
Abstract
Aims:
Efficacy of sequential double plasma molecular adsorb system (DPMAS) and plasma exchange (PE) on patients with acute on chronic liver failure (ACLF) has been rarely reported. We hereby reported the outcomes of a consecutive cohort of ACLF patients treated with sequential and mono DPMAS.
Method:
Patients treated with artificial liver support system between January 2011 and December 2016 in XiJing hospital were retrospectively reviewed. A toal of 125 ACLF patients either received mono (DPMAS only) or sequential DPMAS (PE followed by DPMAS) therapy. One to one propensity-score matching (PSM) was used to compare the effects of sequential and mono DPMAS on survival and liver function.
Results:
After PSM, 80 patients were included with 40 patients in each group. Sequential therapy achieved significantly higher removal of total bilirubin, alanine aminotransferase, glutamic oxaloacetic transaminase, and alkaline phosphatase than mono DPMAS, but stabilized international normalized ratio. The effects of both regimens on white blood cell, platelet, creatinine, and liver function scores were similar. Survival rate on 90-day was 50% in the sequential group and 47.5% in the mono group.
Conclusion:
For ACLF patients, sequential DPMAS and PE seemed to have a better effect on liver function improvement but provided no survival benefit compared with mono DPMAS.
Introduction
Acute on chronic liver failure (ACLF) is a severe clinical syndrome with poor prognosis characterized with jaundice, coagulopathy, hepatic encephalopathy, susceptibility to infections, and multi-organ failure. 1 The mortality rate for ACLF varies from 30% to 70% and liver transplantation (LT) remains the only definitive therapeutic option to salvage patients with ACLF. However, it is hampered by donor organ scarcity and high cost. 2
Artificial liver support system (ALSS) is an effective alternative treatment for patients with ACLF.3,4 ALSS can temporarily eliminate toxic substances and prevent the development or exacerbation of secondary organ failure, thus improve the outcome of ACLF patients. Plasma exchange (PE) using fresh frozen plasma (FFP) as replacement fluid is conventionally performed as the main treatment of liver failure for many years. PE can successfully remove both protein-bound and large molecules such as inflammatory mediators5,6; but it is mainly restricted by increased risk of allergies and infections due to exposure to exogenous plasma. 7 Double plasma molecular adsorption system (DPMAS) is a modified hemoperfusion model that combines anion exchange resin and neutral macroporous resin.8–11 It has been used to increase the efficacy of dialysis by circulating blood over two absorbers to remove protein-bound toxins and bilirubin. In comparison with PE, DPMAS does not require large volumes of plasma and has no risk of plasma-associated allergy or blood borne infections. However, DPMAS is more expensive and time-consuming. It was found that DPMAS was less effective than PE in eliminating bilirubin and high sensitive C-reactive protein, but benefit on survival was similar in 12-week between PE and DPMAS. 9 So far, no studies have compared the efficacy of DPMAS (mono) and PE followed by DPMAS (sequential) in ACLF patients. In present study, the therapeutic efficacy and survival of sequential DPMAS and PE with mono DPMAS on the patients with ACLF were compared by using a propensity-score matched analysis.
Methods
Selection of patients
This retrospective case-control study was performed at XiJing hospital of Digestive Diseases, Xi’an, China. The study protocol was approved by the ethics committee of XiJing Hospital of Air Force Medical University. All patients in this study derived from an ACLF cohort that was closely followed in our facility. Patients were followed up until death or day 90. Etiology of ACLF was identified at admission. Whole blood cell count, liver biochemical indices, coagulation status, renal functions were examined at admission, regularly during hospitalization and after discharge. ACLF was diagnosed according to the diagnosis and treatment of liver failure (APASL) guideline 2009.12,13 The inclusion criteria include: between 18 and 70 years of age; presumptive diagnosis of chronic liver disease or compensated liver cirrhosis, rapidly progressive hyperbilirubinemia with serum total bilirubin (TBIL) ⩾ 5mg/dl within 28 days from symptom onset; coagulopathy with international normalized ratio (INR) ⩾1.5 or plasma prothrombin activity <40% complicated within 4 weeks by ascites and/or hepatic encephalopathy (HE). Cirrhosis was diagnosed according to, medical history, physical examination, laboratory tests, and in combination with ultrasonography or computed tomography (CT). The exclusion criteria were: (1) uncontrolled diabetes or hypertension; (2) chronic heart, lung or kidney diseases; (3) malignancy including liver cancer; (4) age below 18 or above 70 years old; (5) past history of organ transplantation; (6) human immunodeficiency virus (HIV) infection; (7) severe gastrointestinal bleeding; (8) pregnancy.
Data collection
Patients’ demographic, laboratory, and imaging data were extracted from electronic medical record system for all patients. All ACLF patients between January 1, 2011 and December 31, 2016 were retrieved. Survival at day 90 was retrieved from case records, follow-up documents, and confirmed by telephone calls. The severity of the liver disease was assessed by Child–Pugh (CTP), model for end stage liver disease (MELD), and chronic liver failure-sequential organ failure assessment (CLIF-SOFA) scoring systems.
