
Abstract
The effect of type of mechanical circulatory support on stroke risk during the early post-transplant period remains undefined in patients bridged to transplant. This study assesses if the type of circulatory support device affects stroke risk in this population. The study cohort of 4257 adult patients bridged with mechanical support to cardiac transplant were derived from the UNOS transplant registry data. Risk factors assessed were age, gender, ischemic time, diabetes (recipient), durable mechanical support at listing and mechanical ventilation pre-transplant. Descriptive statistics were used to describe characteristics of the study cohort. Univariate logistic regression was used to test if there is a significant association between stroke event and all the potential risk factors. Multivariate logistic regression was used to test such associations while adjusting for all other risk factors. Odds ratios (ORs) and their 95% confidence intervals (CIs) in parenthesis, were calculated. p < 0.05 was considered significant. Patients on Extracorporeal membrane oxygenation (ECMO) had the highest risk of stroke immediately post-transplant prior to discharge (OR 3.03, {1.16, 7.95}) followed by Total Artificial Heart (TAH) (OR 2.03, {1.01, 4.07) as compared to those only on a Left Ventricular Assist Device (LVAD). Ischemic time (OR 1.3 {1.09, 1.45}) and diabetes (OR 1.8 {1.29, 2.51}) were significant risk factors. Patients on ECMO and TAH had a 203% and 103% increase respectively in the odds of having a stroke prior to discharge as compared to those only on LVADS.
Keywords
Introduction
The current era of increasing donor shortage and wait list time has promoted a concomitant rise of improved mechanical circulatory support as bridge to transplantation. One of the important complications in this population is stroke. Cerebrovascular complications in the post-transplant population remain a major cause of morbidity and mortality. The incidence of neurological complications varies in studies, depending on time of diagnosis either at death or deduced from clinical manifestations in survivors. The incidence of ischemic stroke and transient ischemic attack (TIA) appear to be the most common cerebrovascular complications in small studies of cardiac allograft recipients at 13%, while hemorrhagic strokes were much lower at 2.5%. 1 The incidence of neurological complications also appears to be highly variable in cardiac allograft recipients ranging from 23% in the perioperative period to 13% in the first 30 days, and 18% in the first decade post transplantation suggestive of higher incidence in the early post-transplant period.2–4 Interestingly, cerebrovascular complications appear to be higher in the post- transplant population perioperatively than those undergoing elective coronary artery bypass surgeries or valve surgeries. 5 Predisposing factors appear to be requirement of pre transplant intra-aortic balloon pump (IABP), LVAD, prolonged cardiopulmonary bypass (CPB) time, older age, >50 % stenosis of extracranial carotid artery and postoperative hepatic failure.6–8 Such predisposition in the setting of low flow hemodynamics suggests that preoperative cerebral hypoperfusion may influence postoperative CNS complications. Hence bridging patients with mechanical support while on the waitlist appears to be a logical solution to optimize flow. Risk of stroke during the perioperative post-transplant period in patients bridged with mechanical circulatory support has not been well elucidated with respect to device type. This study was undertaken to assess if the type of circulatory support device used while on the waitlist or pre-transplantation could influence risk of strokes in the bridge to transplant population in the early post-transplant period prior to discharge.
Methods
Study design
This study is a retrospective analysis of an adult cohort derived from the UNOS registry database. Data was obtained from UNOS by submitting a formal request. The UNOS/OPTN transplant registry data from 2005 to 2015 was used to derive the cohort for this study. The patients with stroke were identified by using the term “stroke” while querying the database. Due to the structure of the database, differentiation into hemorrhagic versus ischemic stroke was not possible and hence not done.
