
Abstract
Septic shock is a clinical condition with high mortality (40%–70%) and morbidity. During septic shock, there is a significant release of cytokines and other inflammatory mediators that can cause damage to different organs, known as a “cytokine storm.” The cytokine storm can cause hypotension, tissue damage, metabolic acidosis, and renal failure. This clinical picture also seems to be confirmed in the context of Covid-19 patients. Hemoadsorption with CytoSorb represents an adjunctive therapy to attenuate the systemic inflammatory process and helps restore a balanced immune response. We present the clinical case of a 75-year-old man, admitted to our hospital with respiratory failure due to Sars-CoV-2 infection and secondary septic shock due to a sacral decubitus. On admission the patient presented with a clinical picture of mixed acidosis with high levels of lactate and inflammatory indexes. Simultaneously along with antibiotic therapy, we started hemoadsorption treatment with CytoSorb in combination with continuous venous-venous hemodiafiltration. At the end of the treatment the patient had recovered his vital functions and the infection was successfully treated. Use of the CytoSorb device in a Covid-19 positive patient was safe and well-tolerated. Early treatment with CytoSorb decreased interleukin 6 plasma levels and inflammatory indexes, resulting in earlier stabilization of homeostasis. This case report suggests that the use of CytoSorb could be a possible adjuvant therapy in patients with septic shock even when affected by Covid-19.
Introduction
Sepsis is a condition associated with high morbidity and mortality, and septic shock, defined as organ dysfunction caused by a dysregulated host response to infection, leads to substantially increased mortality (40%–70%).1–3 Understanding the complex pathophysiology of sepsis has always represented a medical challenge and is still not completely understood. 4 However, one of the key factors seems to be represented by the excessive release of cytokines and other inflammatory mediators that might cause direct organ damage, leading to a condition of multi-organ dysfunction. 4
The role of inflammatory cytokines seems to be confirmed also in Covid-19 patients. 5 The pathophysiology of SARS-CoV-2 infection is characterized by an aggressive inflammatory response strongly implicated in lung damage, and is even more fatal in older patients with existing respiratory comorbidities. Some patients may be affected by secondary infections due to the altered immune system, and this process may result in a cytokine storm and symptoms of sepsis that are the cause of death in 28% of fatal Covid-19 cases. 5
Blood purification techniques have been developed as possible adjunctive treatments for sepsis and other inflammatory states characterized by an overwhelming cytokine production with the aim of attenuating the systemic inflammatory process, and restoring a balanced immune response. 4 CytoSorb therapy (CytoSorbents Corp, New Jersey, USA) is a CE-mark approved sorbent composed of biocompatible porous polymer beads which are able to remove a wide range of substances from whole blood, including the majority of cytokines, inflammatory mediators, endogenous—and some exogenous—molecules through pore capture and surface adsorption. 6 Experimental and clinical studies6–13 have widely demonstrated CytoSorb’s ability to modulate the excessive and uncontrolled immune response, helping to control many of the complications of organ dysfunction in life-threatening illnesses, especially if adopted early within 24 h 12 in patients not responding to the standard therapy. Because of these characteristics, CytoSorb might represent a helpful therapy in septic shock of different etiologies, also in Covid-19 patients, in which only few published experiences are available,14–16 therefore we consider important to report on our own experience.
Case presentation
We report the case of a 75-year-old male patient, presenting with a clinical picture complicated by various pathologies including Parkinson’s disease, Chronic Obstructive Pulmonary Disease (COPD), severe psychosis, and non-insulin-dependent diabetes mellitus at the beginning of May, 2020. The patient proved Sars-CoV-2 positive, and due to severe respiratory failure, was admitted to our Intensive Care Unit (ICU) after 5 days of hospitalization on the infectious disease unit.
During his initial hospitalization, two doses of Tocilizumab were administered (8 mg/kg) according to the clinical indications of the first phase of the pandemic.
On admission to our ICU the Glasgow Coma Score (GCS) was 5, the patient appeared in a somnolent state, non-responsive to painful stimulus, apyretic, oligo-anuric, dyspnoeic (35 breaths per minute), hypotensive (systolic pressure: 65 mmHg) without inotropic administration. The presence of a sacral decubitus lesion with perineal, scrotal, and upper limb edema was immediately evident leading to the diagnosis of secondary septic shock complicating the clinical picture.