Mono and sequential DPMAS treatment
ACLF patients who were admitted to our center form January 1, 2011 to December 31, 2016 were considered as candidates. All patients received standard medical therapy (SMT) in combination with mono or sequential DPMAS therapy. SMT treatment included antiviral treatment, albumin infusion and other blood constituents (i.e. red blood cells (RBC), platelets (PLT), and FFP), energy supplements, electrolyte maintenance, and acid base equilibrium. Antiviral treatment was given to patients with HBV infection.
Patients who received only DPMAS were defined as the monotherapy group. PE followed by DPMAS was defined as sequential treatment. PE was performed with 0.5 M membrane type plasma separator (B. Braun, Melsungen, Germany). Under electrocardiogram monitoring, the exchange cycle was established through the femoral vein. The total exchanged plasma volume was 2500 mL, and the PE rate was 20–25 mL/min, lasting 2–3 h every session. During PE, 5000 IU of low-molecular-weight heparin calcium was given to patients for anticoagulation. The illustration of DPMAS procedure was shown in Supplemental Figure 1 (modified from Reference, 8 elimination characteristics of both adsorbers (AR350 and BS330) can be regarded as essentially identical). The detailed protocol of DMPAS was as reported9. In our study, we used AR350 type anion exchange resin (Ai’er, Langfang, China) and HA330-II type neutral macroporous resin (Jianfan, Zhuhai, China). The procedure lasted for 3 h or perfusion adsorption capacity was saturated. The velocity of blood flow was 100–120 mL/min and plasma circuit were at a flow rate of 25–50 ml/min. Only one treatment modality (PE or DPMAS) was performed each day. DPMAS and PE were counted as separate treatment.
PE or DPMAS was repeated every 2–4 days. No consensus was available on which treatment to choose in ACLF patients. The decisions on what strategy to use in our study were determined by plasma availability and willing of the patients.
Statistical analyses
To address the imbalance of potential confounders between two groups, we matched treatment groups using propensity scores matching (PSM). The propensity-score model included: age, sex, MELD, CLIF-SOFA, HE, INR. These variables were selected because they were considered to be relevant predictors of short-term mortality. We formed matched pairs between patients who underwent mono DPMAS therapy and sequential DPMAS and PE therapy using a one-to-one nearest neighbor caliper of width 0.1 (maximum allowable difference in propensity scores). Only patients matched with propensity scores were included in analyses. Categorical variables were analyzed using the Chi-square test. Continuous variables were analyzed using the Wilcoxon rank-sum test and the Student t-test after propensity score matching. The overall survival curves were determined using the Kaplan–Meier method and compared using the log-rank test. A multivariate analysis was performed using a Cox proportional hazards model. Statistical analyses were performed using the SPSS 24.0 (SPSS Inc; Chicago, IL, USA). All the statistical analyses were two-tailed.The p-values less than 0.05 were considered to indicate statistical significance.
Result
Patient characteristics
The depiction of patients’ selection was shown in Figure 1. A total of 125 ACLF patients received artificial liver support treatment (ALSS) in our unit between January 1, 2011 and December 31, 2016, among which 42 patients received mono DPMAS and 83 patients received sequential DPMAS. Of the 125 cases of ACLF, most were caused by chronic hepatitis B (109 cases, 87.2%), followed by alcohol abuse (10 cases, 8.0%), and autoimmune factors (6 cases, 4.8%). Both groups were similar with respect to the frequency and type of the precipitating event; time interval between hospital admission and artificial liver support (Table 1). Infection and HE were common. The most common infections were spontaneous bacterial peritonitis (46.8%), Urinary tract infection (14.1%), and pneumonia and upper respiratory tract infection (39.1%; data not shown). No patients in our study met the diagnostic criteria of systemic inflammatory response syndrome (SIRS) criteria. SIRS was assessed according to the recommendations of the American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference. 14 After PSM, 40 patients were finally identified in each group (total number of patients, n = 80). As shown in Table 1, the baseline characteristics such as age, gender, serum albumin, PT, INR, TBIL, Cr, CTP scores, CLIF-SOFA, and MELD scores were similar between the two groups (p > 0.05), differences in INR and prothrombin time activity (PTA) were balanced after PSM.
