
Abstract
Aims:
To elaborate on early survival in patients with mitral valve replacement requiring temporary extracorporeal life support system (ECLS).
Methods:
We analyzed survival, significant bleeding, wound infection, and ECLS duration in 421 from 14,400 patients with postoperative need for ECLS from January 2008 to December 2017 at our institution. Finally, patients were stratified according to the type of surgery performed: the mitral group (mitral valve replacement) n = 63 and the control group (any cardiac surgery excluding the mitral valve) n = 358. In order to adjust for preoperative patient characteristics, a propensity matching analysis was performed. Differences in in-hospital mortality were analyzed accordingly.
Results:
In-hospital mortality was significantly higher in the mitral group as compared to the control group before and after adjustment (p < 0.001). Median duration of ECLS was 4 days in both groups. Perioperative bleeding (p < 0.001) and wound infection (p < 0.001) also showed significant worse outcome parameters in the mitral group. The main causes of death in the mitral group were multiorgan failure, n = 48 (76%), stroke, n = 7 (12%), and intracardiac thrombus formation, n = 5 (10%).
Conclusions:
ECLS is associated with a high in-hospital mortality rate in patients after mitral valve replacement.
Introduction
Extracorporeal life support (ECLS) system has become an indispensable treatment option for cardiothoracic patients experiencing postcardiotomy cardiogenic shock. Postcardiotomy cardiogenic shock occurs in approximately 3%–5% of patients 1 and approximately 1% of these patients eventually require prolonged postoperative circulatory support owing to refractory hemodynamic and or respiratory dysfunction.1–3 There is a relatively high rate of complications in patients with mitral valve prostheses requiring temporary ECLS.3,4 These complications vary from bleeding, wound infection, stroke, intracardiac thrombus formation, multiorgan failure, and eventually death.3,4 The current evidence guiding surgeons in patient selection and the management of ECLS is based mostly on scarce data: retrospective observational data and a few single center case series.4,5
In this study, we evaluated the outcome of patients requiring temporary ECLS support after cardiac surgery. We hypothesize that patients after mitral valve replacement are at an extra risk whenever they require ECLS support.
Methods
Study population and objectives
Our inclusion criteria were patients with postcardiotomy cardiogenic shock requiring temporary ECLS at our institution from January 2008 to the end of December 2017. Patient data were extracted from the institutional database and included the following variables: patient characteristics (e.g. age, sex, height, and weight), clinical history (e.g. previous cardiac operation and cardiovascular risk factors), echocardiographic variables (e.g. ejection fraction, right ventricular function, and valve status and size), ECLS implantation, and duration as well as and laboratory variables and any existing follow-up data. Anticoagulation during ECLS circulation was done using unfractured heparin and partial thromboplastin time was measured every 4 h. Targeted partial thromboplastin time was between 60 and 80 s.
Parameters analyzed
We analyzed significant bleeding (requiring blood transfusion ⩾ 6 packed red blood cells or surgical intervention), wound infection requiring a vacuum assisted treatment and ECLS duration in 421 patients during a 9-year period. We used full heparin coated tubes (tip-to-tip) and membrane oxygenator for the ECLS connection. Finally, patients were stratified according to the type of surgery needed: the mitral group (mitral valve replacement) n = 63 and the control group (no mitral valve replacement) n = 358. Differences in in-hospital mortality were analyzed accordingly. The subvalvular apparatus was spared during mitral valve replacement.
Statistics
Discrete variables are reported as counts (percentages) and continuous variables as median and quartiles. For discrete variables, we tested differences between groups with the χ2-test or Fisher’s exact test when expected cell sizes were less than 5. The Mann–Whitney U test was used for comparison of non-Gaussian continuous variables. To balance for baseline characteristics and differences in terms of risk factors between the two groups we used a propensity score matching technique. About 58 patients in the mitral group were matched with 58 patients in the control group in a 1:1 ratio based on the propensity score using a caliper set at 0.1. Only clinically relevant variables were entered in the propensity score matching analysis. Matching variables were sex, age, BMI, Diabetes mellitus, hypertension, coronary heart disease, hypercholesterinemia, preoperative left ventricular function, and vascular complications. A multivariate logistic regression analysis was performed in order to identify risk factors for increased mortality. The analyses were run using the R software version 3.6.1 for MacOS. A significant p value was set at <0.001.
