
Abstract
The advanced organ support (ADVOS) system allows to eliminate water-soluble as well as protein-bound molecules. Despite its clinical features, to date nothing is known about the elimination of clinically relevant drugs such as antiinfectives. Therefore, we report a case treated with ADVOS, continuous renal replacement therapy (CRRT), and meropenem (1 g 8-hourly) for empiric sepsis therapy monitored by meropenem drug levels. ADVOS showed more efficient elimination of meropenem compared to CRRT which has to be considered when evaluating dosing regimens.
Keywords
Liver injury and failure are common in critically ill patients with an incidence of up to 20%. 1 Patients with acute-on-chronic liver failure (ACLF) and acute liver failure (ALF) can both require intensive care with the main aim of avoiding disease progression and to provide symptomatic treatment. 2 In this scenario, extracorporeal liver support (ECLS) offers the opportunity to either bridge the patient to transplantation or recovery. 3 The current ECLS devices are primarily based on dialysis-like techniques which are often combined with albumin or adsorption cartridges containing charcoal.4,5 In case of ADVOS (advanced organ support system, Advitos GmbH, Munich, Germany) a dialysis-like technique to remove predominantly water-soluble, non-protein-bound substances is combined with an albumin circuit, allowing for removal of protein-bound molecules. During ADVOS the patients’ blood is pumped through two high-flux filters to remove water soluble molecules. Within a second circuit blood is dialyzed against albumin (5%–20%), where free dissociated molecules diffuse towards the albumin site. To recycle albumin and to eliminate toxins, the albumin is regenerated by applying different pH shifts towards acidity or basicity followed again by dialysis. During ADVOS, high blood (200 mL/min) and dialysate-flow (800 mL/min) rates with two polysulfon dialyzers (surface area 1.9 m2) are used in parallel to increase the elimination of toxins.6,7 Since optimal antibiotic exposure is correlated to mortality in sepsis and septic shock, knowledge about the ECLS elimination ratio of commonly prescribed antibiotics is crucial for patient outcome. 8 Therefore, we present a case in which meropenem therapy was guided by therapeutic drug monitoring (TDM) in a patient with liver failure treated with ADVOS and continuous dialysis thereafter. Ethics committee vote was waived due to local regulations allowing for retrospective, anonymous data analysis, and case presentation.
A 75 year old (175 cm, 73 kg), female patient was admitted to the ICU presenting with septic shock due to peritonitis after duodenal ulcera perforation. The patient had pre-existing cryptogenic liver cirrhosis (Child Pugh B, Score 8), with transjugular intrahepatic portosystemic shunting being performed 4 months before ICU admission. Empiric antibiotic therapy was initiated with meropenem according to the in-house guideline for sepsis, whilst taking into account local microbiological surveillance data. Meropenem (1 g) was diluted in 100 mL normal saline and administered IV over 30 min 8 hourly. The patient presented with an acute kidney injury grade 3 accompanied by oligoanuria (100–340 mL urine/d) and severe electrolyte imbalance. Deterioration of liver failure occurred rapidly with an ACLF-Grade 2 and an CLIF-C ACLF Score of 60. 9
ADVOS was initiated on day 1 after ICU admission due to acute renal and liver failure for 2 days of treatment, using the above mentioned parameters. After a total of 2 days of ADVOS, therapy was switched to continuous veno-venous hemodialysis (CVVHD). CVVHD was performed with a 1.4 m2 polysulfon dialysis filter using a blood-flow of 100 mL/min and a dialysate-flow of 2000 mL/h.
During ADVOS and CVVHD, peak and trough levels were drawn according to the in-house standard for routine TDM of total meropenem concentrations. At the same time, additional samples post filter and effluent specimens were taken once. The serum supernatant was analyzed by high performance liquid chromatography with UV-detection (HPLC-UV) after being processed for protein precipitation.
