
Abstract
Introduction:
There were controversial opinions on the use of regional citrate anticoagulation (RCA) versus low molecular weight heparin (LMWH) for continuous renal replacement therapy (CRRT) in hyperlactatemia patients, which was considered as one of the contraindications of citrate. The aim of our present study is to evaluate the efficacy and safety of RCA versus LMWH for CRRT in hyperlactatemia patients.
Methods:
Adult patients with hyperlactatemia who underwent RCA or LMWH CRRT in our center between January 2014 and March 2018 were retrospectively recruited. Filter lifespan, ultrafiltration, purification, bleeding, citrate accumulation, filter clot, and the infusion of blood production were evaluated as endpoints.
Results:
Of the 127 patients included in the original cohort, 81 and 46 accepted RCA and LMWH CRRT, respectively. The filter lifespan was significantly prolonged in the RCA group compared to the LMWH group (44.25 h [2 -83] vs. 24 h [4 -67], p < 0.001). The accumulated filter survival proportions were significantly improved in the RCA group compared to the LMWH group in the original cohort (p < 0.001) as well as the matched group (p < 0.001). The filters clotted more frequently in the LMWH group than in the RCA group in both of the original (52.2% vs 26.8%, p = 0.001) and matched cohort (58.6% vs 19.4%, p = 0.001). The bleeding complication was significantly reduced in the RCA group than in the LMWH group in the matched cohort (28.6% vs 4.5%, p = 0.04).
Conclusion:
In critically ill patients with hyperlactatemia requiring CRRT, RCA is superior to LMWH in terms of filter lifespan and bleeding risk without significantly increased risk of citrate accumulation and citrate related metabolic complications. RCA most likely is a safe and effective anticoagulation method for CRRT in patients with hyperlactatemia.
Keywords
Introduction
It was reported that approximately 8–13% of critically ill patients required renal replacement therapy (RRT).1,2 Continuous renal replacement therapy (CRRT) is the most common modality of RRT applied in the critical care setting.3,4 Some forms of anticoagulation are usually necessary to maintain the patency of the extracorporeal circuit in patients without increased bleeding risk during CRRT. 5 Currently, regional citrate anticoagulation (RCA) is a promising anticoagulation method6,7 and is recommended as the first-line anticoagulation strategy by the KDIGO guideline. 8 Nevertheless, shock with skeletal muscle hypoperfusion was listed in this guideline as a contraindication to RCA. 8 An important marker of hypoperfusion shock is hyperlactatemia, 9 which presented in about 40% of critically ill patients requiring CRRT.10,11 Patients with hyperlactatemia following shock might be at high risk for citrate accumulation (CA), 12 and should be anticoagulated by either unfractionated heparin (UFH) or low-molecular-weight heparin (LMWH) during CRRT according to the latest clinical practice guideline. 8 However, several previous studies10,13 had documented that the incidence of CA during RCA-CRRT was relatively low even in the presence of shock with tissue hypoperfusion, which indicated that RCA could be well tolerated in a majority of hyperlactatemia patients. The advantages and disadvantages of RCA versus UFH had been studied extensively in patients without contraindications to citrate.14–20 However, data on the comparison between RCA and LMWH for CRRT in hyperlactatemia patients are scarce. The aim of this study is to compare RCA versus LMWH regarding efficacy and safety in patients without bleeding risk who underwent CRRT.
Materials and methods
Study design and setting
We performed a single-center retrospective observational study in a university-affiliated tertiary teaching hospital. This study was in accordance with the principles of the Helsinki Declaration and approved by the ethics committee of Xijing Hospital of the Fourth military medical university. The informed consent was waived due to the non-interventional nature of the study and anonymised data.