Results
Patient characteristics
Patient characteristics are shown in Table 1. From 2008 to 2017, 14,400 patients received open heart surgery at our institution. We identified 421 patients (2.9%) meeting the inclusion criteria: mitral group (mitral valve replacement) n = 63 and the control group (no mitral valve replacement) n = 358. In-hospital data was complete within our study period. Median ages in the mitral and control groups were 69 and 60, respectively. The median body mass indices in both groups were 26.3. Median left ventricular ejection fraction was 50% in the mitral group and <35% in the control group. Coronary heart disease was present in 58.7% in the mitral group and in 60.8% in the control group.
Patient demographics after adjustment.
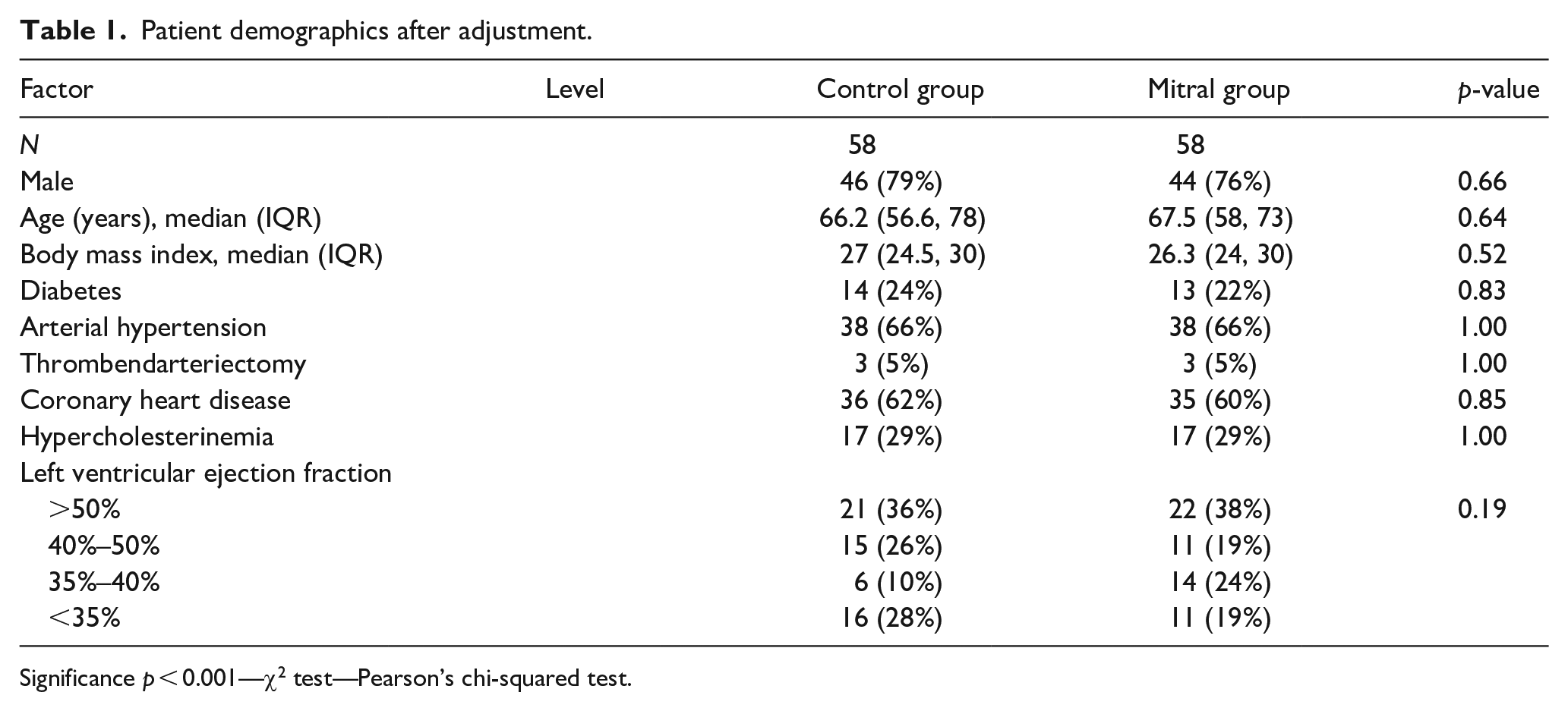
Significance p < 0.001—χ2 test—Pearson’s chi-squared test.
