
Abstract
Objectives:
Left ventricular assist device (LVAD) implantation has become a reliable therapeutic strategy in patients with advanced heart failure. C-reactive protein (CRP) is a well-established biomarker of inflammation. This study aims to determine the prognostic effect of CRP level on clinical outcomes of patients who undergo LVAD implantation.
Methods:
This is a single-center, observational, retrospective study. One hundred fifty-three patients who received continuous-flow LVAD implantation were included and were divided into two groups of high (>3.9 mg/dL) versus low CRP (⩽3.9 mg/dL).
Results:
Patients with high pre-implant CRP levels were prone to severe preoperative clinical conditions and complicated intraoperative procedures. Compared with patients in the low CRP group, elevated pre-implant CRP was associated with increased hospital mortality (31.4% vs 8.4%, p < 0.001), postoperative right ventricular failure (47.1% vs 30.1%, p = 0.031), right ventricular assist device use (34.3% vs 16.9%, p = 0.013), AKI (70% vs 51.8%, p = 0.022) and significantly prolonged duration of postoperative mechanical ventilation and intensive care unit length of stay. Univariate Cox regression showed that high pre-implant CRP was significantly associated with increased risk of long-term mortality (Hazard ratio (HR) 2.632 95%; CI: 1.657–4.183, p < 0.001), and multivariable Cox regression also revealed the higher risk of long-term mortality in patients with elevated pre-implant CRP (HR, 2.848 95%CI: 1.659–4.888, p < 0.001). These results remained stable when treating pre-implant CRP as a continuous variable. Besides, the prognostic effect of post-implant CRP was also observed.
Conclusions:
CRP is a reliable risk-stratification biomarker in patients receiving continuous-flow -LVAD and can be used as a predictor for short- and long-term outcomes.
Introduction
Heart failure (HF) is a growing global health problem and has become a leading cause of morbidity and mortality in patients with cardiovascular disorders. The prevalence of HF is 1% to 2% in the adult population 1 and increases strikingly in older people, with an estimated prevalence of 11.8% in people aged 60 years or older. 2 For patients with advanced HF, heart transplantation and left ventricular assist device (LVAD) implantation have been proposed as the definitive therapy regarding the reduction of mortality and improving quality of life (QoL).3,4 With the severe shortage of donors’ hearts and great improvements of devices, LVAD rapidly becomes an increasing alternative therapy to heart transplantation. 5
C-reactive protein (CRP), as a sensitive marker of both acute and chronic inflammation, could rise robustly and rapidly in response to tissue damage and inflammation. CRP level is routinely monitored in hospitalized patients to assess the severity of initial illness and efficacy of therapeutic interventions. 6 Elevated CRP is recognized as an independent marker and predictor of cardiovascular diseases in the healthy population and an increased risk of cardiovascular events in patients with cardiovascular disease (CVD).6–8 Elevated pre-implant CRP levels are also associated with increased postoperative complications, hospital length of stay (HLOS), all-cause death, and long-term mortality in patients after various cardiovascular interventions.9–12 Besides, in patients with HF, high CRP levels correlate with more severe symptoms and are independently associated with increased mortality and morbidity. 13
A recent study demonstrated that pre-implant CRP could predict postoperative complications and mortality in patients with LVAD support. 14 However, the effect of CRP on perioperative outcomes and postoperative complications is lacking. Therefore, we sought to determine the effect of CRP on perioperative outcomes, postoperative complications, and long-term mortality in patients after continuous-flow LVAD implantation.
Materials and methods
Study population
The Institutional Review Committee approved this single-institution, observational, retrospective cohort study, and written patient consent was waived. Consecutive adult patients who underwent continuous-flow LVAD implantation (HeartMate II, HeartWare, and HeartMate 3) between January 2009 and February 2020 were evaluated for inclusion.
Data collection
Preoperative variables, operative variables, main etiology of heart failure (ischemic cardiomyopathy (ICM), dilatative cardiomyopathy (DCM), and others), and follow-up data were collected retrospectively. Patients’ comorbidities, previous cardiac surgery, and laboratory examinations were extracted from the clinical information system. Quantitative measurement of (non-high-sensitivity) plasma CRP levels before the operation was routinely performed. CRP levels less than the sensitivity threshold of 0.5 mg/dL were regarded as normal, and these values were recorded as a value half of the detection threshold when CRP was analyzed as a continuous variable.
Definitions of outcomes
Perioperative outcomes included the duration of cardiopulmonary bypass, the incidence of concurrent right ventricular assist device (RVAD) implantation, operation time, and aortic clamp time. Postoperative right ventricular failure (RVF) was diagnosed if post-implant inotropes, inhaled nitric oxide, or intravenous vasodilators were administered continuously beyond 1 week after LVAD implantation or if the implantation of a RVAD was required. AKI was determined according to the Kidney Disease Improving Global Outcomes (KDIGO) criteria based on changes in serum creatine. 15 Survival data were obtained from our single-center LVAD follow-up database, and the endpoint was defined as death. Other outcomes include hospital mortality, RVAD use, new-onset renal replacement therapy (RRT), postoperative duration of RVAD support, postoperative duration of mechanical ventilation (MV) time, postoperative intensive care unit length of stay, and postoperative HLOS were extracted from the clinical information system.
