
Abstract
Background:
Despite recent advances in management of patients with advanced heart failure, mortality remains high. Aim of this study was to compare impact of different aetiology of ischaemic and idiopathic cardiomyopathy on early outcomes and long-term survival of patients after left ventricular assist device implantation.
Methods:
European Registry for Patients with Mechanical Circulatory Support (EUROMACS) gathers clinical data and follow-up parameters of LVAD recipients. Patients enrolled in the EUROMACS registry with primary diagnosis of either ischaemic (n = 1190) or idiopathic (n = 812) cardiomyopathy were included. Primary Endpoints were early mortality as well as long-term survival. Secondary endpoint were major postoperative adverse events, such as need for rethoracotomy. Additionally, a propensity-score matching analysis was performed for patients with ischaemic (n = 509) and idiopathic (n = 509) cardiomyopathy.
Results:
In terms of basic demographics and baseline parameters the two groups significantly differed as expected before propensity-score matching due to different aetiology of cardiomyopathy. Seven-day (52 (4.4%) versus 18 (2.2%); p = 0.009), 30-day (153 (12.9%) versus 73 (9.0%); p = 0.008) and in-hospital mortality (253 (19.7%) versus 123 (15.1%); p = 0.009) were significantly lower in the idiopathic cardiomyopathy group compared to the ischaemic cardiomyopathy group, whereas after propensity-score matching 30-day (p = 0.169) was comparable and in-hospital mortality (p = 0.051) was almost significant. Kaplan-Meier survival analysis revealed no significant difference in regard of long-term survival after propensity-score matching (Breslow-test p = 0.161 and LogRank-test p = 0.113).
Conclusion:
Though patients with ischaemic and idiopathic cardiomyopathy suffer from different cardiomyopathy aetiologies, 30-day-mortality and long-term survival of both groups were similar leading to the conclusion that covariates predominately influence mortality and survival of ischaemic and idiopathic cardiomyopathies.
Introduction
Although mortality of heart failure is declining due to improved therapies, the prevalence of cardiomyopathy continues to increase.1,2 Causes for cardiomyopathy are most prevalently of ischaemic or idiopathic nature. 3 The effect of heart failure aetiology on outcomes after LVAD implantation has not been fully investigated. 3 Especially, coronary artery heart diseases cause ischaemic cardiomyopathies, which can be reversible after revascularization.2,4 In contrast to ischaemic cardiomyopathies, in up to 50% of cases the exact cause remains initially unknown, which is specified as idiopathic cardiomyopathy.1,5 Contemporary therapeutic options have led to a substantial improvement in survival of patients with heart failure.6,7
Mechanical circulatory support is an established therapy for end-stage heart failure.7,8 The European Registry for Patients with Mechanical Circulatory Support (EUROMACS), accumulates clinical data related to durable mechanical circulatory.9–11 Thereby improvement of LVAD therapy could be achieved.10,12
The aim of this study was to analyse the impact of different heart failure aetiologies on early clinical outcomes and on long-term survival of LVAD patients suffering from ischaemic and idiopathic cardiomyopathy.
Methods
Data collection and patient population
EUROMACS gathers clinical data and follow-up parameters of LVAD recipients.10,13,14 Enrolled patients with primary diagnosis of either ischaemic (n = 1190) or idiopathic (n = 812) cardiomyopathy were included. The participation of the University Hospital Cologne (Department of Cardiothoracic Surgery) in EUROMACS was approved by the institutional ethical review board and the already participating centres. Participation of patients in EUROMACS is obtained by written informed consent of patients. Moreover, conception and plan of the presented study was sanctioned by the EUROMACS scientific advisory council. The investigation complies with the Declaration of Helsinki.
Due to the multilayered and therefore long-lasting process of analysing large databases time period between 2011 and 2014 was chosen. Patients were prospectively enrolled into the EUROMACS online database collecting anonymised data of demographics and perioperative variables of those with need of an assist device. Preimplantation data regarding patient characteristics are recorded. All types of devices (pulsatile and continuous flow, axial and centrifugal, primary and secondary implants) were included. The definition of adverse events in EUROMACS corresponds to the INTERMACS definition.11,15 Data acquisition has been described elsewhere in detail. 16 Due to several reasons some patients have been excluded as presented in the consort diagram (Figure 1). At the present time more than 50 European and non-European centres in 15 countries are involved. 17 The consort of the study was to analyse the impact of different aetiologies of cardiomyopathy (ischaemic and idiopathic) on early outcomes and long-term survival. Primary Endpoints were early mortality including 30-day and in-hospital mortality as well as long-term survival. Secondary endpoints were major postoperative adverse events, such as need for rethoracotomy. The cohort was divided in patients either suffering from ischaemic cardiomyopathy (n = 1190) or from idiopathic cardiomyopathy (n = 812). In order to better analyse these heterogenous groups and to determine independent factors influencing development of cardiomyopathy, a propensity-score matching analysis was performed. Matching variables were age, gender and INTERMACS classification I-II with 509 patients suffering from either ischaemic or idiopathic cardiomyopathy.
