
Abstract
Objective:
To shorten the preparation time of rabbit decellularized tracheal matrix through a modified detergent-enzymatic method with higher concentration of DNase (50 kU/mL), providing an experimental and theoretical basis for clinical decellularization technology.
Methods:
The control group was a natural trachea, and the experimental group was a tracheal matrix subjected to two and four decellularization cycles. The performance of each group of samples was evaluated by histology and immunohistochemical staining, scanning electron microscopy, biomechanical property testing, inoculation and cytotoxicity tests, and allograft experiments.
Results:
The results showed that the nuclei of the nonchondral areas of the tracheal stroma were essentially completely removed and MHC-I and MHC-II antigens were removed after two decellularization cycles. Histological staining and scanning electron microscopy showed that the extracellular matrix was retained and the basement membrane was intact. Cell inoculation and proliferation tests confirmed that the acellular tracheal matrix had good biocompatibility, and the proliferation capacity of bone mesenchymal stem cells on the matrix was increased in the experimental group compared with the control group (p < 0.05). Histological staining and CD68 molecular marker analysis after the allograft experiment showed that the inflammatory response of the acellular tracheal matrix was weak and the infiltration of surrounding macrophages was reduced.
Conclusion:
A modified detergent-enzymatic method with an increased DNase (50 kU/mL) concentration requires only two cycles (4 days) to obtain a decellularized rabbit tracheal matrix with a short preparation time, good biocompatibility, suitable mechanical properties, and reduced preparation cost.
Keywords
Introduction
Tracheal injury is mainly caused by tumor, infection, trauma, stenosis, and so on. 1 When the injury length is less than 1/2 of the full adult trachea length or 1/3 of the juvenile trachea length, end-to-end anastomosis is considered to be the “gold standard” for the repair of the tracheal injury. 2 When the injury exceeds these lengths, it is difficult to obtain good treatment results by conventional surgical methods, and an airway substitute is required to reconstruct the airway.3,4 Tracheal tissue engineering adopts the principles and techniques of engineering and natural sciences, uses the interaction of biological substitutes and signal transduction systems to repair tracheal damage, reshapes the bioactive and functional trachea, and has gradually become a new approach for tracheal replacement therapy.5–7 Tissue-engineered trachea can be used to prepare nonimmunogenic tracheal replacements for tracheal reconstruction. 8 These tracheal substitutes retain mechanical properties similar to those of natural trachea, maintain lumens, and support epithelial cell growth and angiogenesis, 9 which are key factors for successful tracheal reconstruction therapy.
Decellularization is a common method for preparing tissue-engineered tracheal scaffolds. 7 This process removes the cellular components that cause tissue rejection and preserves the three-dimensional structure of the trachea and the extracellular matrix (ECM) components, providing a material scaffold for cell growth and proliferation.10–13 Currently, decellularized tracheal scaffolds are often prepared by the detergent-enzymatic method (DEM), which removes the tracheal antigens while retaining the three-dimensional structure and ECM of the trachea, providing a compatible and supportive environment for the graft.14–17 There are clinical cases of transplanted acellular tracheal stroma,10,18 some of which have been relatively successful, but the function of these grafts needs to be improved. The clinical applied decellularization protocol has a long preparation cycle and requires several weeks of decellularization,9,10,18 which is often restrictive in emergency clinical applications, such as neonatal tracheal atresia or serious defects,19,20 and can cause respiratory distress after birth, requiring rapid tracheal replacement treatment.
The purpose of this study was to develop a rapid acellular tracheal matrix preparation method. The rabbit trachea was adapted by modified DEM treatment, and changes in the tracheal matrix structure, immunogenicity, biomechanical properties, and biocompatibility after decellularization were observed and evaluated. We hope that this study can provide a short preparation cycle, low-cost, good biocompatibility method for tissue engineering tracheal replacements, and provide ideas and feasible schemes for clinical tracheal replacements.
Materials and methods
Study design
Male New Zealand white rabbits (n = 30) weighing 2.5 ± 0.5 kg were selected as donors and purchased from Yangzhou University Clinical Medical Laboratory Animal Center. All animals received humane care in accordance with the “Guide for Care of Laboratory Animals” formulated by the National Ministry of Science (IACUC NO. SYXK2016-0041). Thirty New Zealand white rabbits were divided into three groups by the random arithmetic method. The control group (n = 10) was New Zealand white rabbits treated with a natural trachea. The experimental group was rabbits treated with a trachea after two and four decellularization cycles, and was divided into two-cycle group (n = 10) and four-cycle group (n = 10). The performance of each group of samples was evaluated by histology and immunohistochemical staining, scanning electron microscopy (SEM), biomechanical property testing, inoculation and cytotoxicity tests, and allograft experiments.
Preparation of the rabbit decellularized tracheal matrix
Three groups of New Zealand white rabbits were sacrificed by air embolization through the ear vein. The trachea was isolated under aseptic conditions, and the connective tissue on the outer wall of the trachea was quickly removed. The control tracheas were immersed in 4°C phosphate-buffered saline (PBS) containing 1% antibiotics and antifungal drugs (AAs) for testing. According to our previous study and using the DEM described above,9,14,21 the experimental group was treated with modified DEM for decellularization. The increased concentration of DNase (50 kU/mL) used in this protocol removes the DNA component of the tracheal tissue, shortens the preparation time, and reduces the detergent residue as much as possible by repeated washing with PBS. The trachea was immersed in 4% sodium deoxycholate (Sigma, USA) solution and incubated on a 20°C shaking table for 4 h. The trachea was washed 3 times with PBS to remove the detergent. Subsequently, the trachea sample was placed in 1 mol/L NaCl containing 50 kU/mL DNase (Sigma, USA) with continuous shaking for 3 h to dissolve the nuclei and degrade the DNA and then washed 3 times with PBS (10 min/wash). Finally, the trachea was placed in 4°C PBS containing 1% AAs for overnight preservation. The next cycle was carried out in the same manner on the following day. The experimental group was subjected to two and four decellularization cycles, and the prepared acellular tracheal matrix was stored in a 4°C PBS buffer containing 1% AAs for testing.