Statistical analysis
The cut-off value for pre-implant and post-implant CRPs was determined by maximizing sensitivity plus specificity from a time-dependent receiver operating characteristic (ROC) curve analysis from censored data with a nearest neighbor estimation methods, and this calculation was performed in R software (version 4.0.2) with the survivalROC package (Version 1.0.3, Heagerty and Saha-Chaudhuri). 16 Continuous variables were expressed as mean ± standard deviation (SD) for normally distributed data or median with interquartile range (IQR) for non-normal distributed data, and independent t-test or Mann-Whitney U tests were used for the comparison between the subgroups. Categorical variables were compared with chi-square or Fisher’s exact test when appropriate. ROC curves were used to evaluate the predictive accuracy of pre-implant CRP. Kaplan–Meier curves with 95% confidence intervals (CI) were used, and the difference between the two groups was compared by log-rank test. Besides, a multivariable Cox regression was performed to estimate the adjusted hazard ratios (HRs) for post-LVAD mortality by incorporating potential predictors identified from univariate Cox regression (inclusion criteria of two-tailed p < 0.05). Besides, the effect of CRP at post-implant 7 days on long-term survival was also investigated by Kaplan–Meier curves and univariate Cox regression. All statistical analyses were performed using SPSS Statistics 26.0 (IBM, Armonk, NY, USA).
Results
Study population
177 adult patients were evaluated for inclusion, and patients who received two LVAD as durable BiVAD support (n = 2), LVAD revisions because of LVAD thrombus or LVAD dysfunction (n = 8), oHTx before LVAD (n = 1), and patients with no pre-implant CRP data (n = 13) were excluded. Finally, a total of 153 patients were included for the final analysis and divided into two groups in terms of high (>3.9 mg/dL) vs low CRP (⩽3.9 mg/dL), according to the cutoff canulated from time-dependent ROC analysis.
Baseline characteristics
The median CRP level of the overall 153 patients was 3.3 mg/dL ([IQR] 1.25 mg/dL to 7.9 mg/dL). The distributions of CRP and log-transformed CRP values are shown in Figure 1, and the baseline characteristic and pre-implant variables are presented in Table 1. Patients with high pre-implant CRP were likely to belong to Intermacs I–II levels. They also had higher prevalences of acute myocardial infarct, hyperuricemia, cardiac arrest, prior coronary artery bypass grafting (CABG), mechanical circulation support, and lower prevalences of dyslipidemia and prior ICD implantation. The laboratory results are summarized in Supplemental Table S1. High pre-implant CRP was associated with increased alanine aminotransferase, lactate dehydrogenase, white blood cells, and reduced red blood cells, hemoglobin, hematocrit, and platelets. The intraoperative variables and outcomes are summarized in Table 2. Compared with patients in the low CRP group, patients with high pre-implant CRP were more likely to undergo median sternotomy for LVAD implantation and extracorporeal membrane oxygenation for extracorporeal life support.
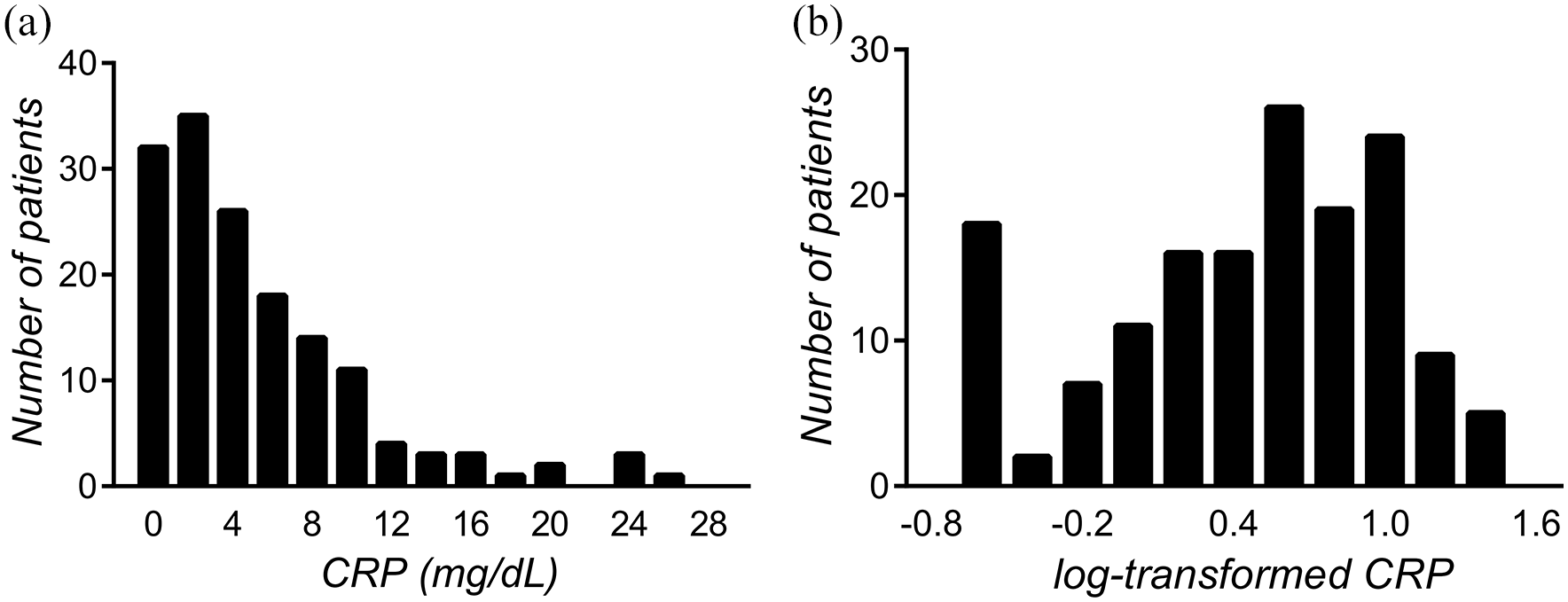
The distributions of CRP (a) and log-transformed CRP values (b).
Baseline characteristics between the high and low pre-implant CRP in patients after continuous-flow LVAD.
