
Abstract
Introduction:
Due to the inability to keep up with the demand for heart transplantation, there is an increased utilization of left ventricular assist devices (LVAD). However, paucity of data exists regarding the association of household income with in-hospital outcomes after LVAD implantation.
Methods:
Retrospective cohort study using the NIS to identify all patients ⩾18 years who underwent LVAD implantation from 2011 to 2017. Statistical analysis was performed comparing low household income (⩽50th percentile) and high income (>50th percentile).
Results:
A total of 25,503 patients underwent LVAD implantation. The low-income group represented 53% and the high-income group corresponded to 47% of the entire cohort. The low-income group was found to be younger (mean age 55 ± 14 vs 58 ± 14 years), higher proportion of females (24% vs 22%), and higher proportion of blacks (32% vs 16%, p < 0.001 for all). The low-income group was found to have higher prevalence of hypertension, chronic pulmonary disease, smoking, dyslipidemia, obesity, and pulmonary hypertension (p < 0.001 for all). However, the high-income cohort had higher rate of atrial tachyarrhythmias and end-stage renal disease (p < 0.001). During hospitalization, patients in the high-income group had increased rates of ischemic stroke, acute kidney injury, acute coronary syndrome, bleeding, and need of extracorporeal membrane oxygenation (p < 0.001 for all). We found that the unadjusted mortality had an OR 1.30 (CI 1.21–1.41, p < 0.001) and adjusted mortality of OR 1.14 (CI 1.05–1.23, p = 0.002).
Conclusion:
In patients undergoing LVAD implantation nationwide, low-income was associated with increased comorbidity burden, younger age, and fewer in-hospital complications and all-cause mortality.
Introduction
Heart failure has become increasingly prevalent with >6.5 million Americans currently impacted. 1 Individuals of lower socioeconomic classes are significantly more likely to develop heart failure compared with their wealthier counterparts. 2 Differences in the allocation of medical resources, access to quality medical care, ability for self-care, level of education, and generalized support are among the multifactorial reasons that contribute to this disparity.2,3 Heart transplantation remains the gold standard for patients experiencing end stage heart disease. However, due to the paucity of donor hearts and the multiple contraindications based on strict transplantation recipient criteria, this option is limited to a small select group of individuals. 4 When controlling for risk factors for post-transplant mortality, individuals of lower socioeconomic class have also been shown to have worse outcomes and decreased post-transplant survival.3–6 Socioeconomic deprivation may modify several cardiovascular risk factors, making these individuals even less likely to be considered for transplantation. The utilization of alternative therapies is currently thriving. LVADs double the 1-year survival rate of patients with end-stage heart failure as compared with drug treatment alone and provide an effective alternative to individuals who are unable to receive a transplant.7,8 LVADs have also advanced to not only serve as a heart transplantation bridge but also as a destination therapy. These serial improvements have led to the growing use of LVADs in a large percentage of the heart failure population. For individuals of lower socioeconomic classes, numerous studies have shown that these patients more often had an upfront strategy with LVAD implantation compared with remaining on pharmacologic therapy and perpetual waiting on the transplant list. 3 The Registry Evaluation of Vital Information for VADs in Ambulatory Life (REVIVAL) study expanded on this by demonstrating that there was a greater preference for individuals with an annual income <$40,000 to receive an LVAD compared with higher income individuals who were significantly more reluctant to accept an LVAD. 9 As the technology driving LVADs continues to improve and as more studies demonstrate the benefits of these devices as destination therapy, together with an increased willingness of a population subset to receive these devices, it is important to look at the rate of utilization of these devices across different socioeconomic classes. Our study aims to analyze the current trends and variances in LVAD utilization and to further delve into the reasons for, and implications of, these socioeconomic disparities.
Material and methods
The National Inpatient Sample (NIS) offers the largest database of hospitalizations, representing a 20% random, stratified, sample of hospital discharges in the United States. To identify the study population, International Classification of Diseases, ninth (ICD-9) and tenth (ICD-10) revisions, Clinical Modification (CM), and Procedure Coding System (PCS) codes were used. All the data under NIS are publicly available. Institutional review board approval was not needed, as all patient information is de-identified within the NIS, and informed consent was waived. Detailed methods used for statistical analyses are presented under the Data Supplement, which can be used for replication of our results.
From 2011 to 2017, a total of 43,077,206 discharge records comprised the NIS for the US adult population (age 18 years or above), corresponding to a national estimate of 214,107,782 hospitalizations across the country. We identified all patients aged 18 years or older undergoing LVAD implantation using ICD-9-PCS code 37.66 and ICD-10-PCS code 02HA0QZ in any procedure field. Our final study cohort comprised 5131 patients undergoing LVAD implantation, corresponding to a weighted estimate of 25,503 overall LVAD implantations during this time period. This estimate was calculated by using discharge weights provided with the NIS files. The study population was reflective of the one device era—the continuous flow (CF) device based on the US Food and Drug Administration approval of CF devices in 2008. ICD-9-CM/PCS and ICD-10-CM/PCS coding for comorbidities, post-LVAD complications and other procedures is listed in Table 1 in the Data Supplement.