Patients selection
Critically ill patients admitted to surgical or medical ICUs in Xijing Hospital who underwent CRRT and received either RCA or LMWH anticoagulation between Jan, 2014 and Mar, 2018 were retrospectively reviewed. Patients who met the following criteria were included: (1) ⩾18 years; and (2) serum lactate level >2 mmol/L. Patients with any of the following characters were excluded: (1) incomplete data; (2) with increased bleeding risk; (3) received therapeutic anticoagulation prior to CRRT; (4) liver dysfunction; (5) pregnant or breastfeeding; (6) type B hyperlactatemia; or (7) intermittent hemodialysis. The eligible patients were subdivided into the RCA group and LMWH group by the anticoagulants they had received. In order to minimize the risk of selection bias, we then matched the LMWH group with the RCA group in terms of SOFA score, serum lactate, INR, and recent surgery or trauma on a 1:1 ratio.
CRRT protocol
All patients were treated with CRRT using the Prismaflex System (Gambro) or DIAPACT (Braun) machine, equipped with Multiflow-100 (0.9 m2, AN69 membrane) and AV600 (polysulfone, 1.4 m2; Fresenius) hollow-fiber filters, respectively. The vascular access was established by inserting a 13.5F double lumen catheter into the jugular or femoral vein. Blood flow was maintained at 180–200 ml/min. The anticoagulation protocol were RCA in patients with increased bleeding risk and LMWH in patients without bleeding risk. A 4% citrate sodium solution was infused at a rate of 200 ml/h and was titrated to achieve a target postfilter ionized calcium range of 0.25–0.35 mmol/L. A 10% calcium gluconate solution was infused separately at the end of the venous line of the extracorporeal circuit maintaining the circulation ionized calcium within a physiological range of 1.1–1.2 mmol/L. The arterial and post-filter ionized calcium were obtained 2 h after the initiation of CVVH and every 4 h thereafter. Arterial blood gas and other serum electrolytes were analyzed every 4 h during the treatment. In cases of suspected citrate accumulation, citrate infusion and blood flow were reduced to avoid metabolic complications. For heparin regimen, an initial bolus of 60–80 U/kg of LMWH was injected subcutaneously with a maintenance doses of 500–1500 U/4 h. In the absence of clotting, the filter was replaced routinely at 72 h following the manufacturer’s recommendations.
Data collection
All the clinical data were extracted from the electronic medical records. The following data were collected: patient baseline characteristics, filter lifespan, bleeding episodes, blood products infusion requirements, and citrate-related complications (i.e. CA, metabolic acidosis/alkalosis, and hypocalcemia). The illness severity was assessed using the following severity scores: Acute Physiology and Chronic Health Evaluation (APACHE) II, Sequential Organ Failure Assessment (SOFA), and Glasgow coma (GCS). Filter lifespan was defined as the time between the initiation and discontinuance of the first filter. The causes of CRRT cessation included filter clotting and non-clotting events (e.g. transportation, resuscitation operations, imaging examination procedures, surgery, or death).
Definitions
The cut-off value of serum lactate for hyperlactatemia was set at 2 mmol/L. 21 Liver dysfunction were defined as serum bilirubin >34.2 μmol/L.22,23 CA was identified based on the following criteria: (1) decreased systemic ionized calcium (<1.1 mmol/L) despite adequate calcium replacement; (2) concomitant tot Ca/ionCa ratio >2.5; and (3) relevant metabolic acidosis (pH < 7.2 and/or BE < −5 mmol/L) without or (4) with an increased anion gap (>11 mmol/L). 24 Filter clotting was defined as (1) transmembrane pressure (TMP) exceeded 300 mm Hg, (2) visible clot obstructing flow through the circuit, or (3) the blood pump was unable to rotate due to clot obstruction in the membrane. 25 The net ultrafiltration (NUF) was defined as the difference between hourly fluid removal from the CRRT machine and hourly replacement fluid. 26 The purification was assessed by calculating the CRRT dose (ml/kg/h) (i.e. effluent volume).