A chest computed tomography (CT) scan showed multiple branched centrilobular opacities spread to both lungs compatible with inflammation. Arterial blood gas analysis confirmed a hypoxemic respiratory failure with metabolic acidosis (Base Excess: 9 mmol/L, lactate: 7.57 mmol/L). His laboratory results were notable for a mild leukocytosis of 11 × 10³/mm³, glomerular filtration rate (GFR) of 26, procalcitonin level (PCT) of 10.23 ng/mL, c-reactive protein (CRP) of 14.3 mg/L, and an altered coagulative status with platelet levels of 58 × 10³/mm³ and an INR of 6.2. In addition, D-dimer levels were also elevated (0.74 mg/mL). Blood cultures revealed the presence of Proteus Mirabilis, urine cultures showed Providencia Stuartii and the bronchoalverolar lavage (BAL) was positive for Klebsiella Pneumoniae.
The patient was intubated and protective ventilation began as a result of the respiratory impairment, and treatment according to sepsis criteria was started. 3 Antibiotic therapy with Piperacillin/Tazobactam (4/0.5 g) was set together with a norepinephrine infusion at 0.6 µg/kg/min.
One hour after intubation, the patient had a PaO2/FiO2 ratio of 143, static lung compliance of 37 cmH2O and mixed acidosis. Hemodynamics remained unstable despite the maximum norepinephrine dose (1.4 µg/kg/min) and therapy Terlipressin was started. With an initial hemoglobin value of 7.9 g/dL, it was decided to give a transfusion of two units of RBCs, after which we reached a post-transfusion value of 10.4 g/dL. The single blood bag infusion rate was variable, with an initial 15-min slow drip infusion (10–15 drip/min), then a 2-mL/min infusion for the next hour and a half.
After 24 h in ICU, the inflammatory indexes were still very high, with an interleukin (IL)-6 level of 6768 pg/mL, and hemodynamic support with norepinephrine and Terlipressin. Lactate levels were 7 mmol/L, creatinine kinase (CK) was 5127 U/L, and thrombocytopenia was also present with a platelet level of 43 × 10³/mm³, however the PaO2/FiO2 ratio had increased to 202.
For the septic clinical picture, CytoSorb treatment was considered, firstly in hemoperfusion-mode and then, due to the persistent oligo-anuric state, in combination with a Continuous Venovenous Hemodiafiltration (CVVHDF) treatment (Multifiltrate, Fresenius Medical Care, Bad Homburg, Germany) with a blood flow of 100 mL/min, weight loss at 50 mL/h, and sodium-heparin anticoagulation started at 300 U/h.
CytoSorb treatment was performed for three consecutive cycles of 24 h each. After 24 h from the start of CytoSorb treatment an improvement in metabolic acidosis was visible with a lactate decrease to 3.3 mmol/L. IVC diameter and delta IVC at the start and in the follow-up examination are as follow: at start IVC diameter was 18 mm and delta IVC was <20% and remained stable throughout follow-up as well.
However, IL-6 was still 6010 pg/mL and the need for hemodynamic support remained with a high-dose of norepinephrine and Terlipressin, associated with a PaO2/FiO2 ratio below 200. This was related to the sacral decubitus that had become more severe, consequently, decubitus curettage and positioning of a VAC (Vacuum Assisted Closure) therapy was then performed.
During the course of treatment, there was a substantial reduction in the inflammation indexes (Figure 1) and IL-6 levels (Figure 2). Norepinephrine and Terlipressin doses were progressively decreased as the hemodynamics stabilized (Figure 3). Indeed, after 72 h, IL-6 values had drastically dropped to 1731 pg/mL, PCT was 1.10 ng/mL, CRP was 9.4 mg/L, and lactate was 1.91 mmol/L. The norepinephrine dose was 0.25 µg/kg/min and Terlipressin therapy was ceased. The patient also showed a progressive restoration of diuresis and the PaO2/FiO2 ratio started to stabilize. After 5 days from the beginning of the treatment hemodynamics were stable and adequate without the need of inotropic support and inflammatory indexes were within the physiological range. After 7 days from admission, the patient was extubated after successful weaning off sedation and the ventilator. Blood and urine cultures were negative.
