
Abstract
The use of hemadsorption has been purposed to reduce cytokine levels during the reperfusion phase during donation after circulatory death (DCD) programs. This paper aims to describe a cases series of the inflammatory cytokine levels before and after hemadsorption during normothermic reperfusion in DCD donors of liver and kidneys. In this observational pilot paper, we describe 8 DCD donors of liver or kidneys in our center from the year 2018 to 2019. All DCD donor subjects had similar age, were younger than 60 years, without evident critical conditions, no liver or kidney dysfunction known, and they presented with poor neurological outcomes instrumentally and clinically documented. We observed in our patients an interesting reduction of IL-10 and TNF-α levels during the normothermic reperfusion with hemadsorption. We transplanted all livers and kidneys from DCD donors without significant compliances.
Keywords
Introduction
In the last decades, the shortage of organs available for transplantation has encouraged the expansion of the donor pool by including the use of extended criteria donors (ECDs) such as donation after circulatory death (DCD).1,2 In Italy, the “no-touch interval” lasts for 20 min, much longer than the worldwide practice of 5 min. It prolongs Warm Ischemia Time (WIT) with potentially adverse effects on the process of donation and transplantation. To limit organ impairment, WIT should not exceed 50 min. WIT is considered to start when systolic blood pressure falls below 50 mmHg and continues until the beginning of the extracorporeal normothermic regional perfusion (NRP), necessary for organ recovery performed with Extracorporeal membrane oxygenator (ECMO).3,4 The reperfusion phase leads to a reperfusion syndrome characterized by a massive release of cytokines and free radicals through various mechanisms, which can be measured in both, blood and potential transplant organs.5 –7 To modulate the immune response in order to preserve organ function and consequently expand the donor pool would be a smart aim. Apart from immune modulating drugs, potentially having numerous adverse effects, blood purification therapy by the use of hemofiltration or hemoadsorption techniques have already been used in the setting of brain-dead donors and proved feasible and safe. 8 The applied CytoSorb hemoadsorption device (CytoSorbents, USA) was initially intended for the use in patients with elevated cytokine levels, as it is the case for generalized hyperinflammatory states of infectious (e.g. sepsis) but also non-infectious origin (e.g. cardiac surgery).9,10 Severals of publications reported on its innate ability to reduce inflammatory parameters (C-reactive protein [CRP], procalcitonin [PCT], Interleukin [IL]-6, tumor necrosis factor [TNF]-α). 11
This observational pilot paper describes a case series of DCD donors measuring inflammatory cytokine levels under hemoadsorption treatment during NRP.
Case reports
We describe 8 DCD donors of liver or kidneys in our center from 2018 to 2019 years, treated with hemoadsorption during NRP. Mean age was 58.1 ± 6.2 years. There were no evident critical conditions and no liver or kidney dysfunction was known. We enrolled three patients with post cardiac arrest syndrome and five patients with cerebral hemorrhagic stroke. All DCD donor subjects presented with poor neurological outcomes instrumentally and clinically documented. All DCD were managed with ECMO with external pump an average of blood flow 364 ± 165 ml/min with an average reperfusion time of 169.25 ± 168 min. The no touch period was of 20 min and the NRP started late 10 min of declaration of deaths.
