
Abstract
Background:
Hemodynamic parameters at rest are known to correlate poorly with peak oxygen uptake (VO2) in heart failure. However, we hypothesized that hemodynamic parameters at rest could predict exercise capacity in patients with left ventricular assist device (LVAD), because LVAD pump rotational speed does not respond during exercise. Therefore, we investigated the relationships between hemodynamic parameters at rest (measured with right heart catheterization) and exercise capacity (measured with cardiopulmonary exercise testing) in patients with implantable LVAD.
Methods:
We performed a retrospective medical record review of patients who received implantable LVAD at our institution from November 2013 to December 2017.
Results:
A total of 20 patients were enrolled in this study (15 males; mean age, 45.8 years; median duration of LVAD support, 356 days). The mean peak VO2 and cardiac index (CI) were 13.5 mL/kg/min and 2.6 L/min/m2, respectively. CI and hemoglobin level were significantly associated with peak VO2 (CI: r = 0.632, p = 0.003; hemoglobin: r = 0.520, p = 0.019). In addition, pulmonary capillary wedge pressure, right atrial pressure, and right ventricular stroke work index were also significantly associated with peak VO2. In multiple linear regression analysis, CI and hemoglobin level remained independent predictors of peak VO2 (CI: β = 0.559, p = 0.006; hemoglobin: β = 0.414, p = 0.049).
Conclusions:
CI at rest and hemoglobin level are associated with poor exercise capacity in patients with LVAD.
Introduction
Implantable left ventricular assist devices (LVADs) are life-saving therapy for patients with advanced heart failure (HF) that do not improve or stabilize with optimal medical therapy. LVAD has increasingly been used as a bridge to transplantation, as destination therapy, and as a bridge to recovery.1–4 Although support with implantable LVAD improves survival,2,5 several studies have shown that some patients continue to have persistent symptoms of severe HF and limited exercise capacity even after device implantation.6–9 It is known that decline in exercise tolerance causes low quality of life and is a powerful prognostic factor, both in HF and in patients with LVAD.9–11 Therefore, it is important to maintain exercise capacity in these patients over long periods. Identification of patients who have symptoms of HF and correction of reversible causes of poor exercise tolerance are important issues in patients with implantable LVAD.
Exercise capacity in patients with HF is strongly determined by cardiac function and skeletal muscle function.12–16 Cardiac contractile reserve and heart rate reserve during incremental exercise contribute to increased peak oxygen uptake (VO2). In contrast, hemodynamic parameters at rest, such as cardiac index (CI) and left ventricular ejection fraction, are known to correlate poorly with peak VO2.12–16 Thus, we cannot estimate exercise tolerance precisely without a stress test in patients with HF. It would be useful and meaningful in the clinical setting if exercise capacity was associated with or could be predicted based on hemodynamics at rest. In patients with LVAD, cardiac output through aortic valve is limited, and, in some patients, all systemic circulation is generated through LVAD because the aortic valve closes continuously. 17 And, increasing pump rotational speed leads to increase in cardiac output and decrease in pulmonary capillary wedge pressure. 18 These findings indicate that hemodynamics at rest in patients with LVAD is strongly affected by and dependent on LVAD pump. Because LVAD pump rotational speed does not change during exercise, the hemodynamics during exercise may approximate that at rest. Thus, we hypothesized that hemodynamic parameters at rest could predict exercise capacity in patients with LVAD. The associations between hemodynamic parameters at rest and exercise capacity in patients with LVAD have not been fully elaborated. Therefore, the purpose of this study was to clarify the associations between hemodynamics at rest and exercise capacity in patients with LVAD by analyzing hemodynamic parameters obtained with right heart catheterization (RHC) and exercise parameters assessed with cardiopulmonary exercise testing (CPX).
Methods
We performed a retrospective medical record review of patients who received implantable LVAD as a bridge to transplantation at our medical center from November 2013 to December 2017. Of these 27 patients, we enrolled the patients who were re-hospitalized for scheduled evaluation and education for LVAD. During this hospitalization, RHC and CPX were performed and the interval of these two examinations was within 1 week. We analyzed these data and evaluated the associations between hemodynamic parameters and peak VO2. All patients were required to be in clinically stable condition with no changes in LVAD setting and medication including diuretics, beta blockers, and angiotensin-converting enzyme inhibitors within 1 month of RHC or CPX.