Outcomes
The primary outcomes were safety and efficacy. Endpoints for safety evaluation included bleeding, transfusion requirements, and occurrence of citrate related complications. Efficacy endpoint was filter lifespan, ultrafiltration, and purification.
Statistical analysis
The distribution of continuous variables was evaluated using the Kolmogorov–Smirnov test. Data were presented as mean ± standard deviation (SD) (normal distribution) or median (interquartile range [IQR]) (non-normal distribution) for continuous variables, and were compared using Student’s t test and the Wilcoxon test, respectively. For categorical variables, data were presented as counts (percentage), and were compared using Chi-square test or Fisher’s exact test where appropriate. The filter survival rates at different time points (12–72 h) were graphically analyzed using Kaplan–Meier survival curves with Log-rank test. Risk factors for filter lifespan were analyzed by using a Cox proportional hazard model. 27 A p value less than 0.05 was considered statistically significant. All statistical analyses were performed by using SPSS 22.0 for Windows (SPSS Inc., Chicago, IL, USA).
Results
Patients inclusion
During the study period, 316 patients with hyperlactatemia underwent CRRT in our hospital were screened. Finally, 127 patients were eligible for this study, with 81 and 46 received RCA and LMWH, respectively. The patient inclusion flow chart was illustrated in Figure 1.
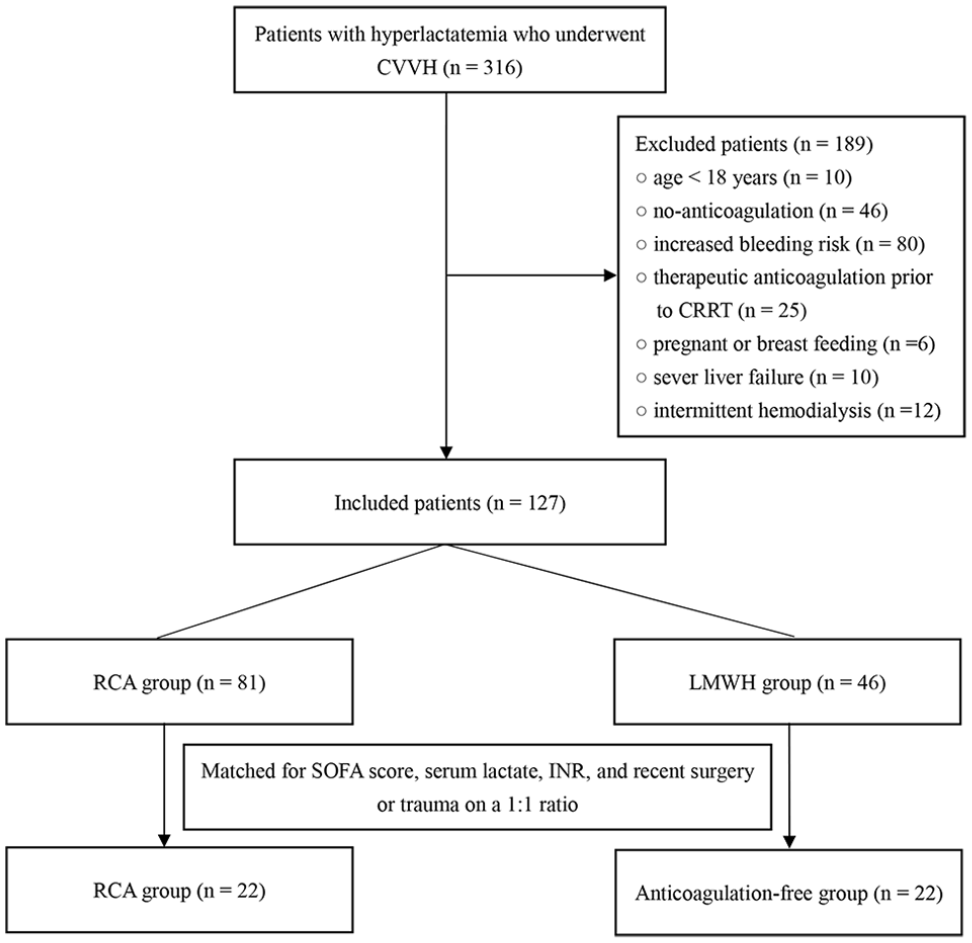
The patient inclusion flow chart.