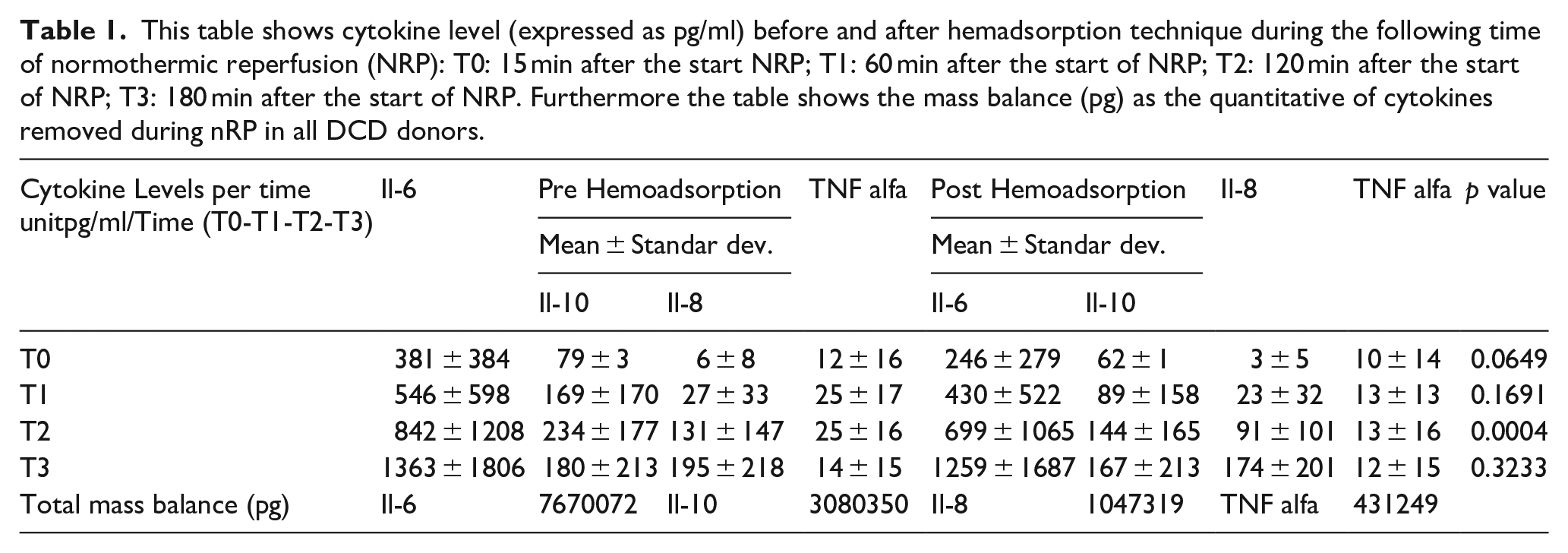
The personal consent to donation, or family member’s decision, was collected, and we managed subjects following Italian law: all decision underwent a shared decision making process. 12 After the declaration of cardiac death, we performed NRP through cannulation of the femoral artery and vein. Later, we placed a Fogarty catheter into the contralateral femoral artery, followed by heparin administration and occlusion of the supra celiac aorta to exclude the supradiaphragmatic circle. The cannulas were connected through an ECMO composed of a centrifugal pump, an oxygenator, and a heat-cooler exchanger. Regional perfusion was performed under normothermic conditions (37°C) using autologous donor blood. NRP was performed in combination with a CytoSorb® adsorber. The CytoSorb cartridge was connected to the primary ECMO circuit (cartridge blood inlet in the positive pressure post-oxygenator, cartridge blood outlet in negative pressure pre-pump). We measured cytokine mass balance (MB) as well as total removal ratio (RR). Total RR is the difference between median pre and post adsorption cartridge IL-6/IL-8/IL-10/TNF-α values. MB represents the difference between pre and post adsorption cartridges median IL-6/IL-8/IL-10/TNF-α values multiplied by median NRP flow and median perfusion time. We performed a longitudinal analysis across the different phases of reperfusion (ANOVA Variance analysis) before and later the hemadsorption, each patient was its control. We also estimated area under the curve for MB during NRP phases. We observed a reduction before and after hemadsorption, significant for IL-8 levels for all entire reperfusion phases, differently, IL-10 and TNF-α levels decreased during the main phases of NRP (Table 1 and Figure 1). We transplanted all livers and kidneys from DCD donors. Receiving patients spent less than 3 days in the intensive care unit and the mean number of days of hospitalization was below 14 days. None of these organs presented with primary non-function or histological necrosis signs. None of the patients underwent renal replacement therapy during his hospital stays. No apparent device-related adverse events occurred during NRP perfusion. At the 1-year follow-up, we did not observe any significant complications such as graft rejection or liver stenosis ducts.
This table shows cytokine level (expressed as pg/ml) before and after hemadsorption technique during the following time of normothermic reperfusion (NRP): T0: 15 min after the start NRP; T1: 60 min after the start of NRP; T2: 120 min after the start of NRP; T3: 180 min after the start of NRP. Furthermore the table shows the mass balance (pg) as the quantitative of cytokines removed during nRP in all DCD donors.