All subjects enrolled in this research have given their informed consent, which has been approved by my institutional committee on human research, and this protocol has been found acceptable by them (approval number: 2017-0031).
Baseline clinical parameters at the timing of RHC, including demographics (age, sex, body mass index, body surface area, etiology, atrial fibrillation), treatments (cardio resynchronization therapy with defibrillator, implantable cardioverter defibrillator), LVAD pump data (pump rotational speed, power, pulse index, pump flow), and laboratory data (hemoglobin, lactate dehydrogenase, creatinine) were reviewed.
CPX was performed with a cycle ergometer (BK-ERG-121; Mitsubishi Electric Engineering Company Limited, Tokyo, Japan), with breath-by-breath gas exchange measurements made with a computerized metabolic cart (AE-300S; Minato Medical Science, Osaka, Japan). After 1 min of rest on the ergometer, exercise began with a 3-min period of unloaded exercise at 50 revolutions per minute followed by a 10-watt increase in loading every minute. Electrocardiogram, heart rate, VO2, and respiratory exchange ratio were continuously monitored throughout the study. No subjects developed new-onset arrhythmia, angina, or significant electrocardiographic changes during exercise. The test was terminated when the patient showed maximal volitional fatigue, VO2 leveled off, or objective withdrawal criteria were met. Peak VO2 was defined as the highest VO2 during the last 30 s of exercise.
For RHC, a 6-French thermodilution catheter (Biosensors International Pte Ltd, Singapore) was introduced via the internal jugular vein and advanced into the pulmonary artery under fluoroscopic observation. Right atrial pressure, mean pulmonary arterial pressure, and pulmonary capillary wedge pressure were measured at the end of expiration. CI was determined with thermodilution by averaging three measurements with a maximum deviation of 10%. Right ventricular stroke volume index was calculated with the following formula: Right ventricular stroke work index (mmHg × mL/m2) = {[mean pulmonary arterial pressure (mmHg)—mean right atrial pressure (mmHg)] × [CI (L/min/m2)/heart rate (beats/min)]. A systemic arterial catheter was also placed via the radial artery to evaluate systemic arterial pressures. The analyzed RHC parameters were at the same pump speed as when the CPX was performed and the pump rotational speed was not changed between these two evaluations.
Echocardiography was performed with the ALOKA ProSound Alpha 7 (Hitachi Aloka Medical Systems, Tokyo, Japan). Left ventricular ejection fraction, left ventricular end-diastolic dimension, and left ventricular end-systolic dimension were measured in standard M-mode. 19 Echocardiography was performed on the day of RHC.
Continuous variables are expressed as mean ± standard deviation or median with lower and upper quartiles, as appropriate. Continuous variables were compared by t-test. The associations between hemodynamic parameters obtained with RHC and peak VO2 were analyzed with Pearson’s correlation coefficient. Age and sex are widely recognized as contributing to peak VO2; CI and hemoglobin level are components of the Fick formula.20,21 Thus, multivariate linear regression analysis was performed to evaluate the predictors of peak VO2 using the variables of age, sex, hemoglobin, and CI. All statistical analyses were performed with PASW Statistics 18 (SPSS Inc., Chicago, IL, USA). P values <0.05 were considered statistically significant.
Results
A total of 20 patients (15 males; mean age, 45.8 years; median duration of LVAD support, 356 days) were analyzed in this study. Patient characteristics at the timing of RHC are listed in Table 1. The LVAD pump used in all patients was HeartMate IITM (Thoratec, Pleasanton, CA). Medical therapy was not changed between RHC and CPX in all patients. The mean left ventricular ejection fraction was 16.5% before the operation and remained low even after LVAD implantation. In three patients the aortic valve opened regularly at rest. To the contrary, in the remaining 17 patients, the aortic valve closed continuously, and two of them showed severe regurgitation. These two cases were managed conservatively as outpatients without surgery because no end-organ damage or pulmonary or systemic congestion resulting from HF was recognized. Hemoglobin level tended to be low as a whole and the prevalence of anemia (Male: hemoglobin level <13 g/dL, female: hemoglobin level <12 g/dL) was considerably high of 75%.
Patient characteristics at the timing of right heart catheterization.