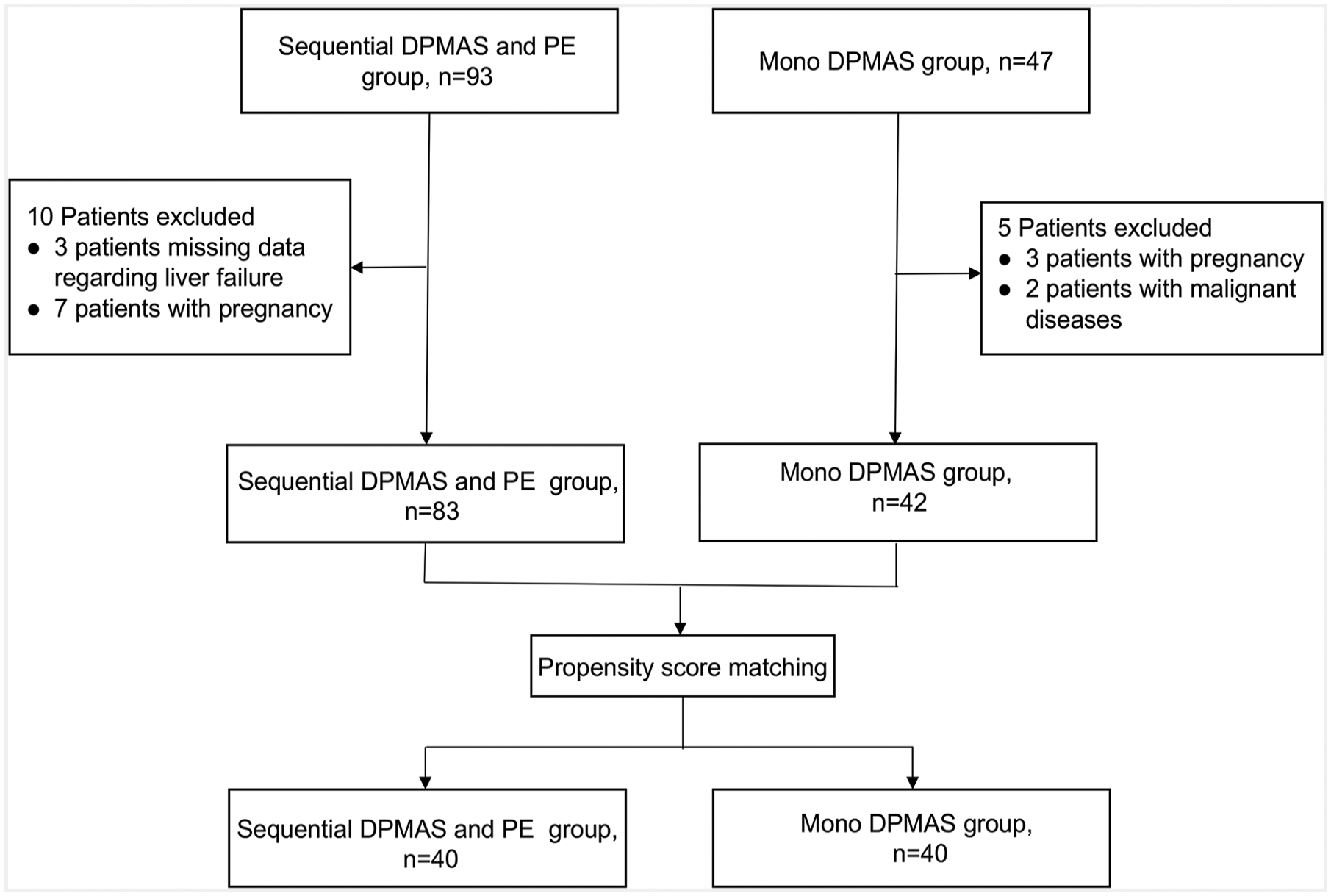
Study flow chart showing selection of ACLF patients.
Baseline characteristics of ACLF patients according to the assigned to treatment before and after propensity-score matching (PSM).
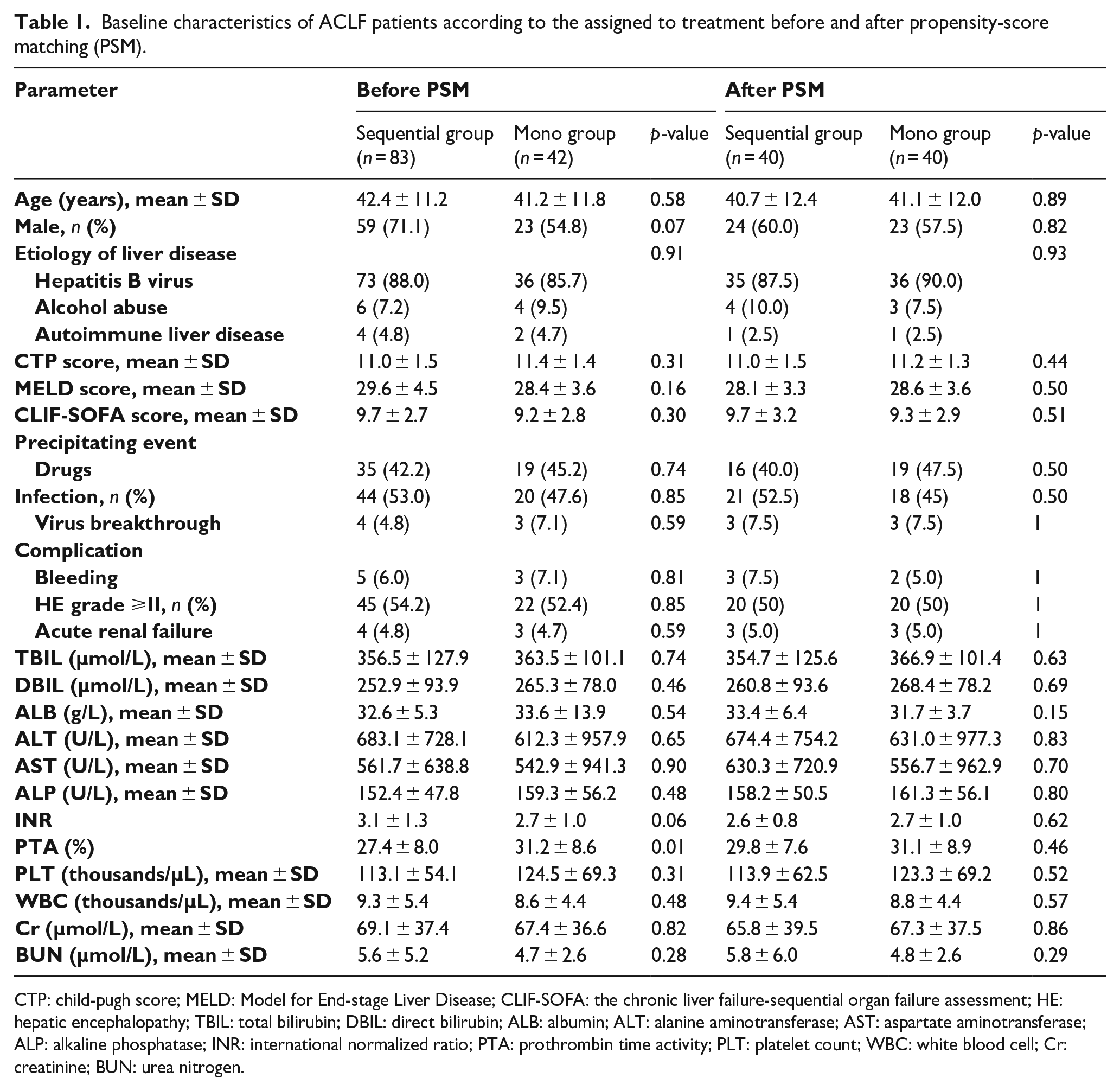
CTP: child-pugh score; MELD: Model for End-stage Liver Disease; CLIF-SOFA: the chronic liver failure-sequential organ failure assessment; HE: hepatic encephalopathy; TBIL: total bilirubin; DBIL: direct bilirubin; ALB: albumin; ALT: alanine aminotransferase; AST: aspartate aminotransferase; ALP: alkaline phosphatase; INR: international normalized ratio; PTA: prothrombin time activity; PLT: platelet count; WBC: white blood cell; Cr: creatinine; BUN: urea nitrogen.
Effects on laboratory parameters and HE