Our primary outcome was post-LVAD implantation all-cause inpatient mortality. Secondary outcomes of interest were intraoperative cardiac arrest, post-procedure ischemic stroke, post-procedure thromboembolism, infections, major gastrointestinal (GI) bleeding, cardiac complications (such as pericardial complications, complete heart block and insertion of permanent pacemaker), short-term percutaneous mechanical circulatory support (PCMS), implant-related complications and acute kidney injury (AKI) for index hospitalization during which patients received LVADs. Detailed methods, including covariate ascertainment, are included under the Data Supplement.
As recommended by the Agency for Healthcare Research and Quality, weighted data were used for all statistical analyses. Temporal trends in LVAD utilization as well as post-LVAD mortality were assessed using the average annual growth rate formula. Baseline characteristics and post-LVAD outcomes were compared using the Pearson Chi-Squared (χ2) tests for categorical variables, independent samples T-test for parametric continuous variables, and Mann-Whitney U test for non-parametric continuous variables. We considered statistical significance when p value was below 0.001. NIS provides median household income for patient’s ZIP code divided by percentile. High-income patients were considered between the 51st to 100th percentile and low-income individuals were considered between 0 and 50th percentile. The association between income and post-LVAD mortality was analyzed using multivariable logistic regression. All multivariable regression models were created using generalized estimating equations. Missing data for race were handled using multiple imputation as recommended by Healthcare Cost and Utilization Project. Missing primary payer status in patients 65 years old or older was imputed to Medicare, whereas missing data for all other variables were imputed to the dominant category (see Supplemental Material). All statistical analyses were performed using SPSS (IBM SPSS Statistics for Mac, Version 23.0. Armonk, NY: IBM Corp.).