Surgical details
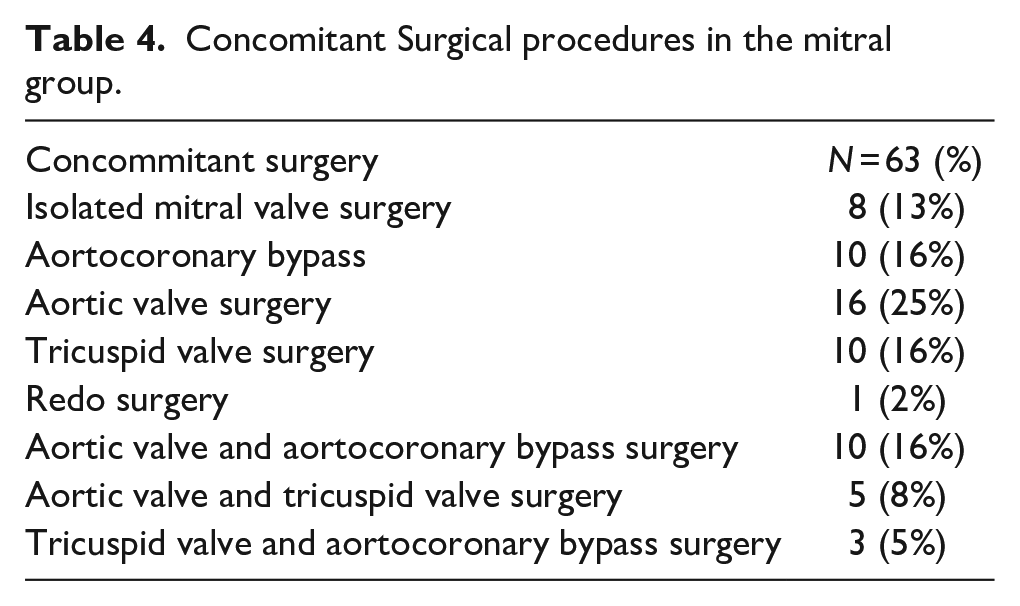
Table 2 show surgical details of the patient cohort. We had 63 patients in the mitral group. The mitral valve pathology was mainly degenerative in nature (Table 3 Supplemental Files). The median cross clamp time was 143 min for the mitral group and 92 min for the control group. Median Bypass time was 215 min for the mitral group and 152 min for the control group. In the mitral group, 52 patients (82.5%) received bioprostheses and 11 patients (17.5%) received mechanical prostheses. More blood products (red blood cells, plasma, and platelet bags) were used in the mitral group (Table 2). Table 4 shows the list of concomitant surgical procedures in the mitral group.
Surgical details of the whole cohort (unadjusted).