Description of study cohort and data analysis
The study cohort consisted of 4257 patients (⩾ 18 years of age) bridged with mechanical circulatory support to cardiac transplant. This cohort was divided into four groups (Left Ventricular Assist Device (LVAD), Right VAD (RVAD), Extracorporeal Membrane Oxygenation (ECMO) and Total Artificial Heart (TAH) depending on the type of support used as bridge to transplant. Risk factors assessed were age, gender, ischemic time, diabetes in the recipient, presence of mechanical support at listing to transplant and use of mechanical ventilation prior to transplant.
Statistical analysis
Descriptive statistics were used to assess the characteristics of the study cohort. Categorical risk factors were summarized as percentages for patients with and without a stroke event, separately. The log2 scale was used to project small changes better. Univariate and multivariate logistic regression was used to test if there was a significant association between stroke event and the potential risk factors in the post-transplant period before discharge. Odds ratios (ORs) and their 95% confidence intervals (CIs) shown in parenthesis were calculated to evaluate these associations. p < 0.05 was considered significant.
Results
Characteristics of the study cohort
Table 1 shows the characteristics of the study cohort. Males comprised approximately 80% of the population. Group A includes the study subjects who have not had a stroke versus group B which comprises of subjects who had experienced a stroke. The donor ethnicity was predominantly white (66% in group A and 63% in group B). Of the minorities Hispanics and Blacks were almost equally represented. Subjects with type II diabetes constituted 27% in group A and 38% in group B. The VAD population comprised of two groups those who had a VAD at listing while those who received it while listed. The “VAD at listing” population includes patients who had the VAD support at the time of listing for transplant. The “VAD while listed” population includes patients who received a VAD during their time on the wait list but did not have a VAD at the time they were listed.
Characteristics of study cohort with mechanical assist devices.
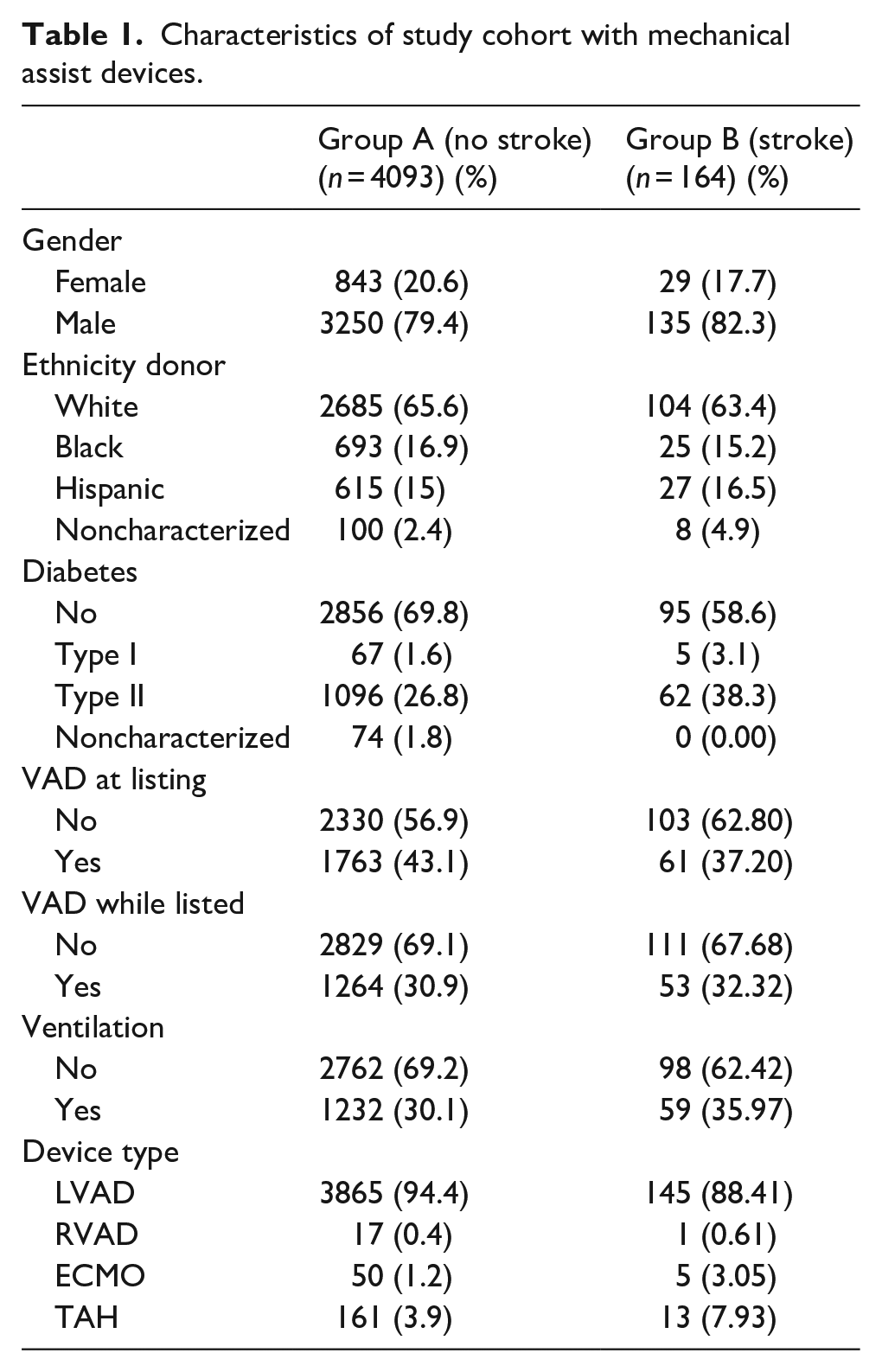
The majority of the study subjects had a LVAD (94% in group A and 88% in group B) while all other types of mechanical support were rare as shown in Table 1. In Table 1 the percentage of patients on ventilation was 30% in group A (no stroke) and 35% in group B (stroke) for the entire cohort. In Table 4 the percentage of patients on ventilation was 29% in group A (no stroke) and 31% in group B (stroke) for the LVAD group.