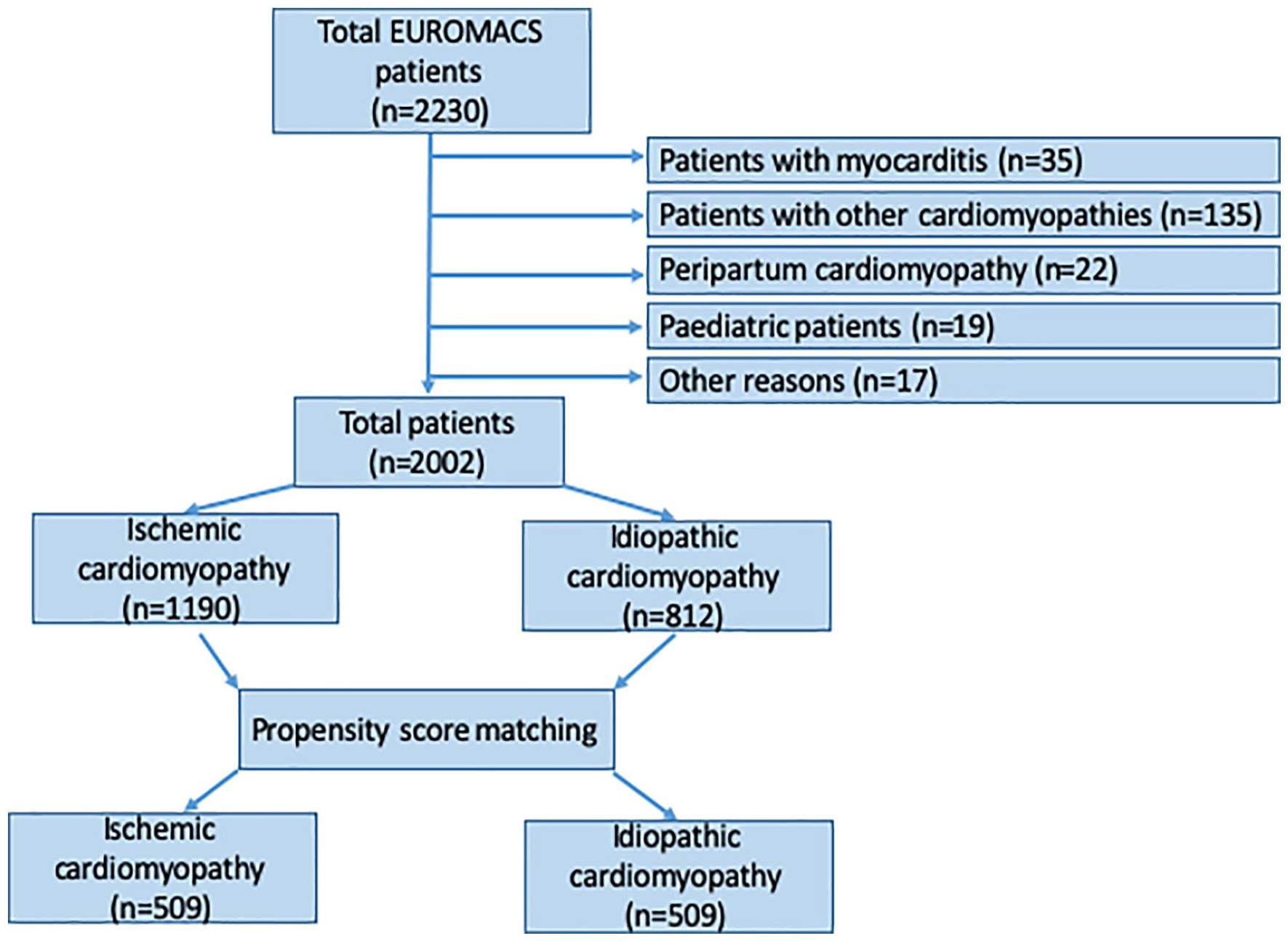
Consort diagram of LVAD patients suffering from ischaemic and idiopathic cardiomyopathy.
Statistical analysis
Statistical analysis was performed using Statistical Package for Social Sciences, version 24.0 (SPSS Inc., Chicago, Illinois). All data were presented as continuous or categorical variables. Categorical data were expressed as total numbers and percentages. Continuous data were expressed as median (interquartile range).
Statistical differences were analysed either with Students’-T or Mann-Whitney U test for normally or non-normally distributed continuous variables, respectively. Pearson Chi-test was used for crosstabulation statistics of categorial variables. In case of small sample sizes (⩽5) Fisher’s exact test was applied instead.