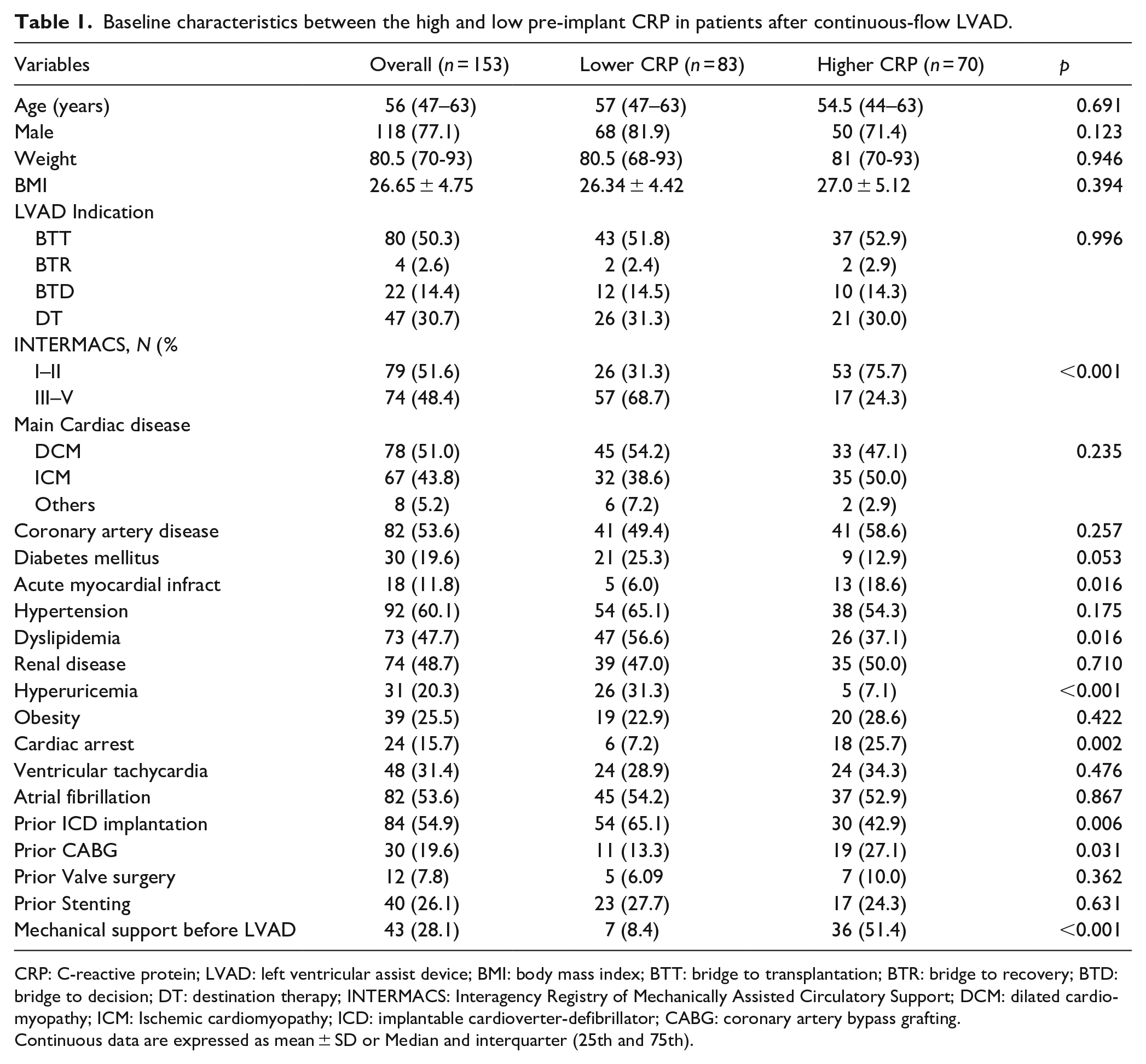
CRP: C-reactive protein; LVAD: left ventricular assist device; BMI: body mass index; BTT: bridge to transplantation; BTR: bridge to recovery; BTD: bridge to decision; DT: destination therapy; INTERMACS: Interagency Registry of Mechanically Assisted Circulatory Support; DCM: dilated cardiomyopathy; ICM: Ischemic cardiomyopathy; ICD: implantable cardioverter-defibrillator; CABG: coronary artery bypass grafting.
Continuous data are expressed as mean ± SD or Median and interquarter (25th and 75th).
Peri-operative characteristics and outcomes between high and low pre-implant CRP groups in patients after continuous flow-LVAD.