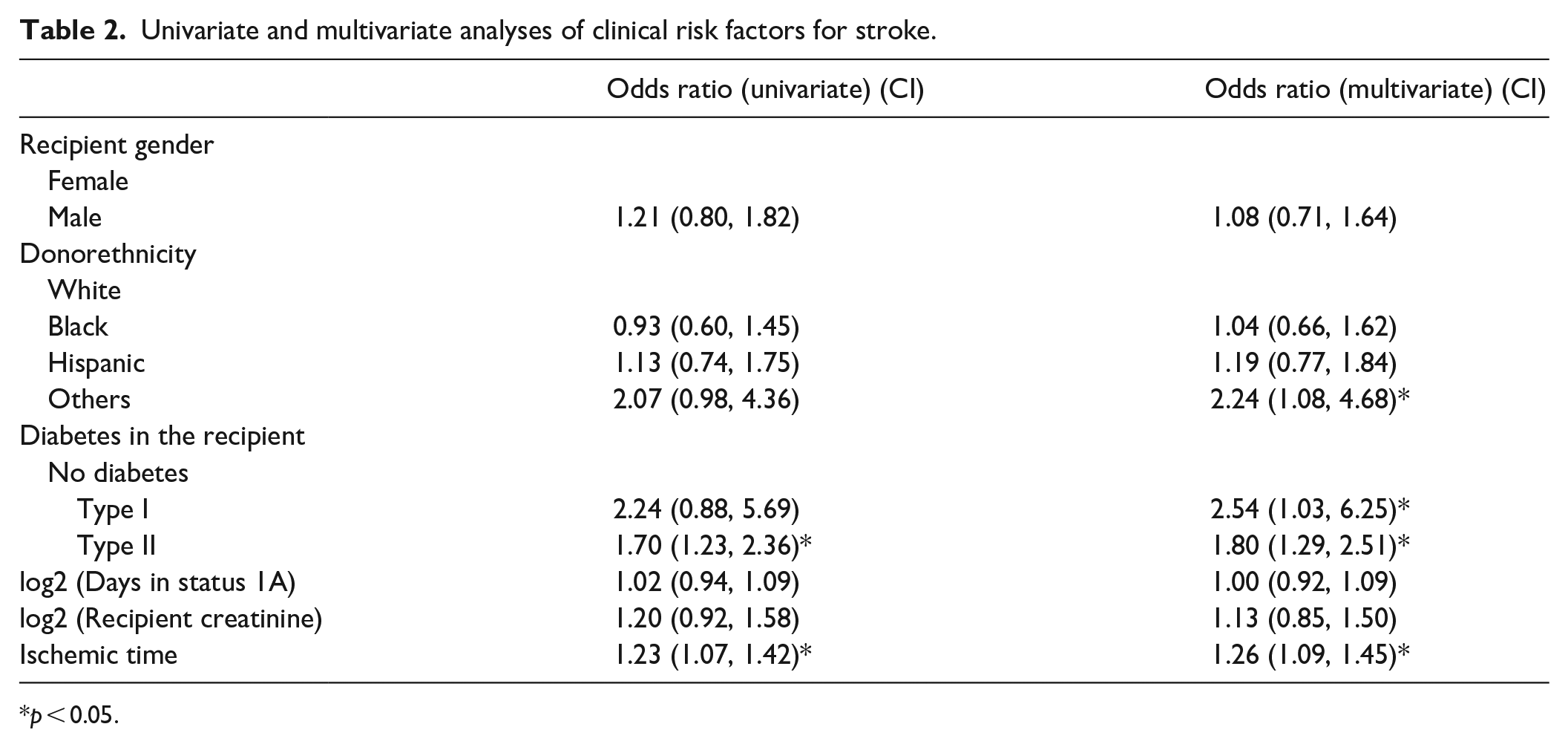
Table 2 shows the univariate and multivariate analyses of clinical risk factors for stroke. The risk factors assessed were donor ethnicity, gender, diabetes, and renal function. Other risk factors assessed included days listed in Status IA and ischemic time. Among the donor ethnicities tested races other than White, Black or Hispanic appeared to be significant in multivariate analyses with an odds ratio of 2.24. Recipient gender was not a significant risk.
Univariate and multivariate analyses of clinical risk factors for stroke.
p < 0.05.
Diabetes types I and II were significant on multivariate analyses. Diabetes type II was significant in both univariate and multivariate analyses while type I was significant only in multivariate analysis. The odds ratios for types I and II were 2.54 and 1.8 respectively on multivariate analyses. Ischemic time greater than 3 h was significant with odds ratios of 1.23 and 1.26 respectively in univariate and multivariate analyses respectively. Days in status 1A and recipient creatinine were not significant in the univariate or multivariate analyses performed.