Results
A total weighted estimate of 25,503 hospitalizations for LVAD implantation were identified during 2011–2017. Average age of the entire cohort was 57 ± 13 years, with a median of 59 years, ranging from 18 to 90 years. Female gender accounted for 23% (n = 5820) of the total population. The high-income group comprised 47% (n = 11,907) of the cohort and the low-income group represented 53% (n = 13,595) (see Table 1). All comparisons henceforth are reported as low-income versus (vs) high-income for consistency. We found an average increased rate of LVAD implantation from 2011 to 2017 of 11% for the low-income group and 8% for higher income individuals (see Figure 1).
Comparison of baseline characteristics of patients undergoing left ventricular assist device by income.
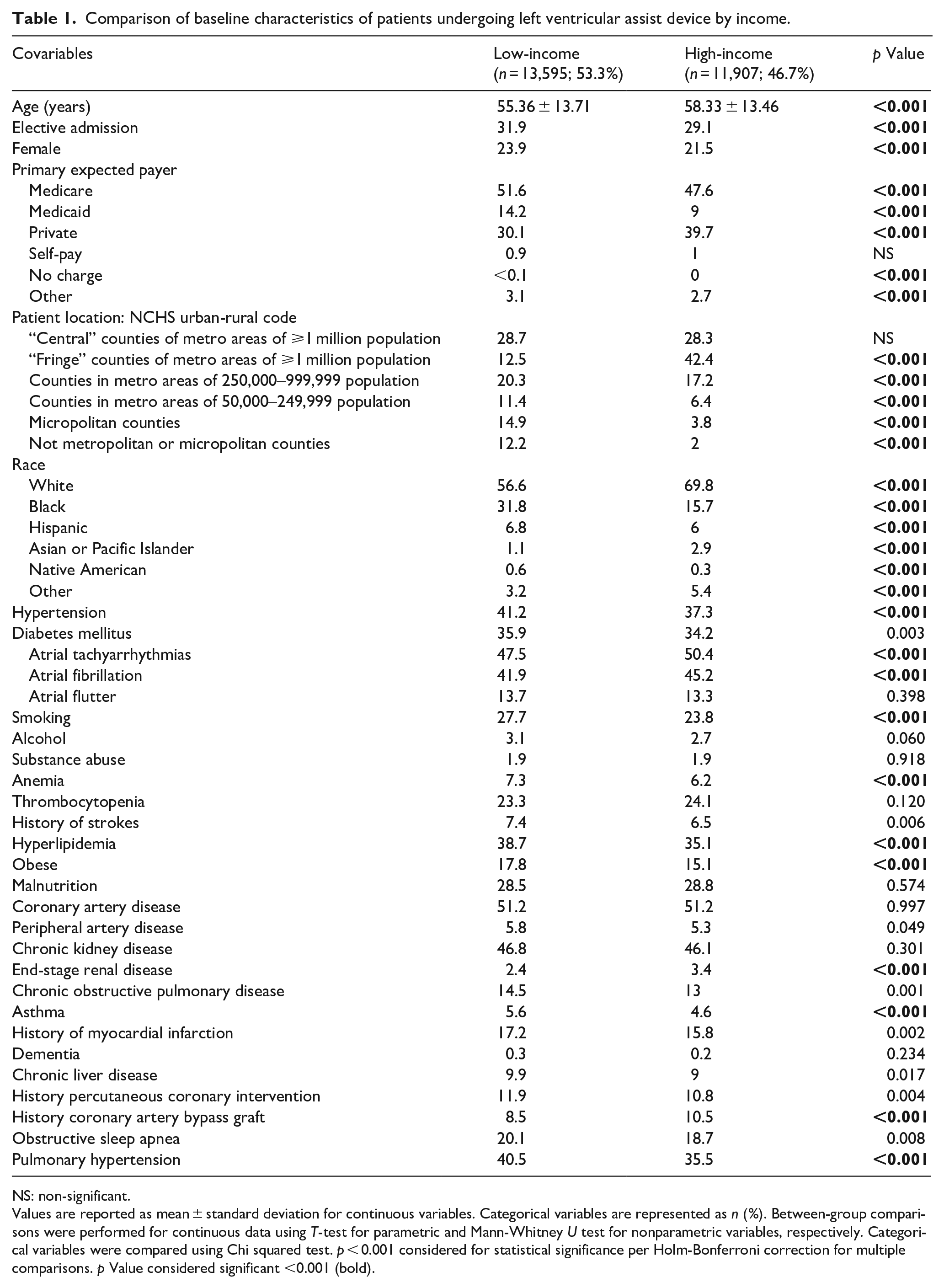
NS: non-significant.
Values are reported as mean ± standard deviation for continuous variables. Categorical variables are represented as n (%). Between-group comparisons were performed for continuous data using T-test for parametric and Mann-Whitney U test for nonparametric variables, respectively. Categorical variables were compared using Chi squared test. p < 0.001 considered for statistical significance per Holm-Bonferroni correction for multiple comparisons. p Value considered significant <0.001 (bold).
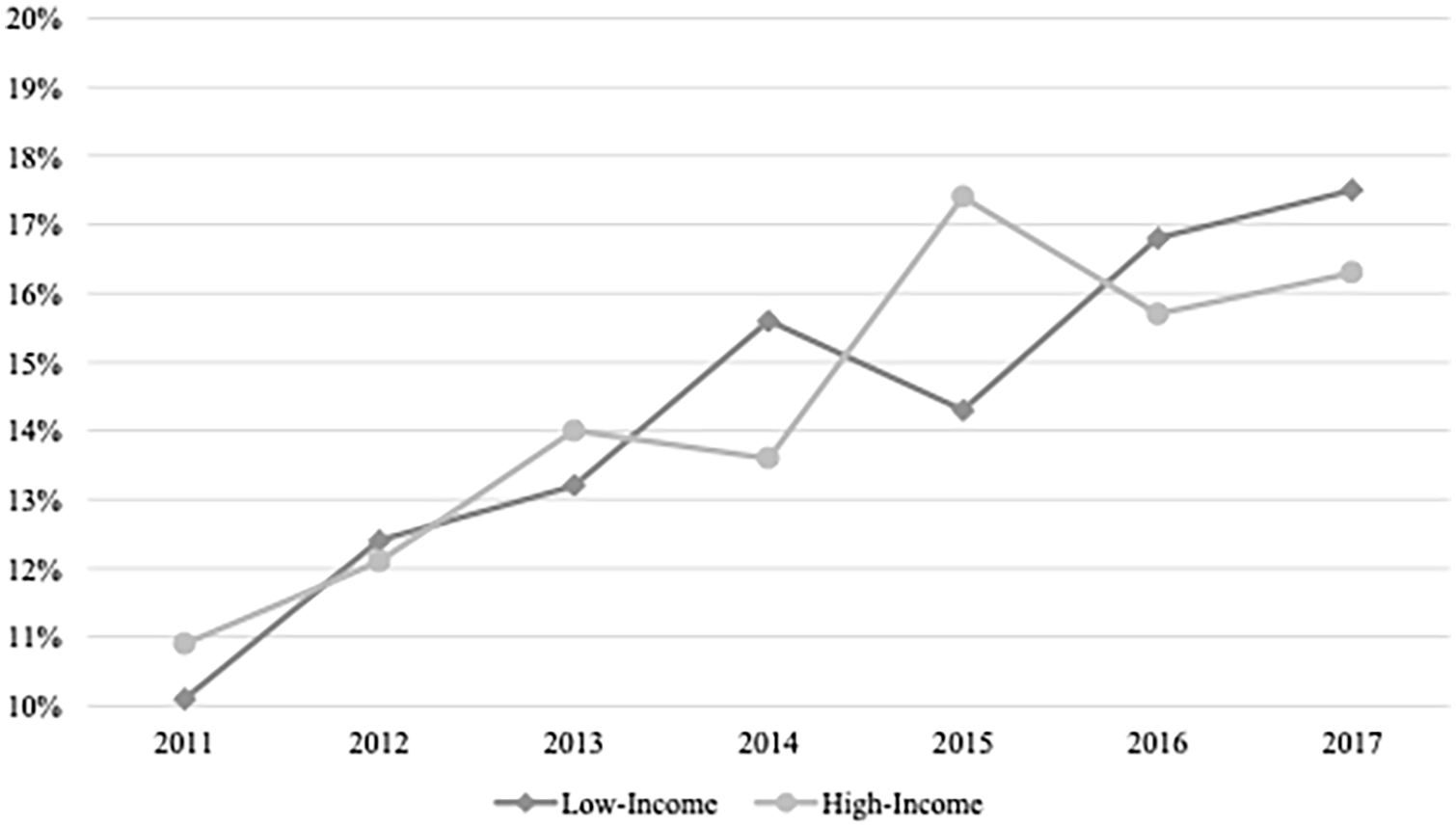
Number of left ventricular assist devices implanted per every calendar year by income. Average increase per year of the low-income group was 11% and for the high-income group was 8%.