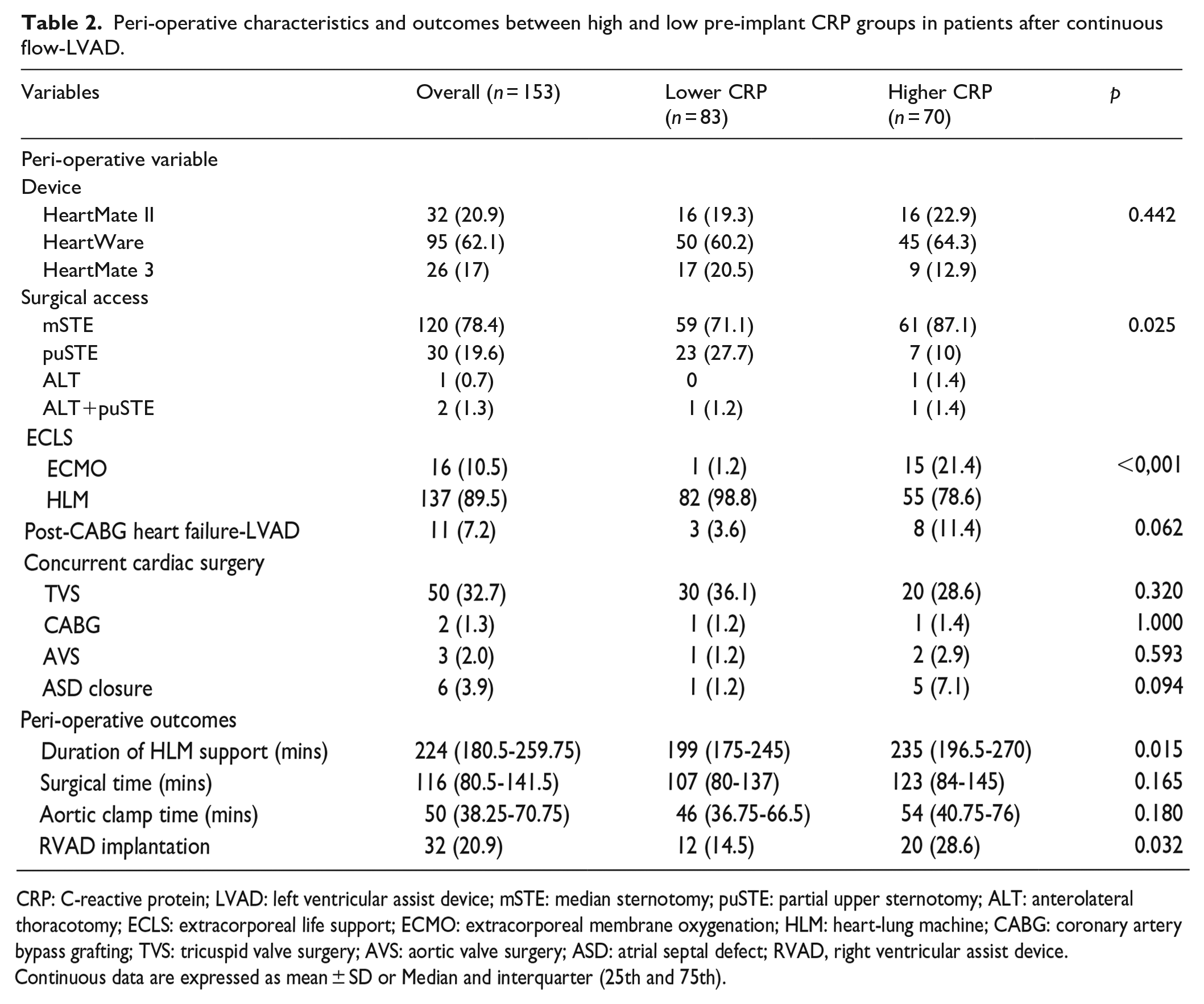
CRP: C-reactive protein; LVAD: left ventricular assist device; mSTE: median sternotomy; puSTE: partial upper sternotomy; ALT: anterolateral thoracotomy; ECLS: extracorporeal life support; ECMO: extracorporeal membrane oxygenation; HLM: heart-lung machine; CABG: coronary artery bypass grafting; TVS: tricuspid valve surgery; AVS: aortic valve surgery; ASD: atrial septal defect; RVAD, right ventricular assist device.
Continuous data are expressed as mean ± SD or Median and interquarter (25th and 75th).
Association of pre-implant CRP with perioperative outcomes
As shown in Table 2, high pre-implant CRP was correlated with a significantly longer duration of cardiopulmonary bypass [235 (196.5–270) vs 199 (175–245), p = 0.015] and increased incidence of concurrent RVAD implantation (28.6% vs 14.5%, p = 0.032). No difference in operation time and aortic clamp time was observed.
Association of pre-implant CRP with postoperative outcomes
Table 3 shows postoperative outcomes. Patients with high pre-implant CRP had significantly increased hospital mortality (31.4% vs 8.4%, p < 0.001) and incidences of postoperative RVF (47.1% vs 30.1%, p = 0.031), RVAD implantation (34.3% vs 16.9%, p = 0.013), and postoperative AKI (70% vs 51.8%, p = 0.022) compared to patients in the low CRP group. ROC curves showed that pre-implant CRP could accurately predict hospital mortality, RVAD implantation, and postoperative AKI, with AUCs of 0.688, 0.623, and 0.623, respectively (Figure 2). Besides, a high pre-implant CRP level was associated with remarkably prolonged postoperative duration of MV and postoperative intensive care unit (ICU) length of stay, and the results remained stable when only including patients who were successfully discharged. No significant differences were detected between groups regarding the incidence of new-onset RRT, re-ICU admission, re-admission within 30 days, duration of RVAD support, and postoperative HLOS.
Postoperative outcomes between the high and low pre-implant CRP groups in patients after continuous-flow LVAD.