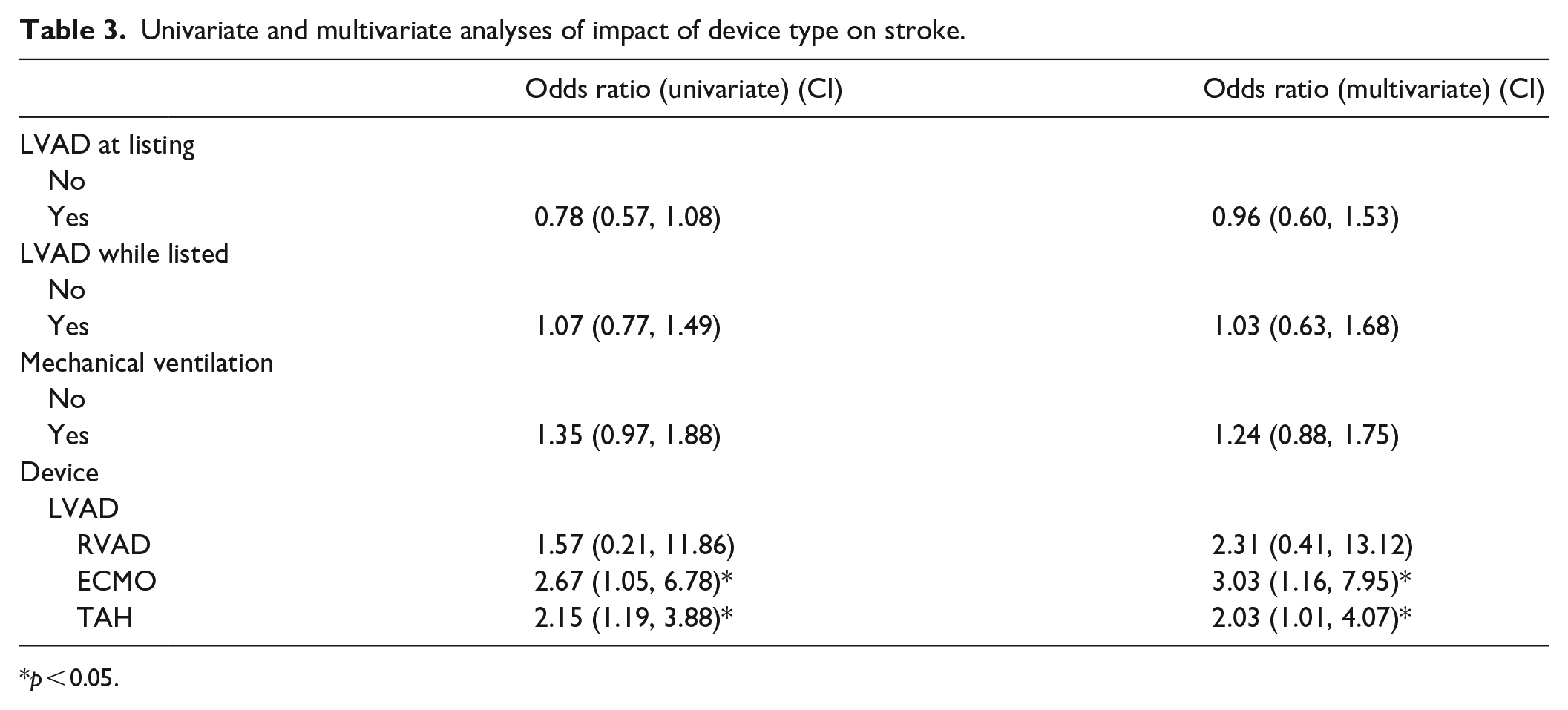
Table 3 shows the univariate and multivariate analyses of device types as risk factors for stroke in the post-transplant period before discharge. The presence of a LVAD at listing or bridged while listed did not make a difference. Mechanical ventilation at transplant was not a significant risk either. Patients supported on ECMO had the highest risk of stroke immediate posttransplant prior to discharge (OR 3.03, {1.16, 7.95}) followed by TAH (OR 2.03, {1.01, 4.07) as compared to those only on a LVAD (p < 0.05).
Univariate and multivariate analyses of impact of device type on stroke.
p < 0.05.