Low-income group mean age was significantly lower (55 ± 14 vs 58 ± 13, p < 0.001), with an increased proportion of females (24% vs 22%, p < 0.001) when compared to the high-income group. Patients with higher income are more likely to be from suburbs of metro areas of ⩾1 million population (13% vs 42%, p < 0.001) and self-identified as White (57% vs 70%, p < 0.001). In term of comorbidities, the low-income group was found to have significantly higher proportions of hypertension (41% vs 37%, p < 0.001), smoking (28% vs 24%, p < 0.001), anemia (7% vs 6%, p < 0.001), dyslipidemia (39% vs 35%, p < 0.001), obesity (18% vs 15%, p < 0.001), and pulmonary hypertension (41% vs 36%, p < 0.001). However, the high-income group had increased rates of atrial tachyarrhythmias including atrial fibrillation and atrial flutter (48% vs 50%, p < 0.001) and history of coronary artery bypass graft (9% vs 11%, p < 0.001). There were no significant differences found in diabetes, alcohol and substance abuse, malnutrition, prior strokes, coronary artery disease, peripheral artery disease, chronic kidney disease, chronic liver disease, history of percutaneous coronary intervention or obstructive sleep apnea between both groups.
However, in the high-income group, we found significantly longer hospital stay (median 29 (20–42) vs 29 (20–44) days, p < 0.001) (see Figure 2), higher hospital charges (median $770,852 (544,193–1,135,933) vs $727,922 (539,402–1,034,619), p < 0.001), increased proportion of post procedure strokes (5.6% vs 8.3%, p < 0.001) with ischemic strokes comparison of 4% vs 7% (p < 0.001), acute kidney injury (59% vs 63%, p < 0.001), bleeding (29% vs 33%, p < 0.001), and need of extracorporeal membrane oxygenation (6% vs 8%, p < 0.001) (see Table 2).
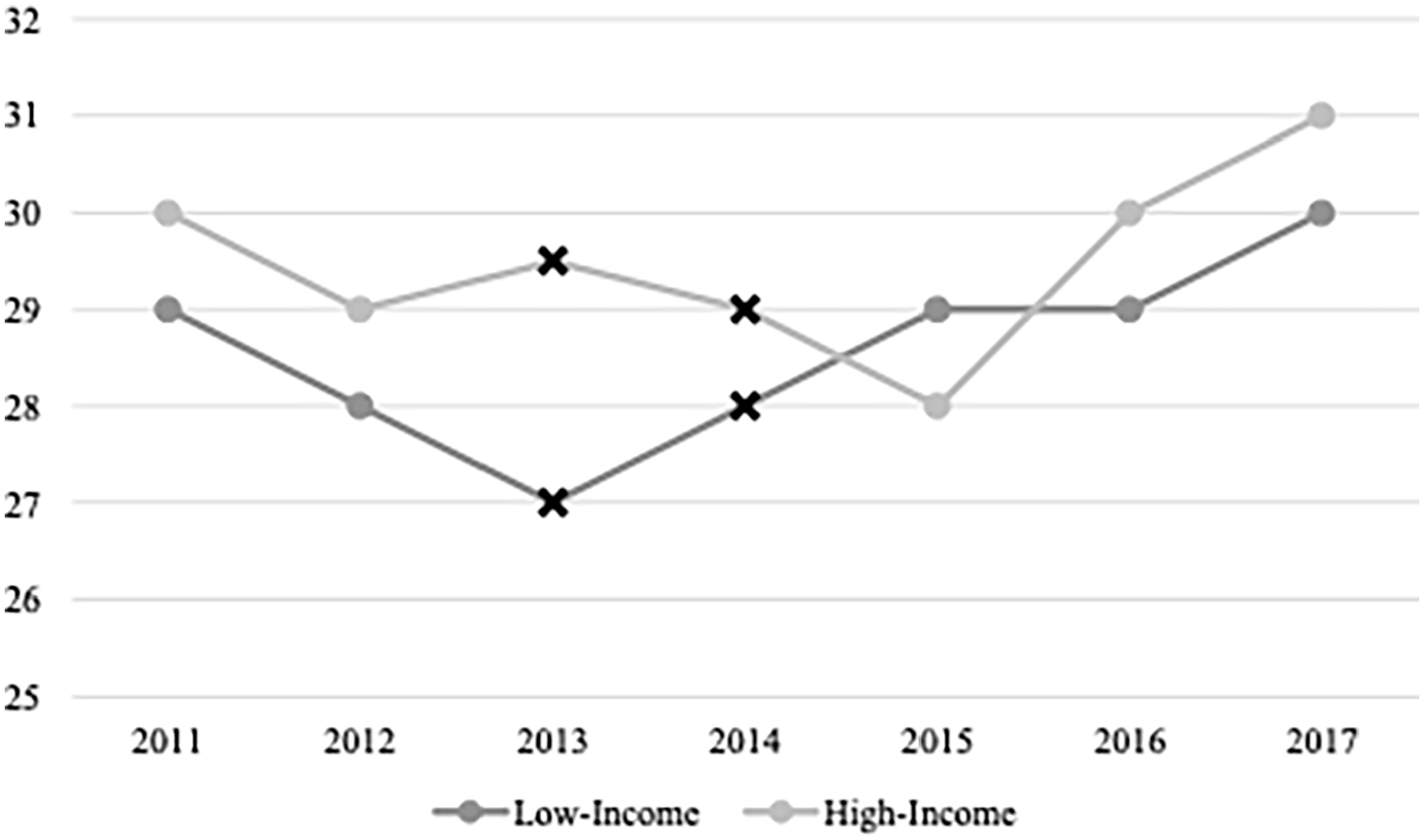
Medium length of stay (LOS) in days in patients undergoing left ventricular assist device (LVAD) implantation by income per every calendar year. Variables were compared using Mann-Whitney U test with p < 0.001 considered for statistical significance (Black X). Dots: non-significant difference.
Comparison of outcomes of patients undergoing left ventricular assist device by income.
NS: non-significant.
Values are reported as mean ± standard deviation and median (IQR 25–75) for parametric and non-parametric continuous variables, respectively. Categorical variables are represented as n (%). Between-group comparisons were performed for continuous data using T-test for parametric and Mann-Whitney U test for nonparametric variables, respectively. Categorical variables were compared using Chi squared test. p < 0.001 considered for statistical significance per Holm-Bonferroni correction for multiple comparisons. p Value considered significant <0.001 (bold).