Kaplan-Meier survival estimation was performed for long-term analysis. Propensity-score matching function of SPSS software was conducted to reduce confounding bias between the groups. A propensity-score for each patient was estimated using a logistic regression model with preoperative characteristics that showed statistically significant differences between the two groups as independent variables. Matching was based on one-to-one nearest neighbour matching method with a tolerance level on the maximum propensity-score distance (callipers of width 0.2 standard deviations of the logit of the propensity-score). This propensity-score-based matching procedure resulted in a number of pairs that were well matched for baseline characteristics. Matching variables were age, gender and INTERMACS classification I-II. A p-value <0.05 was considered significant for all statistical methods. The statistical analyses were performed with SPSS 24 (IBM, Armonk, NY, USA).
Results
Overall analysis of ischaemic cardiomyopathy (ISC) and idiopathic cardiomyopathy (IDC) patients
Median age differed significantly between the groups (57.9 ± 9.1 years ISC vs 51.5 ± 13.0 IDC, p < 0.001). Moreover, ischaemic and idiopathic cardiomyopathy were more frequent in men than in women (Table 1). Preoperative cardiac index was also significantly different (2.1 ± 0.7 L/min/m² ISC vs 1.9 ± 0.7 L/min/m² IDC; p < 0.001). An ejection fraction lower than 20% was significantly more frequent in IDC than in ISC (580 (53.8%) ISC versus 455 (60.8%) IDC; p = 0.003). In contrast, a higher amount of ISC patients were admitted in INTERMACS class I-II (p = 0.040).
Baseline parameters on admission.
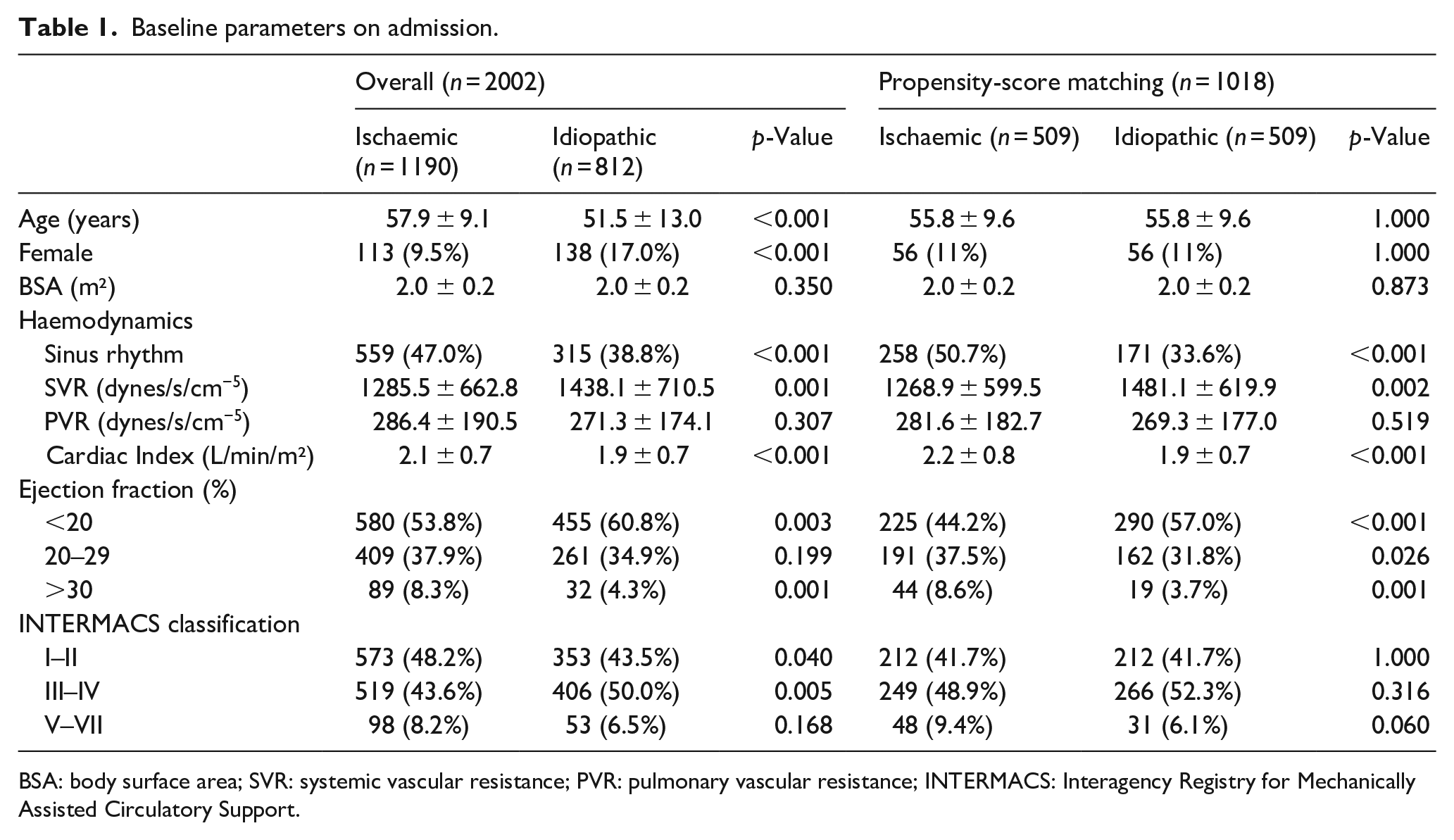
BSA: body surface area; SVR: systemic vascular resistance; PVR: pulmonary vascular resistance; INTERMACS: Interagency Registry for Mechanically Assisted Circulatory Support.