Histology and immunohistochemical staining
The samples were fixed in 10% neutral formalin for 24 h at room temperature. After being dehydrated with an alcohol gradient, the sample was embedded in paraffin and sliced (thickness 4 μm). Morphological changes of the tracheal stromal epithelial layer, mucosa and submucosa, cartilage, glycosaminoglycan (GAG), collagen, and other components were observed by H&E (KeyGEN, China), Safranin O and Masson (Leagene, China) staining, followed by MHC-I and MHC-II staining (both diluted 1:200, Abcam, China) to detect the expression of MHC class antigens in the matrix before and after decellularization.
GAG quantitative analysis
Tracheal samples from each group were lyophilized and weighed, and digested in papain (Sigma, USA). GAG quantification was quantified with a rabbit GAG ELISA kit (Ziker, China) and normalized to dry weight of the samples.
DNA quantification
The tracheal segments of each group were weighed, DNA was extracted according to the operation steps of the animal tissue/cell genomic DNA extraction kit (Solarbio, China), and then quantitative analysis was performed at 260 nm on a microplate reader (BioTeK, Thermo, USA).
Scanning electron microscopy
The trachea samples were fixed in 2.5% glutaraldehyde solution for 24 h and then washed twice with double-distilled water (15 min/wash). After being washed, the samples were subjected to ethanol gradient dehydration, critical point drying, and gold spraying. Scanning electron microscopy (S-4800, Hitachi, Japan) was used to observe changes in the tracheal matrix basement membrane and to remove the experimental group with increased numbers of fissures in the basement membrane.
Biomechanical test
The length, thickness, width, and compression properties of each set of samples were measured using a universal tensile tester (AGS-X-10Kn, Shimadzu, Japan). The sample was fixed in the center of the sensor; the test was started at an initial load pressure of 0.1 N, and constant compression was started at a rate of 5 mm/min at room temperature. The strain pressure, elastic modulus value when the pipe diameter was compressed to 50%, and whether the deformation was restored after compression were recorded.
Cell inoculation and toxicity test
Similar to a previous study, 22 bone mesenchymal stem cells (BMSCs) were cultured to the fourth generation in vitro and then inoculated on each group of tracheal sections of 0.5 × 0.5 cm2, and the critical point was dried and sprayed with gold. The survival state of each group of cells was observed by scanning electron microscopy. The BMSCs cultured to the fourth generation were planted on 0.5 × 0.5 cm2 tracheal sections of each group. Cell Counting Kit-8 (CCK-8) working solution (Biosharp, China) was used according to the kit manufacturer’s protocol, and the OD 450 was measured by a microplate reader (BioTeK, Thermo, USA). The proliferation and adhesion status of the cells of the experimental group and the control group at days 1, 3, 5, and 7 were compared based on the measured values.
Allograft and postoperative tissue analysis
Recipient rabbits were anesthetized with sodium pentobarbital (30 mg/kg, Sigma, USA). The tracheal stroma of the control group and the experimental group were transplanted subcutaneously into the New Zealand white rabbits. The skin on the back of the neck was incised, and the superficial fascia was isolated. The side of the spine was separated to form a skin capsule, and the tissue was embedded into it, followed by interrupted suture, and the transplanted samples of each group were harvested 30 days after transplantation.
The obtained tissue samples were immersed in 10% neutral formalin buffer for 24 h, embedded in paraffin, and sectioned. H&E staining was used to observe changes in the tracheal matrix structure and the inflammatory response in each group. CD68 immunohistochemical staining (1:200 dilution, Abcam, China) was used to observe macrophage changes.
Statistical analysis
The experimental data were analyzed using SPSS 20.0, and each group of data was expressed as the mean ± standard deviation. The significance of the difference between the two groups was analyzed by t-test, and the difference between three groups and above was analyzed by analysis of variance (ANOVA) (p < 0.05 was considered statistically significant).
Results
Macroscopic observation of tracheal matrix
In the control group, alternating red and white colors were seen on the surface of the natural trachea, with white cartilage ring and red matrix. The macroscopic appearance of the acellular tracheal matrix of the two-cycle and four-cycle groups was similar to that of the control group, but their matrix was white. No defect or collapse was found in the lumen of the acellular tracheal matrix (Figure 1).
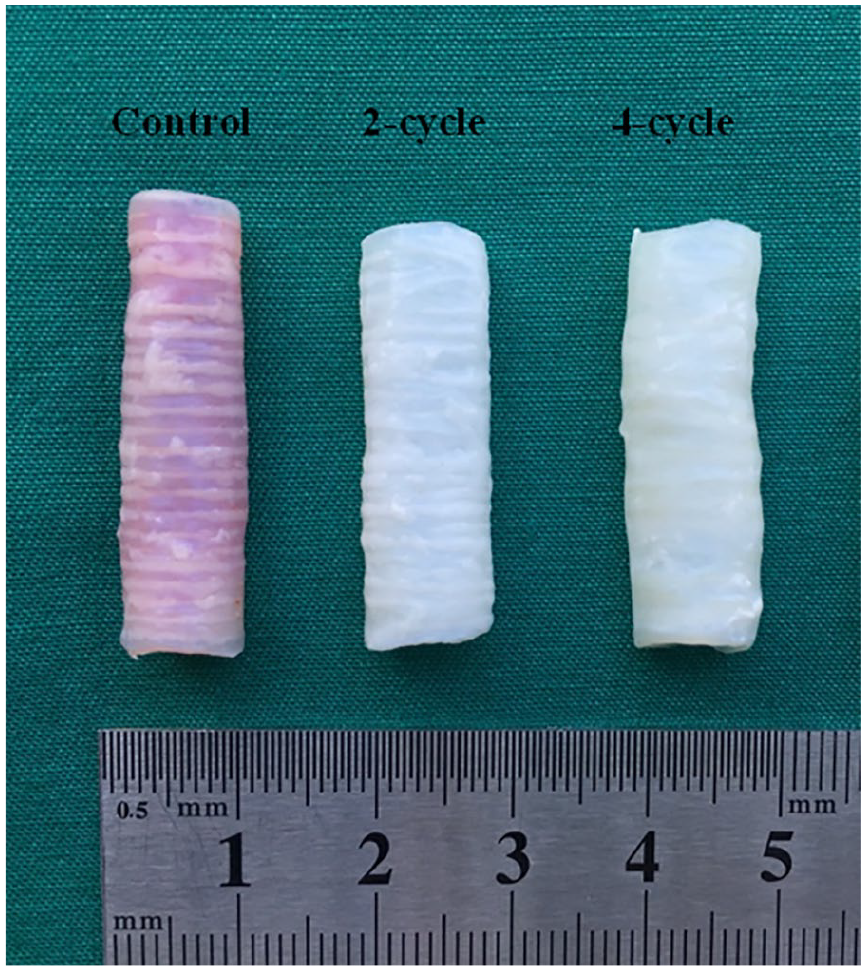
Macroscopic appearance of the trachea matrix of natural trachea, two-cycle group and four-cycle group.
