
Abstract
Percutaneous endoscopic gastrostomy (PEG) tube placement in adults who are already established on peritoneal dialysis (PD) remains challenging due to the limited experience and data in this area which lacks clear guidance. Given the fact that peritoneal dialysis is one of the relative contraindications for PEG tube insertion, and PEG tube on its own is a risk for peritonitis, how to overcome these obstacles and utilize the advantage of PEG tube for feeding malnourished PD patients remains uncertain. Here we report our unique successful experience of treating three adult peritoneal dialysis patients in whom the PEG tube was inserted successfully with no complications. To the best of our knowledge, this is the first successful case series in the literature for treating adult prevalent PD patients by PEG tube placement.
Keywords
Introduction
Percutaneous endoscopic gastrostomy (PEG) tube is the placement of a feeding tube into the stomach percutaneously guided by endoscopy for patients who require long-term enteral nutrition. Prior to the 1980s, permanent feeding tube placement was limited to an open surgical procedure until Gauderer et al. 1 described the safe placement of percutaneous endoscopic gastrostomy (PEG) tubes. This procedure has since expanded beyond the realm of surgeons to include gastroenterologists, thoracic surgeons and interventional radiologists. Several risk factors have been shown to contribute to protein and energy malnutrition (PEM), such as inadequate protein intake due to anorexia and decrease in appetite, inadequate dialysis, infections, inflammations, acidosis and insulin resistance, in addition to dialysate protein loss during peritoneal dialysis (PD). 2 Up to 40% of PD patients develop (PEM). 2 There is ample evidence that strongly correlates (PEM) and inflammation to high cardiovascular morbidity and mortality rate in the dialysis population. In order to mitigate (PEM) in PD, several strategies have been advocated with little progress, and the actual protein intake is frequently below the recommended amount of 1.2 g/kg body weight. The average 24-h-protein and amino acid (AA) loss during peritoneal dialysis is ranging from (5–15 g) to (2–4 g) respectively. 3 The AA dialysate-based solutions were designed to compensate for low dietary protein intake in PD patients, but there is no consensus in the literature about its clinical benefit. 3 In addition, AA dialysate-based solutions can induce metabolic acidosis and raise serum urea levels, precipitating (PEM). Until this moment, AA based dialysate solutions did not gain much popularity in PD. It is of utmost importance that the administration of AA based solutions is accompanied by simultaneous calories intake. This is because amino acid enhances protein synthesis, and the oral calories inhibit protein degradation, therefore boost the positive effects of the AA based solutions on protein balance. 3 If a patient develops feeding difficulties for any reason, percutaneous endoscopic gastrostomy (PEG) tube feeding may be the optimal option to ensure adequate nutrition; knowing that protein malnutrition is a significant contributory factor to the high mortality rate in the PD population. However, studies on the effectiveness of PEG tube feeding in PD patients are limited to the paediatric age group, and some of them are controversial, whether PEG tube or open gastrostomy (OG) should be performed. Here we report our unique successful single-centre experience of treating three PD patients who developed (PEM) secondary to difficulty in oral feeding through PEG tube placement by an intervention radiologist without complications. To the best of our knowledge, this is the first successful case series in the literature for treating prevalent PD patients by PEG tube.
Case 1
A 68-year-old Saudi female with a background history of type 2 diabetes mellitus, dyslipidaemia, bipolar disorder, old stroke with residual weakness, atrial fibrillation and end-stage renal disease (ESRD) on PD for 9 years was admitted on the 15th of March 2020 with urosepsis, impaired level of consciousness and poor oral intake. A nasogastric tube (NGT) was inserted for feeding since admission, and multiple attempts to wean her from the NGT have failed. Feeding options have been discussed with the family, and the decision was made to go with PEG tube insertion as it was the best option in her situation. On the 21st of June 2020, a 10 French gastrotomy tube was placed by a skilled intervention radiologist and its position was confirmed by contrast injection Figure 1. One day prior to the procedure, the PD was withheld in an attempt to keep the abdomen dry, and the patient continued to be off PD for 3 days post-op. During this period, the patient was vitally and clinically stable with acceptable metabolic parameters. Additionally, she was covered with daily prophylactic antibiotics (Ceftriaxone 1 g IP and Vancomycin 1 g IP) and fluconazole 150 mg IV, which was started from the day of the procedure and continued for 3 weeks. PD was resumed on day 4 post-op with a lower fill volume of 1 L and it was gradually increased till we reached 1.9 L over 4 weeks with no leak or other complications. Feeding was introduced through the PEG tube on day 4 post-op at a rate of 10 mL/h in a semi-sitting position and increased gradually till 40 m/h with no complications. The patient developed a PEG exit site infection growing Pseudomonas aeruginosa and was treated effectively with local gentamycin, and repeated cultures were negative. Multiple PD fluid analysis and cultures were done after the PEG tube insertion which were reported negative as well. On week 16, the patient developed a massive myocardial infarction and she succumbed due to her illness 2 weeks after Intensive Care Unit (ICU) admission.