Previous myocardial infarction due to coronary vessel disease (p < 0.001), peripheral vascular disease (p < 0.001), cerebral vascular disease (p = 0.022), renal failure requiring dialysis (p = 0.030), diabetes (p < 0.001), chronic obstructive pulmonary disease (p < 0.001) and previous cardiac surgery (p < 0.001) was more present in ISC patients (Table 2).
Comorbidities on admission.
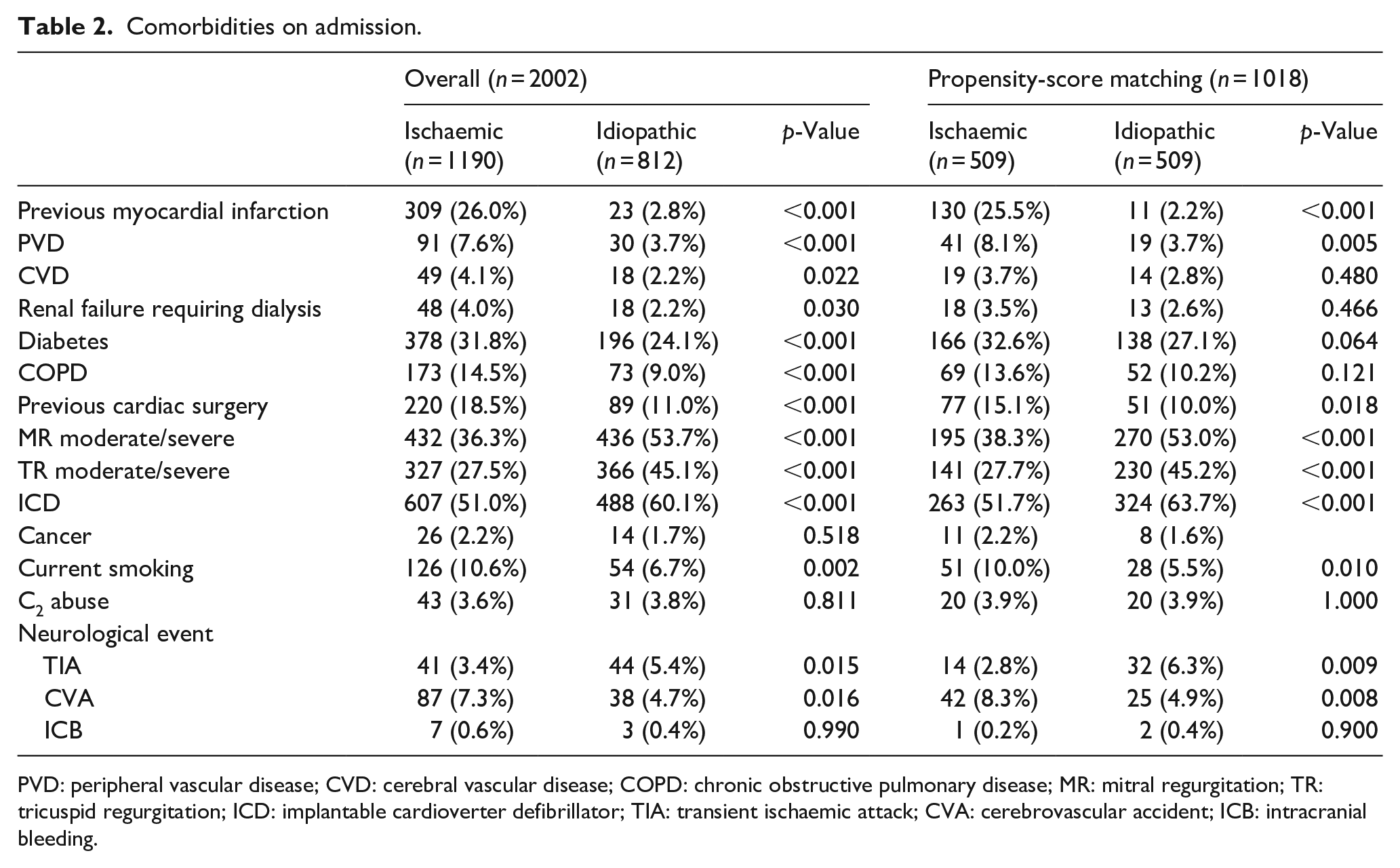
PVD: peripheral vascular disease; CVD: cerebral vascular disease; COPD: chronic obstructive pulmonary disease; MR: mitral regurgitation; TR: tricuspid regurgitation; ICD: implantable cardioverter defibrillator; TIA: transient ischaemic attack; CVA: cerebrovascular accident; ICB: intracranial bleeding.