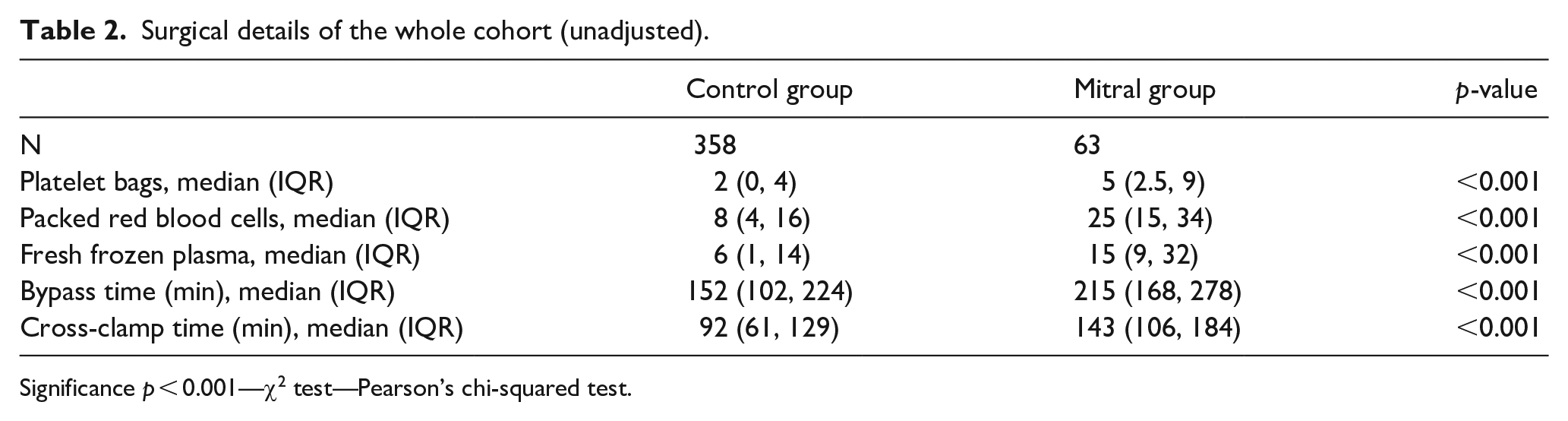
Significance p < 0.001—χ2 test—Pearson’s chi-squared test.
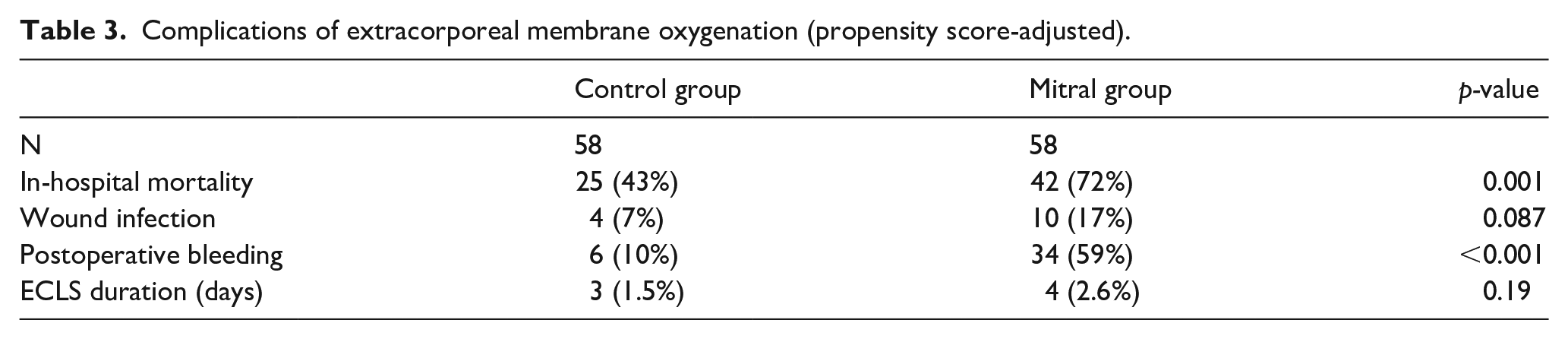
Complications of extracorporeal membrane oxygenation (propensity score-adjusted).
Concomitant Surgical procedures in the mitral group.
ECLS Circuit/Management strategy
All patients in this cohort had a postcardiotomy cardiogenic shock requiring temporary ECLS support. ECLS circulation was routinely established through the femoral vessels. In 5% of the patients (n = 3) in the mitral group, an Impella® (Abiomed, Danvers, USA) was implanted. Other 21% of the patients received an intra-aortic balloon pump (IABP). No device to reduce cardiac afterload was implanted in the control group. Median duration of the ECLS was 4 days in both groups.
Perioperative outcome
Perioperative data is shown in Tables 2 and 3. In-hospital mortality was statistically significantly different with 72.6% in the mitral group and 40.1% in the control group (p < 0.001) before propensity score analysis. After adjustment we observed again statistically significant difference in mortality with 72% for the mitral group and 43% for the control group (p < 0.001; Figures 1 and 2). There was a statistically significant difference in postoperative bleeding with 34% for mitral group and 6% for control group (p < 0.001). Before Propensity score adjustments we had a significant difference in wound infection (p = 0.017). The main causes of death in the mitral group were multiorgan failure with uncontrolled bleeding as well as intracardiac thrombus formation. In the multivariate logistic regression analysis, mitral valve surgery was found to have a strongly significant correlation to mortality (Table 5).