Patient baseline characteristics
The baseline characteristics of the included patients were listed in Table 1. There were no significant between-group differences in terms of age, gender, mean arterial pressure (MAP), illness severity, comorbidities, indication of CRRT, serum lactate, hemoglobin (HGB), and biochemistry parameters at baseline. The proportion of patients who received mechanical ventilation (MV) (76.1% vs 45.7%, p < 0.001) and vasopressors (63% vs 43.2%, p = 0.04) were significantly greater in the LMWH group than that in the RCA group. Regarding to coagulation profile, the activated partial thromboplastin time (APTT) (29.59 ± 6.81 vs 39.52 ± 11.96, p = 0.002) and PLT count (171.62 ± 99.08 vs124 ± 60.76, p = 0.03) were significantly higher in RCA group. In the matched cohort, all baseline characteristics were comparable between the two groups (Additional file 1: Supplemental Table S1).
Baseline characteristics of the included patients in the original cohort.

AKI: acute kidney injury; APTT: activated partial thromboplastin time; CRRT: continuous renal replacement therapy; MV: mechanical ventilation; INR: internationalized normal ratio; MAP: mean artery pressure; PLT: platelet; SOFA: sequential organ failure assessment.
Data are expressed as n (%), mean ± SD or counts (percentage) where appropriate.
Other indications for CRRT included heat shock and rhabdomyolysis.
Efficacy
Filter lifespan
The filter lifespan was significantly prolonged in the RCA group compared to the LMWH group (44.25 h [2–83] vs 24 h [4–67], p < 0.001, Table 2). After matching, the advantage of RCA on filter lifespan was still significant (48 h [4–79] vs 24 h [7–67], p < 0.001, Additional file 2: Supplemental Table S2). The filter survival rates from 0 to 72 h in the original and matched groups were graphically demonstrated by Kaplan-Meier curve in Figure 2(a) and (b), respectively. The curves suggested the filter survival chances were significantly improved in the RCA group compared to the LMWH group before (p < 0.001) and after (p < 0.001) matching.
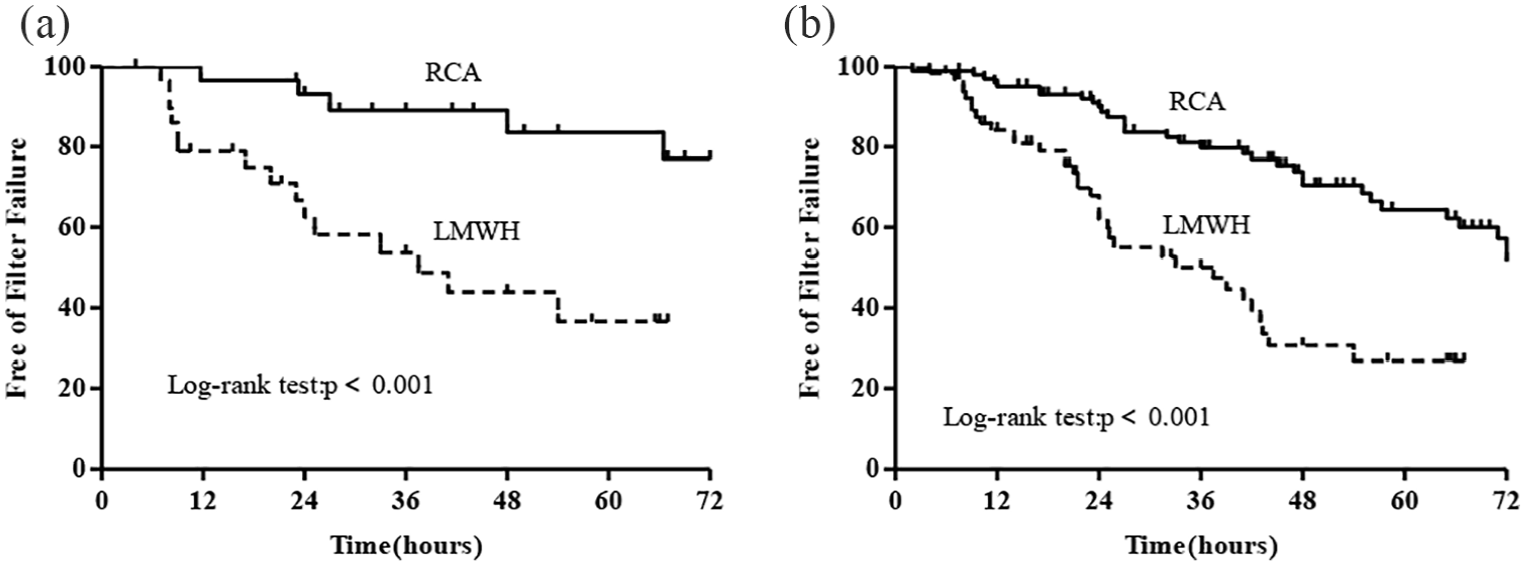