IDC patients presented significantly more moderate/severe atrioventricular valve insufficiency in comparison to ISC patients (mitral regurgitation: 432 (36.3%) ISC versus 436 (53.7%) IDC; p < 0.001; tricuspid regurgitation: 327 (27.5%) ISC versus 366 (45.1%) IDC; p < 0.001) (Table 2).
Preoperative laboratory parameters are shown in Table 3. Blood urea nitrogen was significantly higher in ISC patients (p < 0.001). In addition, serum creatinine was higher in ISC patients (130.2 ± 70.4 mg/dl ISC vs 122.8 ± 63.4 mg/dl; p = 0.032). Hepatic parameter showed higher increase in IDC patients, except for glutamyl oxaloacetic transaminase (GOT) (p = 0.255).
Preoperative laboratory parameters.
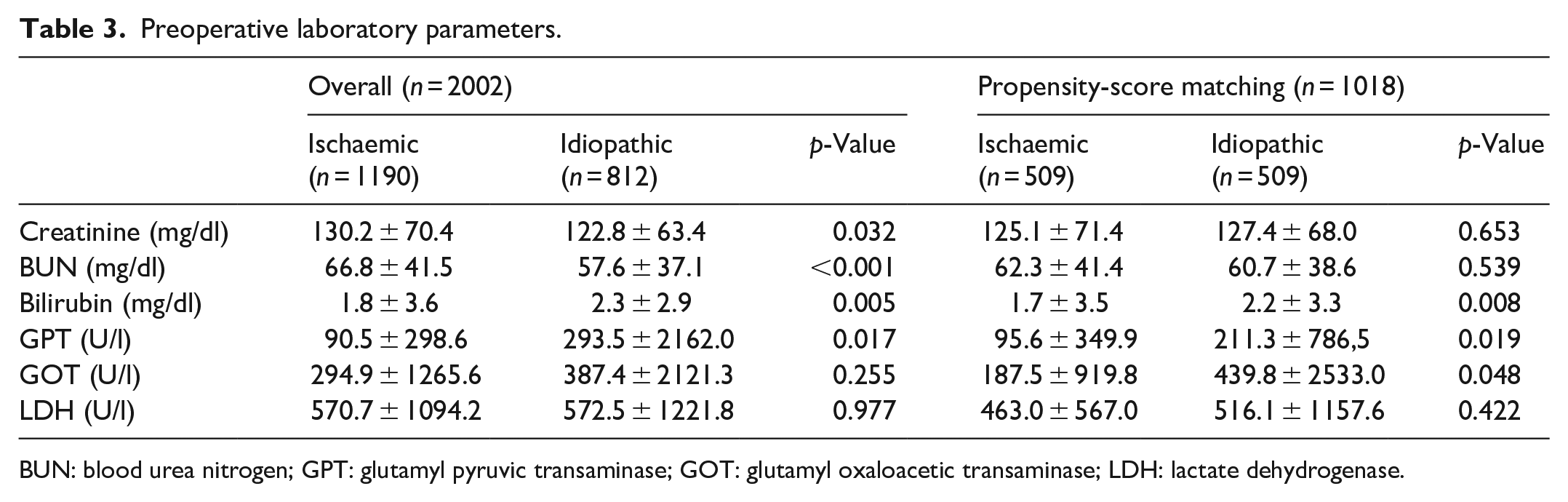
BUN: blood urea nitrogen; GPT: glutamyl pyruvic transaminase; GOT: glutamyl oxaloacetic transaminase; LDH: lactate dehydrogenase.
Outcomes after LVAD implantation are summarised in Table 4. ISC patients were significantly longer intubated (238 h ISC vs 181 h IDC; p = 0.003), leading to a longer stay on intensive care unit (22 days ISC vs 19 days IDC; p = 0.001). Re-thoracotomy for bleeding (p = 0.029) and device related complications (p = 0.003) occurred more often in ISC patients.
Outcomes after LVAD implantation.