Pharmacokinetic parameters such as half-life (t1/2), total clearance (CLT) and volume of distribution (Vd) were calculated whilst assuming first-order kinetics and a one-compartment model. Total meropenem CLT was calculated as follows: CLT = ln(2) × Vd/t1/2. Dialysator CLD was calculated using the equation BFR × (Cpre − Cpost/Cpre), with BFR being the blood-flow rate, Cpre representing the concentration pre filter, and Cpost being the concentration post filter. Residual body Clearance (CLRB) was calculated by CLRD = CLT − CLD.
Meropenem is a predominantly renal eliminated substance with a rather short half-life of 1 h in patients with normal renal function resulting in a CLT of approximately 12 L/h. 10 As a hydrophilic drug meropenem distributes in the interstitial fluids which is also represented by a small Vd of 0.2 L/kg. In critically ill patients Vd is often elevated due to pathophysiological changes during sepsis or septic shock inclunding capillary leackage.11,12 In patients with severe renal failure meropenem t1/2 increases to approximately 4 h. 13 Since meropenem has neglible protein-binding of only 2% and low molecule size (386 Da), elimination via diffusion and filtration by dialysis techniques are likely and to date well described.14–16
During ADVOS, a t1/2 for meropenem of 2.2 h and total CLT of 8.6 L/h was calculated (Table 1) with an individual Vd for meropenem of 26.5 L. This indicates, that elimination rates increase towards the CL rate of patients with mild to moderate renal insufficiency. 13 During one dosing interval of 8 h, a total 75% of meropenem was eliminated by ADVOS with a CLD of 6.3 L/h and a CLRB of 2.3 L/h. Mean meropenem t1/2 during CVVHD was 3 h with a CLT of 4.7 L/h. The Vd for meropenem was 22 L. During the dosing interval, whilst on CVVHD 27% of meropenem was removed. The CLD was calculated with a mean of 1.6 L/h and CLRB was 3.1 L/h. Since an adsorption of meropenem towards polysulfone filter surfaces (1.2 m2) is determined only up to a fraction of 9%, 17 the increase in ADVOS CLD might be explained by the higher dialysate-flow rates. Moreover, no meropenem as well as no internal standard (ertapenem; added according to the HPLC assay), could be detected in the effluent specimens. This might be due to the chemical instability of carbapenems such as meropenem during large shifts in pH which are used in the external circuit of ADVOS to recycle albumin. 18 A potential adsorption may not be excluded but seems less likely, as the same filter types are used in CVVHD, where meropenem is detectable in effluent specimens. 14
Pharmacokinetic parameters under ADVOS and CVVHD.
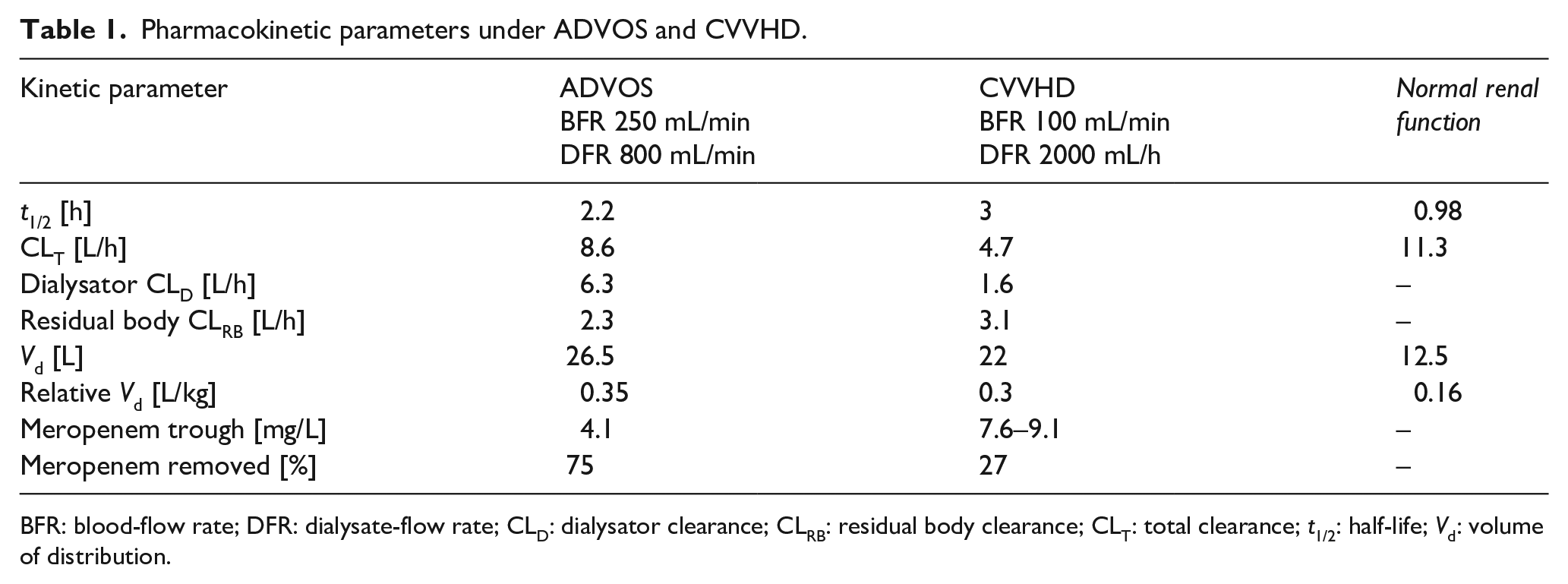