Preliminary observation of the effect of rabbit tracheal decellularization
H&E staining showed that there were many cilia on the surface of the tracheal matrix in the control group, the structure was clear, and a large number of nuclei were present in the mucosa and submucosa (Figure 2(a)). The nuclei of the noncartilage tissue (mucosa, submucosa, and adventitia) of the matrix of the two-cycle group and the four-cycle group were basically removed (Figure 2(b) and (c)). The Masson trichrome staining results showed that the main structures of the tracheal stromal submucosa, basement membrane, and cartilage were retained in the two-cycle and four-cycle groups after decellularization, and there was no obvious structural loss in the experimental groups compared with the control group (Figure 2(d)–(f)). GAG was qualitatively analyzed by Safranin O staining. In the control group, GAG was mainly expressed in the cartilage area (Figure 2(h)). After decellularization, the GAG of the tracheal cartilage was significantly reduced (Figure 2(i) and (f)).
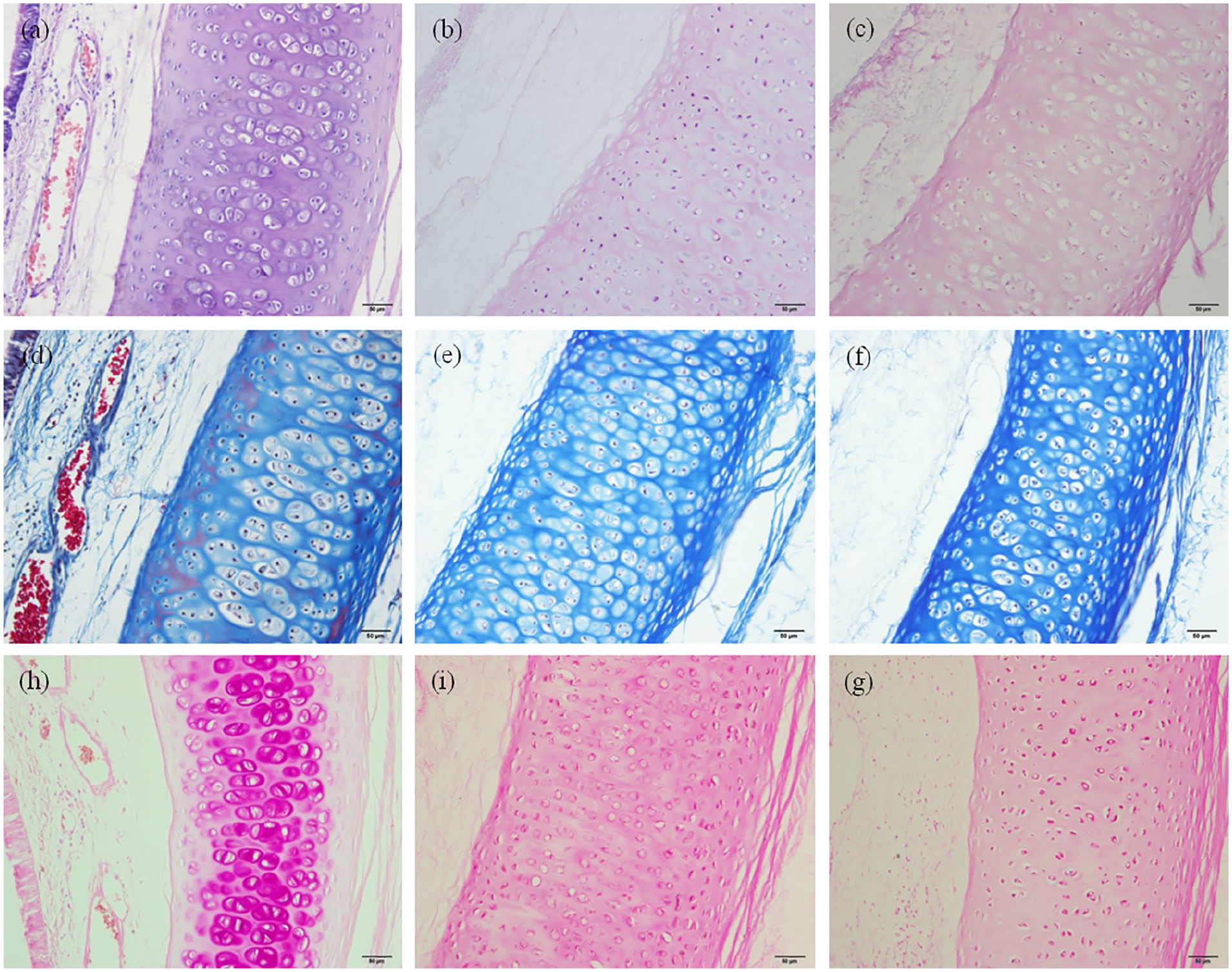
Structural changes of tracheal matrix before and after decellularization. The (a–c) H&E, (d–f) Masson trichrome, and (h–g) Safranin O staining stained (a, d, h) natural trachea, (b, e, i) the two-cycle group, and (c, f, g) the four-cycle group ((a–g): ×200).
Biochemical assay of GAG and DNA
GAG biochemical analysis a 39% loss of GAG in the two-cycle group (49.53 ± 6.42 μg/mg) compared with natural trachea (81.26 ± 4.13 μg/mg, p < 0.05).