Survival curves of the filters in the RCA group versus the filters in the LMWH group: (a) the original cohort and (b) the matched cohort.
Outcomes of the included patients in the original cohort.

CRRT: continuous renal replacement therapy; CA: citrate accumulation; FFP: fresh frozen plasma; PLT: platelet; HIT: Heparin induces thrombocytopenia; RBC: red blood cell; RCA: regional citrate anticoagulation; TotCa/ionCa ratio: total to ionized calcium ratio.
Date are expressed as n (%), mean ± SD or counts (percentage) where appropriate.
Filter clotting rate
The filters clotted more frequently in the LMWH group than in the RCA group in both original (52.2% vs 26.8%, p = 0.001, Table 2) and matched cohort (58.6% vs 19.4%, p = 0.001, Additional file 2: Supplemental Table S2).
Ultrafiltration
There were no significant differences in NUF between the LWMH and the RCA group in both of the original (209 ± 116.1 ml/h vs 196.2 ± 95.8 ml/h, p = 0.5) and the matched cohort (201.4 ± 121.4 ml/h vs 182 ± 83.2 ml/h, p = 0.54). (Table 2)
Purification
The purification of the two groups are comparable as well in the original (33.41 ± 8.57 ml/kg/h vs 35.38 ± 12.13 ml/kg/h, p = 0.34) and the matched cohort (35.02 ± 7.39 ml/kg/h vs 40.36 ±14.25 ml/kg/h, p = 0.14) (Additional file 2: Supplemental Table S2).
Safety
Bleeding and blood products infusion requirement
There were no significant differences regarding new bleeding episodes and blood products infusion requirements between the LMWH and RCA group in the original cohorts (Table 2). In the matched cohort, bleeding episodes were significantly reduced in the RCA group (28.6% vs 4.5%, p = 0.04), although the blood products infusion rate remained comparable (Additional file 2: Supplemental Table S2).
Changes in hemoglobin, serum calcium, and coagulation parameters
At the end of the first CRRT session, the changes in HGB, PLT, totCa/ionCa ratio, INR, and APTT from baseline were comparable between the two groups. In the LMWH group, the patients’ Hb decreased significantly from baseline (Δvalue [−18.08 ± 19.99], ΔP1 = 0.01), whereas the APTT (Δvalue [19.14 ± 39.25], ΔP1 = 0.007), and INR (Δvalue [0.52 ± 1.16], ΔP1 = 0.006) were significantly prolonged (Table 3).