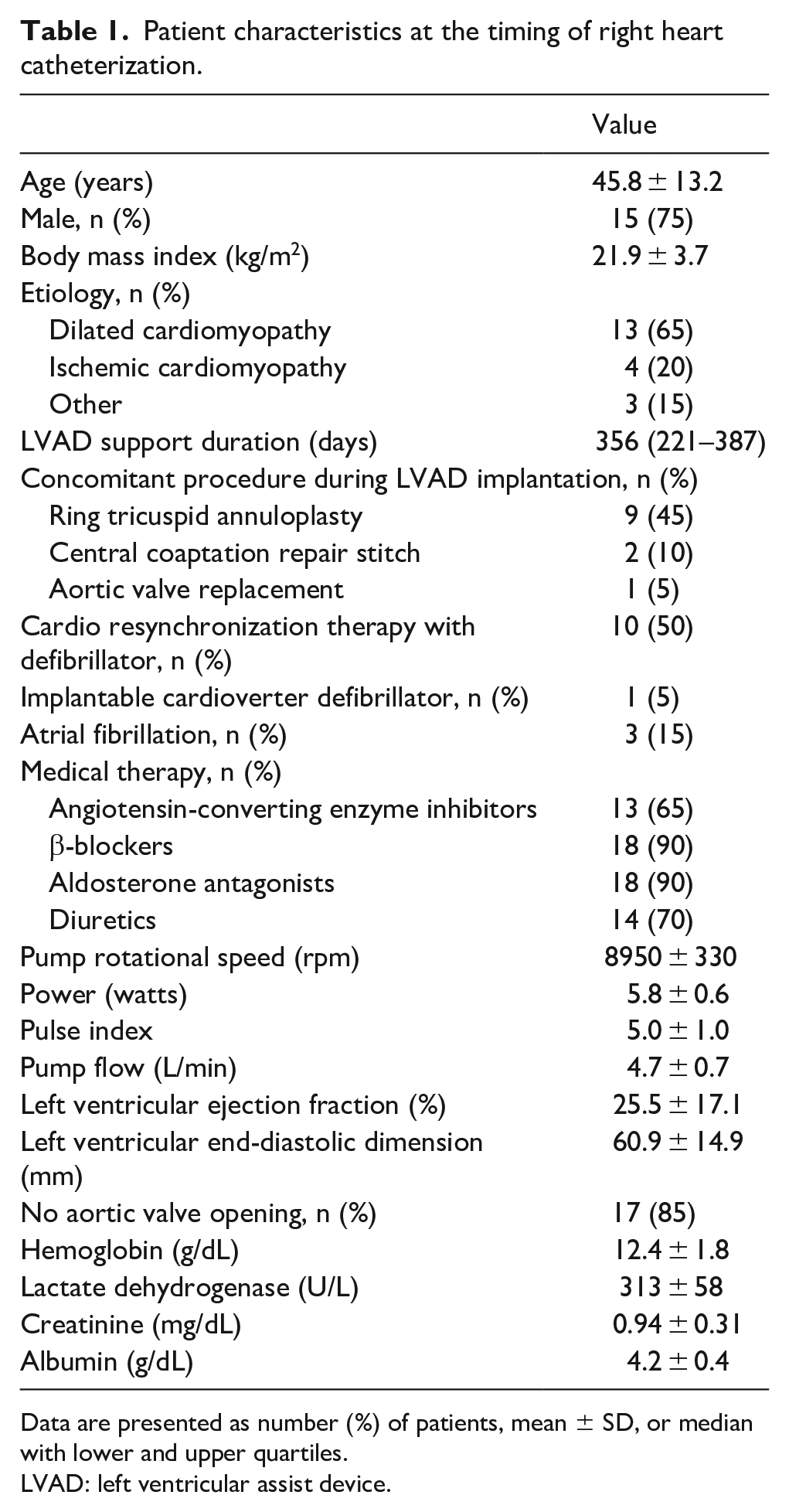
Data are presented as number (%) of patients, mean ± SD, or median with lower and upper quartiles.
LVAD: left ventricular assist device.