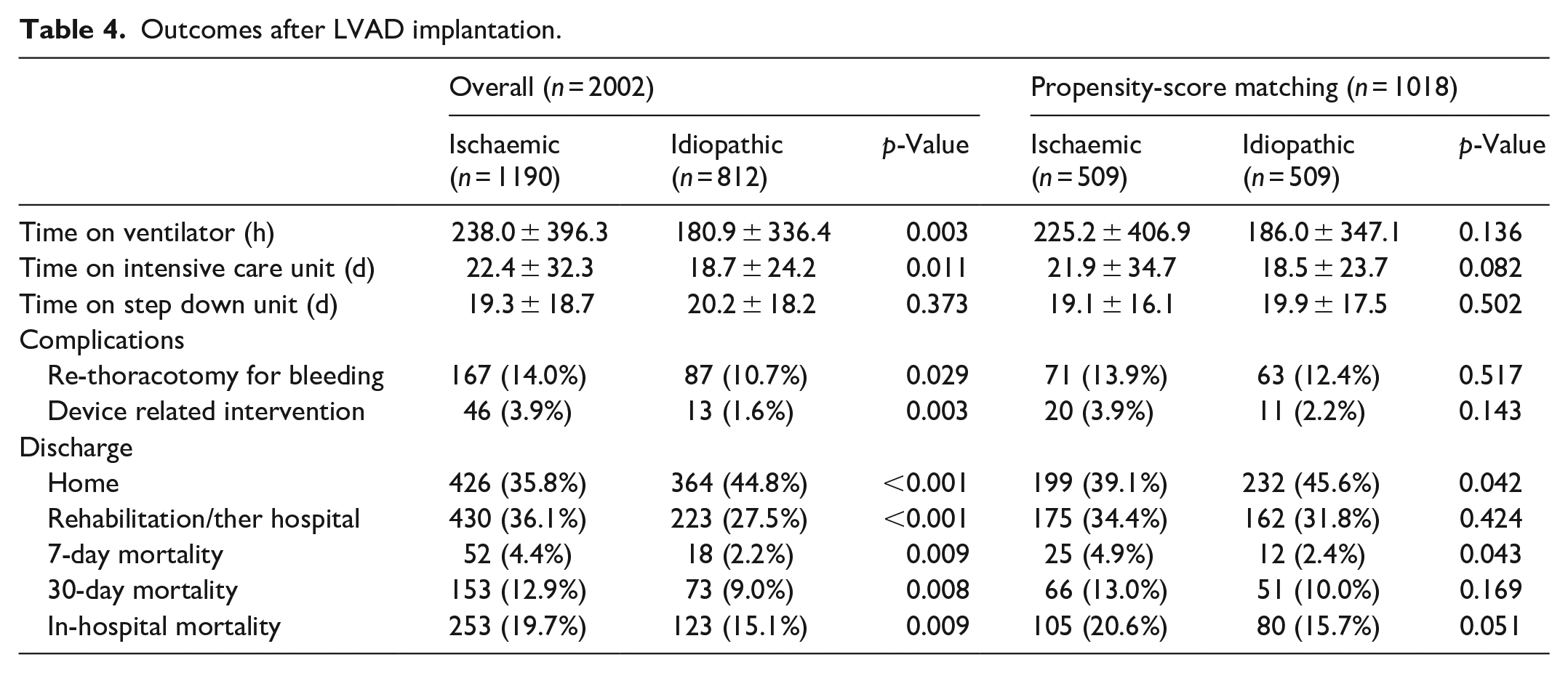
Seven-day (52 (4.4%) ISC vs 18 (2.2%) IDC; p = 0.009), 30-day (153 (12.9%) ISC vs 73 (9.0%); p = 0.008) and in-hospital mortality (253 (19.7%) ISC vs 123 (15.1%) IDC; p = 0.009) were significantly higher in ISC patients. As presented in Kaplan-Meier survival analysis (Figure 2), survival between patients suffering from ischaemic and idiopathic cardiomyopathy also significantly differed.