Overall, 123 mono DPMAS treatment sessions were performed in 40 patients with an average of 3.1(2–5) sessions per patient and 120 sequential DPMAS and PE treatment sessions were applied in another 40 patients with an average of 3 (2–6) sessions for each patient. The average effective treatment duration of sequential therapy for each patient was 16.6 ± 9.6 h, of which 7.3 ± 4.2 h for plasma exchange and 9.0 ± 5.3 h for DPMAS, and the average treatment duration of mono therapy was 8.9 ± 4.9 h per patients.
The effects of different treatment regime on biochemical parameters, coagulations, white blood cells, and platelets were shown in Table 2. Alanine aminotransferase
Laboratory parameters before and after a single treatment with sequential or mono DPMAS therapy (n = 80).
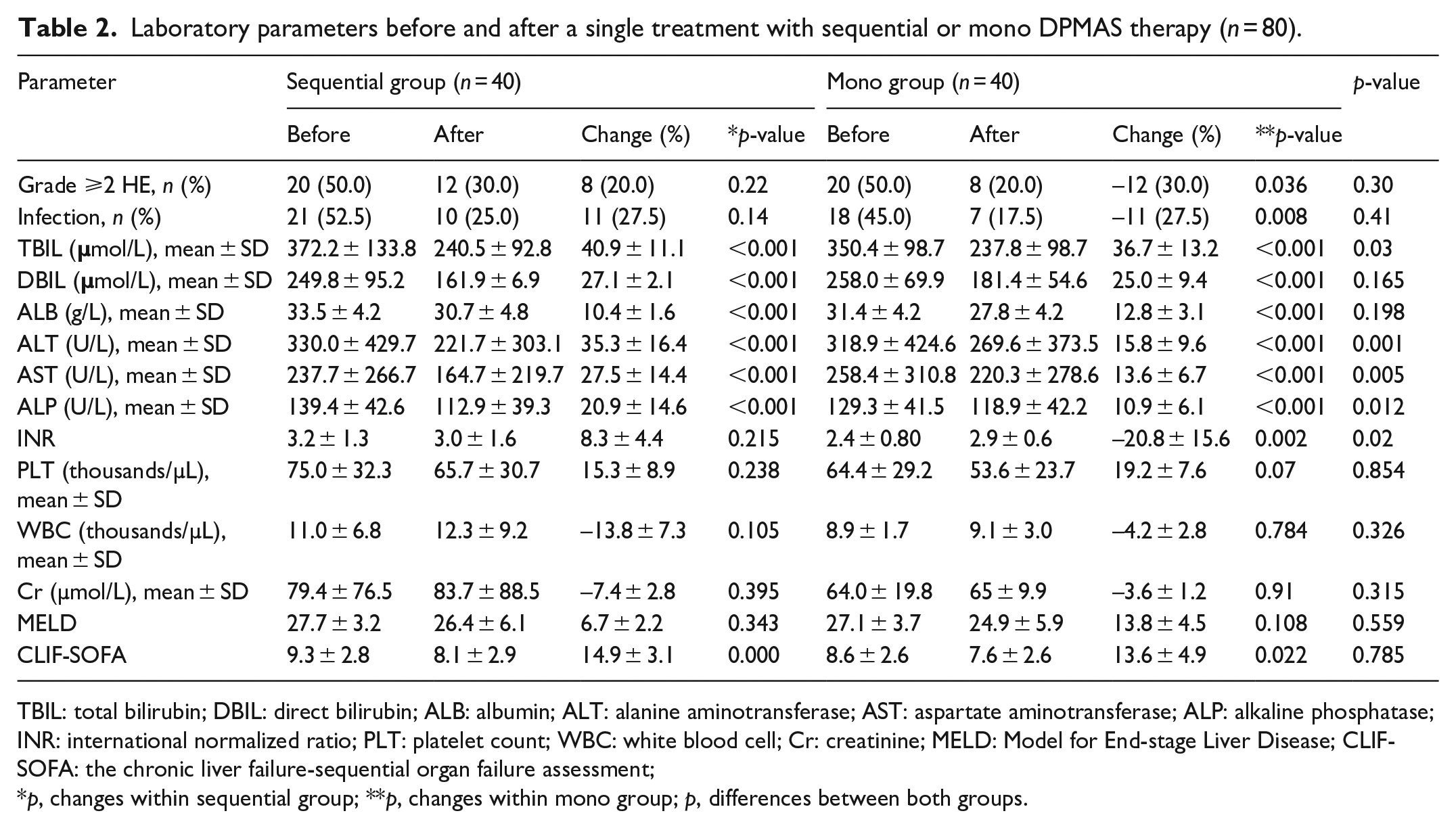
TBIL: total bilirubin; DBIL: direct bilirubin; ALB: albumin; ALT: alanine aminotransferase; AST: aspartate aminotransferase; ALP: alkaline phosphatase; INR: international normalized ratio; PLT: platelet count; WBC: white blood cell; Cr: creatinine; MELD: Model for End-stage Liver Disease; CLIF-SOFA: the chronic liver failure-sequential organ failure assessment;
p, changes within sequential group; **p, changes within mono group; p, differences between both groups.
Sequential assessment of sequential or mono DPMAS therapy on liver tests (mean ± SD).
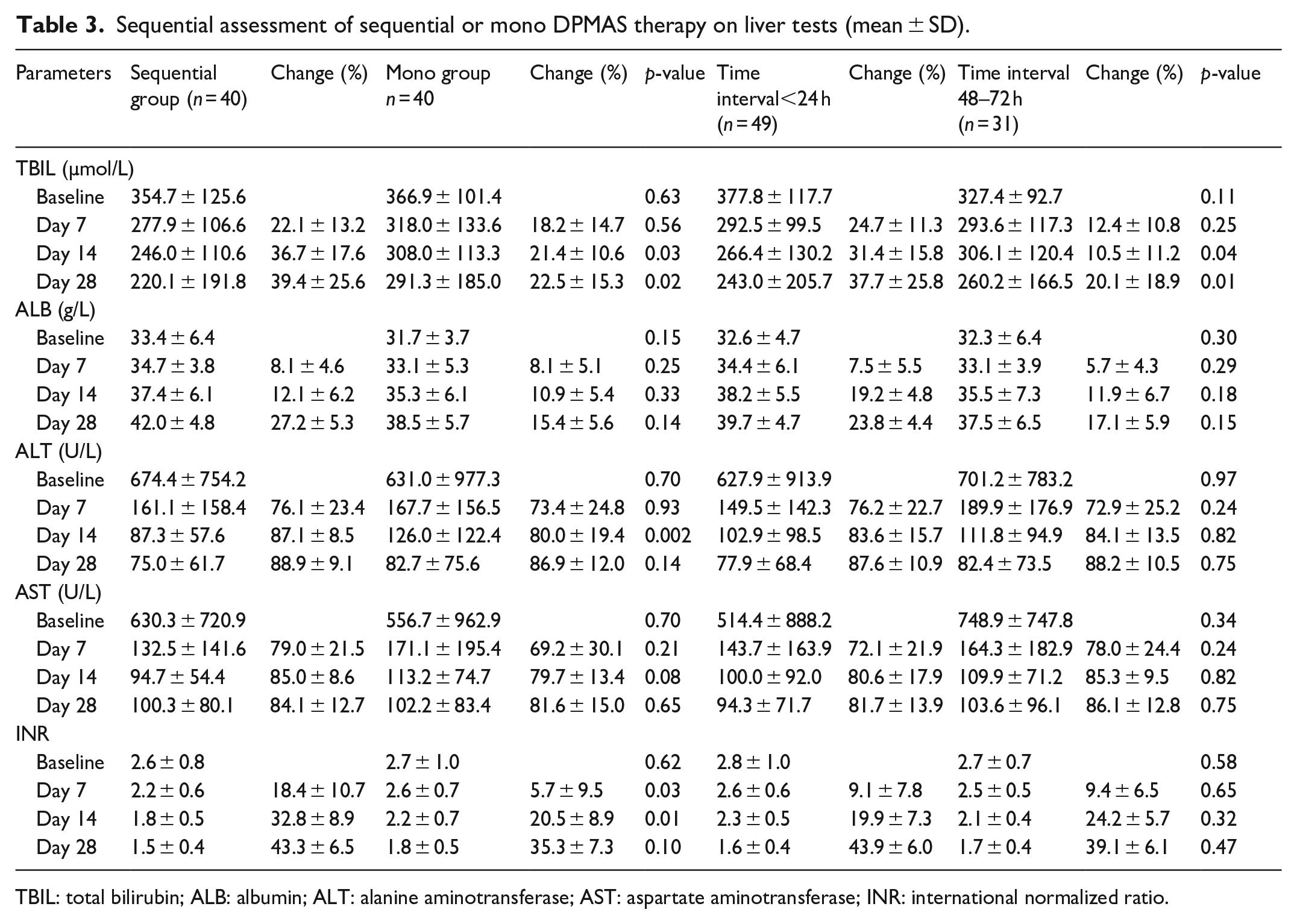
TBIL: total bilirubin; ALB: albumin; ALT: alanine aminotransferase; AST: aspartate aminotransferase; INR: international normalized ratio.