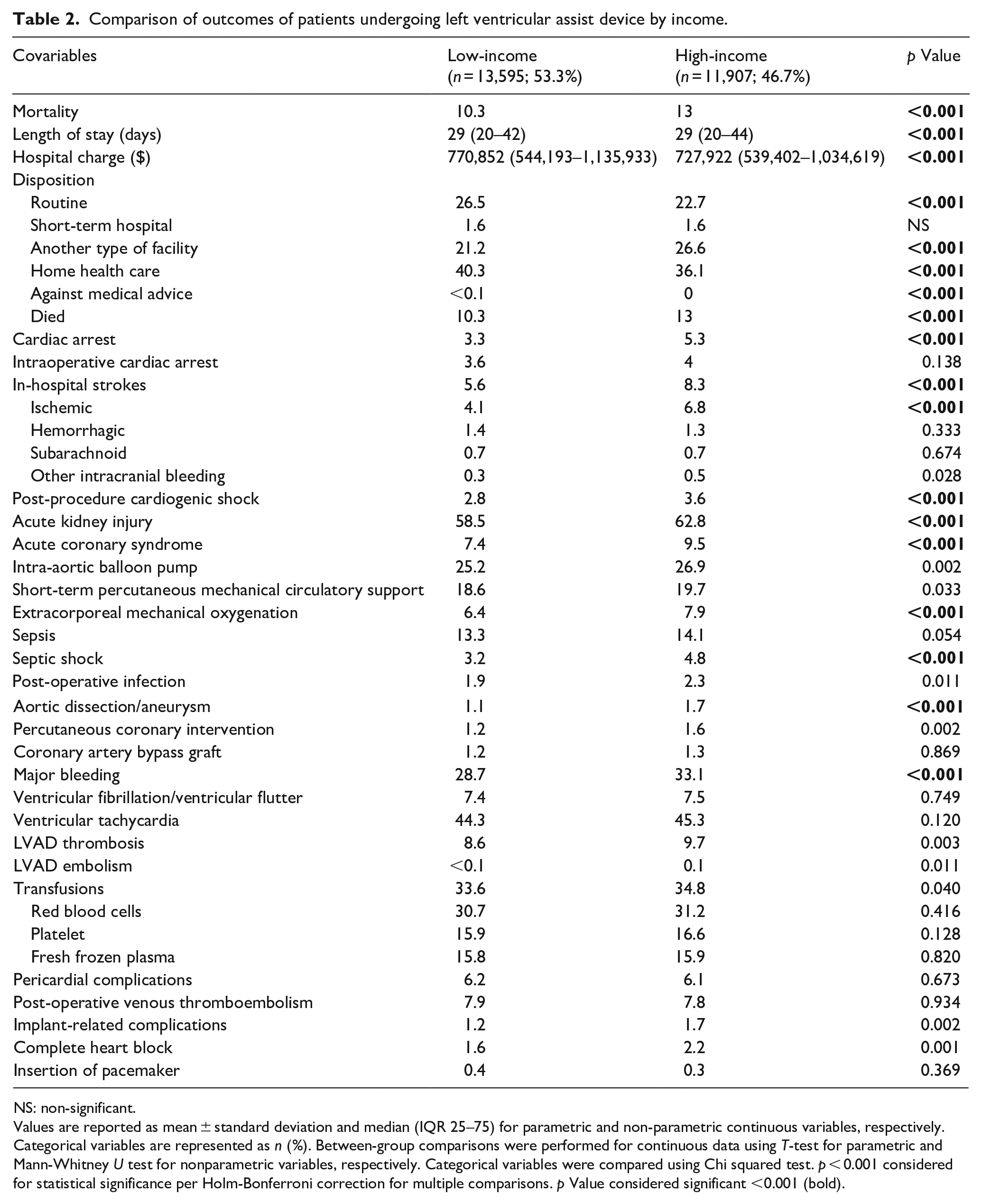
No significant differences were found in the incidences of ventricular arrhythmias, blood product transfusions, pericardial complications, postoperative deep venous thrombosis and pulmonary embolism, LVAD thrombosis or embolism between groups. There was a decreased rate of in-hospital mortality in patients undergoing LVAD from 2011 to 2017 in both groups (see Figure 3).
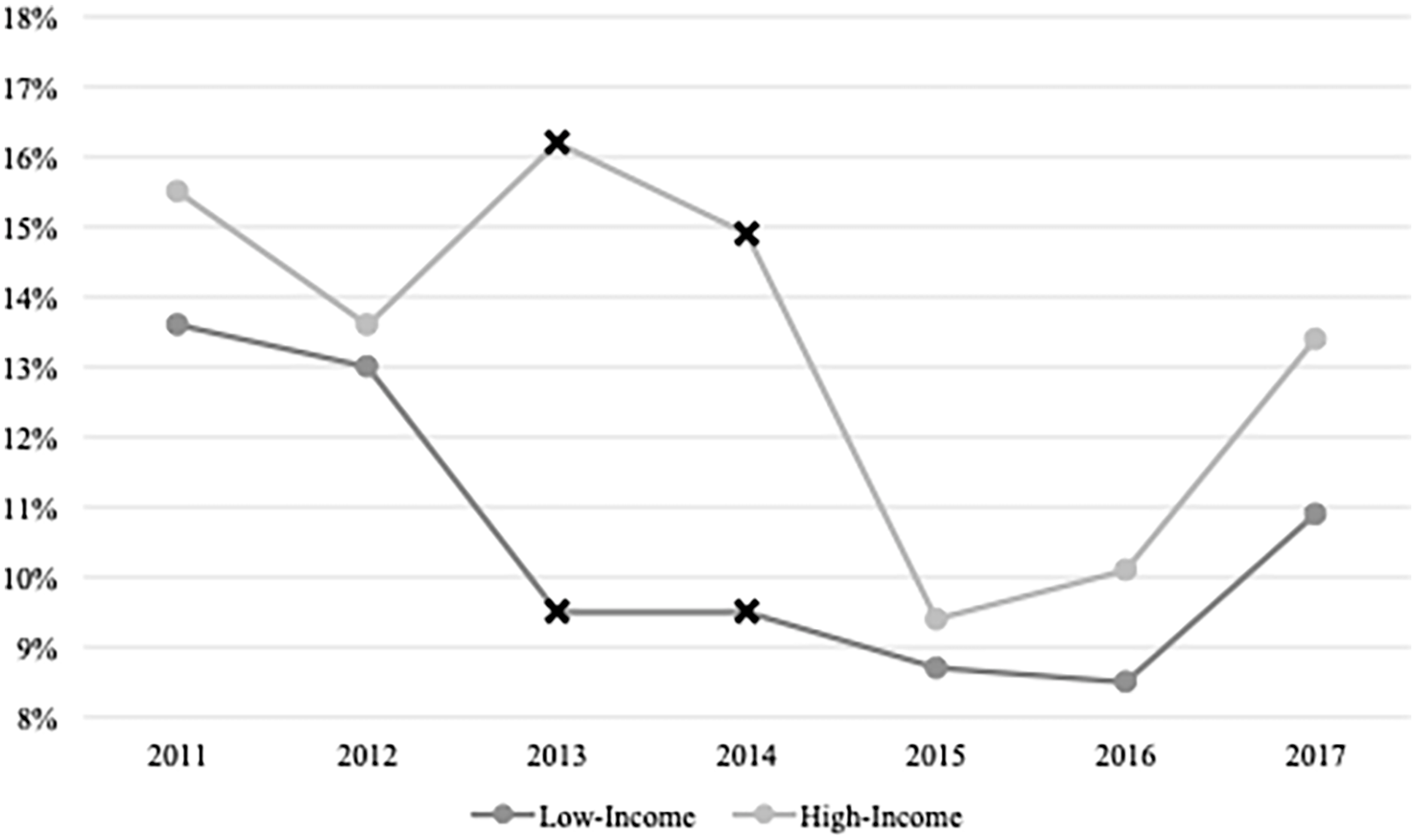
Trend and comparison of inpatient all-cause mortality of patients undergoing left ventricular assist device (LVAD) by income per every calendar year. Variables were compared using Chi squared test with p < 0.001 considered for statistical significance (Black X). Dots: non-significant difference.
Combining data from all years (2011–2017), high-income was associated with higher post-LVAD all-cause inpatient mortality (odds ratio (OR) 1.303; 95% confidence interval (CI) 1.207–1.407; p < 0.001) that remained significant beyond adjustment for demographic factors and comorbidities (OR 1.178; 95% CI 1.085–1.280; p < 0.001).
Discussion
Previous published studies agreed with our results indicating that the primary population of LVAD recipients are middle-aged men of lower socioeconomic class. 10 Our study further demonstrates that low-income recipients had a younger average age at 55 years. Increased burden of medical comorbidities in lower income communities has been long recognized and provides added risk factors for individuals to experience more severe illness at a young age.3,11,12 Several studies have shown that the higher prevalence of cardiovascular risk factors underlies the earlier age of heart failure onset in African Americans, who coincidentally also make up a larger population of the lower socioeconomic class.9,13–15 It is estimated that African Americans are 30% more likely to die from heart disease and are significantly more prone to comorbidities including diabetes, hypertension, and obesity, among many others, which leads to the use of advanced therapies at an earlier age in this population.14–16 The REVIVAL Registry further delves into how socioeconomic factors impact patient preference for LVAD devices. Consistent with our study demonstrating higher LVAD use and acceptance among socioeconomically disadvantaged patients, the REVIVAL study has shown that there is a greater preference for LVAD devices among patients with high school education or less and those with an annual income <$40,000. 9 The reasoning behind this decision making is complex and may reflect limited health literacy, lack of knowledge of alternative therapies, and ineligibility for heart transplantation.9,17