The changes of hemoglobin and coagulation parameters at the end of CRRT treatment in the original cohort.
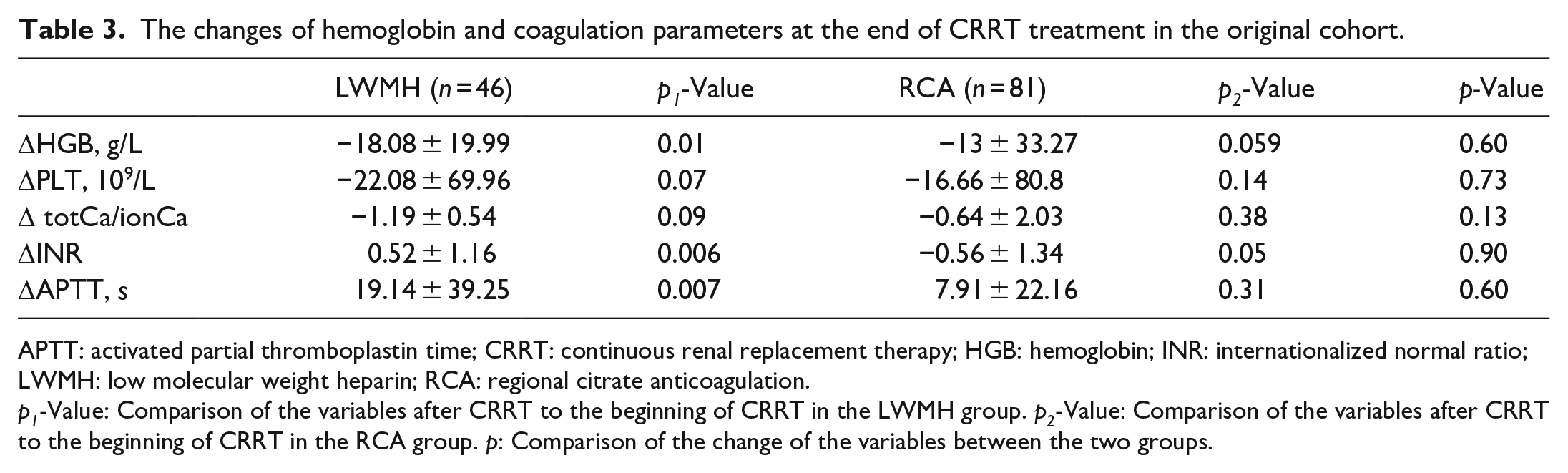
APTT: activated partial thromboplastin time; CRRT: continuous renal replacement therapy; HGB: hemoglobin; INR: internationalized normal ratio; LWMH: low molecular weight heparin; RCA: regional citrate anticoagulation.
p1-Value: Comparison of the variables after CRRT to the beginning of CRRT in the LWMH group. p2-Value: Comparison of the variables after CRRT to the beginning of CRRT in the RCA group. p: Comparison of the change of the variables between the two groups.
In the matched cohort, patients in the LMWH group had a greater reduction in platelet counts compared to RCA group (−34.65 ± 60.46 vs −30.65 ± 63.42, p = 0.03). The changes in the other parameters were similar between the two groups and within each of the groups (Additional file 3: Supplemental Table S3).
Heparin induced thrombocytopenia (HIT)
HIT occurred in one patient (2.2%) in the LMWH group and no patients developed HIT in the RCA group (Table 2).
Citrate related complications
CA occurred in two patients (2.5%) who received RCA-CRRT during the study period. The mean totCa/ionCa ratio was significantly lower in the LMWH group compared to RCA group (1.76 ± 0.45 vs 2.08 ± 0.79, p = 0.02). There were no significant differences in the incidence of metabolic acidosis (2.2% vs 4.9%, p = 0.65) and alkalosis (2.5% vs 4.3%, p = 0.62) between the two groups (Table 2).