Impacts of mono or sequential DPMAS on patients’ survival
During hospitalization and 90-day follow-up, 11 (27.5%) patients died of hepatic encephalopathy, 6 (15%) patients died of organ failure, and 3 (7.5%) died of infection in sequential group, while 10 (25%) patients died of hepatic encephalopathy, 6 (15%) patients died of organ failure, 1 (2.5%) patient died of bleeding, and 4 (10%) patients died of infection in mono group. Kaplan–Meier survival showed no significant difference on survival between two groups, with 90 day accumulate survival rate of 50.0% for sequential group versus 47.5% for mono group (p = 0.66), and mean time to death of 56.2 days versus 52.9 days (Figure 2). The similar outcomes were found in subgroup analyses for ACLF patients with CLIF-SOFA score ⩾10 or TBIL ⩾ 350umol/L (Figure 3).
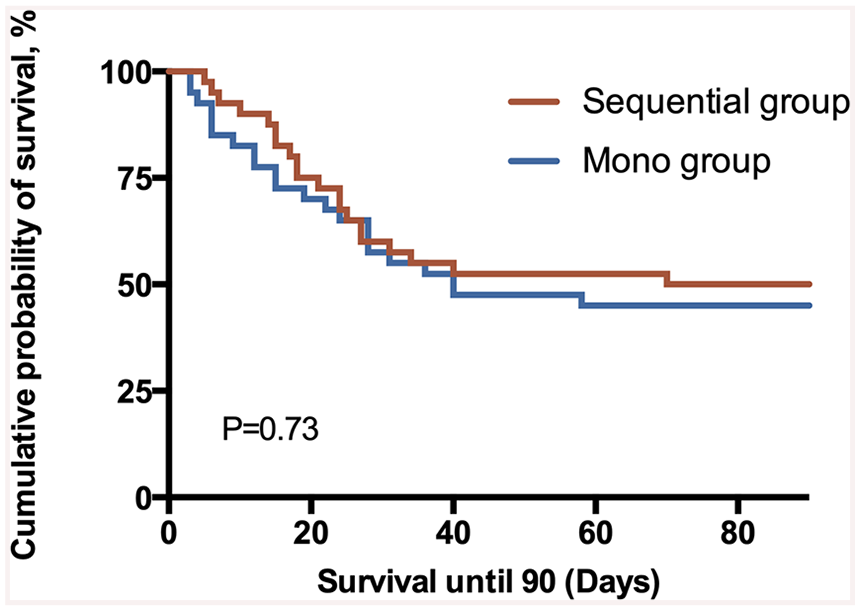
Kaplan–Meier survival curve in ACLF patients treated with sequential and mono DPMAS over follow up of 90 days. Brown line represents the sequential group. Blue line represents the mono group.
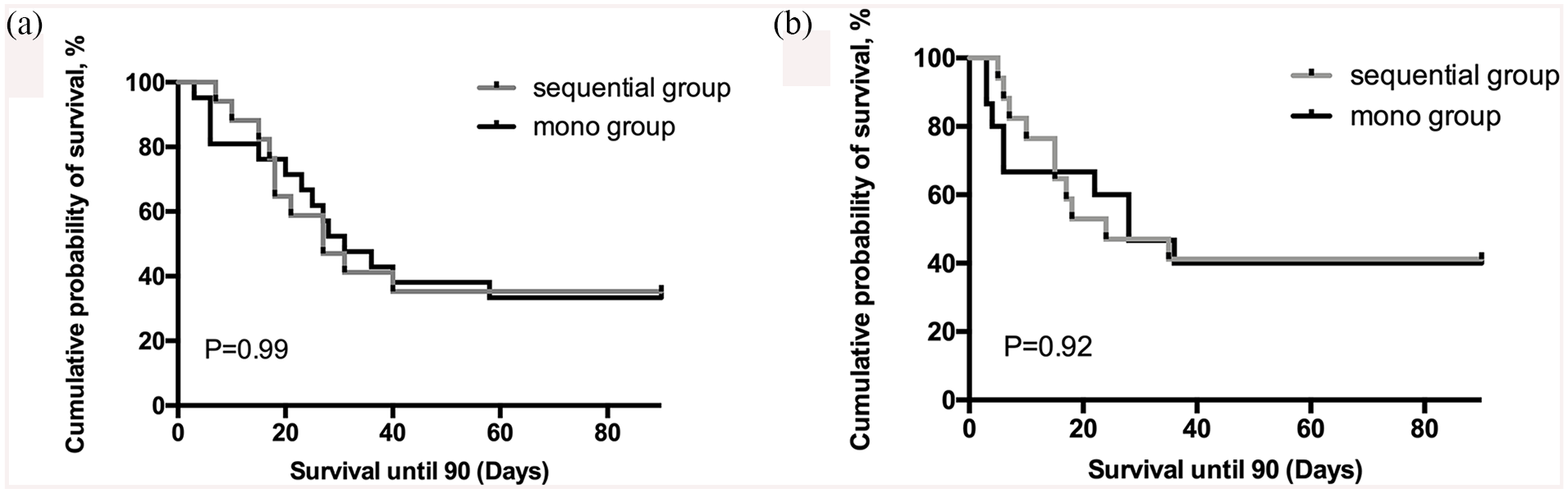
Kaplan–Meier survival curve in ACLF patients with TBIL greater than 350 (a) and CLIF-SOFA score greater than 10 (b). Gray line represents the sequential group. Black line represents the mono group.