The National Survey of Families and Households, the Survey of Income and Program Participation, and the National Health Interview Survey represent the keystone of information necessary to study the link between income and health. Researchers have long noted a positive correlation between wealth and longevity, with higher income individuals having greater life expectancy compared to low-income counterparts. 18 It has been previously shown that the incidence of obesity and smoking has declined as wealth increases in the general United States population, whereas those in the poorest wealth category have a 2.5- and 5-times higher incidence of obesity and tobacco smoking, respectively. 19 However, it would be incorrect to say that higher wealth individuals do not experience health adversity as well. Diseases of affluence primarily reflect chronic non-communicable ailments including, but not limited to: cancer, degenerative autoimmune diseases, chronic lung diseases, type 2 diabetes mellitus, and hypertension. 20 These comorbidities and their chronic progression are risk factors for cardiovascular disease, providing a rudimentary explanation for heart failure and the need for advanced cardiac intervention at a later point in the lives of wealthy individuals.3,21
When differentiating between patients eligible for transplantation versus alternative therapies, many patients with significant comorbidities are deemed ineligible for transplantation, leaving LVADs as one of the few advanced therapy options available. 17 Previous studies indicate that individuals are more willing to receive an LVAD as the severity of their disease worsens and as their health-related quality of life diminishes. Furthermore, many wealthy individuals have at least one contraindication to heart transplantation often stemming from chronic diseases and ailments such as pulmonary hypertension and advanced age. 22 Despite limited options, higher socioeconomic status patients are significantly more reluctant to undergo LVAD implantation as opposed to a heart transplant for a multitude of reasons. 9 Potential reasons for this decision-making include perception of quality-of-life restrictions with the device, death as simply another alternative to refusing therapy rather than a definitive event, and lack of knowledge about both the LVAD device and associated procedure. Patients may instead elect to seek out other options and underestimate the severity of their illness. 9 Delayed decision-making may lead to progression of disease, which might reduce LVAD utility. 23