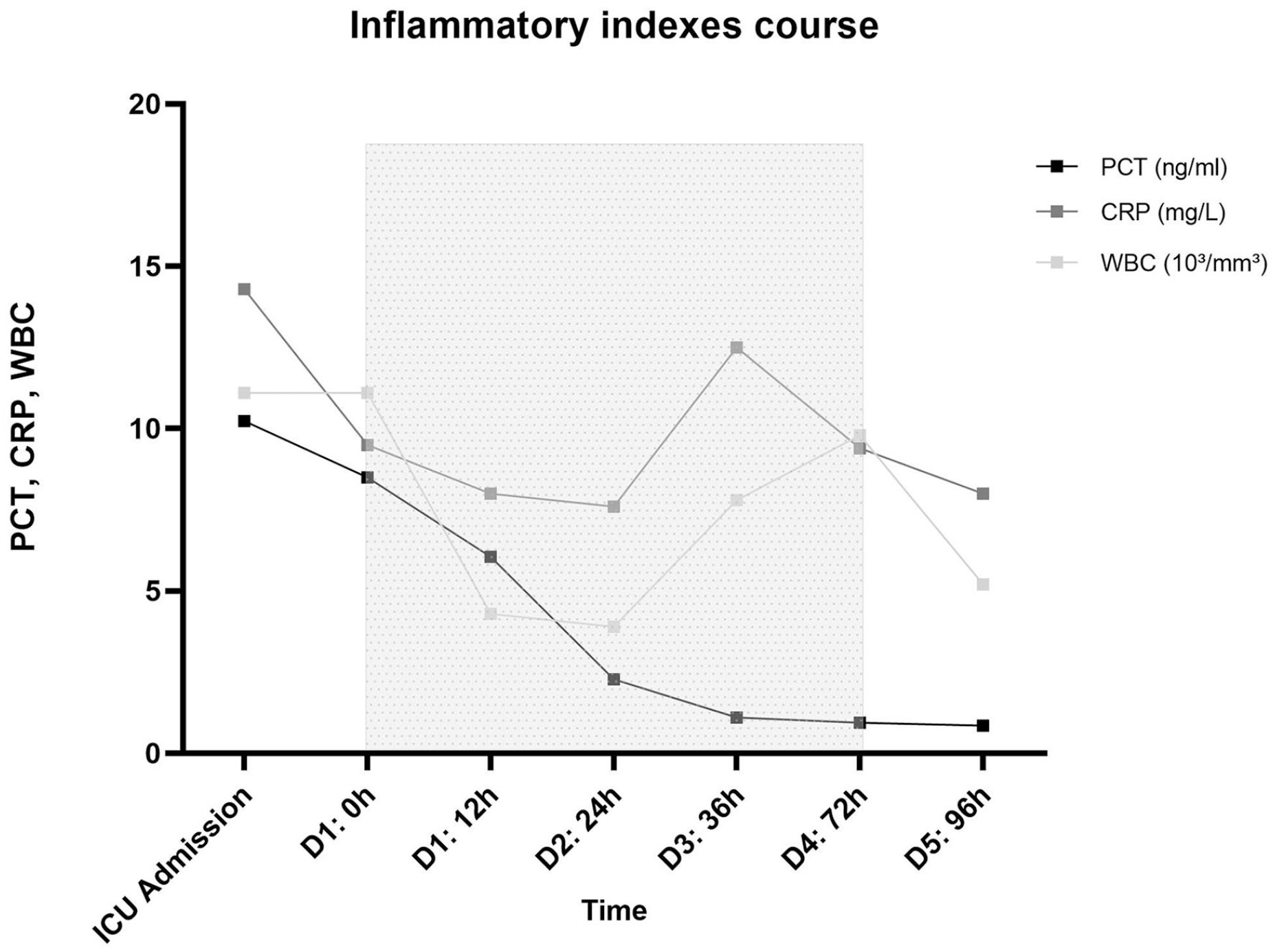
Course of inflammation indexes during the course of the CytoSorb treatment.