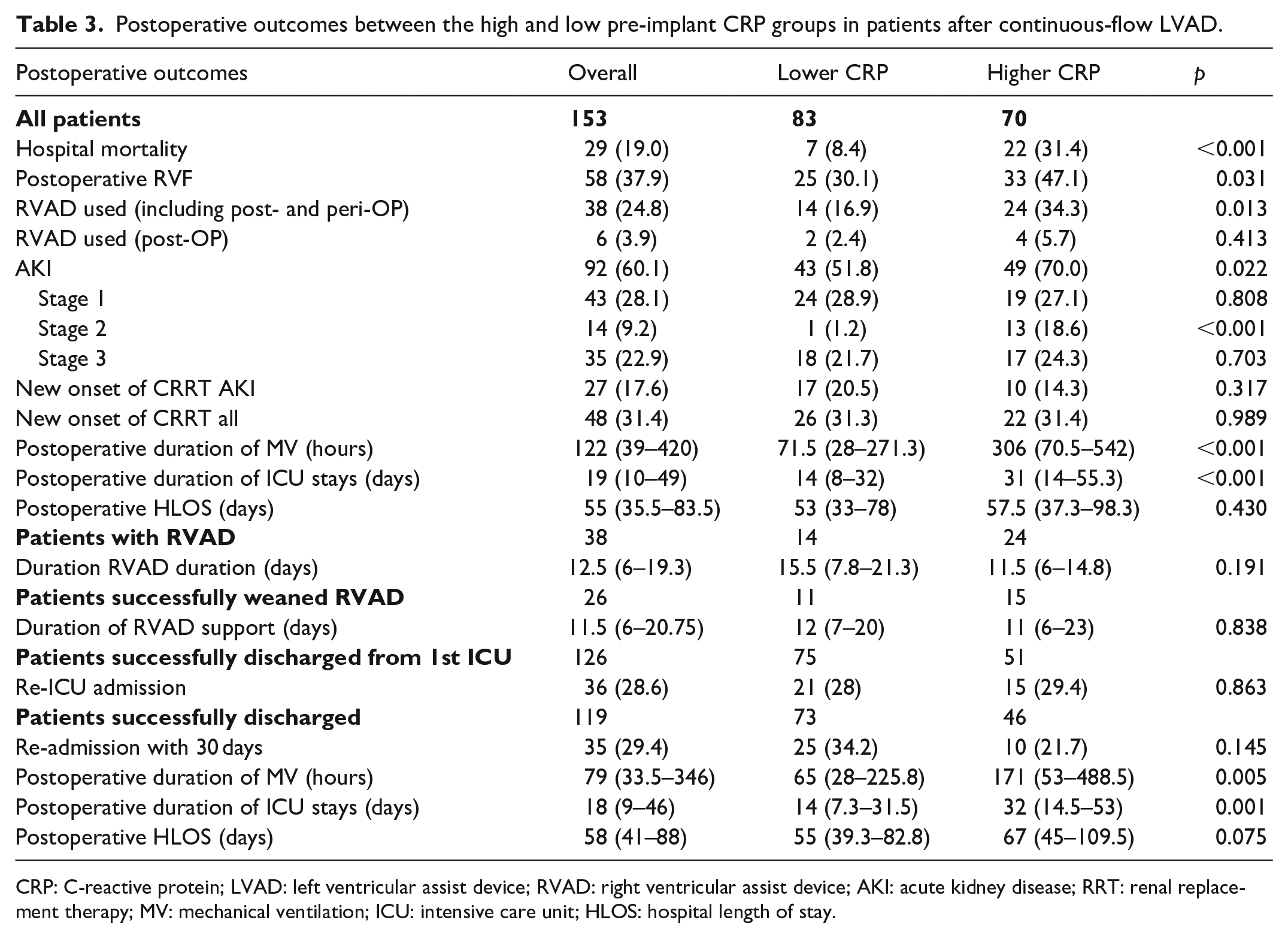
CRP: C-reactive protein; LVAD: left ventricular assist device; RVAD: right ventricular assist device; AKI: acute kidney disease; RRT: renal replacement therapy; MV: mechanical ventilation; ICU: intensive care unit; HLOS: hospital length of stay.
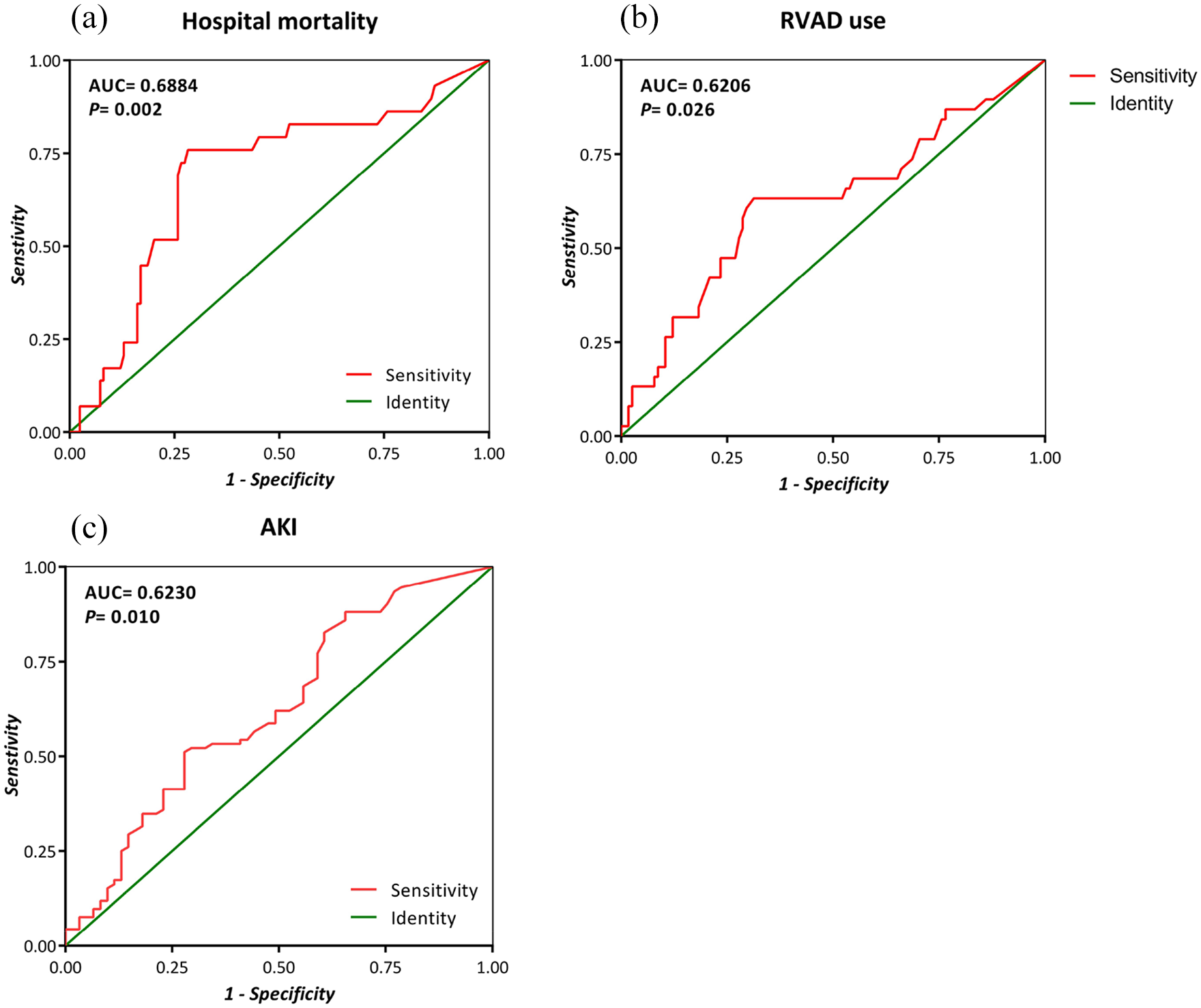
ROC curves for pre-implant CRP to predict (a) hospital mortality, (b) RVAD use, and (c) AKI in patients after CF-LVAD.
