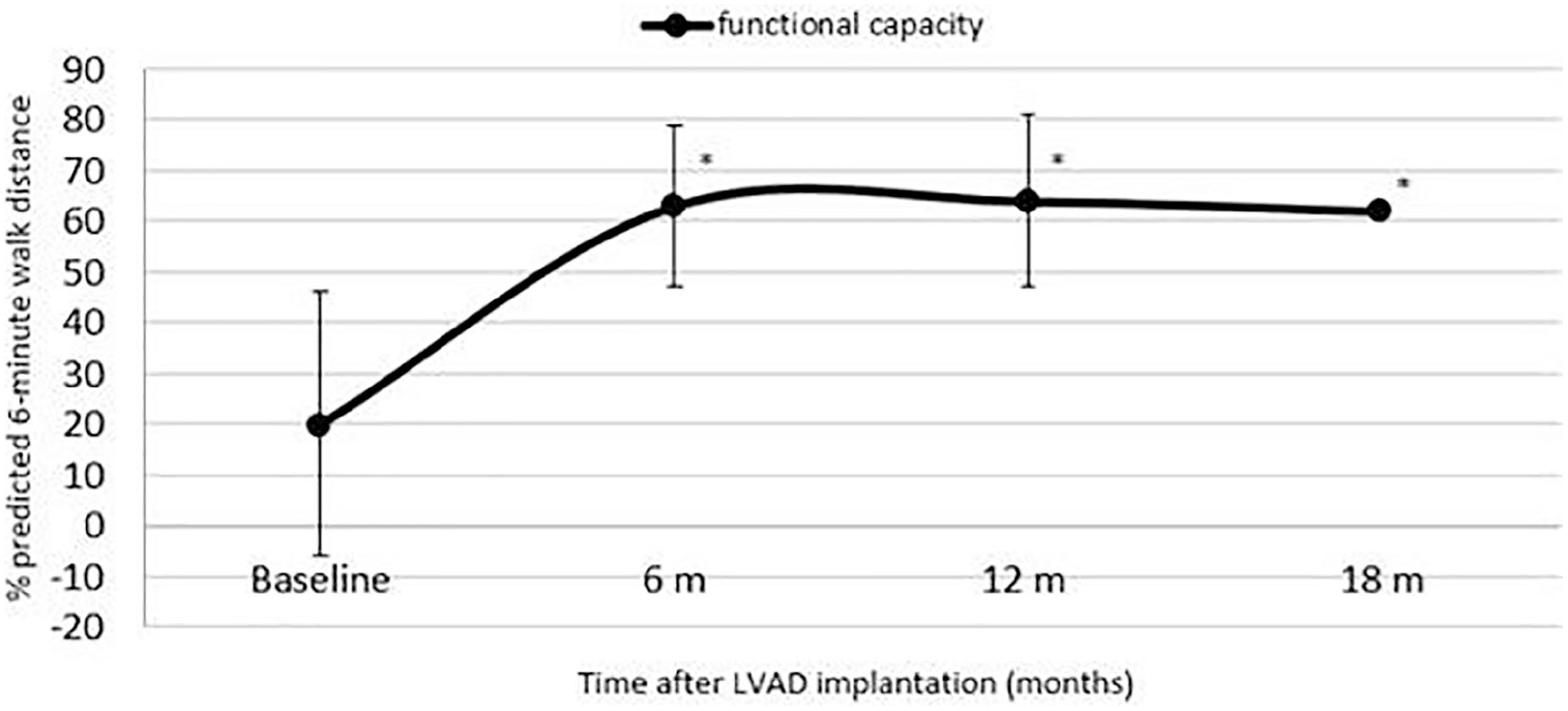
Evolution in functional capacity of the entire cohort (n = 84). The 6MWT is expressed as percentage (±SD) compared to age and sex-specific reference standards.
Similarly, the exercise capacity, expressed as a percentages of expected peak VO2 consumption, did not change between 6 and 18 months after LVAD implantation (from 50% + 14% of the expected value at 6 months to 54% + 13% at 18 months, p = 0.13).
Discussion
The change in BMI after LVAD implantation is an aspect that has received relatively little attention. In our study, we have assessed BMI change over a period of 2 years for various subgroups of LVAD patients.
The changes in body weight during the first 6 months after LVAD implantation seem beneficial: the underweight gain weight and the obese lose weight. Underweight patients evolved to a normal weight over time. We did not investigate the underlying mechanism of weight gain. However, this result seems to reflect reversal of underlying cachexia associated with end-stage heart failure. At the other end of the weight spectrum, LVAD therapy is considered in obese patients who are not currently transplant candidates in the hope that they achieve weight loss in order to facilitate eligibility for transplantation. For these obese patients, there was a significant reduction in BMI at 6 months after LVAD implantation. A similar evolution in BMI was observed in an analysis of the Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS) data. 7 However, in the second year of our observation period all patients, regardless of their initial weight, gain weight. The weight loss of the obese patients was not maintained over time. Therefore, we assume that this initial weight loss is due to achieving euvolemia in the first months after LVAD implantation rather than actual loss of nonlean body mass. In addition, we observed a continuous weight gain in patients with normal weight and overweight at baseline. Their weight evolved toward overweight and obesity, respectively.
We also compared the BMI change over time for patients presenting with new-onset HF versus those suffering from cHF. Where no significant BMI changes were demonstrated for patients presenting with new-onset HF, the BMI of patients suffering from cHF significantly increased up to 24 months to a level of >10% of their baseline BMI. We assume that this can be explained by the fact that patients suffering from cHF are used to a more sedentary life style and that it is difficult for them to change their life style after LVAD implantation.
Our results suggest that LVAD patients infrequently achieve weight loss in the absence of targeted weight-control strategies. Further research should focus on identification and implementation of the most appropriate and effective weight-control strategies, with regard to the overall management of long-term LVAD therapy. There has been growing interest in combining bariatric surgery with LVAD implantation, either at the time of LVAD implantation or after the patient has recovered from the surgery. However, we believe that it is appropriate to use preventive management programs, targeting LVAD patients’ self-management strategies to initiate behavioral changes. 15 As described by Kugler et al., 16 such a multi-dimensional intervention should consist of nutrition management, controlled exercise training, and psychosocial support.
During the initial 6 months, our patients are well supervised by a physiotherapist. A few weeks of home physiotherapy are followed by ambulatory cardiac rehabilitation. We observed a significant improvement in exercise capacity during the first 6 months after LVAD implantation, after which a plateau was reached. This finding is in line with previous studies demonstrating improved functional capacity within the first months after surgery, but no further improvement afterward.17–20 However, the achieved level of functional capacity remains markedly below that of healthy subjects. This strengthens our belief that there is a need for more intensified and continued physical rehabilitation programs, as part of multi-dimensional interventions for outpatients on long-term LVAD support.
Our study does have limitations. It was a single-center study of a relatively small number of patients implanted with an LVAD over a long time-period. Several outcome studies indicate a relation between weight and outcome of ventricular assist device transplant patients.8–13 One can envision several effects of body weight on the occurrence of adverse events like drive line infection stroke and bleeding. Although the clinical outcome is the primary focus of our management, our study population is too small to make any conclusions on the rate of adverse events. The number of patients at the extreme ends of the weight spectrum was small compared with the entire group. Furthermore, available data at 24 months were limited because of transplantation or death.
In conclusion, in this study, we have evaluated BMI changes and evolution of functional capacity over time for LVAD patients. Although the initial 6 months evolve beneficial, patients significantly gain weight in the second year and do not further improve their exercise capacity.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: L.F. was supported by the Frans Van de Werf scholarship.