DNA quantification analysis showed that DNA concentration in tracheal samples decreased significantly after decellularization. Compared with natural trachea (549.23 ± 58.94 ng/mg), the DNA content (76.18 ± 14.55 ng/mg, p < 0.05) in the two-cycle group decreased significantly. With the increase of the decellularization cycle, the DNA residual amount in the four-cycle group (52.14 ± 11.36 ng/mg, p > 0.05) was further reduced compared with the two-cycle group, but the decrease was not significant and had no statistical significance.
Evaluation of matrix antigenicity
MHC immunohistochemical staining showed that mucosal and submucosal MHC-I antigens were positively expressed in the control group, and the antigens were expressed on the cell membrane surface (dark blue nuclei) (Figure 3(a)). The expression of MHC-I antigens in the nonchondral area of the two-cycle group was essentially absent (Figure 3(b)). As the number of decellularization cycles increased, the chondrocyte MHC-I antigen was gradually removed in the four-cycle group (Figure 3(c)). MHC-II immunohistochemical staining further showed that stromal nonchondral tissue MHC-II was completely removed after 2 cycles, and the cellular immune response was weak (Figure 3(e)).
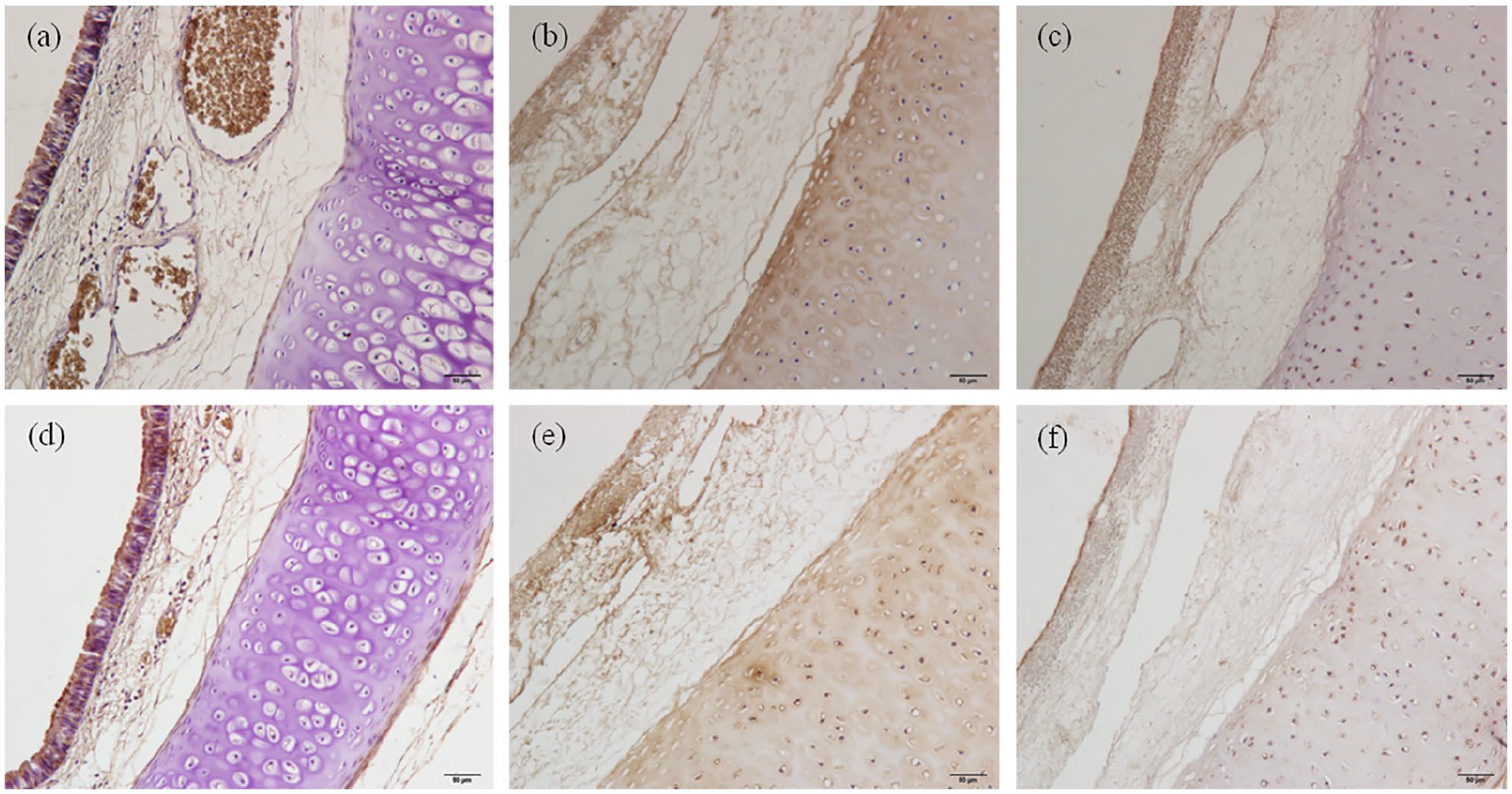
Tracheal antigen removal effects. The (a–c) MHC-I and (d, e) MHC-II stained (a, d) natural trachea, (b, e) the two-cycle group, and (c, f) the four-cycle group. As the number of decellularization cycles increased, the chondrocyte MHC-I and MHC-II antigen was gradually removed ((a–f):×200).
Scanning electron microscopy
Scanning electron microscopy showed that the mucosal layer of the control group was covered with a large number of cilia, and the swing was consistent (Figure 4(a) and (d)). Figure 4(b) and (e) shows that the ciliated epithelial cells of the matrix were removed, the matrix basement membrane was intact, and the surface was undulating in the two-cycle group. The basement membrane of the four-cycle group began to show an increased number of fine gaps, loose structure, collagen fiber exposure, and weakened mechanical strength (Figure 4(c) and (f)). The above results indicate that a tracheal scaffold retaining the ultrastructure (complete basement membrane) can be obtained after two decellularization cycles.