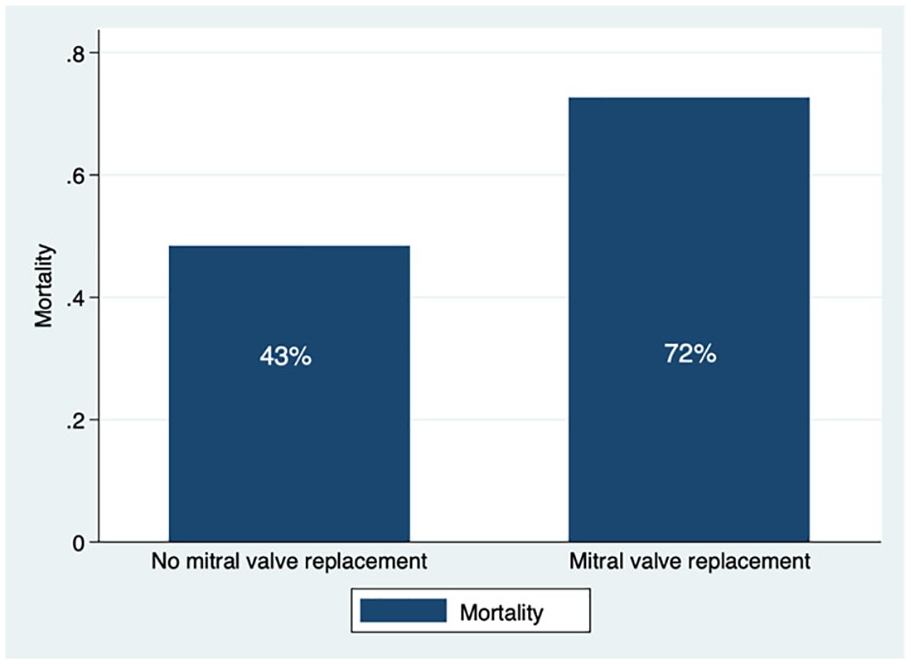
Adjusted in-hospital mortality (p < 0.001).
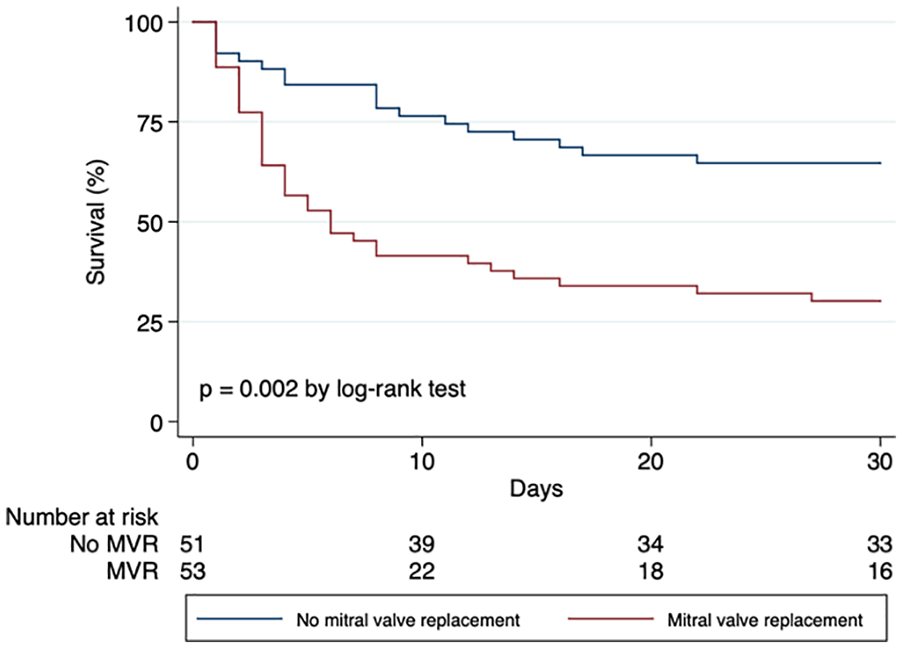
Kaplan–Meier survival curve depicting in-hospital mortality.