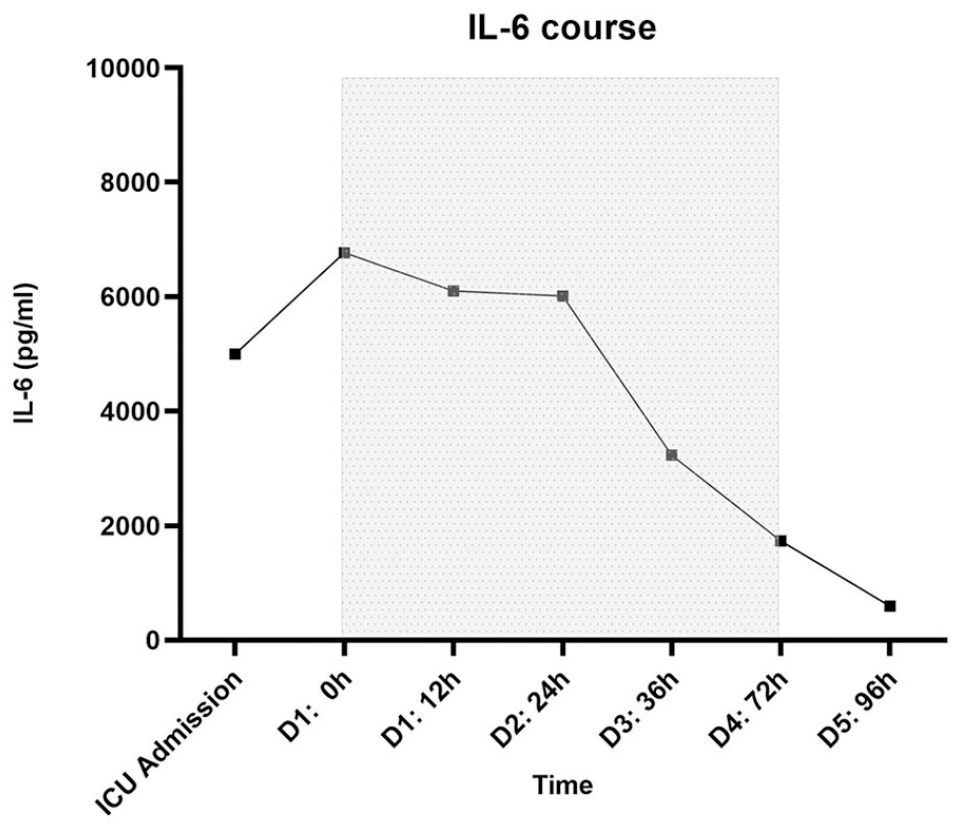
Course of IL-6 during the course of the CytoSorb treatment.
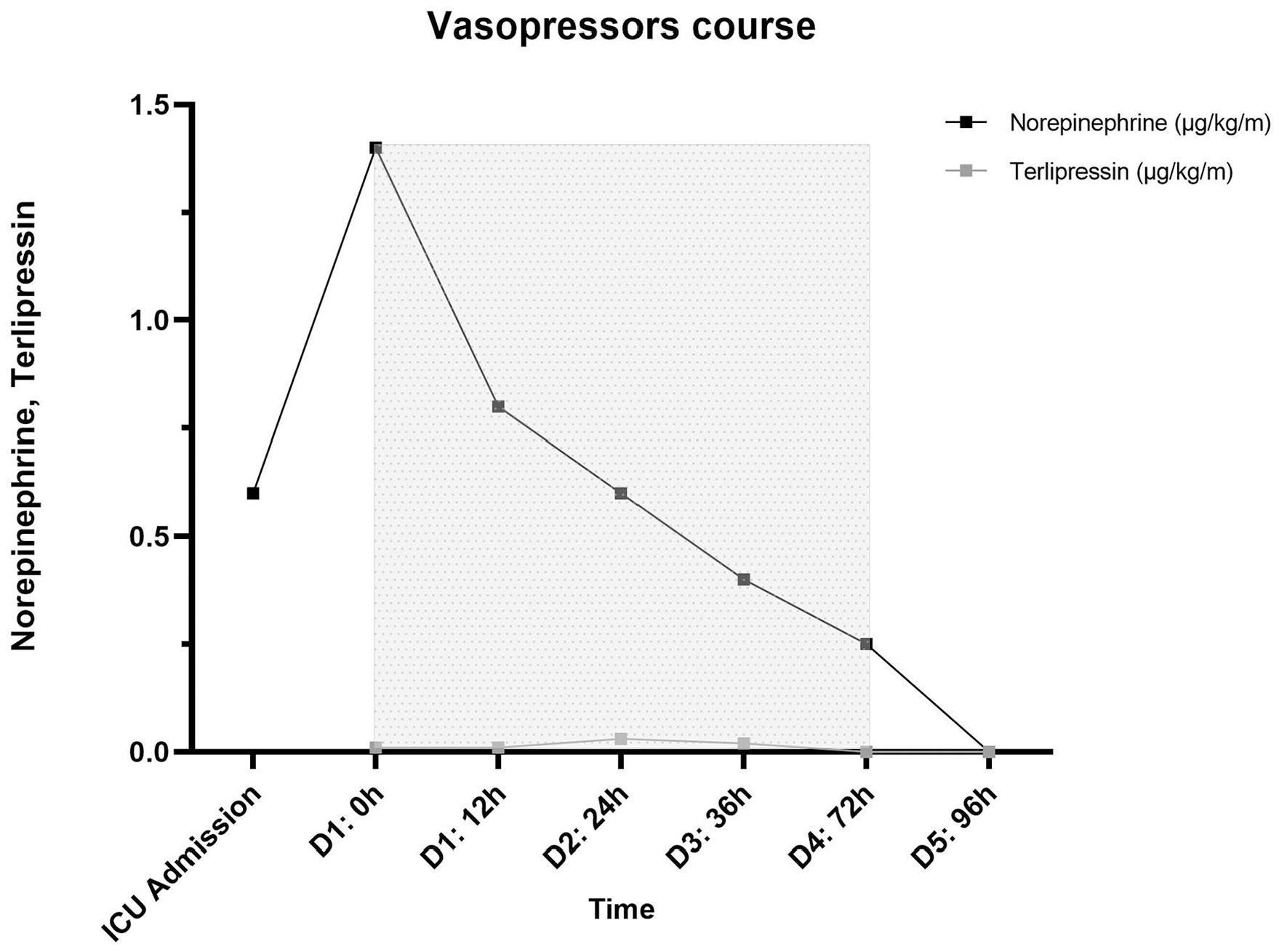
Course of vasopressors during the course of the CytoSorb treatment.
Discussion and conclusions
Sepsis has always been a challenge for the clinicians as it involves all the systems of the body in different ways and is associated with a high risk of death (40%–70% in cases of septic shock). In the panorama of sepsis there are many therapeutic options. Treatment bundles allow clinicians to have a standardized protocol in the management of the first few hours, improving the quality of the treatment and the outcome.1–3 Among the therapeutic possibilities, hemoadsorption might be considered a valid ally in the management of septic shock: the possibility of controlling and limiting the cytokine storm allows the clinician to gain time in an attempt to restore homeostasis. 4 This uncontrolled inflammatory response, typical of septic shock, seems to also be confirmed in the context of Covid-19 patients, aggravating their clinical picture. 5
CytoSorb therapy has shown in in vitro and in animal models, that it is able to remove various anti- and pro-inflammatory cytokines.6,7 Clinical studies in septic shock8–13 confirm these results, showing clinical improvements in term of hemodynamic stability and organ healing, whereas in the field of Covid-19 only few experiences have been reported in the literature.14–16 At the time of the treatment of our patient, the synergistic use of CytoSorb and Tocilizumab in Covid-19 and, generally, in the context of cytokine release syndrome, was supported by the experience of Bottari et al. 17 However, we did not observe any clinical improvement after the sole Tocilizumab administration, perhaps confirming the following results showed by many clinical trials. 18
In our experience, CytoSorb treatment was started in the early phase within 24 h from the admission of the patient into the ICU, according to the literature, 12 showing important improvements already after the first treatment. We observed a progressive drop in the inflammatory indexes, IL-6 values and an improvement in the blood-gas balance, with a progressive stabilization of lactate. The stabilization in hemodynamic parameters led to a progressive decrease of amines and the respiratory parameters returned to normal values leading to successful extubation. CytoSorb treatment was safe and well tolerated by our patient and its application in this field could be very interesting as a new therapeutic strategy for Covid-19 patients with septic shock complications.
A limitation related to the reported case is represented by lack of daily data, as Cardiac Index or Ejection Fraction trends. These data could have been useful to understand deeper the clinical case presented and draw more concrete conclusions. In our experience, even if not shown by actual data, the implementation in daily clinical practice of non-invasive impedance-based monitoring systems (NICOM), allowed us to constantly monitor our patients in order to optimize care and treatments.
Our experience, although promising, is limited and it is obvious that other structured studies should be conducted. In fact, larger case series of patients with clinical pictures similar to the one presented and treated in daily clinical practice could provide more solid and concrete information.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.