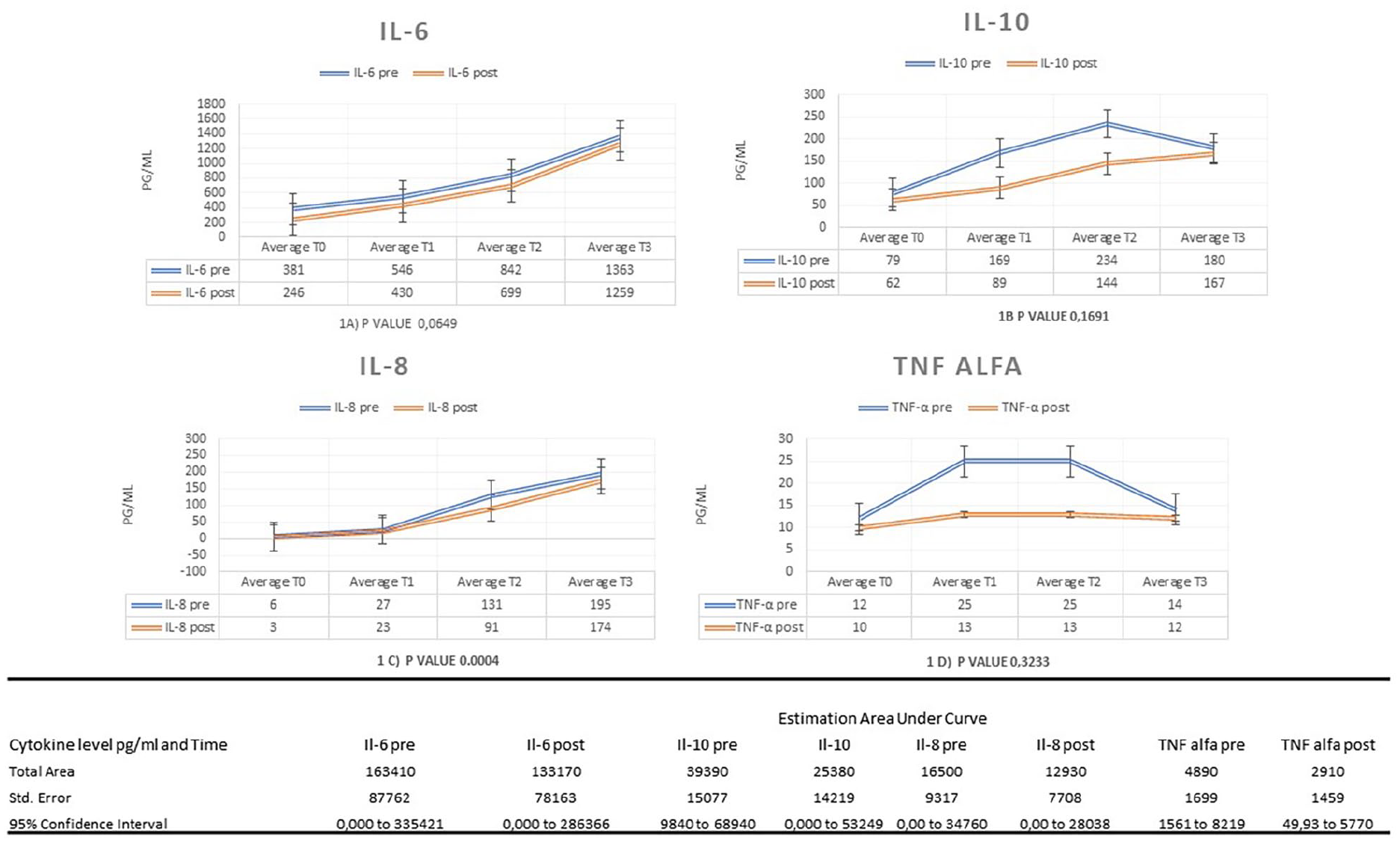
This figure shows cytokine level (expressed as pg/ml) before and after hemadsorption technique during the following time of normothermic reperfusion (NRP): T0: 15 min after the start NRP; T1: 60 mins after the start of NRP; T2: 120 min after the start of NRP; T3: 180 min after the start of NRP. Area under the curve estimated before and after NRP showed a decreased level of cytokine mass balance later the hemadsorption.