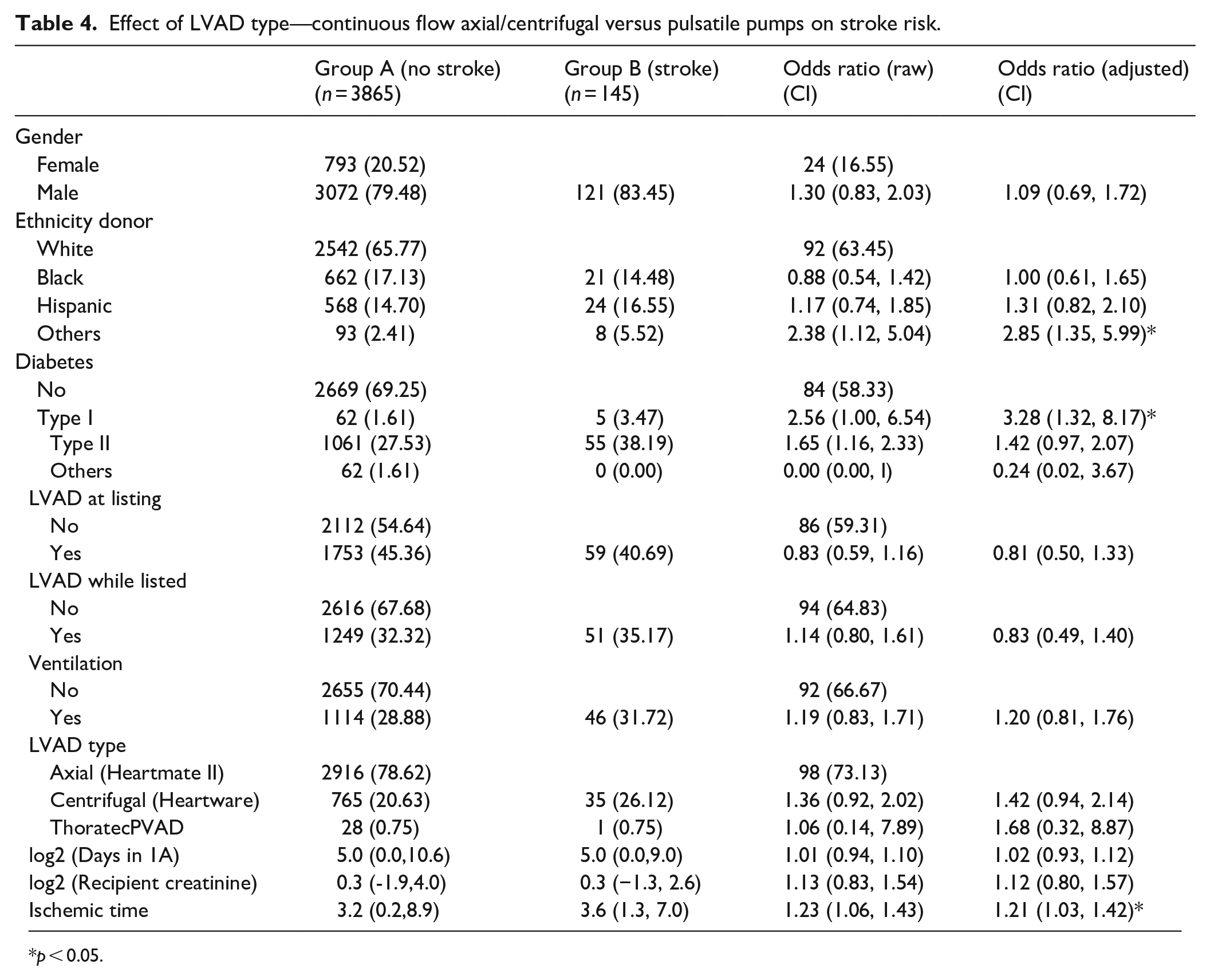
Table 4 shows the univariate and multivariate analyses done to assess if the pulsatile versus centrifugal or axial continuous flow pumps used as LVADs would contribute to increased stroke incidence in the post–transplant period. In this sub analyses the cohort consisted of 3865 patients who did not experience a stroke while 145 patients had a stroke during the posttransplant period prior to discharge. However, the type of LVAD used did not show any significant change in the odds ratio. Type I diabetes showed a significantly high odds ratio of 3.28 in multivariate analyses. Races other than White, Black or Hispanic also showed a significant odds ratio of 2.38 and 2.85 respectively in univariate and multivariate analyses. Ischemic time greater than 3 h was also significant with an odds ratio of 1.21 in this cohort.