BFR: blood-flow rate; DFR: dialysate-flow rate; CLD: dialysator clearance; CLRB: residual body clearance; CLT: total clearance; t1/2: half-life; Vd: volume of distribution.
As the patient received either ADVOS or CVVHD on consecutive days, the differences in meropenem CLT can be associated to the different extracorporeal modalities. Differences due to improving endogenous clearance could be neglected since the patients’ medical condition worsened over the time course. This is also represented by the CLRB of 2.3–3.1 L/h. The relative Vd of 0.35 L/kg is in accordance with the Vd of meropenem in patients with ACLF where the Vd was found to be increased to 0.47 L/kg. 19 During ADVOS and CVVHD meropenem dosing of 1 g 8-hourly provided trough levels of 4.1–9.4 mg/L (Table 1). When targeting gram-negative bacteria including Pseudomonas aeruginosa trough levels of 2-8 mg/L by the end of the dosing interval (100% fT> 1–4x MIC) are recommended for optimal clinical outcome. 20 Prolonging time above MIC for beta-lactam antibiotics is shown to reduce mortality especially in patients with high disease severity scores. 21 This can be achieved by either extending infusion times for meropenem to 3–4 h and guidance by therapeutic drug monitoring. In this case, the patient received meropenem (3x 1 g) as intermittent infusion (30 min) in the assumption that with decreasing renal function and prolonged half-life drug exposure would be equal or close to prolonged infusion modalities. But, as meropenem CL is increased whilst on ADVOS therapy, prolonged infusion rates should be preferred when aiming for 100% fT> 1–4x MIC. 20 Hence, TDM for beta-lactams such as meropenem is currently recommended by experts but its availability is still uncommon.22,23
While ADVOS has the potential to manage electrolyte and acid-base balance in patients with ACLF, it also removes meropenem to a large extent. Using two dialyzers in parallel in ADVOS doubles the active membrane surface (3.8 vs 1.4 m2) compared to CVVHD. This allows higher diffusion rates towards the dialysate side resulting in a higher elimination of meropenem when using ADVOS. Clinicians should be aware of the potential changes in drug elimination and utilize TDM to guide antibiotic therapy. If TDM is not frequently available, practitioners should monitor the clinical presentation and course of disease also in the light of therapy failure due to inappropriate drug exposure.
Footnotes
Author contributions
C.K. measured meropenem levels, calculated pharmacokinetic parameters, all of the authors participated in evaluation of the results and wrote the article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: meropenem quantification was funded by ADVITOS GmbH