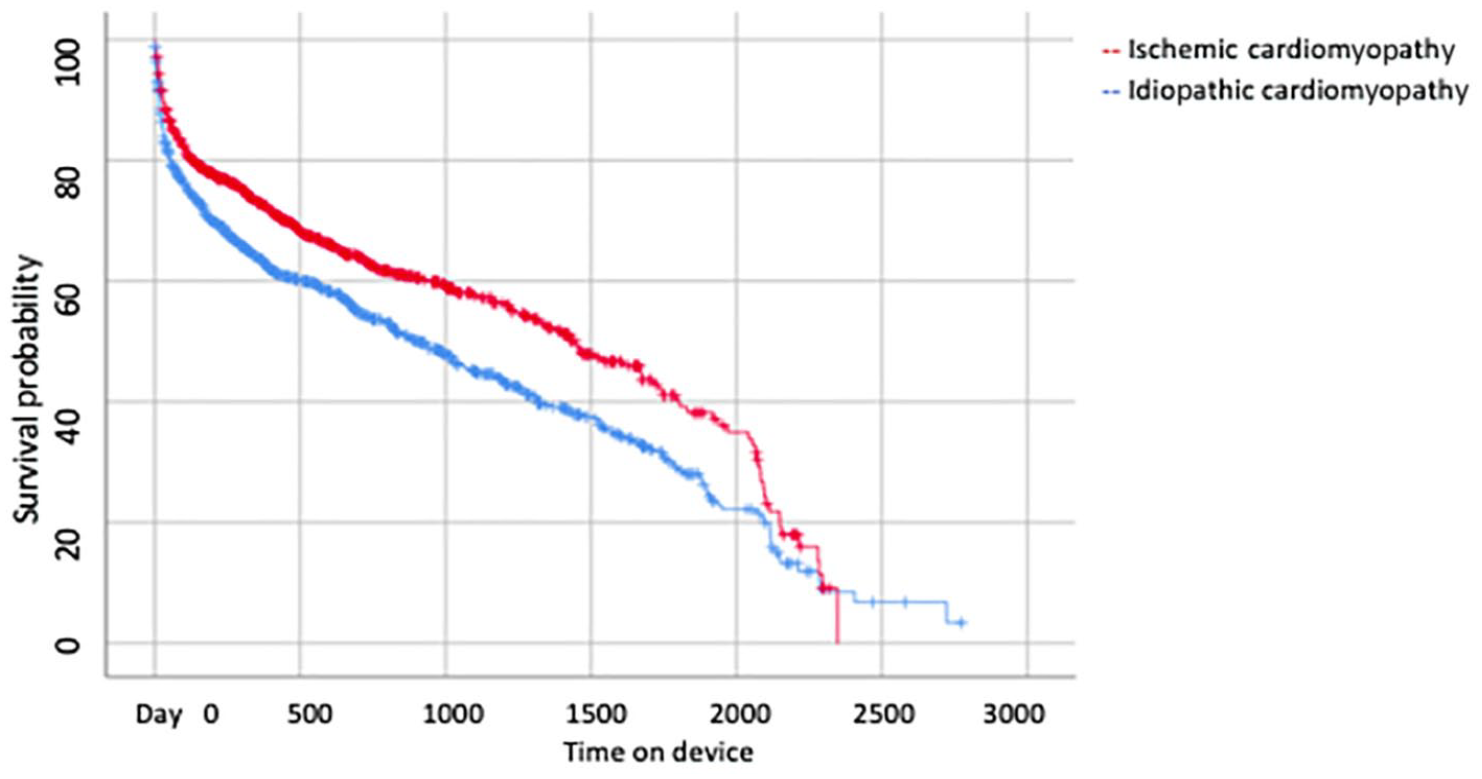
Kaplan-Meier survival analysis before propensity-score matching of patients with ischaemic versus idiopathic cardiomyopathy.
Comparative analysis after propensity-score matching
Propensity-matching was performed in regard of age, gender, body surface area and INTERMACS class I–II. 1018 patients were divided either into ischaemic (n = 509) or idiopathic (n = 509) group after matching. Overall, ISC patients suffered in general more co-morbidities (Table 2). Propensity-scoring showed no significant differences in terms of time on ventilator (p = 0.136), time on intensive care (p = 0.082) and step-down unit (p = 0.502). Moreover, distribution of postoperative complications was similar in both groups. After matching, discharge to rehabilitation or other hospital after LVAD implantation showed no differences (175 (34.4%) in ischaemic group vs 162 (31.8%); p = 0.424). Additionally 30-day was similar in both groups (p = 0.169), whereas variable in-hospital mortality was almost significant (p = 0.051).
Long-term survival for ISC and IDC patients after LVAD implantation
In Kaplan-Meier estimation for long term-survival of almost 7 years both groups differed significantly (Breslow-test p < 0.001 and LogRank-test p < 0.001) (Figure 2). After matching, survival rates were similar (Breslow-test p = 0.161 and LogRank-test p = 0.113) (Figure 3).
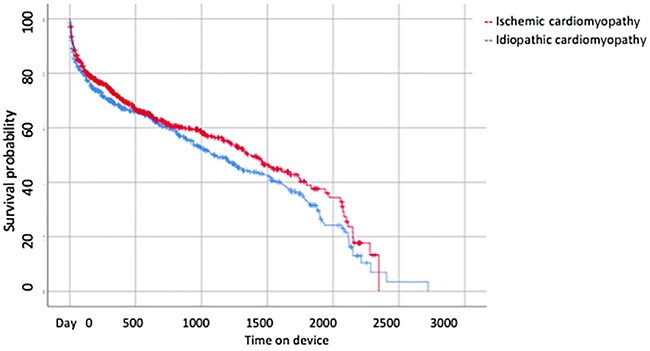
Kaplan-Meier survival analysis after propensity-score matching of patients with ischaemic versus idiopathic cardiomyopathy.