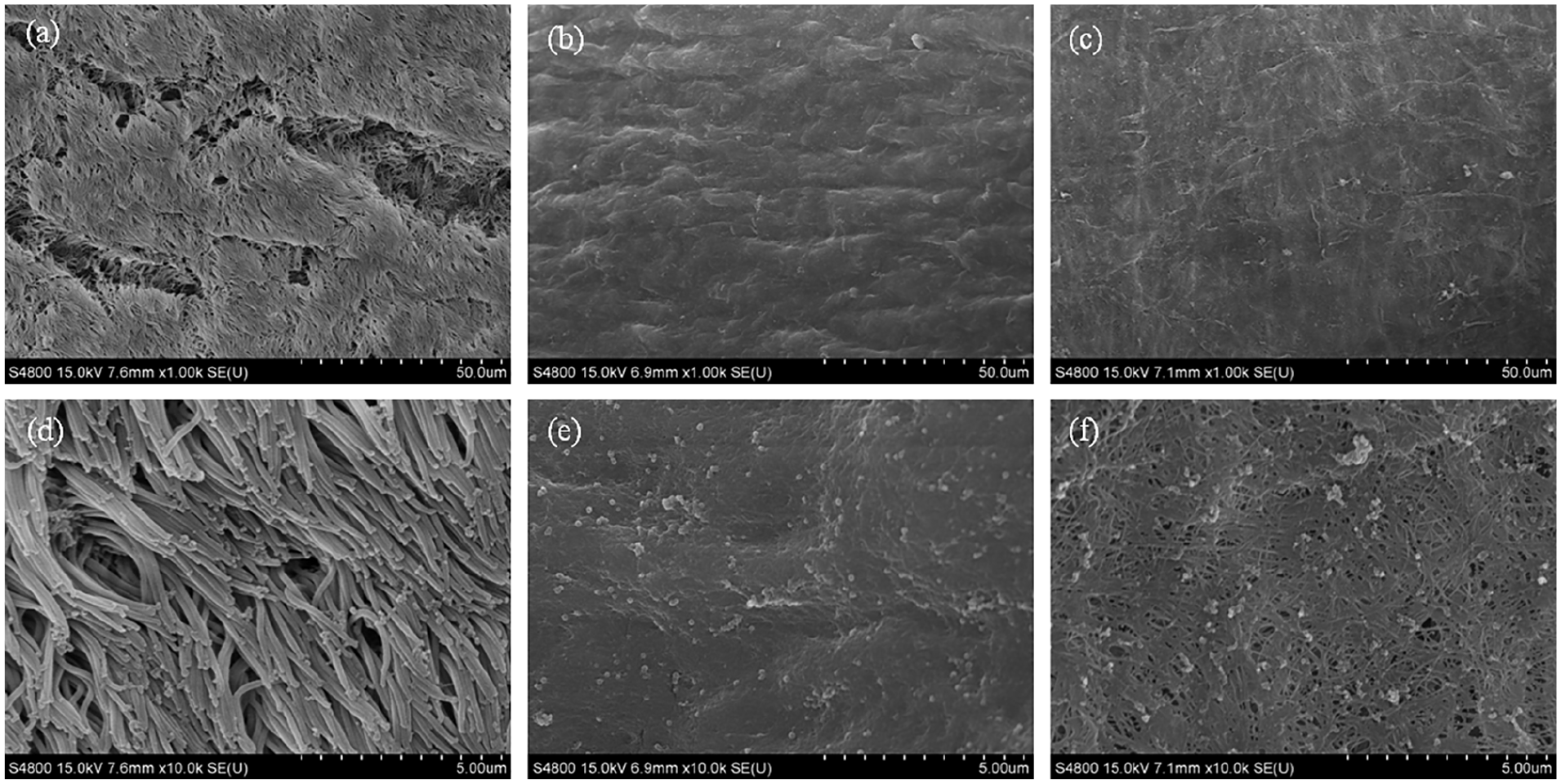
Scanning electron microscopy comparison of tracheal stroma between the control group and the experimental group. (a, d) A large number of regular cilia were observed on the surface of the control group samples. (b, e) The cilia in the two-cycle group samples were all detached, and the basement membrane was relatively smooth. (c, f) Some collagen fibers were exposed in the basement membrane of the four-cycle group samples.
Mechanical properties
The diameter, length, and thickness of the tracheas in the control group, the two-cycle group, and the four-cycle group were measured by the universal tensile tester (Table 1). There was no significant difference between the groups. Compared with that in the control group, the stress loading causing 50% deformation and the elastic modulus of the tracheal matrix decreased slightly in the two-cycle group, and the decrease of elastic modulus was statistically significant (p > 0.05); the stress loading causing 50% deformation and the elastic modulus of the four-cycle group matrix were further decreased (p < 0.05, Table 1). All groups of tracheal stroma could be restored to the initial state of the lumen after the compression test, indicating that the tracheal matrix material retains toughness after decellularization.
Mechanical properties of the tracheal matrix.
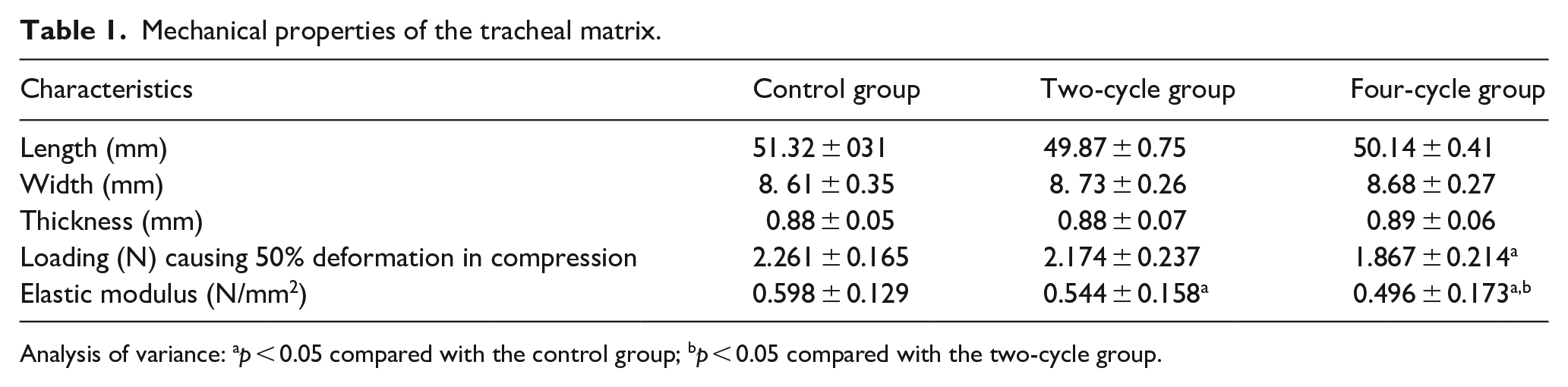
Analysis of variance: ap < 0.05 compared with the control group; bp < 0.05 compared with the two-cycle group.