Multivariate logistic regression.
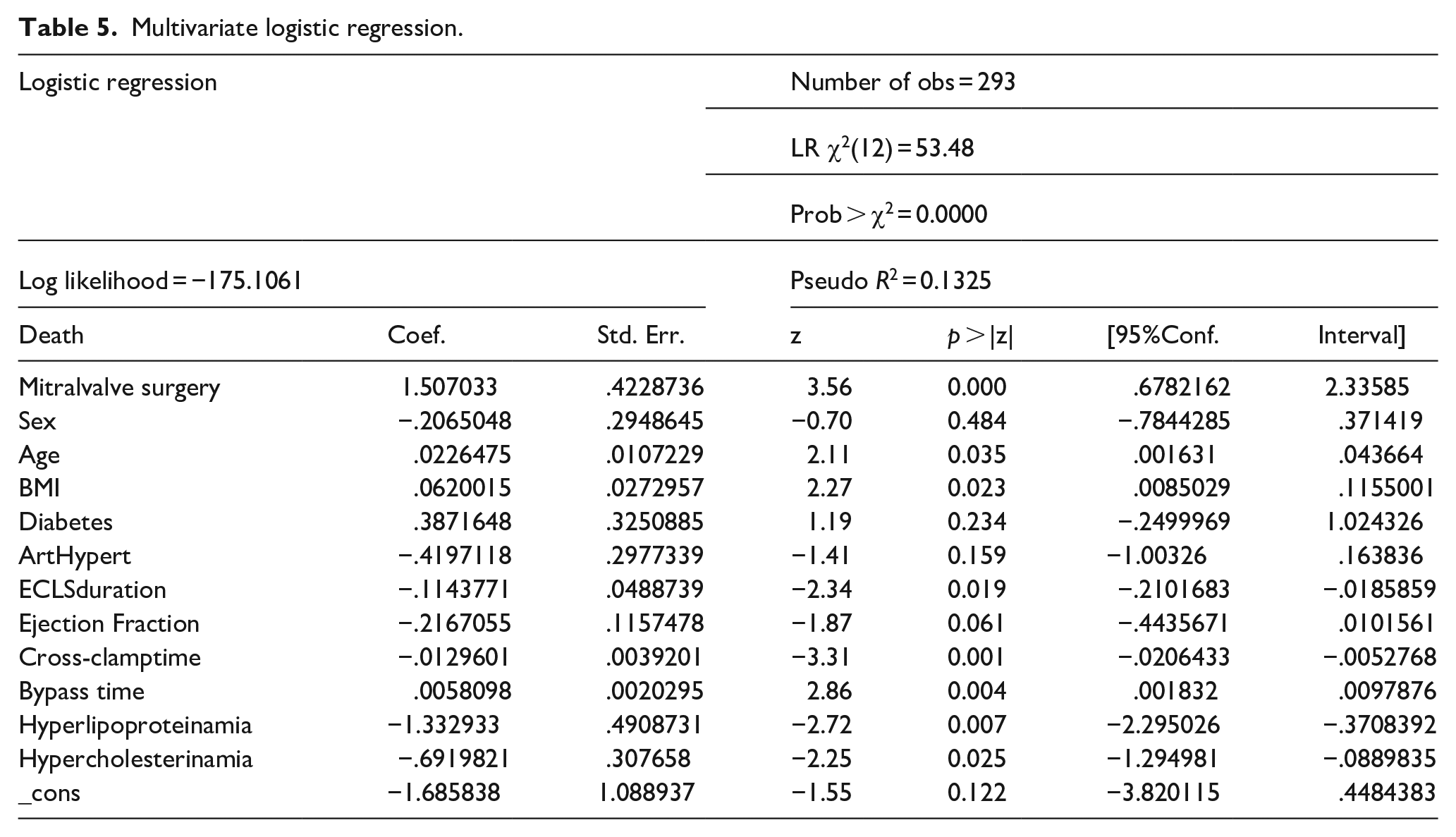
The area under the ROC Curve was 0.7188.