Association of pre-implant CRP with long-term mortality
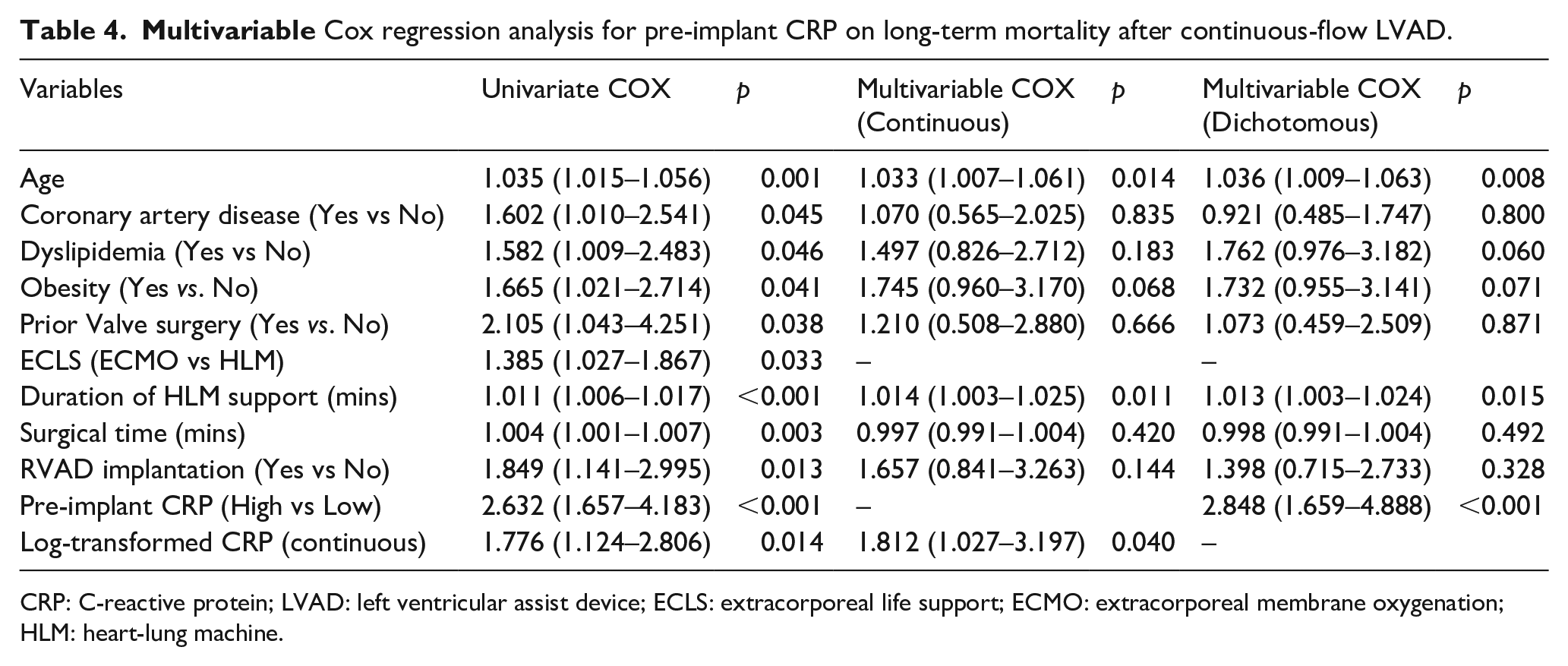
During a median follow-up of 1401 days (IQR 1092 days to 1709 days), 77 died on LVAD, 30 received heart transplantations. Four patients were weaned from LVADs, two were lost to follow-up, and 40 were still alive with LVAD support. Kaplan–Meier survival analysis showed that patients with a high pre-implant CRP had lower survival than patients with low pre-implant CRP (Figure 3, Log-rank p < 0.001). As shown in Table 4, univariate Cox regression shows that high pre-implant CRP was significantly associated with increased risk of long-term mortality (HR 2.632 95%CI: 1.657 to 4.183, p < 0.001). In patients with high baseline CRP, the multivariable HR for long-term mortality was 2.848 (95%CI: 1.659-4.888, p < 0.001) by comparison of patients with low pre-implant CRP. Consistently, when CRP was defined as a continuous variable, the multivariable results also revealed that log-transformed pre-implant CRP correlated positively with mortality in patients after LVAD (HR 1.812 95%CI: 1.027-3.197, p = 0.040).