In vitro biocompatibility assessment
The biocompatibility of a material is one of the key indicators that determine whether it can be used in vivo experiments. SEM qualitatively revealed that the rabbit BMSCs inoculated on the substrate in the control group, the two-cycle group, and the four-cycle group grew well (Figure 5(a) and (d), (b) and (e), (c) and (f)). The basal cells were closely arranged, and the morphology was normal, indicating that the biocompatibility of the acellular matrix was good, supporting cell adhesion and growth.
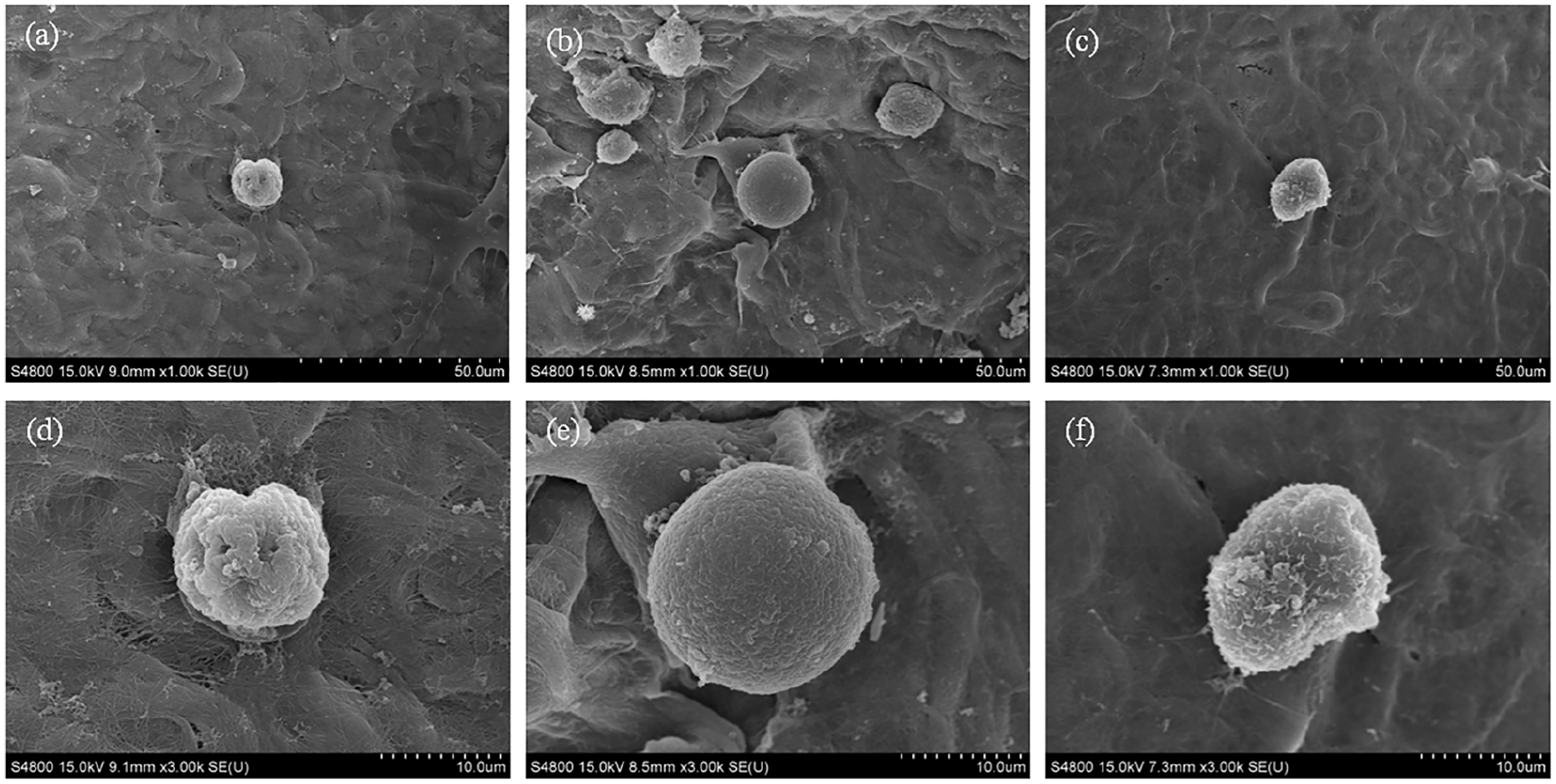
Scanning electron microscopy images after cell inoculation. ((a and d), (b and e), (c and f)) The BMSCs inoculated on the substrate in the control group, the two-cycle group, and the four-cycle group grew well.
The CCK-8 results quantitatively showed that cells in each group proliferated continuously and their number continuously increased in the first 3–5 days; the proliferation of cells in the experimental group was greater than that in the control group (p < 0.05, Table 2). On the seventh day, the number of cells began to decrease, which may be due to contact inhibition and autologous apoptosis. The analysis of the OD values of each group showed that the number of cells in the control group was the lowest, and the number of cells in the two-cycle group and the four-cycle group was increased, indicating that the biocompatibility of the tracheal matrix was increased by decellularization.
The stem cell-inoculated samples were tested by CCK-8 at different time points.