RHC parameters and CPX parameters are shown in Table 2. The mean CI was 2.6 ± 0.5 L/min/m2. The mean pulmonary capillary wedge pressure and right atrial pressure indicated that patients generally had well-controlled HF after LVAD implantation; however, the mean right ventricular stroke work index tended to be low. In the CPX results, the mean peak respiratory exchange ratio was >1.15, indicating maximum or near-maximum exercise stress. Among patients with pacemakers, only one showed an atrial paced rhythm at rest; however, the heart rate was not dependent on the pacemaker during exercise in any patient. Peak VO2 was markedly low at 13.5 ± 3.7 mL/min/kg compared with normal subjects, which was almost equivalent to previously reported peak VO2 after LVAD implantation. 8 Peak VO2 in patients whose aortic valve regularly open was significantly higher than in patients whose aortic valve does not open (18.6 ± 2.1 mL/min/kg vs 12.6 ± 3.2 mL/min/kg, p = 0.007). However, peak VO2 was similar between the patients with or without tricuspid annuloplasty (13.1 ± 2.9 mL/min/kg vs 13.8 ± 4.4 mL/kg/min, p = 0.682) and between the patients with or without aortic valve surgery (11.8 ± 0.61 mL/min/kg vs 13.8 ± 3.97, p = 0.063).
Right heart catheterization and cardiopulmonary exercise testing parameters.
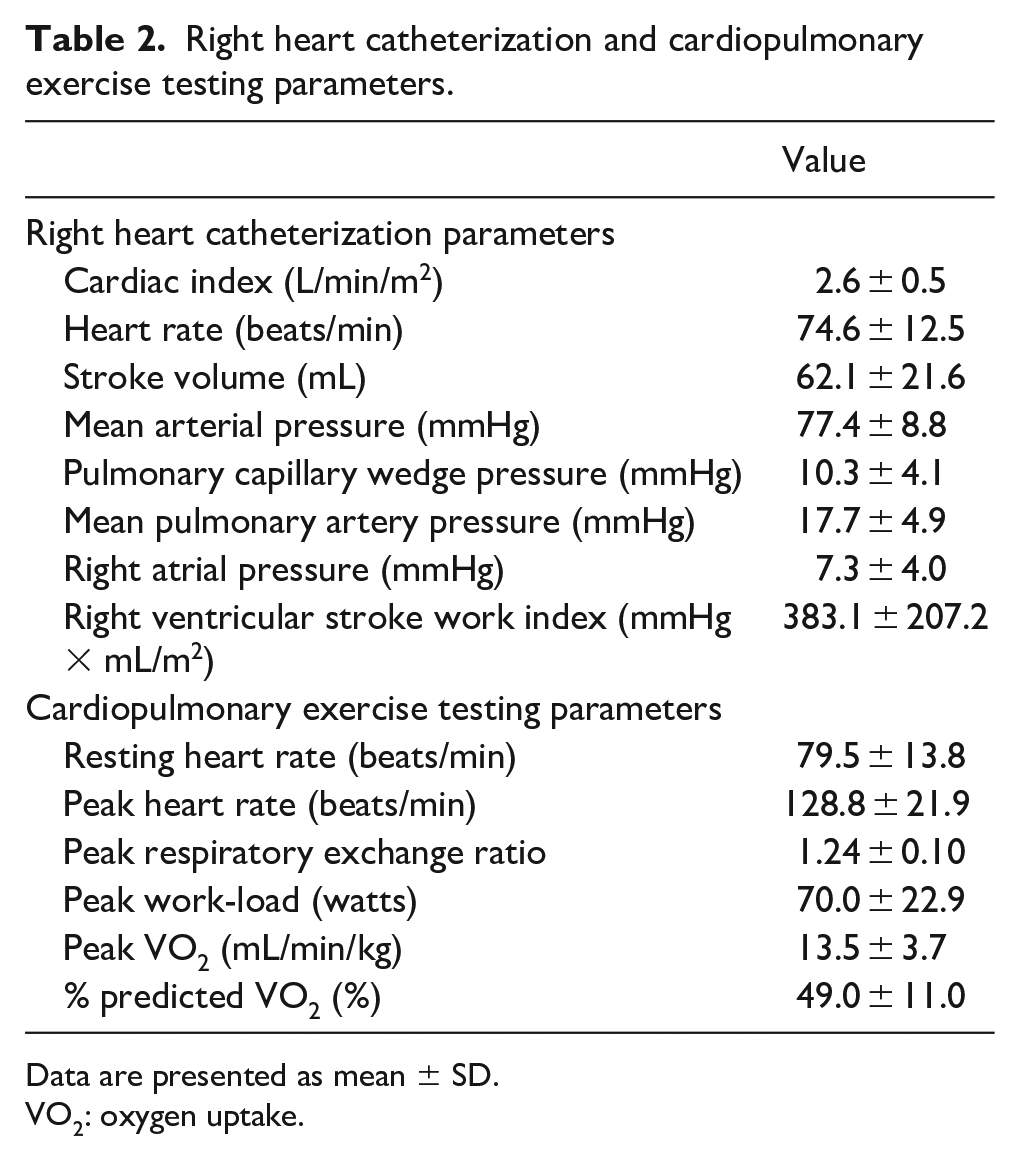
Data are presented as mean ± SD.