Discussion
The present study comparatively analysed the impact of different cardiomyopathy aetiologies on early outcomes and long-term survival of LVAD patients. Ischaemic and idiopathic cardiomyopathy are known as the most common indications for heart transplantation or assist device implantation. 18 Therefore, they are of importance to deal with. Our analysis showed that 30-day mortality and long-term survival were comparable of LVAD-patients suffering from ischaemic and idiopathic cardiomyopathy after propensity-score matching.
As known, patients with ischaemic cardiomyopathy are generally older and sicker than patients suffering from idiopathy cardiomyopathy.3,19 In our study the entire cohort was sicker and in worse clinical condition than idiopathic cardiomyopathy patients at time of referral to hospital. The reason of this was the different aetiology in development of cardiomyopathy. 20 Patients with ischaemic cardiomyopathy patients often suffer from an acute myocardial event, diabetes or peripheral vascular disease, whereas idiopathic cardiomyopathy patients show a more chronical history in development of cardiomyopathy.21–25 Before propensity-score matching, groups significantly differed in terms of perioperative variables and postoperative outcomes as expected. Homogenisation of both groups using propensity-score matching made it possible to harmonise the two groups and to determine factors which were independent of the underlying disease. Thus confounding bias could be reduced. Also, Potapov et al. 26 employed propensity-score matching to reduce heterogeneity between groups in order receive more reliable outcome results.
Outcomes of the entire cohort with patients with ischaemic cardiomyopathy revealed significantly higher early and long-term mortality compared to patients with idiopathic cardiomyopathy, whereas after propensity-score matching 30-day mortality and long-term survival between groups were interestingly comparable.
The mechanisms behind these differences are complex and appear to result from manifold reasons than simply decreased cardiac output. 23 According to our propensity-score results we assume that especially covariates affect mortality and incidence of complications which accompany the patients with ischaemic and idiopathic cardiomyopathy than ischaemic and idiopathic cardiomyopathy themselves.27,28
After LVAD implantation development of right ventricular failure is one of the most feared complications.29,30 Prediction of this clinical situation in LVAD patients is still an enigma. 28 Løgstrup et al. 29 stated that patients with non-ischaemic heart failure revealed an increased incidence of postoperative right heart failure. However, due to different aetiology of ischaemic and idiopathic cardiomyopathy preoperative prediction of preoperative right ventricular failure remains difficult. Recently, Rivas-Lasarte et al. 30 tried to establish a EUROMACS right-sided heart failure risk score. Nonetheless the results indicate that further evaluation and optimisation of the score is necessary. 31
In our entire cohort in-hospital mortality was significantly higher in ischaemic cardiomyopathy patients compared to non-ischaemic cardiomyopathy patients Lourenco et al. 21 corroborated our results. Interestingly after propensity-score matching the difference between both groups decreased and was ‘almost’ significant indicating that using propensity-score matching analysis reduces confounding factors.
Furthermore, in our study patients suffering from ischaemic cardiomyopathy were significantly older than patients suffering from idiopathic cardiomyopathy. In order to avoid age-related bias on outcomes, variable age was a matching variable for our propensity-score analysis. Shore et al. 23 showed that age significantly differed between groups, whereas a Fennira et al. did not find any differences in terms of age.
Moreover, as gender also influences pathophysiology of cardiomyopathy variable gender was made to a propensity-score matching variable in order to reduce gender-related bias. As Divoky et al. 32 and Löchel et al. 33 have already presented, the nuances of gender-specific differences are wide-spread in terms of device indication, implantation and postoperative therapy. In our study more women suffered from idiopathic than from ischaemic cardiomyopathy.
Limitations
Our findings should be interpreted in the light of several limitations. Small sample size precludes generalisations. Also, data quality of a large registry relies on the data input of the participating centres. Another limitation is the observational origin of the data, so our results may be confounded by indication.
Therefore, possibility exists that not all adverse events were reported. Furthermore, the very nature of a registry allows no analyses on centre-specific trends and complications for each device brand.
Conclusion
Patients with ischaemic cardiomyopathy revealed significantly higher early and long-term mortality compared to patients with idiopathic cardiomyopathy, whereas after propensity-score matching long-term survival was similar leading to the conclusion that covariates significantly influence mortality and survival.
Footnotes
Acknowledgements
We are grateful to those colleagues and data managers participating in EUROMACS and who submitted the data to the Registry.
Authors’ note
This paper was presented at the 35th EACTS annual meeting in Barcelona on 13th October 2021.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded and supported by European Association for Cardio-Thoracic Surgery (EACTS).