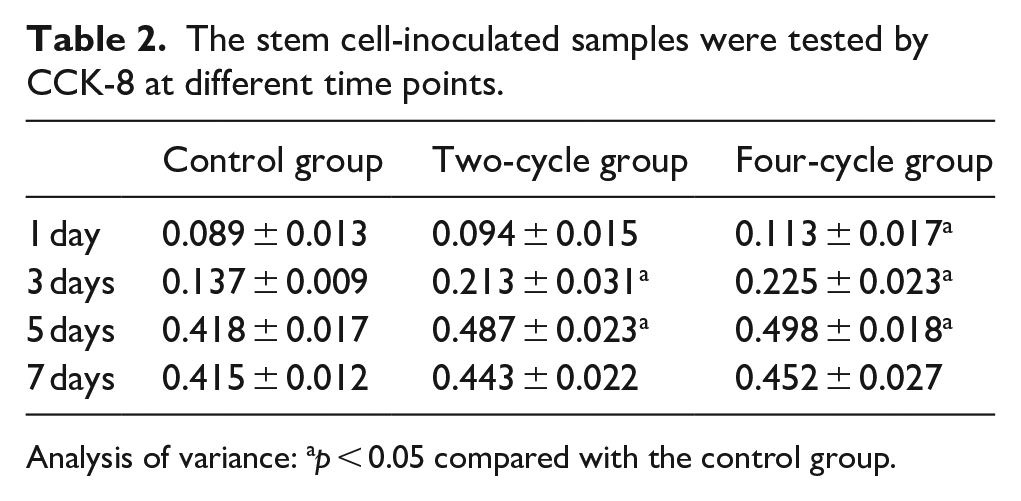
Analysis of variance: ap < 0.05 compared with the control group.
In vivo evaluation of allogeneic transplantation
Postoperative H&E staining showed that host cell infiltration was evident in each group. The structure of the trachea in the natural control group was disordered, the cartilage tissue was destroyed, the gland structure was lost, and increased inflammatory cell infiltration was observed in the matrix (Figure 6(a)). In the two-cycle group, the tracheal matrix structure was clear, inflammatory cell infiltration was reduced, and there were no adverse reactions, such as calcification in the matrix (Figure 6(b)). In the four-cycle group, the matrix structure was loose, and there was inflammatory cell infiltration in the surrounding tissues (Figure 6(c)). Immunohistochemical staining of CD68 showed that the control group had structural disorder and a large number of infiltrating macrophages (Figure 6(d)). The matrix structure of the two-cycle and the four-cycle groups was clear, the cartilage ring structure was visible, and the macrophage infiltration was reduced (Figure 6(e) and (f)).
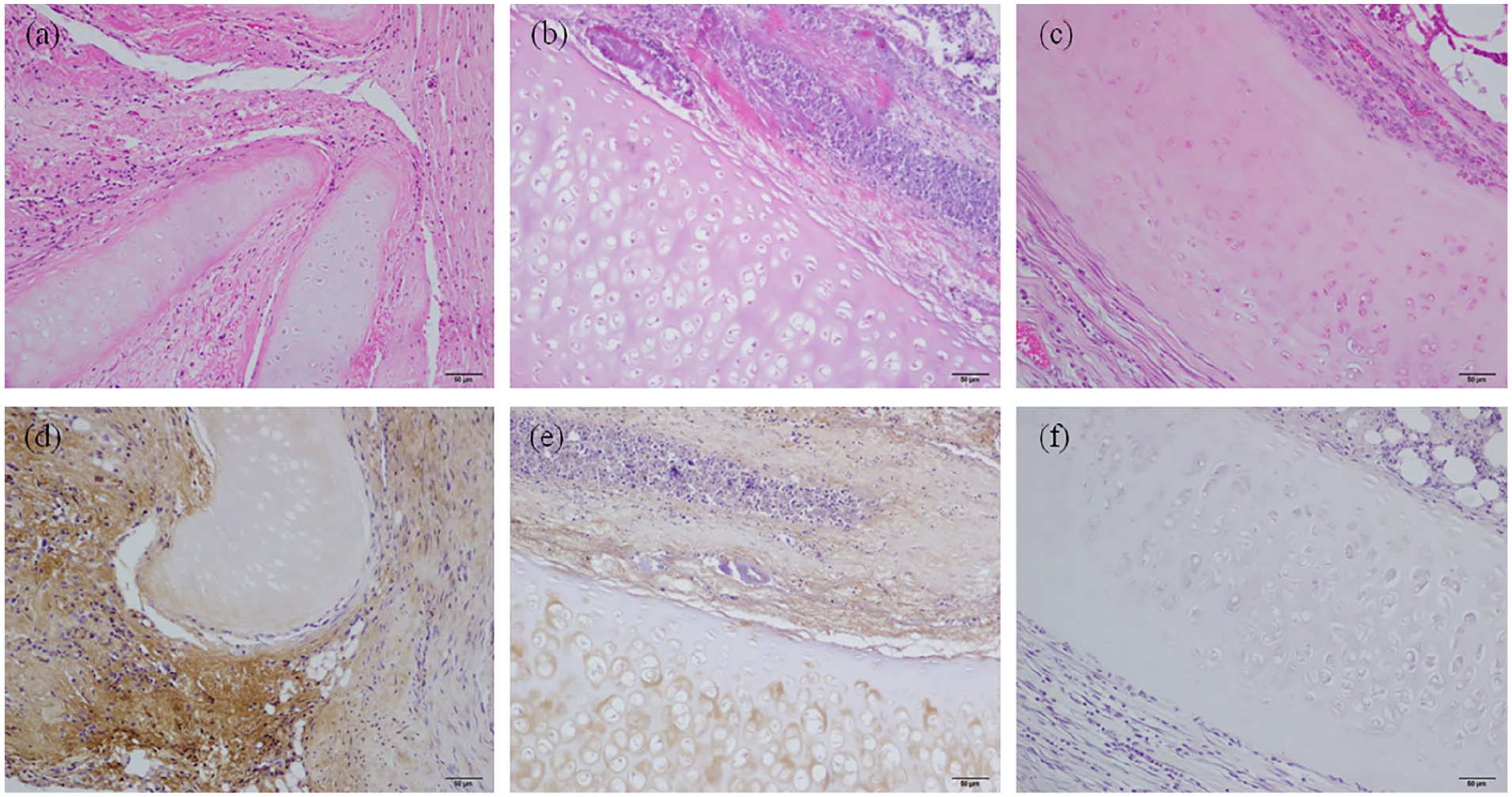
Evaluation of the in vivo biocompatibility in the (a, d)) control group, (b, e) two-cycle group, and (c and f) four-cycle group. Comparison of (a–c) H&E staining and (d–f) CD68 immunohistochemical staining 30 days after allograft transplantation in each group ((a–f): ×200).