For those who elect to undergo LVAD implantation, the mean cost for the procedure alone is $175,420. 24 Patients then remain in the hospital for at least 2–3 weeks as care is adjusted to meet individual patient needs with the median length of stay at 20 days.24,25 Our study found a significantly longer hospital stay for both groups at 35 and 37 days for low- and high-income groups, respectively. A number of pre- and peri-implant factors contribute to hospital length of stay. Increased age, as with the high-income population, is one of the largest risk factors for increased hospital length of stay. 25 Prolonged admission time inevitably increases the all-encompassing cost of this procedure. Thus, longer hospital stays in the high-income population are also reflected in correlational higher hospital charge. Other factors that have been shown to increase length of hospital stay include prior cardiac procedures, such as coronary artery bypass and valve surgery, as well as significant comorbid factors that are taken into consideration when determining LVAD recipient eligibility. 20
In 2013, the Centers for Medicare and Medicaid Services published strict criteria for destination therapy LVAD eligibility. Several risk assessment tools have been developed to predict postoperative complications and mortality and to determine which patients are qualified to receive these therapeutic devices. 15 Most studies have focused on patient populations of men >60 years with ischemic cardiomyopathy. 22 The tremendous impact of patient selection on the outcomes of LVAD implantation has long been recognized. Patients are classified as “high risk” for this intervention if they have any form of liver or renal dysfunction, hematological and coagulation abnormalities, or lower serum albumin levels. 22 As demonstrated in the aforementioned study, many of these high-risk patients crossover with those in the high-income group. Our study shows that compared with lower socioeconomic status individuals, high-income patients are more likely to experience ischemic strokes, acute kidney injury, bleeding abnormalities, and to undergo extracorporeal membrane oxygenation. We also found that higher-income patients have a higher post-LVAD all-cause inpatient mortality (unadjusted and adjusted for comorbidities). Prior studies show that important determinants of in-hospital mortality include poor nutrition, hematological abnormalities, markers of end-organ, or right ventricular dysfunction, and lack of inotropic support. 22 Although difficult to assess the primary cause of mortality in our study due to the nature of the NIS database, we did find a higher proportion of post-operative complications as detailed in Table 2. Taking into consideration all of the above-mentioned factors and in line with the REMATCH trial, there are significant benefits associated with the long-term use of LVAD devices for end-stage heart failure. 26 As we continue to elucidate the benefits of these devices and incorporate them into routine practice, it is imperative to find the balance between survival benefit and risk of surgery when discussing the appropriate timing for LVAD implantation.