VO2: oxygen uptake.
The correlations between hemodynamic parameters at rest and peak VO2 are listed in Table 3. CI and hemoglobin level were strongly and positively correlated with peak VO2 (CI: r = 0.632, p = 0.003; hemoglobin: r = 0.520, p = 0.019) (Figure 1). The right ventricular stroke work index also had a significant relationship with peak VO2 (r = 0.463, p = 0.040). In contrast, pulmonary capillary wedge pressure and right atrial pressure were negatively related to peak VO2. Left ventricular ejection fraction, resting heart rate, and peak heart rate did not have significant correlations with peak VO2. In multiple linear regression analysis (Table 4), CI and hemoglobin level remained independent predictors of peak VO2 (CI: β = 0.559, p = 0.006; hemoglobin: β = 0.414, p = 0.049). Age and sex were not significant predictors of peak VO2 in this study.
Correlations between hemodynamic parameters at rest and peak VO2.
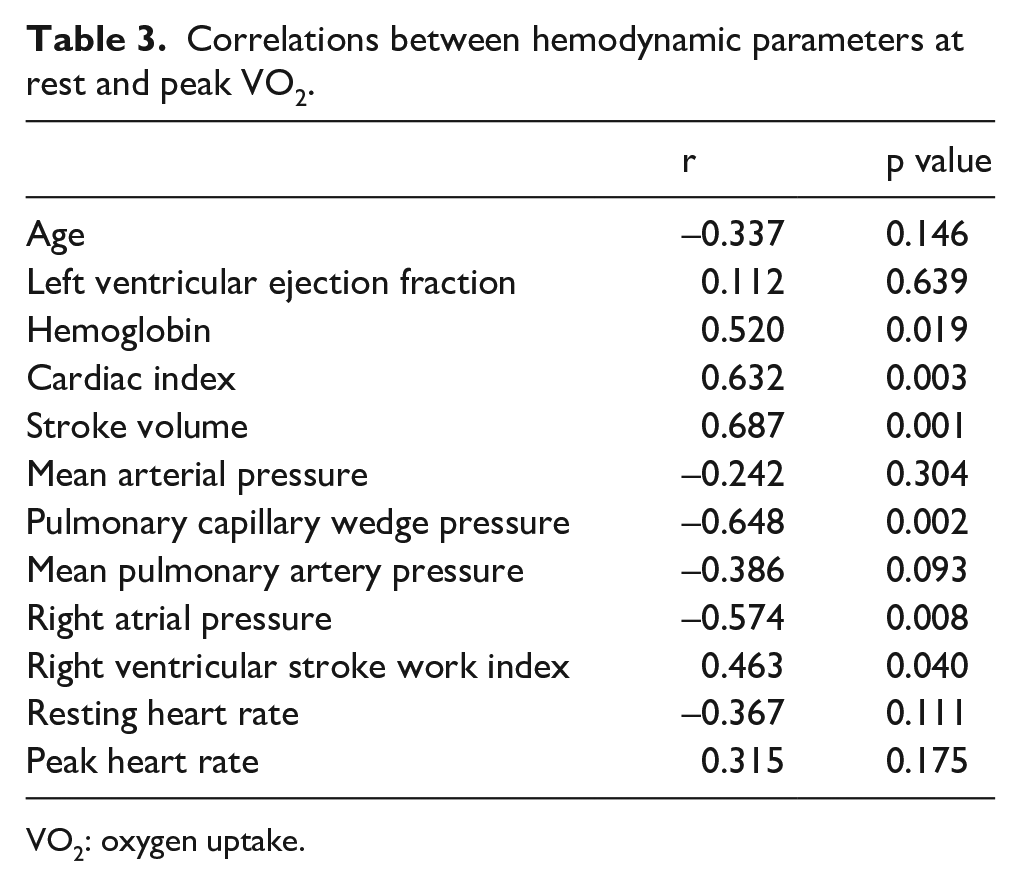
VO2: oxygen uptake.