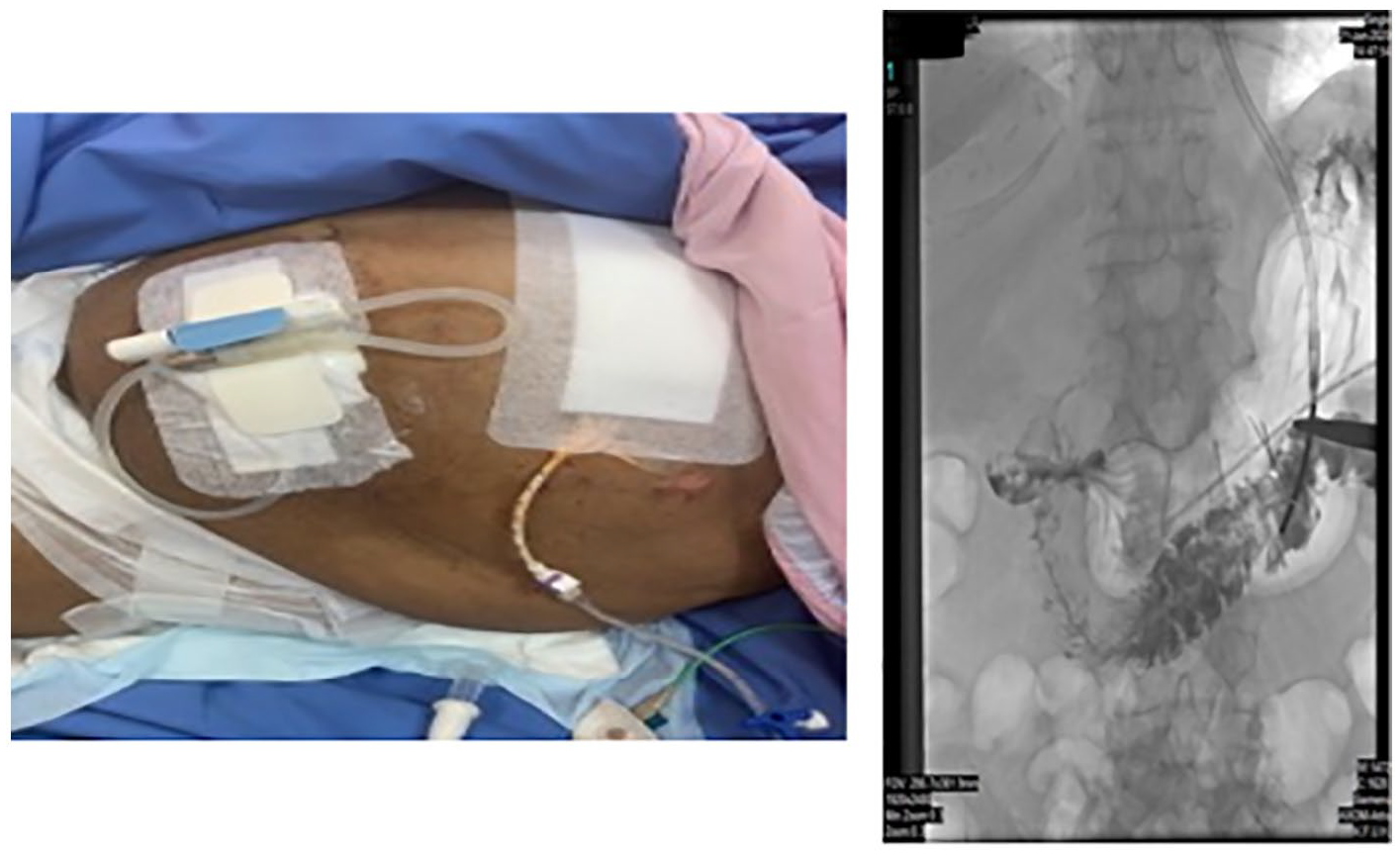
Depicts both peritoneal catheter and PEG tube.
Case 2
An 80-year-old male known to have diabetes mellitus, hypertension, multiple old strokes with residual slurred speech and right-sided weakness, ESRD on Assisted PD (APD) since 2017 was admitted with confusion, decrease level of consciousness with a vegetative state. He was started on an NGT feeding, but with no signs of improvement and after the discussion with his family, the decision for gastrostomy tube insertion was made. A 12 French Pig tube was inserted successfully, APD was withheld for 3 days post-insertion, and all the previous precautions mentioned in our first case have been undertaken in this patient as well, including the gradual introduction of feeding with the escalation of dialysis prescription. The patient was followed by the dietitian on a daily basis, and he was tolerating the feed with no complications. The PD was smooth and uneventful for 10 weeks. However, the patient’s condition deteriorated as he developed hospital-acquired pneumonia and succumbed due to his illness.