Strengths and limitations
Utilization of the NIS provides us with an opportunity to analyze a large number of LVAD patients, from hundreds of nationwide centers, across a 7-year timeframe (weighted estimate of 25,503 LVAD implants). However, as NIS represents hospitalizations and not individual patients, there is a possibility that patients undergoing pump exchanges may feature more than once in the data set. Our analyses are also limited by a lack of longitudinal follow-up and are valid for a short-term period (~10–70 days as suggested by mean ± standard deviation LOS). The inability of NIS to define the proportion of individuals eligible for LVAD implantation despite income, as opposed to the proportion who ultimately undergo LVAD implantation, is important. Lastly, with the NIS, we are unable to assess echocardiographic findings that might affect the eligibility or feasibility of LVAD, laboratories data which is critical for patients undergoing LVAD and the severity of advanced heart failure assessed by INTERMACS score of patients undergoing LVAD implantation. Prospective studies of income differences in patients with advanced heart failure are needed to confirm whether such differences may exist.
Conclusion
Health inequities based on socioeconomic status have long contributed to disparities in cardiac care and treatment strategies. Although patients with low-income were found to have higher comorbidities, they were found to have lower complications and inpatient mortality post-LVAD implantation. Improving our understanding of the impact of socioeconomic factors on patient eligibility, health literacy and pursuit of treatment, and outcomes of LVAD intervention is incredibly important as health care providers continue to integrate and evolve this therapeutic technique into routine practice.
Supplemental Material
sj-pdf-1-jao-10.1177_03913988211056960 – Supplemental material for Comparison of household income in in-hospital outcomes after implantation of left ventricular assist device
Supplemental material, sj-pdf-1-jao-10.1177_03913988211056960 for Comparison of household income in in-hospital outcomes after implantation of left ventricular assist device by Bertrand Ebner, Morgan Karetnick, Jelani Grant, Louis Vincent, Jennifer Maning, Neal Olarte, Odunayo Olorunfemi, Colombo Rosario and Sandra Chaparro in The International Journal of Artificial Organs
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.