Discussion
In this study we report about a relatively aged patient population with poor cardiac function and life-threatening comorbidities. All these factors make the management of these patients relatively challenging. Doll et al. 3 were faced with similar challenges in their study. Patients in the mitral group had a higher perioperative risk of mortality. Similar patient characteristics have been reported by previous studies3,4 which concurs with the data in our study; however, in much smaller cohorts and without matching.
Majority of the patients in the mitral group had a degenerative mitral insufficiency. Dahl et al. 4 reports of patients with similar risk profiles and poor long-term prognosis. The median cross clamp time was 143 min for the mitral group and 92 min for the control group. Median Bypass time was 215 min for the mitral group and 152 min for the control group. More blood products (red blood cells, plasma, and platelet bags) were used in the mitral group. These values are suggestive of the complexity of the surgeries in patients in the mitral group which also corresponds with blood products used in both groups. In the mitral group, 52 patients (82.5%) received bio-prostheses despite a median group age of 69 years. This is concurrent with other studies reporting mitral bio prostheses in relatively younger patients.5,6 This could only imply that this patient cohort was severely sick with a poor life expectancy.
ECLS circulation was routinely established through the femoral vessels. The median ECLS duration in both groups was 4 days. The systemic inflammatory reaction induced by this artificial circuit required systemic anticoagulation to avoid thrombosis formation. Anticoagulation during ECLS circulation was done using unfractured heparin while regularly controlling the partial thromboplastin time. The duration of the ECLS therapy as well as the anticoagulation strategy is consistent with the data published by Williams et al. and Alhussein et al. Higher rate of bleeding complications can be explained in part by higher levels of anticoagulation due to the fear for intracardiac thrombus formation.
The retrograde flow in the ECLS results in an increased afterload with reduced transaortic and transmitral blood flow for the already severely impaired left ventricle. This ultimately leads to stagnation in the left ventricle and left atriums as well as the pulmonary venous system with resulting increased pressure in the left cardiac chambers. This combination sets the stage for subendocardial ischemia, thrombus formation, and eventually pulmonary edema. In particular, thrombus formation on the new mitral prosthesis can easily occur in this no- or very low-flow situation. In a bid to reduce the afterload, some patients (n = 3%/5%) received an Impella® (Abiomed, Danvers, USA) and others (n = 13%/21%) received an IABP. Lorusso 7 as well as other studies on this topic8–11 suggest that the reduction of afterload during ECLS therapy should be established if there is no minimal left ventricular ejection and that this could lead to improved survival even though the overall survival still remains poor. We had a relatively low survival which was comparable to other studies.11–15 This goes to underline the point that optimal management strategies in this patient group still remains unclear
There is a documented high in-hospital mortality rate of 50% to 70% among patients requiring ECLS support.16–24 In these studies, old age, evidence of organ system dysfunction, history of previous cardiac operation, extensive aortic operations, neurologic events, and not reducing afterload were stated as predictors of increased mortality. We documented in-hospital mortality rates of 72.6% in the mitral group and 40.1% in the control group before propensity score analysis. After propensity score adjustment, we still had statistical significance with 72% for the mitral group and 43% for the control group.
We did not find any significant difference in the in-hospital mortality between patients with bioprosthetic and mechanical valves (Figure 3). The main cause of death was intracardiac thrombus formation and multiorgan failure with uncontrolled bleeding in both groups. We reportedly implanted very few devices to reduce the afterload (IABP, Impella®; Abiomed, Danvers, USA) and this may well explain the mortality rates as well as the high rates in intracardiac thrombus formations. The concept of afterload reduction to avoid stagnation and thrombus formation in the left cardiac chambers remains a controversial issue in these patients. While there are advocates for and against venting the left cardiac chambers, a proper balance between potential complications and benefits from this approach should be met. Eventually the type of venting system (IABP or Impella®) should be carefully chosen with respect to price, invasiveness, and patient comorbidities. We had both the Impella® and the IABP as venting options which we did not use aggressively because we feared that the complications would outdo benefits in this already very complex treatment strategy. Our institutional approach with the present data is currently changed to either partial ECLS support only in order to allow some antegrade flow through the mitral valve or full support with the obligatory addition of Impella®.