In the matched cohort, no CA episodes were observed. The mean totCa/ionCa ratio was similar between the RCA and the LMWH group. The incidence of metabolic acidosis in the LMWH and RCA group were 0 and 9.1% (2/22), respectively, and the corresponding rates of metabolic alkalosis were 4.5% (1/22) and 0, respectively (Additional file 2: Supplemental Table S2).
Predictors of filter failure
In univariate analysis, the use of LMWH (HR 3.48, 95%CI [1.79–6.83], p < 0.001) for anticoagulation and SOFA score (HR 1.08, 95%CI [1.009–1.17], p = 0.03) were negatively associated with filter lifespan. In the multivariate Cox regression model, anticoagulation with LMWH remained as an independent predictor of filter failure (HR 4.07, 95%CI [1.75–9.46], p = 0.001) even after adjusted for SOFA score, INR, and serum lactate level (Table 4).
Risk factors of filter failure in patients with hyperlactatemia who underwent CVVH.

APTT: activated partial thromboplastin time; CVVH: continuous venovenous hemofiltration; CI: confidential interval; PLT: platelet; INR: international normalized ratio; HBG: hemoglobin; HR: hazard ratio; RCA: Regional citrate anticoagulation; SOFA: sequential organ failure assessment.
Discussion
In this retrospective cohort study, we found that: (1) compared to LMWH, RCA protocol could significantly prolong filter lifespan without incremental bleeding complication; (2) the incidence of CA in patients who received RCA was relatively low and the rate of citrate-related metabolic complications were not significantly increased; (3) the impact of RCA and LMWH on serum calcium and coagulation parameters was comparable during the study period; (4) In the univariate and multivariable regression analysis, RAC was significantly related to prolonged filter lifespan.
Relations to the previous studies
Filter lifespan and bleeding
The superiority of RCA versus UFH on filter lifespan and bleeding risk for CRRT had been proven by many randomized controlled trials (RCTs) in patients without contraindications to citrate. 28 However, data on the comparison between RCA and LMWH are sparse with conflicting results.18–20 Van der Voort et al. 18 in a prospective observational cohort study reported that the nadroparin based CVVH had a longer filter lifespan than citrate based (median 31.5 h vs 22.5 h, p = 0.0001), and bleeding incidence was significantly reduced in the citrate group (25% vs 14.8%, p = 0.04), although the RBC transfusion requirement was not different between groups. In a non-blinded single-center randomized controlled trial, 19 Oudemans-van Straaten and his colleagues did not find difference in the filter lifespan between nadroparin and citrate groups during CVVH (26 h [IQR 15–43] vs 27 h [IQR 13–47], p = 0.68). They also found favorable result regarding bleeding in the citrate group without difference in transfusion requirement as compared to nadroparin group, which was in accordance with the results of the 2006 study. 18 The similar blood products infusion rate and changes in hemoglobin between citrate and the LMWH groups was also observed in our study. A recent study by Uljas et al. 20 documented that the RCA protocol resulted in significant longer CRRT circuit lifespan compared to the dalteparin protocol. The inter-study heterogeneous results regarding filter lifespan were most likely attributed to the variable dose of anticoagulants and CRRT protocols. The employed maintenance LMWH dose was 475IU/h 18 and 380–456IU/h 19 in the previous studies, which were much higher than 500–1500U/4 h in our study. The relatively lower LMWH dose in our study could have contributed to the shorter filter lifespan in the LMWH group. However, the filter lifespan in both of the RCA and the LMWH groups in our study were much longer than those achieved by the previous two studies,18,19 which exclusively employed post-dilution mode. The prolonged filter lifespan in our study could be explained by the mixed pre-and post-dilution mode. 29
Citrate accumulation and metabolic complications