Case 3
An 88-year-old female with ESRD on APD for 6 months was admitted with acute haemorrhagic stroke associated with a decrease in her level of consciousness, and accordingly, an NGT was inserted for feeding. Multiple attempts to wean her from the NGT have failed, and a PEG tube was inserted uneventfully without complications, similar to the previous two cases. However, she developed urosepsis, and she died 8 weeks after PET tube insertion Figure 2.
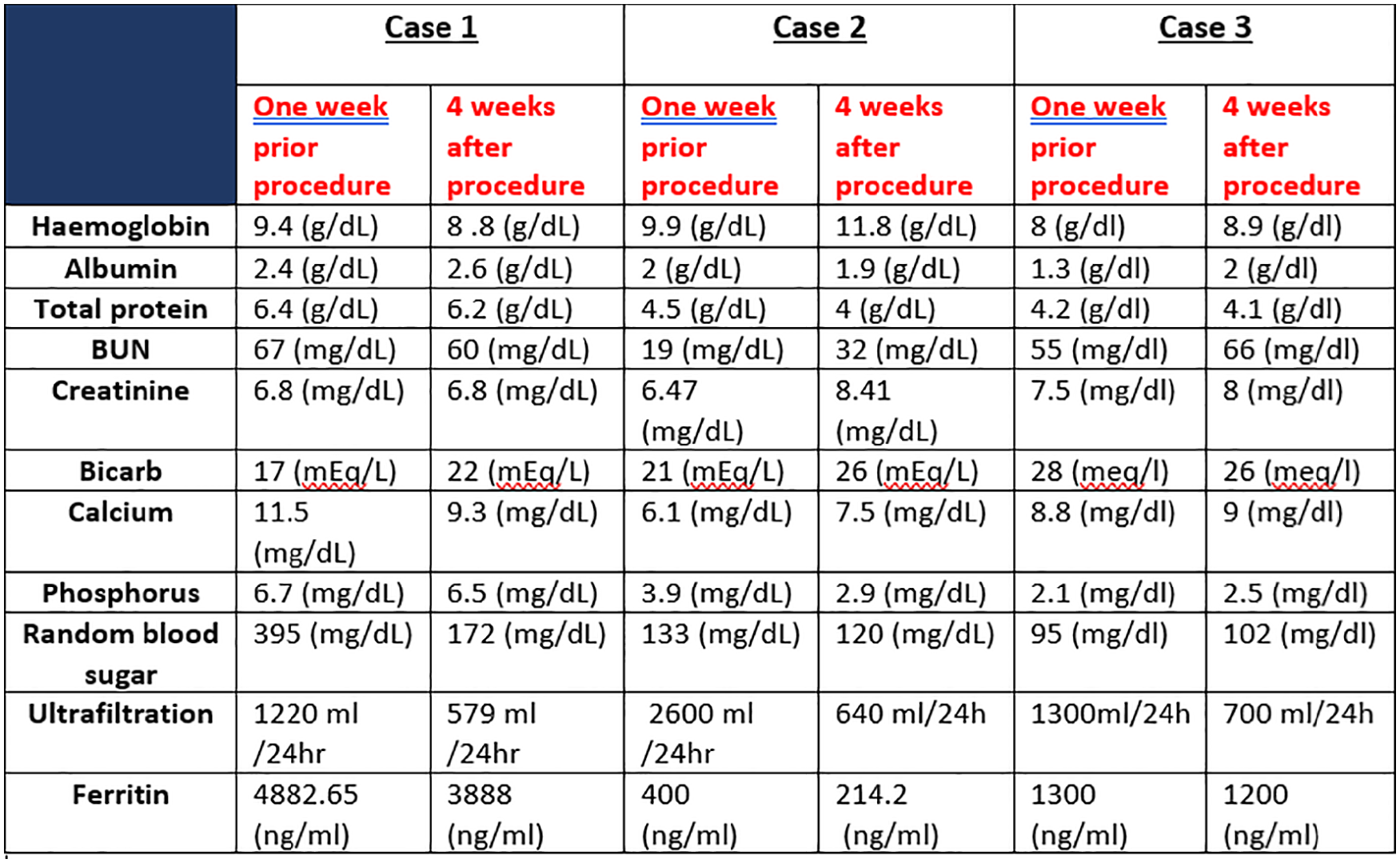
Metabolic parameters before and after PEG tube insertion.