Multivariate linear regression analysis of factors contributing to peak VO2.
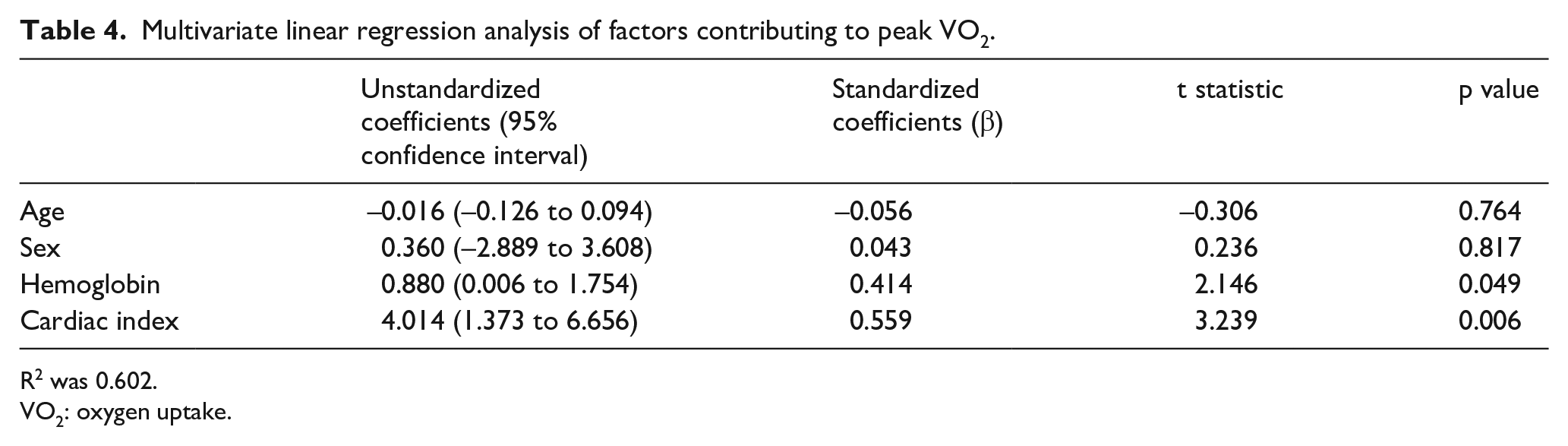
R2 was 0.602.
VO2: oxygen uptake.
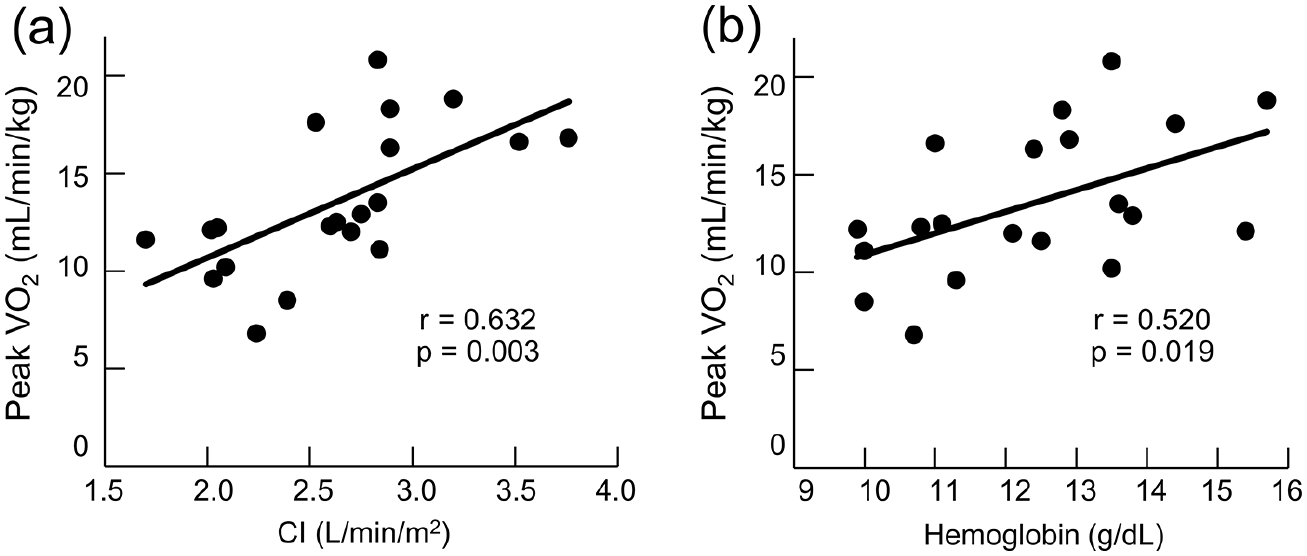
Relationships between CI or hemoglobin level and peak VO2. (a) Relationship between CI and peak VO2, (b) Relationship between hemoglobin level and peak VO2.