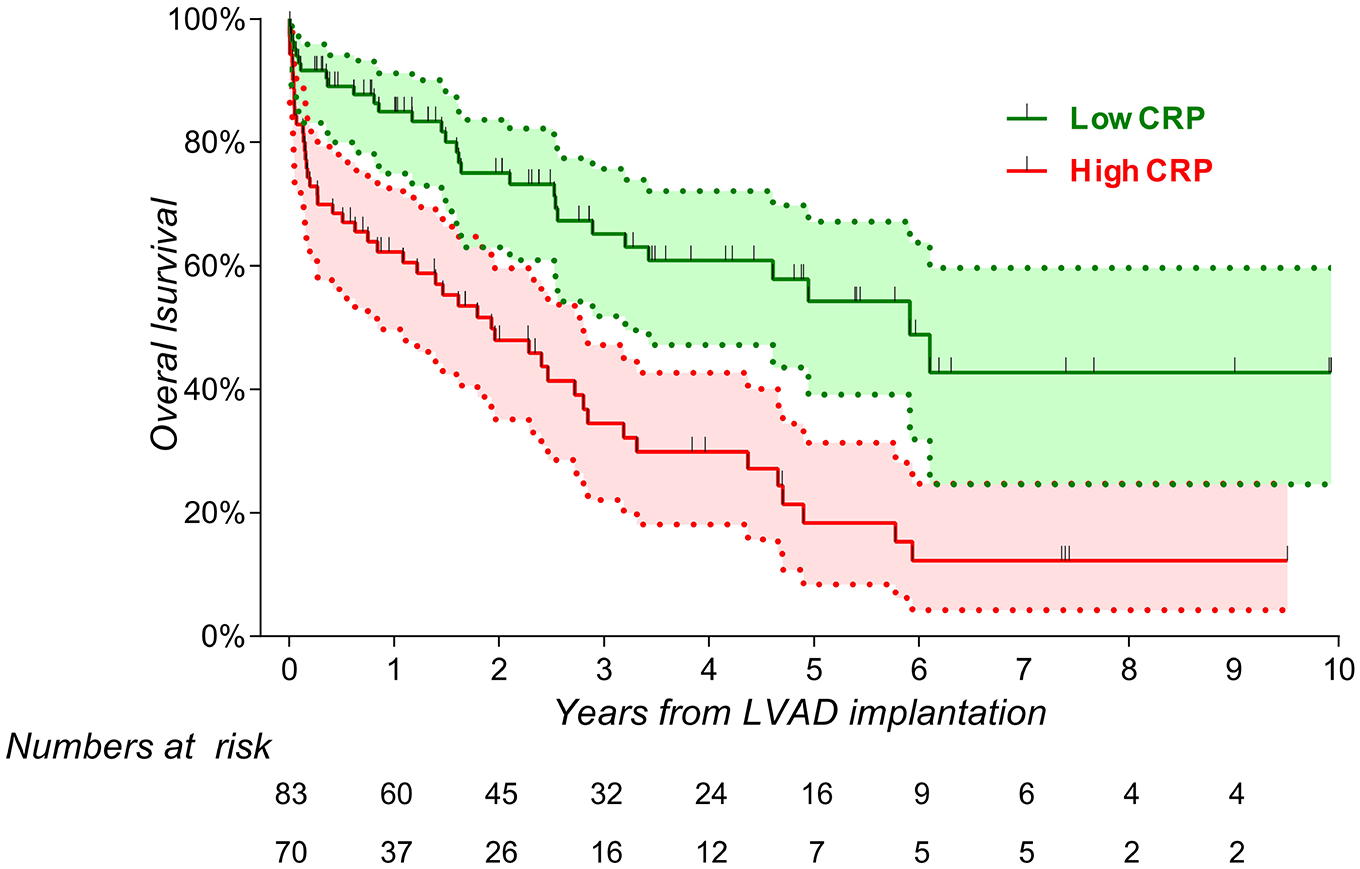
Kaplan–Meier survival curves for the high and low pre-implant CRP on long-term mortality.
CRP: C-reactive protein; LVAD: left ventricular assist device; ECLS: extracorporeal life support; ECMO: extracorporeal membrane oxygenation; HLM: heart-lung machine.
Association of post-implant CRP with long-term mortality
Supplemental Figure S1a shows the CRP change from pre-implant to 7 days after LVAD implantation, and there was a peak of post-implant CRP at 3 days after LVAD implantation (18.04 ± 8.37 mg/dL). Since the CRP level became relatively stable at 7 days after implantation, we further investigate the association of post-implant 7-day CRP with long-term mortality. A total of 143 patients were involved, and the cut-off value for post-implant CRP identified by using time-dependent ROC analysis was 13.3 mg/dL. As shown in Supplemental Figure S1b, patients with a high post-implant CRP (⩾13.3 mg/dL) had a poor survival compared to patients with a low post-implant CRP, with a log-rank p value of 0.015. Univariate Cox regression showed that high post-implant CRP was also associated with increased risk of long-term mortality (HR 1.788 95%CI: 1.111–2.878, p = 0.017).
Discussion
Our study showed that high CRP was associated with a more severe clinical condition before LVAD implantation, indicated by INTERMACS I-II level, higher MCS support, more comorbidities, and abnormal lab results. Secondly, elevated pre-implant CRP was associated with an increased incidence of RVAD implantation. In addition, elevated CRP was associated with increased risks of hospital mortality, postoperative RVF, RVAD use, AKI, and significantly prolonged duration of mechanical ventilation and ICU length of stay. Furthermore, high pre-implant and post-implant CRP was a significant independent predictor for long-term mortality. These findings suggest that pre-implant CRP is a good biomarker for identifying high-risk patients and predicting poor clinical outcomes.