Discussion
Malnutrition is a common condition in the peritoneal dialysis population. If a patient develops feeding difficulties for any reason, a PEG feeding tube may be the optimal option to ensure adequate nutrition, acknowledging that protein malnutrition is an important contributory factor to the increased mortality rate in (PD) patients. However, studies on the effectiveness of PEG feeding in PD patients are limited to the paediatric population, and some of them are controversial; whether PEG or open gastrostomy (OG) should be performed. Since Fein et al. 4 have published the dreadful complications of 10 adults PD patients who had undergone PEG tube placement after PD initiation in 2001, a few cases had been published since then and the majority of them were on the paediatric population, which suggested that the insertion of peritoneal dialysis catheters in patients who have a pre-existent and presumably well-healed PEG may be safe. However, the insertion of gastrostomy tubes in patients receiving peritoneal dialysis is associated with major adverse outcomes, including leaks and fatal or nonfatal peritonitis. Moreover, there seems to be reluctance in re-implementing the procedure, especially in centres with previous undesirable experiences, contributing to the limited experience in PEG insertion after PD initiation. 2 In 2006, Warady 5 had raised an important question: why there is limited data on using PEG on adult patients with ESRD on PD? He attributed this uncertainty to lack of competency and experience of health care providers, fears from dreadful complications, mainly fungal peritonitis, dialysate leakage and patient/family-related issues. Cessation of PD and shifting patients to haemodialysis (HD) has been advocated to decrease the risk of peritonitis: however, even after PD cessation for up to 6–8 weeks, peritonitis and its associated complications can occur. 4 Dahlan et al. have reported that withholding peritoneal dialysis, switching to haemodialysis, and using prophylactic antimicrobials did not prevent the development of fatal peritonitis. They hypothesized that residual peritoneal fluid might prevent effective healing of the PEG site with subsequent spillage of gastric contents into the peritoneal space. It is uncertain whether surgical as opposed to endoscopic placement with a longer healing time would have resulted in a better outcome. Thus, they concluded that gastrostomy tubes should not be placed in adult patients on peritoneal dialysis due to the very high rate of fatal peritonitis. 6 Von Schnakenburg et al. have reported a success rate of 67% in 27 paediatric patients who had undergone PEG insertion after PD catheter placement. Peritonitis rates and fungal peritonitis were 37% and 26% respectively and all patients received intraperitoneal prophylactic antibiotic and intravenous fungal treatment. PD was held for 2–3 days after PD catheter placement with no difference in peritonitis rates pre or post catheter insertion. 2 In our patients, in addition to the coverage with prophylactic antibiotics and antifungal treatment for 2 weeks post catheter insertion, we have attempted inserting the PEG tube on a dry peritoneum after holding the PD for 24 h, allowing a proper time for the PEG site to heal by further holding PD for 72 h. The PEG tube was also inserted by a skilled intervention radiologist using a minimally invasive procedure with a small gauge tube. PD was then resumed at a lower fill volume which was increased gradually. Feeding through the PEG tube was introduced gradually in a semi-sitting position to minimize the spillage of gastric contents into the peritoneal space. We think that all these factors have contributed to our successful experience and helped tremendously prevent peritonitis.
In conclusion, we believe that ‘PEG before PD’ is somehow more acceptable than ‘PD before PEG’ in terms of complications and outcomes. Nevertheless, as physicians, we face a diversity of cases in a way that each case represents a unique medical, technical or social aspect, and sometimes we do not have the luxury of options. Although the procedure represents an extreme practice in terms of preparation and continuous adjustment in feeding and PD prescription, it is always good to know that we have alternatives. According to the timing that had been framed by in previous studies we consider our timing of insertion of PEG as late procedure (after 7 days). If PEG placement was initiated earlier does it change the prognosis, this needs to be explored in future studies.7,8
We hope that these cases will be the source of inspiration and encouragement to our colleagues to report more cases on adult PD patients requiring PEG tube insertion for feeding and consider such a procedure as a viable option to manage malnourished adult PD patients.
Footnotes
Acknowledgements
The authors are pleased to express their great gratitude and appreciation to the ICU staff and peritoneal dialysis nurses at King Fahad University Hospital in Al Khobar for their valuable support during the patient hospitalization.
Author contributions
Dr. Hend, Dr. Lamees and Dr. Moaz were responsible for collecting the cases and drafting the case presentation. Dr. Amani, Dr. Ibraheem and Dr. Reema performed the literature review and drafted the discussion. Prof. Alhwiesh, Dr. Lamees, Prof. Ibraheem and Dr. Khadija contributed to writing and reviewing the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval was obtained from Imam Abdulrahman bin Faisal University Review Board of Medical Center, and all written consents were taken from the patients.