Mariano et al. 13 in a retrospective observational study reported that no CA and metabolic complications occurred in severe burn septic shock patients (baseline serum lactate 1.9 [IQR 1.4–2.7] mmol/L) who underwent RCA-CVVHDF. However, the citrate load in this study was relatively low (20.8 mmol/h) and 60% of which were lost in the effluent fluid. In a 2017 retrospective observational study, 10 patients were stratified by the serum lactate level at initiation of RCA-CRRT, the incidence of CA in the moderate (2.2–4 mmol/L) and severe (⩾4 mmol/L) hyperlactatemia group were 2.69% and 6.33%, respectively. A recently published single-center retrospective observational study 12 reported that the incidence of citrate intolerance were 38%, 44%, and 55%, in patients with peak serum lactate >4, >6, and >7 mmol/L, respectively, versus 7% in those with peak lactate <4 mmol/L, during RCA-CVVH. The incidence of CA in the present study was considerably lower as compared to the previous results, given a mean serum lactate of 6.87 mmol/L at baseline in the citrate group. The low incidence of CA in our study was most likely attributed to the low citrate load (27.2 mmol/h) with sufficient patency of the extracorporeal circuit. 30 Furthermore, we adopted a more rigorous diagnosis criteria of CA than the study by Tan et al. 12 Morgera et al. 31 reported than more than 50% of patients developed metabolic alkalosis during RCA-CRRT. The rate of metabolic alkalosis in our study was significantly lower because the bicarbonate fluid (B fluid) was infused separately and was adjustable in our protocol.
HIT
HIT is a serious complication of heparin, 32 which occurred in 1%–5% of patients with UFH and in less than 1% with LMWH. 33 The relatively higher incidence of HIT (2.2%) in our study may be likely attributed to the small sample size.
Limitations
There exist some limitations in our study. First, there may exist confounding factors and selection bias in our study due to the retrospective and single center nature, which led to significant heterogeneity. However, we matched patients for important clinically relevant factors to increase the comparability between the two groups. Second, we did not subdivide the patients by different cut-off values of serum lactate. Patients with variable serum lactate levels may have different risk for CA. Third, serum citrate concentration, anti-Xa activity, coagulation parameters, and liver and kidney function were not monitored regularly in some patients during CRRT. Further well designed multi-center randomized controlled trials are warranted in this field.
Conclusion
In critically ill patients with hyperlactatemia requiring CRRT, RCA may be superior to LMWH in terms of filter lifespan and bleeding risk without significantly increased risk of CA and citrate related metabolic complications. RCA seems to be a safe and effective anticoagulation method for CRRT in patients with hyperlactatemia. Further multicenter randomized controlled trials are warranted.
Supplemental Material
sj-zip-1-jao-10.1177_03913988211003586 – Supplemental material for Regional citrate anticoagulation versus low molecular weight heparin for CRRT in hyperlactatemia patients: A retrospective case-control study
Supplemental material, sj-zip-1-jao-10.1177_03913988211003586 for Regional citrate anticoagulation versus low molecular weight heparin for CRRT in hyperlactatemia patients: A retrospective case-control study by Lu Li, Ming Bai, Wei Zhang, Lijuan Zhao, Yan Yu and Shiren Sun in The International Journal of Artificial Organs
Footnotes
Author contributions
LL, MB, and WZ contributed equally to this work. LL, MB, and SRS conceived the study, participated in the design, performed statistical analyses and drafted the manuscript. YY, and LJZ helped to collect the data. WZ collected the data and helped to draft the manuscript. MB revised the manuscript critically for important intellectual content. SRS collected the data, performed statistical analyses and helped to revise the manuscript critically for important intellectual content. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (82070699) and Discipline Promotion Project of Xijing Hospital (XJZT18ML16).
Statement of ethics
The study was approved by the ethics committee of the Xijing hospital, the Fourth Military Medical University, and performed in accordance with the Declaration of Helsinki. The informed consent was waived because of the retrospective study design.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.