Discussion
With the successful application of tissue engineering decellularization technology in clinical tracheal transplantation cases,5,9,15 methods to accelerate the preparation of tracheal acellular matrix are being continuously developed by scholars.23–25 In this study, we investigated the effect increasing the DNase concentration in DEM on reducing the number of preparation cycles for rabbit acellular tracheal matrix and evaluated the changes in the main structure, immunogenicity, mechanical properties, ECM components, and biocompatibility of the tracheal matrix before and after acellularization. The experimental results showed that it took only 4 days from the acquisition of the trachea to final decellularized scaffold formation and good biocompatibility and mechanical properties of the tracheal matrix were maintained. Compared with the general rabbit tracheal DEM scheme (9–10 days),26,27 the preparation time of this novel scheme is reduced by more than 1 time, providing an option for patients who need urgent clinical tracheal replacement for a long-term tracheal injury and also provides data supporting the expansion of the clinical application of acellular tracheal matrix.
The immunological rejection of tracheal grafts has been the biggest obstacle to the success of tracheal replacement, and its immunogenicity is mainly derived from the epithelial and mucosal lamina propria.25,27,28 Decellularization technology can effectively dissolve epithelial and mucosal cells in natural trachea through detergents and enzymes, remove the immunogenicity of the matrix, and eliminate the need for immunosuppressive agents to reduce rejection after surgery.9,10 Studies have shown that nonchondral cells, such as those in the epithelium, interstitium, and muscle of the tracheal matrix of rabbits, are completely eliminated by seven DEM cycles, and MHC-II antigens are removed. At seven cycles, scanning electron microscopy showed that the tracheal matrix had a complete basement membrane with a smooth surface. However, as the decellularization cycle number increases, the basement membrane begins to rupture (after 8 DEM cycles), and the mechanical properties decrease. 21 To explore the effect of increasing the DEM DNase concentration on reducing the number of tracheal decellularization cycles, in this experiment, DEM with an increased DNase concentration (50 kU/mL) was used. After two cycles, all nonchondral tissue cells (epithelial, mucosal, submucosal, and adventitial) in the rabbit tracheal matrix were completely removed, and MHC-I and MHC-II antigens were eliminated. The matrix basement membrane also remains intact. However, as the number of decellularization cycles increased, the collagen fibers were exposed and an increased number of fine gaps appeared on the surface of the basement membrane of the experimental group and gradually increased, which is consistent with findings of other studies.14,24
The tracheal matrix has good biocompatibility after decellularization and preserves the tracheal ECM.12,17 The retention of proteins such as collagen and GAGs in the ECM determines the mechanical properties of the tracheal matrix.25,29 We observed that there was no significant change in the collagen fibers of the experimental group after decellularization but Safranin O staining showed that the GAG content in the experimental group was significantly reduced after decellularization. This phenomenon explains the stress loading causing 50% deformation and the elastic modulus result in the experimental group, as other authors have shown.23,30,31 Some studies have shown that the tensile properties of the post acellularization tracheal matrix are similar to those of natural tracheas,17,32 and this has been further confirmed by previous studies in our laboratory. 21 Therefore, this experiment only evaluates the changes in biomechanical properties before and after decellularization by the stress loading causing 50% deformation and the elastic modulus.
The ideal tracheal scaffold supports cell adhesion and growth, providing a supportive environment for functional tracheal remodeling.8,9 The CCK-8 results showed that the proliferation of the acellular stromal cells was greater than that of the control cells on the third to fifth days (p < 0.05). The cell inoculation test also confirmed that BMSCs grew well on the acellular matrix, which is consistent with the findings of other scholars.13,26 The above results indicate that the acellular tracheal matrix prepared in this study has good in vitro biocompatibility and supports cell growth and proliferation.
To further confirm the low immunogenicity of the DEM-prepared matrix using an increased DNase (50 kU/mL) concentration, we embedded the acellular matrix on the backs of New Zealand white rabbits to simulate allogeneic transplantation. Immunosuppressive agents were not used after surgery, and each group of grafts was removed for comparison after 30 days. Compared with the control group, the two-cycle acellular matrix showed no histological signs of obvious rejection, the macrophage infiltration was reduced, and the inflammatory response was significantly reduced. The results of the in vivo experiments further indicate that the prepared acellular tracheal matrix is biocompatible and meets the stringent requirements for successful decellularization. 33
Shortening the preparation time of acellular tracheal matrix is a promising strategy,16,17,34 providing treatment options for patients undergoing clinical and emergency tracheal replacement therapy. In this study, although the modified DEM with an increased DNase concentration shortened the preparation time of the acellular tracheal matrix, the chemicals used in the decellularization process damaged the cells and the ECM, and the residue may also have toxic effects on the tracheal matrix. 14 Therefore, the protocol needs to be further optimized to ensure the effective removal of all immunogenic components in the shortest time and to minimize detergent and enzyme residues.
Conclusion
In summary, a modified DEM with an increased DNase (50 kU/mL) concentration requires only two cycles (4 days) to obtain a decellularized rabbit tracheal matrix with a short preparation time, good biocompatibility, suitable mechanical properties, and reduced preparation cost. This study provides data to support the expansion of the range of clinical decellularization technologies.
Research Data
Orginial_date – Supplemental material for Rapid preparation of decellularized trachea as a 3D scaffold for organ engineering
Supplemental material, Orginial_date for Rapid preparation of decellularized trachea as a 3D scaffold for organ engineering by Zhihao Wang, Fei Sun, Yi Lu, Shu Pan, Wenlong Yang, Guozhong Zhang, Jun Ma and Hongcan Shi in The International Journal of Artificial Organs
Footnotes
Acknowledgements
Thanks to the Center for Comparative Medical Research of Yangzhou University for help, and my teacher Professor Shi for his guidance and colleagues’ encouragement.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the National Natural Science Foundation of China (Grant No. 81770018), Taizhou People’s Hospital Foundation (Grant No.ZL201830), and Jiangsu Graduate Research Innovation Program (Grant No.XKYCX19_153).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.