Pulmonary hypertension and ventricular structural abnormality are important contributors to RVF. Previous studies showed that circulating CRP was independently associated with abnormal right ventricular structural changes 17 and poor clinical outcomes, especially in patients with pulmonary hypertension. 18 Our study also confirms that patients with elevated pre-implant CRP had a poor right ventricular function, as indicated by higher incidences of postoperative RVF and RVAD support use. Since heart and kidney communicate with one another through an intricate network to maintain hemodynamic stability and organ perfusion, AKI usually occurs in patients after cardiac surgery or with HF. In patients after LVAD implantation, the incidence of AKI was considerably high, with a range of 10% to 70%. Cosentino et al. 19 reported that high-sensitivity CRP (hs-CRP) was closely associated with AKI development and severity in acute myocardial infarction patients. A retrospective cohort study with 1656 patients undergoing CABG showed that pre-implant CRP is a predictor of postoperative AKI. 20 Another study conducted in non-cardiac surgical patients indicated that the pre-implant CRP levels were also significantly related to postoperative AKI. 21 Though plenty of evidence exists in various settings, including cardiac and non-cardiac surgeries, no previous study investigated the relationship between pre-implant CRP and postoperative AKI in a specific group of patients who received LVAD. Our study found that AKI occurred in 60.1% of patients undergoing continuous-flow LVAD and it was significantly related to high pre-implant CRP.
Consistent with findings of CRP in other settings,22–24 high pre-implant CRP was associated with increased hospital mortality in patients after LVAD. Besides, the current study indicated that both pre-implant and post-implant CRP is significant predictor of long-term mortality following LVAD implantation. With a longer-time analysis, we shared a similar finding to a previous study with 24 months follow-up. 14 Besides, the significantly prolonged duration of MV, ICU stay, and hospital stay identified in our study also evidenced the poor prognostic factor of pre-implant CRP. Moreover, we also found that high CRP at 7 days after LVAD implantation was also associated with an increased risk of long-term mortality. Taken together, our study reinforced the previous findings by adding more complications and a longer median follow-up of 46 months.
The mechanism between CRP and mortality as well as postoperative complications is still not clear. CRP is well acknowledged as an inflammatory biomarker, and its production is especially stimulated via an upstream proinflammatory cytokine-dependent hepatic biosynthesis. 25 Elevated CRP was usually seen in severely ill patients and considered as a biomarker for an active infection. The severe systematic inflammatory response in such patients is usually related to worse clinical outcomes. However, accumulating studies suggested that neither IL-6 nor CRP only indicated inflammation but were also mediators participating in different signal pathways. 26 Systemic inflammation participates in right ventricular structural changes independent of its effect on the left ventricle. 17 Though the potential mechanisms are still unclear, myocardial nitric oxide synthase-mediated negative inotropic effects of IL-6 might be involved. 27 Inflammation also plays a critical role among all those common causes for AKI. 28 It has been demonstrated that pre-implant CRP contributes to endothelial dysfunction and reduced response to renal vasodilators by promoting coagulation activity and inhibiting nitric oxide production.29,30 Other than inflammation, potential mechanisms of CRP on cardiac function and poor clinical outcomes in patients receiving LVAD need to be further clarified.
The results of our study support the use of CRP as a risk-stratification tool to select high-risk patients. Besides, the relationship between CRP level and postoperative complications such as RVF and AKI may help clinicians to evaluate the severity of patients and assist the decision-making process. Future multi-center, large sample-size studies with long-term follow-up regarding the medical and socio-economic effects of CRP-guided interventions may be helpful. Since hsCRP is more sensitive to be quantified with a low detect threshold, 31 it might act as a more valuable biomarker than CRP in the clinical risk-stratification and prognostic prediction model.
Several limitations exist in the present study. Firstly, our study is a single-center, retrospective cohort study, and the bias because of the study design limits to derive a causal relationship and may include some unidentified confounders. While our results are consistent with a recent large multi-center cohort study using registry data, our study strengthens and expands current evidence with more outcomes and longer follow-up. Secondly, the kinetics of CRP levels and their effect during the follow-up were not tracked. Given that the current study aims to investigate the predictive effect of CRP, the results show that CRP is sufficient to select high-risk patients and predict short and long-term outcomes. Thirdly, though a CRP cut-off of 3.9 mg/dL calculated from ROC analysis could predict poor outcomes in patients after LVAD, the appropriate cut-off remains uncertain and needs further exploration.
Conclusion
In summary, CRP is a comprehensive biomarker of severe clinical presentation before LVAD implantation and a predictor for postoperative complications and long-term mortality. These findings suggest that CRP should be integrated into patients’ risk stratification before LVAD implantation and the prognostic model after LVAD.
Supplemental Material
sj-pdf-1-jao-10.1177_03913988221088614 – Supplemental material for C-reactive protein predicts early clinical outcomes and long-term mortality after left ventricular assisted device
Supplemental material, sj-pdf-1-jao-10.1177_03913988221088614 for C-reactive protein predicts early clinical outcomes and long-term mortality after left ventricular assisted device by Hongtao Tie, Rui Shi, Henryk Welp, Sven Martens, Zhenhan Li, Jürgen Sindermann and Sabrina Martens in The International Journal of Artificial Organs
Supplemental Material
sj-tif-2-jao-10.1177_03913988221088614 – Supplemental material for C-reactive protein predicts early clinical outcomes and long-term mortality after left ventricular assisted device
Supplemental material, sj-tif-2-jao-10.1177_03913988221088614 for C-reactive protein predicts early clinical outcomes and long-term mortality after left ventricular assisted device by Hongtao Tie, Rui Shi, Henryk Welp, Sven Martens, Zhenhan Li, Jürgen Sindermann and Sabrina Martens in The International Journal of Artificial Organs
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.