Baseline and post-treatment predictors for survival at 90 days
Independent baseline risk factors in a multivariate Cox model were as follows: CTP score, HE, TBIL, and INR. No relationship was found between therapeutic modalities and treatment outcome. Moreover, the time elapsed between administration and the start of treatment also had no relationship with treatment outcome (Table 4).
Univariate and multivariate Cox model investigating independent baseline risk factors for the 90 days survival rate of ACLF patients.
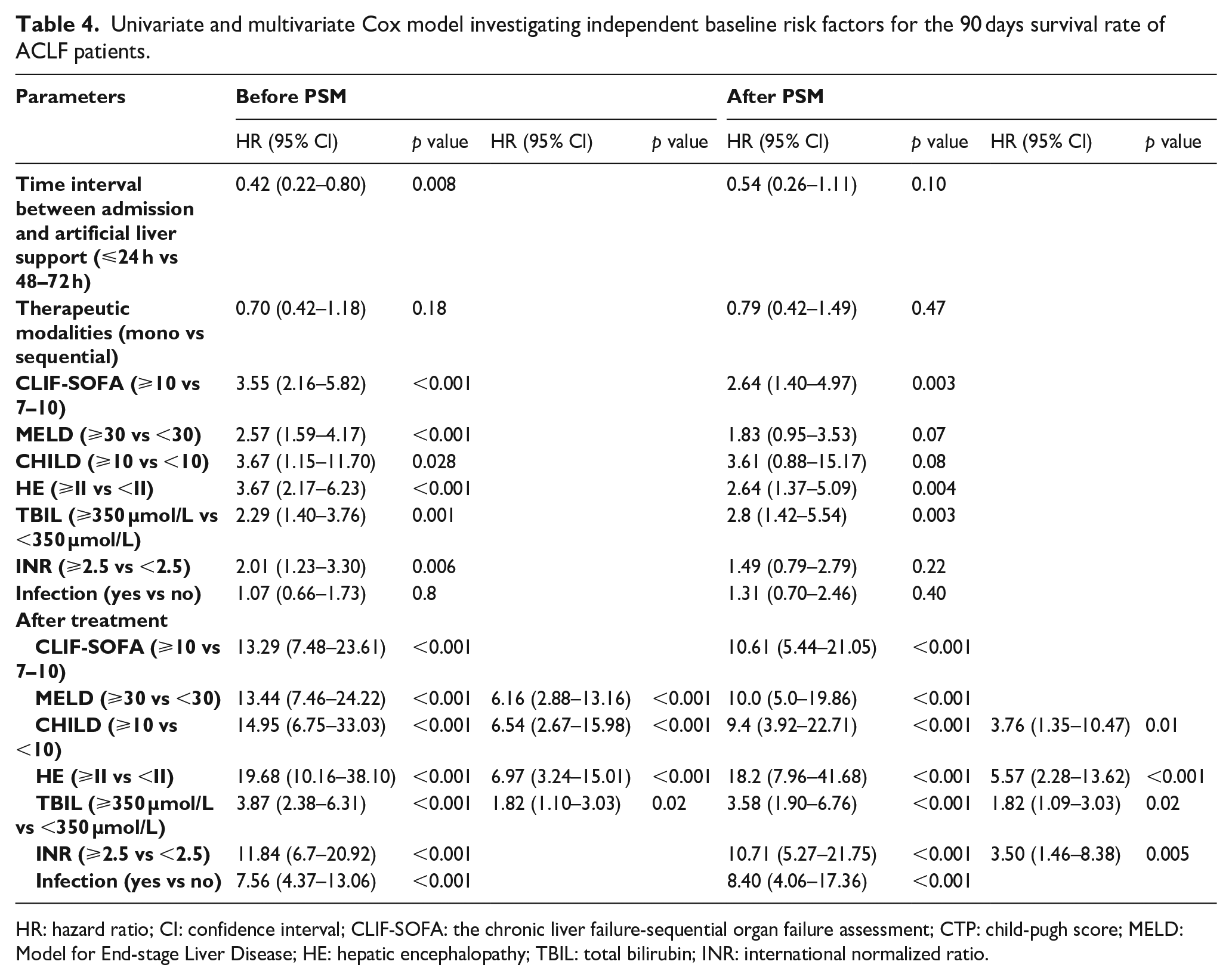
HR: hazard ratio; CI: confidence interval; CLIF-SOFA: the chronic liver failure-sequential organ failure assessment; CTP: child-pugh score; MELD: Model for End-stage Liver Disease; HE: hepatic encephalopathy; TBIL: total bilirubin; INR: international normalized ratio.