Discussion
Abdominal organ perfusion with a dedicated extracorporeal system is fundamental to allow organ recovery in the setting of DCD donation. Inflammation plays a crucial role in organ transplantation. Inflammatory changes occur in the transplanted organ at the time of transplant operation due to tissue trauma as well as ischemia/reperfusion injury and cytokines play a central role in mediating these changes. The specific inflammatory changes may not only affect graft function, but influence graft immunogenicity and adhesion molecule expression and, thus, vulnerability to rejection. 13 We decided to add a CytoSorb hemoadsorber to the normothermic regional perfusion, a device able to adsorb inflammatory mediators and other toxic metabolites such as bilirubin, bile acids, and ammonia. 14 The target is to reduce the inflammatory component, increase the number of organs suitable for transplantation (liver and kidneys), and improve their quality. 15 NRP has been proven to limit ischemic injury and allow for organ assessment before transplantation and is considered the most effective method of preservation and functional evaluation of abdominal organs in DCD donors. 16 With the rationale to control the excessive production of inflammatory molecules, typical of extended WIT and responsible for organ deterioration and primary graft dysfunction, it is hypothesized that the combination of NRP with CytoSorb® allows a reduction in cellular oxidative damage, assessed by a decrease in proinflammatory substances as happened in different settings. 17 Our model shows encouraging data with a potential positive effect of hemadsorption to improve organ quality; which, however, depends on many variables.
We observed increasing levels for several cytokines over time. This phenomenon had already been described by Kellum and co-workers, concluding an ongoing production of these inflammatory mediators. However, when comparing pre-adsorber inlet and post-adsorber outlet levels, we saw a substantial removal of IL-10 and TNF-α levels during normothermic reperfusion with hemadsorption suggesting an effective removal by the device with no evidence of a saturation effect. Whether the increase would have been even higher without the hemadsorption can only be hypothesized, but the increase rate in measured cytokines was less than expected from untreated cases.5,18 If this translates into improved clinical outcomes, for example, short-term organ function, is questionable, given the uncontrolled character of this observational pilot case series. Cytokines play a crucial role in the pathogenesis in all syndromes with ischemia/reperfusion injury, and DCD setting presents the same problem, in fact an artificial organ reperfusion restores with a high production of cytokines release. 19 During the reperfusion phases, we observed an increased level of pro-inflammatory and anti-inflammatory cytokines such as Il-6, Il-8, Il 10 for the reasons, the reperfusion syndromes, and the surgical stress related to a surgical operation for organ donation. The TNF-α decreased at the end of the procedure and this could be linked to the end of the surgical operation and the reduction of the main cell source of productions such as macrophages and T cells, NK cells, mast cells. 20 At the end of the procedure, we observed a possible exhaustion of hemadsorption, but these are preliminary considerations, and more data are necessary to better understand this process. Actually, there is no a validated level of acceptable value for the cytokine concentration to limit an organ impairment.
This study has some limitations. First, due to its retrospective character. However, this is the first series of DCD donors treated with ECMO and the Cytosorb® adsorber, representing a novelty in this setting of patients, although all results should be confirmed in larger studies. The rate of rejections and the absence of histological findings of necrosis are promising signs of acceptable quality of organs.
Conclusion
In this observational pilot case series, the use of hemadsorption during normothermic reperfusion in 8 DCD donors of liver and kidneys was associated with a reduction of IL-10 and TNF-α levels), accompanied by a reduction in blood lactate levels while all donor organs could be transplanted without complications or primary non-function. These results may serve as a first in human validation toward a strategy to improve organ and to increase organ availability for donation and reduce the waiting list. These encouraging results could be used to generate hypothesis and to calculate sample sizes in future large prospective studies.
Footnotes
Author contributions
Stefano Baroni, head of research, writing of the paper. Andrea Marudi, manuscript revision. Simone Rinaldi, data analysis. Silvia Ghedini, writing of the paper. Paolo Magistri, writing of the paper. Chiara Dallai, collection of data. Tiziana Olivieri, collection of data. Marta Talamonti, collection of data. Jessica Maccieri, data analysis. Gian Piero Guerrini, manuscript revision. Fabrizio Di Benedetto, manuscript revision. Elisabetta Bertellini, manuscript revision.
Dataset
Dataset is available upon request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics
The research was conducted ethically in accordance with the World Medical Association of Helsinki. Ethic statement Protocol AOU Modena 25194-2021
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.