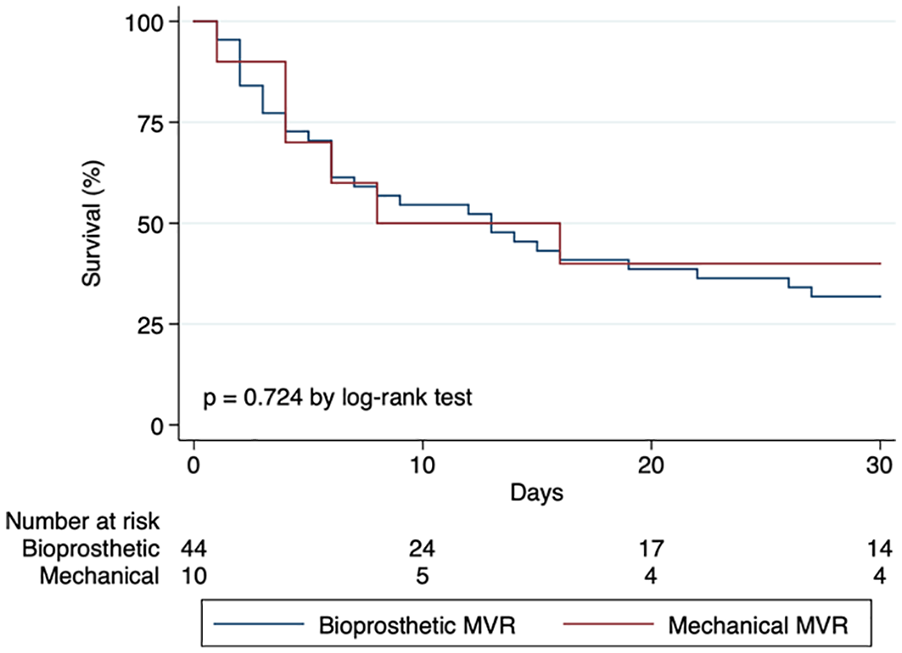
Kaplan Meier survival curve comparing in-hospital mortality between bioprosthetic and mechanical valves.
Mitral valve regurgitation often comes with a boatload of problems for the left ventricle, the main of which is the volume load which eventually leads to left ventricular dysfunction.25–28 The preoperative left ventricular ejection fraction of the adjusted cohort revealed an impaired left ventricular function in 62% of the mitral group and 98% showed at least NYHA stadium two symptoms prior to surgery. Combined to the above factors, the mitral group had significantly longer cross clamp (143 min vs 92 min, p < 0.001) and bypass times (215 min vs 153 min, p < 0.001) compared to the control group. Patients with symptomatic MR and depressed left ventricular functions often present with a diagnostic and management dilemma. We see this clearly reflected in our data and this may be the underlying factor which explains the substantial attrition rate during our observation period.
Vascular complications, wound infection, and perioperative bleeding were higher in our control group, but these complications did not seem to have any significant effect on in-hospital mortality.
Limitations of the study
This is a retrospective study with all adherent limitations. The patient groups and data were disparate and this needed much effort to make them comparable.
Summarizing, ECLS is associated with a high in-hospital mortality rate in patients with mitral valve prostheses. The decision to institute or withdraw this invasive and resource-intensive therapy for postcardiotomy cardiogenic should be an option only in the presence of high-level experience and expertise at individual institution.
Supplemental Material
sj-docx-1-jao-10.1177_0391398820982621 – Supplemental material for Postcardiotomy mechanical support in patients with mitral valve prostheses is associated with poor survival
Supplemental material, sj-docx-1-jao-10.1177_0391398820982621 for Postcardiotomy mechanical support in patients with mitral valve prostheses is associated with poor survival by Clarence Pingpoh, Alaa Salama, Nawras Diab, Maximillian Kreibich, Paul Puiu, Martin Czerny, Christoph Benk, Friedhelm Beyersdorf and Matthias Siepe in The International Journal of Artificial Organs
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This trial was supported by the University Heart Center Freiburg · Bad Krozingen.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.