Discussion
In order to compare the detoxification capacity of sequential and mono treatment, we performed a retrospective analysis of prospectively collected data. We observed both mono DPMAS and sequential PE and DPMAS treatments could improve liver function in ACLF patients. However, there was no difference between two strategies in benefits on patients’ 90 day survival.
ACLF is a serious medical ailment and associated with high short-term mortality. It is characterized by acute liver decompensation and organ failure.15,16 Despite recent progress of medicine, ACLF remains a therapeutic challenge with extremely poor prognosis. Artificial liver support system (ALSS) is an important method for the treatment of liver failure, which provides a useful support by reducing toxins and promoting liver regeneration. 17
Previous studies reported that PE and DPMAS could resulted in significant reduction in ALT, AST, TBIL, DBIL, TBA, and albumin levels in ACLF patients.8,9,18,19 Li et al. 5 reported that PE combined with HP could decrease TBIL and ALT levels more significantly than HP or PE alone. Therefore, different combinations of non-bioartificial therapies were more effective in improving severe metabolic disorders and removing accumulated toxic substances and inflammatory mediators caused by serious damage of liver cells. In our study, propensity score matching was applied to avoid selection bias when comparing the two groups. The number of artificial liver support system (DPMAS and PE vs mono DPMAS) sessions and mean number of hours applied to each patient was comparable. As a result, sequential PE and DPMAS had a better effect on liver function without affecting coagulation, as compared with DPMAS alone. Equally important is the moment of applying the artificial liver support method and end-points assessment. We established a time-based protocol to analyze the changes of liver tests. At all-time points, mean blood clearances tended to be higher during treatment with sequential PE and DPMAS. Significance, however, was not reached, most probably as a result of the large interindividual variation.
Severe HE is a major cause of morbidity and mortality in ACLF and associated with poor prognosis. DPMAS was shown to be able to remove glutamine, an important factor in HE pathogenesis, while PE had no effect on glutamine. 18 We found that mono DPMAS improved HE in 60% of ACLF patients, while 40% patients showed improvement of HE in the sequential treatment group, though the difference was not statistically significant(p = 0.3). The possible explanation may be that sample size for HE patients was relatively small in both treatments.
Infection plays an important role in the pathogenesis and mortality in ACLF. Previous studies demonstrated that infection-related ACLF (I-ACLF), second infections, admission values of high MELD, and low albumin were independent predictors of poor 30-day survival in ACLF. 19 In our study, the incidence of infection was quite high, but infection was not identified as an independent predictor of mortality by multivariate analysis. Explanation might be that the sample size was not big enough and the infection here was not as severe as in I-ACLF, which was defined by the presence of two or more organ failures.
ALSS offers the potential to improve the prognosis of patients with ACLF. However, the literature has been inconsistent on its survival benefit. A meta-analysis reported that ALSS could improve 1- and 3-month survivals in patients with ACLF. 20 Some research reported that TPE significantly reduced the 1- and 3-month mortality of ACLF patients.21,22 A prospective study demonstrated that DPMAS had similar effects on 1- and 3-month survival rates to that of TPE in treatment of HBV-ACLF patients. 9 Fractionated Plasma Separation and Adsorption (Prometheus) also did not show significant improvement for ACLF survival in a prospective trial (HELIOS), as comparing with SMT alone. 23 Just recently the biologic extracorporeal cellular therapy (ELAD)was demonstrated an improvement in transplant-free survival (TFS) for ACLF patients, especially significant on day 28. 24 In our study, no difference on survival was seen between sequential and mono therapy, suggesting that these two strategies may be comparable in treating ACLF patients.
Our study has several limitations. As mentioned above, no control groups treated either with SMT or PE alone were included in our study. Our facility is a tertiary hospital in the northwest of China, patients referred to our hospital are generally very severe and failed SMT. In addition, only very few patients received only PE because of lack of sufficient plasma in our database. Multi-center study could be helpful to clarify this issue. Besides, our study had a moderate sample size, which made detailed subgroup analysis unlikely.
Conclusion
In ACLF patients, sequential PE followed by DPMAS had a better improvement in liver function but did not present an advantage on survival comparing with DPMAS monotherapy.
Summary
ACLF is a severe clinical syndrome with high mortality. ALSS can temporarily eliminate toxic substances and prevent the development or exacerbation of secondary organ failure, thus improve the outcome of ACLF patients. Sequential DPMAS and PE seemed to have a better effect on liver function improvement but provided no survival benefit compared with mono DPMAS.
Supplemental Material
sj-tif-1-jao-10.1177_0391398820987565 – Supplemental material for Sequential versus mono double plasma molecular adsorption system in acute-on-chronic liver failures: A propensity-score matched study
Supplemental material, sj-tif-1-jao-10.1177_0391398820987565 for Sequential versus mono double plasma molecular adsorption system in acute-on-chronic liver failures: A propensity-score matched study by Jing Zhang, Hui Luo, Ying Han and Xinmin Zhou in The International Journal of Artificial Organs
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.