Discussion
In this study, we clarified that CI and hemoglobin level were associated with exercise capacity in patients with implantable LVAD. One of our main results indicates that hemodynamic parameters at rest can help identify patients with poor exercise capacity.
Despite the poor relationship between hemodynamic parameters at rest and exercise capacity in patients with HF,12,15,16 our results indicate that CI at rest was associated with exercise capacity in patients with LVAD. Several hemodynamic features help explain this finding. First, contractile reserve during stress is highly injured in patients with LVAD. Contractile reserve during stress is an important determinant of exercise capacity, but contractility at rest cannot be used to predict exercise capacity in HF patients because of large differences in contractile reserve among patients.12,13,15,16 In contrast, advanced HF patients with severely reduced left ventricular ejection fraction who need to wear implantable LVAD generally have reduced contractile reserve. 22 Thus, contractility during exercise would be similar to and related to contractility at rest. In addition, large dependence on LVAD pump would reduce the effect of contractility reserve on exercise hemodynamics. Second, hemodynamics during exercise is less dependent on heart rate in patients with LVAD than those without LVAD. Although heart rate reserve during stress is the main contributor to elevated CI in HF patients, 14 other studies demonstrated that heart rate elevation did not necessarily lead to increased CI in patients with LVAD.17,23 Finally, most importantly, pump rotational speed does not respond during exercise automatically despite the fact that the flow through the pump is strongly dependent on the pump rotational speed. The above features would result in the specific hemodynamics that is less affected by the heart’s function and is strongly dependent on LVAD pump flow, not only at rest but also during exercise. Therefore, CI at rest was related to exercise capacity because of the similarity between hemodynamics at rest and during exercise in patients with LVAD. However, we have to pay attention to interpreting our result because it was derived from our study population that mainly occupied patients with severely impaired left ventricular function.
The results that CI contributes to exercise capacity provides a beneficial strategy for managing patients with HF symptoms or exercise intolerance after LVAD implantation: increasing CI at rest may improve symptoms in these patients. Several studies demonstrated that increasing pump rotational speed improved both CI at rest and exercise capacity, a finding consistent with our results.24–26 A higher rotational speed has short-term advantages in hemodynamics, but sometimes causes aortic insufficiency and right ventricular failure over the longer term.27–29 Thus, we hope the future study which demonstrates that amelioration of CI without increasing rotational speed is effective in improving exercise intolerance; modifying the CI with medications such as diuretics and pulmonary hypertension drugs. And, physical therapy is more actively recommended for patients with reduced CI. In addition, evaluating CI at rest would be beneficial for detecting patients with impaired exercise capacity. Although CI was evaluated by the invasive method in our study, CI is also calculated by echocardiographic parameters using right ventricular outflow tract velocity time integral and diameter theoretically. 30
Next, the significant relationship between hemoglobin level and exercise capacity also offers several important clinical implications. The reason why anemia relates to exercise capacity can be introduced by Fick formula; that is, decreased arterial oxygen content by anemia impairs oxygen delivery during exercise. Many patients with LVAD complicate anemia and have a relatively high frequency of iron deficiency, 31 and erythrocyte trauma, or hemolysis. 32 Thus, treatment and prevention of anemia against iron deficiency and hemolysis should be attempted.