Effect of LVAD type—continuous flow axial/centrifugal versus pulsatile pumps on stroke risk.
p < 0.05.
Discussion
Mechanical circulatory support is being increasingly used in the advanced heart failure population. Hence predisposition to strokes in these patients has a large impact on their morbidity and mortality. This paper shows that of all the mechanical support devices used to bridge patients to cardiac transplantation, ECMO and TAH as compared to continuous flow- LVADs (CF-LVADs) show the highest risk for stroke in the post-transplant period prior to discharge. The comparisons were made to CF-LVADs as they have become the mainstay in bridging patients to transplantation.
Current literature shows that patients bridged to transplant with ECMO have increased mortality compared to those with CF-LVADs particularly in the early and mid post-transplant period. 9 Use of ECMO as a rescue therapy has increased over time. Although limited in some countries, ECMO has increased over time due to higher listing status while awaiting transplantation.10–12 Therefore adult ECMO use has escalated logarithmically. Current literature points to neurologic complications while on ECMO leading to increased long-term disability and higher morbidity and mortality rates.13–16 The role of ECMO as a bridge to transplantation needs more scrutiny in the setting of the high costs and poor outcomes associated with neurologic complications. 16
Our study shows that a significant risk of stroke exists in the post-transplant period in patients bridged with TAH also. Earlier reports of increased mortality in the post transplantation period as compared to patients supported on left ventricular assist devices has been reported.17,18 In the era of mechanical assist devices as bridge to transplantation there are newer challenges that need to be addressed with all mechanical support. 19 In fact with CF-LVADs which are standard of care in the present day as bridge to transplantation, duration of support appears to increase mid-term post-transplant mortality. 19
In this study no difference in stroke risk between the different types of CF-LVADs (axial versus centrifugal) or pulsatile LVADs studied were noted. This study highlights the importance of increased risk of stroke using ECMO or TAH in the post-transplant period therefore leading to poorer quality of life and survival. The results presented here needs to be validated in other databases and in prospective studies. Further research is warranted to determine strategies to prevent neurologic complications in this patient population to preserve quality of life.
Our study is limited by its retrospective nature and the patient population is derived from a large database where differentiation of hemorrhagic versus ischemic stroke was not possible. In the existing literature from small studies ischemic strokes appear to be predominant as compared to hemorrhagic strokes in the post-transplant population (13% vs 2.5%). 1 The most common type of stroke in the early post-transplant period has been found to be ischemic. 8 It is therefore possible that in this cohort which addresses the early post-transplant period, the predominant type of stroke is ischemic. Further studies are required in this area.
In a small study patients bridged to transplantation directly from ECMO versus those bridged from ECMO via a CF-LVAD device prior to transplantation had a 7-fold higher incidence of stroke. 20 This is possibly due to the sicker condition of the patients on ECMO going directly to transplantation. Additionally, different devices have different stroke rates even within the same class of centrifugal CF-LVADs. 21 These observations lend support to the fact that the clinical condition of the patient may also contribute to the outcomes in a large way in addition to the mechanical circulatory support device types used in each clinical scenario.
In this study the percentage of patients on ventilation was 30% in group A (no stroke) and 36% in group B (stroke) for the entire cohort and the percentage of patients on ventilation was 29% in group A (no stroke) and 32% in group B (stroke) for the LVAD group. Comparison of creatinine in the two groups showed slightly lower values in group B versus group A. Large databases also have the disadvantage of missing and incomplete data which can impact results. Despite these limitations, this study lends credence to the fact that incidence of strokes in the early post-transplant period prior to discharge is also influenced by the type of mechanical support used as the bridge to transplantation in addition to the clinical history of the patients in the perioperative period.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This is funded by the Office of faculty development, texas tech University health science center el paso.