The finding that right ventricular stroke work index, right atrial pressure, and pulmonary capillary wedge pressure were related to peak VO2 may reflect the influence of insufficient unloaded cardiac preload or impaired right heart function on exercise capacity. In fact, patients with reduced right heart function are known to have poor exercise capacity, 33 which would be explained by insufficient blood flow from the right ventricle to the left ventricle during exercise. Thus, management to improve residual right heart function and to prevent its deterioration has an important role in maintaining exercise tolerance in patients with LVAD. In addition, we found a poor relationship between exercise capacity and hemodynamic parameters before LVAD implantation (Supplemental Table S1). This result could be attributed to the poor relationship between hemodynamic parameters before versus after implantation, and implies that exercise capacity after LVAD implantation cannot be predicted based on hemodynamic parameters before implantation.
This study has several limitations that need to be addressed. First, we did not evaluate the impact of skeletal muscle function on exercise capacity in this study. Nevertheless, the effect of own cardiac function and LVAD pump flow on exercise capacity must be larger than that of skeletal muscle function because exercise capacity reaches a plateau at 50% of the level of normal subjects 3 to 6 months after LVAD implantation and improves further after heart transplantation.6–8 Second, our population did not include patients with congenital heart disease or hypertrophic cardiomyopathy; these patients have different HF characteristics than patients with reduced left ventricular ejection fraction. Third, the sample number of patients in this study was limited, which may affect the results. Although more factors that may be related to the exercise capacity other than the age and the gender should have been evaluated, there was no choice but to limit the variables used for the multiple linear regression analysis to avoid model overfitting, leading to the wider 95% confidence interval. Thus, our results should be evaluated in the future study which has a large sample size. Finally, the only LVAD device used at our institution was the Heart Mate IITM. The result is not necessarily the same in other devices due to the difference of pump characteristic curve. The relationship between pump flow and pressure of pump head shows flatter with a wide range of pump flow in centrifugal-flow pump than in axial-flow pump. This indicates that small change of pressure generates larger pump flow increase, and may hypothesize that higher pump flow during exercise in patients with centrifugal-pump leads to higher exercise capacity than in patient with axial-pump. 8 Thus, further study is needed to confirm the relationship between the hemodynamics at rest and exercise capacity in patients with other LVAD.
In conclusion, CI at rest and hemoglobin level are related to exercise capacity in patients with LVAD. Modifying CI at rest and correcting anemia may be beneficial strategies to improve residual HF symptoms and exercise intolerance in this population.
Supplemental Material
Supplementary_Table_S1_20200722 – Supplemental material for Associations between hemodynamic parameters at rest and exercise capacity in patients with implantable left ventricular assist devices
Supplemental material, Supplementary_Table_S1_20200722 for Associations between hemodynamic parameters at rest and exercise capacity in patients with implantable left ventricular assist devices by Toru Kondo, Takahiro Okumura, Hideo Oishi, Yoshihito Arao, Hiroo Kato, Shogo Yamaguchi, Tasuku Kuwayama, Tomoaki Haga, Tsuyoshi Yokoi, Hiroaki Hiraiwa, Kenji Fukaya, Akinori Sawamura, Ryota Morimoto, Masato Mutsuga, Kazuro Fujimoto, Akihiko Usui and Toyoaki Murohara in The International Journal of Artificial Organs
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: T.O. received lecture fees from Ono Yakuhin, Novartis, Medtronics, and Otsuka, and received research grants from Ono Yakuhin, Bayer, Daiichi-Sankyo, and Amgen Astellas (not in connection with the submitted work). A.U. received research grants from TERUMO, Edwards Lifesciences, JAPAN LIFELINE, Mitsubishi Tanabe, Medtronic Japan, Senko medical instrument, St. Jude Medical, Pfizer, Daiichi-Sankyo, iCorNet, Trestech, and NIPRO. T.M. received lecture fees and unrestricted research grants from the Department of Cardiology at Nagoya University Graduate School of Medicine, Bayer, Daiichi-Sankyo, Dainippon Sumitomo, Kowa, MSD, Mitsubishi Tanabe, Boehringer Ingelheim, Novartis, Pfizer, Sanofi-Aventis, Takeda, Astellas, Otsuka, and Teijin.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by JSPS KAKENHI Grant Number 19K17592.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.